Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Effects Of Modified Mindfulness-Based Stress Reduction (MBSR) On The Psychological Health Of Adolescents With Subthreshold Depression: A Randomized Controlled Trial
Authors Zhang JY, Ji XZ, Meng LN, Cai YJ
Received 20 May 2019
Accepted for publication 4 September 2019
Published 17 September 2019 Volume 2019:15 Pages 2695—2704
DOI https://doi.org/10.2147/NDT.S216401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Jia-Yuan Zhang,1,* Xiang-Zi Ji,2,* Li-Na Meng,1 Yun-Jiang Cai1
1Department of Psychological Nursing Science, Harbin Medical University, Daqing, Heilongjiang Province, People’s Republic of China; 2Department of Nursing Science, Suzhou Vocational Health College, Suzhou, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li-Na Meng; Yun-Jiang Cai
Department of Psychological Nursing Science, Harbin Medical University, No. 39 XinYang Street, Daqing, Heilongjiang Province 163319, People’s Republic of China
Email [email protected]; [email protected]
Background: Sub-threshold depression (SD) has been associated with impairments in adolescent health which increase the rate of major depression. Researchers have shown the effectiveness of mindfulness on mental health, however whether the traditional mindful skills were suitable for youngsters, it was not clear. This study investigated the effects of a tailed Mindfulness-based stress reduction (MBSR) on their psychological state.
Methods: A double-blind, randomized controlled trial was carried out. 56 participants who met the inclusion criteria agreed to be arranged randomly to either the MBSR group (n=28) or the control group (n=28). Participants in MBSR group received a tailored 8-week, one time per week, one hour each time group intervention. The effectiveness of intervention was measured using validated scales, which including BDI-II, MAAS, RRS at three times (T1-before intervention; T2-after intervention; T3-three months after intervention). A repeated-measures analysis of variance model was used to analyze the data.
Results: The results showed significant improvements in MBSR group comparing with control group that depression level decreased after the 8-week intervention and the follow up (F =17.721, p < 0.00). At the same time, RRS score was significantly decreased at T2 and T3(F= 28.277, p < 0.00). The results also showed that MBSR promoted the level of mindfulness and the effect persisted for three months after intervention (F=13.489, p < 0.00).
Conclusion: A tailored MBSR intervention has positive effects on psychology health among SD youngsters, including decrease depression and rumination level, cultivate mindfulness.
Keywords: mindfulness, adolescent, subthreshold depression
Introduction
Subthreshold depression (SD), also known as subsyndromal depression, subclinical depression, or mild depression, refers to a state or a subpopulation of individuals who have certain depressive symptoms but do not meet the diagnostic criteria for major depressive disorder.1 A previous study found that the incidence of subthreshold depression was significantly higher than that of major depressive disorders, with an estimated prevalence rate of 25% worldwide, and it had a serious impact on individual life and social psychological function.2 However, there is little agreement on how to address the diagnosis of subthreshold depression; modern classification systems such as the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) have established diagnostic categories for subsyndromal depressive symptoms, including “dysthymia,” “brief recurrent depression,” and “minor depressive disorder”.3 Subthreshold depression is considered to be the precurative stage of major depressive disorder and can predict the occurrence of major depressive disorder in individuals in the future. It should be made clear that it is increasingly recognized that individuals with subthreshold depression do not have a similar prognosis to those who are asymptomatic, and are in fact at elevated risks of later depression and suicidal behaviors.4 Individuals with subthreshold depression have an odds ratio of more than 5 for having a first lifetime episode of major depression disorder.5 Meanwhile, subthreshold depression has also increased the risk of adverse outcomes such as drug abuse and dependence. In recent years, the incidence of subthreshold depression in adolescents has grown rapidly and as high as 36.56%.2 There are adolescents with subthreshold depression who have not yet met the diagnostic criteria for depression, but subthreshold depression has caused a decline in their social function and has placed them at a higher risk of experiencing depressive episodes, which should be highly concerning.6 However, there are limited studies focus on investigating an effective and feasible way to help adolescents with subthreshold depression improve their psychological health.
Mindfulness, derived from Buddhist meditation, is described as a state of being purposeful and giving nonjudgemental attention to the present moment. Its core elements are “the ability to focus on the present” and “keep a curious, open and receptive attitude”.7 Mindfulness intervention is a psychological treatment, which refers to a series of psychological training methods based on “mindfulness,” that can help individuals cultivate and enhance mindfulness. In the late 1970s, American psychologist Kabat-Zinn introduced and developed mindfulness-based stress reduction (MBSR) psychotherapy, which was praised as “the third wave of behavioral and cognitive therapy”.8 MBSR is a systematic non-drug psychological therapy that includes four basic mindfulness skills. Through mindfulness meditations, body awareness and yoga, MBSR can awaken inner mindfulness and improve self-regulation to help people relieve stress. At present, MBSR has been widely used in medical treatment and has become an important part of the biopsychosocial approach medical system to promote psychology and physical health.9 Studies have shown that MBSR can alleviate anxiety and depression among cancer patients.10,11 A recent meta-analysis showed that yoga-based interventions, including mindfulness practice, had significant beneficial effects for pregnant women with mild depressive symptoms.12 However, due to differences in cultural and religious beliefs and economic levels, whether MBSR is suitable for the Chinese adolescent population needs further investigation.
Mindfulness therapy includes formal and informal techniques. The traditional form of mindfulness-based stress reduction therapy is group intervention. Each group is limited to approximately 30 people with 8 practice times of 2 to 2.5 hrs each.13 However, due to time constraints or hard-to-grasp core skills, many people suspend or quit psychological treatment. For adolescents, due to their immature psychological adjustment mechanism, it is difficult for them to grasp the core of mindfulness skills related to meditation in a short amount of time.14 The best way to perform psychological intervention is to allow adolescents to apply the techniques to their life and integrate them into their life over time, thus improving their psychological health. Fewer studies have focused on the longitudinal effects of mindfulness skills on adolescents in China.15 Therefore, a tailored MBSR programme for adolescents with rigorous and well-controlled randomized trials is needed to further test the long-term effects of modified MBSR on the psychological health of adolescents.
This study was designed to evaluate the effects of a tailored simplified MBSR on the psychological health of adolescents with subthreshold depression, including depression levels, rumination and mindfulness levels, in a randomized controlled trial. We hypothesized that modified MBSR training would provide evidence for improving psychological health, thus decreasing depression and rumination levels and increasing mindfulness in Chinese adolescents with subthreshold depression.
Methods
Study Design
This study was a randomized controlled design with double-blind subjects. All participants were divided equally into the MBSR training group and the control group using the random number table by staff members who were independent from the study. All participants received the anonymous letters and they were blinded to their random assignment until the end of the session. When the study was completed, the control group received the same intervention according to their own wishes. The intervention was conducted at the psychological interview room carried out by a qualified psychologist. The anonymous data were collected and analyzed by an assistant who was blinded to the group assignment and all the trials. The design of the entire study is illustrated in a flow diagram in Figure 1.
 |
Figure 1 Study flow diagram: enrollment to analysis. |
Sample And Setting
The sample-size estimation in this study was calculated by using the G*POWER version 3.1 program with a power (1−β) of 0.80 in the paired-samples t-test and a significance level of 0.05. Based on the related data,16 we established an effect size (d) of 0.796; consequently, the total sample size was 52 participants. Allowing for a 5–10% dropout rate, we recruited 56 students in September 2017. Participants were enrolled by putting up a poster on campus. We used two steps to recruit the participants. First, all of the interested students completed questionnaires (Beck depression inventory, BDI and self-rating depression scale, SDS). Participants who had a BDI>14 and an SDS>53 were defined as the preliminary screening group. Second, the structured clinical interview for DSM (SCID) was conducted among the preliminary screening group by a psychologist to perform the second screening. The exclusion criteria were as follows: i) had recently suffered from major stress events; and/or ii) had major depressive disorder, bipolar disorder or other types of mental illnesses. A total of 291 students agreed to participate in the study, and in the end, the study included 56 participants who met the following inclusion criteria: i) volunteered for this study and agreed to obey the rules during the intervention and ii) had subthreshold symptoms of depression (as defined by the questionnaires and structured interviews). Participants who had participated in or were participating in similar interventions (such as yoga or meditation) were also excluded. All participants provided their written consent. The study was approved by the institutional review board at Harbin Medical University (Daqing) and this trial was conducted in accordance with the Declaration of Helsinki.
Intervention
The MBSR Intervention Group
Participants allocated to the MBSR training groups received 8 weeks of modified MBSR training. Based on traditional MBSR theory, the intervention was tailored according to the characteristics of adolescents and emphasized teaching them to apply formal techniques such as body scanning, sitting meditation, and mindfulness yoga to all aspects of the practitioner’s life, including experiencing the pleasant/sad moments in life, walking, sleeping, eating, breathing and exercising to keep the attitude of “mindfulness”. The intervention plan was designed and administered by a qualified psychological expert who has been involved in MBSR treatment for 5 years. Participants in the MBSR group were divided into 4 groups with 7 people per group. Each group received training sessions for 8 weeks, and the sessions occurred once a week for one hour at a time. Each session included 10 mins of free talk (feeling about homework), 15 mins of demonstration and explanation, 20 mins of practice and guidance, and 15 mins of group imitation training. Each session was followed by homework, which was available for the trainer to understand the practice situation of each person. Combined with daily activity, the themes of the intervention were derived from “eye”, “ear”, “nose”, “tongue”, “body” and “thinking”. More details of each session are listed in Table 1.
 |
Table 1 The MBSR Intervention Group Session Details |
The Control Group
Students in the control group continued with their lives as usual. No specific intervention was implemented in the control group. To avoid possible overlap (contamination) with components of the MBSR programme, the students in the control group who planned to attend related associations such as yoga clubs during the intervention period (8 weeks) were excluded. After completion of the study, each student in the control group was provided with the same MBSR course according to their own wishes.
Measures
Beck Depression Inventory-II (BDI-II)
The primary outcome was the severity of depressive symptoms assessed with the BDI-II. The scale was a well-validated and widely used measure of depression that assesses the frequency of depressive symptoms over the previous 2 weeks. It consists of 21 items that are rated on a 4-point scale, with scores ranging from 0 to 63, and cut-off points of 0–13, 14–19, 20–28 and 29–63, which represent no, mild, moderate and severe levels of depression, respectively. The scale has been used in the Chinese adolescent population, revealing good reliability and validity.17
Mindful Attention And Awareness Scale (MAAS)
Participants’ self-reported mindfulness level was measured with the MAAS.18 The scale contains 15 items that assess the most important characteristics of mindfulness. Items are rated on a 6-point scale and scored as (1) almost always to (6) almost never, with higher scores reflecting a greater mindfulness state. The scale has been tested among Chinese college students, revealing good internal consistency reliability (α=0.85) and test-retest reliability (r=0.54).19
Ruminative Response Scale (RRS)
The RRS was compiled by Nolen-Hoeksema and assesses the response to depression. It consists of 22 items rated on a 4-point scale that are scored as (1) never to (4) very often, with scores that ranged from 22 to 88. Higher scores represent a greater level of rumination. It has 3 factors: symptom rumination, forced thinking and introspection. The Chinese version of the Perceived Stress Scale (CPSS) was translated by Han20 and has been tested among Chinese college students, revealing good internal consistency reliability (α = 0.90) and test-retest reliability (r=0.68–0.85).
Procedure
After approval from the institutional review board and ethics committee, we put up a poster on campus for recruitment. The modified 8-week MBSR intervention was carried out by a qualified psychologist. The questionnaires were delivered and collected by two staff members who were independent of our study. All students completed questionnaires at three points. The first point was the initial baseline orientation when the MBSR intervention started, the second point was the end of the 8-week intervention, and the last point was 3 months after the intervention.
Statistical Methods
All data analyses were performed using IBM SPSS 21.0 (version 21.0, IBM Corp., New York, NY, United States) with bilateral inspection by two dependence assistants. The continuous variables were assessed by means with standard deviations or medians with ranges. Baseline data were compared using a t-test or chi-square test between the two groups. A repeated-measures analysis of variance model was used to directly test the outcomes (depression, mindfulness and rumination) between the two groups. Statistical significance was set at p<0.05. A p value of less than or equal to 0.05 was considered statistically significant.
Results
Sociodemographic And Clinical Characteristics Of Participants
The average age of the participants was 18.94 ± 1.31 years, with a range of 17–22 years. Table 2 displays the characteristics of the two groups.
 |
Table 2 Comparison Of Demographic And Clinical Characteristics Of Two Groups (n=56) |
Efficacy Of MBSR On BDI, MAAS, RRS
A repeated-measures analysis of variance model was conducted to examine changes across time between the intervention and comparison conditions on measures of BDI, MAAS, RRS. Table 3 reveals descriptive statistics with mean scores of pre-post measures and significance of the group, time and time-group interactions. The results revealed a significant interaction between time and condition for BDI (F=17.721, p<0.001, η2=0.577), MAAS (F=13.489, p<0.001, η2=0.509), and RRS (F=81.566, p<0.001, η2=0.863).
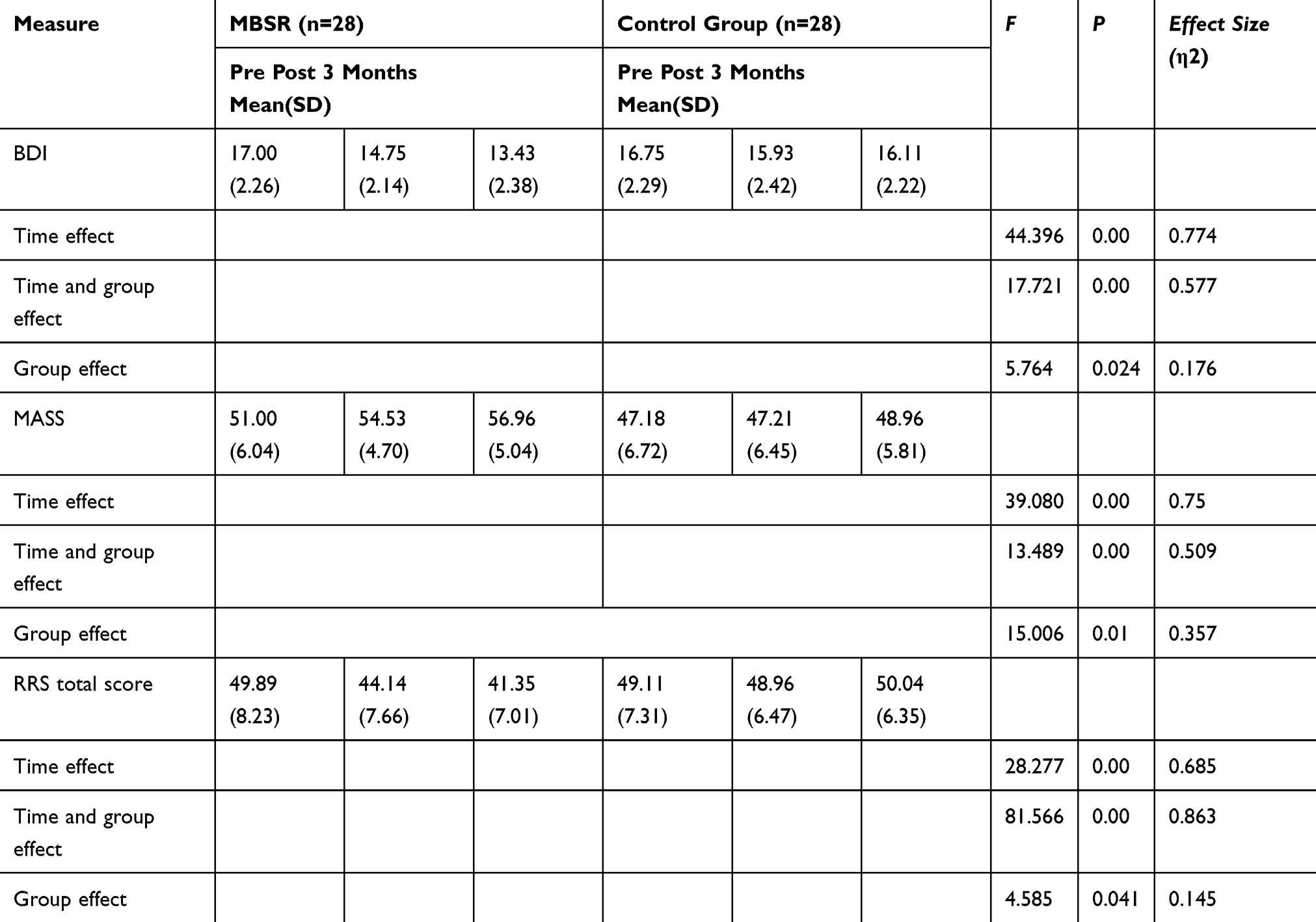 |
Table 3 Comparison Of Two Groups On BDI, MASS And RRS |
Discussion
This study is the first RCT pilot study to apply tailored mindfulness-based stress reduction to mental health on subthreshold depression college students to evaluate the effects of MBSR on their psychological health. Specifically, the benefits of modified MBSR on participants have been tested, such as a decrease in depression and rumination level and an increase in mindfulness state. Although researchers have been studying subthreshold depression for decades, subthreshold depression is still not recognized enough due to the lack of clear and unified diagnostic criteria, and no authoritative academic institutions have issued clear epidemiological reports.21 There has been little research on SD in related academic fields in China.15 Influenced by Chinese cultural values, most people are reluctant to seek psychological counselling or clinical psychotherapy, even if they have clinical symptoms that lead to an increase in the prevalence of major depression in recent years.22 Studies have shown that the incidence of subthreshold depression among adolescents has reached 30~40%.23 Although subthreshold depression does not meet the diagnosis of a clinical depressive episode, it affects the physical and mental health of individuals; thus, it is very necessary for early intervention.24
Mindfulness skills have been systematically used in psychotherapy, and related guidelines have been recommended by NICE for the treatment of depression in the UK.25 However, for Chinese adolescents, the related systematic and professional psychological counselling was difficult for them to grasp in a short period of time. In this study, we designed an eight-week simplified MBSR programme according to adolescent characteristics to examine its effects on college students with subthreshold depression. After intervention, the results revealed that the level of mindfulness in the MBSR group increased with a mean of (51.00±6.04) points, and the levels of depression increased with a mean of (54.55±4.70) points. The effect sizes were significant and lasted for three months. Compared with traditional MBSR trials, the tailored MBSR combined mindfulness skills with daily life, and we summarized the main problems and provided related solutions during intervention, which were more easily accepted by students and more easily accepted for mindfulness cultivation. Previous studies have reported that when people engage in 2 hr or 2.5 hr mindfulness training, it is difficult for them to be clear and focused, and they always experience problems such as feeling sleepy, tired or disturbed.26 Thus, in our study, we decreased the training time and modified the form to establish a tailored MBSR intervention to ensure feasibility. Through listening, observing, eating and smelling mindfully, participants could deal with emotions peacefully and keep a friendly attitude towards themselves, respecting their own abilities without judgement or competition. We aim to let participants grasp basic mindfulness skills through practice and gradually cultivate mindfulness into their lives. The efficacy of MBSR on depression level may be related to mindfulness training. Studies have revealed that mindfulness helps people avoid the reaction of psychological distress, which fundamentally improves their perceptions of negative events and states.27 The core of mindfulness is to focus on the moment without any judgements. Mindfulness training helps individuals to consciously select and recognize thoughts, emotions and feelings but does not produce habitual reactions, which can enhance their ability to regulate emotions, thus gradually eliminating the process of automatic evaluation of negative emotions, which decrease the depression level.28 Increased responsiveness and activity of the hypothalamic-pituitary-adrenal (HPA) axis and sympathetic-adrenal-medullary (SAM) system have been associated with higher levels of stress, depression and anxiety; studies hypothesize that mindfulness techniques dampen the hyperactivity of these systems, which in turns reduces the stress levels.29
This study strengthens the finding of previous studies that mindfulness is an important mechanism for inhibiting rumination and preventing symptoms of depression.30 Rumination is a repeated focus on our own way of thinking of negative emotions and events that impair psychological health.31 The results revealed that adolescents with subthreshold depression had a high level of rumination. After 8 weeks of MBSR intervention, the rumination level decreased significantly, and this effect lasted for 3 months. Mindfulness is the conscious effort of an individual to maintain attention in the present moment and makes no judgement about it.32 Participants in the intervention group were provided with effective mindfulness skills to reduce habitual thinking and over-thinking. Through mindfulness training, our brain’s daily thinking mode changes from “action mode” to “existence mode”. Action mode is the inevitable product of the brain’s automatic thinking. When automatic thinking becomes a habit, our consciousness will be preoccupied not with the present but with memories of the past, problems of the present, and anxieties of the future. The existence mode is a new solution to automatic thinking. It suggests that instead of being trapped in automatic thinking, subjects should focus their consciousness on the present experience and reduce the focus on oneself, which is helpful to relax the body and mind.33 Previous studies have shown that mindfulness training reduced rumination in individuals. Teasdale et al believed that mindfulness training could relieve cognitive interlock when rumination takes place.34 That is, when dealing with stress, individuals will automatically have a non-adaptive response and pay more attention to the present moment through mindfulness training, thereby promoting the transfer of attention from rumination.
Strengths & Limitations
In our research, we combined mindfulness skills with daily life based on the characteristics of adolescents, implemented them in short-term form, considered the feasibility and scientific nature, and preliminarily applied the tailored MBSR to adolescents with subthreshold depression in China. The results showed that the intervention had a positive effect on their psychological health, including alleviating symptoms of depression, decreasing rumination and cultivating mindfulness. The intervention was convenient and had a relatively long effectiveness that lasted for 3 months. Although we use double-blind in the RCT, due to the limitation of source and conditions, our study was limited by a modest sample size. Future studies should add to the sample size to confirm the effects. For future work, the intervention should be combined with other adjunctive or complementary and alternative therapies e.g. probiotic supplementation, which has been shown to alleviate depressive symptoms.35 Moreover, due to limited time, the follow-up period of this study was 3 months. In our future study, we will extend the observation time to test the long-term sustainability of the positive effects.
Conclusions
The results from this randomized controlled trial showed that modified MBSR was effective in cultivating mindfulness and reducing depressive symptom levels and rumination in adolescents with subthreshold depression. This approach is a simple and feasible intervention that promotes the psychological health of adolescent populations suffering from subthreshold depression.
Ethical Approval And Consent To Participate
The University of Institutional review board approved this study (No.2017-10) and informed consent was obtained from every participant.
Consent For Publication
Informed consent for the publication of these have been obtained from all participants. All the students have signed for agreement. The parent or legal guardian provided written informed consent for any participant under the age of 18 years.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
The authors were grateful for all the participants in this study for their cooperation and all the clinical staff for providing the intervention place and the assistance with data collection. This work was supported by the grant of Science Foundation of Ministry of Education of China [No.17YJCZH241] and the Fundamental Research Funds for the Provincial Universities [No.2018wld-02]. Jia-Yuan Zhang and Xiang-Zi Ji are co-first authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Balazs J, Miklosi M, Kereszteny A, et al. Adolescent subthrehold-depression and anxiety: psychopathology, functional impairment and increase suicide risk. J Child Psychol Psychiatry. 2013;6:670–677. doi:10.1111/jcpp.12016
2. Tan X, Zhang J, Yang QL. TCM psychological intervention for subthreshold depression and its mechanism. Chin Gen Pract. 2013;6:2649–2651.
3. Keller MB, Klein DN, Hirschfeld RM, et al. Results of the DSM-IV mood disorders field trial. Am J Psychiatry. 1995;152(6):843–849. doi:10.1176/ajp.152.6.843
4. Fergusson DM, Horwood LJ, Ridder EM, et al. Subthreshold depression in adolescence and mental health outcomes in adulthood. Arch Gen Psychiatry. 2005;62(1):66 –72. doi:10.1001/archpsyc.62.1.66
5. Fogel J, Eaton WW, Ford DE. Minor depression as a predictor of the first onset of major depressive disorder over a 15-year follow-up. Acta Psychiatr Scand. 2006;113:36e43. doi:10.1111/j.1600-0447.2005.00654.x
6. Guberman C, Manassis K. Symptomatology and family functioning in children and adolescents with comorbid anxiety and depression. J Can Acad Child Adolesc Psychiatry. 2011;20:186–195.
7. Eisendrath SJ, Gillung E, Delucchi KL, et al. A randomized controlled trial of mindfulness-based cognitive therapy for treatment-resistant depression. Psychother Psychosom. 2016;85:99–110. doi:10.1159/000442260
8. Kabat-Zinn J. Bringing mindfulness to medicine: an interview with Jon kabat-zinn, PhD. Interview by Karolyn gazelle. Adv Mind Body Med. 2005;21:22–27.
9. MacCoon DG, Imel ZE, Rosenkranz MA, et al. The validation of an active control intervention for mindfulness based stress reduction (MBSR). Behav Res Ther. 2012;50:3–12. doi:10.1016/j.brat.2011.10.011
10. Zhang JY, Zhou YQ, Feng ZW, et al. Randomized controlled trial of mindfulness-based stress reduction (MBSR) on posttraumatic growth of Chinese breast cancer survivors. Psychol Health Med. 2017;1:94–109. doi:10.1080/13548506.2016.1146405
11. Alsubaiea M, Abbottb R, Dunn B, et al. Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: a systematic review. Clin Psychol Rev. 2017;55:74–91. doi:10.1016/j.cpr.2017.04.008
12. Ng QX, Venkatanarayanan N, Loke W, et al. A meta-analysis of the effectiveness of yoga-based interventions for maternal depression during pregnancy. Complement Ther Clin Pract. 2019;34:8–12. doi:10.1016/j.ctcp.2018.10.016
13. Labelle LE, Campbell TS, Carlson LE. Mindfulness-based stress reduction in oncology: evaluating mindfulness and rumination as mediators of change in depressive symptoms. Mindfulness. 2010;1(1):28–40. doi:10.1007/s12671-010-0005-6
14. Lazaratou H, Dikeos DG, Anagnostopoulos DC, Soldatos CR. Depressive symptomatology in high school students: the role of age, gender and academic pressure. Community Ment Health J. 2010;46:289–295. doi:10.1007/s10597-010-9296-2
15. Liu AL, Liu XM. Causes of college students subthreshold depression and comprehensive intervention research. J Hubei Normal Univ. 2016;36:107–110.
16. Zainal NZ, Booth S, Huppert FA. The efficacy of mindfulness-based stress reduction on mental health of breast cancer patients: a meta-analysis. Psychol Oncol. 2013;22:1457–1465. doi:10.1002/pon.3171
17. Yang WH, Wu DJ, Peng F. Application of Chinese Version of beck depression inventory-II to Chinese first-year college students. Chin J Clin Psychol. 2012;6:762–764.
18. Brown RA, Ryan RM. Perils and promise in defining and measuring mindfulness: observationsfrom experience. Clin Psychol Sci Pract. 2004;11:242–248. doi:10.1093/clipsy.bph078
19. Deng YQ, Li S, Tang YY, Zhu LH, Richard R, Kirk B. Psychometric properties of the Chinese translation of the Mindful Attention Awareness Scale (MAAS). Mindfulness. 2012;3:10–14. doi:10.1007/s12671-011-0074-1
20. Han X, Yang HF. Chinese version of Nolen-Hoeksema Ruminative Responses Scale (RRS). Chin J Clin Psychol. 2009;5:78–92.
21. Klein DN, Shankman SA, Lewinsohn PM, Seeley JR. Subthreshold depressive disorder in adolescents: predictorsof escalation to full-syndrome depressive disorders. J Am Acad Child Adolesc Psychiatry. 2009;48:703–710. doi:10.1097/CHI.0b013e3181a56606
22. Ren ZH, Li XY, Zhao LB. The effects of internet cognitive-behavioral therapy on depression and Mechanism. Acta Psychologica Sinica. 2016;48:818–832. doi:10.3724/SP.J.1041.2016.00818
23. Liu HN, Zeng WX, Li XW, et al. Impacts of attentional training on attention bias of sub-clinical depressed undergraduates. Chin J Behav Med Brain Sc. 2016;25:60–66.
24. Costello DM, Swendsen J, Rose JS, Dierker LC. Risk and protective factors associated with trajectories of depressed mood from adolescence to early adulthood. J Consult Clin Psychol. 2008;76:173–183. doi:10.1037/0022-006X.76.2.173
25. Yu QY, Zhang HZ. On analysis of the psychotherapy based on mindfulness meditation. Med Philos. 2013;31:P49–P51.
26. Wu Q, Shi L, Xia ZP, et al. A comparison of intervention effects of three mindfulness training modes on depressed students. Chin J Clin Psychol. 2013;4:685–687.
27. Van Aalderen JR, Donders AR, Giommi F, et al. The efficacy of mindfulness-based cognitive therapy in recurrent depressed patients with and without a current depressive episode: a randomized controlled trial. Psychol Med. 2012;5:989–1001. doi:10.1017/S0033291711002054
28. Tang HB, Luo HJ, Zhang XL, et al. Mechanism of mindfulness training in the intervention in rumination. Chin J Clin Psychol. 2012;6:451–453.
29. Taren AA, Gianaros PJ, Greco CM, et al. Mindfulness meditation training alters stress-related amygdala resting state functional connectivity: a randomized controlled trial. Social Cognit Affective Neurosci. 2015;10(12):1758–1768. doi:10.1093/scan/nsv066
30. Aker M, Harmer C, Landr NI. More rumination and less effective emotion regulation in previously depressed women with preserved executive functions. BMC Psychiatry. 2014;14:334. doi:10.1186/s12888-014-0334-4
31. Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: a psychometric analysis. Cognit Ther Res. 2003;3:247–259. doi:10.1023/A:1023910315561
32. Bishop SR, Lau M, Shapiro S, et al. Mindfulness: a proposed operational definition. Clin Psychol. 2004;11(3):230–241.
33. Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspective Psychol Sci. 2008;5:400–424. doi:10.1111/j.1745-6924.2008.00088.x
34. Teasdale JD. Emotional processing, three modes of mind and the prevention of relapse in depression. Behav Res Ther. 1999;S1:53–77. doi:10.1016/S0005-7967(99)00050-9
35. Ng QX, Peters C, Ho CYX, et al. A meta-analysis of the use of probiotics to alleviate depressive symptoms. J Affect Disord. 2018;1(228):13–19. doi:10.1016/j.jad.2017.11.063
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.