Back to Journals » Clinical Ophthalmology » Volume 16
Effects of Low-Concentration Nitrous Oxide Anesthesia on Patient Anxiety During Cataract Surgery: A Retrospective Cohort Study
Authors Sasajima H ![]() , Zako M, Ueta Y, Murotani K
, Zako M, Ueta Y, Murotani K ![]()
Received 15 July 2022
Accepted for publication 22 August 2022
Published 24 August 2022 Volume 2022:16 Pages 2803—2812
DOI https://doi.org/10.2147/OPTH.S382476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hirofumi Sasajima,1 Masahiro Zako,2 Yoshiki Ueta,1 Kenta Murotani3
1Department of Ophthalmology, Shinseikai Toyama Hospital, Imizu, 939-0243, Japan; 2Department of Ophthalmology, Asai Hospital, Seto, 489-0866, Japan; 3Biostatistics Center, Kurume University, Kurume, 830-0011, Japan
Correspondence: Hirofumi Sasajima, Department of Ophthalmology, Shinseikai Toyama Hospital, 89-10 Shimowaka, Imizu, Toyama, 939-0243, Japan, Tel +81-766-52-2156, Email [email protected]
Purpose: We investigated the effects of 30% low-concentration nitrous oxide (N2O) anesthesia on anxiety, pain, and vital signs and the patient population that would benefit from low-concentration N2O anesthesia during cataract surgery.
Patients and Methods: Sixty-three patients who underwent cataract surgery due to visual impairment from cataracts were included in this single-center retrospective cohort study conducted at the Ophthalmology Department of Shinseikai Toyama Hospital, Japan. Fifty eyes of 39 patients received a combination of local and N2O anesthesia (N2O group), and 30 eyes of 24 patients received local anesthesia without N2O anesthesia (Air group). The primary outcome measures were visual analogue scale (VAS) scores for patient anxiety, pain, and vital signs. The secondary outcome measures were the patient population.
Results: The change in the VAS scores for anxiety and pain decreased significantly (p = 0.002 and p = 0.014, respectively) in the N2O group (− 15.6 ± 22.9 and 12.4 ± 14.9, respectively) compared with that in the Air group (1.2 ± 20.6 and 24.2 ± 22.4, respectively). The systolic and diastolic blood pressure changes did not significantly differ between both groups (p = 0.093 and p = 0.23, respectively). The change in heart rate decreased significantly (p = 0.001) in the N2O group (− 4.8 ± 4.8 bpm) compared with that in the Air group (− 0.6 ± 5.8 bpm). Multivariate analyses demonstrated that the change in anxiety level in the N2O group correlated significantly with patient age (p = 0.045) and preoperative VAS score for anxiety (p = 0.0001), whereas the change in anxiety level in the Air group did not correlate with any factor.
Conclusion: Low-concentration N2O anesthesia showed beneficial effects on intraoperative anxiety and pain during cataract surgery; this may aid the stabilization of intraoperative vital signs. Moreover, low-concentration N2O anesthesia during cataract surgery could benefit young patients and patients with high levels of preoperative anxiety.
Keywords: cataract surgery, low-concentration nitrous oxide anesthesia, patient anxiety
A Letter to the Editor has been published for this article.
A Response to Letter by Dr SHUJA has been published for this article.
Introduction
Some patients experience anxiety or fear during cataract surgery under local anesthesia.1,2 Surgeons are faced with the challenges of ensuring a successful surgery and reducing patient anxiety during surgery. To date, several techniques for reducing patient anxiety during surgery have been attempted, such as listening to music before and during surgery,1,3–5 preoperative patient education,6,7 and hand massage or hand-holding before and during surgery.8,9
Recently, Noguchi et al10 reported that local anesthesia with a low of concentration of nitrous oxide (N2O) could reduce intraoperative patient pain during ptosis surgery. In addition, Noguchi et al11 reported for the first time that low-concentration N2O anesthesia could reduce intraoperative patient anxiety during cataract surgery. N2O is a colorless and virtually odorless gas with a faint sweet smell12 that has both anxiolytic13 and analgesic effects.14,15 N2O has low solubility with a high minimum alveolar concentration (MAC) in the brain; the blood partition coefficient (the ratio of N2O dissolved per gram of brain to that dissolved in 1 mL of blood) was reported to be 1.06,16 and MAC was 104%.17 The rapid onset of action of N2O is associated with rapid recovery. N2O anesthesia has been used in many disciplines of medicine, including dentistry, anesthesia, obstetrics, emergency medicine, and pediatrics,12,18,19 owing to the relative safety of N2O anesthesia, with only a few adverse effects reported.20,21 However, to date, few reports have evaluated the efficacy of N2O anesthesia in cataract surgery,11 and the patient population that would benefit from the low-concentration N2O anesthesia during cataract surgery has not been determined.
In this study, we investigated whether low-concentration N2O anesthesia reduces patient anxiety and pain during cataract surgery and its effects on vital signs. We also aimed to identify the patient population that would benefit from low-concentration N2O anesthesia during cataract surgery.
Patients and Methods
Patients
This retrospective observational study included patients who underwent cataract surgery owing to visual impairment due to cataracts. Each patient received oral and written information regarding the cataract surgery and provided consent before surgery. The study protocol was approved by the Institutional Review Board of Shinseikai Toyama Hospital (reference number: 220,125–2), which adhered to the tenets of the Declaration of Helsinki. We reviewed the medical and ocular histories of patients undergoing cataract surgery between October 12, 2021, and December 23, 2021, in the Department of Ophthalmology of Shinseikai Toyama Hospital (Toyama, Japan).
The inclusion criteria were patients who responded to the questionnaire on anxiety and pain. The patients who could not answer the questionnaire by themselves and had severe cataracts (grades 4 and 5, with nuclei graded according to the Emery–Little classification22) were excluded from the study.
During the study period, 50 eyes of 39 patients underwent cataract surgery under local anesthesia with N2O sedation (N2O group) and met the inclusion criteria. Thirty eyes of 24 patients underwent cataract surgery under local anesthesia without N2O sedation (Air group) and met the inclusion criteria. Bilateral cataract surgeries were performed one eye at a time with an interval of 1–2 weeks.
N2O anesthesia was used when the blood pressure (BP) before entering the operating room was higher than 100/60 mmHg, and the initial vital signs after entering the operating room were normal.
Surgical Procedures and N2O Setting
All the patients received 4% xylocaine eye drop before the procedure. Thirty percent low-concentration N2O (Oxygen: 2 L/min and N2O: 1 L/min; total: 3 L/min) inhalation (SAFER-100®, Nambuk Mednics CO., Ltd, Gyeonggi-do, Korea) with a nasal cannula (SOFTECH®, Hudson RCI®, Teleflex Medical, Dublin, Ireland) was administered following initial measurement of the vital signs and continued until the end of the surgery in the N2O group. All the patients received 2% sub-Tenon’s anesthesia (2 mL) at the lower temporal region. Sub-Tenon’s anesthesia was performed approximately 2–3 min after the initial vital signs were measured in the operating room. Phacoemulsification was performed using a 2.2-mm single-plane sclerocorneal incision and phacoemulsification system (Centurion®, Alcon Laboratories, Inc., Fort Worth, TX, USA). All the surgical procedures were performed by two surgeons (H.S. and Y.U., who perform approximately 450 and 500 cataract surgeries per year, respectively). One surgeon (H.S.) performed 45 cataract surgeries (25 eyes of 21 patients in the N2O group and 20 eyes of 14 patients in the Air group). The other surgeon (Y.U.) performed 35 cataract surgeries (25 eyes of 18 patients in the N2O group and 10 eyes of 10 patients in the Air group). In this study, the surgical procedures were performed similarly, and classical piano music was played from a CD player during the surgery. In addition, we did not use preoperative sedation drugs in any of the cases.
Assessment of Levels for Anxiety, Pain, and Nausea
Patients reported their anxiety level before anesthesia in the hospital room and immediately following cataract surgery using the 100-mm visual analogue scale (VAS),23 ranging from 0 to 100, where 0 indicates no anxiety and 100 indicates the maximum level of anxiety. The VAS score was determined by measuring the distance in millimeters from the left end of the line to the point marked by the patient. In the postoperative VAS, patients reported the amount of anxiety perceived during the surgery. The change in the anxiety level was calculated as the intraoperative VAS score for anxiety minus the preoperative values. After the surgery, the patients answered questions regarding intraoperative pain and nausea using the VAS and were asked whether they had any intraoperative memories as well.
Vital Signs Measurements
Preoperative systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and oxygen saturation (SpO2) were measured immediately after the surgical chair was positioned in the same position as during the surgery. BP was measured using a cuff-type upper-arm sphygmomanometer (Vismo® PVM 2701, NIHON KODEN, Tokyo, Japan), and HR was measured using a two-lead electrocardiogram monitor (Vismo® PVM 2701, NIHON KODEN, Tokyo, Japan). SpO2 was measured on the index finger using a pulse oximeter (Vismo® PVM 2701, NIHON KODEN, Tokyo, Japan). Intraoperative BP, HR, and SpO2 were measured every 5 min until the end of the surgery. We then calculated the mean intraoperative BP, HR, and SpO2 and used the values for statistical analysis. Changes in the vital signs were calculated as the mean intraoperative values minus the preoperative values. The presence or absence of consciousness was determined by response to the call, and the disappearance of spontaneous breathing was confirmed by the SpO2 waveform.
Ophthalmic Examinations
Axial length was measured in all patients using the OA-2000® (Tomey, Nagoya, Japan) before the surgery. The ultrasound and operation times were also evaluated in this study.
Statistical Analysis
A biostatistician (K.M.) performed the statistical analyses using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). The homogeneity of the variance was analyzed using the F-test. An unpaired t-test was used when both groups had equal variance. An unpaired t-test with Welch’s correction was used when both groups did not assume equal variance. Differences in the categorical data between the two groups were analyzed using Fisher’s exact test. All the values were expressed as the mean ± standard deviation. In addition, we also analyzed five factors, namely patient age, sex, first or second eye, preoperative VAS score for anxiety, and surgeon in the N2O and Air groups, to investigate the patient characteristic affecting the change in anxiety level. This analysis was performed using the multiple linear mixed model, which included the patient’s age, sex, first or second eye, preoperative VAS score for anxiety, and surgeon (H.S. or Y.U.) as fixed effects and patients as a random effect. The statistical significance was set at p<0.05.
Results
Patient Characteristics
Baseline patient characteristics are summarized in Table 1. No complications were associated with cataract surgery, and no systemic complications, such as excessive hypotension, unconsciousness, or disappearance of spontaneous breathing, were observed in this study.
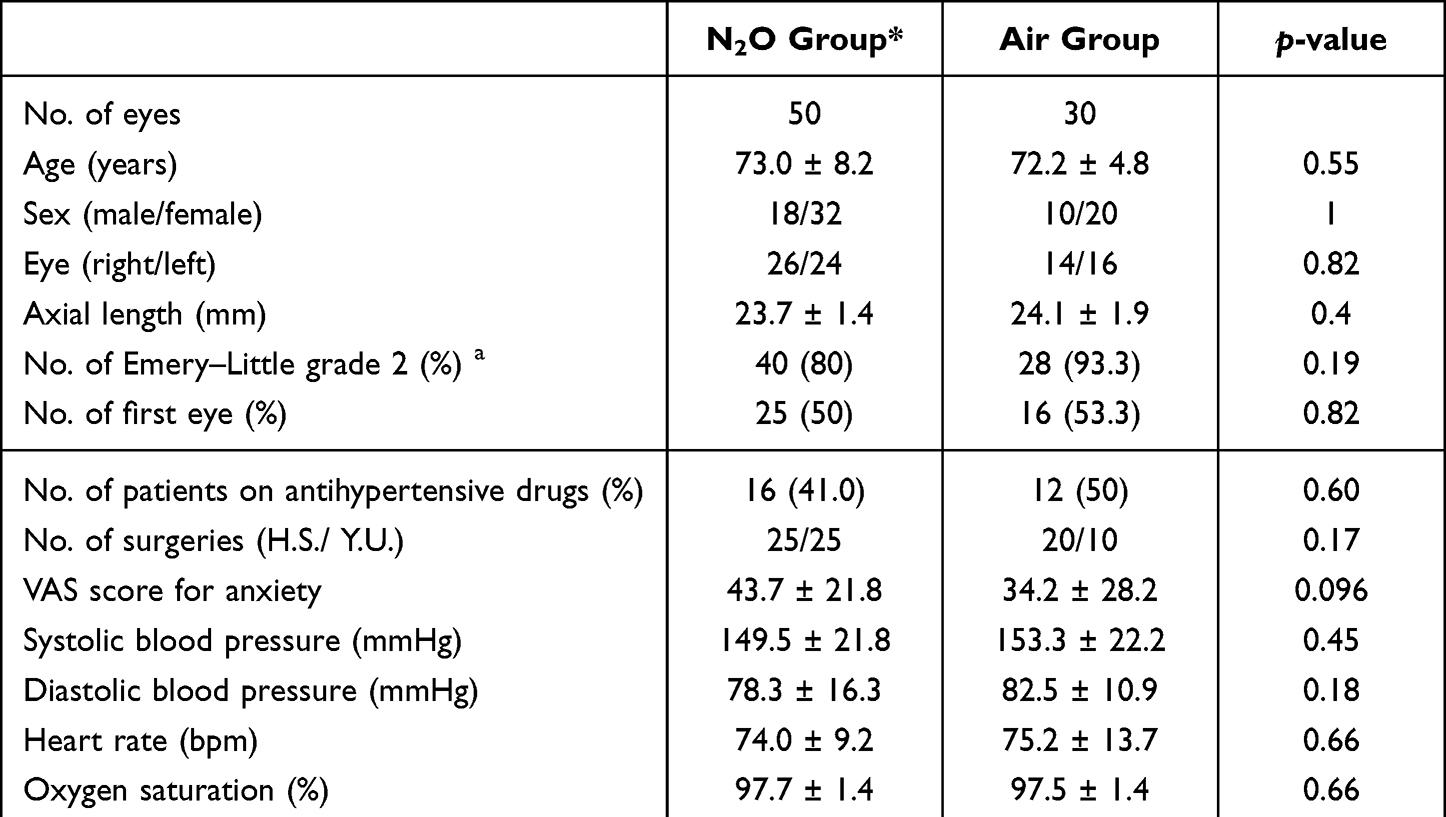 |
Table 1 Summary of the Patients’ Characteristics Including Vital Signs Before Cataract Surgery |
Comparison of the Subjective Measures
The intraoperative VAS score for anxiety did not significantly differ (p=0.24) between the N2O group (28.1±23.6) and the Air group (35.3±30.8) (Figure 1A). However, the change in the VAS score for anxiety was significantly reduced (p=0.002) in the N2O group (−15.6±22.9) compared with the Air group (1.2±20.6) (Figure 1B). In addition, the intraoperative VAS score for pain was significantly reduced (p=0.014) in the N2O group (12.4±14.9) compared to that in the Air group (24.2±22.4) (Figure 1C). The intraoperative VAS score for nausea did not significantly differ (p=0.41) between the N2O group (0.3±1.3) and the Air group (0.1±0.3) (Figure 1D). Four (4/50, 8%) patients in the N2O group (with VAS scores of 1, 1, 2, and 9 points) and 3 (3/30, 10%) patients each in the Air group (with a VAS score of 1 point) complained of intraoperative nausea; no severe nausea, which could cause vomiting and affect cataract surgery, was noted. All the patients were fully conscious during surgery.
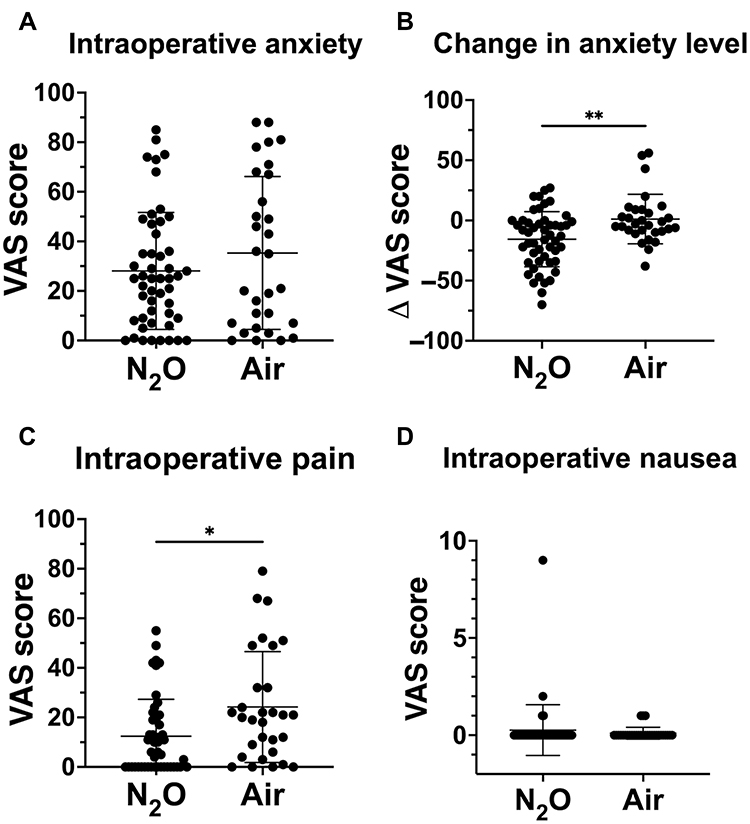 |
Figure 1 Comparison of intraoperative anxiety (A), change in anxiety level (B), intraoperative pain (C), and intraoperative nausea (D) between the nitrous oxide (N2O) anesthesia group and the Air group. The change in anxiety level was calculated as the intraoperative visual analogue scale (VAS) score for anxiety minus the preoperative VAS score for anxiety (B). *p<0.05. **p<0.01. |
Comparison of the Objective Measures
Intraoperative SBP was significantly lower (p=0.046) in the N2O group (147.6±17.9 mmHg) than in the Air group (156.1±18.4 mmHg) (Figure 2A). However, the change in SBP did not significantly differ (p=0.093) between the N2O group (−1.9±12.0 mmHg) and the Air group (2.8±11.6 mmHg) (Figure 2B). Intraoperative DBP was significantly lower (p = 0.016) in the N2O group (76.2±12.6 mmHg) than in the Air group (82.9±9.6 mmHg) as well (Figure 2C). However, the change in the DBP did not significantly differ (p=0.23) between the N2O group (−2.1±11.0 mmHg) and the Air group (0.4±7.0 mmHg) (Figure 2D). Intraoperative HR and the change in HR significantly decreased (p=0.047 and p=0.001, respectively) in the N2O group (69.2±8.4 bpm and −4.8±4.8 bpm) compared to that in the Air group (74.6±13.2 bpm and −0.6±5.8 bpm) (Figure 3A and B). Intraoperative SpO2 and the change in SpO2 significantly increased (p<0.001 and p<0.001, respectively) in the N2O group (99.3±0.7% and 1.6±1.4%) compared to that in the Air group (97.5±1.4% and −0.03±0.7%) (Figure 3C and D).
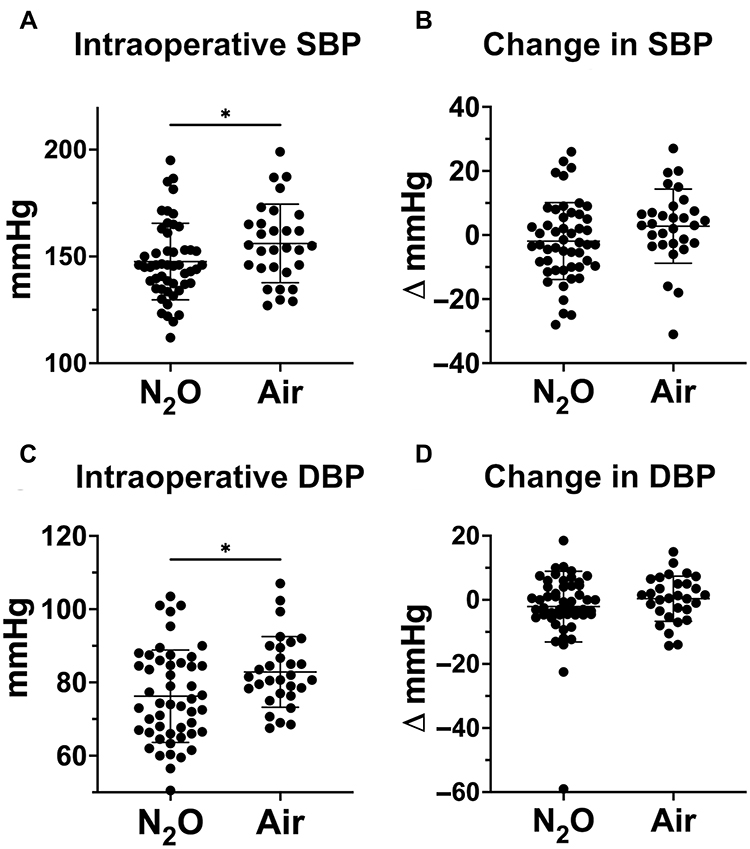 |
Figure 2 Comparison of intraoperative systolic blood pressure (SBP) (A), change in SBP (B), intraoperative diastolic blood pressure (DBP) (C), and change in DBP (D) between the nitrous oxide (N2O) anesthesia group and the Air group. The changes in SBP and DBP were calculated as the mean intraoperative SBP and DBP values minus the preoperative SBP and DBP values, respectively (B and D). * p<0.05. |
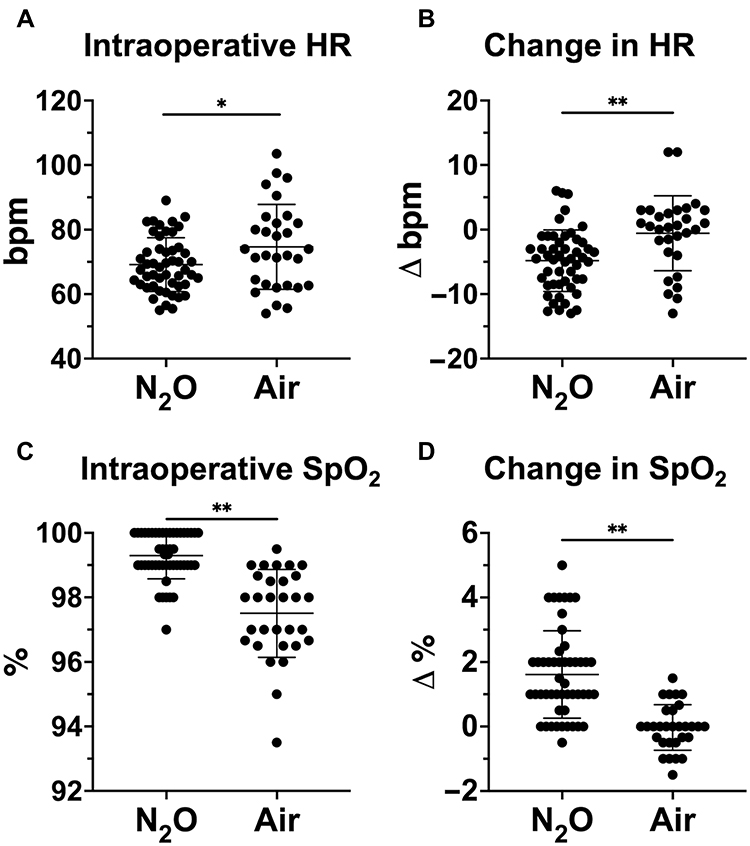 |
Figure 3 Comparison of intraoperative heart rate (HR) (A), change in HR (B), intraoperative oxygen saturation (SpO2) (C), and change in the SpO2 (D) between the nitrous oxide (N2O) anesthesia group and the Air group. The changes in HR and SpO2 were calculated as the mean intraoperative HR and SpO2 values minus the preoperative HR and SpO2 values, respectively (B and D). *p<0.05. **p<0.01. |
Factors Affecting the Change in Anxiety Level Using the Multiple Linear Mixed Model
The results of the multivariate analyses for the change in anxiety level are shown in Table 2. The change in anxiety level in the N2O group significantly correlated with patient age (adjusted coefficient: 0.79, 95% confidence interval (CI): 0.018–1.6, p=0.045) and preoperative VAS score for anxiety (adjusted coefficient: −0.55, 95% CI: −0.82– −0.29, p=0.0001). Meanwhile, the change in anxiety level in the Air group did not correlate with any of the factors.
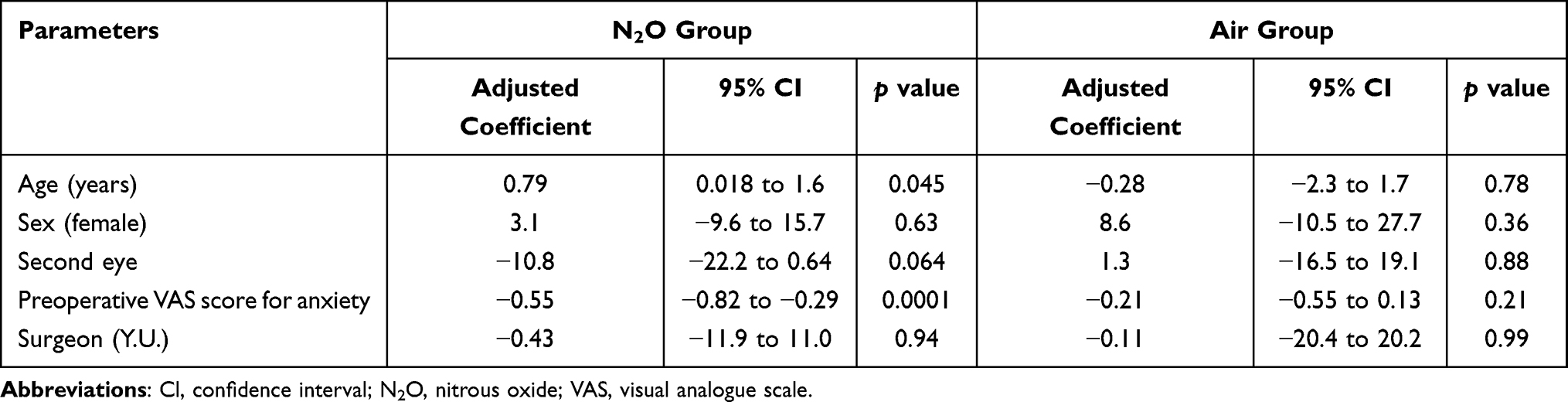 |
Table 2 Factors Affecting the Change in the Anxiety Level in the Multivariate Analyses Using the Linear Mixed Model |
Surgical Procedures
The ultrasound time and operation time did not significantly differ between the N2O group and the Air group (28.5±10.6 s and 24±10.9 s, p=0.075; 487.4±118.7 s and 519.2±101.8 s, p=0.23, respectively).
Discussion
In this study, we demonstrated that the application of low-concentration N2O anesthesia significantly reduced patient anxiety and pain during cataract surgery. Moreover, N2O anesthesia significantly, but not excessively, decreased intraoperative SBP and DBP in the enrolled patients. The change in the HR significantly decreased under N2O anesthesia but did not result in bradycardia. These findings suggest that using low-concentration N2O anesthesia in cataract surgery may help reduce intraoperative patient anxiety and pain, which may help stabilize intraoperative vital signs. Moreover, multivariate analyses demonstrated that changes in anxiety level in the N2O group significantly correlated with patient age and preoperative VAS score for anxiety. This suggests that low-concentration N2O anesthesia during cataract surgery could be more advantageous for young patients and patients with high preoperative anxiety.
Our results demonstrated that the intraoperative anxiety score was lower in the N2O group (28.1±23.6) than in the Air group (35.3±30.8); however, it did not differ significantly (p=0.24). This could be attributed to the sample size.11 Meanwhile, our study demonstrated that the change in the anxiety level decreased significantly (p=0.002) in the N2O group (−15.6±22.9) compared with that in the Air group (1.2±20.6), which may suggest that low-concentration N2O anesthesia is useful in reducing intraoperative anxiety.
In this study, we also investigated the patient characteristics affecting the change in anxiety level in the N2O and Air groups. Table 2 shows that the change in the anxiety level in the N2O group positively correlated with the patients’ age (adjusted coefficient: 0.79, p=0.045) and negatively correlated with the preoperative VAS score for anxiety (adjusted coefficient: −0.55, p=0.0001). These results suggest that N2O anesthesia is more effective in reducing intraoperative anxiety in young patients and patients with high preoperative anxiety.
The intraoperative pain score was significantly lower (p=0.014) in the N2O group (12.4±14.9) than in the Air group (24.2±22.4). The analgesic effect of N2O suggests that 30% N2O is equivalent to 10–15 mg morphine.24 Meanwhile, a previous study did not observe a significant reduction in intraoperative pain score.11 This could be due to the duration of N2O anesthesia; in fact, the operation time was longer in this study (approximately 8 min) than in the previous report (approximately 5 min).11 Further studies with a large number of cases are warranted to elucidate the analgesic effect of low-concentration N2O anesthesia in cataract surgery.
A previous study suggested that the level of patient-perceived anxiety and pain could differ between the first and second cataract eye surgery.25 In addition, the outcome could also be affected by the fact that different surgeons performed the surgeries. Considering these, we analyzed the data using a linear mixed model for statistical comparisons, which was adjusted for the group (N2O or Air), surgeon (H.S. or Y.U.), and first or second eye as fixed effects and patients as a random effect. The results demonstrated that anxiety levels were significantly reduced (adjusted coefficient: −16.4, 95% CI: −26.8– −6.0, p=0.0025) in the N2O group as compared to the Air group. The intraoperative pain score was significantly lower (adjusted coefficient: −12.7, 95% CI: −21.1– −4.3, p=0.0036) in the N2O group than that in the Air group. Thus, we believe that the results of our study are valid.
No significant adverse effects of low-concentration N2O anesthesia were observed in this study. Vital signs, including BP, HR, and SpO2, were stable in each group during cataract surgery, and no disorientation was noted on low-concentration N2O. Although further studies are warranted to elucidate the safety of N2O anesthesia in ophthalmic surgery, our results suggest that N2O anesthesia could be effective in other ophthalmic surgeries such as vitreous, glaucoma, and ptosis surgeries.10 These surgeries generally take longer and sometimes cause more patient anxiety and pain than cataract surgery. Meanwhile, N2O has the potential to escape into the dead space and brings an increase in the intraocular gas bubble size, resulting in a subsequent rise in intraocular pressure.26–28 Although conscious sedation is generally safer than general sedation,29 we should be aware of the possibility of expansion of the intraocular gas caused by N2O, which may result in severe and permanent visual loss.
This study had several limitations. First, a sampling bias inherent to its retrospective nature and relatively small sample size cannot be excluded. Although using low-concentration N2O anesthesia significantly reduced patient anxiety and pain during cataract surgery, additional studies with a larger number of patients are warranted to determine the efficacy of low-concentration N2O anesthesia in cataract surgery. Second, this study was conducted at a single center. Although the use of low-concentration N2O anesthesia significantly reduced patient anxiety, as reported by a previous study,11 it may be necessary to confirm our findings at another medical center. Finally, although vital signs were stable under low-concentration N2O anesthesia in cataract surgery,11 prospective studies with a larger number of cases are warranted to evaluate the safety of N2O.
Conclusion
Our results suggest that low-concentration N2O anesthesia may reduce patient anxiety and pain, which may stabilize the vital signs during cataract surgery. Moreover, low-concentration N2O anesthesia during cataract surgery could be particularly advantageous for young patients and patients with high levels of preoperative anxiety.
Abbreviations
BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; HR, heart rate; MAC, minimum alveolar concentration; N2O, nitrous oxide; SBP, systolic blood pressure; SpO2, oxygen saturation; VAS, visual analogue scale.
Data Sharing Statement
The datasets used in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Shinseikai Toyama Hospital, Toyama, Japan (reference number: 220125-2). Informed consent was obtained from all the patients involved in the study.
Acknowledgments
We want to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Wiwatwongwana D, Vichitvejpaisal P, Thaikruea L, Klaphajone J, Tantong A, Wiwatwongwana A. The effect of music with and without binaural beat audio on operative anxiety in patients undergoing cataract surgery: a randomized controlled trial. Eye. 2016;30(11):1407–1414. doi:10.1038/eye.2016.160
2. Obuchowska I, Konopinska J. Fear and anxiety associated with cataract surgery under local anesthesia in adults: a systematic review. Psychol Res Behav Manag. 2021;14:781–793. doi:10.2147/PRBM.S314214
3. Cruise CJ, Chung F, Yogendran S, Little D. Music increases satisfaction in elderly outpatients undergoing cataract surgery. Can J Anaesth. 1997;44(1):43–48. doi:10.1007/BF03014323
4. Dahshan D, Kuzbel J, Verma V. A role for music in cataract surgery: a systematic review. Int Ophthalmol. 2021;41(12):4209–4215. doi:10.1007/s10792-021-01986-9
5. Guerrier G, Abdoul H, Jilet L, Rothschild P, Baillard C. Efficacy of a web app-based music intervention during cataract surgery: a randomized clinical trial. JAMA Ophthalmol. 2021;139(9):1007–1013. doi:10.1001/jamaophthalmol.2021.2767
6. Morrell G. Effect of structured preoperative teaching on anxiety levels of patients scheduled for cataract surgery. Insight. 2001;26(1):4–9. doi:10.1067/min.2001.113201
7. Zhang MH, Haq ZU, Braithwaite EM, Simon NC, Riaz KM. A randomized, controlled trial of video supplementation on the cataract surgery informed consent process. Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1719–1728. doi:10.1007/s00417-019-04372-5
8. Kim MS, Cho KS, Woo H, Kim JH. Effects of hand massage on anxiety in cataract surgery using local anesthesia. J Cataract Refract Surg. 2001;27(6):884–890. doi:10.1016/S0886-3350(00)00730-6
9. Astbury N. A hand to hold: communication during cataract surgery. Eye. 2004;18(2):115–116. doi:10.1038/sj.eye.6700569
10. Noguchi S, Nakakura S, Noguchi A, et al. Utility and safety of low-concentration nitrous oxide anesthesia in ptosis surgery. Medicine. 2021;100(4):e23753. doi:10.1097/MD.0000000000023753
11. Noguchi S, Nakakura S, Noguchi A, et al. Examination of the safety and effectiveness of low-concentration nitrous oxide anesthesia in cataract surgery. J Cataract Refract Surg. 2022;48(3):317–321. doi:10.1097/j.jcrs.0000000000000749
12. Becker DE, Rosenberg M. Nitrous oxide and the inhalation anesthetics. Anesth Prog. 2008;55(4):124–131. doi:10.2344/0003-3006-55.4.124
13. Jevtović-Todorović V, Todorovć SM, Mennerick S, et al. Nitrous oxide (laughing gas) is an NMDA antagonist, neuroprotectant and neurotoxin. Nat Med. 1998;4(4):460–463. doi:10.1038/nm0498-460
14. Fang F, Guo TZ, Davies MF, Maze M. Opiate receptors in the periaqueductal gray mediate analgesic effect of nitrous oxide in rats. Eur J Pharmacol. 1997;336(2–3):137–141. doi:10.1016/S0014-2999(97)01219-3
15. Sawamura S, Kingery WS, Davies MF, et al. Antinociceptive action of nitrous oxide Is mediated by stimulation of noradrenergic neurons in the brainstem and activation of α 2B adrenoceptors. J Neurosci. 2000;20(24):9242–9251. doi:10.1523/JNEUROSCI.20-24-09242.2000
16. Kety SS, Harmel MH, Broomell HT, Rhode CB. The solubility of nitrous oxide in blood and brain. J Biol Chem. 1948;173(2):487–496. doi:10.1016/S0021-9258(18)57420-2
17. Hornbein TF, Eger IIEI, Winter PM, Smith G, Wetstone D, Smith KH. The minimum alveolar concentration of nitrous oxide in man. Anesth Analg. 1982;61(7):553–556. doi:10.1213/00000539-198207000-00001
18. Annequin D, Carbajal R, Chauvin P, Gall O, Tourniaire B, Murat I. Fixed 50% nitrous oxide oxygen mixture for painful procedures: a French survey. Pediatrics. 2000;105(4):e47–e47. doi:10.1542/peds.105.4.e47
19. Sanders RD, Weimann J, Maze M, Warner D, Warner M. Biologic effects of nitrous oxide. Anesthesiology. 2008;109(4):707–722. doi:10.1097/ALN.0b013e3181870a17
20. Zier JL, Liu M. Safety of high-concentration nitrous oxide by nasal mask for pediatric procedural sedation: experience with 7802 cases. Pediatr Emerg Care. 2011;27(12):1107–1112. doi:10.1097/PEC.0b013e31823aff6d
21. Tsze DS, Mallory MD, Cravero JP. Practice patterns and adverse events of nitrous oxide sedation and analgesia: a report from the pediatric sedation research consortium. J Pediatr. 2016;169(260–265):260–265.e2. doi:10.1016/j.jpeds.2015.10.019
22. Emery JM, Little JH. Phacoemulsification and Aspiration of Cataracts: Surgical Techniques, Complications, and Results. St Louis, MO: C. V. Mosby; 1979:45–48.
23. Aitken RC. Measurement of feelings using visual analogue scales. Proc R Soc Med. 1969;62:989–993.
24. Chapman WP, Arrowood JG, Beecher HK. The analgetic effects of low concentrations of nitrous oxide compared in man with morphine sulphate. J Clin Invest. 1943;22(6):871–875. doi:10.1172/JCI101461
25. Shi C, Yuan J, Zee B. Pain perception of the first eye versus the second eye during phacoemulsification under local anesthesia for patients going through cataract surgery: a systematic review and meta-analysis. J Ophthalmol. 2019;2019:1–8. doi:10.1155/2019/4106893
26. Briggs M, Wong D, Groenewald C, McGalliard J, Kelly J, Harper J. The effect of anaesthesia on the intraocular volume of the C3F8 gas bubble. Eye. 1997;11(1):47–52. doi:10.1038/eye.1997.10
27. Hart RH, Vote BJ, Borthwick JH, McGeorge AJ, Worsley DR. Loss of vision caused by expansion of intraocular perfluoropropane (C3F8) gas during nitrous oxide anesthesia. Am J Ophthalmol. 2002;134(5):761–763. doi:10.1016/S0002-9394(02)01654-9
28. Tanchyk A, Tanchyk A. The absolute contraindication for using nitrous oxide with intraocular gases and other dental considerations associated with vitreoretinal surgery. Gen Dent. 2013;61:e6–e7.
29. Averley PA, Lane I, Sykes J, Girdler NM, Steen N, Bond S. An RCT pilot study to test the effects of intravenous midazolam as a conscious sedation technique for anxious children requiring dental treatment—an alternative to general anaesthesia. Br Dent J. 2004;197(9):553–558. doi:10.1038/sj.bdj.4811808
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.