Back to Journals » Clinical Interventions in Aging » Volume 15
Effects of Domiciliary Professional Oral Care for Care-Dependent Elderly in Nursing Homes – Oral Hygiene, Gingival Bleeding, Root Caries and Nursing Staff’s Oral Health Knowledge and Attitudes
Authors Girestam Croonquist C, Dalum J ![]() , Skott P, Sjögren P, Wårdh I, Morén E
, Skott P, Sjögren P, Wårdh I, Morén E ![]()
Received 20 March 2020
Accepted for publication 8 July 2020
Published 6 August 2020 Volume 2020:15 Pages 1305—1315
DOI https://doi.org/10.2147/CIA.S236460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Caroline Girestam Croonquist,1,2 Jesper Dalum,3 Pia Skott,1,2 Petteri Sjögren,4 Inger Wårdh,2,3 Elisabeth Morén3
1Folktandvården Stockholm AB, Stockholm, Sweden; 2Academic Centre Of Geriatric Dentistry, Stockholm, Sweden; 3Department Of Dental Medicine, Karolinska Institutet, Huddinge, Sweden; 4Oral Care AB, Stockholm, Sweden
Correspondence: Elisabeth Morén Department Of Dental Medicine
Karolinska Institutet, Box 4064, Huddinge 141 04, Sweden
Tel +46 70 165 88 03
Email [email protected]
Purpose: The primary aim was to describe the effects for nursing home residents of monthly professional cleaning and individual oral hygiene instruction provided by registered dental hygienists (RDHs), in comparison with daily oral care as usual. The secondary aim was to study the knowledge and attitudes among nursing staff regarding oral health care and needs.
Patients and Methods: In this randomised controlled trial (RCT), 146 residents were recruited from nine nursing homes in Regions of Stockholm and Sörmland and were randomly assigned (on nursing home level) to either intervention group (I; n=72) or control group (C; n=74). Group I received monthly professional cleaning, individual oral hygiene instructions and information given by an RDH. Group C proceeded with daily oral care as usual (self-performed or nursing staff-assisted). Oral health-related data was registered with the mucosal-plaque score index (MPS), the modified sulcus bleeding index (MSB), and root caries. The nursing staff’s attitudes and knowledge were analysed at baseline and at six-month follow-up. Statistical analysis was performed by Fisher’s exact test and two-way variance analysis (ANOVA).
Results: Improvements were seen in both Group I and Group C concerning MPS, MSB and active root caries. The nursing staff working with participants in Group I showed significant improvements regarding the Nursing Dental Coping Beliefs Scale (DCBS) in two of four dimensions, oral health care beliefs (p=0.0331) and external locus of control (p=0.0017) compared with those working with Group C. The knowledge-based questionnaire showed improvement (p=0.05) in Group I compared with Group C.
Conclusion: Monthly professional oral care, combined with individual oral health care instructions, seems to improve oral hygiene and may reduce root caries among nursing home residents. This may also contribute to a more positive attitude regarding oral hygiene measures among nursing home staff, as compared with daily oral care as usual.
Keywords: aged, residential facilities, nursing staff, dental care, attitude of health personnel, oral health
Introduction
With an ageing population, the need for care support for dependent elderly increases for the general public.1 Domiciliary dental care enables dental services in the patients’ residences and offers the opportunity to provide regular check-ups, preventive measures and dental treatments to individuals who experience difficulties attending a regular dental clinic.2 The dental care performed at home by dental personnel is rudimentary, with rather simple equipment and treatments like scaling of calculus, tooth extractions, tooth restorations, adjustments of dentures and plaque removal.3 A study conducted by Wårdh et al (2012)3 regarding nursing staff’s knowledge and attitudes towards oral health care showed that the majority of the nursing staff believed that the residents would tell them when they needed help with their daily oral hygiene. Furthermore, the majority felt that performing assisted oral care (toothbrushing, interproximal tooth cleaning and/or cleaning of prothesis) was a difficult task and 80% thought the greatest obstacle was the non-cooperation from the residents. Keboa et al (2019) presented, from a nursing staff perspective on performing assisted oral care, that challenges lie in complicated teeth constructions, high workload, resistance towards examine another person’s oral cavity/mouth, and not wanting to performed assisted oral care.4
Residents at nursing homes may face difficulties visiting a dental clinic,5 and a study by Muszalik et al (2015)6 of patients visiting a geriatric clinic showed that elderly persons often have difficulties participating in activities outside their home environment. The major issues were the lack of energy and the presence of pain. Today, elderly in developed countries retain their teeth at a higher age,7–9 but ageing with increased morbidity and polypharmacy often results in frailty and dependence on the care of others, all of which increase the risk of deterioration of oral health and susceptibility to developing oral diseases.10,11 The relatively high number of natural teeth and complicated oral prosthetic constructions (eg, bridges, crowns and oral implants),7,12,16 together with progressing morbidity and care dependence, necessitates that daily oral hygiene activities need to be maintained on a sufficient level, or even intensified.7 The presence of oral health conditions can cause pain, infections and nutritional difficulties.7,8 The common condition oral dryness increases the risk of dental caries, which can relatively rapidly lead to deterioration of oral health.13,14 Additionally, it can cause a social handicap since oral dryness can lead to difficulties speaking, chewing and swallowing, impairment in tasting,14,15 and have a negative impact on quality of life.14,16,17
Oral and general health are strongly related in older individuals16,18 and maintained oral health among the elderly has been related to retained general health.19,20 A study conducted by Hagglund et al (2019)12 showed that the mortality risk observed over one year was significantly higher in older individuals with poor oral health than in those with good oral health. Furthermore, it has been shown that intensified oral care interventions by dental personnel may prevent approximately one in ten deaths from healthcare-associated pneumonia (NNT 8.6–11).21 Both natural teeth and dentures may constitute a reservoir for respiratory pathogens,22 and denture wearing at night doubles the risk of healthcare-associated pneumonia in the oldest adults.23 Barbe et al (2019)24 concluded that professional cleaning performed by a dental nurse every two weeks on residents living at nursing homes maintained and improved the residents’ oral health. Furthermore, domiciliary dental care provides the possibility of reaching individuals with, for example, cognitive impairment and/or functional limitations.19,25
The primary aim of this study was to describe the effects for nursing home residents of professional cleaning and individual oral hygiene instruction provided by registered dental hygienists (RDHs), in comparison with daily oral care as usual. The secondary aim was to study the knowledge and attitudes among nursing staff regarding oral health care and needs.
The hypothesis was that domiciliary prophylactic professional oral care will improve oral health among participants in the intervention group, in comparison with participants in a control group that receives daily oral care as usual.
Materials and Methods
This evaluator-blinded RCT with an open-ended design was performed at nine Swedish nursing homes. One hundred and forty-six residents were recruited to participate in the study; 72 were randomised to the intervention group (Group I) and 74 to the control group (Group C).
Ethical Statement
The study was approved by the Ethics Committee in Stockholm, Sweden (Number 2015/1641-31/2) and was registered in ClinicalTrial.gov (Number NCT02669979).
Randomisation and Recruitment of the Nursing Homes
Four nursing homes in Region Stockholm and five nursing homes in Region Sörmland were recruited to the study. Randomisation was performed at nursing home level.26 The nursing homes were chosen geographically (urban and rural areas) and were managed by both private companies and municipalities. Approval from the head of the nursing home was mandatory for inclusion in the study. After collecting informed consent (for residents showing signs of reduced cognitive function according to Pfeiffer-test,27 informed consent was required from either a relative or an advocate), the randomisation of the nursing homes to either Group I or Group C was decided by a computer-generated sequence and administrated by a coded letter representing each nursing home. The letter was opened by an RDH not otherwise involved in the clinical examinations in the study.
The inclusion criteria were living in a nursing home, ≥85 years of age, and at least ten remaining teeth including dental implants. Exclusion criteria were having full dentures, edentulous, reduced cognitive function that made cooperation impossible for examination and treatment by RDHs, extreme dry mouth assessed by the mirror-sliding friction test28 and ASA risk qualification of 4 or higher.29 The taking of antiplatelet drugs and anticoagulants was not an exclusion criterion but was noted in the study protocol during data collection.
Study Process
At baseline, participants in both study groups received professional cleaning (tooth brushing, interproximal cleaning and scaling of supragingival calculus) performed by three calibrated and blinded RDHs. Home care instructions regarding oral hygiene were given verbally and in writing to participants in both study groups and to nursing staff, and fluoridated toothpaste, a soft toothbrush and interproximal cleaning aids were given free of charge.
Intervention
The participants in Group I received monthly professional cleaning, individual oral hygiene instructions and information by RDHs (not otherwise involved in the oral examination and study protocol registration). The visiting time was approximately 30 minutes.
Control
The participants in Group C received the same baseline procedure as Group I and proceeded with daily oral care as usual, performed either by themselves or assisted by nursing staff, throughout the study, without any additional visits or instructions by a study RDH.
Oral Examination and Study Protocol
Oral examination was performed by using a flashlight, mirror and probe at baseline and the results were registered in a study protocol (available on request) together with medical history and medication use. Indexes used were the mucosal-plaque score index (MPS),30 modified sulcus bleeding index (MSB)31 and root caries. Oral mouth dryness was measured by the participants’ subjective experiences and the mirror-sliding friction test28 on the inside of the buccal mucosa. Registrations according to the study protocol were performed in both groups by the three calibrated RDHs at baseline, after three months and after six months (Figure 1).
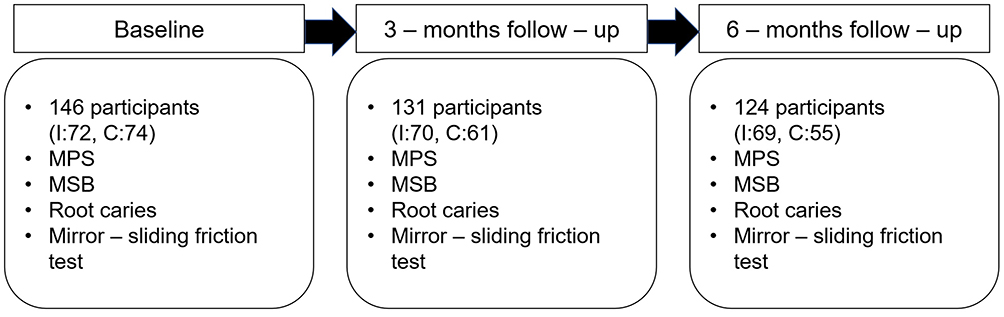 |
Figure 1 Flow chart over clinical registrations according to the study protocol, the total number of residents and also for the intervention group (I) and the control group (C) throughout the study. From baseline to the end of the study at six-month follow-up. Instruments: Mucosal and plaque score index (MPS), modified sulcus bleeding index (MSB) and root caries. |
Indexes
MPS is a combined mucosal score and plaque score index used both for edentulous and dentate individuals. Before oral measurements, dental prostheses were removed if present. Mucosal score (MS) rates changes in the oral mucosa, and plaque score (PS) rates the amount of plaque both on natural teeth and on removable dentures and fixed prosthodontics. MS and PS are rated from 1 to 4 (4 is the most severe). By interpretation of the index, MS and PS are combined. The purpose of the index is to validate oral hygiene and not to serve as a diagnosis.30
MSB was used to measure bleeding from the gingival margin on the buccal surface of the Silness-Loe index teeth12,16,24,32,36,44 or, when missing, the closest tooth32 was assessed according to MSB, which has four levels (0–3) where 3 is the most severe.31
Root caries33 was assessed according to five levels on the buccal surface on Silness-Loe index teeth.
Nursing Staff
Nursing staff from four nursing homes participated in this part of the study, with a total of 50 participants included. The intervention group contained 35 participants at baseline and 20 participants at six-month follow-up. The control group contained 15 participants at baseline and 15 participants at follow-up. Twelve participants from the intervention group and 2 participants from the control group could be followed using a four-digit code number from baseline to six-month follow-up and were therefore designated as the identified group.
Study Process
All nursing staff (nursing aides, assistant nurses, registered nurses and other staff such as administrators and managers) participated in an oral health education programme at study start, given by one RDH who was not otherwise involved in the study.
Intervention
The nursing staff’s knowledge and attitude towards oral health were registered prior to participating in the educational programme at baseline using two questionnaires. The questionnaires were repeated at the six-month follow-up.
Questionnaires
The questionnaires used were the Nursing Dental Coping Belief Scale (Nursing DCBS)34 questionnaire and a knowledge-based questionnaire regarding oral health.35 Both questionnaires were distributed to the current nursing staff working at the nursing homes that day, at baseline and at six-month follow-up. The questionnaires were pseudonymised with a four-digit code number.
The nursing DCBS index is a tool used to measure how groups of nursing staff differ in their priorities and how they meet their responsibilities for oral health care.34 The DCBS was developed by Jacobs & Stewart and is based on three major models of cognitive behavioural psychology consisting of Julian Rotter’s locus of control (divided into IL and EL), Albert Bandura’s self-efficacy and Donald Meichenbaum’s self-instructional technique.36 The DCBS consists of four dimensions: “internal locus of control (IL)”, “external locus of control (EL)”, “self-efficiency (SE)” and “oral health-care beliefs (OHCB)” and has been used in various types of care-related research.37 The IL dimension evaluates people’s self-control and self-experienced beliefs concerning events in life, for example, “I believe brushing can help prevent cavities”, and people with high degrees of IL expect themselves to have great control and responsibility over events in life. In contrast, people with high degrees of EL expect and believe that their lives are influenced by environmental factors outside their own control, for example, “No matter how hard I work on taking care of my teeth, I still get tooth decay”.36 The SE dimension evaluates people’s beliefs concerning their own capability to affect a specific situation,38 for example, “I believe I know how to brush my teeth correctly”.36 The OHBC dimension evaluates faulty and irrational beliefs about dental disease,38 for example, “Once gum disease has started it is almost impossible to stop”.36 The responses in DCBS are listed on a scale, with five options ranging from “strongly agree” to “strongly disagree”, including a “do not know” option.34
The Handbook of Healthcare was the second questionnaire used in the study and is based on questions regarding knowledge about oral health needs in care-dependent elderly. It was retrieved from www.vardhandboken.se, which is a website that was initiated by the Swedish Association of Local Authorities and Regions to provide education and support to care providers. The questionnaire consists of nine questions about the use of dental prostheses and how to clean them, oral dryness, oral hygiene performance, Revised Oral Health Assessment Guide (ROAG), etc. Each correct answer gives 1 point and zero points are awarded for incorrect answers.35
Statistics
The data collected at baseline were presented with mean values and standard deviations (SD) or as frequencies. The results were presented with changes from baseline to the three- and six-month follow-ups in frequency tables. Comparisons between Group I and Group C were made using Fisher’s exact test. P values <0.05 (95% CI) were considered statistically significant.
Statistical methods used for the knowledge and attitude questionnaires were two-way variance analysis (ANOVA) and Fisher’s exact test.
The participants (both the residents and the nursing staff) were treated as independent groups during analysis. The study was originally planned to last for one year but was concluded at six months due to financial reasons.
Results
Residents
The mean number of natural teeth was 20.2 (SD 3.0) and 26% of the study participants received assisted oral care. Ninety-six percent had contact with dental care providers in the previous year. The mean prescribed medication was 9.7 (SD 3.8) and 29% of the participants were registered with dry mouth according to self-experienced reports and the mirror-sliding friction test. A total of 14 participants used their electric toothbrush daily and strained food was medically prescribed for 3% of the participants. Additional baseline data are presented in Table 1. Of the 146 included residents, a total of 124 residents completed the entire study. Reasons for dropouts were events of death or hospitalization. There were more women than men in the total study material but no statistical difference between Groups I and C existed at baseline.
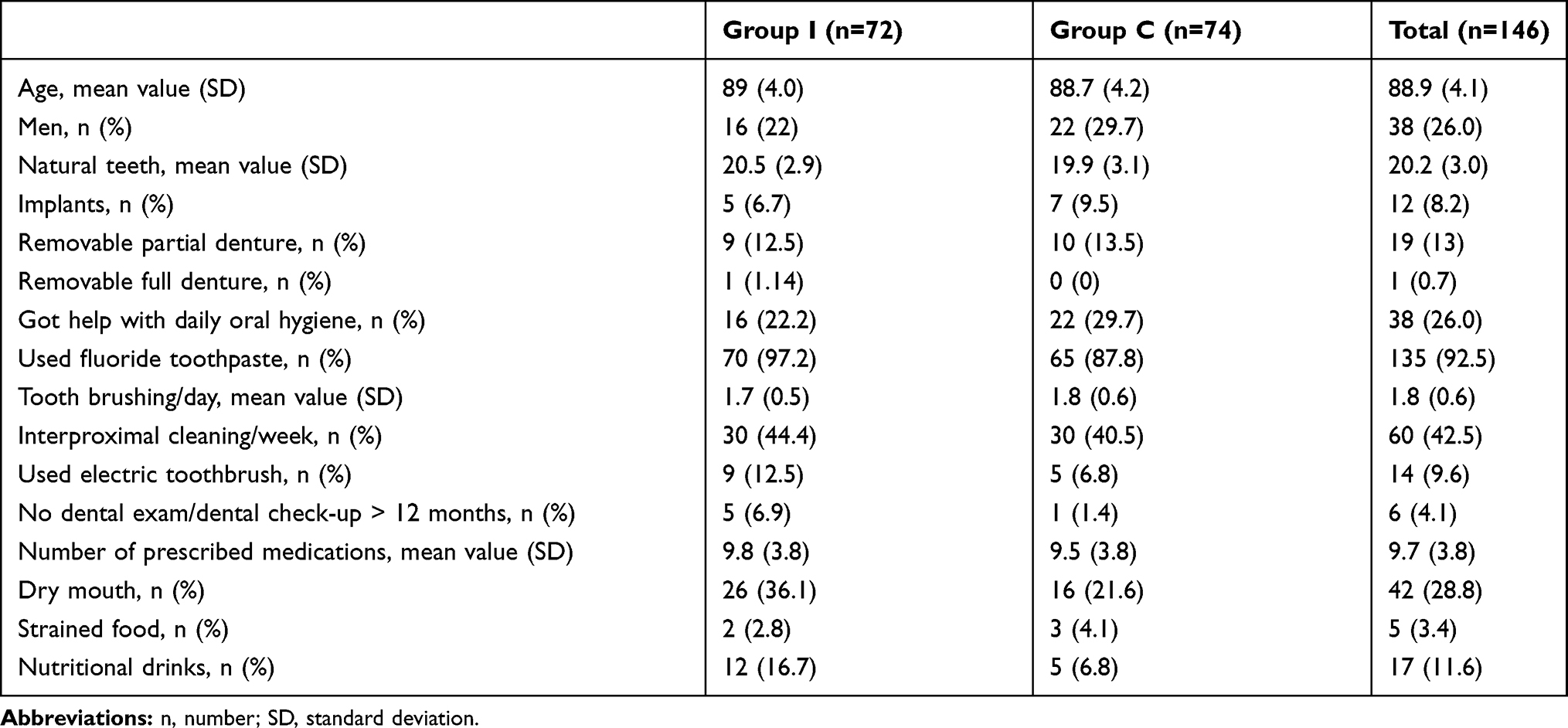 |
Table 1 Baseline Data For Residents |
Oral Hygiene and Root Caries
For MPS, improvements from baseline to six-month follow-up were seen in both Group I and Group C. Both groups showed improved PS, but without significance. For MS, a significant difference between Group I and Group C (p=0.04) was seen within the period between the three- and six-month follow-ups. In Group I, 20% of the participants showed improved MS, in comparison with 13% in Group C (Tables 2–4).
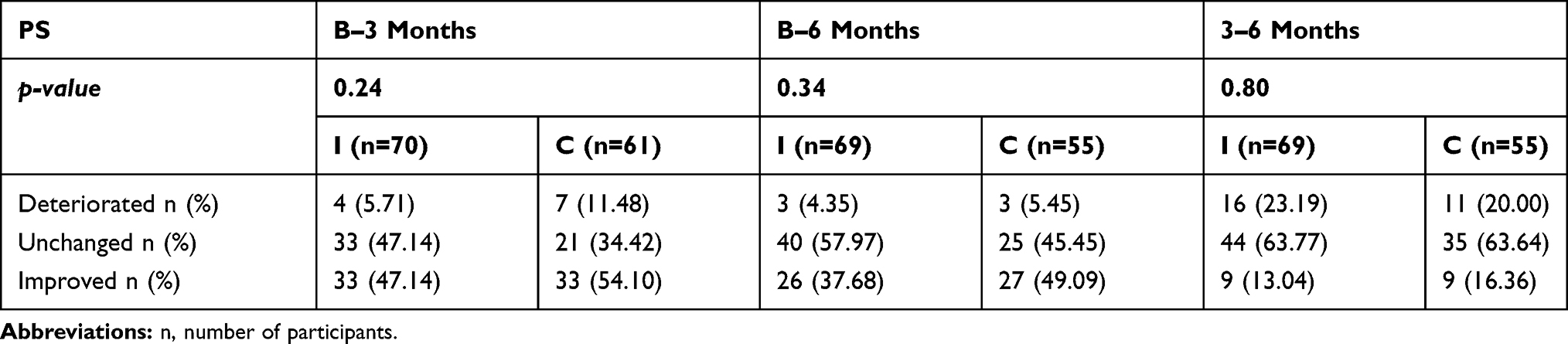 |
Table 2 Plaque Score (PS) from Baseline (B) Among The Intervention (I) and Control (C) Group to Three- and Six-Month Follow-Ups |
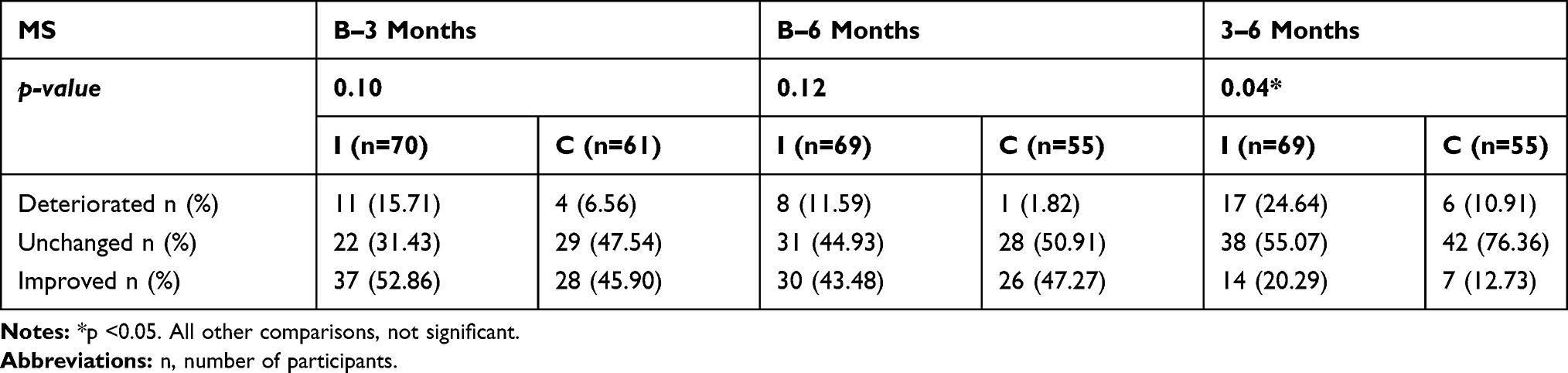 |
Table 3 Mucosal Score (MS) from Baseline (B) Among the Intervention (I) and Control (C) Group to Three- and Six-Month Follow-Ups |
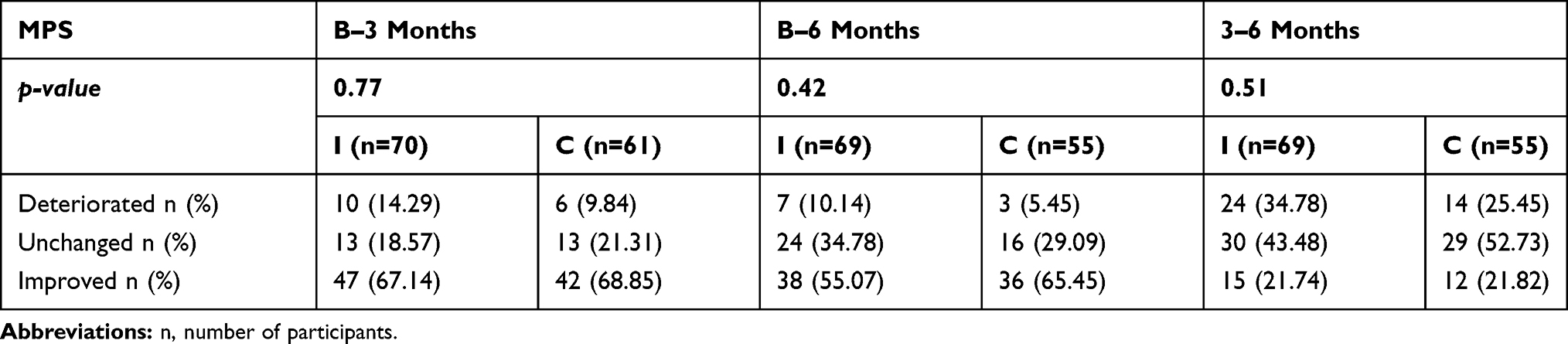 |
Table 4 Mucosal And Plaque Score (MPS) from Baseline (B) Among the Intervention (I) and Control (C) Group to Three- And Six-Month Follow-Ups |
The MSB index was combined and is presented as MSB 0+1 and MSB 2+3. For Group I and Group C, an improvement throughout the study could be seen within the groups (Table 5).
 |
Table 5 Modified Sulcus Bleeding Index (MSB) at Baseline (B), and After Three- And Six-Month (M) Follow-Ups and Difference (Diff) Between Time, Intervention (I) and Control (C) Group |
The root caries index was reduced from five levels to three and is presented as healthy (caries score of 1), initial caries lesion (caries score of 2 and 4) and active caries lesion (caries score of 3 and 5). Improvements were seen in both Group I and Group C for healthy and initial caries lesions throughout the study period, without significant difference between the groups. The last follow-up period between three to six months showed improvement for Group I regarding active caries lesions, with an improvement of 17% in comparison with 4% in Group C (p=0.05) (Table 6–8).
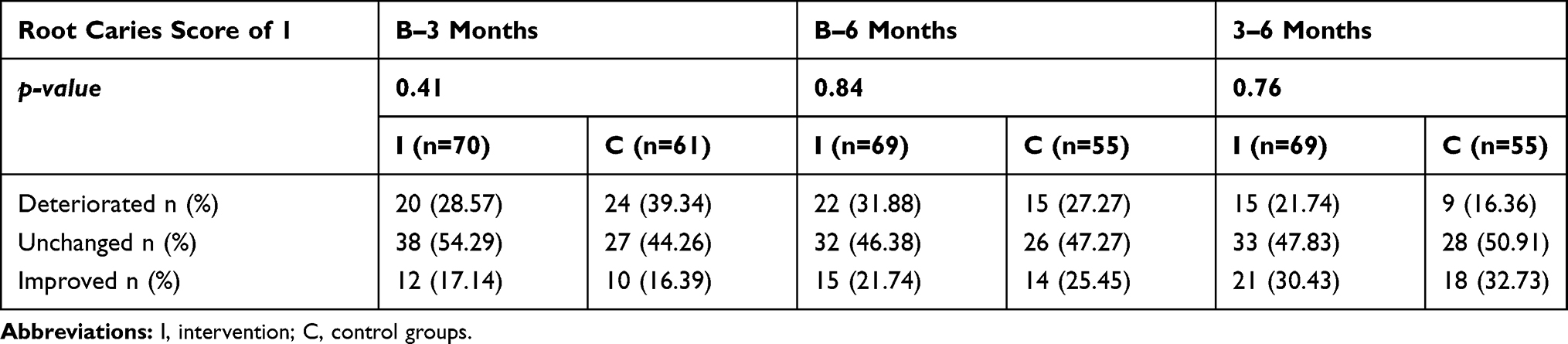 |
Table 6 Root Caries Score of 1 Among The Participants (n) At Baseline (B) And Three- And Six-Month Follow-Ups |
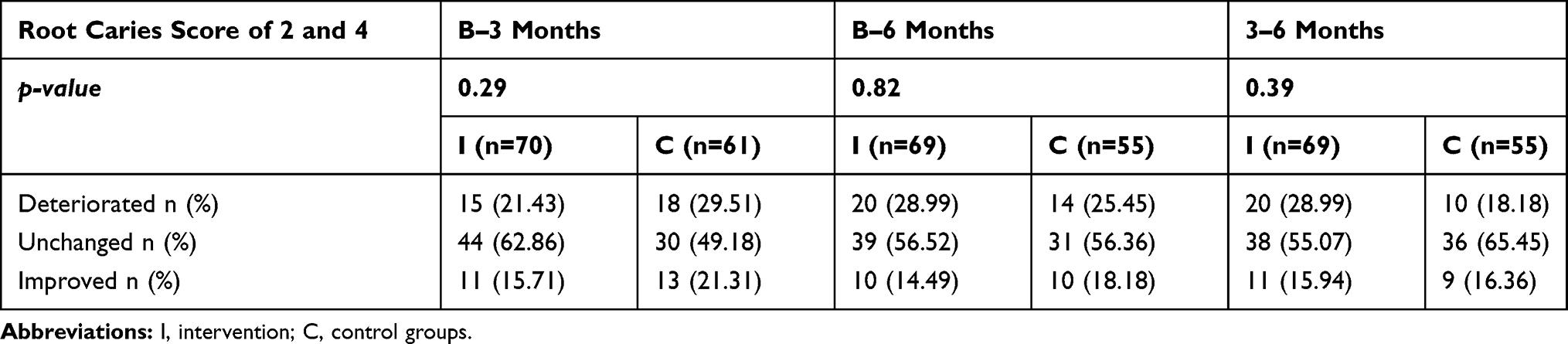 |
Table 7 Root Caries Score of 2 and 4 Among the Participants (n) at Baseline (B) and Three- And Six-Month Follow-Ups |
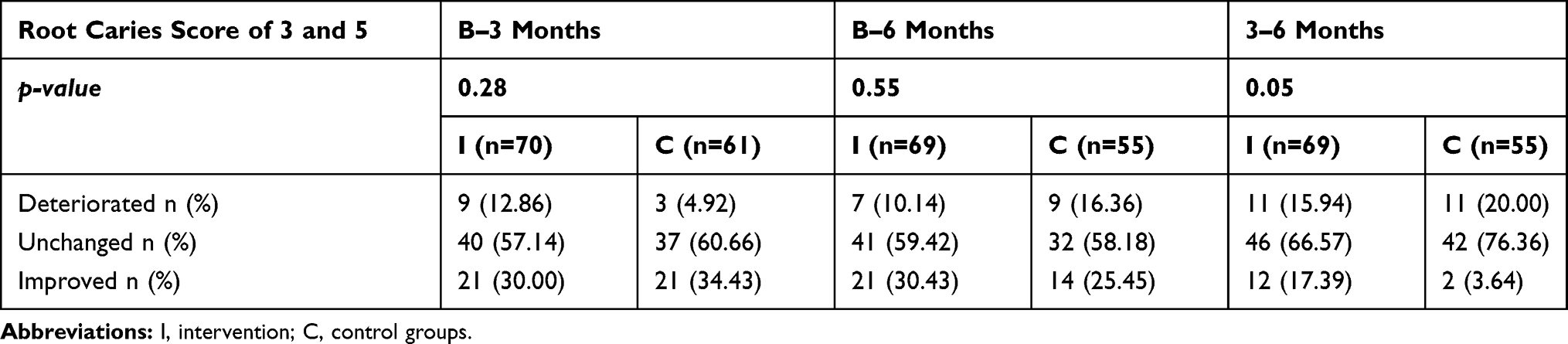 |
Table 8 Root Caries Score of 3 and 5 Among the Participants (n) at Baseline (B) and Three- and Six-Month Follow-Ups |
Nursing Staff
The Nursing Staff’s Knowledge and Attitudes
The intervention group showed a statistically significant improvement in comparison with the control group in the OHCB dimension (p=0.03) and EL dimension (p=0.0017). In the identified group, there was a statistically significant difference in the IL dimension group (p=0.03).
For the knowledge-based questionnaire, an improvement (p=0.05) was found between the intervention and the control group from baseline to six-month follow-up.
Discussion
The present study was a part of a project with the aim to evaluate regular professional cleaning and information/instructions regarding oral health care performed in nursing homes.2 It concluded that professional cleaning has a favourable effect on gingival bleeding, and verbally given individual oral hygiene instruction resulted in greater reduction of dental plaque, which indicates that both education and individual oral hygiene instruction with “hands-on” training ought to be included in domiciliary oral health care programmes.2 In the present study, the intervention has therefore been a combination of these two parts. Furthermore, a root caries index and the knowledge and attitudes of nursing staff towards oral health care were added to the study design.
The indexes used in the study are somewhat subjective since they are performed to estimate the amount of plaque, gingivitis, root caries and mucosal status by visual assessment. For this reason, calibration was performed in this study between the three RDHs collecting data to minimize differences in the assessment tasks. The present study chose the instrument and index for their simple equipment and ease of use and because they are preferable when performing a study in a home environment. According to the World Health Organization (WHO), “The examination for dental caries should be conducted with a plane mouth mirror. The use of radiography for detection of approximal caries is not recommended because the equipment is impractical to utilize in most field situations”.39
Statistical adjustment for background variables was not performed, as they showed no skewness, neither for age nor gender. In the present study, twenty study participants dropped out due to death or hospitalization during the study period, one in Group I and nineteen in Group C (Figure 1). The inclusion criterion of 85 years of age or older is challenging as dropouts due to hospitalization and death are expected.6 The first study in the project included residents ≥65 years of age2 and, considering the age-distribution differences between the first study and the current study, the shorter life expectancy among men40 could be a clarifying factor in the overrepresentation of women seen in the current study. This was somewhat expected as it reflects the natural gender distribution in nursing homes, where women are commonly in the majority.41 We intended to follow the residents for one year but, due to financial constraints, we concluded the study at six months, which is a limitation that probably impacted the results. On the other hand, the surviving proportion of a long-lasting study of nursing home residents is challenging because these participants may represent the healthiest ones, which can also produce misleading results. This could be a potential reason for the improved results in Group C, considering the high dropout rate in this group from baseline to six-month follow-up.
A systematic evaluation of systematic reviews by Ástvaldsdóttir et al (2018)42 presented some observations regarding cost-effectiveness within oral health and dental care for older persons. For example, training in oral health for nursing staff could be cost-effective if duplicated elements were avoided. Another observation regarding cost-effectiveness was that improvements in oral hygiene reduced the risk of pneumonia and could benefit both the health of the older person and the overall cost of care. In Sweden, domiciliary dental care has seemed to lower the societal cost in general compared with dental care at a fixed clinic, but more investigation and scientific evidence are needed to draw any conclusions. To our knowledge, recommendations for domiciliary dental care are lacking, which in the present study has led to difficulties understanding whether prevention through monthly visits by RDHs is economically defensible. For PS (Table 2), improvements in both groups were similar during the study period. Conclusions that may be drawn from the study are that visits every three months could be sufficient to enable prevention, and that the study’s findings might demonstrate the importance of instructing nursing staff to perform assisted oral care, where the presence of RDH once per month could be beneficial since regular “hands-on” training is effective to learn and build the confidence to perform a task.4
Only 29% of the participants were found to be suffering from oral dryness despite a high number of prescribed drugs (mean of 9.7). The results were largely in line with a review by Delwel et al (2018),17 in which various studies showed that xerostomia or self-reported oral dryness was present in 9.1% to 45%, in contrast to 8.4% to 20% in the controls. The mirror-sliding test28 used in this study is included in the validated screening instrument ROAG. It is subjective and not intended to diagnose oral problems, but used to identify individuals at risk of poor oral health.43 For that reason, the results for oral dryness should be interpreted with caution, as well as the fact that measurements were performed at different times of the day and not standardized. Furthermore, xerostomia often does not correspond with the measured salivation rate.44
The MSB and root caries index were grouped to enable the analysis, after consulting statistical expertise. Throughout the study, a tendency for improvement in MSB, MPS and root caries was seen both in Group I and Group C. Potential reasons for the improvements in Group C could be the oral health instruction they received both verbally and in writing at the beginning of the study, as well as the toothbrush and toothpaste they received free of charge. This could have been a reminder to take care of their daily oral hygiene throughout the study period. Furthermore, as mentioned previously, the high dropout rate could have an impact on the results, with survivors potentially consisting of those who were healthiest and best able to handle their daily oral hygiene properly. Also, the awareness of being included in a study could have an effect on the results. The MPS (p=0.04) showed statistical significance in the last time period, from the three- to six-month follow-up, indicating that a prolonged study period is required to show possible changes due to an intervention in this study context.45
In the assessment of the root caries, the dental hygienist who performed the follow-up exams was blinded and unaware of which tooth was examined at baseline. The Silness-Loe index teeth12,16,24,32,36,44 was used, but if missing, the nearest tooth was chosen,32 leading to the possibility that another tooth was examined at the follow-up exams (due to acute extraction, for example). This is a limitation of the study design and choice of tooth should be documented in the following studies.
The Nursing DCBS and the knowledge-based questionnaire showed improvements regarding attitude and knowledge to oral health care and needs. The OHCB (p=0.03) and the EL dimension (p=0.0017) showed significant improvement in the intervention group in comparison with the control group, indicating that the nursing staff improved their knowledge and beliefs in oral health (OHCB) and increased in their responsibility and self-control (EL) over the oral health care among residents. This also indicates that visits by a dental hygienist once per month affect the attitude and knowledge of oral health care among nursing staff. Samson et al (2009)46 showed that improved knowledge among nursing staff contributed to improved oral hygiene among the care-dependent elderly and Coker et al (2014)47 addressed the importance of further studies about improving nurses’ ability to perform oral hygiene care in elderly patients. However, the participation of nursing staff in questionnaire-based studies is challenging due to low response rates,48,49 which was also experienced in the present study. The reasons for dropouts could be changes in workplace, lack of interest and lack of time. Some of the nursing staff had difficulties remembering their four-digit code from baseline to follow-up, and because of this, the identified group probably contained fewer participants at follow-up than it could have. The study showed significant results both in the Nursing DCBS and the knowledge-based questionnaire, but the results should be interpreted with caution due to the small study sample.
In Sweden, about 20 – 21% of the nursing homes are managed by private companies.1 The National board of Health and Welfare (2012)50 investigated the differences in quality of care between nursing homes managed by private companies and those managed by municipalities, but the results differed and it was hard to draw any conclusions. In the present study, no comparison was performed between urban and rural areas nor between nursing homes managed by private companies and those managed by municipalities, which could be interesting to investigate for future studies.
The oral health of care-dependent elderly living in nursing homes is frequently poor16,47,51 and often less prioritized than other nursing tasks.47,52 Education, information and instructions alone have been shown to have an insufficient effect on the oral health of care-dependent elderly,51 a finding corroborated by this project in the first study.2 Frequent visits from dental hygienists can be a new approach to create better guidance for the nursing staff to achieve improved oral health among care-dependent residents.26 With today’s complicated oral health scenario with older people receiving home care, the dental profession needs to be more available for the nursing staff to provide education and support in oral health care,53 and dental professionals need to be included in the standard team for care of the elderly. Today, dental professionals are only included as consultants.54 If collaboration between health care and dental care improves, both oral and general health could benefit from this alliance and be improved among the individuals.53 This is especially important in situations where dependent individuals do not regularly meet dental care providers, such as in the case of home care. As beds in nursing homes are decreasing,40 and daily care support today is frequently provided by home care aides in the care recipients’ own homes, we intend to take the intervention model further into this context.
Conclusion
Monthly professional oral care, combined with individual oral health care instructions, seems to improve oral hygiene and may reduce root caries among nursing home residents. This may also contribute to a more positive attitude regarding oral hygiene measures among nursing home staff, as compared with daily oral care as usual.
Acknowledgments
We thank the study participants and Tommy Johnson at the University of Gothenburg Institution of Odontology for help with statistical analysis. We thank dentist Elin Strömberg and dental hygienists Fridha Okoth Carlén, Nasita Marson and Ulrika Sjöblom for data collection, and dental hygienist Maria Juslin for education of the nursing staff. We also thank Marie Olsson at Comprendo for assistance with the language review.
Disclosure
Petteri Sjögren is employed by a dental company, Oral Care AB. The authors declare that they have no other possible conflicts of interest in this work.
References
1. Welfare NBoHa. Statistik om äldre och personer med funktionsnedsättning efter regiform; 2018. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2019-2-20.pdf.
2. Sjögren P, Girestam C, Skott P, et al. Professional domiciliary oral care for elderly in nursing homes a randomized controlled pilot trial. Health. 2016;08:1112–1119. doi:10.4236/health.2016.811116
3. Wårdh I, Jonsson M, Wikström M. Attitudes to and knowledge about oral health care among nursing home personnel an area in need of improvement. Gerodontology. 2012;29(2):e787792. doi:10.1111/j.1741-2358.2011.00562.x
4. Keboa M, Beaudin A, Cyr J, et al. Dentistry and nursing working together to improve oral health care in a long-term care facility. Geriatr Nurs. 2019;40(2):197–204. doi:10.1016/j.gerinurse.2018.10.002
5. Gronbeck-Linden I, Hagglin C, Petersson A, Linander PO, Gahnberg L. Discontinued dental attendance among elderly people in Sweden. J Int Soc Prev Community Dent. 2016;6(3):224–229. doi:10.4103/2231-0762.183101
6. Muszalik M, Kornatowski T, Zielinska-Wieczkowska H, Kedziora-Kornatowska K, Dijkstra A. Functional assessment of geriatric patients in regard to health-related quality of life (HRQoL). Clin Interv Aging. 2015;10:61–67. doi:10.2147/CIA.S72825
7. Nordenram G, Ljunggren G. Oral status, cognitive and functional capacity versus oral treatment need in nursing home residents: a comparison between assessments by dental and ward staff. Oral Dis. 2002;8(6):296–302. doi:10.1034/j.1601-0825.2002.01788.x
8. Peltola P, Vehkalahti MM, Wuolijoki-Saaristo K. Oral health and treatment needs of the long-term hospitalised elderly. Gerodontology. 2004;21(2):93–99. doi:10.1111/j.1741-2358.2004.00012.x
9. van der Putten GJ, de Baat C, De Visschere L, Schols J. Poor oral health, a potential new geriatric syndrome. Gerodontology. 2014;31(Suppl 1):17–24. doi:10.1111/ger.12086
10. Afshar S, Roderick PJ, Kowal P, Dimitrov BD, Hill AG. Multimorbidity and the inequalities of global ageing: a cross-sectional study of 28 countries using the world health surveys. BMC Public Health. 2015;15:776. doi:10.1186/s12889-015-2008-7
11. Billings RJ, Proskin HM, Moss ME. Xerostomia and associated factors in a community-dwelling adult population. Community Dent Oral Epidemiol. 1996;24(5):312–316. doi:10.1111/j.1600-0528.1996.tb00868.x
12. Hagglund P, Koistinen S, Olai L, Stahlnacke K, Wester P, Levring Jaghagen E. Older people with swallowing dysfunction and poor oral health are at greater risk of early death. Community Dent Oral Epidemiol. 2019;47:494–501. doi:10.1111/cdoe.12491
13. Terezakis E, Needleman I, Kumar N, Moles D, Agudo E. The impact of hospitalization on oral health: a systematic review. J Clin Periodontol. 2011;38(7):628–636. doi:10.1111/j.1600-051X.2011.01727.x
14. Valdez IH, Fox PC. Diagnosis and management of salivary dysfunction. Crit Rev Oral Biol Med. 1993;4(34):271–277. doi:10.1177/10454411930040030301
15. Narhi TO. Prevalence of subjective feelings of dry mouth in the elderly. J Dent Res. 1994;73(1):20–25. doi:10.1177/00220345940730010301
16. Chalmers J, Pearson A. Oral hygiene care for residents with dementia: a literature review. J Adv Nurs. 2005;52(4):410–419. doi:10.1111/j.1365-2648.2005.03605.x
17. Delwel S, Binnekade TT, Perez R, Hertogh C, Scherder EJA, Lobbezoo F. Oral hygiene and oral health in older people with dementia: a comprehensive review with focus on oral soft tissues. Clin Oral Investig. 2018;22(1):93–108. doi:10.1007/s00784-017-2264-2
18. Dermont MA, Sadaghiani SS. Integrating oral health into a dementia care pathway. Community Dent Health. 2014;31(4):196–199.
19. Ishimaru M, Ono S, Morita K, Matsui H, Yasunaga H. Domiciliary dental care among homebound older adults: A nested case-control study in Japan. Geriatr Gerontol Int. 2019;19(7):679–683. doi:10.1111/ggi.13676
20. Webb BC, Whittle T, Schwarz E. Oral health and dental care in aged care facilities in New South Wales, Australia. Part 3 concordance between residents’ perceptions and a professional dental examination. Gerodontology. 2016;33(3):363–372. doi:10.1111/ger.12170
21. Sjogren P, Wardh I, Zimmerman M, Almstahl A, Wikstrom M. Oral care and mortality in older adults with pneumonia in hospitals or nursing homes: systematic review and meta-analysis. J Am Geriatr Soc. 2016;64(10):2109–2115. doi:10.1111/jgs.14260
22. O’Donnell LE, Smith K, Williams C, et al. Dentures are a reservoir for respiratory pathogens. J Prosthodont. 2016;25(2):99–104. doi:10.1111/jopr.12342
23. Iinuma T, Arai Y, Abe Y, et al. Denture wearing during sleep doubles the risk of pneumonia in the very elderly. J Dent Res. 2015;94(3 Suppl):28S36S. doi:10.1177/0022034514552493
24. Barbe AG, Kottmann HE, Derman SHM, Noack MJ. Efficacy of regular professional brushing by a dental nurse for 3 months in nursing home residents a randomized, controlled clinical trial. Int J Dent Hyg. 2019;17(4):327–335. doi:10.1111/idh.12389
25. Komulainen K, Ylostalo P, Syrjala AM, et al. Preference for dentist’s home visits among older people. Community Dent Oral Epidemiol. 2012;40(1):89–95. doi:10.1111/j.1600-0528.2011.00631.x
26. Seleskog B, Lindqvist L, Wardh I, Engstrom A, von Bultzingslowen I. Theoretical and hands-on guidance from dental hygienists promotes good oral health in elderly people living in nursing homes, a pilot study. Int J Dent Hyg. 2018;16(4):476–483. doi:10.1111/idh.12343
27. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23(10):433–441. doi:10.1111/j.1532-5415.1975.tb00927.x
28. Henricsson V, Svensson A, Olsson H, Axell T. Evaluation of a new device for measuring oral mucosal surface friction. Scand J Dent Res. 1990;98(6):529–536. doi:10.1111/j.1600-0722.1990.tb01008.x
29. Doyle DJ, Goyal A, Bansal P, Garmon EH. American Society of Anesthesiologists Classification (ASA Class) [Updated 2020 July 4]. In: StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441940/ Treasure Island FL: StatPearls Publishing LLC; 2020: 1–3.
30. Henriksen BM, Ambjornsen E, Axell TE. Evaluation of a mucosal-plaque index (MPS) designed to assess oral care in groups of elderly. Spec Care Dentist. 1999;19(4):154–157. doi:10.1111/j.1754-4505.1999.tb01378.x
31. Greene JC, Vermillion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13. doi:10.14219/jada.archive.1964.0034
32. Benamghar L, Penaud J, Kaminsky P, Abt F, Martin J. Comparison of gingival index and sulcus bleeding index as indicators of periodontal status. Bull World Health Organ. 1982;60(1):147–151.
33. Fejerskov O, Luan WM, Nyvad B, Budtz-Jorgensen E, Holm-Pedersen P. Active and inactive root surface caries lesions in a selected group of 60- to 80-year-old Danes. Caries Res. 1991;25(5):385–391. doi:10.1159/000261396
34. Wardh I, Sorensen S. Development of an index to measure oral health care priority among nursing staff. Gerodontology. 2005;22(2):84–90. doi:10.1111/j.1741-2358.2005.00063.x
35. Healthcare T The Handbook for Healthcare; 2018 [
36. Wolfe GR, Stewart JE, Hartz GW. Relationship of dental coping beliefs and oral hygiene. Community Dent Oral Epidemiol. 1991;19(2):112–115. doi:10.1111/j.1600-0528.1991.tb00123.x
37. Pihlajamaki T, Syrjala AM, Laitala ML, Pesonen P, Virtanen JI. Oral health care-related beliefs among Finnish geriatric home care nurses. Int J Dent Hyg. 2016;14(4):289–294. doi:10.1111/idh.12227
38. Wolfe GR, Stewart JM, Maeder LA, Hartz GW. Use of dental coping beliefs scale to measure cognitive changes following oral hygiene interventions. Community Dent Oral Epidemiol. 1996;24(1):37–41. doi:10.1111/j.1600-0528.1996.tb00810.x
39. Organization WH. Oral Health Surveys: Basic Methods.
40. Welfare N Vård och omsorg om äldre Lägesrapport; 2019. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2019-3-18.pdf.
41. Welfare TNBoHa. Äldre: Vård Och Omsorg Den 1 Oktober 2012: Kommunala Insatser Enligt Socialtjänstlagen Samt Hälso- Och Sjukvårdslagen. Stockholm: Socialstyrelsen; 2013.
42. Ástvaldsdóttir Á, Boström AM, Davidson T, et al. Oral health and dental care of older persons-A systematic map of systematic reviews. Gerodontology. 2018;35(4):290–304. doi:10.1111/ger.12368
43. Andersson P, Hallberg IR, Renvert S. Inter-rater reliability of an oral assessment guide for elderly patients residing in a rehabilitation ward. Spec Care Dentist. 2002;22(5):181–186. doi:10.1111/j.1754-4505.2002.tb00268.x
44. Wiener RC, Wu B, Crout R, et al. Hyposalivation and xerostomia in dentate older adults. J Am Dent Assoc. 2010;141(3):279–284. doi:10.14219/jada.archive.2010.0161
45. Wardh IM, Wikstrom MB. Long-term effects of using oral care aides at a nursing home for elderly dependent residents–a pilot study. Spec Care Dentist. 2014;34(2):64–69. doi:10.1111/scd.12009
46. Samson H, Berven L, Strand GV. Long-term effect of an oral healthcare programme on oral hygiene in a nursing home. Eur J Oral Sci. 2009;117(5):575–579. doi:10.1111/j.1600-0722.2009.00673.x
47. Coker E, Ploeg J, Kaasalainen S. The effect of programs to improve oral hygiene outcomes for older residents in long-term care: a systematic review. Res Gerontol Nurs. 2014;7(2):87–100. doi:10.3928/19404921-20140110-01
48. Gagne MA, Dubois CA, Prud’Homme A, Borges Da Silva R. A cross-sectional study on workplace experience: a survey of nurses in Quebec, Canada. Hum Resour Health. 2019;17(1):20. doi:10.1186/s12960-019-0358-4
49. Salmi R, Tolvanen M, Suhonen R, Lahti S, Narhi T. Knowledge, perceived skills and activities of nursing staff to support oral home care among older domiciliary care clients. Scand J Caring Sci. 2018;32(4):1342–1347. doi:10.1111/scs.12579
50. Welfare N Kommunal eller enskild regi, spelar det någon roll? - en jämförelse av utförare av vård och omsorg om äldre; 2012. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2012-5-30.pdf.
51. Wikstrom M, Kareem KL, Almstahl A, Palmgren E, Lingstrom P, Wardh I. Effect of 12-month weekly professional oral hygiene care on the composition of the oral flora in dentate, dependent elderly residents: A prospective study. Gerodontology. 2017;34(2):240–248. doi:10.1111/ger.12256
52. Andersson M, Wilde-Larsson B, Carlsson E, Persenius M. Older people’s perceptions of the quality of oral care in short-term care units: A cross-sectional study. Int J Older People Nurs. 2018;13(2):e12185. doi:10.1111/opn.12185
53. Tornkvist L, Hegefjard C. Evaluation of interprofessional training in home care. J Interprof Care. 2008;22(5):509–520. doi:10.1080/13561820802234224
54. Pilotto A, Cella A, Daragjati J, et al. Three decades of comprehensive geriatric assessment: evidence coming from different healthcare settings and specific clinical conditions. J Am Med Dir Assoc. 2017;18(2):192e191192 e111. doi:10.1016/j.jamda.2016.11.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.