Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Hypoglycemic Agents on The Musculoskeletal System: A Comprehensive Review
Authors Zhao J, Lv SS, Lu Q, Cong XX, Zhang XF
Received 14 January 2025
Accepted for publication 16 July 2025
Published 22 July 2025 Volume 2025:19 Pages 6235—6253
DOI https://doi.org/10.2147/DDDT.S517101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Jiao Zhao,1 Shan-shan Lv,2 Qi Lu,3 Xiao-xia Cong,4 Xian-feng Zhang1
1Department of Endocrinology, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Endocrinology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, Jiangsu, People’s Republic of China; 3Shanghai Clinical Research Center of Bone Disease, Department of Osteoporosis and Bone Disease, Shanghai Jiaotong University Affiliated Sixth People’s Hospital, Shanghai, People’s Republic of China; 4Institute for Translational Medicine, The Affiliated Hospital of Qingdao University, College of Medicine, Qingdao University, Qingdao, Shandong, People’s Republic of China
Correspondence: Xian-feng Zhang, Department of Endocrinology, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, No. 261, Huansha Road, Hangzhou, Zhejiang, 310000, People’s Republic of China, Email [email protected]
Abstract: Human life expectancy increases with social development, which poses problems related to rapid population ageing. As a common disease among the elderly, the prevention and control of diabetes is an ongoing challenge. Diabetes is associated with decreased bone mineral density, increased incidence of fractures, and decreased muscle strength. Meanwhile, the effects and mechanisms of different hypoglycemic drugs on musculoskeletal health vary. Currently, there are limited studies on the effects of anti-diabetic drugs on musculoskeletal health. However, it is necessary to take into account the effect of each hypoglycemic agent, alone or in combination, on musculoskeletal health when determining an individualized treatment approach. Medications that further negatively affect musculoskeletal health should be avoided in specific patients (eg thiazolidinediones and sodium-glucose cotransporter-2 inhibitors). At the same time, some hypoglycemic drugs can be used as potential targets for developing new therapies for osteoporosis/sarcopenia (eg metformin and glucagon-like peptide-1 receptor agonists). The aim of this review is to describe the effects and potential mechanisms of anti-diabetic drugs on musculoskeletal health, including metformin, insulin secretagogues, thiazolidinediones, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists, and sodium-glucose cotransporter-2 inhibitors. This review will contribute to the choice of appropriate hypoglycemic drugs to maintain musculoskeletal health in patients.
Keywords: hypoglycemic agents, diabetes, osteoporosis, sarcopenia, fracture, molecular mechanism
Introduction
Diabetes is a metabolic disease caused by genetic and environmental factors, which can lead to insulin insensitivity, insulin deficiency and impaired biological function. According to the Global Burden of Diseases, Injuries, and Risk Factors Study, diabetes is the eighth leading combined cause of death and disability worldwide.1 The prevalence of diabetes is rising globally, and its prevention and control remains an ongoing challenge. A growing body of research suggests that impaired musculoskeletal health is a common complication of diabetes, associated with poor prognosis and increased mortality.
Elevated fracture propensity in diabetic patients cannot be predicted by bone mineral density (BMD) measurements. Instead, elevated fracture risk is attributed to secondary defects in microarchitecture2 and bone tissue material properties.3 The results of skeletal biopsies from diabetic patients demonstrate low bone turnover, reduced osteoblast counts, and a significant reduction in the mineralized surface area of the bone cortex.4 In patients with diabetes, here is a reduction in serum concentrations of both osteocalcin and N-terminal propeptide of type 1 procollagen (P1NP). Concurrently, the volume of bone tissue mineralization is reduced and the rate of bone formation is decreased.5 Furthermore, it has been demonstrated that a state of prolonged hyperglycemia can result in the accumulation of advanced glycation end products (AGEs) within the bone tissue. This, in turn, has the potential to affect the processes of osteoblast differentiation and function, to reduce bone formation, and to increase the risk of fracture.6 Furthermore, it is widely acknowledged that dysregulated bioavailability of insulin-like growth factor 1 (IGF-1),7,8 insulin resistance, enhanced oxidative stress, altered bone mineral and vitamin D homeostasis,9 and regional diabetic microvascular disease have a detrimental effect on bone quality in diabetic patients.10
The mechanism of diabetic skeletal muscle injury is primarily the result of a combination of factors, including elevated glucose levels, insulin resistance, and abnormal release of inflammatory factors. Imbalanced glucose metabolism and excess circulating free fatty acids of diabetic patients have been demonstrated to impair phosphatidylinositol 3-kinase (PI3K)/Akt activity.11 The release of pro-inflammatory cytokines from diabetic patients increases the activity of inhibitor of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB)/NF-κB. At the downstream level, the inhibition of protein synthesis-promoting pathways such as mechanistic target of rapamycin (mTOR), and protein degradation-promoting pathways such as forkhead box O (FoxO)12 and ubiquitin-proteasome system,13,14 which ultimately result in muscle damage. Furthermore, the reduced oxidative capacity of diabetic muscle is closely related to impaired mitochondrial function. The sustained hypermetabolic condition has been demonstrated to augment the intracellular concentration of reactive oxygen species (ROS), resulting in mitochondrial dysfunction and the subsequent development of insulin resistance within skeletal muscle tissue, which further impairs glucolipid metabolic homeostasis.15
Apart from the impact of diabetes itself on the musculoskeletal system, the use of anti-diabetic medications also affects multiple aspects in diabetic patients, including BMD, muscle mass, fracture risk, and motility. In recent years, several guidelines have recommended that the heterogeneous characteristics of patients should be taken into account when developing a treatment plan for patients to individualize treatment. Given the close relationship between diabetes, osteoporosis, and sarcopenia, the effects of different anti-diabetic drugs on musculoskeletal health should be taken into account when developing treatment plans for patients. The aim of this review is to provide a comprehensive overview of the effects of diabetes medications on the musculoskeletal system, integrating current research to guide clinical practice and future studies.
Skeletal Effects of Hypoglycemic Agents
Insulin Sensitizers
Metformin
Clinical Studies
Zinman et al16 found reduced levels of alkaline phosphatase (ALP), P1NP and parathyroid hormone (PTH) in type 2 diabetes mellitus (T2DM) patients treated with metformin (1000mg twice daily) for 12 months. In addition, mildly elevated levels of C-terminal telopeptide of type 1 collagen (CTX) were also seen in female participants.16 In contrast, a study of male patients with T2DM revealed that treatment with metformin at a dosage of 1000 mg twice a day over a period of 24 weeks did not result in alterations in P1NP, CTX and sclerostin levels.17 Bilezikian et al18 found an increase in BMD in both the femoral neck and lumbar spine in postmenopausal women with T2DM treated with metformin (2000 mg total daily dose) for 52 weeks. In a case-control study by Vestergaard et al, metformin treatment was associated with a reduced risk of hip fracture in patients with T1DM and T2DM.19 Another historical cohort study involving 1964 patients with T2DM showed that metformin treatment reduced the risk of fracture after adjustment for other risk factors.20 However, some studies have reported a neutral effect of metformin on fracture risk. The clinical study conducted by Monami et al21 found no effect of metformin on fracture risk in T2DM patients who exposed to metformin for at least 36 months. A Scottish cohort study that included 200000 T2DM patients did not find a significant association between cumulative exposure to metformin and hip fracture incidence during a 9-year follow-up.22
Preclinical Studies
Kanazawa et al23 found that metformin induced the differentiation and maturation of osteoblasts through activation of the adenosine 5ʹ-monophosphate-activated protein kinase (AMPK) signaling pathway. In vitro studies have shown that metformin protected osteoblast function by increasing cell proliferation, ALP activity and calcium deposition, as well as inhibiting ROS formation and apoptosis.24 In addition to affecting bone formation, metformin can regulate bone resorption through the receptor activator of nuclear factor κB (RANK)/receptor activator of nuclear factor κB ligand (RANKL)/osteoprotegerin (OPG) pathway.25 In the ovariectomized (OVX) rat model, administration of 100 mg/kg metformin per day by oral intubation reduced the number of tartrate-resistant acid phosphatase (TRAP)-positive cells, elevated OPG and reduced RANKL, thereby increasing BMD.25 In diabetic male rats, the addition of metformin 100 mg/kg/day to drinking water for 2 weeks reduced TRAP activity, resulting in modest improvements in bone microarchitecture.26 On the contrary, some studies showed a neutral effect of metformin on bone metabolism. Wu et al reported that metformin did not affect the osteogenic differentiation of either human or rabbit bone marrow progenitor cells (BMPCs).27 Jeyabalan et al reported that, in female Wistar rats, there was no difference in bone structure or fracture healing ability between the rats with or without metformin (2 mg/mL) added to drinking water.28 Felice et al29 found no significant changes in bone mineral content (BMC), BMD or other trabecular or cortical bone parameters after 3 weeks of metformin (100 mg/kg/day) treatment in male rats.
Thiazolidinediones
Clinical Studies
Measurements of bone turnover markers in T2DM patients treated with thiazolidinediones (TZDs) revealed no differences in P1NP levels, decreases or increases in ALP, no differences or decreases in osteocalcin, and increases in sclerostin.16,18 However, the findings on the effect of TZDs on BMD were more consistent. A study by Schwartz et al reported that the use of TZDs (troglitazone, pioglitazone, and/or rosiglitazone) was associated with significant bone loss at multiple sites in older women aged 70–79 years with T2DM.30 In patients with T2DM, the fixed-dose combination if rosiglitazone/metformin significantly reduced BMD in the lumbar spine and total hip at week 80 of follow-up, compared with metformin monotherapy.31 The study by Home et al included 4447 T2DM patients who receiving metformin or sulfonylurea monotherapy and randomly assigned these patients to addition of rosiglitazone (8 mg per day) or to a combination of metformin and sulfonylurea.32 They found that the fracture rate was 57% higher in the rosiglitazone group than in the control group, with the fracture rate being approximately 82% higher in women and 23% higher in men.32 Kanazawa et al33 also reported that TZDs treatment was associated with vertebral fracture in postmenopausal women with T2DM, but had no effect on fracture risk in men with T2DM. Schwartz et al34 conducted a prospective study of 6868 patients treated with TZDs in the ACCORD study (rosiglitazone was used by 74% and pioglitazone by 13% of participants) and suggested that the effect of TZDs on fracture risk was reversible in female patients. The fracture risk of female patients taking TZDs for 1~2 years or >2 years was 2.32 and 2.01 times higher than in patients not taking TZDs, respectively.34 And female patients who discontinued TZDs for 1~2 years or >2 years had a 43% lower fracture risk than those who continued to take TZDs.34 In contrast, a meta-analysis by Billington et al suggested that bone loss due to TZDs may be irreversible up to 1 year after discontinuation.35
Preclinical Studies
The mechanism of action of TZDs on bone may be through the activation of peroxisome proliferator-activated receptor γ (PPARγ), and PPARγ can affect osteoblast-specific signaling pathways such as wingless-type MMTV integration site family (Wnt) and IGF-1.36 A recent study showed that rosiglitazone (0.14 mg of rosiglitazone per 1000 mg of food) impaired endochondral fracture healing in C57BL/6J mice by increasing adipogenesis and decreasing osteogenesis of both bone marrow- and periosteum-derived skeletal progenitor cells.37 Lecka-Czernik et al observed rosiglitazone affecting IGF-1 expression in vitro, in mice and in postmenopausal women.38 Several studies have shown TZDs could also affect the bone absorption, the number of osteoclasts and OPG expression.39 In OVX rats, 12 weeks of rosiglitazone treatment (10 mg/kg) was associated with an increase in adipose bone marrow volume, bone loss, and an increase in bone resorption parameters.40 Lazarenko et al observed a decrease in the BMD in adult (6 month) and old (24 month) C57BL/6 mice after administration of rosiglitazone (0.14 mg of rosiglitazone per 1000 mg of food), whereas there was no change in young mice (1 month).41 On the contrary, it has been shown that no significant negative effects on bone turnover markers or BMD were found after 8 weeks of low-dose pioglitazone treatment (3 mg/kg) in a diabetic rat model.42 The neutral effect of pioglitazone on bone may be due to the lower affinity of pioglitazone for PPARγ binding than rosiglitazone.
Insulin Secretagogues
Sulfonylureas
Clinical Studies
Kanazawa et al reported that sulfonylureas significantly reduced the incidence of vertebral fracture in postmenopausal women with T2DM.33 Vestergaard et al reported that sulfonylureas treatment was associated with a significantly lower risk of hip fracture in patients with diabetes compared to untreated patients.19 However, several other studies have reported neutral or negative effects of sulfonylureas on bone health. In a study that included 1945 patients with T2DM, there was no significant association between sulfonylurea treatment (including glibenclamide, gliclazide, glimepiride and other sulfonylureas) and fracture incidence.21 Moreover, a study by Colhoun et al found that hip fracture risk was not associated with long-term sulfonylureas therapy in both male and female T2DM patients.22 The data from the MrOS study showed that the use of sulfonylureas increased the risk of non-vertebral fractures by 66% in older men aged ≥65 years with T2DM.43 In a retrospective cohort study, Rajpathak et al reported that T2DM patients ≥65 years treated with sulfonylureas had a fracture risk that was approximately 46% higher than patients in the non-sulfonylureas group.44 Most studies concluded that sulfonylureas increase fracture risk primarily through elevated risk of falls, and not related to direct effects of the drugs on bone metabolism or BMD.45
Preclinical Studies
There are relatively few preclinical studies of the effects of insulin secretagogues agents on bone health. Glimepiride has been found to significantly enhance osteoblast proliferation and differentiation through activation of the PI3K/Akt pathway.46 Ma et al reported that glimepiride treatment (10 μmol/L) of primary osteoblasts enhanced the mRNA expression of runt-related transcription factor 2 (Runx2), osteocalcin and ALP, and significantly improve osteoblasts differentiation.47 Furthermore, in the OVX rats, glimepiride (0.8 mg/kg via stomach tube) promoted bone formation and inhibited estrogen deficiency-induced alterations in skeletal development.48 In the presence of estrogen (in un-OVX rats), glimepiride also promoted bone formation, but to a lesser extent.48
Glinides
Clinical Studies
Chen et al conducted a retrospective analysis of T2DM patients in Taiwan’s National Health Insurance claims database in from 2000 to 2010. They found that repaglinide increased the risk of fracture, particularly among older female patients aged 65 to 74 years, whereas nateglinide did not increase the risk of fracture in T2DM patients.49 In contrast, a network meta-analysis found that nateglinide was associated with a 35% increased risk of fracture in patients with T2DM.50 Another study of elderly T2DM patients aged 65 years or over found that glinides treatment was not associated with an increased risk of vertebral or hip fractures compared to metformin.51 Given that falls due to hypoglycemia are often cited as a cause of fractures with insulin secretagogues, we examined the risk of hypoglycemia with the glinides. Overall, glinides were associated with a lower probability and severity of hypoglycemia than sulfonylureas.52 Also, the risk of hypoglycemia was higher with repaglinide than with nateglinide. The probability of hypoglycemic symptoms was higher in the repaglinide group than in the nateglinide group in both studies (7% vs 0% and 17.2% vs 6.1%).53,54
Preclinical Studies
Few preclinical studies have been conducted on the effects of glinides on bone. A study by Viertel et al revealed when female rats were exposed to repaglinide (30 and 80 mg/kg) during late gestation and/or lactation, skeletal development of the limbs of offspring would be affected, with malformations of the scapula, proximal epiphysis of the humerus and femur.55
Incretins
Dipeptidyl Peptidase-4 Inhibitors
Clinical Studies
Dipeptidyl peptidase-4 (DPP-4) inhibitors have beneficial or neutral effects on bone health in diabetic patients. Sitagliptin (100 mg per day, for 12 weeks) was found to reduce ALP and urinary deoxypyridinoline levels in postmenopausal women with diabetes.56 In contrast, there were no significant changes in CTX or ALP levels after 1 year of treatment with vildagliptin (100 mg per day) in patients with T2DM.57 Gamble et al58 found that DPP-4 inhibitors did not increase the risk of fracture compared with sulfonylureas or insulin. A Korean study revealed no significant differences in the incidences of osteoporosis and osteoporotic fractures between DPP-4 inhibitors users and non-users in a T2DM population older than 50 years.59 In addition, subgroup analyses by gender and age showed consistent results. An analysis of patients aged 60 years and older found that the use of DPP-4 inhibitors (including sitagliptin, linagliptin, and vildagliptin) was negatively associated with the incidence of fractures.60 Another meta-analysis showed that DPP-4 inhibitors not only are safe for fracture in T2DM patients but also that the administration of 100 mg of sitagliptin per day may have protective effects on bone.61 Tsai et al showed that DPP-4 inhibitors had a neutral effect on fracture risk compared to placebo, but increased fracture risk compared to GLP-1 receptor agonists and sulfonylureas.62
Preclinical Studies
Studies on the effects of DPP-4 inhibitors on bone have yielded mixed results. Gallagher et al found that DPP-4 inhibitor MK-0626 (4 g/kg, supplemented chow) had a neutral effect on osteoblast differentiation, as well as trabecular and cortical bone mass in a male diabetic mouse model.63 Glorie et al reported that sitagliptin (2 g/L, dissolved in drinking water) reduced bone resorption markers, improved the reduction in trabecular number and increase in trabecular spacing in streptozotocin-induced diabetic male Wistar rats.64 Wang et al found that sitagliptin (10 mg/kg and 25mg/kg, daily intragastric administration for 4 weeks) applied to OVX mice could effectively reduce bone loss by inhibiting osteoclastogenesis and affecting osteoclast-specific transcription factors.65 DPP-4 inhibitors may increase the serum concentration of 25-hydroxyvitamin D3, thereby affecting fracture risk and BMD through vitamin D-related and other related signaling pathways.66 The accumulation of crosslinks to AGEs is thought to play an important role in diabetes-related osteoporosis, and vildagliptin was found to inhibit the formation and accumulation of AGEs.60 In the diabetic rat, vildagliptin (10 mg/kg/day for 5 weeks) reversed pioglitazone-induced bone loss, increased trabecular volume and BMD, and returned bone turnover markers to normal levels.67 However, a study by Sbaraglini et al found that saxagliptin (2 mg/kg/day, administered in drinking water for 3 weeks) reduced the number of metaphyseal osteoblasts and the mean height of the proximal cartilage growth plate in young male non-diabetic Sprague Dawley rats.68 Meanwhile, saxagliptin inhibited the osteogenic potential of bone marrow mesenchymal stem cells (BMSCs) in vitro.68
Glucagon-Like Peptide-1 Receptor Agonists
Clinical Studies
A clinical trial including 62 newly diagnosed T2DM patients found no significant change in BMD or bone turnover markers after 24 weeks of exenatide (10 μg injection, twice daily) treatment.69 In a group of healthy obese women with a body mass index of 34±0.5 kg/m2, treatment with liraglutide (1.2 mg/d for 52 weeks) increased levels of the bone formation marker P1NP and prevented bone loss.70 A cohort study including 216816 patients with T2DM revealed that no reduction in fracture risk in patients receiving glucagon-like peptide-1 receptor agonists (GLP-1RAs) compared with non-GLP-1RAs users.71 Su et al analyzed 16 randomized controlled trials including a total of 11206 patients and found on association between the use of GLP-1RAs and risk of fracture.72 However, a subgroup analysis showed that liraglutide significantly reduced fracture risk, whereas exenatide increased fracture risk.72 A meta-analysis of 39795 T2DM patients showed that treatment with liraglutide and lixisenatide significantly reduced the risk of fracture, whereas other GLP-1 RAs did not show superiority to placebo or other anti-diabetic drugs.73 In addition, these beneficial depend on the duration of GLP-1RAs treatment, with GLP-1RAs treatment for more than 52 weeks significantly reducing fracture risk in T2DM patients.73 The different molecular structures and pharmacokinetic characteristics of exenatide and liraglutide contribute be their differences in action. Liraglutide has 97% homology with GLP-1, and exenatide has only 50% homology with GLP-1.62
Preclinical Studies
It has been shown that GLP-1 analogs increase the expression of type 1 collagen, Runx2, ALP and osteocalcin in MC3T3E1 cells and prevent the differentiation of human BMPCs into adipocytes.74 In a study of type 2 diabetic male rats, the administration of subcutaneous injections of exenatide (5 nmol/kg) twice a day for a period of three weeks resulted in a reduction in sclerostin levels and an enhancement in femoral BMD. These findings suggest that GLP-1RAs may have the capacity to stimulate osteogenesis by modulating the Wnt signaling pathway.75 Eminov et al reported that treatment with exenatide (3μg/kg/day for 12 weeks) reversed significant decreases in BMD, trabecular number, trabecular thickness, and trabecular area in OVX rats.76 Recent studies have shown that liraglutide reduced RANKL-induced osteoclast differentiation, and this effect is mediated by the inhibition of the NF-κB and mitogen-activated protein kinase (MAPK) pathways via GLP-1 receptor.77 Treatment of female diabetic mice with liraglutide (0.6 mg/kg/day for 8 weeks) alone or in combination with insulin (liraglutide 0.6 mg/kg/day + insulin 10 units/kg/day for 8 weeks) significantly restored trabecular volumetric BMD and cortical volumetric BMD, and partially restored the trabecular microstructure of the tibia.78 In high-fat diet (HFD)-induced diabetic mice, administration of exenatide (25 nmol/kg twice daily for 52 days) significantly improved bone mechanical properties at the organ and tissue levels by altering cortical microarchitecture and bone compositional parameters.79 Meanwhile, in vitro studies have shown that liraglutide can activate PI3K/Akt and cyclic AMP/protein kinase A (cAMP/PKA) signaling, thereby promoting osteogenic differentiation and bone formation.80
Sodium-Glucose Cotransporter-2 Inhibitors
Clinical Studies
A study involving patients with inadequately controlled T2DM on metformin found that dapagliflozin (10 mg daily for 102 weeks) had no statistically significant effect on bone turnover markers as well as BMD.81 Bilezikian et al found that canagliflozin (100 mg or 300 mg daily) treatment reduced total hip BMD marginally, but had no effect on BMD of the femoral neck, spine, or radius in T2DM patients aged 55 to 80 years.82 Observational studies on sodium-glucose cotransporter-2 (SGLT-2) inhibitors-related fractures showed that the canagliflozin group (51.10%) had the highest incidence of fractures, followed by the dapagliflozin group (24.60%) and the empagliflozin group (23.66%).83 A meta-analysis evaluating the safety of canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin found that all four SGLT-2 inhibitors increased the risk of fractures.84 Ueda et al conducted a study on a matched cohort of new users of SGLT-2 inhibitors (dapagliflozin, 61%; empagliflozin, 38%; canagliflozin, 1%) and new users of GLP-1RAs. The study found that SGLT-2 inhibitors treatment did not increase fracture risk in comparison with GLP-1RAs treatment.85 A retrospective study of patients treated with SGLT-2 inhibitors (including canagliflozin, dapagliflozin, or empagliflozin) revealed a significant increase in fracture risk during the first 14 days of SGLT-2 inhibitors therapy in comparison with DPP-4 inhibitors treatment, and beyond this initial stage, SGLT-2 inhibitors had no significant effect on fracture incidence.86 Another retrospective cohort study by van Dalem et al demonstrated that high cumulative dose (≥6.30 g dapagliflozin equivalents) of SGLT-2 inhibitors increased the risk of major osteoporotic fracture compared with sulfonylureas, suggesting that the duration of SGLT-2 inhibitors treatment may be associated with fracture risk.87
Preclinical Studies
Some studies suggested that SGLT-2 inhibitors act on bone primarily through systemic metabolism and mineralization dysregulation, rather than directly at cellular and molecular levels.88 Taylor et al suggested that SGLT-2 inhibitors increased phosphate reabsorption in the proximal tubule, induced secretion of PTH and fibroblast growth factor 23, and ultimately stimulated bone resorption.89 In the study conducted by Yokono et al, male rats were administered ipragliflozin (10 mg/kg once daily) for a period of 4 weeks in an attempt to treat the obesity that was induced by HFD. The results of this study demonstrated that there was no reduction in lean body mass or BMD in the rats exposed to this treatment.90 The administration of canagliflozin (20 mg/kg/day for 10 weeks) partially, but not completely, ameliorated defects in trabecular bone structure and reduction in bone strength in TallyHO T2DM mice.91 Dapagliflozin (1 mg/kg/day for 28 days) improved bone tissue material properties, bone matrix strength, and matrix biomechanics (maximum load, indentation modulus, and hardness) in male diabetic mice.92 Song et al93 showed that canagliflozin, but not dapagliflozin or empagliflozin, increased BMD in mice with T2DM and improved bone microarchitecture. In addition, at high glucose concentrations, 5 mM canagliflozin promoted osteoblast differentiation; however, it is an inhibitor of MC3T3E1 proliferation at concentrations up to 10 mM.93
Muscle Effects of Hypoglycemic Agents
Insulin Sensitizers
Metformin
Clinical Studies
Weight loss is common in diabetic patients during metformin treatment, especially the reduction of fat mass (FM), but no significant change in fat free mass (FFM).94 A study of patients with newly diagnosed T2DM found an increase in lean-to-fat ratio in patients treated with metformin (1000 mg twice daily) for 6 months.94 A clinical study investigating the effects of metformin (1700 mg per day) in combination with a progressive resistance training (PRT) program in healthy older participants (aged ≥65 years) showed that individuals treated with metformin exhibited muscle hypertrophy, strength gains and maintenance of functional independence.95 However, another study showed that metformin administration (1700 mg per day) negatively impacts the hypertrophic response to PRT in healthy older individuals.96 In another similar study, treatment with metformin (1000mg twice daily) in healthy older adults who underwent 12 weeks of aerobic exercise training attenuated the expected improvement in maximal oxygen uptake and skeletal muscle mitochondrial respiration from aerobic training.97 In terms of physical function, a study including non-diabetic participants aged 60 years and older showed that walking speed was significantly higher in the metformin-treated group (1500 mg daily) than in the control group, but there were no differences in grip strength or myostatin level.98
Preclinical Studies
Lyu et al showed that metformin treatment for 5 months could prevent sarcopenia by inhibiting ectopic lipid deposition and the inflammatory response in skeletal muscle in an AMPK-dependent manner in sarcopenic mice.99 Oral metformin treatment (320 mg/day) ameliorated HFD-induced muscle atrophy in obese rats. Specifically, metformin treatment resulted in elevated peroxisome proliferator-activated receptor-γ coactivator 1α (PGC-1α) and decreased FoxO3, atrogin-1/muscle atrophy F-box (MAFbx) and muscle RING finger 1 (MuRF-1) in the soleus muscle of HFD-fed rats, which may be involved in PGC-1α-FoxO3 pathway regulation.100 In premature aging mice model, metformin (1 g/kg dry food for 10 weeks) ameliorated frailty in senescent mice, including muscle mass and physical function.101 However, some studies have shown that metformin is ineffective at restoring muscle mass and strength. One study showed that long-term administration (up to 8 weeks) of metformin did not alter the loss of muscle mass caused by overactivation of mechanistic target of rapamycin complex 1(mTORC1) in the fasted state in aged male mice (23 months of age).102 Consistent with the findings of the above study, another study showed that metformin administration for 6 weeks had a limited effect on restoring normal metabolism and growth signaling in adipose tissue and muscle in older mice (22 months of age).103 Wessels et al showed that both in healthy and diabetic rats, metformin (30, 100 or 300 mg/kg/day) treatment for 2 weeks impairs muscle oxidation in a dose-dependent manner.104
Thiazolidinediones
Clinical Studies
Sporadic case reports have reported the occurrence of pioglitazone or troglitazone induced acute rhabdomyolysis in T2DM patients.105 However, results on the effects of TZDs on muscle health are inconsistent. Lee et al have shown that treatment with TZDs significantly reduced muscle mass but did not affect walking speed in older women with diabetes.106 Yokota et al discovered that male patients suffering from metabolic syndrome experienced a substantial enhancement in skeletal muscle energy metabolism and whole-body aerobic capacity following a 4-month course of oral pioglitazone at a dosage of 15 mg per day.107 A clinical trial by Shea et al demonstrated that pioglitazone application (30mg/day) to an older (aged 65–79 years) nondiabetic obese male population resulted in subjects losing more thigh muscle volume.108 Marsh et al revealed that resistance training improves muscle strength in overweight elderly adults (aged 65–79 years), and pioglitazone (30mg/day for 13 weeks) enhances this effect in the women but not in men.109 Another study found that pioglitazone did not prevent skeletal muscle loss in older non-diabetic overweight or obese individuals on a weight loss program compared to resistance training.108 Bastien et al found that treatment with rosiglitazone (titrated to a maximal dose of 8 mg/day) significantly increased subcutaneous FM and decreased aerobic exercise capacity in male with T2DM and stable coronary artery disease.110
Preclinical Studies
Administration of rosiglitazone (8mg/kg/day) to male mice with spontaneous T2DM improved the insulin resistance index and abnormal PI3K/Akt signaling and inhibited FoxO3 and downstream atrogin-1/MAFbx and MuRF-1.111 It also reduced the activity of caspase-3 in muscle, thereby inhibiting protein degradation. Pioglitazone could inhibit oxidative stress, NF-κB signalling activation and inflammation in skeletal muscle, there by alleviating muscle atrophy in male mice with spinal cord and bulbar muscular atrophy.112 Furthermore, in vitro studies have shown that rosiglitazone reduced skeletal muscle cell apoptosis through a PPARγ-dependent mechanism.113 It has been reported that rosiglitazone can effectively inhibit the transcription of NF-κB induced by inflammatory mediators, thereby reducing protein degradation in the muscle ducts of cultured skeletal muscle.114 Moreover, TZDs can promote the processing and oxidation of fatty acids in skeletal muscle,115 reduce the triglyceride content in muscle cells, and prevent the development of fat cells in muscle fibers.116 However, pioglitazone (15 mg/kg/day for 15 days) alone or as an adjunct to exercise training failed to improve maximal aerobic speed, endurance and grip strength, and mitochondrial function in young (3 months old) non-diabetic mice.117
Insulin Secretagogues
Sulfonylureas
Clinical Studies
In many studies, sulfonylureas are comparative drugs, and it is difficult to analyze whether sulfonylureas are harmful or beneficial to muscle function. Several studies found patients taking sulfonylureas had a higher frequency of falls than those using other medications,118 but the above studies could not determine what proportion of the increase in fall frequency could be attributed to skeletal muscle dysfunction. According to the United States Food and Drug Administration Adverse Event Reporting System database, muscle atrophic events were significantly associated with the use of glibenclamide, but not with other sulfonylureas.119 Another study found that patients with T2DM who were treated with glimepiride (0.5 mg per day, titrated to 1.0 mg per day over 24 weeks) did not have any significant changes in FM, free bone mass (FBFM) or FBFM/FM.120
Preclinical Studies
Given the close relationship between ATP-sensitive K+ (KATP) channels and skeletal muscle function, the inhibitory effects of sulfonylureas and glinides on KATP channels increase the possibility that these drugs may have adverse effects on muscle health.121 Studies showed that the improvement of glucose uptake in skeletal muscle by gliclazide is associated with the increase of membrane content of glucose transporter 1.122 Glibenclamide (150 μM) has also been shown to increase fatigue slow muscle tone in mice and chickens in vitro, through direct effect on skeletal muscle KATP channels.123 Tricarico et al investigated the involvement of KATP channels and glibenclamide in the atrophy of slow-twitch and fast-twitch muscles in vitro in drug-induced muscle atrophy and in vivo in 14-day-hindlimb-unloaded rats. They revealed that glibenclamide enhanced caspase-3 activity in slow-twitch muscle and decreased the ratio of protein concentration to muscle weight.124
Glinides
Clinical Studies
According to a study by Mele et al in the United States Food and Drug Administration Adverse Event Reporting System database, muscle atrophy was not observed with repaglinide or nateglinide during the 8-month observation period.119 This difference between glibenclamide and glinides suggested that the drug-induced muscle atrophy may be associated with blockade of KATP channels and increased mitochondrial succinate dehydrogenase activity. However, there have been other studies suggesting a potential atrophic effect of the glinides (repaglinide and nateglinide), and should therefore be used with caution in diabetic patients.125
Preclinical Studies
KATP channels are also affected by the inhibitory effect of glinides, which may have a negative impact on muscle health.121 Mele et al assessed the effects of the insulin secretagogues on the protein content/muscle weight, fibers viability, mitochondrial succinic dehydrogenases activity and channel currents in different types of mice muscle fibers.119 Compared with those in the control group, the protein content/muscle weight were significantly decreased after incubated with sulfonylureas and glinides for 24 hours. Among them, repaglinide and glibenclamide enhanced mitochondrial succinate dehydrogenase activity in atrophic flexor digitorum brevis muscles, indicating that mitochondrial targets may be involved in the atrophy process.
Incretins
Dipeptidyl Peptidase-4 Inhibitors
Clinical Studies
An observational study showed that there were no significant differences in visceral fat area, subcutaneous fat area, and hepatic attenuation index between patients receiving DPP-4 inhibitors and non-DPP-4 inhibitors for T2DM, whereas the skeletal muscle index (SMI) was higher in patients in the DPP-4 inhibitors group.126 In a study that included elderly T2DM patients aged 65 years or older, those treated with DPP-4 inhibitors (vildagliptin 100 mg/day or sitagliptin 100 mg/day or saxagliptin 5 mg/day) had better muscle-generating parameters, including FFM, skeletal muscle mass (SMM), gait speed and muscle strength than those treated with sulfonylureas.127 A retrospective study showed that adding DPP-4 inhibitors to T2DM therapy improved muscle strength in older patients (mean age 72.6 ± 7.1).128 Ishii et al reported that after 24 weeks of sitagliptin treatment (25 mg titrated to 50 mg daily), SMM was significantly increased in overweight/obese T2DM patients.120 However, several studies have found that DPP-4 inhibitors could cause musculoskeletal adverse events such as myalgia, limb pain, muscle weakness, and joint pain.129 In addition, published case reports indicate that sitagliptin (100 mg/day), when used in combination with statins, is associated with rhabdomyolysis.130
Preclinical Studies
Sitagliptin (10 mg/kg/day) has been shown to increase glucose transporter 4 displacement and expression in the skeletal muscle in a rat model of T2DM.131 In the Klotho-/- mouse model of premature aging, treatment with linagliptin (0.083 g/kg diet) for 4 weeks slowed the progression of aging and improved weight loss and muscle mass loss.132 Bianchi et al reported that the vildagliptin analogue PKF275-055 (10 mg/kg for 5 weeks) partially ameliorated muscle damage in streptozotocin-induced diabetic rats, leading to an increase in body and muscle weight.133 In diabetic rats, sitagliptin dose-dependently upregulated circulating irisin and PGC-1α.134 In addition, DPP-4 inhibitors may inhibit apoptosis in muscle tissue by increasing glucose utilization and inhibiting the apoptosis of islet cells.135 However, high doses of DPP-4 inhibitors can cause acute toxicity in monkeys, particularly in crab-eating macaques, the use of high doses (160 mg/kg) of vildagliptin, could result in extremely high creatine kinase activity and limb skeletal muscle necrosis and intramuscular bleeding.136 The researchers noted, although, that this a phenomenon appears to be unique to monkeys, and it is uncertain whether the acute toxicity caused by vildagliptin will occur in humans.137
Glucagon-Like Peptide-1 Receptor Agonists
Clinical Studies
In overweight and obese elderly T2DM patients (mean age 68.2 ± 3.9 years), there was no muscle loss after 24 weeks of treatment with liraglutide (up to 3 mg per day).138 Li et al showed that in patients with T2DM, after 12 weeks of liraglutide treatment (1.2 mg once daily), there was a significant weight loss but a 2.3% increase in relative total body lean mass (LM), and this change was significantly associated with elevated plasma atrial and brain natriuretic peptide levels.139 Exenatide treatment (5 μg twice daily for 4 weeks then 10 μg twice daily for 8 weeks) significantly increased irisin in obese patients with T2DM, and the upregulation of irisin might be a novel mechanism for the beneficial effects of exenatide in T2DM patients.140 However, there are also studies that have shown that GLP-1RAs did not have a significant effect on skeletal muscle mass. Rondanelli et al found that the change in SMM after 24 weeks of liraglutide (up to 3 mg/d) application in overweight and obese T2DM patients was not significant.141 A randomized clinical trial that included patients with heart failure found no difference in 6-minute walk distance between the liraglutide group (1.8 mg/d) and the placebo group after 6 months of treatment.142 Another study showed that application of liraglutide in patients with T2DM did not lead to a significant improvement in maximal oxygen uptake, cycle ergometry time and 6-minute walk distance.143
Preclinical Studies
GLP-1RAs improves muscle mass and muscle function in a variety of skeletal muscle atrophy model animals.88,144 In vitro studies have shown that exenatide and liraglutide could promote glucose uptake in skeletal muscle in L6 myotubes in an insulin-independent manner by activating AMPK.145 Hong et al reported that exenatide inhibited the expression of myostatin and muscular atrophic factors (atrogin-1 and MuRF-1) and promoted the expression of myogenic factors (MyoG and MyoD).146 This effect is associated with the activation of the PKA and Akt signaling pathways after GLP-1 receptor activation and the inhibition of phosphorylated NF-κB protein expression.146 In the HFD rat model, liraglutide (200 μg/kg twice daily for 4 weeks) could improve skeletal muscle capillary density and endothelial function by increasing expression of vascular endothelial growth factor and phosphorylation of AMPK.147 Ren et al revealed that treatment of HFD-fed mice with semaglutide (30 nmol/kg/day) resulted in a significant increase in relative muscle mass, muscle protein synthesis, and muscle function, possibly by altering the metabolism of muscle lipids and organic acids.148 A similar study also demonstrated that liraglutide (400 μg/kg/d) and semaglutide (60 μg/kg/d) reduced weight gain, excess lipid accumulation, and muscle atrophy in HFD-fed mice, eliminated increases in muscle atrophy markers in skeletal muscle and C2C12 cells, and found that the protective effect of these drugs on skeletal muscle is by affecting the sirtuin1 pathway.149
Sodium-Glucose Cotransporter-2 Inhibitors
Clinical Studies
A study by Nagai et al demonstrated a significant decrease in both FM and LM in T2DM patients treated with 24 weeks of ipragliflozin (50 mg/day).150 Similarly, overweight T2DM patients treated with luseogliflozin (up to 5 mg daily) for 12 weeks showed a reduction in FM and SMM.151 A study conducted in Japan showed that obese patients with T2DM treated with tofogliflozin (20 mg/day) for 12 weeks had significantly lower SMI for both men and women.152 Yamakage et al showed that compared with T2DM patients received non-SGLT-2 inhibitors treatment, those treated with dapagliflozin (5 mg/day for 24 weeks) had lower myostatin levels, with no difference in SMM.153 There are few studies on the relationship between SGLT-2 and muscle strength. Sano et al showed that T2DM patients treated with SGLT-2 inhibitors (ipragliflozin 50 mg, luseogliflozin 2.5 mg, or dapagliflozin 5 or 10 mg daily) for 10 weeks had an increase in grip strength in both hands.154 A clinical study of elderly T2DM patients (mean age 74.1 years) revealed empagliflozin (10 mg daily) treatment for 52 weeks had no significant effect on muscle mass or grip strength.155
Preclinical Studies
Preclinical studies have shown complex effects of SGLT-2 inhibitors on muscle metabolism. Okamura et al reported that luseogliflozin (added 0.01% w/w in chow) could improve muscle atrophy in db/db mice and inhibit FoxO1 expression.156 Hata et al showed that db/db mice with dietary luseogliflozin (0.01% w/w in chow) had lower levels of gene expression of FoxO1, tripartite motif containing 63, atrogin-1, and histone deacetylase 4 than mice on a low-carbon diet, suggesting luseogliflozin had beneficial effects on muscle.157 Otsuka et al showed that canagliflozin (30 mg/kg) affected slow and fast muscles differently in non-diabetic mice, with FoxO1, atrogin-1, and MuRF-1 increased in slow muscles, while fast muscles were not affected.158 In addition, Tanaka et al showed that canagliflozin (0.03% of diet) combined with exercise training for 4 weeks enhanced the PI3K/Akt pathway in skeletal muscle and maintained skeletal muscle mass in HFD-induced obese mice.159 Another study similarly showed that hyperglycemia-induced overactivation of the c-Jun N-terminal kinase (JNK)/Smad2 signaling pathway could lead to poor exercise response in mice, whereas treatment with canagliflozin (30 mg/kg/day) could normalize this pathway.160 Nambu et al investigated the effects of empagliflozin (300 mg/kg of food) in mice with heart failure after myocardial infarction and found that the drug increased ketone body levels while improving their exercise tolerance, but did not improve spontaneous physical activity, skeletal muscle mass, or skeletal muscle strength.161 However, Lv et al showed that muscle regeneration and myoblast differentiation required increased mitochondrial leucyl tRNA synthetase (LARS2) expression, but canagliflozin reduced LARS2 expression in muscle stem cells, which negatively affected the recovery of ischemic skeletal muscle in mice.162
Conclusions
In this review, we point out how hypoglycemic drugs play an important role in influencing musculoskeletal health (Table 1 and Table 2) and their mechanisms of action (Figures 1 and 2). The musculoskeletal health of patients with diabetes is a frequently overlooked aspect of their health, and these patients are more susceptible to a range of adverse outcomes such as fractures, falls and reduced mobility due to the disease itself. At the same time, the use of antidiabetic medications has a differential impact on the presence of musculoskeletal health. Consequently, musculoskeletal effects need to be considered in addition to glycemic status when developing an individualized diabetes treatment plan. Drugs that further negatively affect musculoskeletal health (eg TZDs, SGLT-2 inhibitors) should be avoided in patients at high risk or in patients with osteoporosis/sarcopenia. At the same time, pharmaceuticals that can benefit musculoskeletal health in diabetic patients (eg metformin) can reduce the risk of osteoporosis or sarcopenia while controlling blood glucose. In the future, as combination therapies become more common in the management of diabetes, the potential of these approaches to affect musculoskeletal health in diabetes management will require careful and ongoing evaluation. Nevertheless, there is still a lack of definitive clinical data to guide the rational choice of antidiabetic drugs, with conflicting results from different studies, and a lack of research on muscle strength and physical function. Therefore, large cohort studies are needed to clarify the effects of hypoglycemic drugs on musculoskeletal health in order to guide clinical use.
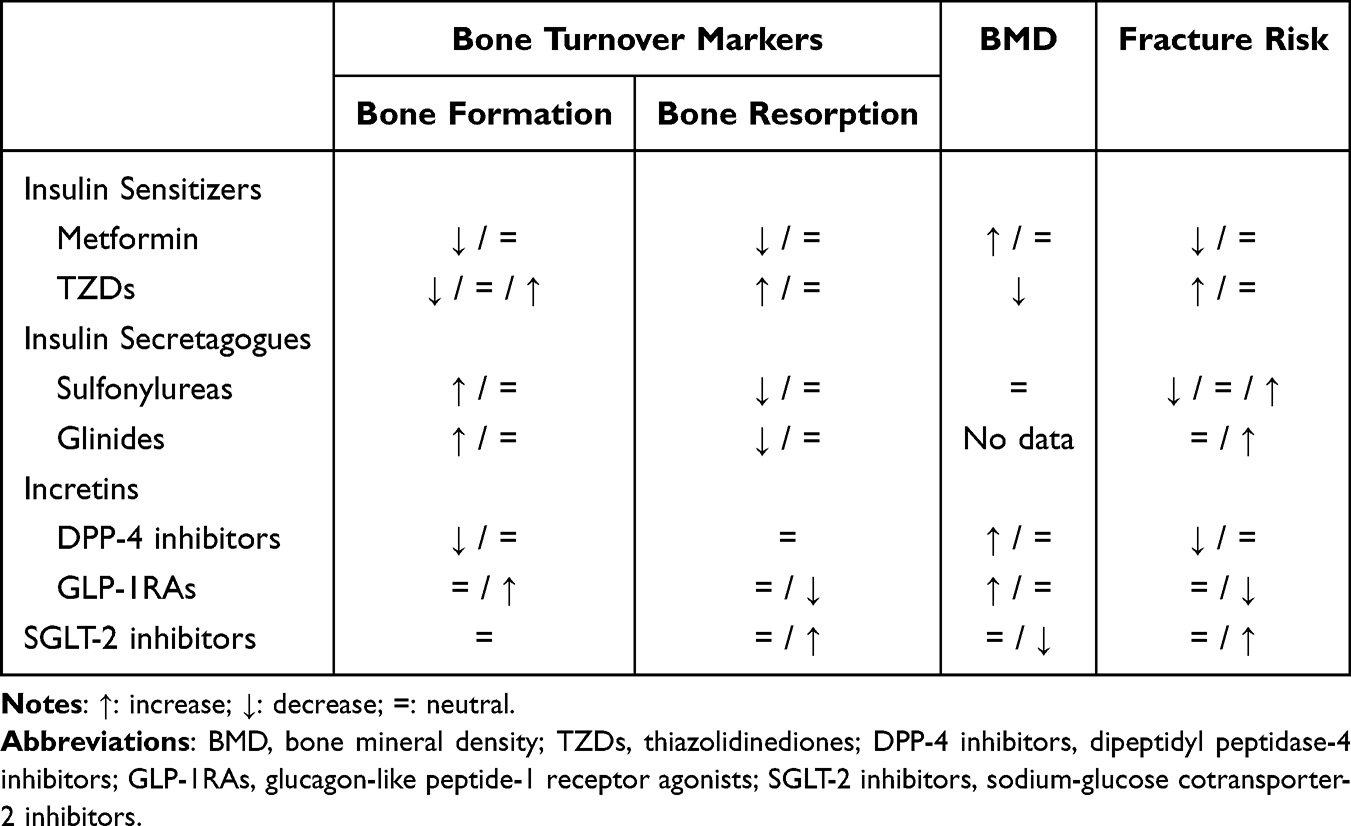 |
Table 1 Summary of Skeletal Effects of Hypoglycemic Agents: Clinical Evidences |
 |
Table 2 Summary of Muscle Effects of Hypoglycemic Agents: Clinical Evidences |
 |
Figure 1 Mechanisms by which hypoglycemic agents might impact skeleton health. ↑: increase; ↓: decrease. Green color indicates benefits for skeleton health; red color indicates harmful to skeleton health. Abbreviations: TZDs, thiazolidinediones; DPP-4 inhibitors, dipeptidyl peptidase-4 inhibitors; GLP-1RAs, glucagon-like peptide-1 receptor agonists; SGLT-2 inhibitors, sodium-glucose cotransporter-2 inhibitors; AMPK, adenosine 5-monophosphate-activated protein kinase; BMPCs, bone marrow progenitor cells; ROS, reactive oxygen species; RANKL, receptor activator of nuclear factor κB ligand; OPG, osteoprotegerin; GLP-1, glucagon-like peptide-1; GLP-2, glucagon-like peptide-2; GIP, glucose-dependent insulinotropic polypeptide; AGEs, advanced glycation end products; PTH, parathyroid hormone; FGF23, fibroblast growth factor 23; PI3K, phosphatidylinositol 3-kinase; BMSCs, bone marrow mesenchymal stem cells; PPARγ, peroxisome proliferator-activated receptor γ; IGF-1, insulin-like growth factor-1. |
 |
Figure 2 Mechanisms by which hypoglycemic agents might impact muscle health. ↑: increase; ↓: decrease. Green color indicates benefits for skeleton health; red color indicates harmful to muscle health. Abbreviations: TZDs, thiazolidinediones; DPP-4 inhibitors, dipeptidyl peptidase-4 inhibitors; GLP-1RAs, glucagon-like peptide-1 receptor agonists; SGLT-2 inhibitors, sodium-glucose cotransporter-2 inhibitors; ROS, reactive oxygen species; AMPK, adenosine 5-monophosphate-activated protein kinase; mTOR, mammalian target of rapamycin complex; PCG-1α, peroxisome proliferator-activated receptor-γ coactivator 1α; FoxO3, forkhead box O3; MuRF-1, muscle RING finger 1 MuRF-1; MAFbx, muscle atrophy F-box; GLUT4, glucose transporter 4; LARS2, mitochondrial leucyl tRNA synthetase; FoxO1, forkhead box O1; PI3K, phosphatidylinositol 3-kinase; KATP, ATP-sensitive K+; SIRT1, sirtuin1. |
Furthermore, the potential for some hypoglycemic drugs and the mechanisms by which they interact with the musculoskeletal system could be used as potential targets to develop new treatments for osteoporosis/sarcopenia is worthy of consideration (eg metformin, GLP-1RAs). There have been a number of preclinical studies using metformin in the treatment of osteoarthritis,163 diabetic periodontitis,164 and sarcopenia,165 demonstrating the potential of anti-diabetic medication in the treatment of musculoskeletal diseases. The majority of the extant studies relevant to this field have focused on patients with diabetes, and there is a need for future studies to target those without diabetes as well, including those with impaired glucose tolerance and those with normal glucose metabolism. Given the close links between musculoskeletal function, glucose and fat metabolism in health and disease, these marketed medications for diabetes deserve a more thorough review as potential avenues for the treatment of osteoporosis and sarcopenia.
With the increasing life expectancy of the population, more and more elderly people are suffering from a variety of age-related diseases at the same time, and the development of new uses of these existing drugs is expected to be a new treatment for the geriatric syndrome. This review will help clinicians select appropriate hypoglycemic medication to avoid further damage to the patient’s musculoskeletal system and even protect bone and muscle quality.
Abbreviations
BMD, bone mineral density; P1NP, N-terminal propeptide of type 1 procollagen; AGEs, advanced glycation end products; IGF-1, insulin-like growth factor 1; PI3K, phosphatidylinositol 3-kinase; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; mTOR, mechanistic target of rapamycin; FoxO, forkhead box O; ROS, reactive oxygen species; ALP, alkaline phosphatase; PTH, parathyroid hormone; CTX, C-terminal telopeptide of type 1 collagen; T2DM, type 2 diabetes mellitus; AMPK, adenosine 5-monophosphate-activated protein kinase; RANK, receptor activator of nuclear factor κB; RANKL, receptor activator of nuclear factor κB ligand; OPG, osteoprotegerin; OVX, ovariectomized; TRAP, tartrate-resistant acid phosphatase; BMPCs, bone marrow progenitor cells; BMC, bone mineral content; FM, fat mass; FFM, fat-free mass; PRT, progressive resistance training; HFD, high-fat diet; PGC-1α, peroxisome proliferator-activated receptor-γ coactivator 1α; MAFbx, muscle atrophy F-box; MuRF-1, muscle RING finger 1; mTORC1, mechanistic target of rapamycin complex 1; Runx2, runt-related transcription factor 2; KATP channels, ATP-sensitive K+ channels; FBFM, bone free mass; TZDs, thiazolidinediones; PPARγ, peroxisome proliferator-activated receptor γ; Wnt, wingless-type MMTV integration site family; DPP-4, dipeptidyl peptidase-4; AGEs, advanced glycation end products; BMSCs, bone marrow mesenchymal stem cells; SMI, skeletal muscle index; SMM, skeletal muscle mass; GLP-1RAs, glucagon-like peptide-1 receptor agonists; MAPK, mitogen-activated protein kinase; cAMP/PKA, cyclic AMP/protein kinase A; LM, lean mass; SGLT-2, sodium-glucose cotransporter-2; JNK, c-Jun N-terminal kinase; LARS2, mitochondrial leucyl tRNA synthetase.
Data Sharing Statement
The data supporting this review are from previously reported studies and datasets, which have been cited.
Funding
This research was funded by the National Natural Science Foundation of China (32100671), the Medical and Health Technology Project of Hangzhou (A20230111) and the Zhejiang Province Medical Health Science and Technology Plan Project (2025KY1063).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Collaborators GD. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–234. doi:10.1016/s0140-6736(23)01301-6
2. Burghardt AJ, Issever AS, Schwartz AV, et al. High-resolution peripheral quantitative computed tomographic imaging of cortical and trabecular bone microarchitecture in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab. 2010;95(11):5045–5055. doi:10.1210/jc.2010-0226
3. Farr JN, Drake MT, Amin S, Melton LJ, McCready LK, Khosla S. In vivo assessment of bone quality in postmenopausal women with type 2 diabetes. J Bone Miner Res. 2014;29(4):787–795. doi:10.1002/jbmr.2106
4. Manavalan JS, Cremers S, Dempster DW, et al. Circulating osteogenic precursor cells in type 2 diabetes mellitus. J Clin Endocrinol Metab. 2012;97(9):3240–3250. doi:10.1210/jc.2012-1546
5. Ardawi MS, Akhbar DH, Alshaikh A, et al. Increased serum sclerostin and decreased serum IGF-1 are associated with vertebral fractures among postmenopausal women with type-2 diabetes. Bone. 2013;56(2):355–362. doi:10.1016/j.bone.2013.06.029
6. Saito M, Marumo K. Collagen cross-links as a determinant of bone quality: a possible explanation for bone fragility in aging, osteoporosis, and diabetes mellitus. Osteoporosis Int. 2010;21(2):195–214. doi:10.1007/s00198-009-1066-z
7. Thrailkill KM. Insulin-like growth factor-I in diabetes mellitus: its physiology, metabolic effects, and potential clinical utility. Diabetes Technol Ther. 2000;2(1):69–80. doi:10.1089/152091599316775
8. Moyer-Mileur LJ, Slater H, Jordan KC, Murray MA. IGF-1 and IGF-binding proteins and bone mass, geometry, and strength: relation to metabolic control in adolescent girls with type 1 diabetes. J Bone Miner Res. 2008;23(12):1884–1891. doi:10.1359/jbmr.080713
9. Thrailkill KM, Fowlkes JL. The role of vitamin D in the metabolic homeostasis of diabetic bone. Clin Rev Bone Miner Metab. 2013;11(1):28–37. doi:10.1007/s12018-012-9127-9
10. Vehik K, Hamman RF, Lezotte D, et al. Increasing incidence of type 1 diabetes in 0- to 17-year-old Colorado youth. Diabetes Care. 2007;30(3):503–509. doi:10.2337/dc06-1837
11. Huang X, Liu G, Guo J, Su Z. The PI3K/AKT pathway in obesity and type 2 diabetes. Int J Bio Sci. 2018;14(11):1483–1496. doi:10.7150/ijbs.27173
12. Perry BD, Caldow MK, Brennan-Speranza TC, et al. Muscle atrophy in patients with type 2 diabetes mellitus: roles of inflammatory pathways, physical activity and exercise. Exerc Immunol Rev. 2016;22:94–109.
13. Zhang L, Pan J, Dong Y, et al. Stat3 activation links a C/EBPδ to myostatin pathway to stimulate loss of muscle mass. Cell Metab. 2013;18(3):368–379. doi:10.1016/j.cmet.2013.07.012
14. Sriwijitkamol A, Christ-Roberts C, Berria R, et al. Reduced skeletal muscle inhibitor of kappaB beta content is associated with insulin resistance in subjects with type 2 diabetes: reversal by exercise training. Diabetes. 2006;55(3):760–767. doi:10.2337/diabetes.55.03.06.db05-0677
15. Fiorentino TV, Monroy A, Kamath S, et al. Pioglitazone corrects dysregulation of skeletal muscle mitochondrial proteins involved in ATP synthesis in type 2 diabetes. Metabolism. 2021;114:154416. doi:10.1016/j.metabol.2020.154416
16. Zinman B, Haffner SM, Herman WH, et al. Effect of rosiglitazone, metformin, and glyburide on bone biomarkers in patients with type 2 diabetes. J Clin Endocrinol Metab. 2010;95(1):134–142. doi:10.1210/jc.2009-0572
17. van Lierop AH, Hamdy NA, van der Meer RW, et al. Distinct effects of pioglitazone and metformin on circulating sclerostin and biochemical markers of bone turnover in men with type 2 diabetes mellitus. Eur J Endocrinol. 2012;166(4):711–716. doi:10.1530/eje-11-1061
18. Bilezikian JP, Josse RG, Eastell R, et al. Rosiglitazone decreases bone mineral density and increases bone turnover in postmenopausal women with type 2 diabetes mellitus. J Clin Endocrinol Metab. 2013;98(4):1519–1528. doi:10.1210/jc.2012-4018
19. Vestergaard P, Rejnmark L, Mosekilde L. Relative fracture risk in patients with diabetes mellitus, and the impact of insulin and oral antidiabetic medication on relative fracture risk. Diabetologia. 2005;48(7):1292–1299. doi:10.1007/s00125-005-1786-3
20. Melton LJ, Leibson CL, Achenbach SJ, Therneau TM, Khosla S. Fracture risk in type 2 diabetes: update of a population-based study. J Bone Miner Res. 2008;23(8):1334–1342. doi:10.1359/jbmr.080323
21. Monami M, Cresci B, Colombini A, et al. Bone fractures and hypoglycemic treatment in type 2 diabetic patients: a case-control study. Diabetes Care. 2008;31(2):199–203. doi:10.2337/dc07-1736
22. Colhoun HM, Livingstone SJ, Looker HC, et al. Hospitalised Hip fracture risk with rosiglitazone and pioglitazone use compared with other glucose-lowering drugs. Diabetologia. 2012;55(11):2929–2937. doi:10.1007/s00125-012-2668-0
23. Kanazawa I, Yamaguchi T, Yano S, Yamauchi M, Sugimoto T. Metformin enhances the differentiation and mineralization of osteoblastic MC3T3-E1 cells via AMP kinase activation as well as eNOS and BMP-2 expression. Biochem Biophys Res Commun. 2008;375(3):414–419. doi:10.1016/j.bbrc.2008.08.034
24. Zhen D, Chen Y, Tang X. Metformin reverses the deleterious effects of high glucose on osteoblast function. J Diab Complications. 2010;24(5):334–344. doi:10.1016/j.jdiacomp.2009.05.002
25. Mai QG, Zhang ZM, Xu S, et al. Metformin stimulates osteoprotegerin and reduces RANKL expression in osteoblasts and ovariectomized rats. J Cell Biochem. 2011;112(10):2902–2909. doi:10.1002/jcb.23206
26. Tolosa MJ, Chuguransky SR, Sedlinsky C, et al. Insulin-deficient diabetes-induced bone microarchitecture alterations are associated with a decrease in the osteogenic potential of bone marrow progenitor cells: preventive effects of metformin. Diabetes Res Clin Pract. 2013;101(2):177–186. doi:10.1016/j.diabres.2013.05.016
27. Wu W, Ye Z, Zhou Y, Tan WS. AICAR, a small chemical molecule, primes osteogenic differentiation of adult mesenchymal stem cells. Int J Artif Organs. 2011;34(12):1128–1136. doi:10.5301/ijao.5000007
28. Jeyabalan J, Viollet B, Smitham P, et al. The anti-diabetic drug metformin does not affect bone mass in vivo or fracture healing. Osteoporosis Int. 2013;24(10):2659–2670. doi:10.1007/s00198-013-2371-0
29. Felice JI, Schurman L, McCarthy AD, Sedlinsky C, Aguirre JI, Cortizo AM. Effects of fructose-induced metabolic syndrome on rat skeletal cells and tissue, and their responses to metformin treatment. Diabetes Res Clin Pract. 2017;126:202–213. doi:10.1016/j.diabres.2017.02.011
30. Schwartz AV, Sellmeyer DE, Vittinghoff E, et al. Thiazolidinedione use and bone loss in older diabetic adults. J Clin Endocrinol Metab. 2006;91(9):3349–3354. doi:10.1210/jc.2005-2226
31. Borges JL, Bilezikian JP, Jones-Leone AR, et al. A randomized, parallel group, double-blind, multicentre study comparing the efficacy and safety of Avandamet (rosiglitazone/metformin) and metformin on long-term glycaemic control and bone mineral density after 80 weeks of treatment in drug-naïve type 2 diabetes mellitus patients. Diabetes Obesity Metab. 2011;13(11):1036–1046. doi:10.1111/j.1463-1326.2011.01461.x
32. Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet. 2009;373(9681):2125–2135. doi:10.1016/s0140-6736(09)60953-3
33. Kanazawa I, Yamaguchi T, Yamamoto M, Sugimoto T. Relationship between treatments with insulin and oral hypoglycemic agents versus the presence of vertebral fractures in type 2 diabetes mellitus. J Bone Miner Metab. 2010;28(5):554–560. doi:10.1007/s00774-010-0160-9
34. Schwartz AV, Chen H, Ambrosius WT, et al. Effects of TZD use and discontinuation on fracture rates in ACCORD bone study. J Clin Endocrinol Metab. 2015;100(11):4059–4066. doi:10.1210/jc.2015-1215
35. Billington EO, Grey A, Bolland MJ. The effect of thiazolidinediones on bone mineral density and bone turnover: systematic review and meta-analysis. Diabetologia. 2015;58(10):2238–2246. doi:10.1007/s00125-015-3660-2
36. Li Y, Jin D, Xie W, et al. PPAR-γ and wnt regulate the differentiation of MSCs into adipocytes and osteoblasts respectively. Curr Stem Cell Res Ther. 2018;13(3):185–192. doi:10.2174/1574888x12666171012141908
37. Mehta D, Dankert J, Yim N, Leclerc K, Leucht P. Rosiglitazone induces adipogenesis of both marrow and periosteum derived mesenchymal stem cells during endochondral fracture healing. J Orthop Sci. 2023;28(2):460–467. doi:10.1016/j.jos.2021.11.005
38. Lecka-Czernik B, Ackert-Bicknell C, Adamo ML, et al. Activation of peroxisome proliferator-activated receptor gamma (PPARgamma) by rosiglitazone suppresses components of the insulin-like growth factor regulatory system in vitro and in vivo. Endocrinology. 2007;148(2):903–911. doi:10.1210/en.2006-1121
39. Syversen U, Stunes AK, Gustafsson BI, et al. Different skeletal effects of the peroxisome proliferator activated receptor (PPAR)alpha agonist fenofibrate and the PPARgamma agonist pioglitazone. BMC Endocr Disord. 2009;9:10. doi:10.1186/1472-6823-9-10
40. Sottile V, Seuwen K, Kneissel M. Enhanced marrow adipogenesis and bone resorption in estrogen-deprived rats treated with the PPARgamma agonist BRL49653 (rosiglitazone). Calcif Tissue Int. 2004;75(4):329–337. doi:10.1007/s00223-004-0224-8
41. Lazarenko OP, Rzonca SO, Hogue WR, Swain FL, Suva LJ, Lecka-Czernik B. Rosiglitazone induces decreases in bone mass and strength that are reminiscent of aged bone. Endocrinology. 2007;148(6):2669–2680. doi:10.1210/en.2006-1587
42. Tsirella E, Mavrakanas T, Rager O, et al. Low dose pioglitazone does not affect bone formation and resorption markers or bone mineral density in streptozocin-induced diabetic rats. J Physiol Pharmacol. 2012;63(2):201–204.
43. Napoli N, Strotmeyer ES, Ensrud KE, et al. Fracture risk in diabetic elderly men: the MrOS study. Diabetologia. 2014;57(10):2057–2065. doi:10.1007/s00125-014-3289-6
44. Rajpathak SN, Fu C, Brodovicz KG, Engel SS, Lapane K. Sulfonylurea use and risk of Hip fractures among elderly men and women with type 2 diabetes. Drugs Aging. 2015;32(4):321–327. doi:10.1007/s40266-015-0254-0
45. Starup-Linde J, Gregersen S, Frost M, Vestergaard P. Use of glucose-lowering drugs and risk of fracture in patients with type 2 diabetes. Bone. 2017;95:136–142. doi:10.1016/j.bone.2016.11.026
46. Ma P, Gu B, Ma J, et al. Glimepiride induces proliferation and differentiation of rat osteoblasts via the PI3-kinase/Akt pathway. Metabolism. 2010;59(3):359–366. doi:10.1016/j.metabol.2009.08.003
47. Saura M, Tarin C, Zaragoza C. Recent insights into the implication of nitric oxide in osteoblast differentiation and proliferation during bone development. Sci World J. 2010;10:624–632. doi:10.1100/tsw.2010.58
48. Fronczek-Sokół J, Pytlik M. Effect of glimepiride on the skeletal system of ovariectomized and non-ovariectomized rats. Pharmacol Rep. 2014;66(3):412–417. doi:10.1016/j.pharep.2013.12.013
49. Chen HH, Horng MH, Yeh SY, et al. Glycemic control with thiazolidinedione is associated with fracture of T2DM patients. PLoS One. 2015;10(8):e0135530. doi:10.1371/journal.pone.0135530
50. Loke YK, Singh S, Furberg CD. Long-term use of thiazolidinediones and fractures in type 2 diabetes: a meta-analysis. CMAJ. 2009;180(1):32–39. doi:10.1503/cmaj.080486
51. Tamaki J, Ogawa S, Fujimori K, et al. Hip and vertebral fracture risk after initiating antidiabetic drugs in Japanese elderly: a nationwide study. J Bone Miner Metab. 2023;41(1):29–40. doi:10.1007/s00774-022-01372-0
52. Meneilly GS. Effect of repaglinide versus glyburide on postprandial glucose and insulin values in elderly patients with type 2 diabetes. Diabetes Technol Ther. 2011;13(1):63–65. doi:10.1089/dia.2010.0105
53. Kawamori R, Kaku K, Hanafusa T, Kashiwabara D, Kageyama S, Hotta N. Efficacy and safety of repaglinide vs nateglinide for treatment of Japanese patients with type 2 diabetes mellitus. J Diabetes Invest. 2012;3(3):302–308. doi:10.1111/j.2040-1124.2011.00188.x
54. Rosenstock J, Hassman DR, Madder RD, et al. Repaglinide versus nateglinide monotherapy: a randomized, multicenter study. Diabetes Care. 2004;27(6):1265–1270. doi:10.2337/diacare.27.6.1265
55. Viertel B, Güttner J. Effects of the oral antidiabetic repaglinide on the reproduction of rats. Arzneimittel-Forschung. 2000;50(5):425–440. doi:10.1055/s-0031-1300227
56. Hegazy SK. Evaluation of the anti-osteoporotic effects of metformin and sitagliptin in postmenopausal diabetic women. J Bone Miner Metab. 2015;33(2):207–212. doi:10.1007/s00774-014-0581-y
57. Bunck MC, Poelma M, Eekhoff EM, et al. Effects of vildagliptin on postprandial markers of bone resorption and calcium homeostasis in recently diagnosed, well-controlled type 2 diabetes patients. J Diabetes. 2012;4(2):181–185. doi:10.1111/j.1753-0407.2011.00168.x
58. Gamble JM, Donnan JR, Chibrikov E, Twells LK, Midodzi WK, Majumdar SR. The risk of fragility fractures in new users of dipeptidyl peptidase-4 inhibitors compared to sulfonylureas and other anti-diabetic drugs: a cohort study. Diabetes Res Clin Pract. 2018;136:159–167. doi:10.1016/j.diabres.2017.12.008
59. Ustulin M, Park SY, Choi H, Chon S, Woo JT, Rhee SY. Effect of dipeptidyl peptidase-4 inhibitors on the risk of bone fractures in a Korean population. J Korean Med Sci. 2019;34(35):e224. doi:10.3346/jkms.2019.34.e224
60. Ohyama K, Okamoto T, Hori Y. Inverse association between DPP-4 inhibitor use and fracture in older adults: a disproportionality analysis of the FAERS and JADER. Int J Clin Pharmacol Ther. 2023;61(1):16–23. doi:10.5414/cp204266
61. Kong QX, Ruan Q, Fan C, Liu BL, Reng LP, Xu W. Evaluation of the risk of fracture in type 2 diabetes mellitus patients with incretins: an updated meta-analysis. Endokrynol Pol. 2021;72(4):319–328. doi:10.5603/EP.a2021.0031
62. Tsai WH, Kong SK, Lin CL, et al. Risk of fracture caused by anti-diabetic drugs in individuals with type 2 diabetes: a network meta-analysis. Diabetes Res Clin Pract. 2022;192:110082. doi:10.1016/j.diabres.2022.110082
63. Gallagher EJ, Sun H, Kornhauser C, et al. The effect of dipeptidyl peptidase-IV inhibition on bone in a mouse model of type 2 diabetes. Diabetes/Metab Res Rev. 2014;30(3):191–200. doi:10.1002/dmrr.2466
64. Glorie L, Behets GJ, Baerts L, De Meester I, D’Haese PC, Verhulst A. DPP IV inhibitor treatment attenuates bone loss and improves mechanical bone strength in male diabetic rats. Am J Physiol Endocrinol Metab. 2014;307(5):E447–55. doi:10.1152/ajpendo.00217.2014
65. Wang C, Xiao F, Qu X, et al. Sitagliptin, an anti-diabetic drug, suppresses estrogen deficiency-induced osteoporosis in vivo and inhibits RANKL-induced osteoclast formation and bone resorption in vitro. Front Pharmacol. 2017;8:407. doi:10.3389/fphar.2017.00407
66. Barchetta I, Cimini FA, Bloise D, Cavallo MG. Dipeptidyl peptidase-4 inhibitors and bone metabolism: is vitamin D the link? Acta Diabetol. 2016;53(5):839–844. doi:10.1007/s00592-016-0882-9
67. Eom YS, Gwon AR, Kwak KM, et al. Protective effects of vildagliptin against pioglitazone-induced bone loss in type 2 diabetic rats. PLoS One. 2016;11(12):e0168569. doi:10.1371/journal.pone.0168569
68. Sbaraglini ML, Molinuevo MS, Sedlinsky C, Schurman L, McCarthy AD. Saxagliptin affects long-bone microarchitecture and decreases the osteogenic potential of bone marrow stromal cells. Eur J Pharmacol. 2014;727:8–14. doi:10.1016/j.ejphar.2014.01.028
69. Li R, Xu W, Luo S, et al. Effect of exenatide, insulin and pioglitazone on bone metabolism in patients with newly diagnosed type 2 diabetes. Acta Diabetol. 2015;52(6):1083–1091. doi:10.1007/s00592-015-0792-2
70. Iepsen EW, Lundgren JR, Hartmann B, et al. GLP-1 receptor agonist treatment increases bone formation and prevents bone loss in weight-reduced obese women. J Clin Endocrinol Metab. 2015;100(8):2909–2917. doi:10.1210/jc.2015-1176
71. Driessen JH, Henry RM, van Onzenoort HA, et al. Bone fracture risk is not associated with the use of glucagon-like peptide-1 receptor agonists: a population-based cohort analysis. Calcif Tissue Int. 2015;97(2):104–112. doi:10.1007/s00223-015-9993-5
72. Su B, Sheng H, Zhang M, et al. Risk of bone fractures associated with glucagon-like peptide-1 receptor agonists’ treatment: a meta-analysis of randomized controlled trials. Endocrine. 2015;48(1):107–115. doi:10.1007/s12020-014-0361-4
73. Cheng L, Hu Y, Li YY, et al. Glucagon-like peptide-1 receptor agonists and risk of bone fracture in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Diabetes/Metab Res Rev. 2019;35(7):e3168. doi:10.1002/dmrr.3168
74. Sanz C, Vázquez P, Blázquez C, Barrio PA, Alvarez Mdel M, Blázquez E. Signaling and biological effects of glucagon-like peptide 1 on the differentiation of mesenchymal stem cells from human bone marrow. Am J Physiol Endocrinol Metab. 2010;298(3):E634–43. doi:10.1152/ajpendo.00460.2009
75. Kim JY, Lee SK, Jo KJ, et al. Exendin-4 increases bone mineral density in type 2 diabetic OLETF rats potentially through the down-regulation of SOST/sclerostin in osteocytes. Life Sci. 2013;92(10):533–540. doi:10.1016/j.lfs.2013.01.001
76. Eminov E, Hortu I, Akman L, Erbas O, Yavasoglu A, Cirpan T. Exenatide preserves trabecular bone microarchitecture in experimental ovariectomized rat model. Arch Gynecol Obstetrics. 2018;297(6):1587–1593. doi:10.1007/s00404-018-4776-7
77. Li Z, Li S, Wang N, Xue P, Li Y. Liraglutide, a glucagon-like peptide-1 receptor agonist, suppresses osteoclastogenesis through the inhibition of NF-κB and MAPK pathways via GLP-1R. Biomed Pharmacother. 2020;130:110523. doi:10.1016/j.biopha.2020.110523
78. Yu J, Shi YC, Ping F, et al. Liraglutide inhibits osteoclastogenesis and improves bone loss by downregulating Trem2 in female type 1 diabetic mice: findings from transcriptomics. Front Endocrinol. 2021;12:763646. doi:10.3389/fendo.2021.763646
79. Mansur SA, Mieczkowska A, Flatt PR, Chappard D, Irwin N, Mabilleau G. The GLP-1 receptor agonist exenatide ameliorates bone composition and tissue material properties in high fat fed diabetic mice. Front Endocrinol. 2019;10:51. doi:10.3389/fendo.2019.00051
80. Wu X, Li S, Xue P, Li Y. Liraglutide, a glucagon-like peptide-1 receptor agonist, facilitates osteogenic proliferation and differentiation in MC3T3-E1 cells through phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT), extracellular signal-related kinase (ERK)1/2, and cAMP/protein kinase A (PKA) signaling pathways involving β-catenin. Exp Cell Res. 2017;360(2):281–291. doi:10.1016/j.yexcr.2017.09.018
81. Bolinder J, Ljunggren Ö, Johansson L, et al. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obesity Metab. 2014;16(2):159–169. doi:10.1111/dom.12189
82. Bilezikian JP, Watts NB, Usiskin K, et al. Evaluation of bone mineral density and bone biomarkers in patients with type 2 diabetes treated with canagliflozin. J Clin Endocrinol Metab. 2016;101(1):44–51. doi:10.1210/jc.2015-1860
83. Zhao B, Shen J, Zhao J, Pan H. Do sodium-glucose cotransporter 2 inhibitors lead to fracture risk? A pharmacovigilance real-world study. J Diabetes Invest. 2021;12(8):1400–1407. doi:10.1111/jdi.13481
84. Qiu M, Ding LL, Zhang M, Zhou HR. Safety of four SGLT2 inhibitors in three chronic diseases: a meta-analysis of large randomized trials of SGLT2 inhibitors. Diabetes Vasc Dis Res. 2021;18(2):14791641211011016. doi:10.1177/14791641211011016
85. Ueda P, Svanström H, Melbye M, et al. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: nationwide register based cohort study. BMJ. 2018;363:k4365. doi:10.1136/bmj.k4365
86. Adimadhyam S, Lee TA, Calip GS, Smith Marsh DE, Layden BT, Schumock GT. Sodium-glucose co-transporter 2 inhibitors and the risk of fractures: a propensity score-matched cohort study. Pharmacoepidemiol Drug Saf. 2019;28(12):1629–1639. doi:10.1002/pds.4900
87. van Dalem J, Werkman NCC, van den Bergh JP, et al. Use of sodium-glucose co-transporter 2 inhibitors, changes in body mass index and risk of fracture: a population-based cohort study. Diabetes Res Clin Pract. 2022;190:109993. doi:10.1016/j.diabres.2022.109993
88. Kalaitzoglou E, Fowlkes JL, Popescu I, Thrailkill KM. Diabetes pharmacotherapy and effects on the musculoskeletal system. Diabetes Metab Res Rev. 2019;35(2):e3100. doi:10.1002/dmrr.3100
89. Taylor SI, Blau JE, Rother KI. Possible adverse effects of SGLT2 inhibitors on bone. Lancet Diabetes Endocrinol. 2015;3(1):8–10. doi:10.1016/s2213-8587(14)70227-x
90. Yokono M, Takasu T, Hayashizaki Y, et al. SGLT2 selective inhibitor ipragliflozin reduces body fat mass by increasing fatty acid oxidation in high-fat diet-induced obese rats. Eur J Pharmacol. 2014;727:66–74. doi:10.1016/j.ejphar.2014.01.040
91. Thrailkill KM, Bunn RC, Uppuganti S, et al. Canagliflozin, an SGLT2 inhibitor, corrects glycemic dysregulation in TallyHO model of T2D but only partially prevents bone deficits. Bone. 2020;141:115625. doi:10.1016/j.bone.2020.115625
92. Mieczkowska A, Millar P, Chappard D, Gault VA, Mabilleau G. Dapagliflozin and liraglutide therapies rapidly enhanced bone material properties and matrix biomechanics at bone formation site in a type 2 diabetic mouse model. Calcif Tissue Int. 2020;107(3):281–293. doi:10.1007/s00223-020-00720-4
93. Song P, Chen T, Rui S, et al. Canagliflozin promotes osteoblastic MC3T3-E1 differentiation via AMPK/RUNX2 and improves bone microarchitecture in type 2 diabetic mice. Front Endocrinol. 2022;13:1081039. doi:10.3389/fendo.2022.1081039
94. Aghili R, Malek M, Valojerdi AE, Banazadeh Z, Najafi L, Khamseh ME. Body composition in adults with newly diagnosed type 2 diabetes: effects of metformin. J Diabetes Metab Disord. 2014;13(1):88. doi:10.1186/s40200-014-0088-z
95. Long DE, Peck BD, Martz JL, et al. Metformin to Augment Strength Training Effective Response in Seniors (MASTERS): study protocol for a randomized controlled trial. Trials. 2017;18(1):192. doi:10.1186/s13063-017-1932-5
96. Walton RG, Dungan CM, Long DE, et al. Metformin blunts muscle hypertrophy in response to progressive resistance exercise training in older adults: a randomized, double-blind, placebo-controlled, multicenter trial: the MASTERS trial. Aging Cell. 2019;18(6):e13039. doi:10.1111/acel.13039
97. Konopka AR, Laurin JL, Schoenberg HM, et al. Metformin inhibits mitochondrial adaptations to aerobic exercise training in older adults. Aging Cell. 2019;18(1):e12880. doi:10.1111/acel.12880
98. Laksmi PW, Setiati S, Tamin TZ, et al. Effect of metformin on handgrip strength, gait speed, myostatin serum level, and health-related quality of life: a double blind randomized controlled trial among non-diabetic pre-frail elderly patients. Acta Med Indones. 2017;49(2):118–127.
99. Lyu Q, Wen Y, He B, et al. The ameliorating effects of metformin on disarrangement ongoing in gastrocnemius muscle of sarcopenic and obese sarcopenic mice. Biochim Biophys Acta Mol Basis Dis. 2022;1868(11):166508. doi:10.1016/j.bbadis.2022.166508
100. Hasan MM, Shalaby SM, El-Gendy J, Abdelghany EMA. Beneficial effects of metformin on muscle atrophy induced by obesity in rats. J Cell Biochem. 2019;120(4):5677–5686. doi:10.1002/jcb.27852
101. Fielder E, Wan T, Alimohammadiha G, et al. Short senolytic or senostatic interventions rescue progression of radiation-induced frailty and premature ageing in mice. eLife. 2022;11:e75492. doi:10.7554/eLife.75492
102. Dungan CM, Li Z, Wright DC, Williamson DL. Hyperactive mTORC1 signaling is unaffected by metformin treatment in aged skeletal muscle. Muscl Nerv. 2016;53(1):107–117. doi:10.1002/mus.24698
103. Mennes E, Dungan CM, Frendo-Cumbo S, Williamson DL, Wright DC. Aging-associated reductions in lipolytic and mitochondrial proteins in mouse adipose tissue are not rescued by metformin treatment. J Gerontol A Biol Sci Med Sci. 2014;69(9):1060–1068. doi:10.1093/gerona/glt156
104. Wessels B, Ciapaite J, van den Broek NM, Nicolay K, Prompers JJ. Metformin impairs mitochondrial function in skeletal muscle of both lean and diabetic rats in a dose-dependent manner. PLoS One. 2014;9(6):e100525. doi:10.1371/journal.pone.0100525
105. Slim R, Ben salem C, Zamy M, Biour M. Pioglitazone-induced acute rhabdomyolysis. Diabetes Care. 2009;32(7):e84. doi:10.2337/dc09-0593
106. Lee CG, Schwartz AV, Yaffe K, Hillier TA, LeBlanc ES, Cawthon PM. Changes in physical performance in older women according to presence and treatment of diabetes mellitus. J Am Geriatr Soc. 2013;61(11):1872–1878. doi:10.1111/jgs.12502
107. Yokota T, Kinugawa S, Hirabayashi K, et al. Pioglitazone improves whole-body aerobic capacity and skeletal muscle energy metabolism in patients with metabolic syndrome. J Diabetes Invest. 2017;8(4):535–541. doi:10.1111/jdi.12606
108. Shea MK, Nicklas BJ, Marsh AP, et al. The effect of pioglitazone and resistance training on body composition in older men and women undergoing hypocaloric weight loss. Obesity. 2011;19(8):1636–1646. doi:10.1038/oby.2010.327
109. Marsh AP, Shea MK, Vance Locke RM, et al. Resistance training and pioglitazone lead to improvements in muscle power during voluntary weight loss in older adults. J Gerontol a Biol Sci Med Sci. 2013;68(7):828–836. doi:10.1093/gerona/gls258
110. Bastien M, Poirier P, Brassard P, et al. Effect of PPARγ agonist on aerobic exercise capacity in relation to body fat distribution in men with type 2 diabetes mellitus and coronary artery disease: a 1-yr randomized study. Am J Physiol Endocrinol Metab. 2019;317(1):E65–e73. doi:10.1152/ajpendo.00505.2018
111. Wang X, Hu Z, Hu J, Du J, Mitch WE. Insulin resistance accelerates muscle protein degradation: activation of the ubiquitin-proteasome pathway by defects in muscle cell signaling. Endocrinology. 2006;147(9):4160–4168. doi:10.1210/en.2006-0251
112. Iida M, Katsuno M, Nakatsuji H, et al. Pioglitazone suppresses neuronal and muscular degeneration caused by polyglutamine-expanded androgen receptors. Hum Mol Genet. 2015;24(2):314–329. doi:10.1093/hmg/ddu445
113. Meshkani R, Sadeghi A, Taheripak G, Zarghooni M, Gerayesh-Nejad S, Bakhtiyari S. Rosiglitazone, a PPARγ agonist, ameliorates palmitate-induced insulin resistance and apoptosis in skeletal muscle cells. Cell Biochem Funct. 2014;32(8):683–691. doi:10.1002/cbf.3072
114. Remels AH, Langen RC, Gosker HR, et al. PPARgamma inhibits NF-kappaB-dependent transcriptional activation in skeletal muscle. Am J Physiol Endocrinol Metab. 2009;297(1):E174–83. doi:10.1152/ajpendo.90632.2008
115. Cha BS, Ciaraldi TP, Park KS, Carter L, Mudaliar SR, Henry RR. Impaired fatty acid metabolism in type 2 diabetic skeletal muscle cells is reversed by PPARgamma agonists. Am J Physiol Endocrinol Metab. 2005;289(1):E151–9. doi:10.1152/ajpendo.00141.2004
116. De Coppi P, Milan G, Scarda A, et al. Rosiglitazone modifies the adipogenic potential of human muscle satellite cells. Diabetologia. 2006;49(8):1962–1973. doi:10.1007/s00125-006-0304-6
117. Sanchis-Gomar F, Pareja-Galeano H, Martinez-Bello VE. PPARgamma agonist pioglitazone does not enhance performance in mice. Drug Test Anal. 2014;6(9):922–929. doi:10.1002/dta.1587
118. Mesinovic J, Scott D, Seibel MJ, et al. Risk factors for incident falls and fractures in older men with and without type 2 diabetes mellitus: the concord health and ageing in men project. J Gerontol a Biol Sci Med Sci. 2021;76(6):1090–1100. doi:10.1093/gerona/glab062
119. Mele A, Calzolaro S, Cannone G, Cetrone M, Conte D, Tricarico D. Database search of spontaneous reports and pharmacological investigations on the sulfonylureas and glinides-induced atrophy in skeletal muscle. Pharmacol Res Perspect. 2014;2(1):e00028. doi:10.1002/prp2.28
120. Ishii S, Nagai Y, Kato H, Fukuda H, Tanaka Y. Effect of the Dipeptidyl Peptidase-4 inhibitor sitagliptin on muscle mass and the muscle/fat ratio in patients with type 2 diabetes. J Clin Med Res. 2020;12(2):122–126. doi:10.14740/jocmr4078
121. Wasada T, Yano T, Ohta M, Yui N, Iwamoto Y. ATP-Sensitive potassium channels modulate glucose transport in cultured human skeletal muscle cells. Endocr J. 2001;48(3):369–375. doi:10.1507/endocrj.48.369
122. Tsiani E, Ramlal T, Leiter LA, Klip A, Fantus IG. Stimulation of glucose uptake and increased plasma membrane content of glucose transporters in L6 skeletal muscle cells by the sulfonylureas gliclazide and glyburide. Endocrinology. 1995;136(6):2505–2512. doi:10.1210/endo.136.6.7750472
123. Andrade F, Trujillo X, Sánchez-Pastor E, et al. Glibenclamide increases post-fatigue tension in slow skeletal muscle fibers of the chicken. J Comp Physiol B. 2011;181(3):403–412. doi:10.1007/s00360-010-0527-1
124. Tricarico D, Mele A, Camerino GM, et al. The KATP channel is a molecular sensor of atrophy in skeletal muscle. J Physiol. 2010;588(Pt 5):773–784. doi:10.1113/jphysiol.2009.185835
125. de Luis Román D, Gómez JC, García-Almeida JM, et al. Diabetic Sarcopenia. A proposed muscle screening protocol in people with diabetes: expert document. Rev Endocr Metab Disord. 2024;25(4):651–661. doi:10.1007/s11154-023-09871-9
126. Bouchi R, Fukuda T, Takeuchi T, et al. Dipeptidyl peptidase 4 inhibitors attenuates the decline of skeletal muscle mass in patients with type 2 diabetes. Diabetes/Metab Res Rev. 2018;34(2):e2957. doi:10.1002/dmrr.2957
127. Rizzo MR, Barbieri M, Fava I, et al. Sarcopenia in elderly diabetic patients: role of Dipeptidyl peptidase 4 inhibitors. J Am Med Directors Assoc. 2016;17(10):896–901. doi:10.1016/j.jamda.2016.04.016
128. Sencan C, Dost FS, Ates Bulut E, Isik AT. DPP4 inhibitors as a potential therapeutic option for sarcopenia: a 6-month follow-up study in diabetic older patients. Exp Gerontology. 2022;164:111832. doi:10.1016/j.exger.2022.111832
129. Men P, He N, Song C, Zhai S. Dipeptidyl peptidase-4 inhibitors and risk of arthralgia: a systematic review and meta-analysis. Diabetes Metab. 2017;43(6):493–500. doi:10.1016/j.diabet.2017.05.013
130. Khan MW, Kurian S, Bishnoi R. Acute-onset rhabdomyolysis secondary to sitagliptin and atorvastatin interaction. Int J Gene Med. 2016;9:103–106. doi:10.2147/ijgm.S98543
131. Hu H, Xu M, Qi R, et al. Sitagliptin downregulates retinol-binding protein 4 and upregulates glucose transporter type 4 expression in a type 2 diabetes mellitus rat model. Int J Clin Exp Med. 2015;8(10):17902–17911.
132. Hasegawa Y, Hayashi K, Takemoto Y, et al. DPP-4 inhibition with linagliptin ameliorates the progression of premature aging in klotho-/- mice. Cardiovasc Diabetol. 2017;16(1):154. doi:10.1186/s12933-017-0639-y
133. Bianchi R, Cervellini I, Porretta-Serapiglia C, et al. Beneficial effects of PKF275-055, a novel, selective, orally bioavailable, long-acting dipeptidyl peptidase IV inhibitor in streptozotocin-induced diabetic peripheral neuropathy. J Pharmacol Exp Ther. 2012;340(1):64–72. doi:10.1124/jpet.111.181529
134. Witham MD, Granic A, Pearson E, Robinson SM, Sayer AA. Repurposing drugs for diabetes mellitus as potential pharmacological treatments for sarcopenia—a narrative review. Drugs Aging. 2023;40(8):703–719. doi:10.1007/s40266-023-01042-4
135. Cetrone M, Mele A, Tricarico D. Effects of the antidiabetic drugs on the age-related atrophy and sarcopenia associated with diabetes type II. Curr Diabetes Rev. 2014;10(4):231–237. doi:10.2174/1573399810666140918121022
136. Hoffmann P, Martin L, Keselica M, et al. Acute toxicity of vildagliptin. Toxicol Pathol. 2017;45(1):76–83. doi:10.1177/0192623316672944
137. Zhang X, Zhao Y, Chen S, Shao H. Anti-diabetic drugs and sarcopenia: emerging links, mechanistic insights, and clinical implications. J Cachexia Sarcopenia Muscle. 2021;12(6):1368–1379. doi:10.1002/jcsm.12838
138. Perna S, Guido D, Bologna C, et al. Liraglutide and obesity in elderly: efficacy in fat loss and safety in order to prevent sarcopenia. A perspective case series study. Aging Clin Exp Res. 2016;28(6):1251–1257. doi:10.1007/s40520-015-0525-y
139. Li CJ, Yu Q, Yu P, et al. Changes in liraglutide-induced body composition are related to modifications in plasma cardiac natriuretic peptides levels in obese type 2 diabetic patients. Cardiovasc Diabetol. 2014;13:36. doi:10.1186/1475-2840-13-36
140. Liu J, Hu Y, Zhang H, Xu Y, Wang G. Exenatide treatment increases serum irisin levels in patients with obesity and newly diagnosed type 2 diabetes. J Diab Complications. 2016;30(8):1555–1559. doi:10.1016/j.jdiacomp.2016.07.020
141. Rondanelli M, Perna S, Astrone P, Grugnetti A, Solerte SB, Guido D. Twenty-four-week effects of liraglutide on body composition, adherence to appetite, and lipid profile in overweight and obese patients with type 2 diabetes mellitus. Patient Prefer Adherence. 2016;10:407–413. doi:10.2147/ppa.S97383
142. Margulies KB, Hernandez AF, Redfield MM, et al. Effects of liraglutide on clinical stability among patients with advanced heart failure and reduced ejection fraction: a randomized clinical trial. JAMA. 2016;316(5):500–508. doi:10.1001/jama.2016.10260
143. Cava E, Yeat NC, Mittendorfer B. Preserving healthy muscle during weight loss. Adv Nutr. 2017;8(3):511–519. doi:10.3945/an.116.014506
144. Gurjar AA, Kushwaha S, Chattopadhyay S, et al. Long acting GLP-1 analog liraglutide ameliorates skeletal muscle atrophy in rodents. Metabolism. 2020;103:154044. doi:10.1016/j.metabol.2019.154044
145. Andreozzi F, Raciti GA, Nigro C, et al. The GLP-1 receptor agonists exenatide and liraglutide activate Glucose transport by an AMPK-dependent mechanism. J Transl Med. 2016;14(1):229. doi:10.1186/s12967-016-0985-7
146. Hong Y, Lee JH, Jeong KW, Choi CS, Jun HS. Amelioration of muscle wasting by glucagon-like peptide-1 receptor agonist in muscle atrophy. J Cachexia Sarcopenia Muscle. 2019;10(4):903–918. doi:10.1002/jcsm.12434
147. Chai W, Fu Z, Aylor KW, Barrett EJ, Liu Z. Liraglutide prevents microvascular insulin resistance and preserves muscle capillary density in high-fat diet-fed rats. Am J Physiol Endocrinol Metab. 2016;311(3):E640–8. doi:10.1152/ajpendo.00205.2016
148. Ren Q, Chen S, Chen X, et al. An effective glucagon-like peptide-1 receptor agonists, semaglutide, improves sarcopenic obesity in obese mice by modulating skeletal muscle metabolism. Drug Des Devel Ther. 2022;16:3723–3735. doi:10.2147/dddt.S381546
149. Xiang J, Qin L, Zhong J, Xia N, Liang Y. GLP-1RA liraglutide and semaglutide improves obesity-induced muscle atrophy via SIRT1 pathway. Diabetes Metab Syndr Obes. 2023;16:2433–2446. doi:10.2147/dmso.S425642
150. Nagai Y, Fukuda H, Kawanabe S, Nakagawa T, Ohta A, Tanaka Y. Differing effect of the sodium-glucose cotransporter 2 inhibitor ipragliflozin on the decrease of fat mass vs. lean mass in patients with or without metformin therapy. J Clin Med Res. 2019;11(4):297–300. doi:10.14740/jocmr3785
151. Bouchi R, Terashima M, Sasahara Y, et al. Luseogliflozin reduces epicardial fat accumulation in patients with type 2 diabetes: a pilot study. Cardiovasc Diabetol. 2017;16(1):32. doi:10.1186/s12933-017-0516-8
152. Kamei S, Iwamoto M, Kameyama M, et al. Effect of tofogliflozin on body composition and glycemic control in Japanese subjects with type 2 diabetes mellitus. J Diabetes Res. 2018;2018:6470137. doi:10.1155/2018/6470137
153. Yamakage H, Tanaka M, Inoue T, Odori S, Kusakabe T, Satoh-Asahara N. Effects of dapagliflozin on the serum levels of fibroblast growth factor 21 and myokines and muscle mass in Japanese patients with type 2 diabetes: a randomized, controlled trial. J Diabetes Invest. 2020;11(3):653–661. doi:10.1111/jdi.13179
154. Sano M, Meguro S, Kawai T, Suzuki Y. Increased grip strength with sodium-glucose cotransporter 2. J Diabetes. 2016;8(5):736–737. doi:10.1111/1753-0407.12402
155. Yabe D, Shiki K, Homma G, Meinicke T, Ogura Y, Seino Y. Efficacy and safety of the sodium-glucose co-transporter-2 inhibitor empagliflozin in elderly Japanese adults (≥65 years) with type 2 diabetes: a randomized, double-blind, placebo-controlled, 52-week clinical trial (EMPA-ELDERLY). Diabetes Obesity Metab. 2023;25(12):3538–3548. doi:10.1111/dom.15249
156. Okamura T, Hashimoto Y, Osaka T, Fukuda T, Hamaguchi M, Fukui M. The sodium-glucose cotransporter 2 inhibitor luseogliflozin can suppress muscle atrophy in Db/Db mice by suppressing the expression of foxo1. J Clin Biochem Nutr. 2019;65(1):23–28. doi:10.3164/jcbn.18-114
157. Hata S, Okamura T, Kobayashi A, et al. Gut microbiota changes by an SGLT2 inhibitor, luseogliflozin, alters metabolites compared with those in a low carbohydrate diet in db/db mice. Nutrients. 2022;14(17):3531. doi:10.3390/nu14173531
158. Otsuka H, Yokomizo H, Nakamura S, et al. Differential effect of canagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, on slow and fast skeletal muscles from nondiabetic mice. Biochem J. 2022;479(3):425–444. doi:10.1042/bcj20210700
159. Tanaka K, Takahashi H, Katagiri S, et al. Combined effect of canagliflozin and exercise training on high-fat diet-fed mice. Am J Physiol Endocrinol Metab. 2020;318(4):E492–e503. doi:10.1152/ajpendo.00401.2019
160. MacDonald TL, Pattamaprapanont P, Cooney EM, et al. Canagliflozin prevents hyperglycemia-associated muscle extracellular matrix accumulation and improves the adaptive response to aerobic exercise. Diabetes. 2022;71(5):881–893. doi:10.2337/db21-0934
161. Nambu H, Takada S, Fukushima A, et al. Empagliflozin restores lowered exercise endurance capacity via the activation of skeletal muscle fatty acid oxidation in a murine model of heart failure. Eur J Pharmacol. 2020;866:172810. doi:10.1016/j.ejphar.2019.172810
162. Lv XH, Cong XX, Nan JL, et al. Anti-diabetic drug canagliflozin hinders skeletal muscle regeneration in mice. Acta Pharmacol Sin. 2022;43(10):2651–2665. doi:10.1038/s41401-022-00878-7
163. Li D, Ruan G, Zhang Y, et al. Metformin attenuates osteoarthritis by targeting chondrocytes, synovial macrophages and adipocytes. Rheumatology. 2023;62(4):1652–1661. doi:10.1093/rheumatology/keac467
164. Gong J, Ye C, Ran J, et al. Polydopamine-mediated immunomodulatory patch for diabetic periodontal tissue regeneration assisted by metformin-ZIF system. ACS nano. 2023;17(17):16573–16586. doi:10.1021/acsnano.3c02407
165. Tezze C, Amendolagine FI, Nogara L, et al. A combination of metformin and galantamine exhibits synergistic benefits in the treatment of sarcopenia. JCI Insight. 2023;8(15):e168787. doi:10.1172/jci.insight.168787
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.