Back to Journals » Clinical Ophthalmology » Volume 20
Effects of Selective Laser Trabeculoplasty on 24-Hour Intraocular Pressure in Patients with Well-Controlled in the Clinic but Progressing Primary Open Angle Glaucoma
Authors Kubota N ![]() , Nakamoto K, Sugimoto S, Shiratori N
, Nakamoto K, Sugimoto S, Shiratori N ![]() , Nakano Y, Tobita Y, Nishio Y, Okamoto F
, Nakano Y, Tobita Y, Nishio Y, Okamoto F
Received 16 November 2025
Accepted for publication 27 January 2026
Published 4 February 2026 Volume 2026:20 578484
DOI https://doi.org/10.2147/OPTH.S578484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Noriko Kubota,1 Kenji Nakamoto,1 Shio Sugimoto,1 Naka Shiratori,1 Yuji Nakano,1 Yutaro Tobita,2 Yusuke Nishio,3 Fumiki Okamoto1
1Department of Ophthalmology, Nippon Medical School, Tokyo, Japan; 2Department of Ophthalmology, Nippon Medical School Chiba Hokuso Hospital, Chiba, Japan; 3Department of Ophthalmology, Nippon Medical School Tama Nagayama Hospital, Tokyo, Japan
Correspondence: Noriko Kubota, Department of Ophthalmology, Nippon Medical School, Tokyo, Japan, Tel +81-3-3822-2131, Email [email protected]
Purpose: To evaluate the effects of selective laser trabeculoplasty (SLT) on 24-hour intraocular pressure (IOP) in patients with primary open-angle glaucoma (POAG) with well-controlled IOP but who exhibit glaucoma progression.
Methods: This retrospective study included all POAG patients with disease progression despite a well-controlled IOP in the clinic (≤ 14 mmHg) after antiglaucoma eye drops administration (mean number of medications = 3.93 ± 0.96). All patients underwent 24-hour IOP measurement before and after SLT. Using the iCare HOME tonometer, IOP was self-measured at several intervals for over 10 days at home in a sitting position. The analysis calculated the 24-hour IOP data after dividing it into eight time periods, while the average IOP values were calculated over each 3-hour period. The average, maximum, minimum, and fluctuation (maximum-minimum) were compared before and after SLT.
Results: In 16 eyes of the 13 enrolled patients, the mean 24-hour IOP was significantly reduced after SLT (11.3 (10.2– 13.4) (median (interquartile range) mmHg before vs 10.5 (9.4– 11.8) mmHg after, p=0.029). Significant IOP reductions were observed between 3 to 6 AM and 6 to 9 PM after SLT (p=0.004 and p=0.043, respectively). Although there was a significant reduction in the maximum 24-hour IOP (p=0.039), the minimum IOP did not significantly change after SLT (p=0.083). There were also no changes after SLT in the 24-hour, diurnal and nocturnal IOP fluctuations.
Conclusion: SLT significantly reduced nocturnal and maximum IOP in POAG patients whose IOP was already well-controlled in the clinic.
Plain Language Summary: SLT significantly reduced IOP between the 3 to 6 AM and 6 to 9 PM periods, and the maximum IOP. SLT may improve 24-hour IOP control in patients with POAG who show disease progression despite low clinic IOP under anti-glaucoma eye drops.
Keywords: circadian rhythm, intraocular pressure, selective laser trabeculoplasty, 24-hour intraocular pressure fluctuation
Introduction
Lowering intraocular pressure (IOP) remains the only proven therapeutic strategy for reducing the risk of glaucomatous vision loss.1 In addition to determining the mean IOP, the other recognized risk factor for glaucoma progression is IOP fluctuation. As demonstrated in the Advanced Glaucoma Intervention Study, visual field progression has been associated with large, long-term IOP fluctuations, even in patients with a relatively low mean IOP.2 Furthermore, higher peaks and greater fluctuations in 24-hour IOP in normal-tension glaucoma (NTG) have been linked to worse visual field damage.3
The laser therapy, selective laser trabeculoplasty (SLT), has been shown to reduce the IOP by improving aqueous outflow through the trabecular meshwork. As a result, due to its cost-effectiveness, minimal side effects, and ability to preserve the trabecular meshwork architecture while remaining a repeatable procedure, SLT has become an essential part of glaucoma management.4 It has been reported that SLT’s IOP-lowering effect is comparable to that found for a single prostaglandin analog, with this effect sustained throughout a 24-hour period.5,6 In general, there is a greater IOP reduction in eyes with a higher baseline IOP after SLT, although it has also been shown that SLT reduces the IOP over long periods in NTG patients.7 SLT’s mechanism of action makes it unlikely that it would lower the IOP below the episcleral venous pressure, which according to previous reports is approximately 8–10 mmHg.8,9 However, it is possible that SLT could suppress nocturnal IOP elevations, which have been reported to occur even in eyes that have been treated with multiple different antiglaucoma eye drops.
In the present study, we enrolled POAG patients who were being treated with multiple antiglaucoma eye drops, had well-controlled IOP in the clinic, but who continued to show disease progression, and then attempted to evaluate the effects of SLT on their 24-hour IOP patterns.
Methods
The Ethics Committee of Nippon Medical School (ID: M-2025-262), in accordance with the ethical review processes utilized at our institution, reviewed and approved this retrospective study.10 All patients provided written consent for their information to be stored in the hospital’s database and to be used for research purposes. This study was performed according to the tenets of the Declaration of Helsinki.
Patient Selection and IOP Measurement
Medical records from January 2018 to December 2024 were reviewed for consecutive patients with well-controlled (clinic IOP before SLT ≤14 mmHg) but who exhibited progressing POAG while being treated with glaucoma medications in conjunction with undergoing 24-hour IOP monitoring before and after SLT. Progressing POAG was defined as eyes that demonstrated visual field progression, indicated by a worsening of the mean deviation (MD) value on Humphrey Field Analyzer (HFA) testing. All patients were in a sitting position when using the iCare HOME tonometer to measure the IOP while at home during several intervals over more than 10 days. The IOP values that were recorded were then classified into eight time periods. Subsequently, we compared the average, maximum, minimum, and fluctuation (maximum-minimum) of the 24-hour IOP before and after SLT. When using the iCare HOME or iCare HOME 2 tonometer, all of the pre-treatment IOP measurements were conducted within 12 months prior to the SLT. All of the post-treatment measurements were then obtained within 6 months after the SLT. A calibrated Goldmann applanation tonometer was used to measure the clinic IOP while the patients were in a sitting position. Within 1 month prior to the SLT, all patients underwent pre-treatment IOP measurements at the clinic. These patients then underwent post-treatment measurements between 4 and 12 weeks after the initial SLT.
Patients that had a previous history of glaucoma surgery, active ocular infection or inflammation, and an inability to be able to reliably measure the IOP when using the iCare HOME device were excluded from the analysis. The clinical details collected from the medical records included patient age, gender, clinic IOP, optical coherence tomography (OCT) parameters, and the HFA results.
Visual Function Assessment
Best-corrected visual acuity (BCVA) was measured using a standard Japanese decimal visual acuity chart at a distance of 5 meters. The decimal values were converted to the logarithm of the minimal angle of resolution (logMAR) units for the statistical analyses. OCT imaging was performed using spectral-domain OCT (RS-3000 Advance, NIDEK). Ganglion cell complex (GCC) thickness was measured according to the manufacturer’s standard protocol. OCT measurements obtained within 6 months before and after SLT were included in the analysis, and when two or more measurements were available within each period, their mean values were used for analysis. A Humphrey Field Analyzer 3 (Carl Zeiss Meditec) was used to evaluate the visual field function. This analysis included all of the MD values within 6 months before and after the SLT.
Laser Technique
After the administration of local anesthesia, two experienced glaucoma specialists (K.N., N.S.) performed the SLT. Using an energy setting of 0.3–0.6 mJ, a Q-switched Nd:YAG laser (Tango, Ellex) was applied to 360° of the trabecular meshwork. Immediately before and after the procedure, 1% apraclonidine hydrochloride was administered to prevent post-procedural IOP spikes. Throughout the study period, patients continued to use their originally prescribed glaucoma medications.
Statistical Analysis
The mean scores and standard deviations were calculated for age, BCVA, ganglion cell complex (GCC) thickness, MD, and follow-up duration. A Wilcoxon’s signed-rank test was used to analyze the differences in the clinic IOP, GCC thickness, and MD values before and after SLT treatment. Statistical significance was set at p<0.05 for all tests of association. SPSS Statistics (version 29.0, IBM) was used to carry out all of the analyses.
Results
Clinical characteristics of the study patients are summarized in Table 1. After enrolling 13 patients (4 men and 9 women) with a mean age of 56.4 ± 14.9 (mean ± SD) years, 16 total eyes were then evaluated. The mean BCVA was 0.0685 ± 0.28 (logMAR), while the mean central corneal thickness was 520.8 ± 29.6 µm. After SLT, the IOP measurements obtained at the clinic for 11 of 16 eyes (69%) showed there was over a 20% reduction in the IOP. Although there was a tendency for the post-SLT IOP to be lower than baseline, this difference was not found to be statistically significant (p=0.063). In addition, no significant changes were observed in the HFA MD (before SLT: −12.9 ± 5.9 dB; after SLT: −14.0 ± 8.1; p=0.36). Similarly, there were no significant changes in GCC thickness (before SLT [superior / inferior]: 61.1 ± 9.8 / 56.9 ± 8.0µm; after SLT: 60.5 ± 9.2 / 56.7 ± 7.0 µm; p=0.244 / 0.818). All patients continued to take the same medications before and after the SLT, with an average number of antiglaucoma medications of 3.9 ± 0.96. The mean duration between SLT and the 24-hour IOP measurement was 3.93 ± 2.1 months.
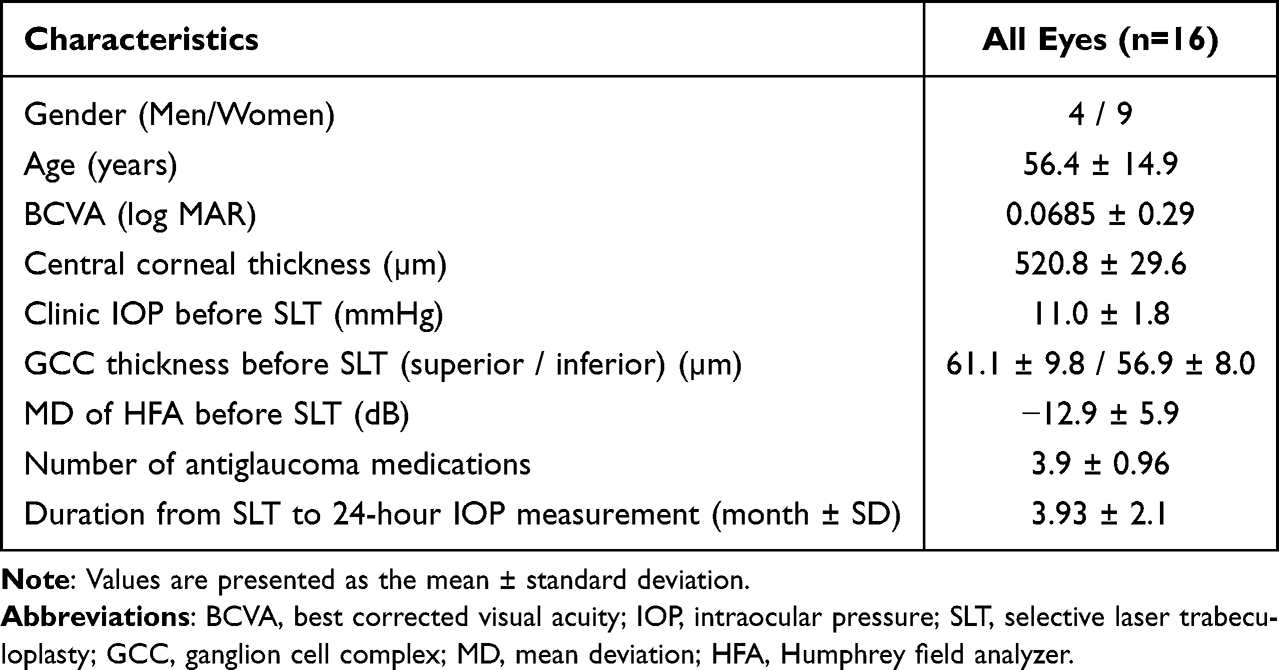 |
Table 1 Demographics and Baseline Clinical Characteristics of Patients |
Figure 1 shows the 24-hour circadian IOP curves before and after SLT. Notably, there was a significant reduction in the average IOP during the periods between 3 AM to 6 AM and 6 PM to 9 PM (p=0.004 and p=0.043, respectively).
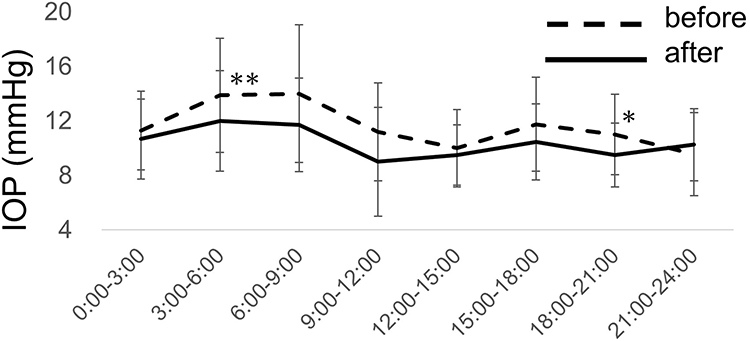 |
Figure 1 Changes in 24-hour circadian intraocular pressure (IOP) curves before and after selective laser trabeculoplasty (SLT). Notes: After performing SLT, the average IOP was significantly reduced between 3 AM to 6 AM and 6 PM to 9 PM. *p<0.05, **p<0.005, Wilcoxon’s signed-rank test. |
Figure 2 shows the changes in the 24-hour average IOP before and after SLT. The results showed a modest but significant decrease in IOP (11.3 (10.2–13.4) (median (interquartile range) mmHg before vs 10.5 (9.4–11.8) mmHg after, p=0.029).
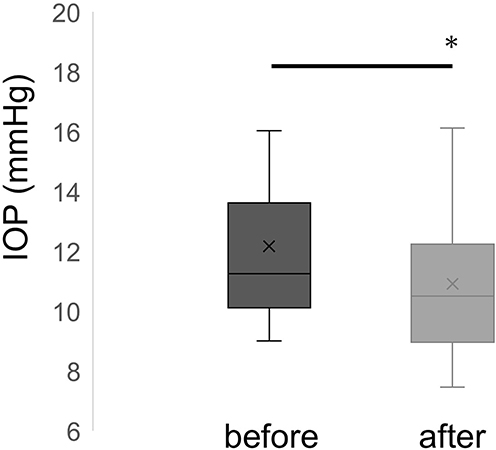 |
Figure 2 Changes in the 24-hour average intraocular pressure (IOP) before and after selective laser trabeculoplasty (SLT). Notes: A statistically significant decrease in 24-hour average IOP was observed after SLT. The horizontal lines indicate the median, while the × marks represent the mean values. *p<0.05, Wilcoxon’s signed-rank test. |
Figure 3A shows the change in the maximum IOP over the 24-hour period. A modest but statistically significant decrease was observed following the SLT (14.7 (12.9–17.7) before vs.12.3 (11.9–15.3) mmHg after, p=0.039). In contrast, Figure 3B further shows that the change in the minimum IOP remained unchanged before and after the SLT (8.6 (7.9–11.3) before vs 8.8 (6.8–10.1) mmHg after, p=0.083).
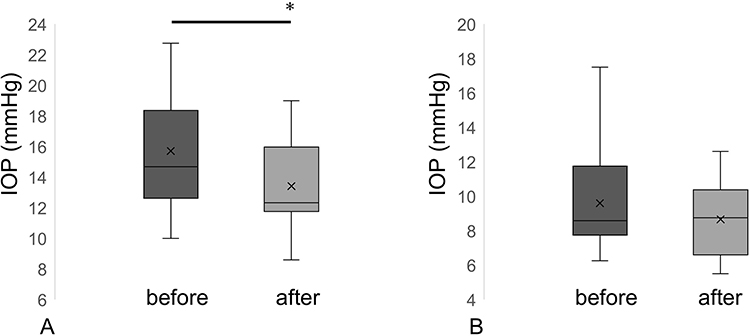 |
Figure 3 24-hour maximum (A) and minimum (B) intraocular pressure (IOP). Notes: A statistically significant decrease in the 24-hour maximum IOP was observed (A), whereas no statistically significant change was observed in the minimum IOP (B). The horizontal lines indicate the median, while the × marks represent the mean values. *p<0.05, Wilcoxon’s signed-rank test. |
Figure 4 shows the changes in IOP fluctuations across the 24-hour (Figure 4A), diurnal (9 AM to 6 PM) (Figure 4B) and nocturnal (9 PM to 6 AM) (Figure 4C) periods. IOP fluctuations did not show a statistically significant change in any of these periods following SLT.
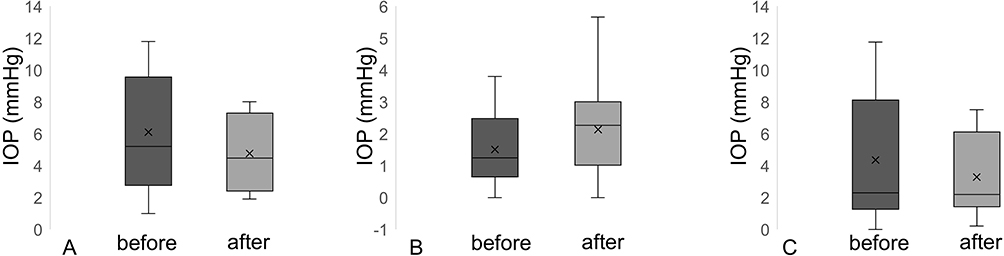 |
Figure 4 Fluctuations in the 24-hour (A), diurnal (B) and nocturnal (C) periods. Notes: The 24-hour, diurnal and nocturnal intraocular pressure (IOP) fluctuations did not significantly change after selective laser trabeculoplasty. The horizontal lines indicate the median, while the × marks represent the mean values. Wilcoxon’s signed-rank test. |
Discussion
The present study evaluated the effect of SLT on 24-hour IOP in patients with POAG whose IOP was medically controlled during clinic hours. While the potential benefits of SLT have been well studied, data on its influence on 24-hour IOP in patients with well-controlled clinic IOP remain limited.
Our results demonstrated that there was a significant reduction in the SLT for the nocturnal IOP between 3 AM to 6 AM, as well as for the 24-hour average IOP and the 24-hour maximum IOP. The findings of our present study suggest that there may be additional benefits provided by SLT through the lowering of the IOP levels. Although these changes may be undetectable during routine clinic visits, this action could potentially contribute to changes in the glaucoma progression.
Other previous studies have evaluated and demonstrated the effect of SLT in 24-hour IOP.5,11 Shi et al5 compared the 24-hour IOP profiles of SLT and latanoprost when used as the initial treatment for eyes with ocular hypertension and POAG. Their results showed that both treatments were able to significantly reduce the IOP during both the nocturnal and diurnal periods. Pillunat et al11 evaluated patients who were already being treated with antiglaucoma eye drops and then examined the efficacy of adjunctive SLT. Their findings showed that not only was the mean 24-hour IOP reduced by adjunctive SLT, but that there was also an additional benefit in the reduction of the IOP fluctuation and the nocturnal peak IOP. The average number of medications in their study was 2.9 ± 0.9. Similarly, there was also a higher number of antiglaucoma medications (3.9 ± 0.96) being administered in our study patients, with our results also demonstrating that SLT can further reduce nocturnal and maximum IOP. These findings suggest the potential efficacy in patients who are receiving near-maximal medical treatments.
Previous studies12,13 that have assessed IOP measurements in patients during regular clinic visit times have reported finding that 360 SLT was more effective in reducing IOP fluctuations in addition to achieving better long-term IOP control compared to 180° SLT. Furthermore, Dahlgren et al14 investigated the SLT treatment parameters utilized in patients. Their results showed that 360° SLT when using sufficient power to induce cavitation bubbles in 50% to 75% of the laser applications was able to provide optimal outcomes. However, our study used 360° SLT with a relatively low power, which was a level that did not generate any cavitation bubbles. Even so, our results showed there were significant reductions in the nocturnal IOP and peak IOP, which suggests that even when using a low power, a useful effect can be achieved.
Our findings showed that a reduction in the maximum IOP was observed, suggesting there may be a potential role for SLT in mitigating IOP spikes. As a result, this could contribute to potentially improving long-term glaucoma management. Hughes et al15 monitored 24-hour IOP in patients and identified high IOP levels along with wide IOP variations as being major risk factors for glaucoma progression. Therefore, when evaluating patients, it is necessary to consider potentially undetected IOP peaks that could occur outside of the clinic, particularly in those patients who demonstrate a well-controlled clinic IOP but also a progressing visual field.
Finally, the clinical interpretation of IOP changes should be considered in the context of baseline IOP levels. In patients with relatively high baseline IOP, larger absolute reductions may be observed and are often expected. In contrast, in populations with well-controlled and relatively low baseline IOP, such as the cohort included in this study, large absolute reductions are inherently less likely to occur. Therefore, the modest absolute changes observed in the present study should be interpreted within the context of the selected study population rather than as an indication of limited treatment effect.
There were several limitations in the present study. First, this was a retrospective study that only contained a small sample size, and the study population consisted of patients with well-controlled and relatively low baseline intraocular pressure. In addition, some patients contributed both eyes to the analysis, and inter-eye correlation was not accounted for, which may have influenced the statistical significance of the results. Second, nocturnal IOP measurements were not conducted in the habitual (supine) positions. As the supine position is known to have a higher IOP as compared to the sitting position, the nocturnal IOP-lowering effect of SLT could potentially differ depending upon the body posture of the subject. A more precise assessment of the IOP change could potentially be obtained by utilizing a continuous 24-hour IOP monitoring device such as a contact lens sensor. Third, the outcomes of the SLT could have varied due to differences in the number and types of antiglaucoma medications being used among the patients, and medication adherence was not objectively assessed, which may have influenced the observed IOP changes. Fourth, the iCare HOME and iCare HOME 2, which are two different devices, were both used for the IOP measurements. While the iCare HOME 2 device was used to obtain the IOP data from 4 eyes of 2 patients, only the sitting position measurements were included when matching the conditions for the iCare HOME. As a result, we cannot completely rule out the potential device-related differences in the IOP. Finally, due to the relatively short follow-up period, this makes it difficult to assess the long-term stability of the SLT’s effects. In order to confirm these findings and optimize the timing and parameters of SLT treatment, future studies with larger sample sizes, longer follow-up durations, and more standardized IOP monitoring methods will need to be conducted. In addition, multiple outcome measures and time windows were analyzed without formal adjustment for multiple comparisons, which may have increased the risk of type I error. Therefore, the statistical significance of the findings should be interpreted with caution.
In conclusion, SLT significantly reduced 24-hour average IOP, nocturnal IOP at 3 AM to 6 AM, and 24-hour maximum IOP in POAG patients who have a low controlled IOP in the clinic. Even though no significant changes were observed in the IOP fluctuation, the present findings indicate that SLT was associated with modest changes in nocturnal and peak IOP values that are often not captured by routine clinic measurements. However, given the retrospective and observational nature of this study, these findings should be interpreted with caution. In order to clarify the role of SLT in comprehensive glaucoma management, further studies with larger sample numbers, longer follow-up, and continuous IOP monitoring are warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kiuchi Y, Inoue T, Shoji N, Nakamura M, Tanito M; Glaucoma Guideline Preparation Committee, Japan Glaucoma Society. The Japan glaucoma society guidelines for glaucoma 5th edition. Jpn J Ophthalmol. 2023;67(2):189–7. PMID: 36780040. doi:10.1007/s10384-022-00970-9
2. Caprioli J, Coleman AL. Intraocular pressure fluctuation a risk factor for visual field progression at low intraocular pressures in the advanced glaucoma intervention study. Ophthalmology. 2008;115(7):1123–1129.e3. PMID: 18082889. doi:10.1016/j.ophtha.2007.10.031
3. Sakata R, Aihara M, Murata H, et al. Intraocular pressure change over a habitual 24-hour period after changing posture or drinking water and related factors in normal tension glaucoma. Invest Ophthalmol Vis Sci. 2013;54(8):5313–5320. PMID: 23821194. doi:10.1167/iovs.13-11792
4. Latina MA, Tumbocon JAJ. Selective laser trabeculoplasty: a new treatment option for open angle glaucoma. Curr Opin Ophthalmol. 2002;13(2):94–96. doi:10.1097/00055735-200204000-00007
5. Shi Y, Zhang Y, Sun W, et al. 24-Hour efficacy of single primary selective laser trabeculoplasty versus latanoprost eye drops for Naïve primary open-angle glaucoma and ocular hypertension patients. Sci Rep. 2023;13(1):12179. PMID: 37500642; PMCID: PMC10374636. doi:10.1038/s41598-023-38550-7
6. Kiddee W, Atthavuttisilp S. The effects of selective laser trabeculoplasty and travoprost on circadian intraocular pressure fluctuations: a randomized clinical trial. Medicine. 2017;96(6):e6047. PMID: 28178150; PMCID: PMC5313007. doi:10.1097/MD.0000000000006047
7. Naito T, Nitta K, Miki T, et al. Two-year outcome of selective laser trabeculoplasty for normal-tension glaucoma in Japan: first-line or second-line selective laser trabeculoplasty (FSS) study. J Clin Med. 2025;14(10):3459. PMID: 40429454; PMCID: PMC12111932. doi:10.3390/jcm14103459
8. Goel M, Picciani RG, Lee RK, Bhattacharya SK. Aqueous humor dynamics: a review. Open Ophthalmol J. 2010;4(1):52–59. PMID: 21293732; PMCID: PMC3032230. doi:10.2174/1874364101004010052
9. Gulati V, Fan S, Gardner BJ, et al. Mechanism of action of selective laser trabeculoplasty and predictors of response. Invest Ophthalmol Vis Sci. 2017;58(3):1462–1468. PMID: 28264102; PMCID: PMC5361453. doi:10.1167/iovs.16-20710
10. Otsuka T, Matsuyama K. Nippon medical school’s ethical review processes for studies involving human subjects. J Nippon Med Sch. 2024;91(2):136–139. PMID: 38777779. doi:10.1272/jnms.JNMS.2024_91-216
11. Pillunat KR, Kocket GA, Herber R, Jasper CS, Lenk J, Pillunat LE. Efficacy of selective laser trabeculoplasty on lowering intraocular pressure fluctuations and nocturnal peak intraocular pressure in treated primary open-angle glaucoma patients. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):1979–1985. PMID: 36418515; PMCID: PMC10271892. doi:10.1007/s00417-022-05897-y
12. Prasad N, Murthy S, Dagianis JJ, Latina MA. A comparison of the intervisit intraocular pressure fluctuation after 180 and 360 degrees of selective laser trabeculoplasty (SLT) as a primary therapy in primary open angle glaucoma and ocular hypertension. J Glaucoma. 2009;18(2):157–160. PMID: 19225355. doi:10.1097/IJG.0b013e3181752c97
13. Nirappel A, Klug E, Ye R, et al. Effectiveness of selective laser trabeculoplasty applied to 360° vs. 180° of the angle. J Ophthalmol. 2021;2021:8860601. PMID: 33643665; PMCID: PMC7902141. doi:10.1155/2021/8860601
14. Dahlgren T, Ayala M, Zetterberg M. Optimal performance of selective laser trabeculoplasty: results from the Swedish optimal SLT multicenter randomized controlled trial. Ophthalmol Glaucoma. 2024;7(2):105–115. PMID: 37838088. doi:10.1016/j.ogla.2023.10.004
15. Hughes E, Spry P, Diamond J. 24-hour monitoring of intraocular pressure in glaucoma management: a retrospective review. J Glaucoma. 2003;12(3):232–236. PMID: 12782841. doi:10.1097/00061198-200306000-00009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.