Back to Journals » Clinical Interventions in Aging » Volume 21
Effects of Positive Event Recording on Rehabilitation Outcomes in Elderly Patients with Coronary Heart Disease and Anxiety
Authors Yuan DJ ![]() , Chen CL, Zhang K, Ji YC, Peng LY, Wu Q, Xue Y
, Chen CL, Zhang K, Ji YC, Peng LY, Wu Q, Xue Y ![]()
Received 22 December 2025
Accepted for publication 17 May 2026
Published 24 June 2026 Volume 2026:21 590893
DOI https://doi.org/10.2147/CIA.S590893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
De-Jing Yuan,1,* Cui-Lian Chen,1,* Ke Zhang,2 Yi-Chun Ji,2 Li-Yu Peng,2 Qing Wu,1 Yuan Xue1
1Department of Cardiology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2School of Nursing, Suzhou Medical College, Soochow University, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qing Wu, Department of Cardiology, The First Affiliated Hospital of Soochow University, No. 899 Pinghai Road, Gusu District, Suzhou, 215006, People’s Republic of China, Email [email protected] Yuan Xue, Department of Cardiology, The First Affiliated Hospital of Soochow University, No. 899 Pinghai Road, Gusu District, Suzhou, 215006, People’s Republic of China, Email [email protected]
Background: Elderly patients with coronary heart disease (CHD) are prone to psychological disorders during treatment. Strengthening psychological well-being can improve rehabilitation outcomes. This study aimed to explore the effects of recording positive events on anxiety, psychological capital, treatment compliance, and major adverse cardiovascular events (MACE) in elderly CHD patients with anxiety symptoms.
Methods: A total of 309 elderly CHD patients with anxiety were enrolled and randomly assigned to an intervention group (n=154) and a control group (n=155). After the intervention, assessments were conducted using the Self-Rating Anxiety Scale (SAS), the Positive Psychological Capital Questionnaire (PPQ), and a treatment compliance scale, along with collection of clinical indicators and data on MACE. Primary outcomes were changes in anxiety and treatment compliance behaviors. Secondary outcomes included changes in the positive psychological capital scores, clinical indicators, and incidence of MACE.
Results: The intervention group showed significantly lower anxiety scores than the control group at the end of the intervention (3 months after discharge) and the end of follow-up period (6 months after discharge) (p< 0.05). Additionally, the intervention group scored significantly higher on the PPQ and CHD Treatment Compliance Behavior Scale (p< 0.05). Improvements in clinical indicators (except systolic blood pressure) were significantly greater in the intervention group (p< 0.05). Furthermore, the incidence of MACE was significantly lower in the intervention group (12 cases vs. 36 cases, p< 0.05), and compared with the control group, the relative risk (RR) of adverse cardiovascular events was 0.33 (95% confidence interval: 0.18– 0.61, p = 0.025).
Conclusion: Recording positive events can alleviate anxiety, enhance psychological capital and treatment compliance, reduce the occurrence of MACE, and effectively improve rehabilitation outcomes in elderly CHD patients.
Keywords: coronary heart disease, positive events, rehabilitation, psychological capital
Introduction
Coronary heart disease (CHD) is one of the non-communicable chronic diseases with high mortality rates worldwide.1 According to “The 2023 Summary Report on Cardiovascular Health and Diseases in China”, the current number of CHD patients in China has reached 11.39 million.2 Despite significant symptom relief with percutaneous coronary intervention (PCI), CHD patients retain a risk of major adverse cardiovascular events (MACE).3 Previous studies have shown that negative emotions such as anxiety can increase the incidence of vascular restenosis and MACE, thus adversely affecting patient prognosis.4 Besides, Patients with CHD exhibit a higher susceptibility to psychological complications, such as anxiety and depression, and tend to experience more severe psychological distress.5 Additional research also suggests that implementing diversified intervention models for CHD patients can help improve blood pressure control, medication adherence and quality of life.6 These interventions can also increase therapeutic cooperation and facilitate lifestyle modifications toward healthier behaviors.7,8 Therefore, targeted management of known risk factors will maximize patient benefits.
Positive psychology, as a psychological discipline, focuses on cultivating psychological resilience and behavioral patterns by emphasizing positive subjective experiences and developing personal strengths.9,10 Currently, positive psychology has been widely applied internationally in fields such as obstetrics, gynecology, and diabetes management.11,12 Corno et al (2018) found that positive psychological interventions can help reduce anxiety and depression in pregnant women,13 thereby enhancing their well-being. Huffman et al (2015) also demonstrated that positive psychological interventions enhance treatment compliance in type 2 diabetes patients.14
The development of positive psychology remains relatively nascent, and primarily concentrate in education and mental health domains.15–18 For example, Wang et al (2019) confirmed that positive psychological interventions alleviate psychosocial distress in stroke survivors.19
Positive psychology encompasses diverse implementation approaches including expressive writing, mindfulness therapy, gratitude interventions, and hope therapy.10 Writing represents a unique human behavior for expression, communication, and creation. Therefore, the positive event recording implemented in this study aims to evoke personally relevant positive experiences or emotions through writing. This concept, initially proposed by Pennebaker JW and Beall SK, involves encouraging participants to freely express their thoughts and feelings about real-life events during brief daily sessions of 15–20 minutes.20 The therapeutic benefits originate from event reappraisal, cognitive reorganization, and construction of meaningful narrative.21 Numerous studies have confirmed that recording positive events significantly enhances participants’ well-being and helps stabilize mental health in psychiatric patients.22
Given that CHD patients undergo stressful experiences such as emergency treatment, surgical procedures, and hospitalization, coupled with insufficient understanding of disease prognosis, they are prone to develop psychological disorders including anxiety, which necessitates greater clinical attention.23 However, current research on positive event recording interventions for CHD patients with anxiety remains in its nascent stages both domestically and internationally, characterized by insufficient systematic approaches and targeted methodologies.
Thus, it is necessary to implement positive psychological interventions for this patient population to investigate their effects on rehabilitation outcomes, thereby establishing a theoretical foundation for developing more tailored positive psychological intervention protocols for CHD patients in China.
This six-month randomized clinical trial aimed to investigate the effects of positive event recording on anxiety, psychological capital, treatment compliance, and MACE in elderly patients with CHD and anxiety. Our study addresses a gap in the application of psychological interventions in CHD rehabilitation and provides a theoretical foundation for the implementation of diverse psychological intervention approaches in future research.
Methods
Participants
Elderly patients with CHD were recruited from the Cardiology Ward of a tertiary (A-grade) hospital affiliated with Soochow University (Jiangsu, China) between August 2022 and August 2023. Inclusion criteria were: age ≥60 years; meeting diagnostic criteria for CHD;24 Self-Rating Anxiety Scale score ≥ 50;25 provision of written informed consent; clear consciousness, normal cognition, and adequate communication ability.
Exclusion criteria included: severe cognitive impairment, psychiatric disorders, or uncooperative status; other life-threatening conditions such as terminal cancer.
Withdrawal criteria comprised: failure to record events for two consecutive weeks; unreachable by phone for three consecutive follow-up attempts; voluntary withdrawal during the study.
The sample size was determined using the formula for two independent sample means: n1=n2=2(Zα/2+Zβ)2σ2/δ2, where σ represents the population standard deviation (6.7), δ the margin of error (3), Zα/2 the two-tailed standard normal quantile (1.96 at α=0.05), and Zβ(1.282 at β=0.10).26 The calculated sample size was 105 per group. Accounting for a 10–20% attrition rate, the final target enrollment was set at 240 participants. Following screening, 309 eligible patients were randomized using SPSS 25.0 software into an intervention group (n=154) and a control group (n=155).
Randomization and Blinding
Eligible participants who provided written informed consent for the clinical trial were randomly assigned to either the intervention or control group at a 1:1 allocation ratio. The intervention group received a 3-month positive event recording protocol, while the control group received standard health management. Both groups were followed for an additional 3 months after the intervention period, with a total study duration of 6 months. Each participant in the intervention group was provided with a dedicated positive event recording notebook and a unified CHD health education handbook, and the control group was given the same health education handbook to eliminate confounding factors from health education.
Study Procedures
Following randomization, patients completed a general information questionnaire, the Self-Rating Anxiety Scale (SAS, total score range: 20–80 points, with higher scores indicating more severe anxiety), the Positive Psychological Capital Questionnaire (PPQ, total score range: 26–182 points, with higher scores indicating greater psychological capital), the CHD Treatment Compliance Behavior Scale (total score range: 21–105 points, with higher scores indicating better treatment compliance), as well as data collection on MACE and clinical indicators. Evaluations using the SAS, PPQ, and CHD Treatment Compliance Behavior Scale, along with collection of clinical indicators, were conducted at baseline (enrollment), the end of (3 months after discharge) and the end of follow-up period (6 months after discharge). MACE were tracked and recorded throughout the 6-month study period, and the incidence was statistically analyzed at the end of follow-up period (details in Table 1).
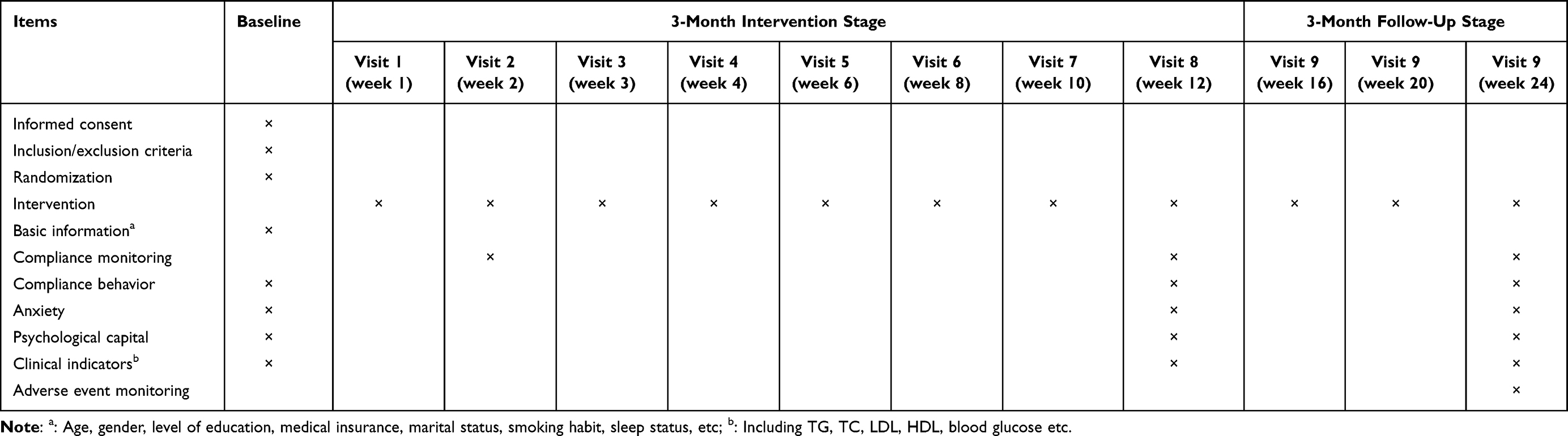 |
Table 1 Schedule of Enrollment, Intervention, and Assessment |
Measures
The primary outcome was change in anxiety and treatment compliance behavior from baseline to 6 months after discharge. Secondary outcomes included Positive Psychological Capital score at 3 months and 6 months after discharge; changes in clinical indicators; and incidence of MACE at 6 months after discharge.
General Information Collection
The collected data include information such as age, sex, educational level, smoking history, comorbid chronic diseases, blood pressure, left ventricular ejection fraction, total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, etc. Clinical features are obtained and filled in by researchers by reviewing patients’ electronic medical records.
Self-Rating Anxiety Scale (SAS)
The Chinese version of SAS comprises 20 items rated on a 4-point Likert scale ranging from 1 (“none of the time”) to 4 (“most of the time”), with total raw scores ranging from 20 to 80.25 Using a standard cutoff score of 50, higher scores indicate more severe anxiety symptoms. The reliability of this scale has been established in previous research, confirming its applicability for assessing anxiety in CHD patients.27 In this study, the Cronbach’s α coefficient for scale was 0.883, indicating that the scale has good reliability and validity.
Positive Psychological Capital Questionnaire (PPQ)
The original scale was developed by Zhang et al (2010).28 It consists of 26 items and covers four dimensions: self-efficacy, adaptability, optimism and hope. PPQ employs a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with total scores ranging from 26 to 182. Higher scores indicate greater levels of psychological capital. Currently, this instrument has been widely applied in studies involving breast cancer patients, oral cancer patients, and diabetic patients, demonstrating good reliability and validity. The Cronbach’s α coefficient of our questionnaire is 0.90, confirming its applicability for CHD patients.
CHD Treatment Compliance Behavior Scale
The World Health Organization (WHO) defines compliance as “the extent to which a person’s behavior including taking medication corresponds with agreed recommendations from a health care provider.”29 Optimal patient compliance may effectively enhance treatment outcomes.30 The CHD treatment compliance behavior scale was developed by Zhang et al (2007)31 This scale comprises 21 items across seven dimensions: physical activity, dietary management, medication compliance, psychological adjustment, social function maintenance, follow-up compliance, and smoking/alcohol restriction. Each item employs a 5-point Likert scale (1: completely non-compliant to 5: fully compliant). The scale demonstrated satisfactory psychometric properties, with an internal consistency reliability of 0.79 and content validity of 0.72. Total score ranges from 21 to 105, where higher scores indicate better treatment compliance. In our study, the scale showed a Cronbach’s α coefficient of 0.81, suggesting it is a suitable tool for assessing compliance behavior in CHD patients.
MACE and Clinical Parameters
In this study, MACE was defined as the occurrence of any of the following during the follow-up period: sudden cardiac death, acute myocardial infarction, unstable angina, malignant arrhythmia, acute heart failure, or repeat revascularization. Clinical indicators included blood pressure, lipid profiles, and left ventricular ejection fraction. MACE is manually reviewed by attending physicians with clinical experience in cardiovascular and cerebrovascular diseases through electronic medical records of inpatient or outpatient visits during follow-up, combined with telephone follow-up, and ultimately confirmed by two physicians. Clinical features are obtained and filled in by researchers by reviewing patients’ electronic medical records.
Intervention
This study adopted a parallel control design, with participants randomly assigned to the intervention group and the control group at a 1:1 ratio. The control group received standard clinical health management for CHD consistent with clinical practice guidelines, while the intervention group was administered a 3-month positive event recording intervention on the basis of the same standard care. Previous studies suggest that positive psychological interventions lasting 8 weeks or longer can significantly alleviate negative emotions and foster positive psychological states.32,33 Both groups were followed up for an additional 3 months after the intervention, with a total study duration of 6 months for all participants. To ensure the standardization and consistency of the intervention, the research team unified the intervention materials, formulated detailed implementation protocols, and conducted pre-intervention training for all implementers.
Each participant in the intervention group was provided with a dedicated positive event recording notebook and a unified CHD health education handbook, and the control group was given the same health education handbook to eliminate confounding factors from health education. The specific implementation content, execution procedures and quality control measures of the two groups are detailed as follows:
Intervention Measures for the Intervention Group
On the basis of standard CHD health management, the intervention group implemented a phased positive event recording intervention combined with regular follow-up guidance, which was divided into a 3-month intervention stage (1 to 3 months after discharge) and a 3-month follow-up stage (4 to 6 months after discharge). The intervention was developed for the physiological and psychological characteristics of elderly CHD patients with anxiety, based on Seligman’s positive psychology intervention framework, supplemented by an extensive literature review and multiple rounds of expert consultations.9 The core goal was to guide patients to perceive and record positive events in daily life and disease management, and to transform positive emotions into healthy behavioral patterns. The specific implementation measures included three aspects: regular follow-up and dynamic guidance, standardized positive event recording guidance, and recording log management and adherence assessment.
Regular Follow-Up and Dynamic Guidance
Follow-up was mainly conducted through telephone and text messages, with the core of tracking the completion of positive event recording, solving the problems encountered by patients in the implementation process, and conducting targeted psychological counseling and health education. The follow-up frequency was strictly standardized: weekly follow-up in the first month after discharge (intervention initial stage), every two weeks follow-up in the second and third months (intervention middle and late stages), and monthly follow-up in the 3-month follow-up stage, until the end of the study. Each follow-up lasted 5–15 minutes, and the duration could be appropriately extended according to the patients’ actual consultation needs and emotional state. The follow-up content included verifying the completion of weekly recording tasks, evaluating the quality of positive event recording, guiding patients to optimize recording methods combined with their actual situation, and conducting brief psychological intervention for patients with obvious negative emotions, while reminding them of standardized medication and regular reexamination. Example (Record of Daily Positive Events): Today, I took the prescribed medication for coronary heart disease as directed by the doctor. In the afternoon, I took a 15-minute slow walk in the community. I felt no chest tightness or discomfort. My mood was relaxed and stable I felt a sense of security brought by adhering to a healthy lifestyle.
Standardized Positive Event Recording Guidance
The positive event recording intervention was implemented for 12 consecutive weeks after discharge, with clear and quantifiable weekly recording themes, completion requirements and operational guidelines for each stage (see Table 2 for the detailed intervention protocol). The research team conducted unified pre-intervention training for all implementers to ensure the consistency and accuracy of recording guidance. The implementers guided patients to record positive events in a standardized manner according to the weekly theme, focusing on guiding patients to perceive positive experiences in disease management (eg., completing exercise as prescribed, taking medication on time), daily life and social interaction, and requiring patients to record the specific content, occurrence time and their own emotional experience of positive events in the dedicated notebook. For patients with low educational level or poor writing ability, the implementers guided their family members to assist in recording to ensure the smooth progress of the intervention.
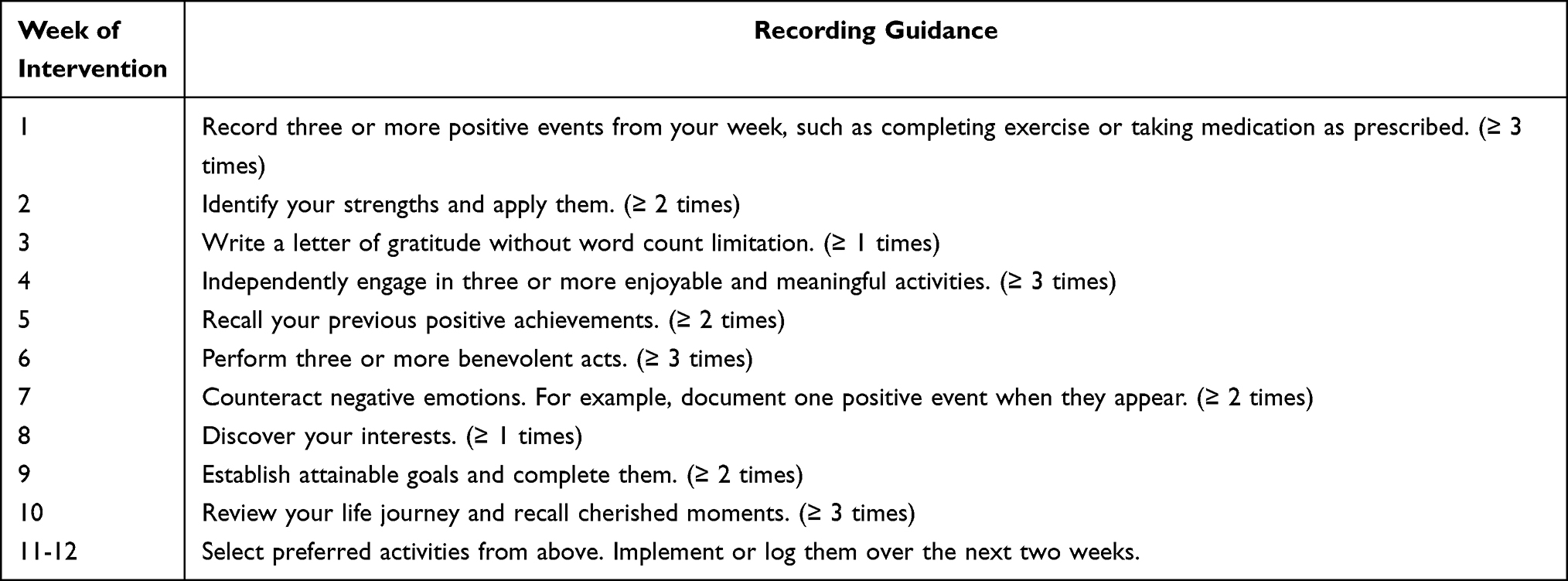 |
Table 2 Protocol for Positive Event Documentation |
Recording Log Management and Adherence Assessment
Each participant was provided with a unified recording logbook, and was required to record the specific content, completion frequency and single recording duration of positive event recording every week in a standardized manner. The research team collected and reviewed the logbooks during regular follow-up, and calculated the intervention adherence rate according to the formula: Adherence rate (%) = [Actual number of recordings/Minimum required recordings for the study] × 100%. For patients with an adherence rate lower than 70%, the research team timely analyzed the reasons (eg., personal inertia, poor physical condition, low recognition of the intervention) and conducted targeted intervention and guidance, such as simplifying the recording requirements appropriately and increasing follow-up frequency, to improve the intervention adherence rate and ensure the implementation effect.
Intervention Measures for the Control Group
The control group received standardized routine health management for CHD without additional intervention of positive event recording, while receiving synchronous follow-up consistent with the intervention group to ensure comparability between the two groups.
One-on-One Routine Health Education
On the first day of enrollment, each patient received one-on-one standardized health education conducted by designated researchers. The content covered key points of secondary prevention for CHD, scientific dietary recommendations (low-salt, low-fat, and low-sugar), appropriate weight management, individualized exercise guidance (moderate walking, tai chi, etc)., the importance of regular follow-up visits and standardized medication, as well as the prevention and management of MACE. This was performed to alleviate fear and anxiety caused by uncertainty about the condition. Meanwhile, patients were guided to practice slow deep breathing, muscle relaxation, and bed rest to reduce tension and physical discomfort. Family accompaniment was encouraged and doctor-patient communication was strengthened to enhance patients’ sense of security and treatment confidence.
Regular Follow-Up for Routine Management
Follow-up was conducted through telephone or text messages once a month after discharge for a total of 6 follow-ups until the end of the 6-month study period. Each follow-up lasted about 5–15 minutes, with the main content including answering the patients’ questions about disease management and medication, tracking the patients’ basic physical and mental status and clinical symptoms, reminding the patients of regular reexamination and standardized medication, and recording the occurrence of MACE.
Unified Data Collection and Strict Quality Control
To ensure the scientificity, accuracy and reliability of the study results, the research team formulated a unified data collection plan and strict quality control standards, which were implemented in the whole process of intervention and follow-up for both groups, and the data collection personnel were blinded to the group assignment of the patients.
Unified Data Collection Time Nodes and Methods
Baseline data (including general demographic information, psychological scale scores, and clinical indicators) were collected for all patients at the time of enrollment; post-intervention data (Self-Rating Anxiety Scale [SAS], Positive Psychological Capital Questionnaire [PPQ], CHD treatment compliance scale scores and clinical indicators) were collected the at the end of the intervention and the end of follow-up period; MACE were tracked and recorded throughout the 6-month study period. The scale investigation was conducted in a unified on-site or online standardized filling manner, and the clinical indicators (blood pressure, blood lipid, left ventricular ejection fraction, etc.) were collected through the hospital’s unified clinical examination and testing system to ensure the consistency of detection methods and standards.
Standardized Data Entry and Management
The data were independently double-entered into the Epidata 3.0 system by two full-time postgraduates who did not participate in the intervention implementation and data collection, and the entered data were cross-checked and verified for errors. The research database was set with special access rights, and unauthorized personnel were prohibited from accessing and modifying the data to ensure the integrity, confidentiality and accuracy of the data. After data verification, SPSS 25.0 software was used for statistical analysis.
Whole-Process Intervention Quality Supervision
The research team set up a special quality supervision group to conduct random spot checks on the implementation process of the intervention in the two groups, including the consistency of follow-up content, the standardization of recording guidance, the completion of data collection and the compliance of logbook recording. The spot check frequency was no less than once a month, and the non-standard operations found were corrected in a timely manner. For the implementers with irregular operation, re-training was conducted to ensure that the whole intervention process was carried out in strict accordance with the research protocol.
Outcome Assessment Schedule
For both groups, the SAS, PPQ and CHD treatment compliance scales were used to evaluate psychological status and treatment adherence, and clinical indicators were collected at baseline (enrollment), the end of the intervention (3 months after discharge) and the end of follow-up period (6 months after discharge). MACE were tracked and recorded throughout the 6-month study period, and the incidence was statistically analyzed at the end of the follow-up.
Statistical Analysis
All analyses were carried out using SPSS 25.0. The normality and homogeneity of variance for continuous variables were assessed using the Kolmogorov–Smirnov test. The results indicated that all measurement data followed a normal distribution and were expressed as mean ± standard deviation. Dependent variables included scores on the SAS, PPQ, CHD compliance behavior scale, and clinical indicators. If the interaction effect is statistically significant, simple effects analysis will be further conducted. Categorical data were described as frequencies (percentage), and between-group comparisons were performed using the chi-square test or Fisher’s exact test. The statistical significance level was set at α = 0.05, with a two-tailed p < 0.05 considered statistically significant.
Results
Participant Characteristics
During the research process, demographic data of participants who dropped out from both the intervention and control groups were compared to determine whether attrition was random, thereby minimizing the impact of selection bias on the study results. 47 patients could not be reached after three consecutive phone calls (12 in the intervention group, 35 in the control group), and 22 patients withdrew from the study due to inability to adhere to the experimental protocol or non-compliant records (all from the intervention group), as detailed in Table 3 34(p>0.05). Ultimately, 120 patients in the intervention group and 120 in the control group completed the study. In the intervention group, there were 66 males and 54 females, with a mean age of 70.18 ± 8.34 years. In the control group, there were 73 males and 47 females, with a mean age of 72.25 ± 6.89 years. No statistically significant differences were observed in baseline demographic characteristics, clinical data, or other variables between the two groups, as detailed in Table 4 34 (p>0.05).
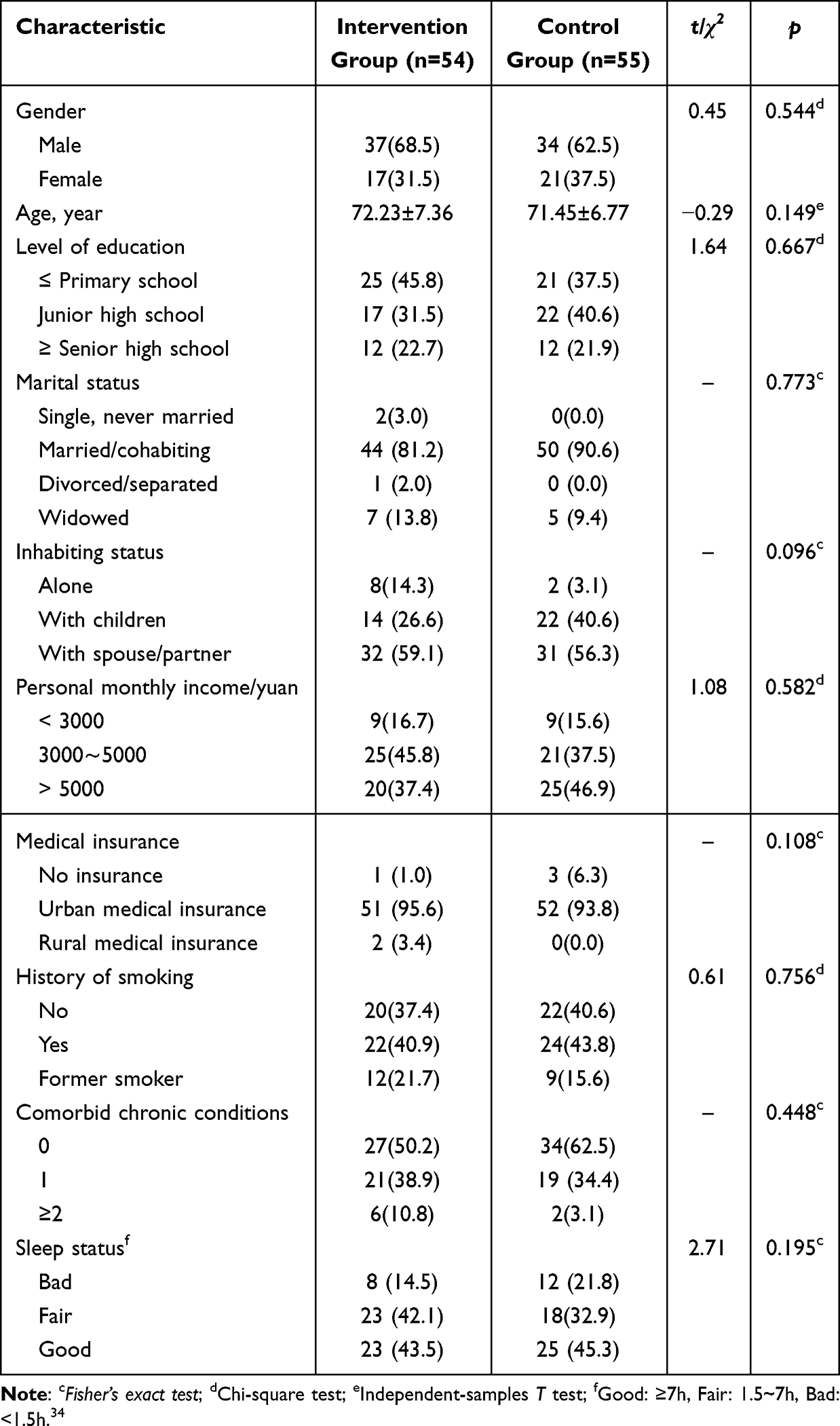 |
Table 3 Intention-to-Treat (ITT) Analysis [Frequency (%)/( |

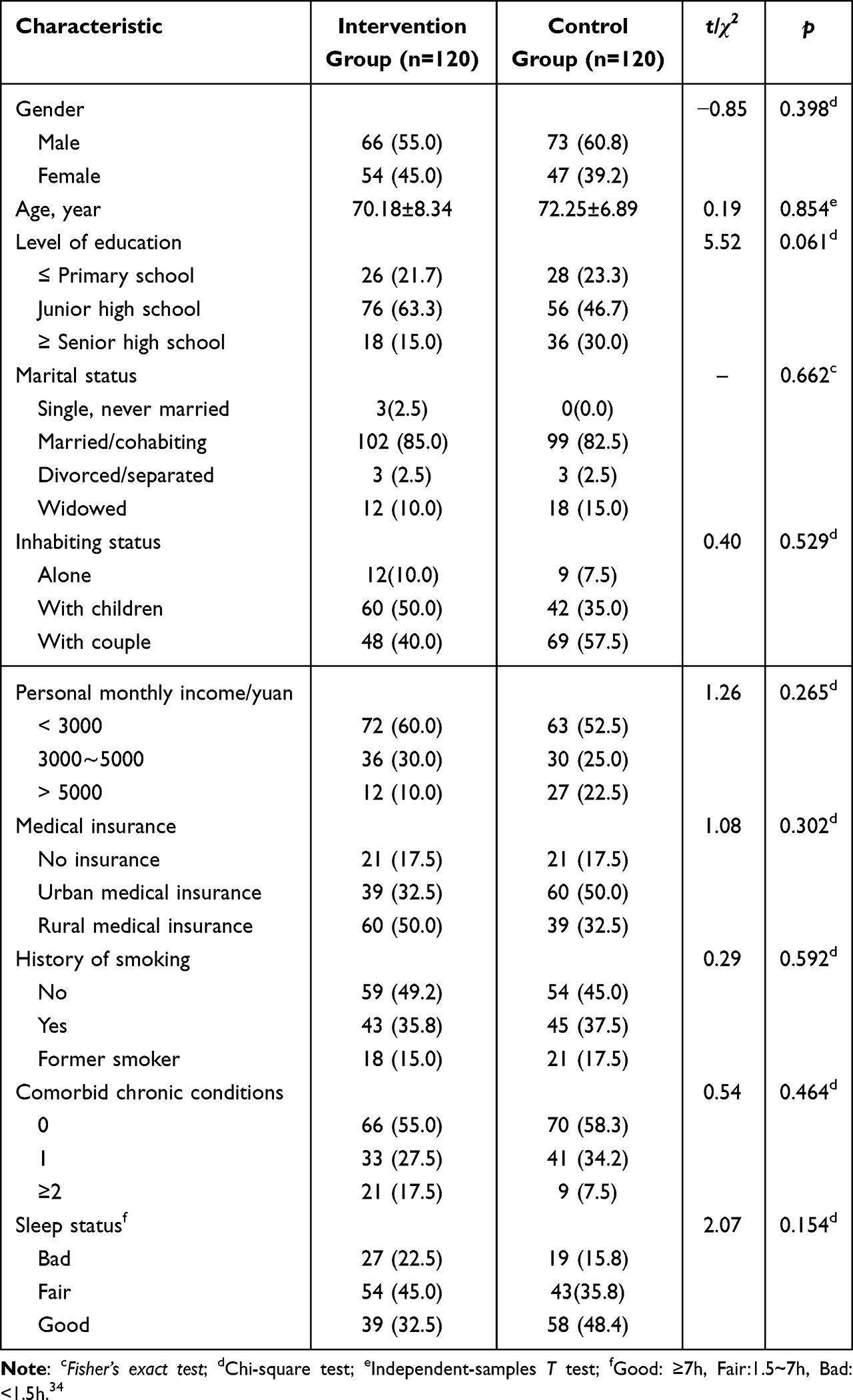 |
Table 4 Demographic and Clinical Characteristics [Frequency (%)/( |

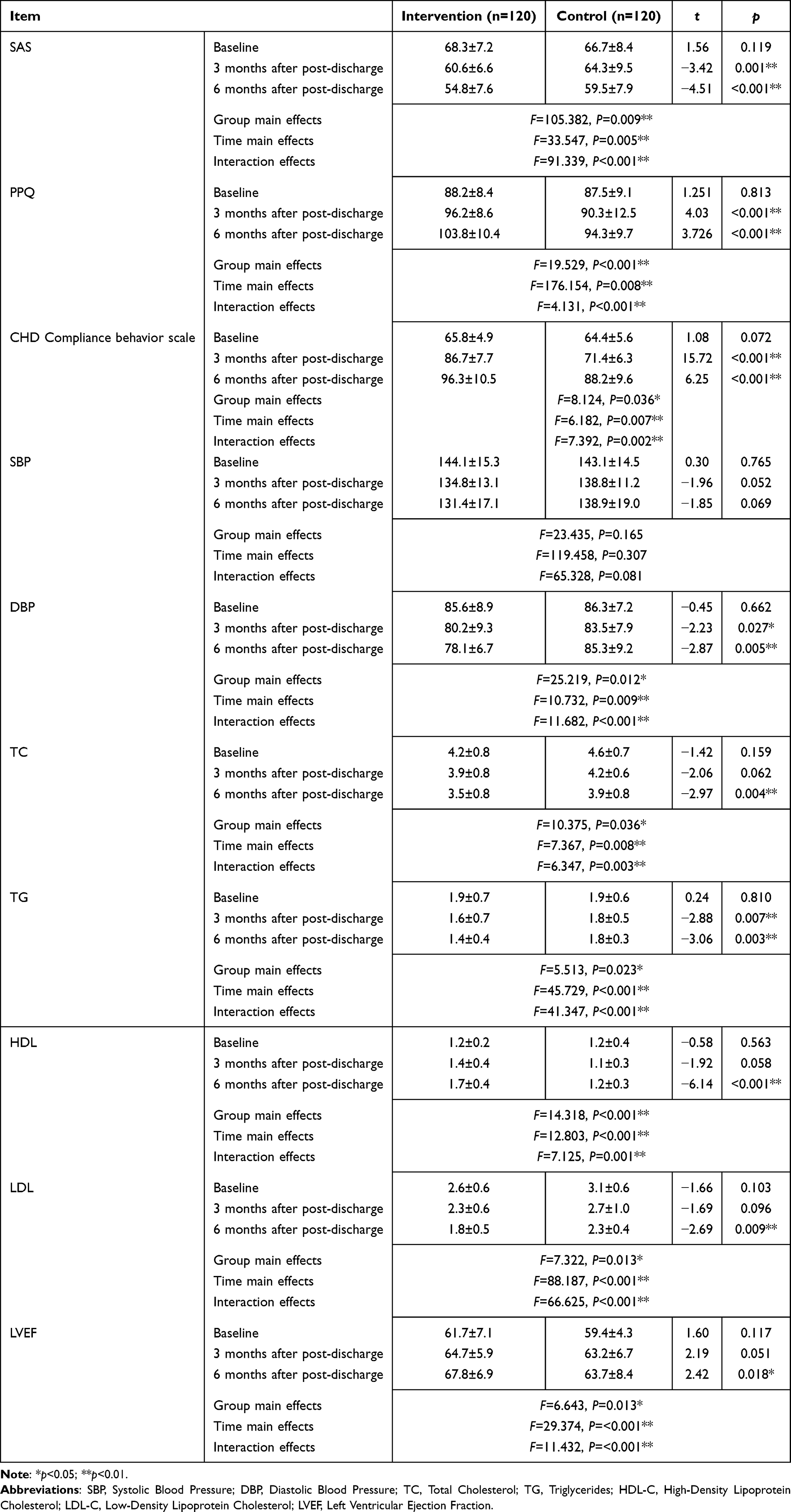 |
Table 5 Comparison of Anxiety, Psychological Capital, Treatment Adherence, and Clinical Indices Between Intervention and Control Groups Across Time Points ( |

Feasibility Analysis
Researchers collected written logs of patients’ positive event recordings to calculate adherence.
Adherence rate (%) = [Actual number of recordings/Minimum required recordings for the study] × 100%. Only when the adherence rate was ≥70%29 would the study proceed; otherwise, reasons were identified and protocol adjustments were made. In this study, the adherence rate in the intervention group was 85% after 2 weeks of implementation, 86.7% at the end of the intervention, and 83.2% at the end of follow-up period, all exceeding 70%. These results indicate that the intervention protocol is feasible.
No structural adjustments were made to the core intervention protocol during the study. Based on feedback from elderly patients, we only optimized the wording of recording guidance, simplified expressions, and flexibly arranged follow-up time to improve the feasibility and compliance of the intervention.
Comparison of Baseline Scores for SAS, PPQ, CHD Treatment Compliance Behavior Scale Between Two Groups
At baseline, the score of SAS, PPQ, CHD treatment compliance behavior scale, and clinical indicators in both groups are presented in Table 5. Independent samples t-test results indicated no statistically significant differences in anxiety (t=0.43, p=0.561), positive psychological capital (t=1.25, p=0.813), or CHD treatment compliance behavior scores (t=2.39, p=0.694) between the two groups. No statistically significant differences were observed in clinical indicators (systolic blood pressure (t=0.30, p=0.765), diastolic blood pressure (t=−0.45, p=0.662), total cholesterol (t=−1.42, p=0.159), triglycerides (t=0.24, p=0.810), high-density lipoprotein (t=−0.58, p=0.563), low-density lipoprotein (t=−1.66, p=0.103), and left ventricular ejection fraction (t=1.60, p=0.117) between the two groups.
The Scores of Various Scales at Three Time Points and the Results of Repeated Measures Analysis of Variance (ANOVA) for Two Groups
Simple effects analysis demonstrated that the intervention group exhibited significantly lower anxiety scores compared to the control group both at the end of the intervention (3 months after discharge) (p=0.036) and at the end of follow-up period (p=0.029) (Table 5). Furthermore, within the intervention group, anxiety scores were significantly lower at both post-intervention time points compared to baseline (both p<0.001).
Results for PPQ scores and CHD treatment compliance behavior scale scores were consistent with SAS (Table 5). Also, simple effects analysis revealed that the scores of PPQ and CHD treatment compliance behavior scale in the intervention group were significantly higher at both the end of the intervention (3 months after discharge) and the end of follow-up period (6 months after discharge) compared to baseline (p<0.001).
The analysis results of various clinical indicators also showed that at the end of the intervention (3 months after discharge) and at the end of follow-up period (6 months after discharge), except for systolic blood pressure, the diastolic blood pressure (p=0.014, 0.028), total cholesterol (p=0.008, p<0.001), triglycerides (p=0.029, p=0.031), and low-density lipoprotein (p=0.004, p<0.001) of the intervention group were significantly lower than those of the control group, while high-density lipoprotein (p=0.036, 0.027) and left ventricular ejection fraction (p=0.041, 0.025) were significantly increased compared with the baseline period. The above results indicate that active event recording can effectively improve the clinical symptoms of elderly patients with CHD complicated with anxiety.
Comparison of the Incidence of MACE Between the Two Groups After Intervention
At the end of follow-up (6 months after discharge), a total of 48 cardiovascular events occurred in both groups, with an overall incidence rate of 20%. Specifically, the cardiovascular event rate was 10.0% (12 cases) in the intervention group and 30.0% (36 cases) in the control group. The intervention significantly reduced the incidence of cardiovascular events (χ2=5.39, p<0.05). The relative risk (RR) of adverse cardiovascular events in the intervention group compared with the control group was 0.33 (95% CI: 0.18–0.61, p = 0.025), indicating a 67% relative risk reduction associated with positive event recording (Table 6).
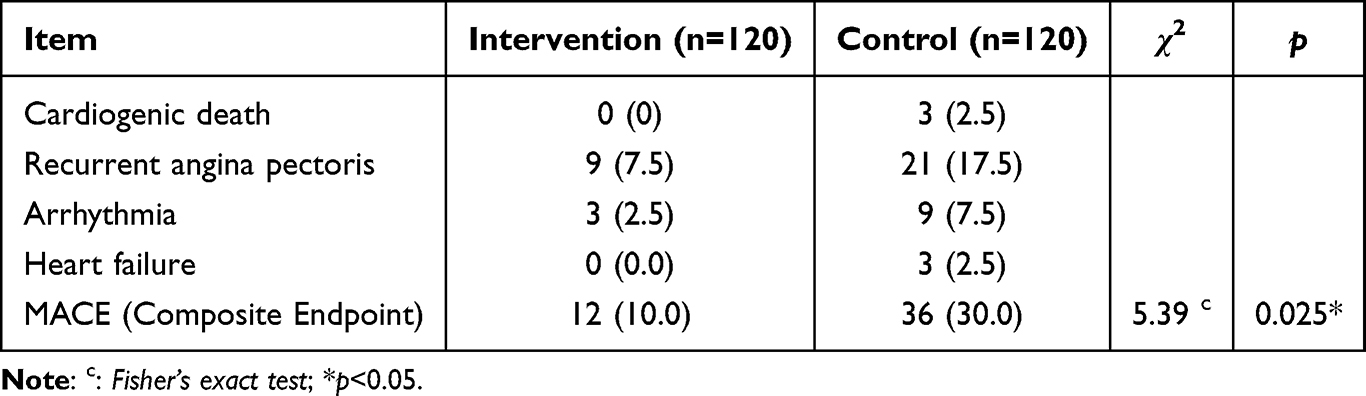 |
Table 6 Comparison of MACE Within 6 Months [Frequency (%)] |
Discussion
This study investigated the impact of positive event recording on the rehabilitation outcomes of elderly CHD patients with anxiety. The findings demonstrate that positive event recording effectively alleviates anxiety levels in this population. At both the conclusion of the intervention and the 3-month follow-up, the intervention group exhibited significantly lower SAS scores compared to the control group. Furthermore, the intervention group showed significantly higher scores in psychological capital and treatment compliance behavior than the control group. These results indicate that through positive event recording, patients can develop a more optimistic attitude toward their condition, thereby enhancing their initiative in treatment compliance and maintaining healthier lifestyles and medication behaviors. Additionally, the study revealed a lower incidence of MACE in the intervention group, along with better clinical indicators (except for systolic blood pressure) compared to the control group. This observation may be attributed to the study’s focus on elderly patients with CHD. Compared with younger populations, elderly CHD patients typically exhibit significantly reduced arterial elasticity, which is mainly caused by the natural aging-related decrease in elastic fibers and excessive proliferation of collagen fibers in the vascular wall, further leading to vascular stiffness and impaired diastolic function. The improvement in clinical treatment outcomes was mainly attributed to the enhancement of patients’ treatment compliance. The recording of positive events alleviated patients’ anxiety and strengthened their psychological resilience, thereby promoting their continuous adherence to drug treatment, lifestyle adjustments, and subsequent follow-up measures. The improvement in compliance further reduced cardiovascular risk factors and decreased the occurrence of adverse events.
Currently, CHD has become a leading cause of death among urban and rural residents in China.2 Relying solely on pharmacological or surgical interventions cannot fully reverse the pathological progression of coronary atherosclerosis. Postoperative negative emotional states such as anxiety can influence patients’ behavioral patterns (including smoking, dietary habits, physical activity, and treatment compliance) or directly impact the occurrence and progression of cardiovascular diseases through biological mechanisms.35 Fredrickson et al (2008) proposed the “Broaden-and-Build” theory, suggesting that positive emotions can expand individuals’ cognitive and behavioral capacities, thereby promoting health and development.36 Positive event recording constitutes an active process of emotional expression. Our study focused on patients’ latent positive resources, assisting them in discovering their inherent strengths, enhancing positive emotions, and fostering positive development through employing the intervention of positive event recording. This approach provides novel insights and references for developing secondary prevention strategies for CHD.
Our previous research has investigated the impact of negative emotions on patient prognosis, showing that anxiety and other negative emotions increase the risk of postoperative adverse cardiovascular events, thereby establishing a solid practical foundation for current work.37 The results of this study indicate that the intervention group demonstrated over 85% compliance with positive event recording, reflecting good acceptance of various recording themes among CHD patients with anxiety. During follow-up, most patients reported no difficulties in maintaining the 3-month recording regimen, though individual patients acknowledged occasional challenges due to personal inertia. Notably, all intervention group patients expressed willingness to continue maintaining records and integrating positive awareness into their daily lives.
In this trial, no significant differences were observed in baseline characteristics between the two groups. Post-intervention comparisons of anxiety levels revealed that the intervention group demonstrated significantly lower anxiety scores than the control group both at the end of the intervention (3 months after discharge) and the end of follow-up period (6 months after discharge). CHD patients often face disease-related stress and insufficient health literacy. Notably, recording positive events helps prevent emotional withdrawal and guides patients in rationally managing their emotions, thereby enhancing their active participation in treatment. Regarding psychological capital improvement, the intervention group showed significantly higher scores than the control group. This can be attributed to positive event recording activating patients’ intrinsic psychological resources, consequently improving individual psychological capital across four dimensions: self-efficacy, optimism, hope, and resilience. The intervention group also established significantly higher CHD treatment compliance behavior scale scores than the control group, indicating that patients developed more constructive attitudes toward their condition through positive event recording, leading to greater initiative in treatment compliance and maintenance of healthy lifestyles and medication regimens.
During the process of positive event recording, patients serve as the primary participants by documenting events they perceive as positive. This approach effectively engages their initiative in disease management while maintaining operational simplicity and cost-effectiveness. Furthermore, positive event recording can effectively help patients establish healthy lifestyles to cope with stress. Currently, this approach has been established as a secondary prevention measure for CHD patients in China, potentially offering novel insights for the management of CHD patients in other regions worldwide.38
Limitations
Although our study has achieved certain outcomes, several limitations should be acknowledged. First, constrained by time, human resources, and funding, this research was conducted solely in a single hospital in Soochow (Jiangsu, China). Future trials should incorporate CHD patients with anxiety from hospitals at different levels to further explore the role of positive psychology. Second, the current investigation employed only one positive psychological intervention method. Third, this study did not take the Transtheoretical Model of Behavior Change (TTM) as the theoretical basis in the design stage. In the future, the TTM model will be combined to optimize the positive event recording intervention from the perspective of behavior change stages. Subsequent studies could integrate multiple psychological intervention approaches to identify optimal treatment protocols. We plan to conduct large-sample, multi-center, high-quality randomized controlled trials in future research to further validate the role of positive event recording in health maintenance and promotion, thereby potentially providing reliable evidence for its clinical implementation and application.
Conclusions
In conclusion, positive event recording demonstrates promising role in managing anxiety among patients with CHD. This intervention significantly alleviates anxiety symptoms, enhances psychological capital, improves treatment compliance, and reduces the incidence of MACE in elderly CHD patients. As a rapid, cost-effective, practical, and easily implementable approach, it potentially provides a safer and more effective adjunctive therapeutic option for CHD patients with anxiety. Future applications could integrate this method with other psychological interventions to further optimize rehabilitation outcomes and enhance overall well-being in this patient population.
Data Sharing Statement
The datasets generated and analyzed in the study are available from the corresponding author, Qing Wu, on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee of Soochow University (Jiangsu, China) (Ethics Approval No. SUDA20200604H01) and was performed in treatment compliance with the Declaration of Helsinki. The trial is registered in the Chinese Clinical Trial Registry (Registration Code: ChiCTR2000034538). All study participants were fully voluntary, and any participant could choose to withdraw from the study at any stage. Written informed consent was obtained from all participants.
Acknowledgments
De-Jing Yuan and Cui-Lian Chen are co-first authors for this study. This study was supported by the Project of Suzhou Key Laboratory of Geriatric Intelligent nursing and health preservation. The authors thank all the subjects who participated in this study and the staff at the First Affiliated Hospital of Soochow University, for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This trial was supported by Research Project of Suzhou Nursing Society in 2024 (SZHL-A-202407), Nursing Research Project of the First Affiliated Hospital of Soochow University in 2026 (HLYJ-2026-09), the 2025 Nursing Discipline Research Project of the Chinese Medical Association Press (CMAPH-NRG2025036) and the Multi-center Clinical Research Project for Major Diseases in Suzhou (Grant Number: DZXYJ202302). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. GBD. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–16. doi:10.1016/S0140-6736(18)32203-7
2. Center For Cardiovascular Diseases The Writing Committee Of The Report On Cardiovascular Health And Diseases In China N; National Center For Cardiovascular Diseases The Writing Committee Of The Report On Cardiovascular Health And Diseases In China. Report on cardiovascular health and diseases in China 2023: an updated summary. Biomed Environ Sci. 2024;37(9):949–992. doi:10.3967/bes2024.162
3. Moussa ID, Mohananey D, Saucedo J, et al. Trends and outcomes of restenosis after coronary stent implantation in the United States. J Am Coll Cardiol. 2020;76(13):1521–1531. doi:10.1016/j.jacc.2020.08.002
4. Cole JA, Smith SM, Hart N, Cupples ME. Do practitioners and friends support patients with coronary heart disease in lifestyle change? a qualitative study. BMC Fam Pract. 2013;14(1):126. doi:10.1186/1471-2296-14-126
5. Liu JX, Lei SY, Cheng JN, Yang F. Best evidence summary on anxiety and depression management in adult patients with coronary heart disease. Chin J Health Manag. 2022;16:565–571.
6. Blumenthal JA, Smith PJ, Jiang W, et al. Effect of exercise, escitalopram, or placebo on anxiety in patients with coronary heart disease: the understanding the benefits of exercise and escitalopram in anxious patients with coronary heart disease (UNWIND) randomized clinical trial. JAMA Psychiatry. 2021;78(11):1270–1278. doi:10.1001/jamapsychiatry.2021.2236
7. Shepardson RL, Buchholz LJ, Weisberg RB, Funderburk JS. Psychological interventions for anxiety in adult primary care patients: a review and recommendations for future research. J Anxiety Disord. 2018;54:71–86. doi:10.1016/j.janxdis.2017.12.004
8. Li J, Gao X, Hao X, et al. Yoga for secondary prevention of coronary heart disease: a systematic review and meta-analysis. Complement Ther Med. 2021;57:102643. doi:10.1016/j.ctim.2020.102643
9. Seligman MEP. Positive psychology: a personal history. Annu Rev Clin Psychol. 2019;15(1):1–23. doi:10.1146/annurev-clinpsy-050718-095653
10. Park N, Peterson C, Szvarca D, Vander Molen RJ, Kim ES, Collon K. Positive psychology and physical health: research and applications. Am J Lifestyle Med. 2016;10(3):200–206. doi:10.1177/1559827614550277
11. Pan L, Yeung NCY. Positive psychology interventions for improving self-management behaviors in patients with type 1 and type 2 diabetes: a narrative review of current evidence. Curr Diab Rep. 2023;23(11):329–345. doi:10.1007/s11892-023-01525-z
12. Macaskill A. Review of positive psychology applications in clinical medical populations. Healthcare. 2016;4(3):66. doi:10.3390/healthcare4030066
13. Corno G, Etchemendy E, Espinoza M, et al. Effect of a web-based positive psychology intervention on prenatal well-being: a case series study. Women Birth. 2018;31(1):e1–e8. doi:10.1016/j.wombi.2017.06.005
14. Huffman JC, DuBois CM, Millstein RA, Celano CM, Wexler D. Positive psychological interventions for patients with type 2 diabetes: rationale, theoretical model, and intervention development. J Diabetes Res. 2015;2015:428349. doi:10.1155/2015/428349
15. Hardie P, O’Donovan R, Jarvis S, Redmond C. Key tips to providing a psychologically safe learning environment in the clinical setting. BMC Med Educ. 2022;22(1):816. doi:10.1186/s12909-022-03892-9
16. Hobbs C, Armitage J, Hood B, Jelbert S. A systematic review of the effect of university positive psychology courses on student psychological wellbeing. Front Psychol. 2022;13:1023140. doi:10.3389/fpsyg.2022.1023140
17. Brooks HL, Rushton K, Lovell K, et al. The power of support from companion animals for people living with mental health problems: a systematic review and narrative synthesis of the evidence. BMC Psychiatry. 2018;18(1):31. doi:10.1186/s12888-018-1613-2
18. Huffman JC, Feig EH, Zambrano J, Celano CM. Positive psychology interventions in medical populations: critical issues in intervention development, testing, and implementation. Affective Sci. 2023;4(1):59–71. doi:10.1007/s42761-022-00137-2
19. Wang X, Shang S, Yang H, et al. Associations of psychological distress with positive psychological variables and activities of daily living among stroke patients: a cross-sectional study. BMC Psychiatry. 2019;19(1):381. doi:10.1186/s12888-019-2368-0
20. Pennebaker JW, Beall SK. Confronting a traumatic event: toward an understanding of inhibition and disease. J Abnorm Psychol. 1986;95(3):274–281. doi:10.1037/0021-843X.95.3.274
21. Tian X, Zhou X, Sun M, et al. The effectiveness of positive psychological interventions for patients with cancer: a systematic review and meta-analysis. J Clin Nurs. 2024;33(9):3752–3774. doi:10.1111/jocn.17358
22. Lai J, Song H, Wang Y, et al. Efficacy of expressive writing versus positive writing in different populations: systematic review and meta-analysis. Nursing Open. 2023;10(9):5961–5974. doi:10.1002/nop2.1897
23. Ski CF, Taylor RS, McGuigan K, et al. Psychological interventions for depression and anxiety in patients with coronary heart disease, heart failure or atrial fibrillation. Cochrane Database Syst Rev. 2024;4(4):Cd013508. doi:10.1002/14651858.CD013508.pub3
24. Ge JB, Xu Y, Wang C. Internal Medicine.
25. Duan QQ, Sheng L. The clinical validity of the self-rating anxiety and depression scale. Chinese J Mental Health. 2012;26:676–679.
26. Huang YQ. Control of random errors and sample size determination in medical research. Chin Mental Health J. 2015;11:874–880.
27. Shen Q, Wu Y, Zhou Y, et al. A cross-sectional study of risk factors for coronary heart disease in secondary prevention for patients with the disease in China. J Clin Nurs. 2025;34(7):2864–2884. doi:10.1111/jocn.17428
28. Zhang K, Zhang S, Dong YH. Positive psychological capital: its measurement and relationship with mental health. J Psychology Behav Res. 2010;8:58–64.
29. De Geest S, Sabaté E. Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs. 2003;2(4):323. doi:10.1016/S1474-5151(03)00091-4
30. Lu M, Ma J, Lin Y, Zhang X, Shen Y, Xia H. Relationship between patient’s health literacy and adherence to coronary heart disease secondary prevention measures. J Clin Nurs. 2019;28(15–16):2833–2843. doi:10.1111/jocn.14865
31. Zhang H, Zhao QH. The impact of family health education on compliance behavior of coronary heart disease patients. Guangdong Med J. 2007;2011–2013.
32. Fernandes AC, McIntyre T, Coelho R, Prata J, Maciel MJ. Impact of a brief psychological intervention on lifestyle, risk factors and disease knowledge during Phase I of cardiac rehabilitation after acute coronary syndrome. Revista Portuguesa de Cardiologia. 2019;38(5):361–368. doi:10.1016/j.repc.2018.09.009
33. Hernandez R, Cohn M, Hernandez A, et al. A web-based positive psychological intervention to improve blood pressure control in spanish-speaking hispanic/latino adults with uncontrolled hypertension: protocol and design for the ¡Alégrate! randomized controlled trial. JMIR Res Protoc. 2020;9(8):e17721. doi:10.2196/17721
34. Makarem N, Castro-Diehl C, St-Onge M-P, et al. Redefining cardiovascular health to include sleep: prospective associations with cardiovascular disease in the mesa sleep study. J Am Heart Assoc. 2022;11(21):e025252. doi:10.1161/JAHA.122.025252
35. Huang P, Yan L, Li Z, et al. Potential shared gene signatures and molecular mechanisms between atherosclerosis and depression: evidence from transcriptome data. Comput Biol Med. 2023;152:106450. doi:10.1016/j.compbiomed.2022.106450
36. Fredrickson BL, Cohn MA, Coffey KA, Pek J, Finkel SM. Open hearts build lives: positive emotions, induced through loving-kindness meditation, build consequential personal resources. J Pers Soc Psychol. 2008;95(5):1045–1062. doi:10.1037/a0013262
37. Hu -Y-Y, Jiang X, Mao F-Y, et al. Effect of positive event recording based on positive psychology on healthy behaviors and readmission rate of patients after PCI: a study protocol for a prospective, randomized controlled trial. Trials. 2022;23(1):1013. doi:10.1186/s13063-022-06964-9
38. Zhao D, Hu DY. New evidence and insights of cardiac rehabilitation strategies in secondary prevention of coronary heart disease in China. Chinese J Cardiovascu Dis. 2024;52:973–975.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.