Back to Journals » Journal of Pain Research » Volume 13
Effects of Trigger Point Dry Needling on Neuromuscular Performance and Pain of Individuals Affected by Patellofemoral Pain: A Randomized Controlled Trial
Authors Ma YT, Li LH, Han Q, Wang XL, Jia PY, Huang QM ![]() , Zheng YJ
, Zheng YJ
Received 28 November 2019
Accepted for publication 8 June 2020
Published 7 July 2020 Volume 2020:13 Pages 1677—1686
DOI https://doi.org/10.2147/JPR.S240376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Yan-Tao Ma, 1, 2,* Li-Hui Li, 2, 3,* Qi Han, 1 Xiao-Lei Wang, 1 Pei-Yu Jia, 1 Qiang-Min Huang, 2 Yong-Jun Zheng 1
1Department of Pain Management, Huadong Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China; 2Department of Sport Rehabilitation, School of Kinesiology, Shanghai University of Sport, Shanghai, People’s Republic of China; 3School of Medicine, Southern University of Science and Technology, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong-Jun Zheng; Qiang-Min Huang Email [email protected]; [email protected]
Purpose: To investigate the effects of trigger point dry needling (TrP-DN) on exercise-induced patellofemoral pain syndrome (PFPS).
Patients and Methods: In this randomized, single-blind, parallel-group trial, 50 patients with PFPS were randomly allocated to the following two groups: the TrP-DN group (n = 25) and the Sham needling group (n = 25). Patients in both groups were asked to perform a stretching exercise of the quadriceps daily after needling. The needling group received a single session of TrP-DN to trigger points (TrPs) in the vastus medialis oblique (VMO), vastus lateralis (VL), and rectus femoris muscles (once a week for 6 weeks), and the Sham group received placebo needling. Visual analogue scale (VAS) for pain intensity and Kujala questionnaire for the functional status were assessed before treatment, 3 and 6 weeks after treatment, and at the 3-month follow-up. The ratio of the myoelectric amplitude of the vastus medialis oblique and vastus lateralis muscles (VMO/VL) was assessed before treatment and 6 weeks after treatment.
Results: There was no significant difference in the general data between the two groups. The VAS scores and Kujala scores in the TrP-DN group were significantly improved and increased at the 3-week treatment visit, 6-week treatment visit, and 3-month follow-up compared to the scores before treatment; and the scores in the Sham group were only significantly improved at the 3-week treatment visit, and 6-week treatment visit. VAS scores in the TrP-DN group were significantly lower and Kujala scores were significantly higher at the 6-week treatment visit and the 3-month follow-up compared to those in the Sham group. The VMO/VL ratio in the TrP-DN group was significantly increased at the 6-week treatment visit compared to that before treatment.
Conclusion: TrP-DN at the quadriceps combined with stretch can reduce the pain, and improves the clinical symptoms and function, the VMO/VL ratio, and the coordination of VMO and VL in patients with PFPS.
Keywords: patellofemoral pain syndrome, myofascial trigger points, stretching
Corrigendum for this paper has been published
Introduction
Patellofemoral pain syndrome (PFPS) is one of the most common forms of knee pain in adults under the age of 40.1 It has been reported that almost 2530% of all injuries seen in sports medicine clinics and up to 40% of clinical visits for knee problems are attributed to PFPS. PFPS accounts for 3318% of all knee injuries in female and male athletes, respectively.2,3 Patellofemoral pain is mainly characterized by diffuse retropatellar and peripatellar pain that is aggravated with squatting, prolonged sitting, and stair activities.4 Its impact is profound, often reducing the ability to exercise, physical activity, and work-related activities.5 As a persistent musculoskeletal condition that is no longer considered self-limiting, PFPS is a refractory condition that may persist for many years and is a likely contributor to long-term patellofemoral osteoarthritis.6
Despite the prevalence of the disorder, the etiology of PFPS is poorly understood.7 A number of abnormal biomechanical and neuromuscular factors may contribute to increased stress on the patellofemoral joint, which, in turn, can ultimately lead to pain and dysfunction.8 Among the factors influencing the PFPS, quadriceps muscle insufficiency is one of the most studied factors. Numerous studies have proven that quadriceps muscle insufficiency (rectus femoris, vastus medialis, and vastus lateralis) may cause pain, myofascial trigger point, and muscle strain.9 Generally, any factor that leads to disruption of the extensor mechanism of the knee can reduce muscle strength and cause abnormal patellar tracking and it can finally lead to PFPS.8,10 Specifically, because the medial and lateral components of the quadriceps exert different mediolateral forces at the patella, their unbalanced activation may alter the pressure distribution across the patellofemoral joint and patellar kinematics.11
A widely investigated indicator of coordination between vastus muscle activation in PFPS is the relative timing of activation of vastus medialis oblique (VMO) and vastus lateralis (VL) muscles during movement. However, a systematic review has only found a trend towards delayed activation of VMO relative to VL mainly due to the large amount of unexplained variability in the study. Although timing measurements are readily available and they provide valuable information, they only identify the time differences in muscle activation. Although timing measurements can be easily obtained, they only recognize temporary differences in muscle activation. However, the force exerted by the muscle is mainly determined by the number of effective motor units (MU) and the rate of discharge, Therefore, altered neural drive of VMO and VL may be related to PFPS.
Clinical practice guidelines for the management of patients with PFPS recommend multimodal intervention programs, which include strengthening exercises of the hip and knee musculature, patellar taping, patient education, and activity modification. However, according to the results of the systematic review, the effectiveness of these interventions is limited.12 Trigger points (TrPs) are defined as hypersensitive spots within the taut bands of the skeletal muscle, which are painful on palpation and usually give rise to referred pain.13 Travell and Simons described TrPs in three quadriceps muscles, which, when palpated, could generate the peripatellar and anterior knee pain, which is the characteristic of PFPS.14
It has been confirmed that needling the TrPs can effectively reduce the pain and disability of PFPS.5,15 However, it is still unknown whether needling the PFPS quadriceps trigger points can change the ratio of the myoelectric amplitude of the medial oblique and lateral muscles (VMO/VL).
Therefore, the purpose of this study was to determine whether trigger point dry needling (TrP-DN) is more effective in reducing pain and disability and promoting coordination of the medial oblique and lateral femoral muscles than placebo treatment in individuals with PFPS. We hypothesized that females in the TrP-DN group would experience greater improvements in their symptoms and promotion of coordination of motor unit activation of the medial oblique and lateral femoral muscles than those assigned to the Sham needling group.
Patients and Methods
Study Population
Between March 2017 and September 2017, 50 patients with PFPS satisfied all the eligibility criteria, and they agreed to participate in the study. They were simply randomized to the TrP-DN group (n=25) and the Sham needling group (n=25) by an independent researcher using Microsoft Excel 2013 via computerized random numbers. The flow chart of the procedures involving study participation and follow-up is illustrated in Figure 1. As shown, 2 participants randomized to the Sham needling group withdrew from the study due to poor efficacy (Figure 1). The characteristics of the participants in the two study groups were assessed at baseline, and no significant differences were found in age, gender, height, weight, and body mass index between the two groups at baseline (Table 1). Data are presented as mean±SD. All variables were normally distributed. No significant complications related to dry needling were observed at the baseline.
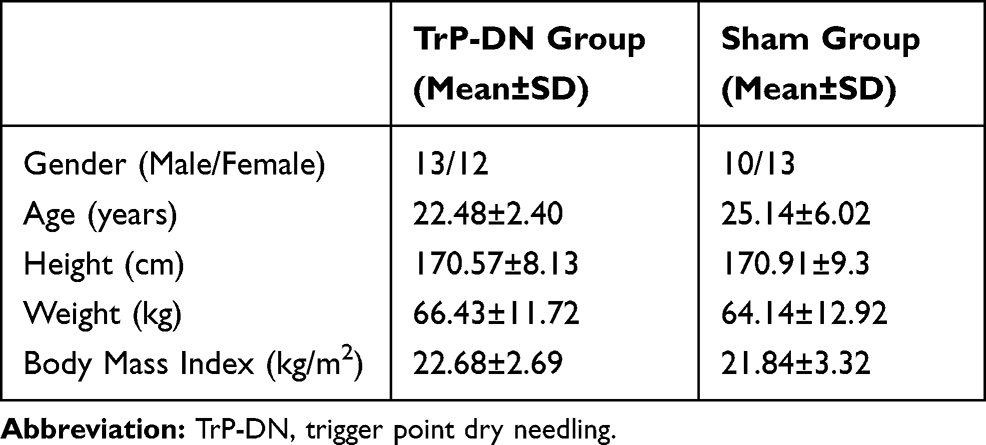 |
Table 1 Age, Gender, Height, Weight, and Body Mass Index Between the Two Groups at Baseline |
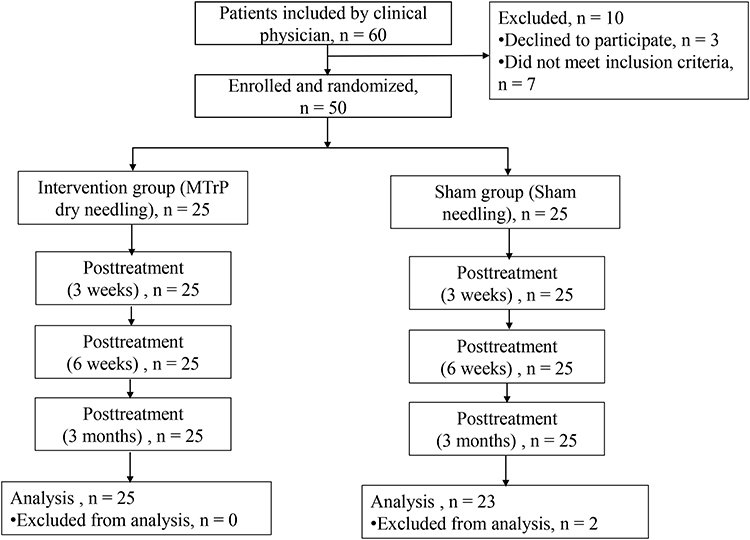 |
Figure 1 The enrollment and outcomes of patients. |
A total of 50 participants were recruited from the Pain Clinic of Shanghai Sports Institute and the Pain Department of Shanghai Hudong Hospital between March 2017 and September 2017. The study was approved by the Ethics Committee of Shanghai Sports Institute (approval code: 2,017,017), and it was prospectively registered (www.chictr.org.cn; ChiCTR-INR-17,011,560) and this study was carried out in accordance with the World Medical Association’s Declaration of Helsinki (1964). All participants were informed about the objectives of the study, and they signed the Informed Consent Form.
Power analysis was conducted using the G*Power software (Version 3.1.9.2). According to the results of the pre-experiment, the sample size was dependent on the difference in pain, functional score, and surface EMG before and after treatment. Assuming a two-tailed Wilcoxon signed-rank test at the 0.05 significance level with a statistical power of 80%, this analysis showed that 23 subjects would be required in each group. Considering the risk of dropouts; an expected dropout rate of 5%, the sample size was increased by 20% in each group, and the final sample size was determined as 25 subjects in each group.
Randomization
The subjects with PFPS were randomly assigned to the dry needling group (TrP-DG) or the Sham needling group (SG). Concealed allocation was conducted using a computer-generated randomized table of numbers created by an external statistician. Individual and sequentially numbered index cards with random assignment were prepared. The index cards were folded and placed in sealed opaque envelopes. Another researcher opened the envelope and proceeded with allocation. Treatment allocation was revealed to the participants after the collection of baseline outcomes. Clinicians collecting the outcomes were blinded to group assignment.
Inclusion criteria: The ages of all participants ranged from 18 to 40 years and they had a clinical diagnosis of PFPS. The diagnosis of PFPS was determined based on a complaint of retropatellar or anterior knee pain provoked by two or more of the following activities: squatting, stair ascent, stair descent, prolonged sitting, kneeling or isometric quadriceps contraction, and exhibition of at least 1 active TrP reproducing their symptom. Individuals were excluded if they had a history of prior knee surgery, any competing knee pathology (meniscal tears, patellar tendinopathy, ligamentous sprains, and osteoarthritis), any systemic disease and/or connective tissue disorders, or signs of lumbosacral nerve root compression. Individuals were also excluded if they had received acupuncture, injection, or dry needling treatment for the knee or quadriceps femoris muscles within the prior 6 months were currently taking anticoagulant medications, had a medical history of a bleeding disorder, or if they were pregnant. Participants were also required to have a minimum pain score of three on the numerical pain scale.
Exclusion criteria: The criteria were as follows: participants who had received any treatment for PFPS within the previous 3 months, history of lower extremity surgery, lower extremity trauma in the past year, and/or fracture, presence of musculoskeletal diseases, such as acute-herniated disc or spondylolisthesis, any structural disturbances of the lower extremity (eg, osteoarthritis of the hip or knee joints, prosthesis), or central or peripheral neurological pathology and any chronic disease (eg, diabetes mellitus). Patients with a fear of needles or a coagulation disorder were excluded to avoid any potential risk in the needling group. Screening was performed by a physiotherapist with >2 years of clinical experience in musculoskeletal assessment.
Interventions
The diagnosis of active myofascial trigger points (MTrPs) was based on the following criteria: (1) a palpable, hypersensitive tender spot in a taut band, (2) pain reproduced by compression of the tender spot, (3) local twitch response on muscle palpation, and (4) referred and spontaneous pain elicited by firm compression.16
After the baseline examination, manual palpation of three superficial quadriceps femoris muscles (vastus medialis, rectus femoris, and vastus lateralis) ipsilateral to the symptomatic knee was performed to detect the presence of TrPs in the DG. The TrP-DN intervention was performed with 0.35 × 40 mm disposable stainless-steel needles (Wujiang Jiachen Acupuncture Equipment Co., Ltd, Jiangsu, China) into three of the four quadriceps femoris muscles (vastus medialis, rectus femoris, and vastus lateralis). Once the active TrP was located, the “clean technique” was used throughout the treatment procedure, which included hand washing, use of latex-free examination gloves, and skin-surface preparation with an alcohol wipe. In the current trial, the fast-in and fast-out technique described by Hong was applied.17 The needle was inserted into the skin at the TrP area until the first local twitch response was obtained. The depth of the needle depended on the muscle and it ranged from 15 to 20 mm for the vastus medialis and from 30 to 35 mm for the vastus lateralis muscle and rectus femoris. Once the first local twitch response was obtained, the needle was moved up and down (35 mm vertical motions with no rotations) at approximately 1 Hz until no more local twitch responses were elicited.
The TrP-DN group received treatment at the trigger points. The methods of choosing the trigger points were the same. For the SG group, similar stainless steel needles (0.35*75 mm) were used, but the tips had been cut off to prevent the needle penetrating into the skin and the cut ends were manually smoothed with a sandpaper under clean conditions. The acupuncturist pretended to insert the needle and to use the sparrow pecking technique, and then he removed the needles. TrP-DN was performed by two clinicians who had received 4 years of dry needling training. All subjects were asked to perform one repetition of a standing static quadriceps stretch for 60 s, and then repeat it three times daily. The subjects were asked to stand on the healthy side, with the side of the hand holding the table or the wall and the other hand grasping the affected side of the ankle, and they were asked to stretch backwards until the affected quadriceps or knee joint had a feeling of soreness, static maintenance for 60 s, and then repeat it three times daily.
Surface electromyography (SEMG) signals were recorded using an sEMG system (MyoMove-EOW, China Shanghai Nuocheng) operating at a sampling rate of 1000 Hz and bandpass filter frequency of 10–500 Hz. The sEMG signals of the medial oblique and lateral femoral muscles were concentrically recorded at a speed of 60º/s by an isokinetic dynamometer (CON-TREX, Physiomed, Germany) before the treatment and at 1 week after the sixth treatment.
All subjects were not allowed to perform any strenuous exercise within 24 hrs before participating in the electromyography test. The painful side was used as the test subject, if both sides were painful, and the test was performed on the most painful side. Before the test, the test precautions were explained to the patients in detail, and they were asked to perform 5 mins of warming up for the bicycle and static muscle stretching of the quadriceps and hamstrings (3 times, 1 min/time). The isokinetic concentric strength-open kinetic chain of the knee joint at 60°/s was measured by an isokinetic dynamometer (CON-TREX, Physiomed Germany), and the synchronous electromyography collection test was performed.
The patients were seated upright with 85° hip flexion and were restrained in the chair by a 4-point seatbelt across the torso. A strap was fixed midway across the thigh. The axis of rotation of the dynamometer was aligned with the assumed axis of rotation of the knee. The length of the lever arm was individually adjusted to the length of each participant’s leg. Following direct measurement of the mass of the lower limb lever system at 0°of knee extension, gravity correction procedures were applied to reduce the risk of inaccurate data. The resistance pad of the shank of the dynamometer was fixed to the lower leg at 2cm above the malleolus externus.
Subjects were required to wear loose short pants and expose the thighs during the experiment. Electrodes (LT-301 Ag/Ag Cl) were attached to two belly muscles (the VMO and VL) and were placed along the longitudinal axis of the muscle fibers, the interelectrode distance was 2 cm, and the electrodes and wires were secured with an adhesive tape. The electrode for VL was positioned on the line from the anterior superior iliac spine to the superolateral border of the patella and was attached at 10 cm from the superolateral border of the patella and orientated 15° to the vertical. The electrode for VMO was positioned at 4 cm from the superomedial border of the patella and was orientated 55° to the vertical. The electrode placements were based on previous studies.18,19 Before the electrodes were attached to the muscles, the skin hairs were shaved and the skin was wiped with 75% alcohol swabs to reduce the electrical impedance. The ground electrode was placed over the fibulae capitulum.
EMG signals were normalized to a maximal voluntary isometric extension contraction at 60° of knee flexion for 5 s. The AEMG produced during the contraction was used as a reference for the calculation, and the outcome used to calculate the VMO/VL ratio was a percentage of two AEMGs. To familiarize with the testing procedure and the dynamometer, each subject performed a 5 repetitions trial session at 60◦/s in a concentric mode. Afterwards, three concentric isokinetic trials at 60◦/s were performed with 5 repetitions, and the participants were verbally encouraged and required to perform the session with maximum efforts. Electromyographic (EMG) activity of the VMO and VL was recorded during testing per trial. Different sets were separated by 120 s rest periods. After testing, the participants were instructed to perform a cooldown and stretching session to prevent injury. All signals were analyzed by Shanghai Nuocheng Mainproject1.0 processing software, and the waveform was rectified and normalized to extract the average electromyogram (AEMG) of the EMG signal.20
Outcome Measures
Visual Analog Scale
The VAS is an appropriate and sensitive scale for the clinical and experimental evaluation of pain intensity. The score on the 100-point scale ranges from 0 (no pain) to 100 (worst imaginable pain). Participants were instructed to score their pain and circle the appropriate number on the VAS form before and after each treatment intervention.
The Kujala Patellofemoral Scale
The Kujala Patellofemoral Scale is a valid and reliable questionnaire to evaluate functioning in patients with PFPS. The scores range from a maximum of 100 to a minimum of 0, with lower scores indicating greater pain and disability.
Vmo/Vl
The mean myoelectric amplitude ratio (AEMG%) was measured by the AEMG of the VMO over that of the VL.
Statistical Analysis
All data were analyzed using the Statistical Package for Social Sciences (SPSS) V.22.0. The mean and SD for each quantitative variable were calculated after confirming normal distribution of the data using the Shapiro–Wilk test. Independent t-test was used to compare differences in the underlying data of the subjects included. Two-way repeated ANOVA analysis together with Eta squared test and Cohen’s d for Bonferroni’s comparisons, with a Post-hoc Bonferroni correction were used for data analysis. A P-value of <0.05 was considered to be statistically significant.
Results
As shown in Figure 2, the VAS scores in the TrP-DN group were significantly decreased at the 3-week treatment visit, 6-week treatment visit, and 3-month follow-up compared to those before treatment (VAS: 46.67±11.97 vs 25.71±10.76 vs 10.48±9.21 vs 6.19±12.84, p < 0.05); the scores in the Sham group were only significantly improved at the 3-week treatment visit, and the 6-week treatment visit (VAS: 42.38±7.68 vs 30.48±9.73 vs 24.77±7.5, p < 0.05). However, there was no significant difference in the VAS score at the 3-month follow-up compared with that at the pre-treatment time point (p>0.05). The VAS scores in the TrP-DN group were significantly lower at the 6-week treatment visit and the 3-month follow-up compared to those in the Sham group (VAS: 10.48±9.21 vs 24.77±7.5; 6.19±12.84 vs 33.81±12.03, p < 0.05).
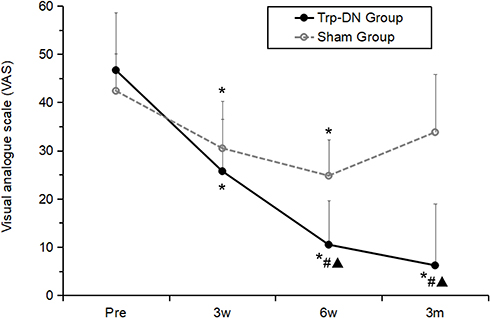 |
Figure 2 The VAS scores in the TrP-DN group and the Sham group. Notes: *Compared with the same group at pre-treatment p<0.05, #Compared with the same group at 3 weeks after treatment p<0.05, ▲Compared with the control group p<0.05. n=25 in the TrP-DN Group; n=23 in the Sham group. Abbreviations: TrP-DN, trigger point dry needling; Pre, Pre-treatment; 3w, 3 weeks after treatment; 6w, 6 weeks after treatment; 3m, 3 months after treatment. |
As shown in Figure 3, the Kujala score in the TrP-DN group was significantly increased at the 3-week treatment visit, 6-week treatment visit, and 3-month follow-up compared to those before treatment.
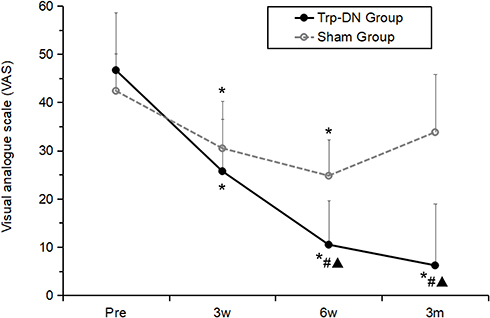 |
Figure 3 The Kujala scores in the TrP-DN group and the Sham group. Notes: *Compared with the same group at pre-treatment p<0.05, #Compared with the same group at 3 weeks after treatment p<0.05, ▲Compared with the control group p<0.05. n=25 in the TrP-DN Group; n=23 in the Sham group.Abbreviations: TrP-DN, trigger point dry needling; Pre, Pre-treatment; 3w, 3 weeks after treatment; 6w, 6 weeks after treatment; 3m, 3 months after treatment. |
(Kujala: 66.42±9.95 vs 83.47±8.8 vs 90.68±7.05 vs 92.21±7, p < 0.05); and in the Sham group, the scores were only significantly improved at the 3-week treatment visit and 6-week treatment visit (Kujala: 68.05±8.91 vs 75.95±8.46 vs 77.85±8.03, p < 0.05). However, there was no significant difference in the Kujala score at the 3-month follow-up compared with that at the pre-treatment time point (p>0.05). Comparison between groups showed that there was no significant difference between the TrP-DN group and the Sham group before treatment (p>0.05), but the Kujala scores were significantly higher at the 6-week treatment visit and the 3-month follow-up compared to those in the Sham group (Kujala: 90.68±7.05 vs 77.85±8.03; 92.21±7 vs 74.75±8.58, p < 0.05).
With respect to VMO/VL, there was a significant increase in the TrP-DN group at 6 weeks of treatment (0.91±0.04 vs 0.79±0.02, p < 0.05), while the Sham group showed no significant difference (p>0.05) after 6 weeks of treatment compared with pre-treatment (p>0.05). The comparison between the groups showed that there was no significant difference between the TrP-DN group and the Sham group before treatment (p>0.05). The dry needling group showed a significant increase after 6 weeks of treatment (0.91±0.04 vs 0.79±0.04, p < 0.05).
Discussion
This study shows that the effectiveness of TrP-DN treatment on PFPS was significantly better than that of Sham treatment. From the data collected, the VAS score and Kujala score of the dry needling group were significantly better than before treatment. The trigger point was a contracture nodule of muscle fiber formation on the skeletal muscle, which could be active or latent, and the active trigger point was related to spontaneous pain. When palpated, the patient’s local pain or referred pain may be completely or partially reproduced. Travell and Simons described that the trigger points of the rectus femoris, lateral femoral muscles, and the medial femoral muscles in the quadriceps muscle can produce referred pain in the anterior and posterior tibial features, which are characteristic of PFPS when palpated.13 In contrast, latent trigger points do not produce referred pain.21
Current trigger point studies have focused on the histopathology and electrophysiology, and according to Simons and Mense, long-term eccentric contraction or concentric contraction muscle activity leads to sustained and excessive release of acetylcholine (Ach) at the motor endplate, causing contraction of the sarcomere, forming a pile of bead-like contracture nodules, while contracting nodules will squeeze the local capillary network, hinder blood circulation, resulting in insufficient energy supply; thus, leading to an energy crisis.22–24 Compressed tissue releases sensitizing chemicals, such as serotonin, bradykinin, and substance P, and stimulates nociceptors, causing localized pain and referred pain.
Accurate positioning and needling of these nodules can effectively block this vicious cycle. There is ischemia in the trigger point area. The study under Doppler ultrasound and infrared thermography showed that the blood flow is increased and the local microcirculation is improved after the TrP-DN.25,26 The study by Liu confirmed that the acetylcholine reactant and acetylcholinesterase in the region of the precise needling trigger point were markedly increased.27
Thomas compared the immediate and 72 hrs pain and function of the dry needling group and the placebo needling group after treatment of PFPS.28 The results showed that the two groups had significant improvement compared with that before treatment, but due to the shorter time period and as all participants were instructed to follow a basic home exercise program of isometric quadriceps femoris contractions and quadriceps stretching exercises, the dry needling group was not significantly better than the Sham needling group.
However, studies by Hamideh et al have shown that physical therapy combined with dry needling is more effective for PFPS than simple physical therapy.14 A study by Shabnam showed that ischemic compression of the medial femoral muscle trigger point was significantly superior to manual therapy in the treatment of PFPS.29 Gemma also showed that physical therapy combined with dry needling can effectively alleviate PFPS pain and improve the muscle strength of the quadriceps.15
Dry needling treatment is usually supplemented with static stretching. Specifically, the goal of the dry needling technique is to accurately puncture the trigger point, while the target of the stretch is the muscle with the trigger point.30 Studies have shown that stretching can reduce the tension of the quadriceps muscle and decrease the reaction force that may be caused by increased muscle tone, especially during the extension of the knee joint.31 Hakkinen reported that stretching can reduce musculoskeletal pain by 94%.32 Budini et al tested 19 subjects for the tendon tap reflex (T-reflex), H reflex, and motor-evoked potentials in ankle flexors and extensors immediately, and at 5 and 10 min after 1 min static stretching, and the results showed that 1 min of static stretching primarily decreased the muscle spindle sensitivity and that skeletal muscle pain was significantly associated with increased muscle spindle sensitivity; therefore, static stretching for 1 min can reduce muscle spindle sensitivity and thus relieve muscle pain.33 In this experiment, the control group was a combination of Sham needling and stretching training. From the results, the VAS score and Kujala score of the control group showed good results in the middle stage, but they showed no further improvement in the later stage. The follow-up evidence showed that there was a recurrence trend. It can be seen that stretching the quadriceps contributes to the relief of pain in PFPS patients, but the effect is limited.
The mechanical balance between the lateral femoral and femoral oblique muscles is considered to be the most important factor between PFPS and quadriceps dysfunction. The lateral oblique and lateral femoral muscles of the quadriceps exert different lateral forces on the tibia, and their unbalanced activation may alter the patellofemoral trajectory and the pressure distribution on the tibial joint.11 Currently, the imbalance study of VMO and VL is mainly reflected by the myoelectric amplitude of the electromyogram. A systematic review by Chester et al found that VMO has a tendency to delay activation relative to VL, but there is great variability and unreliability.34
It is known that the production of muscle strength is related to the function and anatomy of muscles, and it has an important relationship with the recruitment of motor units.35 Therefore, the activation rate of the motor unit by the magnitude of myoelectricity becomes an important indicator of the response of VMO and VL. Numerous studies have confirmed the imbalance of VMO/VL relative to normal in patients with PFPS, consistent with the results of this study.36,37 At present, many treatments have focused on the internal oblique muscles. It is believed that the functional damage of VMO causes the weakening of the muscle strength of VMO and it cannot effectively resist the outward force of VL.38 Some studies have also suggested that pain and muscle weakness in VMO are actually inhibition of reflexes in VMO caused by active myofascial trigger points in VL.39 However, according to the studies by Gallina and Tucker, pain and function of the muscle is mutually compatible.25,26 Pain does not cause inhibition of the quadriceps muscle, or the interaction of VL enhancement and VMO attenuation. In fact, to complete the target movement, the activation of the motor unit of the painful muscle changes.
Specifically, trigger points in the muscle cause muscle dysfunction, weakened muscle strength, and reduced cross-sectional area of the muscle fiber, and to better complete the movement of the quadriceps muscle, by compensating for muscle dysfunction, more motor units should be activated.24 However, VL has a larger cross-sectional area than VMO and it has a greater mechanical advantage in the sagittal plane; therefore, it causes more activation and produces more force.40 In the current study, the isokinetic muscle strength test was used to allow the patients with PFPS to complete the concentric contraction of the knee joint at 60°/s, which can ensure the maximum torque of the patient at every angle of contraction. In the test, the maximum torque of the patient can be guaranteed at each angle of the contraction, and at that time, the acquired surface electromyogram signal can well reflect the skeletal muscle function of the subject. The average electromyogram (AEMG) selected in this experiment can reflect the average level of VMO and VL discharge during the same time, regardless of the length of time.
The results of the study showed that there was no significant difference in the VMO/VL ratio of AEMG before and after treatment in the control group. The VMO/VL ratio of AEMG after treatment in the experimental group was significantly higher than that before treatment, and the comparison between groups after treatment showed that the VMO/VL ratio of the experimental group was significantly higher than that of the control group. Studies have shown that the trigger point causes abnormal release of acetylcholine at the neuromuscular junction, resulting in spontaneous electrical activity;, and therefore, the activation efficiency of muscle fibers in the motor unit decreases.41 Abbaszadeh found that dry needling can regulate the biochemical environment around the trigger point, reduce the leakage of acetylcholine, decrease the irritation of the endplates, and repair the damage of the neuromuscular junction.42 Therefore, based on the findings of this study, we believe that acupuncture at the quadriceps trigger point helps to restore the function and muscle strength of the VMO and avoids excessive activation of the VL motor unit.
The study by Zarei43 showed the added effect of dry needling to the gluteus medius (GM) and the quadratus lumborum (QL) along with regular strengthening exercise in female athletes with patellofemoral pain (PFP). The reason may be that the stability of the lumbar spine and hip joints is enhanced by treating the trigger points of the gluteal and lumbar quadriceps muscles, which improves the biomechanical relationship of the lower limbs, and then improves the abnormal trajectory and motion of reducing the load it bears. The reason may be that the stability of the lumbar spine and hip joints is enhanced by treating the trigger points of the gluteal and lumbar quadriceps muscles, which improves the biomechanical relationship of the lower limbs, and then improves the abnormal trajectory and reduces the load that it bears. The trigger point is also used to treat knee osteoarthritis, and Eleuterio’s44 study showed that the inclusion of DN into an exercise program does not reduce pain or disability in patients with knee osteoarthritis. Research by Sánchez-Romero45 also showed DN added to a therapeutic exercise program is not significantly better than the Sham-DN combined exercise group of older adults with knee osteoarthritis but they could neither exclude the effect of DN alone or the influence of exercise alone on KOA pain and disability. Another study showed that quadriceps vastus medialis TrP-DN in conjunction with a rehabilitation protocol in subacute patients with surgical reconstruction of complete anterior cruciate ligament (ACL) rupture increases the ROM and functionality.46
Limitations
There are some limitations to this experiment, The number of treated and active trigger points was not registered, which may have caused some differences in the number of trigger points treated in each group and there is a lack of supervision of the patient’s self-stretching. To cover ethical considerations, this study compared two treatment groups but it did not investigate the pure effect of superficial dry needling in comparison to the placebo method. In this experiment, only the VMO/VL ratio of the isokinetic muscle strength test at 60°/s angular velocity was studied, and the isokinetic test at other speeds and the test under isometric contraction conditions were not performed. More research and large sample size studies are needed to confirm the relationship between VMO/VL coordination and dry needling.
Conclusion
TrP-DN at the quadriceps combined with stretch can effectively alleviate pain, and improve the function and coordination of VMO and VL in patients with PFPS.
Data Sharing Statement
The authors confirm that the data underlying the findings described in this manuscript are available from the corresponding author upon reasonable request.
Acknowledgments
The present study was supported by the Department of Pain Management, Huadong Hospital key discipline (grant number H1153) and The Shanghai Science and Technology Commission Project (grant number 15DZ1940104) and The National Key R&D Program of Strategic Advanced Electronic Materials (grant number: 2017YFB0403803). We are grateful to the Shanghai University of Sport’s Citizen Physical Fitness Research Center for providing the isokinetic dynamometer and Dr. Qing-guang Liu from Tongji University for his help with EMG analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dey P, Callaghan M, Cook N, et al. A questionnaire to identify patellofemoral pain in the community: an exploration of measurement properties. BMC Musculoskelet Disord. 2016;17:1–11. doi:10.1186/s12891-016-1097-5
2. Witvrouw E, Callaghan MJ, Stefanik JJ, et al. Patellofemoral pain: consensus statement from the 3rd international patellofemoral pain research retreat held in vancouver, September 2013. Br J Sports Med. 2014;48:411–414. doi:10.1136/bjsports-2014-093450
3. Halabchi F, Abolhasani M, Mirshahi M, et al. Patellofemoral pain in athletes: clinical perspectives. Open Access J Sports Med. 2017;8:189–203. doi:10.2147/OAJSM.S127359
4. Crossley KM, Stefanik JJ, Selfe J, et al. Patellofemoral pain consensus statement from the 4th international patellofemoral pain research retreat, manchester. Part 1: terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures. Br J Sports Med. 2016;50:839–843. doi:10.1136/bjsports-2016-096384
5. Fernández-De-Las-Peñas C, Nijs J. Trigger point dry needling for the treatment of myofascial pain syndrome: current perspectives within a pain neuroscience paradigm. J Pain Res. 2019;12:1899–1911. doi:10.2147/JPR.S154728
6. Thomas MJ, Wood L, Selfe J, et al. Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: a systematic review. BMC Musculoskelet Disord. 2010;11:201. doi:10.1186/1471-2474-11-201
7. Doménech J, Sanchis-Alfonso V, Espejo B. Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain. Knee Surgery Sports Traumatol Arthroscopy. 2014;22:2295. doi:10.1007/s00167-014-2968-7
8. Clijsen R, Fuchs J, Taeymans J. Effectiveness of exercise therapy in treatment of patients with patellofemoral pain syndrome: systematic review and meta-analysis. Phys Ther. 2014;94:1697–1708. doi:10.2522/ptj.20130310
9. Dolak KL, Silkman C, Medina MJ, et al. Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: a randomized clinical trial. J Orthopaedic Sports Phy Ther. 2011;41:560–570. doi:10.2519/jospt.2011.3499
10. Barton C, Balachandar V, Lack S, et al. Patellar taping for patellofemoral pain: a systematic review and meta-analysis to evaluate clinical outcomes and biomechanical mechanisms. Br J Sports Med. 2014;48:417. doi:10.1136/bjsports-2013-092437
11. Lorenz A, Müller O, Kohler P, et al. The influence of asymmetric quadriceps loading on patellar tracking an in vitro study. Knee. 2012;19:818–822. doi:10.1016/j.knee.2012.04.011
12. Wilson T. The measurement of patellar alignment in patellofemoral pain syndrome: are we confusing assumptions with evidence? J Orthopaedic Sports Phy Ther. 2007;37:330–341. doi:10.2519/jospt.2007.2281
13. Kashyap R, Iqbal A, Alghadir AH. Controlled intervention to compare the efficacies of manual pressure release and the muscle energy technique for treating mechanical neck pain due to upper trapezius trigger points. J Pain Res. 2018;11:3151–3160. doi:10.2147/JPR.S172711
14. Simons DG, Mense S. Diagnosis and therapy of myofascial trigger points. Schmerz. 2003;17:419–424. doi:10.1007/s00482-003-0253-7
15. Espí-López GV, Serra-Añó P, Vicent-Ferrando J, et al. Effectiveness of inclusion of dry needling into a multimodal therapy program for patellofemoral pain: a randomized parallel-group trial. J Orthopaedic Sports Phy Ther. 2017;47:1–43. doi:10.2519/jospt.2017.7389
16. Liu L, Huang QM, Wang LB. Whether lidocaine or dry needling should be the favored treatment after meta analysis. J Bodyw Mov Ther. 2014;18:517–518. doi:10.1016/j.jbmt.2014.04.001
17. Hong C. Lidocaine injection versus dry needling to myofascial trigger point. The importance of the local twitch response. Am J Phys Med Rehabil 1994. 1994;73:256–263. doi:10.1097/00002060-199407000-00006
18. Chen S, Chang WD, Wu JY, et al. Electromyographic analysis of hip and knee muscles during specific exercise movements in females with patellofemoral pain syndrome: an observational study. Medicine. 2018;97:e11424. doi:10.1097/MD.0000000000011424
19. Cowan SM, Hodges PW, Bennell KL, et al. Altered vastii recruitment when people with patellofemoral pain syndrome complete a postural task. Arch Phys Med Rehabil. 2002;83:989–995. doi:10.1053/apmr.2002.33234
20. Canning CG, Ada L, O’dwyer N. Slowness to develop force contributes to weakness after stroke. Arch Phys Med Rehabil. 1999;80:66. doi:10.1016/S0003-9993(99)90309-X
21. Li LH, Huang QM, Barbero M, et al. Quantitative proteomics analysis to identify biomarkers of chronic myofascial pain and therapeutic targets of dry needling in a rat model of myofascial trigger points. J Pain Res. 2019;12:283–298. doi:10.2147/JPR.S185916
22. Simons DG, Travel JG. Myofascial Pain and Dysfunction: The Trigger Point manual.Volume1: Upper Half of Body. Baltimore: Williams&Wilkins; 1999:71–72.
23. Mense S, Simons DG, Hoheisel U, et al. Lesions of rat skeletal muscle after local block of acetylcholinesterase and neuromuscular stimulation. J Appl Physiol. 2003;94(6):2494. doi:10.1152/japplphysiol.00727.2002
24. Huang QM, Ye G, Zhao ZY, et al. Myoelectrical activity and muscle morphology in a rat model of myofascial trigger points induced by blunt trauma to the vastus medialis. Acupuncture Med. 2013;31:65–73. doi:10.1136/acupmed-2012-010129
25. Yen RH, Danoff J, Gebreab TM, et al. Poster 147: novel use of ultrasound imaging to investigate myofascial trigger points and the effects of dry needling: a case series. PM R. 2009;1:S167–S168. doi:10.1016/j.pmrj.2009.08.167
26. Dibai-Filho AV, Guirro RRDJ. Evaluation of myofascial trigger points using infrared thermography: a critical review of the literature. J Manipulative Physiol Ther. 2014;38:86. doi:10.1016/j.jmpt.2014.10.010
27. Qing-Guang L, Lin L, Qiang-Min H, et al. Decreased spontaneous electrical activity and acetylcholine at myofascial trigger spots after dry needling treatment: a pilot study. Evidence Based Complement Alternative Med. 2017;2017:1–7.
28. Golden A, King K, Morris WB, et al. Short-term effects of trigger point dry needling on pain and disability in subjects with patellofemoral pain syndrome. Int J Sports Phys Ther. 2018;13:462–473. doi:10.26603/ijspt20180462
29. Behrangrad S, Kamali F. Comparison of ischemic compression and lumbopelvic manipulation as trigger point therapy for patellofemoral pain syndrome in young adults: A double-blind randomized clinical trial. J Bodyw Mov Ther. 2017;21:554. doi:10.1016/j.jbmt.2016.08.007
30. Li LH, Huang QM, Barbero M, et al. Proteins and signaling pathways response to dry needling combined with static stretching treatment for chronic myofascial pain in a RAT model: an explorative proteomic study. Int J Mol Sci. 2019;20:E564. doi:10.3390/ijms20030564
31. Bishop MD, George SZ. Pain sensitivity and torque used during measurement predicts change in range of motion at the knee. J Pain Res. 2017;10:2711–2716. doi:10.2147/JPR.S150775
32. Häkkinen A, Kautiainen H, Hannonen P, et al. Strength training and stretching versus stretching only in the treatment of patients with chronic neck pain: a randomized one-year follow-up study. Clin Rehabil. 2008;22:592–600. doi:10.1177/0269215507087486
33. Budini F, Gallasch E, Christova M, et al. One minute plantar flexors’ static stretch transiently increases H-reflex excitability and exerts no effect on corticospinal pathways. Exp Physiol. 2017;102:901–910. doi:10.1113/EP086374
34. Chester R, Smith TO, Sweeting D, et al. The relative timing of VMO and VL in the aetiology of anterior knee pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2008;9(1):64. doi:10.1186/1471-2474-9-64
35. Hooten WM, Smith JM, Eldrige JS, et al. Pain severity is associated with muscle strength and peak oxygen uptake in adults with fibromyalgia. J Pain Res. 2014;7:237–242. doi:10.2147/JPR.S61312
36. Pal S, Besier TF, Draper CE, et al. Patellar tilt correlates with vastus lateralis: vastus medialis activation ratio in maltracking patellofemoral pain patients. J Orthopaedic Res. 2012;30:927–933. doi:10.1002/jor.22008
37. Owings TM, Grabiner MD. Motor control of the vastus medialis oblique and vastus lateralis muscles is disrupted during eccentric contractions in subjects with patellofemoral pain. J Orthopaedic Sports Phy Ther. 2003;33(1):60.
38. Powers CM. Patellar kinematics, part I: the influence of vastus muscle activity in subjects with and without patellofemoral pain. Phys Ther. 2000;80:956–964. doi:10.1093/ptj/80.10.956
39. Kowall MG, Kolk G, Nuber GW, et al. Patellar taping in the treatment of patellofemoral pain: a prospective randomized study. Am J Sports Med. 1996;24:61.
40. Gallina A, Hunt MA, Hodges P, et al. Vastus lateralis motor unit firing rate is higher in females with patellofemoral pain. Arch Phys Med Rehabil. 2018;99:907. doi:10.1016/j.apmr.2018.01.019
41. Margalef R, Sisquella M, Bosque M. Experimental myofascial trigger point creation in rodents. J Appl Physiol. 2019;126:160–169. doi:10.1152/japplphysiol.00248.2018
42. Abbaszadeh-Amirdehi M, Ansari NN, Naghdi S, et al. Therapeutic effects of dry needling in patients with upper trapezius myofascial trigger points. Acupuncture Med. 2017;35:85–92. doi:10.1136/acupmed-2016-011082
43. Zarei H, Bervis S, Piroozi S, et al. Added value of gluteus medius and quadratus lumborum dry needling in improving knee pain and function in female athletes with patellofemoral pain syndrome: a randomized clinical trial. Arch Phys Med Rehabil. 2020;101(2):265–274. doi:10.1016/j.apmr.2019.07.009
44. Sánchez-Romero Eleuterio A, Daniel P-M, César C-L, et al. Effects of dry needling in an exercise program for older adults with knee osteoarthritis. Medicine. 2018;97(26):e11255. doi:10.1097/MD.0000000000011255
45. Eleuterio A, Sánchez, et al. Is a combination of exercise and dry needling effective for knee OA? Pain Med. 2019;21(2):349–363.
46. Velázquez-Saornil J, Ruíz-Ruíz B, Rodríguez-Sanz D, et al. Efficacy of quadriceps vastus medialis dry needling in a rehabilitation protocol after surgical reconstruction of complete anterior cruciate ligament rupture. Medicine. 2017;96(17):e6726. doi:10.1097/MD.0000000000006726
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.