Back to Journals » Clinical Ophthalmology » Volume 20
Effects of Multimodal and Unimodal Physical Training Interventions on Visual Function in Glaucoma and Elderly Controls – A Pilot Study
Authors Moffack Djuloun C, Al-Nosairy KO, Beyer R, Freitag CW, Stolle FH, Behrens M, Behrendt T, Prabhakaran GT, Thieme H, Schega L, Hoffmann MB ![]()
Received 17 October 2025
Accepted for publication 25 February 2026
Published 20 April 2026 Volume 2026:20 574933
DOI https://doi.org/10.2147/OPTH.S574933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Cynthia Moffack Djuloun,1 Khaldoon O Al-Nosairy,1 Rosalie Beyer,1 Constantin W Freitag,2 Francie H Stolle,1 Martin Behrens,3,4 Tom Behrendt,2 Gokulraj T Prabhakaran,1 Hagen Thieme,1 Lutz Schega,2,* Michael B Hoffmann1,5,*
1Ophthalmic Department, University Hospital, Magdeburg, Germany; 2Department of Sport Science, Institute III, Otto von Guericke University, Magdeburg, Germany; 3University of Applied Sciences for Sport and Management, Potsdam, Germany; 4Department of Orthopedics, Rostock University Medical Center, Rostock, Germany; 5Center for Behavioral Brain Research, Magdeburg, Germany
*These authors contributed equally to this work
Correspondence: Michael B Hoffmann, Ophthalmic Department, University Hospital, Magdeburg, Germany, Tel +49 391 67 13585, Fax +49 391 67 13570, Email [email protected]
Purpose: This study aimed to investigate the effects of a 12-week multimodal motor-cognitive and resistance training (MMI) compared to a unimodal resistance training intervention (UMI) on static and dynamic visual function in glaucoma (GLA) patients and healthy controls (HC).
Methods: Fifteen GLA and 24 age-matched HC participated in this randomized, controlled longitudinal pilot study. Visual function was assessed using clinical parameters and on a treadmill (TM) while standing (static, S0) as well as during walking at 3.5 km/h (S3.5) and a self-preferred speed (SSelf). The following outcomes were measured pre and post 12-weeks of intervention (MMI or UMI): (a) standard clinical measures and (b) TM-related measures, i.e.: 1) best-corrected visual acuity without (VAS) and with crowding (VAC); 2) visual field sensitivity (VF); and 3) contrast sensitivity (CS). A 4-factorial repeated-measures ANOVA (SPEED [S0; S3.5; SSelf] × TIME [pre; post] × INTERVENTION [UMI; MMI] × GROUP [GLA; HC]) was applied to determine significant interaction effects (p ≤ 0.05) and the effect size partial-eta-squared was calculated.
Results: Post-interventional improvement of visual function was absent or minor. Only the main effect of TIME (visual acuity; p = 0.024) and a TIME × INTERVENTION interaction (foveal sensitivity; p = 0.039) were found for standard clinical measures. For S0 vs. S3.5 small effects appeared in post-hoc comparisons, but TIME and TIME × SPEED just failed to reach significance for CS (p = 0.059) and VAs (p = 0.052), respectively. No GROUP interactions were observed.
Conclusion: While trends were evident in this pilot study, the effect of the 12-week interventions on visual function was non-significant and, especially for TM-walking, largely independent of group and intervention type. In future studies, a greater sample size, with more advanced GLA cases, should be included to probe for significant visual function differences between groups and intervention types.
Keywords: dynamic visual function, glaucoma, multimodal training, cognitive training, mobility
Introduction
Glaucoma (GLA), a progressive optic neuropathy, is a leading global cause of irreversible blindness.1 Current estimates expect an increase of affected individuals from 76 million to 112 million by 2040.1 GLA damage impedes activities important for daily living not exclusively in the visual domain, but also with respect to mobility, e.g., via an increased incidence of falling during walking.2 Consequently, GLA has an impact at the individual level due to quality of life reduction3,4 and at the societal level due to health-care cost increase.5,6 However, these conventional measures often overlook broader aspects of functional impairment in GLA patients, particularly those related to motor and cognitive abilities.7 A growing body of evidence suggests that GLA shares morpho-functional changes in the eye and brain similar to those seen in neurodegenerative disorders such as Alzheimer’s disease and that there might be an association with cognitive impairment.8
It has been shown that resistance training mitigated the risk of falls in elderly9,10 and might also increase cognitive performance.11 Recent reports12 also indicate that the combination of motor and cognitive exercise has beneficial effects on motor and/or cognitive function in patients with neurodegenerative diseases, e.g., Alzheimer’s disease8,13,14 and in healthy participants with cognitive decline.15 Moreover, this interventional approach might reduce the risk of falls.9,10 Due to the fact that GLA might be associated with cognitive dysfunction,8 combining motor-cognitive exercises12 with resistance training in GLA management might be of promise to improve mobility and cognitive function eventually translating in an increased quality of life. This prompts the question of whether a combination of motor-cognitive and resistance training (i.e., multimodal intervention [MMI]) improves motor-cognitive function more than resistance training alone (i.e., unimodal intervention [UMI]) in GLA patients, which has, to our knowledge, not been addressed so far.
The present study reflects on a subset of data from a larger randomized controlled trial examining the effects of two physical training interventions (MMI and UMI) on several primary and secondary outcomes (German Clinical Trial Register, ID: DRKS00022519, 05.08.2020, https://drks.de/search/de/trial/DRKS00022519). The primary endpoints include gait kinematics and functional brain connectivity addressed in separate works.2
In the present pilot study, visual function, as a secondary endpoint, is addressed. Specifically, we investigated the influence of a 12-week MMI and UMI on visual function during treadmill (TM) walking in GLA patients and healthy elderly controls. The baseline findings, which were collected 2–3 weeks prior to intervention and previously published,16 indicated that TM walking, compared to standing, showed reduced visual function similarly in both GLA patients and elderly controls (i.e., a visual acuity loss by more than 0.02 logMAR and visual field sensitivity by 1.0 dB visual field mean deviation). Consequently, it is of interest whether MMI or UMI can improve visual function and thus ultimately, reduce the risk of falls. While these interventions may not restore lost retinal ganglion cells, they may facilitate better gait control and hence visual information processing during locomotion, attentional control, and overall adaptation to visual impairment, potentially leading to improve functional vision and quality of life. The underlying rationale being that movement interventions improve gait control and stability and in turn benefit visual tasks that are affected during walking.17 We hypothesized that visual function will be improved after the interventions in GLA, especially following MMI, as this intervention specifically targets visuo-cognition compared to UMI.
Methods
Study Design
To investigate the effect of MMI and UMI, a two-arm randomized controlled prospective longitudinal study was conducted from August 2020 to December 2022. Patients with glaucoma (GLA) and age-matched healthy control (HC) subjects were recruited and randomly assigned to either MMI or UMI using counterbalanced randomization and allocation ratio of 1:1 (Figure 1).
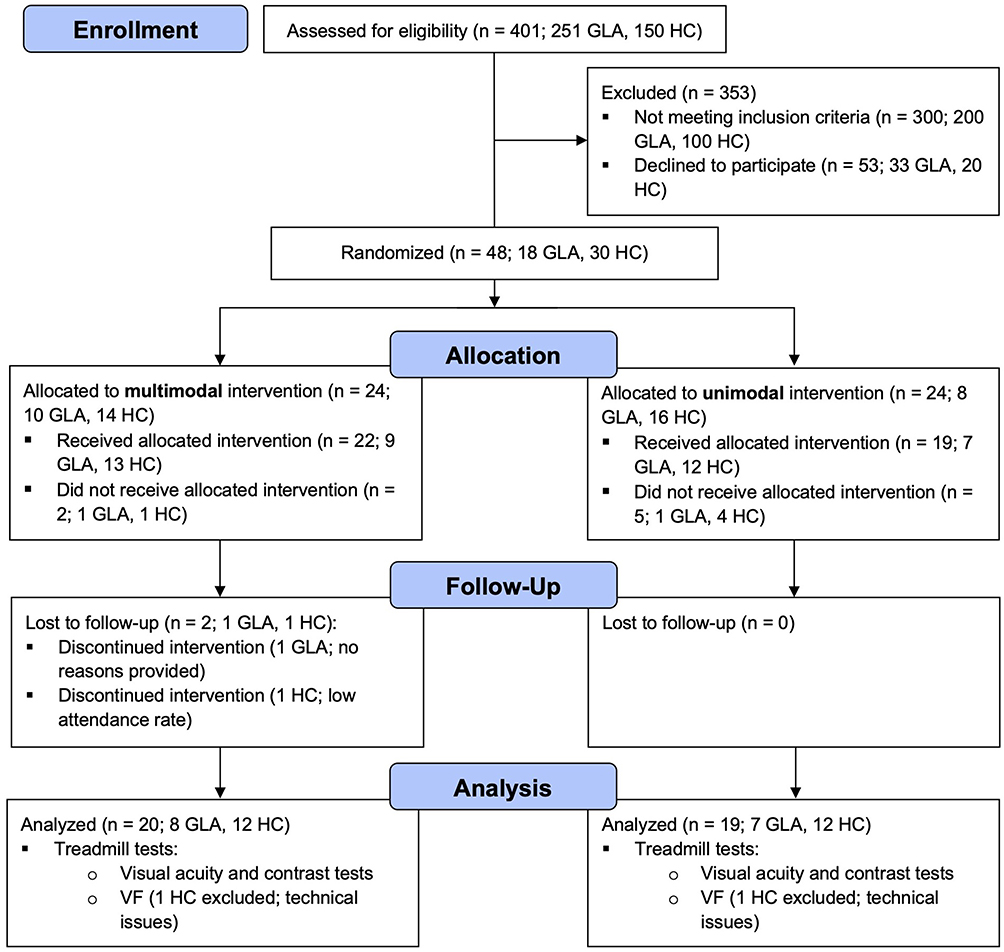 |
Figure 1 CONSORT flow chart for the recruitment process shows the number of participants and dropouts through the study phases. Abbreviations: GLA, glaucoma participants; HC, healthy participants. |
The experimental protocol was approved by the Ethics Committee of the Otto-von-Guericke University of Magdeburg in Germany (registration number: 32/18) and all procedures were in line with the Declaration of Helsinki on experiments on human beings. All visual-function related measurements were taken in the Department of Ophthalmology and at the Otto-von-Guericke University Magdeburg, Germany. The interventions were performed in the Department of Sport Science at the Otto-von-Guericke University Magdeburg, Germany. Reporting was performed in accordance with the Consolidated Standards of Reporting Trials Statement (Consort) for randomized pilot trials.18 All participants gave written informed consent.
Participants
A total of 39 participants, including 15 GLA and 24 HC, were recruited in this study. For GLA, only two of the participants had an advanced stage, two had a mild stage and the rest had a pre-perimetric stage.
Participants underwent complete ophthalmological examination, which is detailed elsewhere.19 Briefly, we assessed best corrected visual acuity, refractive correction for far (at 5 m) with early treatment diabetic retinopathy study charts (ETDRS), slit-lamp exam, intraocular pressure (IOP), fundus exam, and standard tests for visual field (VF) and retinal structure. GLA was defined according to the European Glaucoma Society Terminology and Guidelines for Glaucoma.20 For GLA staging, we used the Hodapp-Parrish Anderson criteria. The following inclusion criteria were applied: 1) age ≥ 60 years; 2) diagnosis of open-angle GLA; 3) patients are under intraocular pressure medications; 4) best corrected visual acuity (BCVA) ≥ 0.8 decimal unless GLA-related in the GLA group; 5) normal visual function parameters unless GLA related; 6) no other conditions affecting visual function such as age-related macular degeneration or retinal detachment; 7) ability to walk at least 6 min without walking support; and 8) visual field defects classified according to the Hodapp-Parish Anderson criteria21 in GLA with defects. Exclusion criteria were as follows: 1) neurological disorders; 2) rheumatism; 3) cardiovascular disorders; 4) stroke; and 5) orthopedic diseases including arthrosis (grade II or higher), musculoskeletal impairment, tendinitis, tenosynovitis, myositis, prosthesis in the lower extremities, and joint replacements.
Interventions
The training (i.e., MMI and UMI) was conducted twice a week on non-consecutive days for 12 weeks resulting in a total of 24 sessions. Each session lasted 60 min and was supervised by experienced instructors.
The MMI was split into: 1) motor-cognitive training; 2) resistance training; and 3) cool-down (i.e., static stretching). Over the course of the intervention, the proportion of time spent on motor-cognitive and resistance training changed (see Table 1). The motor-cognitive exercises consisted of simultaneously performed motor, cognitive, and visual tasks based on the LifeKinetik program.22 These exercises were designed in such a way that it is almost impossible to perform them without making mistakes. If the exercises were performed correctly in 6 out of 10 attempts, the instructor continued with a more difficult exercise. As examples, two exercises are briefly explained below: 1) balls of different colors (e.g., yellow, green, red) are thrown in a circle, whereby a corresponding name must be said for each color (e.g., yellow = persons own name, green = name of the person to whom the ball is to be thrown; and 2) participants line up next to each other and after an announcement (e.g., left, right, front, back) they walked in the corresponding direction (line of vision remained the same, i.e., no returns), whereby a corresponding name for each direction were varied (e.g., right = “1”, left = “2”, front = “3”, back = “4”).
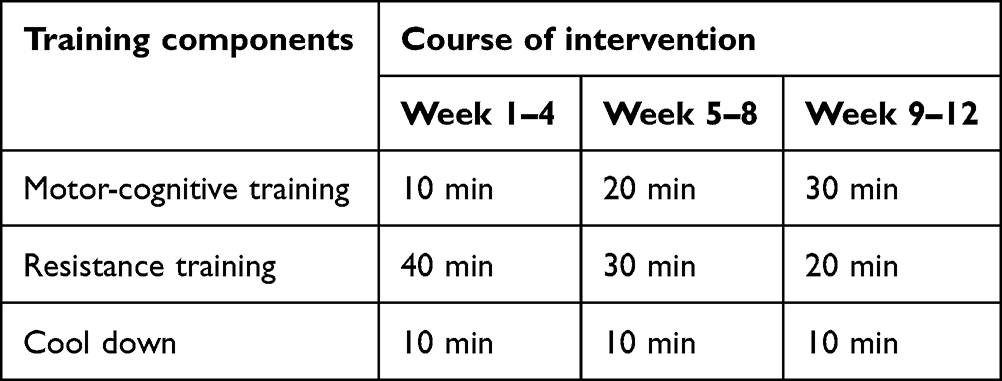 |
Table 1 Multimodal Training Schedule |
The UMI consisted of: 1) 10-min standardized warm-up (i.e., 5 min fast walking and dynamic stretching); 2) 40-min resistance exercises; and 3) 10-min cool-down (i.e., static stretching). The resistance training included multiple-set (2 × 7 repetitions, 30 s rest between sets, time under tension: 2 s concentric and eccentric) circuit training using free weights and weight machines (e.g., dumbbell seated front raise and seated leg press) (Table 2). External training load was adjusted by increasing the weight and controlled via individuals’ rating of perceived exertion (RPE) using the Borg CR 10 Scale (i.e., RPE = 3–4 (moderate to somewhat severe).
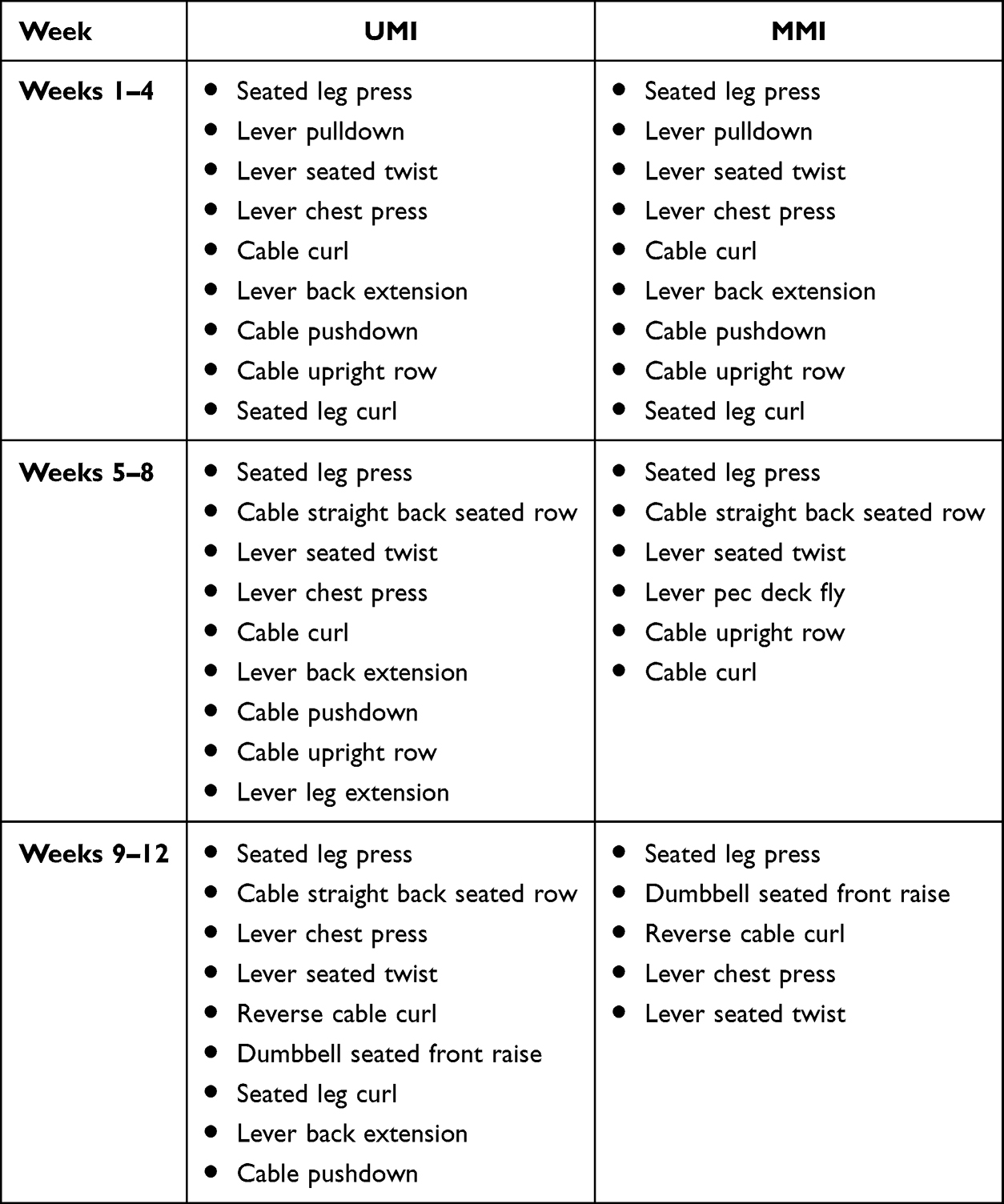 |
Table 2 Resistance Exercises |
Resistance training was carried out in the same way as the MMI, although the number of exercises and its duration varied (see Tables 1 and 2). All exercises were performed while sitting because exercising in a supine or other positions affects the intraocular pressure.23,24 Both interventions ended with a 10-min cool-down consisting of static stretching for the major muscle groups (e.g., standing side stretch, standing forward fold, overhead triceps stretch).
Outcome Parameters
At the start of this study, participants’ demographic and anthropometric data as well as their physical activity level, and visual function were recorded. Standard ophthalmology tests included: i) standard automated perimetry (SAP) for visual field estimation with 24–2 SITA-Fast test (Humphrey Field Analyzer, Carl Zeiss Meditec AG, Jena, Germany) and ii) optical coherence tomography (OCT) of macula and disc using a spectral-domain OCT device with a Glaucoma Module Premium Edition (Heidelberg Spectralis®, Heidelberg Engineering, Heidelberg, Germany). Of note, single- and dual-task gait performance (i.e., stride length, gait velocity) as well as gaze behavior (i.e., saccade duration, fixation duration) were also assessed at the beginning of the study.2,19 Effects of the interventions were scrutinized for: (A) the standard clinical tests including BCVA, VF parameters, e.g., foveal sensitivity and VF MD; and for (B) TM walking testing. For TM walking testing, four visual function tests were performed binocularly [BCVA without crowding (VAs), BCVA with crowding (VAc), contrast sensitivity (CS) and binocular visual field (Bin-VF)] as detailed below. Further, heart rate was also measured during these measurements and averaged for each speed condition.
Heart rate was monitored with a wireless transmitter belt (POLAR Heart Rate Sensor H9) wrapped around the lower part of the chest coupled with the h/p/cosmos® TM setup (h/p/cosmos sports and medical gmbh, Germany). For each Speed condition, the median heart rate was calculated. In case of technical malfunctions with the heart rate transmitter, we used the heart rate value at the end of each session.
Visual Function During TM Walking
Visual function was tested at 5 m and to account for variable viewing distance during TM walking as a confound factor, visual functions were corrected using a distance sensor (Vivior® sensor) as detailed in Beyer et al.16
TM Walking Testing Procedure
Visual functions were tested for 3 speed conditions in a fixed order: 1) static (S0), 2) TM speed of 3.5 km/h (S3.5) and 3) a self-preferred TM speed (SSelf).
Visual Function Testing Procedure
For each speed condition, three binocular visual tests were performed respectively using Freiburg Vision Test (FrACT®)25 in a dimly-lit room at 5-m distance and repeated twice in the following order: 1) VAS, 2) VAc and 3) CS. This was followed by one Bin-VF test using Ocusweep (Ocusweep®, Ocuspecto Ltd, Turku, Finland) in an ambient room light. Total experiments duration was about 75 min.
1) VAs: An 8-alternative-forced choice (AFC) single Landolt ring was presented to estimate VA and reported as a logarithmized minimal angle of resolution (logMAR).
2) VAc: The same applies to VAs but with using a single optotype surrounded by a circle (“©”).
3) CS: An 8-alternative-forced choice (AFC) optotype with varying contrasts was used to determine the weber contrast (logCS).
4) Bin-VF: A square stimulus comprised of 9 LEDs (5.2 mm × 5.2 mm) was presented at near distance (~40 cm) without proximity sensor to estimate the mean deviation of VF sensitivity (MD). Ocusweep® allowed for VF testing while TM walking since it requires no fixed head or chin rest. The device adjusts to ambient light levels using light sensors. The outcome measure was the binocular VF mean deviation (Bin-VF-MD).
All visual functions were performed using BCVA except for Bin-VF where near refractive correction is not mandatory as long as the VA < 0.1 logMAR.
Statistical Analysis
After testing for normal distribution (Shapiro–Wilk test) and for assumptions for repeated measures analysis of variance (RM-ANOVA), data were analyzed and presented accordingly. Data were reported as mean ± standard deviation (SD) for normally distributed data and as median and range for non-normally distributed data. The analyses of standard clinical test outcomes were performed employing a 3-way RM-ANOVA with the factors TIME (pre and post), INTERVENTION type (MMI and UMI), and GROUP (GLA and HC). In addition, data of the specific visual tests performed during the different TM walking conditions were analyzed using a 4-way RM-ANOVA with the factors: TIME, INTERVENTION, GROUP, as well as SPEED (S0, S3.5 and SSelf). If a violation of sphericity was detected, the Greenhouse-Geisser correction was applied. In case of significant interactions or main effects, post-hoc tests with Sidak-correction were performed. The effect size partial eta-squared (η2p) was calculated and interpreted as small (0.01–0.05), medium (0.06–0.13), and large effect (≥ 0.14) according to Cohen (1988).26 Effects were classified as significant if p ≤ 0.05 and relevant, if at least a medium effect size was observed. Data analysis was conducted in R27 and SPSS (Statistical Package for the Social Sciences; IBM, Armonk, NY, USA). For IOP and heart rate data across factors, linear mixed model was used, since data was missing for few participants.
Results
Participants (18 GLA and 30 HC) were randomly assigned to either MMI (GLA: n = 8, HC: n =12) or UMI group (GLA: n = 7; HC: n = 12). There was no age difference between groups (p = 0.276, Table 3). Three GLA and 6 HC had dropped out during the intervention period due to personal reasons. Baseline and demographic characteristics of the included participants are given in Table 3.
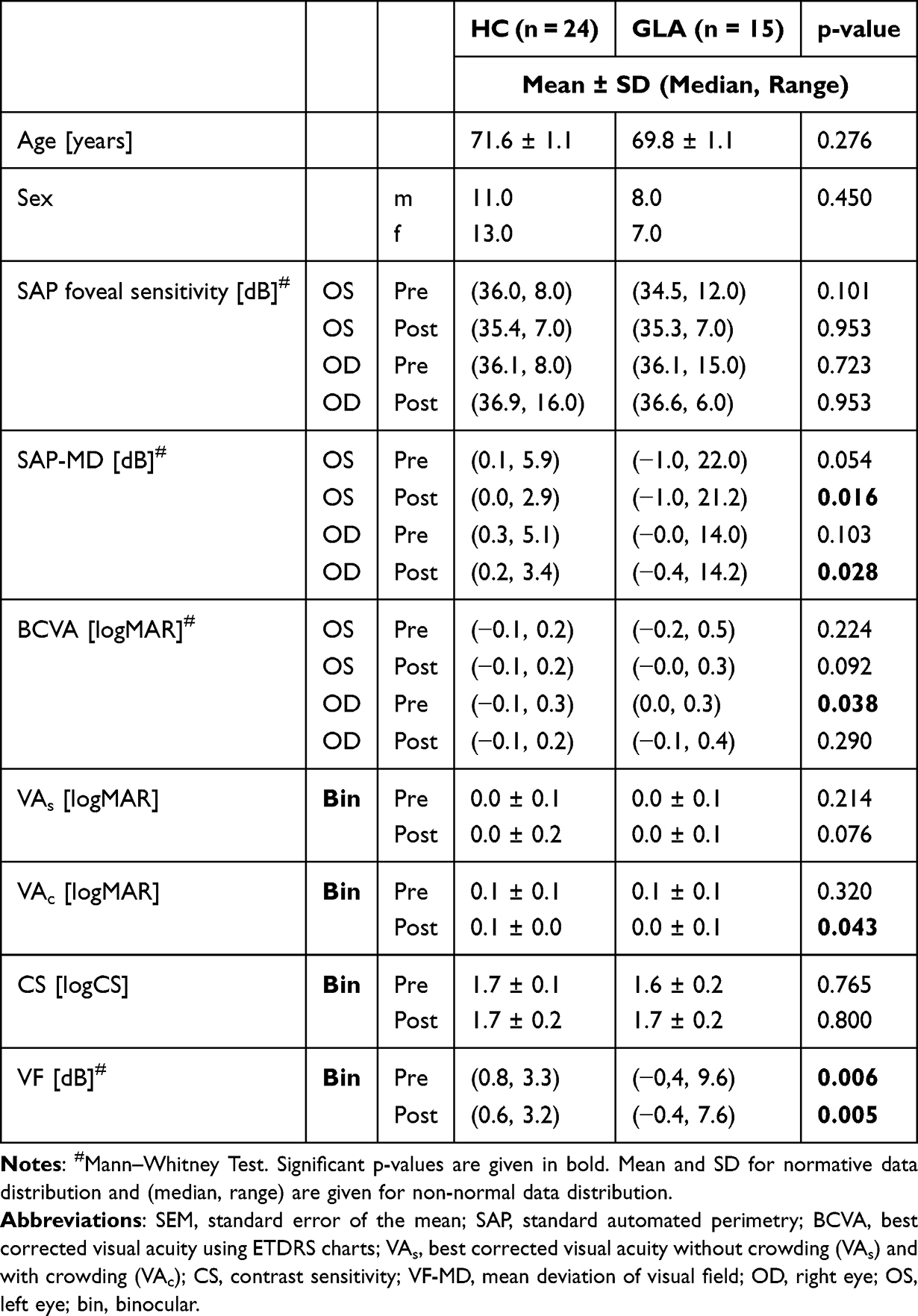 |
Table 3 Patients’ Demographic and Clinical Results Before and After the 12-Week Interventions |
We next detailed the effects of the 12-week intervention on A) standard clinical tests and B) the TM based visual functional tests.
Effect of the Interventions on Standard Clinical Tests
Main effects: We observed a significant TIME effect with regard to ETDRS BCVA (p = 0.024, η2p = 0.15), i.e., an improvement by 0.03 logMAR after the 12-week interventions. Interaction effects: There was a significant TIME × INTERVENTION interaction effect for the VF parameter “foveal sensitivity” (p = 0.039, η2p = 0.12). Post-hoc tests indicated an improvement of foveal mean sensitivities only for UMI, by 1.07 dB compared to the pre-intervention foveal sensitivities (35.2 dB), p = 0.024 (Table 4A). (Table 4A).
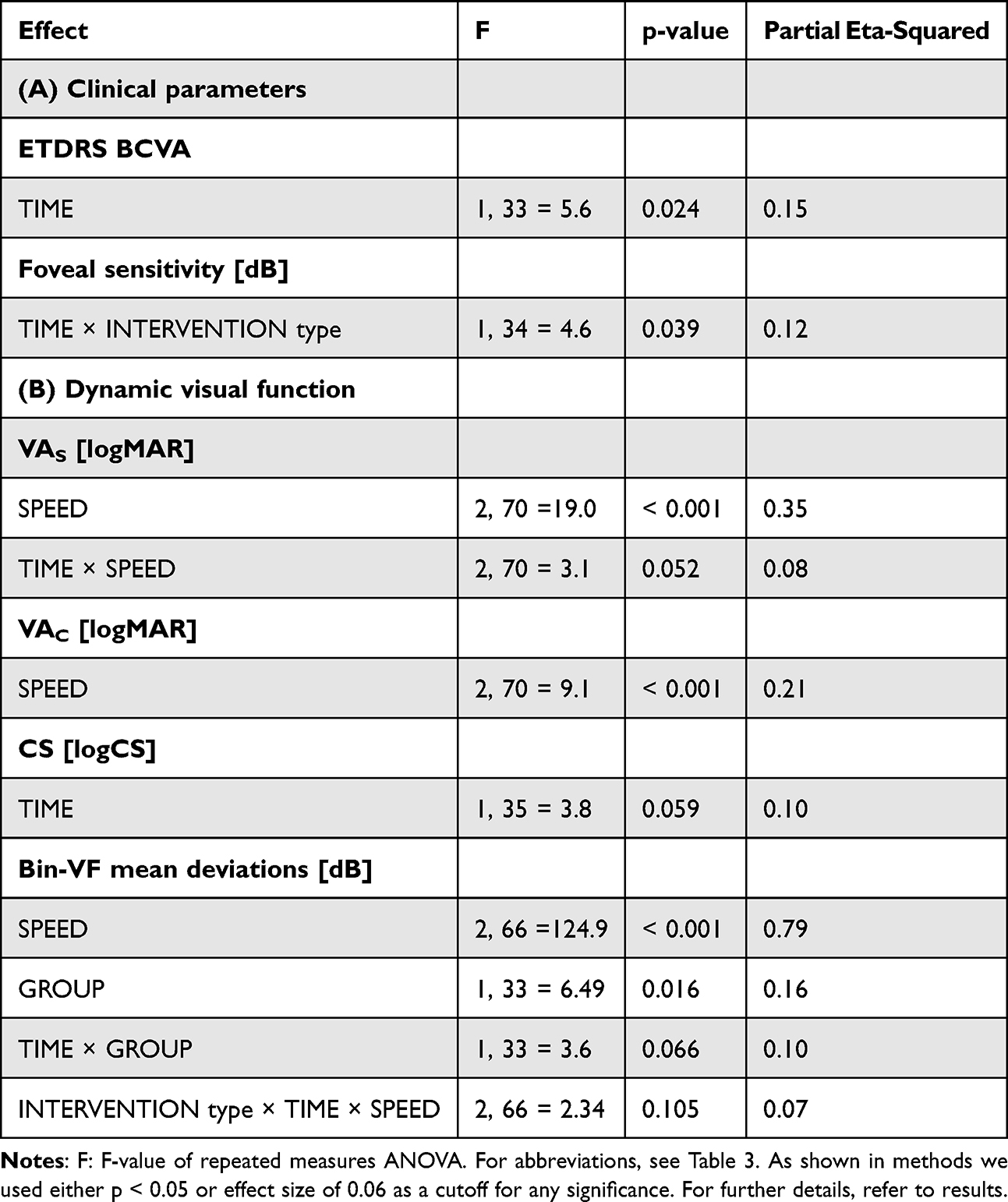 |
Table 4 Overview of Statistical Outcomes of the RM-ANOVAs of Only Significant Effects of SPEED, TIME, and INTERVENTION Type on Visual Function Parameters for the Study GROUPs |
For IOP measurements, there were neither significant main nor interaction effects of different factors. However, there was a trend of lower IOP measurements before training, 15.2 mmHg compared to post-training 16.2 mmHg, p > 0.054. For effects on heart rate, GLA had lower heart rates, 92.9 beats per minute (BPM), compared to HC, 95.2 BPM, p = 0.007.
Effects of the Interventions on TM Walking Visual Function
TM Walking SPEED Effects (S0 vs. S3.5 and SSelf)
Some of the results of the pre-intervention data set have previously been reported by Beyer et al.16 Of note, the present study analyzed data of a smaller sample due to dropouts during the intervention period (GLA: 3, HC: 6). Main effects (significant effects detailed in Table 4B): For VAs, the mean BCVA static (mean ± SD: −0.015 ± 0.11 logMAR) was better than dynamic readings (mean ΔS0-S3.5 [ΔS0-SSelf] ± SD: –0.03 ± 0.04, p = 0.001, see Figure 2A. Participants also had better VAC at S0 (0.031 ± 0.09 logMAR) than S3.5 [SSelf] (mean S0-S3.5 [S0-S3.5] difference ± SD: –0.02 ± 0.05, p = 0.100 [–0.043 ± 0.061, p < 0.001]). For CS there was no effect of speed (comparable CS across different speeds with an average of 1.65 ± 0.16 logCS, see Figure 2B). Bin-VF were reduced during dynamic compared to static viewing (S0: 0.12 ± 01.83 dB) by a mean deviation loss of –0.9 ± 0.44 dB during both S3.5 and SSelf, p < 0.001, see Figure 2C.
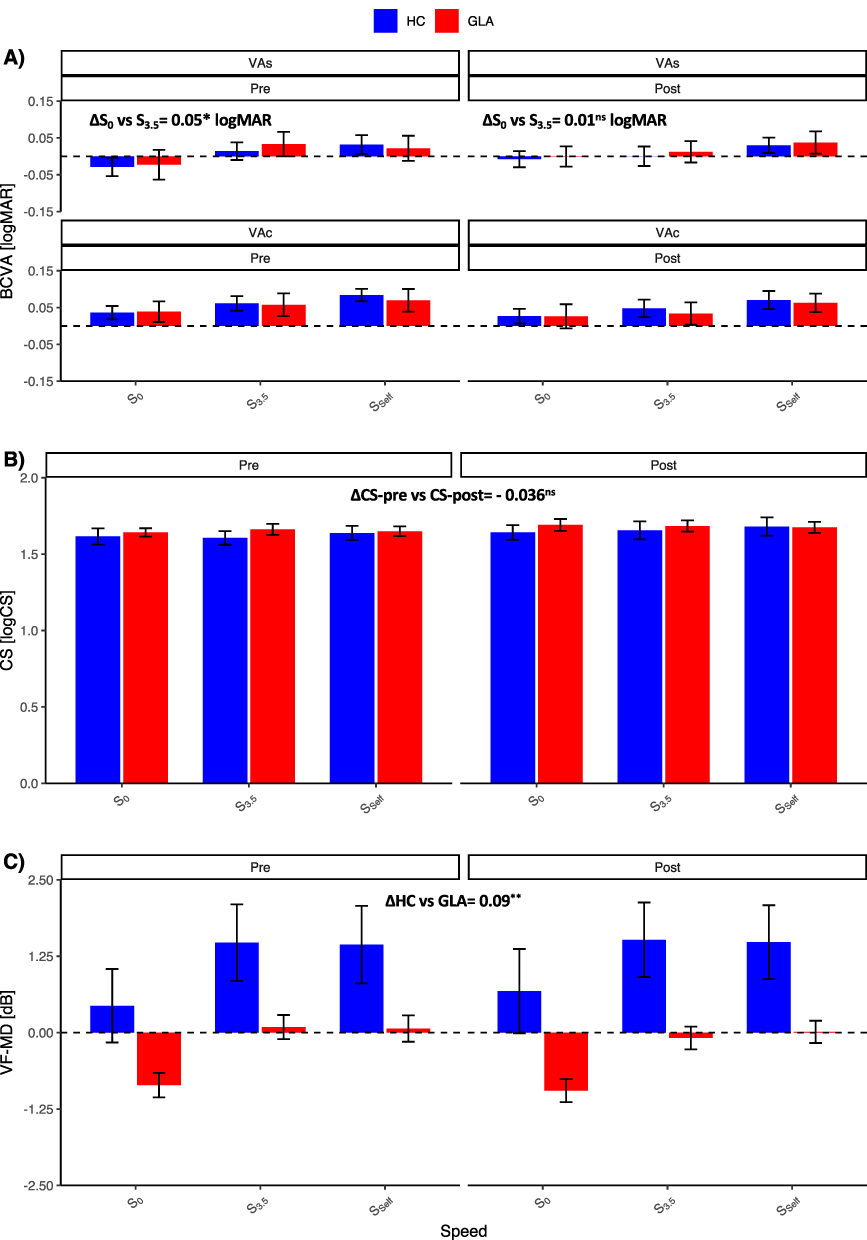 |
Figure 2 RM-ANOVA analysis of visual performance before (pre) and after (post) the 12-week interventions TIME for the two intervention modalities (multimodal, MMI & unimodal, UMI) at 3 treadmill (TM) walking speeds. (A) Best-corrected visual acuity with (VAS, upper panel) and without (VAC, lower panel) crowding: For VAS, TIME × SPEED interaction indicated that pre-interventional VA at a 3.5 km/h (S3.5) was 0.05 logMAR worse than static (S0) VA, p < 0.05. For VAC, there were no significant effects. (B) Contrast sensitivity (CS) effects: There is an effect of TIME based on partial eta squared cutoff in which participants had a 0.036 higher CS [logCS] than pre-intervention. No other main or interaction effects. (C) Binocular visual field mean deviations (VF-MD) in decibels (dB): There was only a group effect in which VF-MD was lower in glaucoma (GL) than HCs by 0.09 dB, p < 0.01. For statistics, see Table 4. Dotted line indicates zero-read-out. Intervention types’ effects are pooled due to lack of significant differences. Ns: non-significant test result; * p value < 0.05; ** p value < 0.001. |
Time Effects
Overall, visual function did not differ significantly after the 12-week intervention. Main effects: We observed a non-significant small trend of CS improvement after intervention (by 0.04 ± 0.1 logCS, p = 0.059, ηp2 = 0.10 Interaction effects: For VAs, there was a non-significant trend of TIME × SPEED interaction effect, p = 0.052, ηp2= 0.08.
Intervention Effects (MMI vs. UMI)
The intervention effects were not differentially affected by the two intervention types (MMI or UMI). Main interaction effects: There were no significant effects.
GROUP Effects (GLA vs. HC)
Only for Bin-VF, VF mean deviations were reduced for GLA, as expected from the pathology, –1.20 ± 2.4 dB than HC, 0.25 ± 0.91 dB, p = 0.016. Interaction effects: None detected.
Discussion
The present study investigated the effect of MMI and UMI on visual function: 1) tested with clinical parameters; and 2) during TM walking at different speeds. While trends were evident, the effect of the 12-week interventions on visual function were small and largely independent of group and intervention type.
Intervention Effects on Visual Performance
The observed intervention effects were marginal and reached significance only for the standard clinical measures of BCVA and foveal luminance sensitivity. Although improvements in dynamic CS and VA were not statistically significant, enhanced visual function is generally associated with a better health-related quality of life.28 Moreover, both BCVA and CS have been identified as strong predictors of a GLA patient’s ability to perform activities of daily living.29 The absence of strong effects is likely due to the early stage of GLA in most of the included patients. This demonstrates the robustness of visual outcomes at this stage and underscores the clinical relevance of monitoring progression for preventing future visual loss. We also demonstrated an improved foveal sensitivity of 1 dB following the intervention. However, since this change was not group specific, we regarded it as non-clinically significant. Accordingly, Lee et al, investigating more advanced GLA cases, reported a 10% improvement of glaucomatous VF following 1-week of moderate-vigorous physical exercise.30 Even in healthy athletes, exercise, namely ocular-motor, has beneficial effects on dynamic visual acuity.31
Beyond visual function, combined cognitive and physical training also positively influenced balance, cerebral health and cognition in older adults.31 It has been also shown that patients with cerebral vascular disease benefited from dual task rehabilitation training to improve balance and gait as well as prevent falls.17 In the context of neurodegenerative disorders, the relationship between motor function and cognitive abilities is also established. It has been shown that dual task training improved gait performance in Parkinson’s disease.33 Moreover, aerobic and resistance training have been shown to improve brain structure and function in patients with mild cognitive impairment.34 Thereby, the higher cognitive function seems independent of the intervention type,32 meaning that both physical and cognitive training have beneficial effects.
Several factors might explain the lack of relevant positive effects from our interventions on visual function readouts, including the early stage of disease progression in GLA patients and small sample size. Clinical endpoints to capture the consequences of motor-intervention on visual function in early-stage GLA might need to be re-considered. For example, BCVA might not be sensitive enough given that a 5-letter improvement compared to baseline is often considered the threshold for a minimal clinically important difference,35 which was not reached in our study (3 letters). Such small changes of visual function might also reflect insensitivity due to small sample size. While our initial sample size calculation to detect medium sized effects (f = 0.23) resulted in a sample size of 39 participants, our post-hoc power analysis based on the current results suggests a sample of n = 218 for the applied intervention schemes. Further, the intervention effects in early GLA might be better captured by non-visual outcomes related to visuo-cognitive-motor skills, including kinematic measures during physical locomotion, rather than basic visual function. Finally, the intervention type applied might need adjustment. The lack of superiority of MMI might be explained by the relatively low dose of resistance training in the Life Kinetik® program22 compared to higher exercise volume36 in UMI and/or insufficiently embedded intervention type to drive additive benefits in gait in GLA.22 Further, the effect of the Life Kinetik® program might not reflect on behavioral parameters, as determined in the present study, as its cognitive challenges might not translate into improvement of gait parameters, but rather act as secondary distractors. Other cognitively challenging interventions might be more effective in this respect. Hamacher et al37 for example, employed a 6-month dancing program, which showed greater beneficial effects than a combined exercise intervention in elderly. In contrast to the Life Kinetic program,22 Hamacher et al37 integrates cognitive challenges into the motor task rather than rendering them as secondary distractors. Consequently, gait improvement might benefit better from such an intervention program. This might also allow for the detection of such effects with a sample size considerable smaller than the one determined in the present study.
Limitations and Outlook
When interpreting the results of the present pilot study, several limitations must be considered. First, the sample size was small mainly due to the impact of the COVID-19 pandemic on recruitment and regular study/intervention participation, as reflected in the “pilot study” nature of our report. Second, most GLA patients were in the early stages of GLA, which may have resulted in the small magnitude of the observed effects of the interventions as one might have expected in the later stages. This is confirmed by our previous findings16 that healthy elderly and early GLA participants have comparable visual function loss during TM walking. Hence, to realistically capture intervention impacts, in future studies more advanced GLA stages should be included where functional deficits are larger and might benefit from our training programs. Further, pointwise analysis of VF metrics in more advanced GLA stages might elucidate more evident intervention or time related changes. Finally, follow-up of the training intervention at the retinal structural and vascular levels might promise valuable insights.
Conclusion
In summary, while the intervention approach of the present study established a foundation for a novel movement-related intervention regime for GLA, the effect of the 12-week interventions specifically on visual function were small. Based on the data of the present study, future trials should recruit a larger sample size and participants with more severe GLA stages in order to identify the effects MMI und UMI on visual function to prevent GLA-induced loss of quality of life.
Data Sharing Statement
Data is available upon request to the corresponding author.
Ethical Approval
The study was approved by the Ethics Committee of the Otto-von-Guericke University of Magdeburg in Germany (registration number: 32/18) and all procedures were in line with the Declaration of Helsinki on experiments on human beings. A consent form was obtained from all participants.
Acknowledgment
We thank the study participants for their support of the study. We acknowledge support by the Open Access Publication fund of the medical faculty of the Otto-von-Guericke-University Magdeburg. This paper has been uploaded to medRxiv as a preprint: https://www.medrxiv.org/content/10.1101/2025.01.30.25321400v1
Funding
This study is funded by the German Research Foundation (DFG; Project: 423926179; HO-2002/20-1 &SCHE 1584/5-1). There was no role of the funders in planning, conducting or reporting the current study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–13. doi:10.1016/j.ophtha.2014.05.013
2. Freitag CW, Behrens M, Menrad T, et al. Single- and dual-task gait performance in patients with open-angle glaucoma: a cross-sectional study. Transl Vis Sci Technol. 2023;12(11):31. doi:10.1167/tvst.12.11.31
3. Fea AM, Hengerer F, Lavia C, Au L. Glaucoma Quality of Life. J Ophthalmol. 2017;2017:4257151. doi:10.1155/2017/4257151
4. Moreno-Montañés J, Antón-López A, Duch-Tuesta S, et al. Lifestyles guide and glaucoma (i). Sports and activities. Arch Soc Esp Oftalmol. 2018;93(2):69–75. doi:10.1016/j.oftal.2017.09.005
5. Feldman RM, Cioffi GA, Liebmann JM, Weinreb RN. Current knowledge and attitudes concerning cost-effectiveness in glaucoma pharmacotherapy: a glaucoma specialists focus group study. Clin Ophthalmol Auckl NZ. 2020;14:729–739. doi:10.2147/OPTH.S236030
6. Allison K, Patel D, Alabi O. Epidemiology of glaucoma: the past, present, and predictions for the future. Cureus. 2020;12(11):e11686. doi:10.7759/cureus.11686
7. Tanabe S, Yuki K, Ozeki N, Shiba D, Tsubota K. The association between primary open-angle glaucoma and fall: an observational study. Clin Ophthalmol Auckl NZ. 2012;6:327. doi:10.2147/OPTH.S28281
8. Arrigo A, Aragona E, Saladino A, et al. Cognitive dysfunctions in glaucoma: an overview of morpho-functional mechanisms and the impact on higher-order visual function. Front Aging Neurosci. 2021;13:747050. doi:10.3389/fnagi.2021.747050
9. Fragala MS, Cadore EL, Dorgo S, et al. Resistance training for older adults: position statement from the national strength and conditioning association. J Strength Cond Res. 2019;33(8):2019–2052. doi:10.1519/JSC.0000000000003230
10. Persch LN, Ugrinowitsch C, Pereira G, Rodacki ALF. Strength training improves fall-related gait kinematics in the elderly: a randomized controlled trial. Clin Biomech Bristol Avon. 2009;24(10):819–825. doi:10.1016/j.clinbiomech.2009.07.012
11. Fiatarone Singh MA, Gates N, Saigal N, et al. The Study of Mental and Resistance Training (SMART) study—resistance training and/or cognitive training in mild cognitive impairment: a randomized, double-blind, double-sham controlled trial. J Am Med Dir Assoc. 2014;15(12):873–880. doi:10.1016/j.jamda.2014.09.010
12. Herold F, Hamacher D, Schega L, Müller NG. Thinking while moving or moving while thinking – concepts of motor-cognitive training for cognitive performance enhancement. Front Aging Neurosci. 2018;10:228. doi:10.3389/fnagi.2018.00228
13. de M CFG, Andrade LP, Pedroso RV, et al. Multimodal exercise intervention improves frontal cognitive functions and gait in Alzheimer’s disease: a controlled trial. Geriatr Gerontol Int. 2013;13(1):198–203. doi:10.1111/j.1447-0594.2012.00887.x
14. Puente-González AS, Sánchez-Sánchez MC, Fernández-Rodríguez EJ, Hernández-Xumet JE, Barbero-Iglesias FJ, Méndez-Sánchez R. Effects of 6-month multimodal physical exercise program on bone mineral density, fall risk, balance, and gait in patients with alzheimer’s disease: a controlled clinical trial. Brain Sci. 2021;11(1):1. doi:10.3390/brainsci11010063
15. de Oliveira Silva F, Ferreira JV, Plácido J, et al. Three months of multimodal training contributes to mobility and executive function in elderly individuals with mild cognitive impairment, but not in those with Alzheimer’s disease: a randomized controlled trial. Maturitas. 2019;126:28–33. doi:10.1016/j.maturitas.2019.04.217
16. Beyer R, Al-Nosairy KO, Freitag C, et al. Treadmill-walking impairs visual function in early glaucoma and elderly controls. Graefes Arch Clin Exp Ophthalmol. 2024. doi:10.1007/s00417-024-06530-w
17. Ercan Yildiz S, Fidan O, Gulsen C, Colak E, Genc GA. Effect of dual-task training on balance in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2024;121:105368. doi:10.1016/j.archger.2024.105368
18. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239. doi:10.1136/bmj.i5239
19. Freitag CW, Behrens M, Bielitzki R, et al. Gaze behavior in open-angle glaucoma patients during visuo-cognitive-motor tasks: a cross-sectional study. Sci Rep. 2024;14(1):20978. doi:10.1038/s41598-024-70987-2
20. BMJ Publishing Group Ltd. BMA House TS. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021;105(Suppl 1):1–169. 10.1136/bjophthalmol-2021-egsguidelines.
21. Hodapp E, Parrish RK, Anderson DR. Clinical Decisions in Glaucoma. Mosby; 1993.
22. Lutz H. Life Kinetik® - Gehirntraining durch Bewegung.
23. Al-Nosairy KO, van den BJJON, Pennisi V, et al. Use of a novel telemetric sensor to study interactions of intraocular pressure and ganglion-cell function in glaucoma. Br J Ophthalmol. 2021. doi:10.1136/bjophthalmol-2020-316136
24. Lara PM, Redondo B, Jerez-Mayorga D, Martínez-García D, García-Ramos A, Vera J. Influence of the body positions adopted for resistance training on intraocular pressure: a comparison between the supine and seated positions. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):1971. doi:10.1007/s00417-023-06009-0
25. Bach M. The Freiburg Visual Acuity test--automatic measurement of visual acuity. Optom Vis Sci off Publ Am Acad Optom. 1996;73(1):49–53. doi:10.1097/00006324-199601000-00008
26. Cohen J. Statistical Power Analysis for the Behavioral Sciences. L Erlbaum Associates. 1988.
27. R Core Team. R: The R Project for Statistical Computing. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2023. Available from: https://www.r-project.org/.
28. Mangione CM, Phillips RS, Lawrence MG, Seddon JM, Orav EJ, Goldman L. Improved visual function and attenuation of declines in health-related quality of life after cataract extraction. Arch Ophthalmol. 1994;112(11):1419–1425. doi:10.1001/archopht.1994.01090230033017
29. Richman J, Lorenzana LL, Lankaranian D, et al. Importance of visual acuity and contrast sensitivity in patients with glaucoma. Arch Ophthalmol Chic IL 1960. 2010;128(12):1576–1582. doi:10.1001/archophthalmol.2010.275
30. Lee MJ, Wang J, Friedman DS, Boland MV, De Moraes CG, Ramulu PY. Greater physical activity is associated with slower visual field loss in glaucoma. Ophthalmology. 2019;126(7):958–964. doi:10.1016/j.ophtha.2018.10.012
31. Minoonejad H, Barati AH, Naderifar H, Heidari B, Kazemi AS, Lashay A. Effect of four weeks of ocular-motor exercises on dynamic visual acuity and stability limit of female basketball players. Gait Posture. 2019;73:286–290. doi:10.1016/j.gaitpost.2019.06.022
32. Intzandt B, Vrinceanu T, Huck J, et al. Comparing the effect of cognitive vs. exercise training on brain MRI outcomes in healthy older adults: a systematic review. Neurosci Biobehav Rev. 2021;128:511–533. doi:10.1016/j.neubiorev.2021.07.003
33. Li Z, Wang T, Liu H, Jiang Y, Wang Z, Zhuang J. Dual-task training on gait, motor symptoms, and balance in patients with Parkinson’s disease: a systematic review and meta-analysis. Clin Rehab. 2020;34(11):1355–1367
34. Huang X, Zhao X, Cai Y, Wan Q. The cerebral changes induced by exercise interventions in people with mild cognitive impairment and Alzheimer’s disease: a systematic review. Arch Gerontol Geriatr. 2022;98:104547. doi:10.1016/j.archger.2021.104547
35. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4):407–415. doi:10.1016/0197-2456(89)90005-6
36. Herold F, Törpel A, Schega L, Müller NG. Functional and/or structural brain changes in response to resistance exercises and resistance training lead to cognitive improvements - a systematic review. Eur Rev Aging Phys Act off J Eur Group Res Elder Phys Act. 2019;16:10. doi:10.1186/s11556-019-0217-2
37. Hamacher D, Hamacher D, Rehfeld K, Hökelmann A, Schega L. The effect of a six-month dancing program on motor-cognitive dual-task performance in older adults. J Aging Phys Act. 2015;23(4):647–652
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.