Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Effects of multiple training modalities in patients with Alzheimer’s disease: a pilot study
Authors Tai SY, Hsu CL, Huang SW, Ma TC, Hsieh WC, Yang YH
Received 2 July 2016
Accepted for publication 31 August 2016
Published 1 November 2016 Volume 2016:12 Pages 2843—2849
DOI https://doi.org/10.2147/NDT.S116257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wai Kwong Tang
Shu-Yu Tai,1–4 Chia-Ling Hsu,5 Shu-Wan Huang,5 Tzu-Chiao Ma,6,7 Wen-Chien Hsieh,8,9 Yuan-Han Yang5,7,10,11
1Department of Family Medicine, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung Medical University, 2Department of Family Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, 3Department of Family Medicine, School of Medicine, College of Medicine, Kaohsiung Medical University, 4Research Center for Environmental Medicine, Kaohsiung Medical University, 5Department of Neurology, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung Medical University, 6Graduate Institute of Oral Health Sciences, Kaohsiung Medical University, 7Mentality Protection Center, Fo Guang Shan Compassion Foundation, 8Department of Social Work, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung Medical University, 9Department of Sociology and Social Work, Kaohsiung Medical University, 10Department of Neurology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, 11Department of and Master’s Program in Neurology, Faculty of Medicine, Kaohsiung Medical University, Kaohsiung City, Taiwan
Objective: This pilot study investigated the effects of multiple training modalities on cognition, neuropsychiatric symptoms, caregivers’ burden, and quality of life in patients with Alzheimer’s disease (AD).
Patients and methods: This intervention study was conducted in 24 patients with AD aged ≥65 years with a Clinical Dementia Rating (CDR) score of 0.5–1. The patients were assigned to receive multiple training modalities (1 hour for each training: Tai Chi, calligraphy, and drawing) over a 6-week period in either the experimental group (n=14) or the comparison group (n=10). A series of neuropsychological tests – namely the Traditional Chinese version Mini-Mental Status Examination, Cognitive Assessment Screening Instrument (CASI), Neuropsychiatric Inventory and the Neuropsychiatric Inventory Caregiver Distress Scale, and the Clinical Dementia Rating Sum of Boxes scale – were conducted at the baseline and after the intervention. The World Health Organization Quality of Life-BREF (WHOQOL-BREF) and Zarit Caregiver Burden Scale were used to assess the quality of life and caregivers’ burden, respectively. Independent sample t-test and paired sample t-test were used to analyze the data.
Results: After the intervention, the experimental group reported higher scores in the orientation domain of CASI (P=0.007) and in the psychiatry domain of WHOQOL-BREF (P=0.042) compared with the comparison group. Caregivers’ distress was significantly decreased in the experimental group (P=0.035) but not in the comparison group (P=0.430).
Conclusion: The multiple training modalities improved scores in the orientation domain of CASI and psychiatry domain of WHOQOL-BREF in patients with AD. Moreover, the intervention reduced caregivers’ distress.
Keywords: multiple training modalities, Alzheimer’s disease, quality of life, cognitive function, caregivers’ burden
Introduction
The rapid increase in the elderly population (≥65 years) has become a challenging medical problem in developed countries.1,2 The proportion of elderly people in the total population of Taiwan has risen continually over the past 3 decades from 4.1% in 1980 to 11.5% in 2013; this is the highest rate of aging worldwide.3 Dementia is a major public health problem related to the aging population in developed countries, and Alzheimer’s disease (AD), a chronic neurodegenerative disease that usually starts slowly and worsens over time, accounts for 60%–70% of dementia cases.4,5 As the disease progresses, symptoms can include problems with language, disorientation (eg, getting lost easily), mood swings, loss of motivation, lack of self-care, and challenging behavior.4,5 These symptoms progressively interfere with vital activities of daily living and independence.6 Effective nonpharmacological interventions that entail fewer side effects compared with pharmacological interventions must be developed to lessen the functional impact of AD.7,8
Some traditional Chinese approaches may improve cognitive and physical function in the elderly.9,10 For example, Tai Chi Chuan (Tai Chi) is a traditional Chinese aerobic mind–body exercise with mild-to-moderate intensity that has recently become popular worldwide; it is appropriate for all ages.9 Recent studies have demonstrated that Tai Chi is safe and effective for patients with neurological diseases (eg, stroke, Parkinson’s disease, traumatic brain injury, multiple sclerosis, and cognitive dysfunction),11–13 orthopedic diseases (eg, osteoarthritis, osteoporosis, lower back pain, and musculoskeletal disorder),14 and cardiovascular diseases (eg, acute myocardial infarction, coronary artery bypass grafting surgery, and heart failure).15 Tai Chi also promotes general health and well-being.16
Chinese calligraphic handwriting and drawing, two traditional Chinese arts, require integration of the mind and body with characters (Chinese alphabet) through an interwoven dynamic process. These arts involve visual perception of the characters, spatial structuring of the characters, cognitive planning, and maneuvering of the brush to follow specific character configurations. Clinical research has found that calligraphy used as therapy may improve behavioral and psychosomatic disorders.17 They also have a therapeutic effect on hypertension and other diseases, such as type 2 diabetes.18,19 Moreover, calligraphic writing may improve attention span and concentration and may facilitate relaxation and emotional stabilization.20,21 For instance, calligraphy has been reported to successfully enhance spatial ability, visual attention, and picture memory in people with AD.22,23 Similarly, intellectual leisure activities, such as calligraphy, in later life may delay cognitive deterioration.24
Tai Chi, calligraphy, and drawing interventions appear to have the potential to minimize age-related problems; therefore, we initiated a pilot trial to examine the effects of short-term multiple training modalities in patients with AD. This trial enables us to determine the feasibility of the combined intervention as a nondrug training modality against age-related cognitive and psychiatric dysfunction in the Taiwanese population.
Patients and methods
We conducted a pretest–posttest comparison pilot study to evaluate the effects of multiple training modalities on the level of cognition, neuropsychiatric symptoms, caregivers’ burden, and quality of life (QOL) in patients with AD. The study was conducted from July 27, 2014 to May 26, 2015.
Ethical considerations
Patients were voluntary participants in the study, and they were informed about the purpose of the study. A written informed consent that includes the research title, purpose, explanation of the research, and the procedures of the study was obtained from each eligible participant. Risks and benefits were also explained clearly to the participants. Side effects arising from the multiple training modalities are rare. Normal reactions, including dyspnea and tiredness while engaged in Tai Chi, that may occur were easily resolved by resting. Each participant was given the opportunity to ask questions and he or she was free to refuse to answer any questions and any assessments, and may withdraw from the study at any time. Participants were protected from discomfort and harm during the study. All procedures were approved by the Institutional Review Board of Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUHIRB-20140015).
Participants
Participants were recruited from the neurological outpatient department of Kaohsiung Municipal Ta-Tung Hospital located in the southern part of Taiwan. The inclusion criteria were as follows: 1) >65 years of age, 2) AD with a Clinical Dementia Rating (CDR) score of 0.5–1, 3) upper limb mobility sufficient to perform requisite finger-pointing tasks, such as flexing and extending the shoulder, elbow, wrist, and fingers, and 4) no neurological or musculoskeletal diseases, such as stroke and visual and auditory impairments. The exclusion criteria were as follows: 1) could not finish the 6-week training course and 2) could not accept the neuropsychological tests. Any participant, who missed any of the 6-week training course or pre/posttest were withdrawn from the study. Twenty-four participants who met the inclusion and exclusion criteria were invited. After obtaining the written informed consent, 14 and ten participants were assigned to the experimental and comparison groups, respectively.
Multiple training modalities
In Asian countries, Tai Chi, calligraphy, and drawing are the three most widely practiced traditional Chinese leisure activities. The Tai Chi program is a 24-form Yang style Tai Chi, which was modified and tailor-made for our target population by two Tai Chi experts. This modified 24-form Tai Chi is designed for easy learning and mastery in a shorter period. The modified forms were also reviewed by an experienced physiotherapist to confirm their safety and feasibility to be used on the target participants. During the Tai Chi practice sessions, an experienced Tai Chi instructor will lead the participants who will replicate the motions, postures, and speed of movement. Chinese calligraphy handwriting, or the Chinese brush writing, often regarded as a unique form of art in Chinese culture, is the writing of Chinese characters by hand using a soft-tipped brush. Drawing is a form of visual art in which a person uses various drawing instruments to mark paper or another two-dimensional medium. They are often practiced to stabilize and improve both the mind and body. In the multiple training modalities intervention employed in this study, specialists trained the participants for 1 hour in each of these three modalities.
Procedure
Participants in the intervention group (N=14) attended 3 hours of multiple training modalities trained by the specialists twice per week for 6 weeks. This duration is based on previous studies, that is, an average frequency of once per week for 12-week intervention of Tai Chi can improve physical performance of healthy elderly people25 and patients with chronic illnesses.26 We chose 6 weeks (twice per week) for our subjects as the training period to evaluate the effect of the short-term multiple training modalities. Participants in the comparison group (N=10) were advised to maintain their routine activities. To enhance the internal validity of the study findings, participants in the comparison group were arranged to join non-health-related social activities such as playing cards and singing at the activity center during the same period. Both at the beginning and after 6 weeks of the training, the senior neuropsychologist spent about 1 hour to assess each participant’s cognition, psychological (and behavior) status, global functional status, and QOL using a series of neuropsychiatric assessment tools. The burden of care on the caregivers was also assessed.
Measurement outcomes
To evaluate the effects of multiple training modalities on AD, each participant underwent a series of neuropsychological tests – namely the Traditional Chinese version Mini-Mental Status Examination (TC-MMSE),27 the Cognitive Assessment Screening Instrument (CASI),28 the Neuropsychiatric Inventory (NPI) and the Neuropsychiatric Inventory Caregiver Distress Scale (NPI-D)29 for patients and caregivers, respectively, and the CDR Sum of Boxes (CDR-SB)30 scale – at the baseline and after 6 weeks of the intervention. In addition, the Chinese version of the short-form Geriatric Depression Scale (GDS-S),31,32 which has high internal consistency and test–retest reliability,33 was used to assess the depression status of informants (GDS-S_inf) and patients (GDS-S_pt).
The World Health Organization Quality of Life-BREF (WHOQOL-BREF) test34 was used to assess the QOL. This instrument was derived from the WHOQOL-100. The WHOQOL-BREF questionnaire contains two items from the Overall QOL and General Health and 24 items of satisfaction that were divided into the following four domains: Physical health with seven items (domain 1), psychological health with six items (domain 2), social relationships with three items (domain 3), and environmental health with eight items (domain 4).35,36 The WHOQOL-BREF was reliable and valid in the assessment of the QOL of all population.37–39 To collect data on caregivers, the Zarit Caregiver Burden Scale was used.40 This scale has 22 items and measures the mental burden on caregivers. All assessments were performed by a blinded and senior neuropsychologist. Information from a knowledgeable collateral source, usually a spouse or an adult child, was also collected. CASI comprises 25 items whose sum scores range from 0 to 100. CASI has ten subscales that assess attention (maximum score: 8), concentration (10), orientation (18), short-term memory (12), long-term memory (10), language abilities (10), visual construction (10), category fluency (10), and abstraction (6) and judgment (6).41
Data analysis
Descriptive statistics was used to summarize the sample characteristics and target variables. The frequency distributions were determined for nominal data (ie, gender), and mean and SD were calculated for continuous data (ie, age, educational level, and neuropsychiatric assessment scores). Paired t-test analysis of covariance was used to compare the differences of pre/posttest in neuropsychiatric assessments scores, depression status, QOL, and caregivers’ burden. Independent sample t-tests were applied to examine between-group differences in assessment outcomes. P<0.05 was considered statistically significant. Data were analyzed using SPSS for Windows 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Table 1 lists the demographic characteristics of the participants in the study groups. Twenty-four participants were recruited for this study, and 14 and ten participants were assigned to the experimental and comparison groups, respectively. All participants completed the baseline and postintervention assessments. No significant differences were observed between the experimental and comparison groups for all the baseline variables.
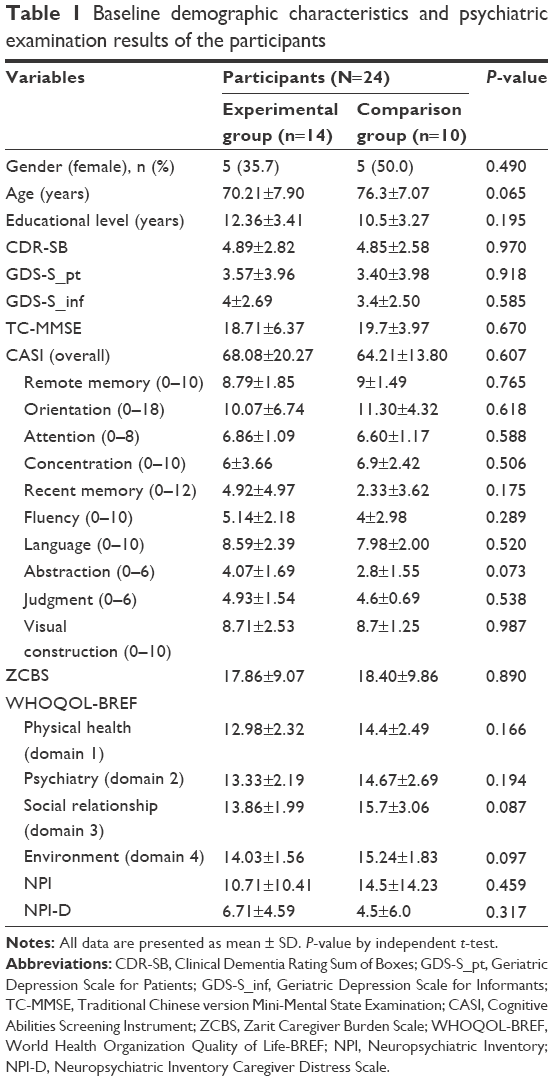 | Table 1 Baseline demographic characteristics and psychiatric examination results of the participants |
Assessment of cognitive function and depression
The baseline–postintervention differences in the TC-MMSE and CDR-SB scores were nonsignificant in both the experimental and comparison groups, as shown in Table 2 (TC-MMSE: P=0.124 in the experimental group vs P=0.626 in the comparison group; CDR-SB: P=0.525 in the experimental group vs P=0.329 in the comparison group). Compared with the baseline GDS-S scores, the postintervention GDS-S_pt and GDS-S_inf scores did not significantly decrease in the experimental group (GDS-S_pt: P=0.272; GDS-S_inf: P=0.749) and in the comparison group (GDS-S_pt: P=0.173; GDS-S_inf: P=0.456). The baseline–postintervention CASI scores did not differ significantly, but in the subscale scores for orientation, a significant increase in the experimental group (P=0.045) and a significant decrease in the comparison group (P=0.045) were observed; no significant differences were observed in the other nine subscales. In addition, a significant difference was observed between groups on the orientation and language subscale (P=0.007 and 0.020).
 | Table 2 Effect of multiple training modalities on cognitive function and depression assessment |
Assessment of quality of life, caregiver burden, and neuropsychiatric symptoms
The WHOQOL-BREF uses four domains to assess the QOL of patients, namely physical health, psychiatry, social relationships, and environment (Table 3). Compared with the baseline score, the postintervention score for the domain of psychiatry increased in the experimental group and decreased in the comparison group, with a significant between-group difference (P=0.042). The scores for the other domains did not differ significantly. The Zarit score did not change significantly in the experimental group (P=0.858) or in the comparison group (P=0.089). However, the NPI-D score decreased significantly in the experimental group (P=0.035) but not in the comparison group (P=0.758; Table 3).
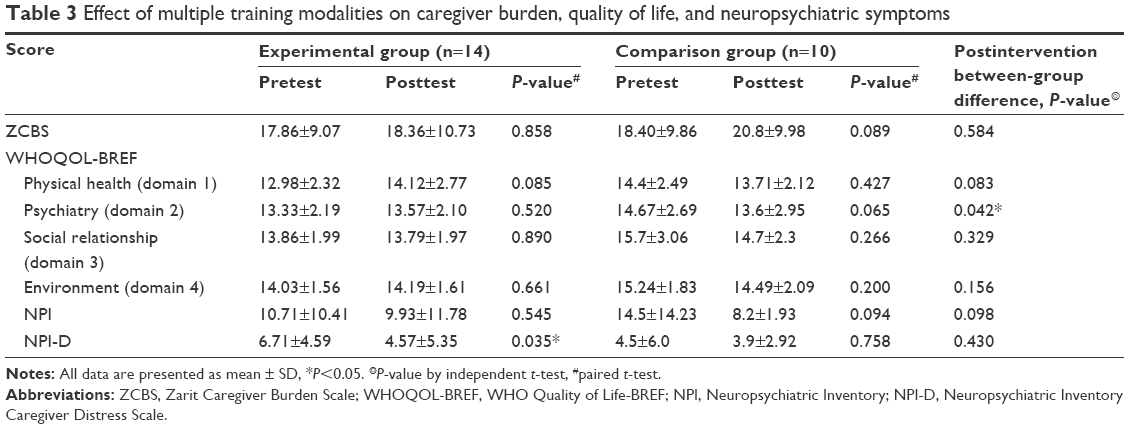 | Table 3 Effect of multiple training modalities on caregiver burden, quality of life, and neuropsychiatric symptoms |
Discussion
This experimental study was conducted to investigate the effects of short-term multiple training modalities on AD. The 6-week intervention program led to a significant difference between the experimental and comparison groups in the orientation subscale and NPI-D scores. Furthermore, scores for the psychiatry domain of WHOQOL-BREF improved slightly in the experimental group but decreased in the comparison group; the between-group difference was significant.
Previous studies have evidenced the positive effects of Tai Chi9–13,42–45 and calligraphy therapy17,19,21,22,24 on the cognitive and physical functions of elderly with and without cognitive impairment. However, the measures of effect were limited.44 In addition, the study duration of the previous similar studies was on average 30–60 minutes per week for 12–24 weeks, which was less frequent but longer than our study.9 Besides, they usually explored the effect of the single training modality. This is the first study to use multiple neuropsychological tests to measure depression status, QOL, and caregivers’ burden after short-term multiple training modalities in patients with AD. With AD progression, patients with AD gradually lose their independence in performing tasks and develop many other neuropsychological problems, which affect the caregivers as well.46 We conducted this study on patients with AD with a CDR score of 0.5–1 (ie, patients with early-stage AD who could meaningfully participate in the intervention program) to explore whether short-term multiple training modalities could facilitate rapid amelioration of various AD symptoms.
This pilot study’s result also indicates that the orientation (a subscale of CASI) significantly responded to multiple training modalities. The training program, including the integration of the mind and body, may enhance the visuospatial skills of patients with AD,20 despite no significant difference in the overall CASI and TC-MMSE scores. However, the language subscale was declined in the experimental group; in contrast, improved in the comparison group with significant between-group difference. Compared with the other similar studies, the results were equivocal about the effect of exercise (eg, Tai Chi, aerobic exercise or mind–body practition) on language.11 However, the interventions and tests are different. Language is the ability to acquire and use complex systems of communication, and the training needs practice. Maybe the short-term multiple training modalities, which focus on the mind–body exercise and imitation, are not beneficial for the language training; it still needs additional studies to clarify. A comparison of the pretest and posttest means of the GDS-S_pt and GDS-S_inf scores revealed no significant differences between the study groups. However, a significant between-group difference was observed in the psychiatry domain of WHOQOL-BREF. This short-term intervention could not improve depression; nevertheless, it may help improve other psychiatric problems. In a future study, we will explore the effects of the proposed intervention on various mood-related disorders.
AD socially, psychologically, physically, and economically burdens caregivers.47 High incidence rates of physical and mental disorders have been reported in caregivers of patients with dementia.2 Therefore, we analyzed the Zarit scores to investigate the effects of multiple training modalities on caregiver workload. No significant changes in Zarit scores were observed after the intervention. However, a comparison of the pretest and posttest NPI-D means showed a significant decrease in the scores in the experimental group, whereas the comparison group showed no significant change. The NPI-D is a reliable and valid measure of subjective distress in caregivers of patients experiencing the neuropsychiatric symptoms of AD (lower score means lower distress). Generally, compared with rather than cognitive symptoms, neuropsychiatric symptoms are more strongly associated with caregivers’ distress.48 Additional studies are needed to confirm the long-term effects of multiple training modalities on caregivers’ burden.
These encouraging findings must be interpreted in light of these several limitations of this study. First, this study was based on a small sample whose recruitment was not random. Second, demographic data (eg, family history and caregiver status) and certain medical information (eg, comorbidity and comedication), which could influence the results, were unavailable. A comprehensive large-scale randomized clinical trial is necessary to address these limitations.
Conclusion
Short-term multiple training modalities may benefit the orientation and psychiatry domains of QOL in patients with AD. In addition, the proposed program may reduce caregivers’ distress. However, additional large-scale randomized studies that analyze more variables and employ a long-term follow-up must be conducted to verify our findings.
Acknowledgments
The authors appreciate the participants for their cooperation; Mentality Protection Center, Fo Guang Shan Compassion Foundation, and Fo Guang Shan Nan Ping Temple for the space supplement. This study was funded by Kaohsiung Municipal Ta-Tung Hospital (KMTTH-103-034) and partly supported by the grant from Research Center for Environmental Medicine, Kaohsiung Medical University (KMU-TP104A34), Kaohsiung, Taiwan.
Disclosure
The authors report no conflicts of interest in this work.
References
Nowrangi MA, Rao V, Lyketsos CG. Epidemiology, assessment, and treatment of dementia. Psychiatr Clin North Am. 2011;34(2):275–294. | ||
Ritchie K, Lovestone S. The dementias. Lancet. 2002;360(9347):1759–1766. | ||
Staff TCPn. Taiwan Must Address the Challenges of an Aging Society. The China Post News Staff, 2013 Oct 13. | ||
Fisher TJ, Schwartz AC, Greenspan HN, Heinrich TW. Dementia: a complex disease with multiple etiologies and multiple treatments. Int J Psychiatry Med. 2016;51(2):171–181. | ||
Burns A, Iliffe S. Alzheimer’s disease. BMJ. 2009;338:b158. | ||
Salthouse T. Consequences of age-related cognitive declines. Annu Rev Psychol. 2012;63(1):201–226. | ||
Marmeleira J. An examination of the mechanisms underlying the effects of physical activity on brain and cognition. Eur Rev Aging Phys Activity. 2013;10(2):83–94. | ||
Hogan M. Physical and cognitive activity and exercise for older adults: a review. Int J Aging Hum Dev. 2005;60(2):95–126. | ||
Wayne PM, Walsh JN, Taylor-Piliae RE, et al. Effect of Tai Chi on cognitive performance in older adults: systematic review and meta-analysis. J Am Geriatr Soc. 2014;62(1):25–39. | ||
Sun J, Kanagawa K, Sasaki J, Ooki S, Xu H, Wang L. Tai Chi improves cognitive and physical function in the elderly: a randomized controlled trial. J Phys Ther Sci. 2015;27(5):1467–1471. | ||
Miller SM, Taylor-Piliae RE. Effects of Tai Chi on cognitive function in community-dwelling older adults: a review. Geriatr Nurs. 2014;35(1):9–19. | ||
Lam LC, Chan WM, Kwok TC, Chiu HF. Effectiveness of Tai Chi in maintenance of cognitive and functional abilities in mild cognitive impairment: a randomised controlled trial. Hong Kong Med J. 2014;20(3 suppl 3):20–23. | ||
Fogarty JN, Murphy KJ, McFarlane B, et al. Taoist Tai Chi(R) and memory intervention for individuals with mild cognitive impairment. J Aging Phys Act. 2016;24(2):169–180. | ||
Wu G, Millon D. Joint kinetics during Tai Chi gait and normal walking gait in young and elderly Tai Chi Chuan practitioners. Clin Biomech (Bristol, Avon). 2008;23(6):787–795. | ||
Lan C, Lai JS, Wong MK, Yu ML. Cardiorespiratory function, flexibility, and body composition among geriatric Tai Chi Chuan practitioners. Arch Phys Med Rehabil. 1996;77(6):612–616. | ||
Lan C, Chen SY, Lai JS, Wong AM. Tai Chi Chuan in medicine and health promotion. Evid Based Complement Alternat Med. 2013;2013:502131. | ||
Kao HSR. Shufa: Chinese calligraphic handwriting (CCH) for health and behavioural therapy. Int J Psychol. 2006;41(4):282–286. | ||
Guo NF, Kao HSR, Liu X. Calligraphy, hypertension and the type-A personality. Ann Behav Med. 2001;23:S159. | ||
Kao HSR, Ding BK, Cheng SW. Brush handwriting treatment of emotional problems in patients with type II diabetes. Int J Behav Med. 2000;23:S085. | ||
Yang XL, Li HH, Hong MH, Kao HS. The effects of Chinese calligraphy handwriting and relaxation training in Chinese nasopharyngeal carcinoma patients: a randomized controlled trial. Int J Nurs Stud. 2010;47(5):550–559. | ||
Kao HSR, Zhu L, Chao AA, Chen HY, Liu IC, Zhang M. Calligraphy and meditation for stress reduction: an experimental comparison. Psychol Res Behav Manag. 2014;7:47–52. | ||
Kao HSR, Gao GD, Wang M. Brush handwriting treatment of cognitive deficiencies in Alzheimer’s disease patients. Neurobiol Aging. 2000;21(1S):14. | ||
Kao HSR, Gao GD, Wang MQ, Cheung HY, Chiu J. Chinese calligraphic handwriting: treatment of cognitive deficiencies of Alzheimer’s disease patients. Alzheimers Rep. 2000;3:281–287. | ||
Kwok TCY, Bai X, Kao HSR, Li JCY, Ho FKY. Cognitive effects of calligraphy therapy for older people: a randomized controlled trial in Hong Kong. Clin Interv Aging. 2011;6:269–273. | ||
Lindemann U, Hammer W, Muche R, Nikolaus T, Becker C. Postural control in the elderly: effect of a twelve week Tai Chi-Qigong intervention in healthy elderly. Eur J Geriatr. 2003;5:182–186. | ||
Chan AW, Lee A, Lee DT, et al. The sustaining effects of Tai Chi Qigong on physiological health for COPD patients: a randomized controlled trial. Complement Ther Med. 2013;21(6):585–594. | ||
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. | ||
Lin KN, Wang PN, Liu CY, Chen WT, Lee YC, Liu HC. Cutoff scores of the cognitive abilities screening instrument, Chinese version in screening of dementia. Dement Geriatr Cogn Disord. 2002;14(4):176–182. | ||
Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44(12):2308–2314. | ||
Morris JC. The clinical dementia rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–2414. | ||
Burke WJ, Roccaforte WH, Wengel SP. The short form of the Geriatric Depression Scale: a comparison with the 30-item form. J Geriatr Psychiatry Neurol. 1991;4(3):173–178. | ||
Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982–1983;17(1):37–49. | ||
Mui AC. Geriatric Depression Scale as a community screening instrument for elderly Chinese immigrants. Int Psychogeriatr. 1996;8(3):445–458. | ||
Lucas-Carrasco R, Skevington SM, Gomez-Benito J, Rejas J, March J. Using the WHOQOL-BREF in persons with dementia: a validation study. Alzheimer Dis Assoc Disord. 2011;25(4):345–351. | ||
Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychological medicine. 1998;28(3):551–558. | ||
Skevington SM, Sartorius N, Amir M. Developing methods for assessing quality of life in different cultural settings. Soc Psychiatry Psychiatr Epidemiol. 2004;39(1):1–8. | ||
Xia P, Li N, Hau KT, Liu C, Lu Y. Quality of life of Chinese urban community residents: a psychometric study of the mainland Chinese version of the WHOQOL-BREF. BMC Med Res Methodol. 2012;12:37. | ||
Chien CW, Wang JD, Yao G, Hsueh IP, Hsieh CL. Agreement between the WHOQOL-BREF Chinese and Taiwanese versions in the elderly. J Formos Med Assoc. 2009;108(2):164–169. | ||
Zhang Y, Qu B, Lun S, Wang D, Guo Y, Liu J. Quality of life of medical students in China: a study using the WHOQOL-BREF. PLoS One. 2012;7(11):e49714. | ||
Ko KT, Yip PK, Liu SI, Huang CR. Chinese version of the Zarit caregiver burden interview: a validation study. Am J Geriatr Psychiatry. 2008;16(6):513–518. | ||
Teng EL, Hasegawa K, Homma A, et al. The cognitive abilities screening instrument (CASI): a practical test for cross-cultural epidemiological studies of dementia. Int Psychogeriatr. 1994;6(1):45–58; discussion 62. | ||
Li F, Harmer P, Liu Y, Chou LS. Tai Ji Quan and global cognitive function in older adults with cognitive impairment: a pilot study. Arch Gerontol Geriatr. 2014;58(3):434–439. | ||
Lu X, Siu KC, Fu SN, Hui-Chan CW, Tsang WW. Effects of Tai Chi training on postural control and cognitive performance while dual tasking – a randomized clinical trial. J Complement Integr Med. 2016;13(2):181–187. | ||
Zheng G, Liu F, Li S, Huang M, Tao J, Chen L. Tai Chi and the protection of cognitive ability: a systematic review of prospective studies in healthy adults. Am J Prev Med. 2015;49(1):89–97. | ||
Walsh JN, Manor B, Hausdorff J, et al. Impact of short- and long-term Tai Chi mind-body exercise training on cognitive function in healthy adults: results from a hybrid observational study and randomized trial. Glob Adv Health Med. 2015;4(4):38–48. | ||
Forstl H, Kurz A. Clinical features of Alzheimer’s disease. Eur Arch Psychiatry Clin Neurosci. 1999;249(6):288–290. | ||
Thompson CA, Spilsbury K, Hall J, Birks Y, Barnes C, Adamson J. Systematic review of information and support interventions for caregivers of people with dementia. BMC Geriatr. 2007;7:18. | ||
Kaufer DI, Cummings JL, Christine D, et al. Assessing the impact of neuropsychiatric symptoms in Alzheimer’s disease: the neuropsychiatric inventory caregiver distress scale. J Am Geriatr Soc. 1998;46(2):210–215. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.