Back to Journals » Clinical Ophthalmology » Volume 20
Effects of Lotilaner Ophthalmic Solution, 0.25% on Demodex Blepharitis Patients with Meibomian Gland Disease
Authors Gupta PK ![]() , Gaddie IB
, Gaddie IB ![]() , Shultz MC, Vollmer P, Silverstein SM
, Shultz MC, Vollmer P, Silverstein SM ![]() , Shen Lee B
, Shen Lee B ![]() , O’Dell L, Dhamdhere K, Yeu E
, O’Dell L, Dhamdhere K, Yeu E ![]()
Received 18 June 2025
Accepted for publication 9 December 2025
Published 28 January 2026 Volume 2026:20 527753
DOI https://doi.org/10.2147/OPTH.S527753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Preeya K Gupta,1 Ian Benjamin Gaddie,2 Mitchell C Shultz,3 Patrick Vollmer,4 Steven Marc Silverstein,5 Bridgitte Shen Lee,6 Leslie O’Dell,7 Kavita Dhamdhere,7 Elizabeth Yeu7,8
1Triangle Eye Consultants, Raleigh, NC, USA; 2Gaddie Eye Centers, Louisville, KY, USA; 3Shultz Chang Vision, Los Angeles, CA, USA; 4Vita Eye Clinic, Shelby, NC, USA; 5Silverstein Eye Centers, Kansas City, MO, USA; 6Vision Optique, Houston, TX, USA; 7Tarsus Pharmaceuticals, Inc., Irvine, CA, USA; 8Virginia Eye Consultants, Norfolk, VA, USA
Correspondence: Preeya K Gupta, Triangle Eye Consultants, 9650 Brier Creek Parkway, Suite 103, Raleigh, NC, 27617, USA, Tel +1 919-391-7224, Email [email protected]
Purpose: To evaluate the safety and efficacy of lotilaner ophthalmic solution, 0.25% compared with vehicle in Demodex blepharitis patients with meibomian gland disease.
Patients and Methods: This was a pooled analysis of two prospective, randomized, double-masked studies of Demodex blepharitis patients with meibomian gland disease, Ersa (N=39), and Rhea (N=40). The two studies had the same design, eligibility criteria, and sample size, except Ersa studied lotilaner ophthalmic solution, 0.25% while Rhea studied the associated vehicle. Study outcomes were collarette grading, meibomian gland secretion score (MGSS), number of glands yielding any liquid secretions (MGYLS), number of glands yielding clear liquid secretions (MGYCLS), patient-reported outcomes, and adverse events (AEs).
Results: On Days 43 and 85, there was a statistically significantly higher proportion of patients in the lotilaner group versus the vehicle group with collarette reduction to grade 0 (0– 2 collarettes/lid) (44.7% vs 0.0% and 65.8% vs 0.0%) and grade 0 or 1 (0– 10 collarettes/lid) (81.6% vs 8.8% and 100% vs 0.0%) (all p< 0.001). Mean MGSS, MGYLS, and MGYCLS in the lotilaner group were statistically significantly higher than in the vehicle group. The proportion of lotilaner patients achieving improvement to ≥ 3 glands with clear meibum (grade 3) was significantly higher than the vehicle group on Day 43 (44.7% vs 17.6%, p< 0.05) and Day 85 (78.9% vs 18.2%, p< 0.001). At Days 43 and 85, fluctuating vision, itching, burning, and redness were significantly better in the lotilaner group than in the vehicle group. No serious treatment-related AEs were reported.
Conclusion: In patients with Demodex blepharitis and meibomian gland disease, lotilaner ophthalmic solution, 0.25% demonstrated statistically significant improvements in collarette reduction, meibomian gland function, and patient-reported outcomes at 6 and 12 weeks compared to baseline. Following lotilaner treatment, these parameters were also significantly better than vehicle at 6 and 12 weeks, with a similar safety profile.
Keywords: Demodex blepharitis with meibomian gland disease, Demodex blepharitis and meibomian gland disease, meibomian gland function, meibomian glands yielding liquid secretions, collarette reduction, lotilaner, ocular surface disease
Introduction
Meibomian gland disease is a common eye condition characterized by a chronic, diffuse abnormality of the meibomian glands, terminal-duct obstruction, and/or qualitative/quantitative variations in glandular secretion.1 Meibomian gland disease is the leading cause of the most common form of ocular surface disease, evaporative dry eye. Currently, up to 40 million people in the United States (US) suffer from dry eye disease, and the overall economic burden is estimated to approach $4 billion.2–4
Luo et al found that symptomatic meibomian gland disease was more prevalent in patients with Demodex blepharitis (90%) than in dry eye patients without Demodex (64%), and the patients with Demodex also demonstrated a higher degree of meibomian gland loss (58%) compared to dry eye patients without Demodex blepharitis (2.2%).5 Conversely, Demodex infestation has been reported in 57% to 89% of meibomian gland disease cases compared to 34% to 44% of non-meibomian gland disease controls.6–9 Bhandari et al reported that Demodex infestation of the lashes was nearly twice as high in patients with meibomian gland disease than in non-meibomian gland disease controls.6
Demodex mites can pathologically infest the meibomian glands and have been implicated in causing or exacerbating meibomian gland disease.7,10 Demodex infestation has been correlated with changes in meibomian gland structure and meibum quality,7,11 with ≥96% of individuals with moderate to severe Demodex blepharitis demonstrating structural and/or functional meibomian gland disease.11 Changes in meibum secretion or lipid composition in meibomian gland disease may, in turn, provide a more favorable environment for Demodex mites to proliferate, triggering a cyclical worsening of both conditions.
Several thermal pulsation systems, including LipiFlow, iLux, and TearCare, have been approved by the US Food and Drug Administration (FDA) for use in patients with meibomian gland disease.12–14 In addition, microblepharoexfoliation, intense pulsed light (IPL), radio frequency, and low-level light therapy have also been utilized in the management of meibomian gland disease.15–17 Although these treatments have been documented to yield significant improvements in meibomian gland function and patients’ ocular irritation, they do not treat Demodex blepharitis or address mite infestation in the meibomian glands. Historically, Demodex blepharitis has been addressed with lid hygiene regimens, over-the-counter options such as tea tree oil (TTO) or manuka honey, and off-label use of antiparasitics like ivermectin and metronidazole, with varying levels of efficacy, safety, and tolerability.18–25 Among these, some forms of TTO have been shown to be harmful to the meibomian glands in vitro.26
Recently, lotilaner ophthalmic solution, 0.25% (Tarsus Pharmaceuticals, Irvine, CA), a gamma-aminobutyric acid (GABA)-gated chloride channel inhibitor selective for mites, was approved by the FDA for the treatment of Demodex blepharitis following an extensive clinical trial program in humans that demonstrated high levels of safety and efficacy.27–32 The purpose of the present study was to ascertain whether treatment with lotilaner ophthalmic solution, 0.25%, an approved treatment for Demodex blepharitis, could also influence meibomian gland disease outcomes in patients with both conditions.
Materials and Methods
The present study was a post-hoc pooled analysis of two prospective, randomized, double-masked studies that evaluated lotilaner ophthalmic solution, 0.25% (Ersa, NCT05454956) or vehicle (Rhea, NCT06054217) in Demodex blepharitis patients with meibomian gland disease. Ersa recruited 39 Demodex blepharitis patients across five US clinical sites from August 2022 to May 2023, and Rhea recruited 40 Demodex blepharitis patients across two US clinical sites from August 2023 to March 2024. Both studies were conducted under institutional review board (IRB)-approved protocols (Advarra IRB) that adhered to the tenets of the Declaration of Helsinki. All enrolled patients provided written informed consent using the IRB-approved informed consent form. Although the two studies were performed at different time points, with lotilaner (Ersa) or vehicle (Rhea) as noted above, they otherwise had the same study design, eligibility criteria, and sample size.
For each of the studies, patients needed to meet all of the following criteria (in at least one eye to be enrolled): >10 upper lid lashes with collarettes (Grade 2 or higher), ≥1.0 mites/lash on epilated lashes from the upper/lower eyelids combined, meibomian gland secretion score (MGSS) of 12–32 (out of 45), ≥Grade 1 erythema of the lower eyelid, tear breakup time (TBUT) <10 seconds, and ≥33% total gland area of the lower eyelid with intact partial to full meibomian glands (per meibography). Additional inclusion criteria were a visual analog scale (VAS) score >40 for at least one patient-reported outcome (eg, fluctuating vision, itching, burning, or redness) within the week prior to Day 1 and corrected distance visual acuity (CDVA) better than or equal to 0.7 logMAR on the Early Treatment of Diabetic Retinopathy Study (ETDRS) scale in each eye at Day 1.
Patients were excluded from either study if they had used any artificial tear product within 24 hours of Day 1; systemic antihistamines within 30 days of Day 1; cyclosporine or lifitegrast within 60 days of Day 1; any topical prostaglandin analog within 6 months of Day 1; isotretinoin within 2 years of Day 1; or other prescription drugs, systemic drugs, drug delivery implants, or ocular topical antibacterial, antiparasitic or anti-inflammatory corticosteroid treatments within 14 days of Day 1 or anticipated using any of these treatments during the study. Patients could not have used any treatment(s) for blepharitis within 14 days of Day 1 or lid hygiene measures (eg, lid scrubs, warm compresses, or lid massage) within 7 days of Day 1, or be unwilling to forego the use of these treatments for the duration of the study. The use of lid heating therapies, IPL, meibomian gland probing or therapeutic meibomian gland expression in either eye within 6 months of Day 1 or during the study was prohibited, as were the use of contact lenses, artificial eyelashes, eyelash extensions or other cosmetic eyelash or eyelid procedures (eg, eyeliner tattooing, eyelash tinting, eyelash curling perm, etc.) within 7 days of Day 1 or for the duration of the study.
Patients were excluded from participating in either study if they had conditions or prior procedures that, in the opinion of the investigator, could affect study outcomes including a history of corneal transplant, a recent history of ocular surgery, eyelid abnormalities, ocular surface abnormality or disorder, punctal plugs, corneal disease, active ocular infection or inflammation other than blepharitis and meibomian gland disease, or systemic disease or medications known to cause dry eye. Patients with known hypersensitivity to lotilaner or any of the formulation components and those who were pregnant or lactating were also excluded.
In the Ersa study, eligible patients were randomly assigned in a 1:1 ratio to receive twice daily (BID, n = 21) or three times daily (TID, n = 18) dosing of lotilaner ophthalmic solution, 0.25% for 12 weeks, followed by a 30-day untreated safety follow-up period. In the Rhea study, 12 patients were dosed with vehicle BID for 12 weeks, 11 patients TID for 12 weeks, and 17 patients were dosed TID for six weeks and then BID for six weeks.
The study parameters were collarette grading; meibum quality; MGSS; number of meibomian glands yielding any liquid secretions (MGYLS); number of glands yielding clear liquid secretions (MGYCLS); patient-reported outcomes; and adverse events (AEs) assessments. Collarettes were graded from 0 to 4 (Grade 0= 0 to 2 lashes with collarettes per eyelid; Grade 1= 3 to 10 lashes with collarettes per eyelid; Grade 2= >10 to <1/3 of the lashes with collarettes per eyelid; Grade 3= ≥1/3 to <2/3 of the lashes with collarettes per eyelid; and Grade 4= ≥2/3 of the lashes with collarettes per eyelid). Meibum quality was graded from 0 to 3, with a higher grade meaning better meibum quality (0=no secretion, 1=inspissated/toothpaste, 2=cloudy, 3=clear). MGSS was calculated by summing the meibum quality scores for each of the 15 glands of the lower eyelid (5 consecutive glands in each of the temporal, central, and nasal regions) to determine the overall MGSS (range: 0–45). The number of MGYLS (cloudy or clear liquid with a grade of 2 or 3) and the number of MGYCLS (grade 3) for all 15 glands were evaluated on the lower eyelid, with a range of 0 to 15. Patient-reported outcomes, including fluctuating vision, itching, burning, and redness, were rated on a VAS score from 0 (no discomfort) to 100 (maximal discomfort).
To assess if the two studies were homogeneous enough to be poolable, propensity scores were calculated through a logistic regression with the following baseline and disease burden characteristics as covariates: age, collarette grade, eyelid margin erythema grade, MGSS, MGYLS, MGYCLS, patient-reported fluctuating vision, patient-reported itching, patient-reported redness, and patient-reported burning. The demographic and baseline covariates were balanced between the lotilaner ophthalmic solution, 0.25% (Ersa) and vehicle (Rhea) groups (Table 1) and the two studies were determined to be poolable.
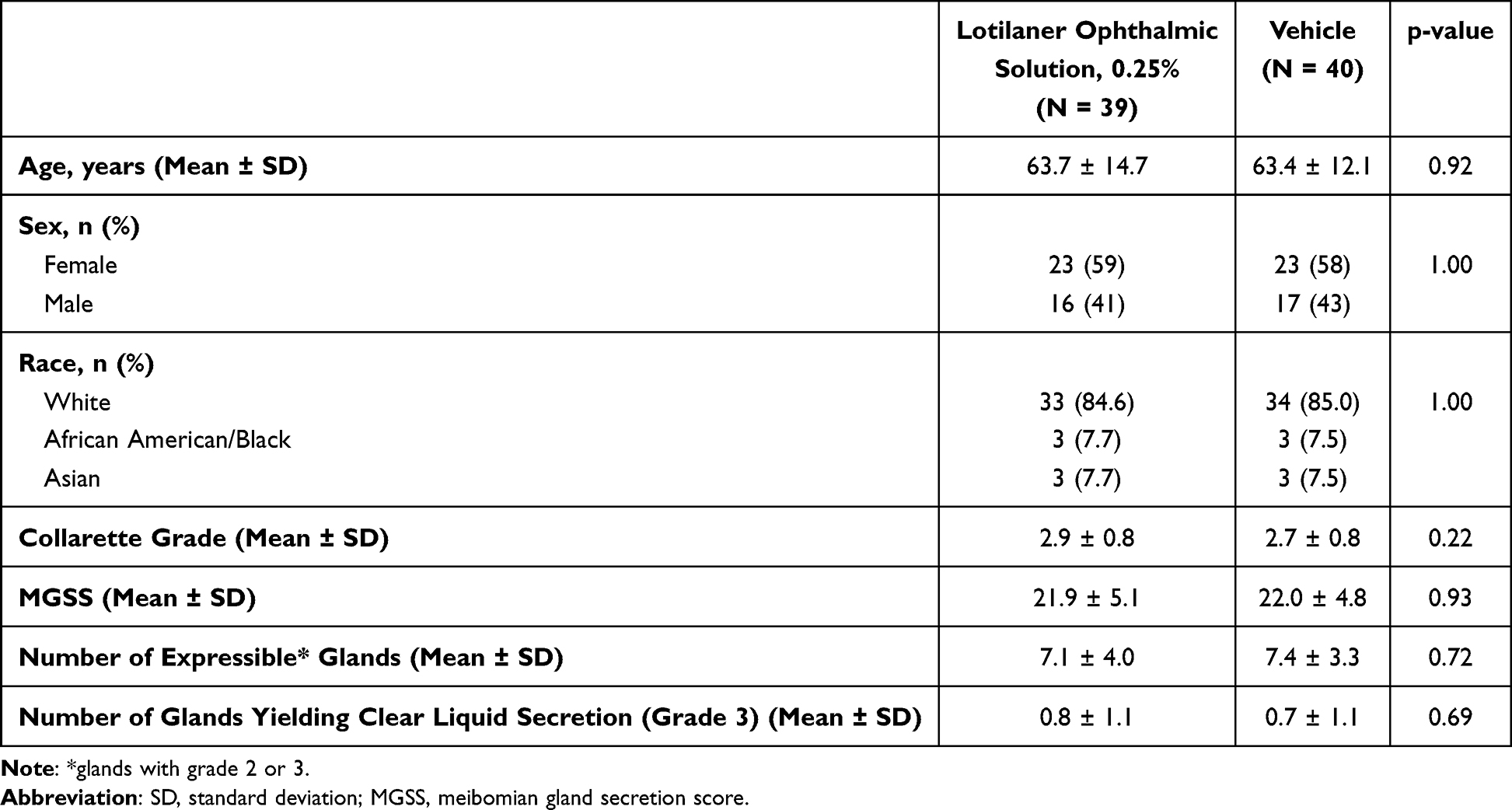 |
Table 1 Demographic and Baseline Characteristics |
The Intent-to-Treat (ITT) population included all randomized subjects. The safety population included all subjects who received any amount of study drug. The analysis eye was defined as the eye that met all inclusion criteria. If both eyes met all inclusion criteria, then the eye with the lowest MGSS at Day 1 was chosen as the analysis eye.
Continuous variables were analyzed as mean and standard deviation (SD) and were compared between the lotilaner ophthalmic solution, 0.25% and vehicle groups using the 2-sample t-test. Categorical variables were presented as frequencies and percentages and were analyzed using the chi-square test. Meibomian gland disease function and patient-reported outcomes were compared between baseline and follow-up visits (Day 43 and Day 85) within the lotilaner ophthalmic solution, 0.25% and vehicle groups using a paired t-test. P <0.05 was considered statistically significant.
Results
There were no statistically significant differences in baseline characteristics by dosing frequency arm (BID/TID) in either study. Outcomes were also comparable whether dosed BID or TID. Therefore, this manuscript presents the findings for the pooled data of all lotilaner-treated patients together (N = 39) and all vehicle-treated patients together (N = 40), regardless of dosing frequency in either group.
Table 1 shows the demographics and baseline characteristics of patients in the lotilaner treatment and vehicle groups. No statistically significant differences were observed between the lotilaner treatment and vehicle study groups at baseline.
Collarette Reduction
On Day 43 and Day 85, the lotilaner treatment group showed a statistically significantly higher proportion of patients with collarette reduction to grade 0 (0–2 collarettes/lid) (Figure 1A) and grade 0 or 1 (0–10 collarettes/lid) (Figure 1B) compared to the vehicle group (p <0.001).
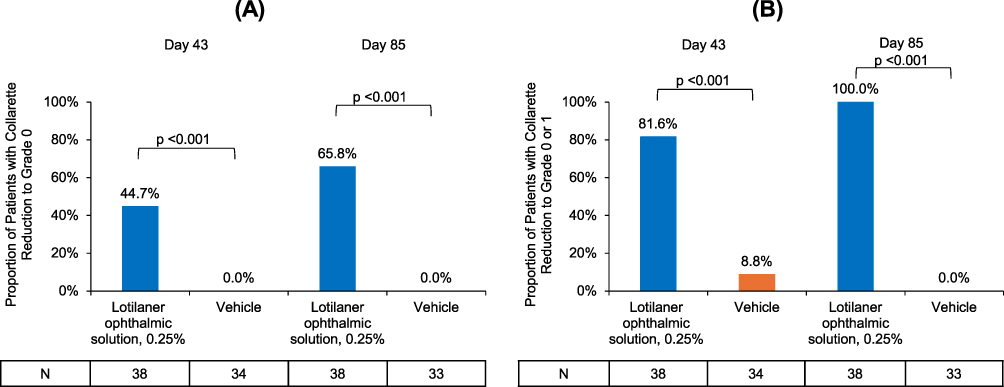 |
Figure 1 Proportion of patients showing collarette reduction to (A) grade 0 and (B) grade 0 or 1 in the lotilaner treatment group versus the vehicle group. |
Meibomian Gland Function
On Days 43 and 85, the lotilaner treatment group demonstrated statistically significantly higher mean MGSS compared to baseline. The between-group comparison showed statistically significantly better mean MGSS in the lotilaner treatment group than in the vehicle group (Figure 2).
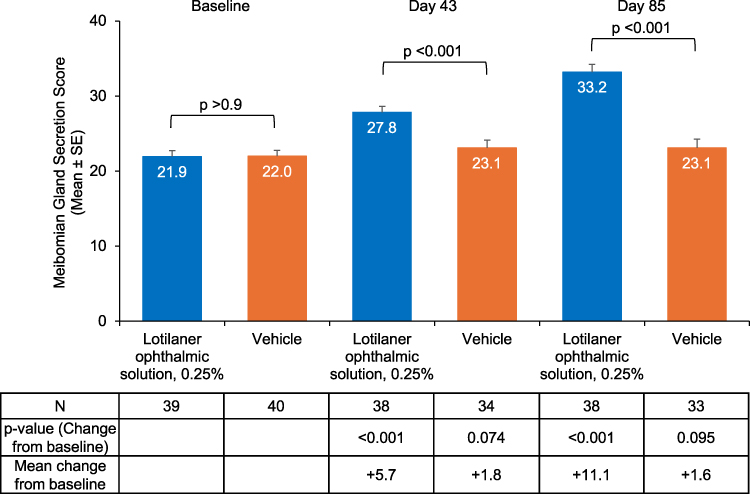 |
Figure 2 Mean meibomian gland secretion score (MGSS) at baseline, Day 43 and Day 85 in the lotilaner treatment group versus the vehicle group. |
The mean MGYLS (grade 2 or 3) in the lotilaner group was statistically significantly higher on post-treatment Days 43 and 85 than at baseline. The between-group comparison showed a statistically significantly higher mean MGYLS in the lotilaner group compared to the vehicle group (Figure 3).
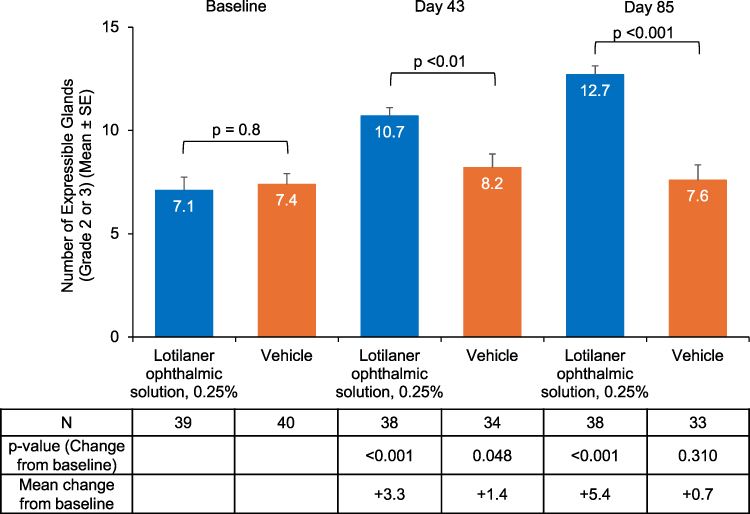 |
Figure 3 Mean number of meibomian glands yielding any liquid secretions (MGYLS) (grade 2 or 3) at baseline, Day 43 and Day 85 in the lotilaner treatment group versus the vehicle group. |
The lotilaner treatment group achieved a statistically significantly higher mean MGYCLS (grade 3) than the vehicle group on Day 43 (p <0.01) and Day 85 (p <0.001) (Figure 4). Correspondingly, the proportion of patients achieving improvement to at least 3 glands (at least 20% of the examined 15 glands) with clear meibum (grade 3) was significantly higher in the lotilaner group than in the vehicle group on Days 43 and 85 (Figure 5).
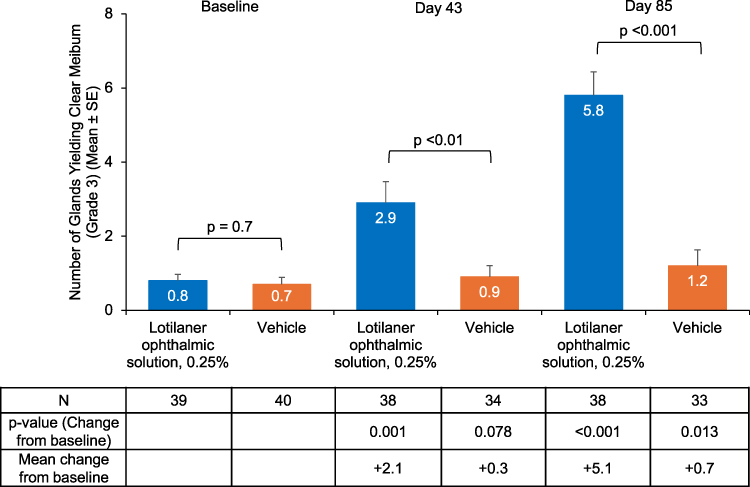 |
Figure 4 Mean number of meibomian glands yielding clear liquid secretions (MGYCLS) (grade 3) at baseline, Day 43 and Day 85 in the lotilaner treatment group versus the vehicle group. |
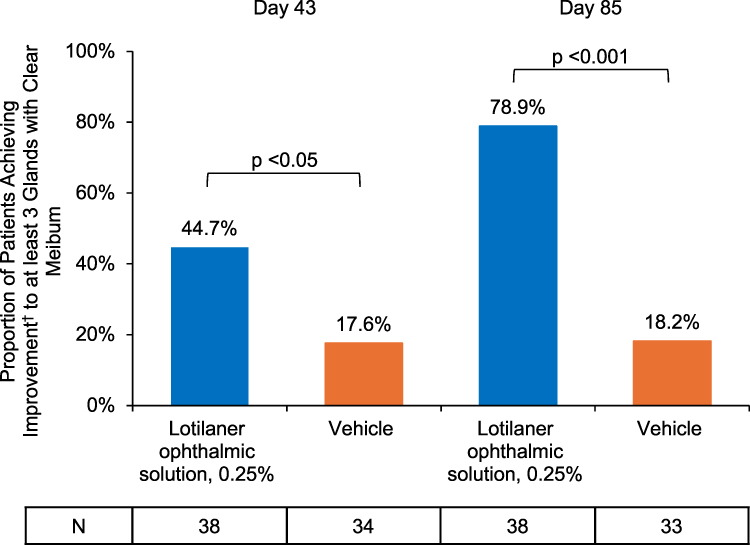 |
Figure 5 Proportion of patients achieving improvement to at least 3 glands with clear meibum at Day 43 and Day 85 in the lotilaner treatment group versus the vehicle group. Note: †denotes improvement from baseline. |
Patient-Reported Outcomes
The mean VAS score in the lotilaner group was statistically significantly lower (better) on Days 43 and 85 from baseline for all patient-reported outcomes (fluctuating vision, itching, burning, and redness). The lotilaner group also showed lower VAS scores when compared to the vehicle group on Days 43 and 85 for all patient-reported outcomes (Figure 6A–D).
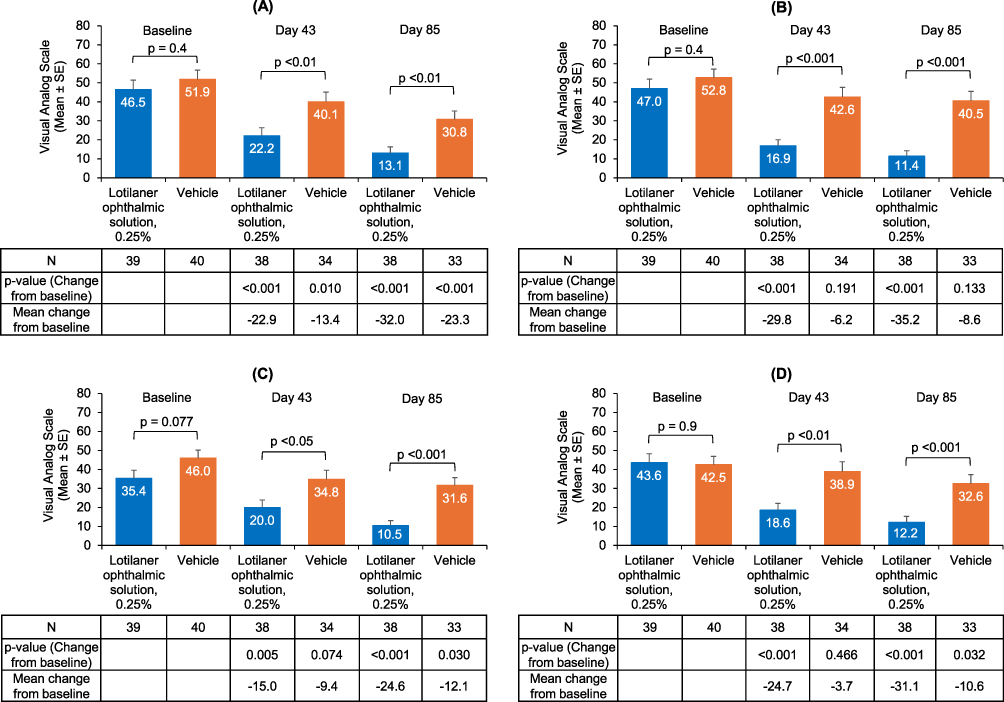 |
Figure 6 Patient-reported outcomes based on Visual Analog Scale (VAS score ranging from 0 to 100) at baseline, Day 43 and Day 85 in the lotilaner treatment group versus the vehicle group, (A) Fluctuating vision, (B) Itching, (C) Burning, and (D) Redness. |
Safety and Tolerability
Two patients (5.1%) in the lotilaner group and 7 patients (17.5%) in the vehicle group reported treatment-related ocular adverse events (AEs) (Table 2). No serious treatment-related AEs were observed. No AEs led to discontinuation from treatment or discontinuation from the study in the lotilaner group.
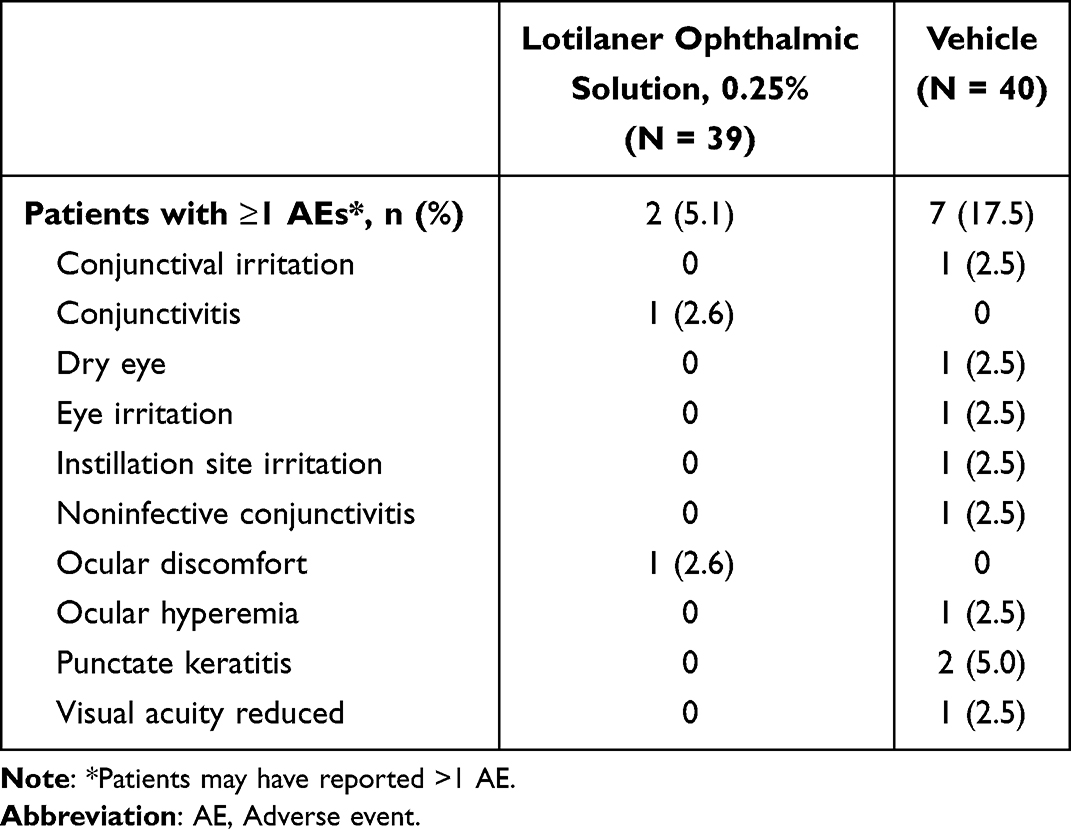 |
Table 2 Treatment-Related Ocular Adverse Events in the Lotilaner and the Vehicle Groups |
Discussion
Several previous studies have documented that Demodex mites play a pathogenic role in the development of meibomian gland disease.7,10,33–36 Compared to Demodex-negative meibomian gland disease patients, Demodex-positive meibomian gland disease patients are reported to have significantly worse meibum quality, meibomian gland expression, plugging of meibomian gland orifices, lid margin abnormality, and meibomian gland dropout.35 Such literature-reported findings suggest that it is important to pay attention to the diagnosis and treatment of Demodex infestation in meibomian gland disease.
Lotilaner ophthalmic solution, 0.25% is the first FDA-approved drug to target Demodex mites, the root cause of Demodex blepharitis.37 In previous lotilaner clinical trials, a 6-week BID treatment regimen was followed, yielding significant reductions in collarettes and mite eradication.27,30–32 In the present study, the treatment period was extended to 12 weeks with the dosing frequency of BID or TID. This extension of the treatment regimen was based on the hypothesis that concomitant lid margin diseases could prove more resistant to treatment and require a longer duration of therapy. Additionally, there may be multiple pathogenic mechanisms by which Demodex infestation influences meibomian gland disease, including inflammatory, bacterial, and mechanical effects.7,33,38–40
In the present study, we observed good improvement up to 6 weeks, and continued improvement in MGSS (the meibomian gland secretion score), MGYLS (the number of glands yielding any liquid secretions), MGYCLS (the number of meibomian glands yielding clear liquid secretions), and patient-reported VAS outcomes at 12 weeks. There were no statistically significant differences based on dosing frequency in either the lotilaner or vehicle arm, suggesting that more frequent dosing does not have much impact.
The quality and quantity of meibomian gland secretions are critical for ocular surface health. In the lotilaner-treated group, significant improvements from baseline were observed in the total MGSS and the number of glands yielding any liquid (MGYLS). Also, the statistically significant difference between groups on Day 43 and Day 85 points to the efficacy of lotilaner treatment in Demodex blepharitis patients with meibomian gland disease. Of note, compared to baseline, the lotilaner group exhibited a 50.7% improvement from baseline in MGYLS on Day 43 and 78.9% on Day 85. Correspondingly, in the lotilaner group, the percentage of patients achieving improvement to ≥3 glands (20% of the examined 15 glands) with clear meibum (MGYCLS) was 44.7% (17/38) on Day 43 and 78.9% (30/38) on Day 85.
Restoration of meibomian gland function may lead to a reduction in the symptoms of meibomian gland disease, and thus improved patient-reported outcomes. On Days 43 and 85, the lotilaner group demonstrated a statistically significant decrease from baseline in the mean VAS score for fluctuating vision, itching, burning, and redness. Additionally, the mean VAS scores for all four of these measures were significantly lower in the lotilaner group compared to the vehicle group at both time points post-treatment, which is clinically meaningful.41 Fluctuating vision, a hallmark symptom of meibomian gland disease, is known to interfere with quality of life, work performance, productivity, and other daily activities.1,42,43 Moreover, in patients with ocular surface disease and fluctuating vision, preoperative measurements can often be erroneous and may negatively impact patient satisfaction post-cataract surgery.44 Itch has been identified not only as highly characteristic of Demodex blepharitis, but also one of its most bothersome symptoms for patients.45–49 Ocular redness, which can occur in various lid margin and ocular surface diseases, is also highly bothersome and has a number of psychosocial impacts because it is noticeable to others.48 The improvements observed in the patient-reported outcomes in the present study support the efficacy of lotilaner treatment in patients with Demodex blepharitis and meibomian gland disease.
Lotilaner ophthalmic solution, 0.25% and its vehicle have been shown to be well-tolerated eye drops.27–32 Regular use of any comfortable eye drop might be expected to relieve ocular irritation in meibomian gland disease. By comparing lotilaner-treated patients to vehicle-treated patients, the present study can help to distinguish between the effects of lotilaner ophthalmic solution, 0.25% and its vehicle.
Demodex blepharitis patients with meibomian gland disease represent an important sub-population for further study. A recent paper showed that nearly all patients (96% to 99%) with moderate to severe Demodex blepharitis (collarette grades 2 to 4) were found to have either reduced meibum quality or meibomian gland atrophy suggestive of meibomian gland disease.11 Since Trattler et al previously reported the prevalence of Demodex blepharitis among meibomian gland disease patients to be 57.3%, it is recommended that patients with meibomian gland disease be evaluated for Demodex and vice versa.9
Although the sample size in this study was relatively small, this limitation is mitigated by highly statistically significant results. The patients included in the study all had Demodex blepharitis and meibomian gland disease that could be characterized as mild to moderate, an important stage for the treatment of meibomian gland disease prior to gland atrophy. Future studies in Demodex blepharitis patients with more severe meibomian gland disease and/or other ocular surface diseases could be beneficial, as could studies with longer follow-up. Additionally, there may be potential bias due to unobserved confounders. The results of the present study indicate that treatment with lotilaner ophthalmic solution, 0.25% is beneficial for Demodex blepharitis patients with concomitant meibomian gland disease.
Conclusion
To conclude, for patients presenting with Demodex blepharitis with meibomian gland disease, lotilaner ophthalmic solution, 0.25% demonstrated statistically significant improvements in measures of meibum quality, meibomian gland function, and patient-reported outcomes at 6 weeks and 12 weeks compared to baseline. Following lotilaner treatment, these parameters were also significantly improved when compared with vehicle. The drug was well tolerated with a similar safety profile as the vehicle group.
Abbreviations
MGSS, meibomian gland secretion score; MGYLS, number of glands yielding any liquid secretions; MGYCLS, number of glands yielding clear liquid secretions; FDA, Food and Drug Administration; IPL, intense pulsed light; TTO, tea tree oil; GABA, gamma-aminobutyric acid; TBUT, tear breakup time; VAS, visual analog scale; CDVA, corrected distance visual acuity; ETDRS, Early Treatment of Diabetic Retinopathy Study; BID, twice daily; TID, three times daily; AEs, adverse events; ITT, Intent-to-Treat; SD, standard deviation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Preeya K. Gupta) upon reasonable request.
Acknowledgments
The authors wish to thank Jan Beiting (Wordsmith Consulting) and Raman Bedi, MD (IrisARC - Analytics, Research & Consulting) for their assistance in preparing this manuscript. Funding for their services was provided by Tarsus Pharmaceuticals, Inc. The paper was presented at the 2025 ASCRS Annual Meeting, April 2025, Los Angeles, CA, USA, as a conference talk. The paper’s abstract is available at the ASCRS website [https://ascrs.confex.com/ascrs/25am/meetingapp.cgi/Paper/109380].
Funding
Funding for this study was provided by Tarsus Pharmaceuticals, Inc., Irvine, CA, USA. Tarsus Pharmaceuticals, Inc., had a role in the study design; analysis and interpretation of data; writing of the report; and the decision to submit the report for publication.
Disclosure
PKG, IBG: Consulting fees, Tarsus Pharmaceuticals, Inc. PKG reports personal fees from Alcon, Bausch + Lomb, Sight Sciences, Carl Zeiss Meditech, and Tissue Tech, outside the submitted work. IBG reports grants and/or personal fees from Bausch and Lomb, Alcon, Harrow, and Orasis, outside the submitted work. MCS, SMS, and BSL: Research and consulting fees, Tarsus Pharmaceuticals, Inc. BSL reports reports personal fees from Bausch & Lomb, Dompe, LENZ Therapeutics, Sun Pharmaceutical Industries, Inc, Tarsus Pharmaceuticals, Carl Zeiss Meditec, Inc, Johnson and Johnson Vision, SightGlass Vision, and Viatris Inc, outside the submitted work. PV: Speaking, research, and consulting fees, Tarsus Pharmaceuticals, Inc.; LO’D, KD, and EY: Employee, Tarsus Pharmaceuticals, Inc. The authors report no other conflicts of interest in this work.
References
1. Nichols KK. The international workshop on meibomian gland dysfunction: introduction. Invest Ophthalmol Vis Sci. 2011;52(4):1917–12. doi:10.1167/iovs.10-6997
2. McDonald M, Patel DA, Keith MS, Snedecor SJ. Economic and humanistic burden of dry eye disease in Europe, North America, and Asia: a systematic literature review. Ocul Surf. 2016;14(2):144–167. doi:10.1016/j.jtos.2015.11.002
3. Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379–387. doi:10.1097/ICO.0b013e3181f7f363
4. Chester T, Ferguson T, Chester E. Localized heat treatment for meibomian gland dysfunction: a single-center retrospective analysis of efficacy over time. Optom Vis Sci. 2023;100(9):625–630. doi:10.1097/OPX.0000000000002053
5. Luo X, Li J, Chen C, Tseng S, Liang L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;36(Suppl 1):S9–S14. doi:10.1097/ICO.0000000000001361
6. Bhandari V, Reddy JK. Blepharitis: always remember: demodex. Middle East Afr J Ophthalmol. 2014;21(4):317–320. doi:10.4103/0974-9233.142268
7. Cheng S, Zhang M, Chen H, Fan W, Huang Y. The correlation between the microstructure of meibomian glands and ocular Demodex infestation: a retrospective case-control study in a Chinese population. Medicine. 2019;98(19):e15595. doi:10.1097/MD.0000000000015595
8. Lim-Bon Siong R, de Venecia AB III. Demodex sp. infestation in anterior blepharitis, meibomian-gland dysfunction, and mixed blepharitis. Philipp J Ophthalmol. 2011;36:15–22.
9. Trattler W, Karpecki P, Rapoport Y, et al. The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign. Clin Ophthalmol. 2022;16:1153–1164. doi:10.2147/OPTH.S354692
10. Rabensteiner DF, Aminfar H, Boldin I, et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am J Ophthalmol. 2019;204:7–12. doi:10.1016/j.ajo.2019.03.007
11. Yeu E, Koetting C. Meibomian gland structure and function in patients with Demodex blepharitis. J Cataract Refract Surg. 2025;51(5):359–365. doi:10.1097/j.jcrs.0000000000001619
12. Gupta PK, Holland EJ, Hovanesian J, et al. TearCare for the treatment of meibomian gland dysfunction in adult patients with dry eye disease: a masked randomized controlled trial. Cornea. 2022;41(4):417–426. doi:10.1097/ICO.0000000000002837
13. Lane SS, DuBiner HB, Epstein RJ, et al. A new system, the lipiflow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396–404. doi:10.1097/ICO.0b013e318239aaea
14. Tauber J, Owen J, Bloomenstein M, Hovanesian J, Bullimore MA. Comparison of the iLUX and the lipiflow for the treatment of meibomian gland dysfunction and symptoms: a randomized clinical trial. Clin Ophthalmol. 2020;14:405–418. doi:10.2147/OPTH.S234008
15. Giannaccare G, Taroni L, Senni C, Scorcia V. Intense pulsed light therapy in the treatment of meibomian gland dysfunction: current perspectives. Clin Optom. 2019;11:113–126. doi:10.2147/OPTO.S217639
16. Park Y, Kim H, Kim S, Cho KJ. Effect of low-level light therapy in patients with dry eye: a prospective, randomized, observer-masked trial. Sci Rep. 2022;12(1):3575. doi:10.1038/s41598-022-07427-6
17. Moon SY, Han SA, Kwon HJ, et al. Effects of lid debris debridement combined with meibomian gland expression on the ocular surface MMP-9 levels and clinical outcomes in moderate and severe meibomian gland dysfunction. BMC Ophthalmol. 2021;21(1):175. doi:10.1186/s12886-021-01926-2
18. Filho PA, Hazarbassanov RM, Grisolia AB, Pazos HB, Kaiserman I, Gomes JA. The efficacy of oral ivermectin for the treatment of chronic blepharitis in patients tested positive for Demodex spp. Br J Ophthalmol. 2011;95(6):893–895. doi:10.1136/bjo.2010.201194
19. Fromstein SR, Harthan JS, Patel J, Opitz DL. Demodex blepharitis: clinical perspectives. Clin Optom. 2018;Volume 10:57–63. doi:10.2147/OPTO.S142708
20. Holzchuh FG, Hida RY, Moscovici BK, et al. Clinical treatment of ocular Demodex folliculorum by systemic ivermectin. Am J Ophthalmol. 2011;151(6):1030–1034e1031. doi:10.1016/j.ajo.2010.11.024
21. Messaoud R, El Fekih L, Mahmoud A, et al. Improvement in ocular symptoms and signs in patients with Demodex anterior blepharitis using a novel terpinen-4-ol (2.5%) and hyaluronic acid (0.2%) cleansing wipe. Clin Ophthalmol. 2019;13:1043–1054. doi:10.2147/OPTH.S198585
22. Salem DA, El-Shazly A, Nabih N, El-Bayoumy Y, Saleh S. Evaluation of the efficacy of oral ivermectin in comparison with ivermectin-metronidazole combined therapy in the treatment of ocular and skin lesions of Demodex folliculorum. Int J Infect Dis. 2013;17(5):e343–347. doi:10.1016/j.ijid.2012.11.022
23. Savla K, Le JT, Pucker AD. Tea tree oil for Demodex blepharitis. Cochrane Database Syst Rev. 2020;6(6):CD013333. doi:10.1002/14651858.CD013333.pub2
24. Zhang AC, Muntz A, Wang MTM, Craig JP, Downie LE. Ocular Demodex: a systematic review of the clinical literature. Ophthalmic Physiol Opt. 2020;40(4):389–432. doi:10.1111/opo.12691
25. Craig JP, Cruzat A, Cheung IMY, Watters GA, Wang MTM. Randomized masked trial of the clinical efficacy of MGO Manuka Honey microemulsion eye cream for the treatment of blepharitis. Ocul Surf. 2020;18(1):170–177. doi:10.1016/j.jtos.2019.11.009
26. Chen D, Wang J, Sullivan DA, Kam WR, Liu Y. Effects of terpinen-4-ol on meibomian gland epithelial cells in vitro. Cornea. 2020;39(12):1541–1546. doi:10.1097/ICO.0000000000002506
27. Gaddie IB, Donnenfeld ED, Karpecki P, et al. Lotilaner ophthalmic solution 0.25% for demodex blepharitis: randomized, vehicle-controlled, multicenter, phase 3 trial (Saturn-2). Ophthalmology. 2023;130(10):1015–1023. doi:10.1016/j.ophtha.2023.05.030
28. Gonzalez-Salinas R, Karpecki P, Yeu E, et al. Safety and efficacy of lotilaner ophthalmic solution, 0.25% for the treatment of blepharitis due to Demodex infestation: a randomized, controlled, double-masked clinical trial. Cont Lens Anterior Eye. 2022;45(4):101492. doi:10.1016/j.clae.2021.101492
29. Gonzalez-Salinas R, Yeu E, Holdbrook M, et al. Safety and efficacy of topical lotilaner ophthalmic solution 0.25% for the treatment of Demodex blepharitis: a pilot study. J Ophthalmol. 2021;2021:3862684. doi:10.1155/2021/3862684
30. Gonzalez-Salinas R, Yeu E, Holdbrook M, et al. Collarette elimination and Demodex mite eradication with topical lotilaner ophthalmic solution, 0.25. J Ocul Pharmacol Ther. 2021;37(8):479–484. doi:10.1089/jop.2021.0011
31. Yeu E, Holdbrook M, Baba SN, et al. Treatment of Demodex blepharitis: a prospective, randomized, controlled, double-masked clinical trial comparing topical lotilaner ophthalmic solution, 0.25% eyedrops to vehicle. Ocul Immunol Inflamm. 2023;31(8):1653–1661. doi:10.1080/09273948.2022.2093755
32. Yeu E, Wirta DL, Karpecki P, Baba SN, Holdbrook M, Saturn ISG. Lotilaner ophthalmic solution, 0.25%, for the treatment of Demodex blepharitis: results of a prospective, randomized, vehicle-controlled, double-masked, pivotal trial (Saturn-1). Cornea. 2023;42(4):435–443. doi:10.1097/ICO.0000000000003097
33. Gao H, Chen H, Xie H-T, Xu -K-K, Shi B-J, Huang Y-K. Changes in meibum lipid composition with ocular Demodex infestation. Transl Vis Sci Technol. 2021;10(14):6. doi:10.1167/tvst.10.14.6
34. Lee SH, Chun YS, Kim JH, Kim ES, Kim JC. The relationship between Demodex and ocular discomfort. Invest Ophthalmol Vis Sci. 2010;51(6):2906–2911. doi:10.1167/iovs.09-4850
35. Sun X, Liu Z, Sun S, Zhao S, Zhang X, Huang Y. The correlation between Demodex infestation and meibomian gland dysfunction at different ages. BMC Ophthalmol. 2022;22(1):388. doi:10.1186/s12886-022-02610-9
36. Zhang X-B, Ding Y-H, He W. The association between Demodex infestation and ocular surface manifestations in meibomian gland dysfunction. Int J Ophthalmol. 2018;11(4):589. doi:10.18240/ijo.2018.04.08
37. XDEMVY™ (lotilaner ophthalmic solution) 0.25%, for topical ophthalmic use. Prescribing information, initial U.S. Approval: 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217603s000lbl.pdf.
38. Liu J, Sheha H, Tseng SC. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10(5):505–510. doi:10.1097/ACI.0b013e32833df9f4
39. Rhee MK, Yeu E, Barnett M, et al. Demodex blepharitis: a comprehensive review of the disease, current management, and emerging therapies. Eye Contact Lens. 2023;49(8):311–318. doi:10.1097/ICL.0000000000001003
40. Chioveanu FG, Niculet E, Torlac C, Busila C, Tatu AL. Beyond the surface: understanding Demodex and its link to blepharitis and facial dermatoses. Clin Ophthalmol. 2024;18:1801–1810. doi:10.2147/OPTH.S440199
41. Papas EB, Keay L, Golebiowski B. Estimating a just-noticeable difference for ocular comfort in contact lens wearers. Invest Ophthalmol Vis Sci. 2011;52(7):4390–4394. doi:10.1167/iovs.10-7051
42. Tomlinson A, Bron AJ, Korb DR, et al. The international workshop on meibomian gland dysfunction: report of the diagnosis subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):2006–2049. doi:10.1167/iovs.10-6997f
43. Wei Z, Liang J, Cao K, et al. A multi-center study evaluating the correlation between meibomian gland dysfunction and depressive symptoms. Sci Rep. 2022;12(1):443. doi:10.1038/s41598-021-04167-x
44. Venkateswaran N, Luna RD, Gupta PK. Ocular surface optimization before cataract surgery. Saudi J Ophthalmol. 2022;36(2):142–148. doi:10.4103/sjopt.sjopt_190_21
45. Aumond S, Bitton E. Palpebral and facial skin infestation by Demodex folliculorum. Cont Lens Anterior Eye. 2020;43(2):115–122. doi:10.1016/j.clae.2019.09.001
46. Kabatas N, Dogan AS, Kabatas EU, Acar M, Bicer T, Gurdal C. The effect of Demodex infestation on blepharitis and the ocular symptoms. Eye Contact Lens. 2017;43(1):64–67. doi:10.1097/ICL.0000000000000234
47. Luo KS, Xie A, Yang JJ, Shen EP. Critical value of Demodex count per lash for symptomatic and clinical improvement of Demodex blepharitis. Eye. 2022;36(3):663–665. doi:10.1038/s41433-021-01442-z
48. O’Dell L, Dierker DS, Devries DK, et al. Psychosocial impact of Demodex blepharitis. Clin Ophthalmol. 2022;16:2979–2987. doi:10.2147/OPTH.S374530
49. Schachter S, Yeu E, Holdbrook MJ, Baba SN, Gomes PJ. Clinical manifestations of Demodex blepharitis. Invest Ophthalmol Vis Sci. 2021;62(8):1268.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.