Back to Journals » Drug, Healthcare and Patient Safety » Volume 12
Effects of Eperisone Hydrochloride and Non-Steroid Anti-Inflammatory Drugs (NSAIDs) for Acute Non-Specific Back Pain with Muscle Spasm: A Prospective, Open-Label Study
Authors Pinzon RT ![]() , Wijaya VO
, Wijaya VO ![]() , Paramitha D
, Paramitha D ![]() , Bagaskara RR
, Bagaskara RR
Received 24 August 2020
Accepted for publication 20 October 2020
Published 16 November 2020 Volume 2020:12 Pages 221—228
DOI https://doi.org/10.2147/DHPS.S278467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Rizaldy Taslim Pinzon,1,2 Vincent Ongko Wijaya,1,2 Dessy Paramitha,1,2 Raymondus Rangga Bagaskara1,2
1Faculty of Medicine, Duta Wacana Christian University, Yogyakarta, Indonesia; 2Bethesda Hospital, Yogyakarta, Indonesia
Correspondence: Rizaldy Taslim Pinzon
Faculty of Medicine, Duta Wacana Christian University, 5-25 Dr. Wahidin Sudirohusodo Street, Yogyakarta, 55224, Indonesia
Email [email protected]
Background: Low back pain (LBP) occurs as a common condition and may harm the patient’s quality-of-life. Non-steroid anti-inflammatory drugs (NSAIDs) and eperisone form a drug regiment that has been reported as effective in improving low back pain, yet the evidence for its efficacy and safety is lacking.
Objective: The aim of this study was to evaluate the effect of eperisone hydrochloride and ibuprofen compared with ibuprofen alone in reducing symptoms of patients with acute non-specific back pain with a muscle spasm.
Methods: This was an open-label, prospective study involving 100 subjects with symptoms of back pain and muscle spasm. Eligible participants were randomly allocated to an experimental group (54 patients) and a control group (46 patients). The experimental group received eperisone 50 mg three times daily + ibuprofen 400 mg twice daily, and the control group received ibuprofen 400 mg twice daily over a 4-week duration. The primary outcomes were measured with the visual analog scale (VAS), and finger-to-floor (FTF) distance at baseline, week 2, and week 4.
Results: After 4 weeks of follow-up, results from 59 subjects were collected. In both groups, VAS and FTF were decreased compared to baseline. Clinically significant pain reduction (> 50% than baseline) was observed to be higher in the experimental group compared with the control group in the fourth week (72.4% vs 46.7%, P< 0.05). At the end of the study, pain reduction in the experimental group was more significant compared to the control group (28.13± 24.72 vs 34.42± 28.47) and participants mobility (FTF distance < 10 cm) improved in both groups, especially in the experimental group (75.9% vs 70%). There was no difference in adverse events between groups (P> 0.05).
Conclusion: The combination of eperisone hydrochloride and ibuprofen effectively reduces pain and improves functional outcomes over ibuprofen alone with a similar safety profile in these patients with acute non-specific back pain with muscle spasm.
Keywords: low back pain, eperisone hydrochloride, pain reduction, comparison
Introduction
Low back pain (LBP) is a common complaint and occurs in more than 80% of the population.1 It refers to an unpleasant sensory and emotional experience associated with actual or potential tissue damage felt near the mid-line in the lumbar or sacral region.2 The prevalence of low back pain is approximately 38.4%, more than one third among the productive age population. The intensity of pain that affects daily activities impacts the socio-economic aspect not only of individuals but also of their families, communities, industry, and governments.3 Low back pain is also the main cause of years of life with a disability (YLD).4
Eperisone hydrochloride, a centrally acting muscle relaxants, has shown a potential effect in pain management. Its action mechanism involves inhibition of neural activity and pain sensation by blocking the voltage-gated sodium channels (VGSC) in the brain stem.5 Moreover, eperisone was found to be beneficial in reducing symptoms (eg, pain, stiffness) of patients with cervical spondylosis and painful rheumatic conditions.6 A systematic review found that eperisone may be effective in pain reduction in acute LBP patients by improving paraspinal blood flow with less adverse events.7 However, the study regarding therapeutics use of eperisone hydrochloride in combination with NSAIDs in back problems is limited, and the result of those studies was not concluded. The study’s purpose was to evaluate the efficacy of eperisone hydrochloride and ibuprofen compared with ibuprofen alone for the treatment of acute non-specific back pain with a muscle spasm.
Methods
Study Design and Sample Size
This was an open-label, prospective study design of 4 weeks duration conducted in the neurology clinic at Bethesda Hospital, Yogyakarta, Indonesia. Participants of this study were patients with signs and symptoms of LBP who were referred to the Neurology clinic. The sample size for the study was calculated by taking the most probable prevalence of low back pain from previous studies as 50% and considering the power of 80% and a level of significance of 5%. Considering the drop-out rate of 10%, the total sample size was fixed as 100 subjects.3,4
Inclusion and Exclusion Criteria
The inclusion criteria were adult patients aged >18 years old, either diagnosed with acute non-specific back pain or with a history of muscle spasm in the last 7 days. The diagnosis of back pain with muscle spasm was made by attending neurologists based on physical and radiology examinations. All patients did not have any other supportive treatments or non-pharmacotherapy pain relief.
The exclusion criteria were subjects with known hypersensitivity to eperisone or NSAIDs, patients with other causes of back pain due to trauma, malignancy, infection, abnormal metabolism, osteoarthritis of the hip or any other disease, back pain referred from other organs, patients with a history of peptic ulceration or gastrointestinal bleeding or severe dyspepsia, or had participated in another clinical trial within 1 month, or patients with significant comorbidity of the renal, hepatic, gastrointestinal tract, and cardiovascular disease, or pregnant and nursing mothers.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. The procedures of the treatment were explained to the eligible participants by the attending physician. After the patient agrees with the study protocol, the written consent form was signed by the patient. This trial has been approved by the Research Ethics Committee of Duta Wacana Christian University (protocol number: 988/C.16/FK/2019) and registered in the Indonesia Clinical Research Registry (No. Registry: INA-OB1RAKC). All the eligible participants received reimbursement for their contribution and were not charged for any treatments in this study.
Randomization and Patients’ Enrollment
Eligible participants were randomized with a computer-generated randomization program at the ratio of 1:1 to each group of the study. It was presumed that participants were distributed almost equally with respect to gender and age in both interventions. The authors of this study did not participate in randomization process. The study was conducted over 4 weeks duration. Subjects were randomized to one of the study treatments: experimental group (group 1) with a combination of ibuprofen 400 mg twice daily (b.i.d) + eperisone hydrochloride 50 mg three times daily (t.i.d), or the control group (group 2) with ibuprofen 400 mg twice daily (t.i.d). Adverse events (AEs) were monitored regularly during study duration, and subjects may discontinue from the study at any time.
Outcome Measures
The main outcomes of this trial were the proportion of subjects with clinical response at Week 0 (as baseline comparison), Week 2 (visit 1), and Week 4 (visit 2). The clinical response was measured based on pain intensity and spinal mobility. Patients rated their average pain intensity over the last 48 hours using the 100-mm visual analog scale (VAS), where 0 is no pain, and 100 is the worst pain at each visit. The finger-to-floor (FTF) test is used to evaluate the mobility of the spine and the pelvis in the bending forward position’s motion. The finger-to-floor test evaluation was done by measuring the distance between the patient’s finger and ground on centimeters when the patient was in a bending forward position, trying to touch the floor. The FTF test has excellent reliability to assess patients with low back pain.5,8
Statistical Analysis
The baseline characteristics between the two groups were analyzed using univariate analysis, and ANOVA was used to compare the means between related groups. Chi-square or Fisher exact test was used to assess categorical variables. Multivariate analysis was performed to identify any statistically significant relationship between variables. Statistical significance was set at the level of less than 0.05 (Two-tailed P-values). The analysis was performed with SPSS version 21.0.
Results
A total of 100 eligible subjects were initially enrolled and randomly divided into two groups of the experimental group (54 in group 1), treated with a combination of ibuprofen and eperisone hydrochloride, and the control group (46 in group 2), treated with ibuprofen alone. The baseline characteristics of the two groups were similar (Table 1). At the end of Week 2, six subjects (five losses of follow-up and one case because of AE) in the experimental group and three subjects (two losses of follow-up and one because of AE) in the control group discontinued the study. A total of 15 subjects dropped out from the study for various reasons, including loss of contacts, did not appear at the next visit, and personal reasons. At the end of the study follow-up in Week 4, collected data from 59 patients, including 29 participants in group 1 and 30 in group 2, were finally analyzed (CONSORT flow chart; Figure 1).
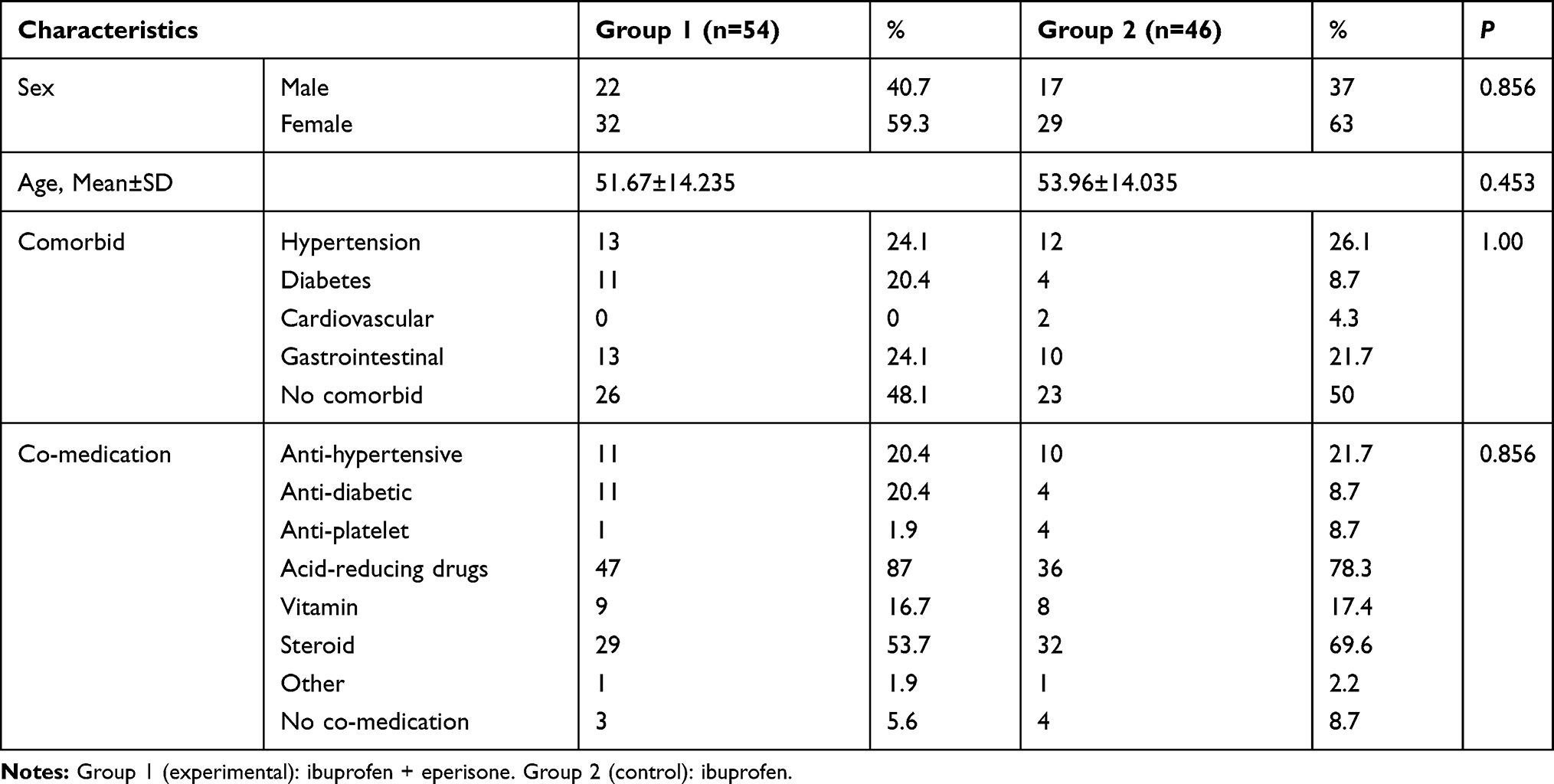 |
Table 1 Baseline Characteristic Between Two Groups |
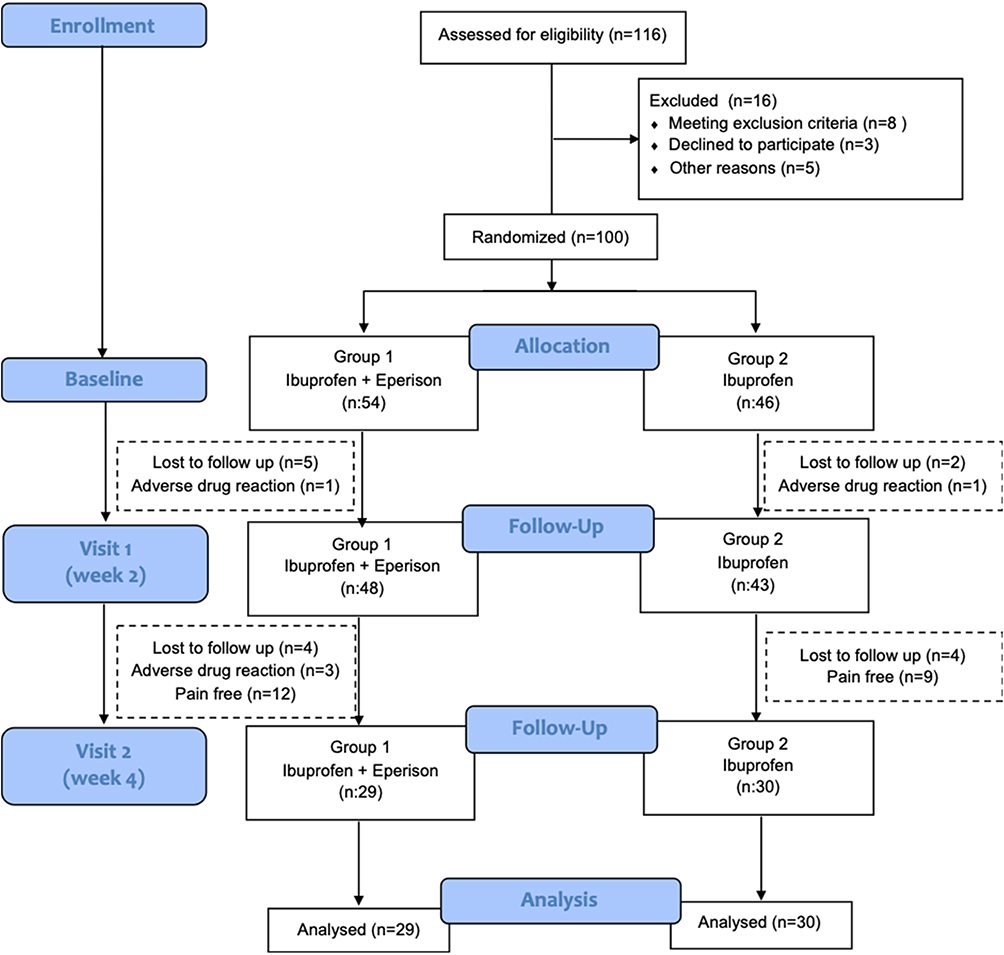 |
Figure 1 The Consolidated Standards of Reporting Trials (CONSORT) diagram of the study. |
Baseline Characteristics
Initially, all the subjects (100 participants) recruited were analyzed for their baseline characteristics. In this study, 39 patients (39%) were male, and 61 (61%) were female. The mean age of the study subjects in the experimental group was 51.67±14.23 years and 53.96±14.03 years in the control group. There was no difference in age and sex between the experimental and control group in this study. The most common comorbidity in group 1 was hypertension or gastrointestinal tracts disorder, such as mild or moderate dyspepsia, whereas hypertension was the most common comorbidity in group 2. Most participants have also received co-medication, and the most prescribed drug in both groups was acid-reducing drugs (87% in group 1 and 78% in group 2), including proton-pump inhibitor or H2-antagonist receptor. The baseline characteristics between the two groups are shown in Table 1.
Pain Reduction
The pain severity score was measured three times during the study period with a visual analog scale. The mean (mm)±standard deviation (SD) score of pain severity at the baseline was 58.33±20.25 mm in the experimental group. The severity was not significantly different in the baseline with the control group (56.52±21.31 mm). The comparison of pain severity between the two groups on the first visit (Week 2) was 28.13±24.72 mm vs 34.42±28.47 mm. The pain severity at the last visit (Week 4) was only 20.34±23.82 in the experimental group, compared with 28.71±20.12 mm in the control group. Table 2 presents the comparison of pain reduction in both groups during the study period, indicating that group 1 had better pain reduction than group 2.
 |
Table 2 Comparison of Pain Severity Between Two Groups |
Overall, pain reduction in the experimental group (group 1) was greater compared to the control group (group 2) in the first (28.13±24.72 mm vs 34.42±28.47 mm) and the second visit during 4 weeks duration of the trial. Table 3 shows the percentage of pain reduction between each group in Week 2 and Week 4 (20.34±23.82 mm vs 28.71±20.12 mm). Moderate pain reduction with more than 30% reduction of pain severity from the baseline was observed in 81.3% patients in the experimental group compared with only 67.4% in the control group. Clinically significant pain reduction (>50% baseline) was observed higher in the experimental group compared with the control group in the fourth week (72.4% vs 46.7%; P<0.05).
 |
Table 3 Comparison of Pain Reduction Percentage Between Two Groups |
Functional Improvement
We measured the functional and mobilization status of the patients with the finger-to-floor test. Table 4 shows the comparison of finger-to-floor distance test result. Both groups showed improvement of finger-to-floor distance test during visit 1 and 2 compared with the baseline. Initially, those in control group had better mobility based on FTF distance of <10 cm in comparison with the control group (23.9% vs 18.5%), and most participants had a FTF distance in the range of 10–30 cm in both groups (50% in group 1 and 54.3% in group 2). At follow-up in week 2, the FTF distance improved and most participants can reach a distance of <10 cm (62.5% in group 1 and 55.8% in group 2). At the end of the study, participant’s mobility (FTF distance <10 cm) improved in both groups, especially in the experimental group (75.9% vs 70%). Although the results achieved with eperisone and ibuprofen were slightly better than those with ibuprofen alone, no statistically significant difference was observed between the two groups at any time.
 |
Table 4 Effects of Functional Improvement in a 30-Day Treatment in Group 1 (Experimental) and Group 2 (Control); Evaluated by Finger-to-Floor Test |
Adverse Events
Adverse events occurrence were frequently similar between the two groups, as seen in Table 5. The adverse events reported were minor events such as dizziness, stomach pain, and skin rash. There were no serious adverse events reported (eg, anaphylaxis). At the first follow-up during visit 1 (Week 2), four patients (8.3%) in the experimental group (group 1) had adverse events (one discontinued the study due to stomach pain) and three patients in the control group (group 2) had adverse events (one discontinued the study due to stomach pain). At the second follow-up (Week 4), three patients (11.5%) with adverse events withdrew from the study. There is no significant difference in adverse events between the two groups (P>0.05). All patients with adverse events received rescue medications symptomatically.
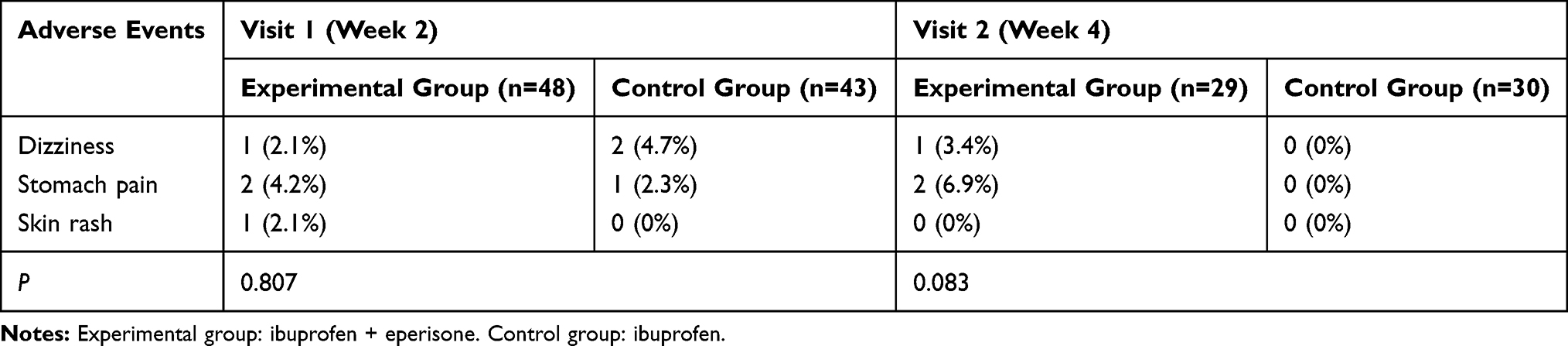 |
Table 5 The Adverse Events Occurrence Between Two Groups |
Discussion
NSAIDs are widely used for symptomatic relief in a clinical setting as they had a role as an analgesic, antipyretic, and anti-inflammatory agent.9 Low back pain is one of the pain-related disorders that prescribe with NSAIDs for its analgesic properties.10 Even so, there was a report on activation of nociception by inflammation and muscle spasm of the spine, thus rationalized use of eperisone as a muscle relaxant on treating low back pain.11
A past trial has shown that eperisone had a beneficial effect on patients with cervical spondylosis and other symptoms related to muscle stiffness.12 Another trial showed eperisone was superior to baclofen in reducing muscular tone and improvement in joint mobility in patients with spastic palsy. Eperisone activity has been linked with its inhibition on the spinal reflex pathway and vasodilation, resulting in improvement on blood flow and inhibition of the pain pathway. This may explain the reason of eperisone analgesic activity in reducing pain intensity.13
A previous study measured VAS in patients and grouped it as severe (75–100 mm), moderate (45–74 mm), mild (5–44 mm), and no pain (0–4 mm). They considered a clinically significant improvement if VAS score was reduced from the more severe group to the milder one. In patients with rheumatoid arthritis, the minimally clinically significant change has been estimated as 1.1 points. VAS has demonstrated sensitivity to pain changes assessed within hours to 4 weeks following analgesic therapy.14,15
In our study, both groups significantly affected the VAS and FTF distance, particularly in combination treatment of eperisone and ibuprofen, because of the muscle relaxant action of eperisone. This study provides new evidence that a combination of NSAIDs and eperisone had a higher efficacy on reducing pain severity on low back pain compared with NSAIDs alone. It showed a faster decrease in pain severity score on the experimental group than in the control group, leading to a more significant decrease in pain severity score in the second or third visit. Another study that also confirmed eperisone efficacy as a treatment for low back pain showed a similar result by reduction of “pain at rest,” “pain on palpation,“ and a decline in value of numeric pain scale before and after therapy.5,9,16,17
Finger-to-floor distance test was used in this study based on a report showing that early changes on the finger-to-floor test result were a good and valid predictor in self-reported disability scores over 1 year.18 Another study also reported everyday functioning problems raised by movement avoidance (fear-avoidance beliefs) induced by low back pain disorder.18 Improvement of finger-to-floor test results occurred in all the groups throughout this study, with more significant improvement from the experimental group starting from week 2 (first visit). This means the response rate of eperisone and ibuprofen was superior to ibuprofen monotherapy in making improvements on the finger-to-floor test result, thus it might positively affect the self-reported disability score over 1 year.
The combination therapy with eperisone and ibuprofen is more beneficial and safe, with similar rates of adverse effects occurrence compared to treatment with ibuprofen alone in patients with low back pain. This evidence supports the use of eperisone and NSAIDs as a treatment of acute low back pain with muscle spasm. A past comparative study between eperisone and baclofen also showed that both drugs have similar tolerability with no differences and minimum adverse effects.13,19 In rheumatology practice, it is a common practice to combine analgesic (eg, NSAIDs) with a muscle relaxant (eg, thiocolchicoside or dantrolene), even using fixed-dose combinations to achieve a satisfactory reduction of both pain and muscle contracture.20,21
There are several limitations to this study. The open-label design of this study may results in study bias due to lack of blinding, especially in the treatment group. Moreover, it may contribute to the relatively large number of drop-outs/lost to follow-up subjects. Also, the sample size was relatively small in both groups. Another limitation is the lack of a second, placebo preparation being given to the ibuprofen alone group. These limitations can have a significant impact on the efficacy of the therapy. We suggest to carry out a double-blind study design with large populations and the use of identical placebo to increase the validity and statistical power of a similar study in the future. Further studies should involve other conditions as a comparison.
Since acute low back pain is a common condition with very high prevalence, results on a sample of 59 patients, cannot be completely generalized to the whole population. However, the findings on this study can suggest to clinicians the potential treatment regimens of eperisone hydrochloride plus ibuprofen for patients with acute non-specific low back pain with muscle spasm.
Conclusion
The combination of eperisone hydrochloride and ibuprofen appeared to be more effective in reducing pain and providing functional improvement than ibuprofen alone, with a similar safety profile in these patients with acute non-specific back pain with muscle spasms.
Data Sharing Statement
The authors intend to share participants’ data collected during the trial, after deidentification. This includes, study protocol, statistical analysis plan, informed consent forms, and clinical study report. The data will be available based on the request of investigators whose proposed use of the data has been approved by an independent review committee by sending an email to the corresponding author. Data are available immediately following publication with no end date.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. The Lancet. 2012;379(9814):482–491. doi:10.1016/s0140-6736(11)60610-7.
2. Visser EJ, Davies S. What is pain? I: terms, definitions, classification, and basic concepts. Australian Anaesthesia. 2009;29–33.
3. Novitasari DD, Sadeli HA, Soenggono A, Sofiatin Y, Sukandar H, Roesli RMA. Prevalence and characteristics of low back bain among productive age population in Jatinagor. Althea Med J. 2016;3(3):469–476. doi:10.15850/amj.v3n3.863
4. Khan AF, Parveen K, Khan AS. Efficacy and tolerability of eperisone versus tizanidine in patients suffering from low back pain with muscle spasm. Int J Res Med Sci. 2017;5(6):2694–2700. doi:10.18203/2320-6012.ijrms20172472
5. Maaz SH, Khandelwal PN, Baig SM, Doifode SM, Ghotkar UM. Evaluation of efficacy and tolerability of eperisone and thiocolchicoside in treatment of low back pain associated with muscle spasm: an open-label, prospective, randomized controlled trial. Int J Basic Clin Pharmacol. 2016;5(6):2669–2674. doi:10.18203/2319-2003.ijbcp20164144
6. Bose K. The efficacy and safety of eperisone in patients with cervical spondylosis: results of a randomized, double-blind, placebo-controlled trial. Method Find Exp Clin Pharmacol. 1999;21:209–213. doi:10.1358/mf.1999.21.3.534831
7. Bavage S, Durg S, Ali Kareem S, Dhadde SB. Clinical efficacy and safety of eperisone for low back pain: a systematic literature review. Pharmacol Rep. 2016;68(5):903–912. doi:10.1016/j.pharep.2016.05.003.
8. Perret C, Poiraudeau S, Fermanian J, Colau MM, Benhamou MA, Revel M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch Phys Med Rehabil. 2001;82(11):
9. Widyantanti MAS, Pinzon RT. The use of eperisone hydrochloride reduce pain for acute low back pain patients at Bethesda Hospital Yogyakarta. Media Farmasi. 2017;14:177–192.
10. Chandanwale AS, Chopra A, Goregaonokar A, et al. Evaluation of eperisone hydrochloride in the treatment of acute musculoskeletal spasm: a randomized, double blind, placebo controlled trial. J Postgrad Med. 2011;57(4):278–285. doi:10.4103/0022-3859.90076
11. Cabitza P, Randelli. Efficacy and safety of eperisone hydrochloride in patient with low back pain: a double-blind randomized study. Eur Rev Med Pharmacol Sci. 2008;12(4):229–235.
12. Sartini S, Guerra L. Open experience with a new myorelaxant agent for low back pain. Adv Ther. 2008;25:1010–1018. doi:10.1007/s12325-008-0108-9
13. Bresolin N, Zucca C, Pecori A. Efficacy and tolerability of eperisone and baclofen in spastic palsy: a double-blind randomized trial. Adv Ther. 2009;26:563–573. doi:10.1007/s12325-009-0031-8
14. Wolfe F, Michaud K. Assessment of pain in rheumatoid Arthritis: minimal clinically significant difference, predictor, and the effect of anti-tumor necrosis therapy. J Rheumatol. 2007;34:1674–1683.
15. Hawker G, Samra AM. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short‐Form McGill Pain Questionnaire (SF‐MPQ), Chronic Pain Grade Scale (CPGS), Short Form‐36 Bodily Pain Scale (SF‐36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63.
16. Rani S, Kumar S, Joytt VPK, Lamba D, Saini R. To compare the efficacy and safety of eperisone with thiocolchicoside in patients with acute lower backache associated with muscle spasm. Ind J Pharm Pharmacol. 2016;3(2):79–83. doi:10.5958/2393-9087.2016.00018.2
17. Rusinyol FC, Perice RV, Boronat ER, Bosch FF. Effect of two different doses of eperisone in the treatment of acute low back pain. J Appl Res. 2009;9(1–2):23–29.
18. Ekedahl H, Jönsson B, Frobell RB. Fingertip-to-floor test and straight leg raising test: validity, responsiveness, and predictive value in patients with acute/subacute low back pain. Arch Phys Med Rehabil. 2012;93:2210–2215. doi:10.1016/j.apmr.2012.04.020.
19. Grabovac I, Dorner TE. Association between low back pain and various everyday performances. Wien Klin Wochenschr. 2019;131:541–549. doi:10.1007/s00508-019-01542-7
20. Snapinn SM. Evaluating the efficacy of a combination therapy. Stat Med. 1987;6:657–665. doi:10.1002/sim.4780060603
21. Borenstein DG, Lacks S, Wiesel SW. Cyclobenzaprine and naproxen versus naproxen alone in the treatment of acute low back pain and muscle spasm. Clin Ther. 1990;12:125.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.