Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Dexmedetomidine Nasal Sprays on Postoperative Sleep Quality in Patients Who Underwent Laparoscopic Gynaecological Surgery: A Single-Centre, Double-Blind, Randomized Controlled Study
Authors Fan K, Ma J, Liu W, Chen X
Received 7 June 2025
Accepted for publication 3 October 2025
Published 15 October 2025 Volume 2025:19 Pages 9291—9302
DOI https://doi.org/10.2147/DDDT.S545452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Keke Fan,1 Junyi Ma,2 Wenxing Liu,2 Xi Chen3
1Department of Anesthesiology, Shenzhen Children’s Hospital, Shenzhen, Guangdong Province, People’s Republic of China; 2Department of Anesthesiology, Guangzhou Women and Children’s Medical Center, Guangzhou, Guangdong Province, People’s Republic of China; 3Department of Anesthesiology, The Third Affiliated Hospital of Southern Medical University, Guangzhou, Guangdong Province, People’s Republic of China
Correspondence: Xi Chen, Email [email protected]
Background: Dexmedetomidine nasal sprays is effective for perioperative sedation, analgesia, and anxiolysis. Nevertheless, its impact on postoperative sleep quality along with the optimal dosage and overall efficacy remains unclear in patients undergoing laparoscopic gynecological surgery.
Methods: A total of 150 adult patients undergoing laparoscopic gynecological surgery were enrolled, with 144 included in the final analysis. Patients in the dexmedetomidine (Dex) group received 50 μg of intranasal dexmedetomidine 30 minutes before sleep on the first postoperative night, while the control group received an equivalent volume of saline. Primary outcomes included objective sleep parameters (sleep duration, deep sleep duration, REM sleep duration and light sleep duration) measured via a portable sleep monitor, as well as subjective sleep parameters assessed by Athens Insomnia Scale (AIS) and Numerical Rating Scale (NRS) scores one night before and on the first night after surgery. Secondary outcomes comprised postoperative pain measured by VAS, nausea and vomiting, and average heart rate.
Results: The sleep duration, deep sleep duration and REM sleep duration of patients in the control group decreased after laparoscopic gynaecological surgery (vs preoperative control group, P=0.021, P< 0.001, P=0.005, respectively), whereas the fragmented sleep duration and NRS score increased (vs preoperative control group, P=0.017, P=0.032, respectively) . In contrast, those treated with dexmedetomidine (Dex group) exhibited significantly improved sleep quality postoperatively, with greater sleep duration, deep sleep duration, and REM sleep durations (vs control group, P< 0.001, P< 0.001, P< 0.001, respectively). There were no significant differences in postoperative pain or nausea and vomiting between the two groups.
Conclusion: Dexmedetomidine nasal sprays improved postoperative sleep quality in patients who underwent laparoscopic gynaecological surgery.
Trial Registration: Chinese Clinical Trial Registry (clinical trial number: ChiCTR2400080181).
Keywords: dexmedetomidine, nasal sprays, sleep disturbance, gynaecological surgery
Introduction
Sleep disorders are common during the perioperative period, with an incidence rate of approximately 8.8–79.1%.1–3 Postoperative sleep disorders (PSD) refer to changes in a patient’s early postoperative sleep quality and structure and are characterized by reduced REM sleep, an abnormal circadian rhythm and fragmented sleep.4–6 Previous studies have shown that the incidence of sleep disorders within one week after gynecological laparoscopic surgery is approximately 40–60%, which may be due to the fact that it covers high-risk factors for PSD, such as female sex, older age, postoperative nausea and vomiting, postoperative pain and anxiety.7,8 PSD may contribute to postoperative cognitive dysfunction and cardiovascular complications and affect postoperative recovery.9,10 Therefore, improving postoperative sleep quality may be beneficial for the recovery of surgical patients.
Dexmedetomidine has been effectively used for perioperative anaesthesia in patients because of its sedative, analgesic, and anxiolytic effects.11 Dexmedetomidine can induce deep sedation by increasing the deep sleep duration (N3 sleep) shown on electroencephalography (EEG)12 and nonrapid eye movement (NREM) sleep.13,14 Some studies have reported that dexmedetomidine can promote sleep in postoperative or intensive care unit (ICU) patients.15,16 Previous studies have indicated that dexmedetomidine is generally administered through intraoperative intravenous infusion or intranasal administration via a syringe.17,18 Compared with intravenous infusion, the administration of a dexmedetomidine nasal sprays is convenient, has a quick onset and is highly bioavailable.19 Intranasal administration via a syringe often fails to ensure precise dosing and optimal bioavailability, but dexmedetomidine nasal sprays can ensure bioavailability and a precise dosage. There is evidence that the dexmedetomidine nasal sprays is an effective method for treating PSD, it has been applied in paediatric examinations and has been shown to improve postoperative sleep quality in patients undergoing nasal endoscopic surgery.19–21 Therefore, in this study, the bioavailability and safety of dexmedetomidine administered via nasal spray were confirmed.
However, the effects of dexmedetomidine nasal sprays on postoperative sleep quality in patients undergoing laparoscopic gynecological surgery and the optimal dosage and overall effect remain unclear. This double-blind, randomized controlled study aimed to investigate the effects of dexmedetomidine nasal sprays on postoperative sleep quality the first night after surgery in patients who underwent laparoscopic gynaecological surgery.
Methods
Study Design
This was a randomized, double-blinded controlled trial conducted at the Guangzhou Women and Children’s Medical Center. The study protocol was approved by the Research Ethics Committee of Guangzhou Women and Children’s Medical Center on November 10, 2023 and was registered in the Chinese Clinical Trial Register (ChiCTR2400080181, http://www.chictr.org.cn). All participants signed informed consent forms before inclusion. A total of 150 patients who underwent laparoscopic gynaecological surgery and entered the operating room by 8:00 am at Guangzhou Women and Children’s Medical Center between January 2024 and October 2024 were enrolled.
Participants
The inclusion criteria were as follows: (1) patients aged 18–60 years; (2) patients who had an American Society of Anaesthesiologists (ASA) classification of I or II; (3) patients who were scheduled to undergo laparoscopic gynaecological surgery; and (4) patients who entered the operating room by 8:00 am. The exclusion criteria were as follows: (1) patients who had poor preoperative sleep quality (a Pittsburgh Sleep Quality Index (PSQI) score ≥ 7 points or an Insomnia Severity Index (ISI) score ≥ 8 points),8 (2) patients who had obstructive sleep apnoea hypopnea syndrome; (3) patients who were taking sedatives or antidepressants or had drug or alcohol dependence; (4) patients taking any other regular medications (such as central nervous system stimulants, antipsychotic drug, antiepileptics) that affect sleep (5) patients who could not cooperate for any reason; (6) patients who had a history of mental illness, cardiovascular disease, nasopharyngeal carcinoma, nosebleeds, or other nasal diseases; and (7) patients who refused to participate in the study.
Randomization and Blinding
For this study, we included 150 participants who underwent laparoscopic gynaecological surgery and entered the operating room by 8:00 am. A computer-generated random number table (http://www.randomization.com) was used for group randomization. The participants were assigned to two groups at a ratio of 1:1, namely, the control group (n=75) and the 50µg dexmedetomidine (Dex) group (n=75). Independent researchers who did not participate in the experimental process were responsible for the preoperative evaluation and postoperative follow-up. Additionally, the patients were blinded to the groupings.
Interventions and Intraoperative Management
The following data were collected by the investigators before surgery: baseline patient data, including age, body weight, body mass index (BMI), ASA classification, and PSQI score;22 data on objective sleep quality, including sleep duration, deep sleep duration, REM sleep duration, and light sleep duration, measured via a portable sleep monitor (WSM-LN-01, Guangzhou Zhongke Xinzhi Technology Co., Ltd).; and data on subjective sleep quality, measured via the Athens Insomnia Scale (AIS) and numerical rating scale (NRS) scores.16,23
After entering the operating room, the patients underwent standard perioperative monitoring, including oxygen saturation (SpO2), noninvasive blood pressure (NIBP), and electrocardiogram monitoring. Tracheal intubation was performed with the following drugs: propofol (2mg.kg−1), sufentanil (0.3-0.5µg.kg−1), and cisatracurium (2mg.kg−1). The maintenance medications used included 2% sevoflurane and remifentanil (0.2ug.kg−1 min−1). Patient blood pressure was maintained at 20% of the baseline level throughout the entire surgical period. After surgery, the tracheal tube was removed by an anaesthesiologist in the operating room when the patients were awake. Postoperative pain was controlled through patient-controlled intravenous analgesia (PCIA) with sufentanil (100ug), a total volume of 120 mL of physiological saline, at an infusion rate of 2 mL. h−1, a push infusion of 0.5 mL, and a locking time of 15 minutes. Patients in the control group received an equivalent volume of saline, and patients in the Dex group received a dexmedetomidine nasal sprays (50µg) (H20230006, Shanghai Hengrui Pharmaceutical Co., Ltd). 30 minutes before going to sleep on the first postoperative night. The administration method was as follows: before the first use, it was necessary to pre-spray 7 times to activate the nasal spray pump. The administration of the dexmedetomidine nasal sprays was performed by medical personnel as follows: the patients were asked to sit with their head tilted forwards, and the delivery device was kept upright and sprayed into the nasal cavity, for a total of 2 sprays (1 spray in each nostril; totalling 50 μg).
Surgical Ward Conditions
All patients stayed in a 3-bedroom ward with a room temperature ranging from 18–22°C and a humidity ranging from 50–60%. Each hospital bed had independent bed curtains and independent light control switches to reduce the impact of noise and light on sleep. In general, the postoperative ward remained quiet, and the lights were turned off at night.
Surgical Classification
The following surgeries were considered simple surgeries: laparoscopic oophorocystectomy, laparoscopic salpingo-oophorectomy and laparoscopic myomectomy. Complex surgery was defined as laparoscopic hysterectomy.
Outcome Measurements
The primary outcomes were as follows: objective sleep quality, including sleep duration, deep sleep duration, light sleep duration, and REM sleep duration, measured via a portable sleep monitor; and subjective sleep quality, measured via the AIS and NRS one night before surgery and on the first postoperative night. The NRS score and AIS score (≥6 points) are used to determine whether a patient’s sleep quality is poor.16,24 The secondary outcomes included the ; surgical classification; postoperative pain, which was measured via the VAS (total possible score of 0–10 points; 0 points = no pain; 1–3 points = mild pain; 4–6 points = moderate pain; and 7–10 points = severe pain); postoperative nausea and vomiting (PONV), which was measured by PONV Severity Score (0= None; 1=Mild; 2= moderate 3= severe) and the average heart rate.25
Sample Size Calculation and Statistical Analysis
Previous studies have shown that postoperative sleep quality can be estimated by the NRS, with an NRS score of 6 points or higher considered to indicate poor sleep quality;16,24,26 therefore, we evaluated postoperative sleep quality via the NRS score on the first night after surgery in. An NRS score >6 points was considered to indicate poor sleep quality. According to the results of the pilot study, 25% of patients in the control group had NRS > 6, while, 7% of patients in the Dex group had NRS > 6. We recruited 60 patients in the pilot study, 2 patients were excluded due to not meeting inclusion criteria. Finally, patients in control group (n=30) received an equivalent volume of saline and patients in dexmedetomidine (Dex) group (n=28) received dexmedetomidine nasal sprays (50ug) 30 minutes before sleep on the first postoperative night. According to the results of the pilot study, 25% of patients in the control group had NRS > 6, while, 7% of patients in the Dex group had NRS > 6. This study included 150 patients on the basis of the assumption of a bilateral alpha threshold of 0.05, a power (1 beta) of 80%, and a dropout and follow-up loss rate of 10%. Statistical analysis was conducted using IBM SPSS Statistics for Windows software (version 26.0; IBM Corp., Armonk, NY, USA). The distribution of continuous data was analysed via the Kolmogorov‒Smirnov test. The independent sample t-test was used to compare differences between groups for data that conformed to a normal distribution. The Mann‒Whitney test was used to compare differences between groups for data that did not conform to a normal distribution. A paired t-test was used to compare differences between preoperative and postoperative data that conformed to a normal distribution within groups. The Wilcoxon signed rank test was used to compare differences between preoperative and postoperative data that did not conform to a normal distribution within groups.
Results
Study Population
A total of 150 patients were enrolled in the study; 2 patients were excluded because they did not meet the inclusion criteria, 2 patients were excluded because they refused to participate, and 2 patients were excluded because they were transferred to the ICU after surgery. Ultimately, 144 participants were included in the statistical analysis (Figure 1). The basic clinical data of all patients are shown in Table 1. There were no significant differences between the control group and the Dex group in terms of age, body weight, BMI, ASA classification, PSQI score, surgical complexity, surgical duration or anaesthesia duration.
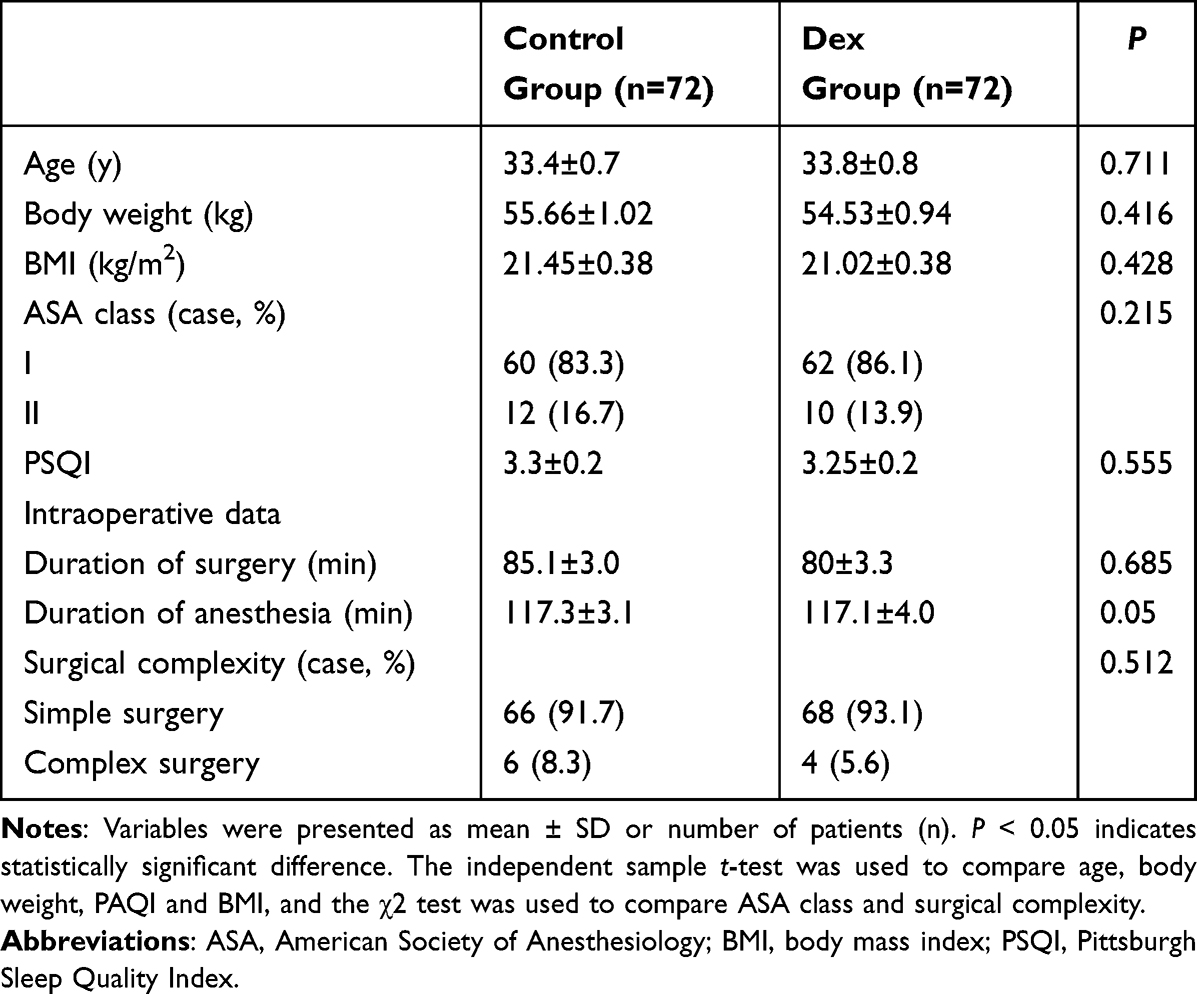 |
Table 1 Clinical Characteristic of Patients in Control Group and Dex Group |
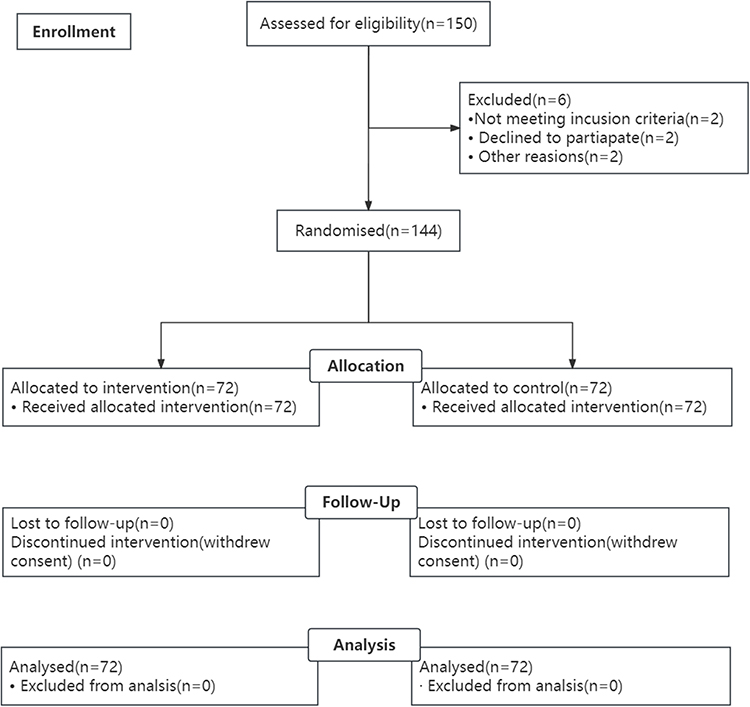 |
Figure 1 Consolidated standards of reporting trials flowchart of the study. |
Primary Outcomes
As shown in Figure 2A, the postoperative sleep duration was shorter than the preoperative sleep duration in the control group (P = 0.021), whereas there was no significant difference in the Dex group. Compared with that in the control group, the postoperative sleep duration in the Dex group was longer (P < 0.001). As shown in Figure 2B, the postoperative deep sleep duration was shorter than the preoperative deep sleep duration in the control group (P < 0.001), whereas there was no significant difference in the Dex group. Compared with that in the control group, the postoperative deep sleep duration in the Dex group was longer (P < 0.001). As shown in Figure 2C, there were no significant differences between the preoperative light sleep duration and postoperative light sleep duration in the control and Dex groups (P > 0.05). There were also no significant differences in postoperative light sleep duration between the Dex group and the control group (P > 0.05). As shown in Figure 2D, the postoperative awakening duration was longer than the preoperative awakening duration in the control group (P = 0.017), whereas there was no significant difference in the Dex group. Compared with that in the control group, the postoperative awakening duration in the Dex group was shorter (P < 0.001). As shown in Figure 2E, the postoperative REM sleep duration was shorter than the preoperative REM sleep duration in the control group (P = 0.005), whereas there was no significant difference in the Dex group. Compared with that in the control group, the postoperative REM sleep duration in the Dex group was longer (P < 0.001). As shown in Figure 2F, there were no significant differences between the preoperative sleep cycle and postoperative sleep cycle in the control and Dex groups (P > 0.05). There were also no significant differences between the control and Dex groups in the postoperative sleep cycle (P > 0.05). As shown in Figure 2G, there were no significant differences between the preoperative sleep efficiency and postoperative sleep efficiency in the control and Dex groups (P > 0.05). Compared with that in the control group, the postoperative sleep efficiency in the Dex group was greater (P = 0.01). As shown in Figure 3A, the postoperative NRS score was higher than the preoperative NRS score in the control group (P = 0.032), whereas the postoperative NRS score was lower than the preoperative NRS score in the Dex group (P = 0.019). Compared with that in the control group, the postoperative NRS score in the Dex group was lower (P < 0.001). As shown in Figure 3B, there were no significant differences between the preoperative and postoperative AIS scores in the control group (P > 0.05), whereas the postoperative AIS score was lower than the preoperative AIS score in the Dex group (P < 0.001). Compared with that in the control group, the postoperative AIS score in the Dex group was lower (P < 0.001). In summary, these results suggest that the dexmedetomidine nasal sprays improved postoperative sleep quality in patients who underwent laparoscopic gynaecological surgery.
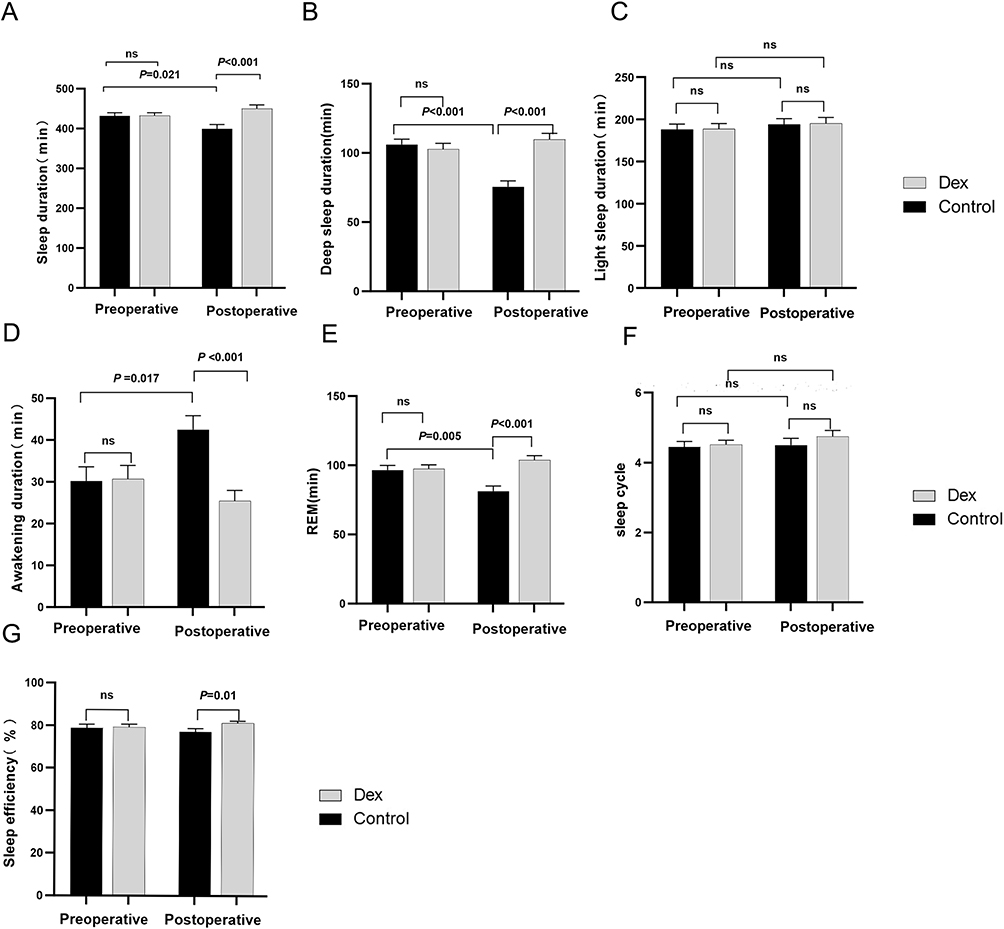 |
Figure 2 Dexmedetomidine nasal sprays improved postoperative sleep quality measured by the Portable sleep Monitor in patients undergoing gynecological laparoscopic operation. (A) Comparison of sleep duration between control and Dex group. (n=72, P = 0.021, vs preoperative group, paired t-test, P < 0.001 vs control group, Mann–Whitney Test). (B) Comparison of deep sleep duration between control and Dex group. (n=72, P < 0.001, vs preoperative group, paired t-test, P < 0.001 vs control group, Mann–Whitney Test). (C) Comparison of light sleep duration between control and Dex group. (D) Comparison of awakening duration between control and Dex group. (n=72, P = 0.017, vs preoperative group, paired t-test, P < 0.001 vs control group, Mann–Whitney Test). (E) Comparison of REM between control and Dex group. (n=72, P = 0.005, vs preoperative group, paired t-test, P < 0.001 vs control group, Mann–Whitney Test). (F) Comparison of sleep cycle between control and Dex group. (n=72, ns: no significance, P > 0.05 vs preoperative group, paired t-test, ns: no significance, P > 0.05 vs control group, Mann–Whitney Test). (G) Comparison of sleep efficiency between control and Dex group (n=72, P = 0.01 vs control group, Mann–Whitney Test). |
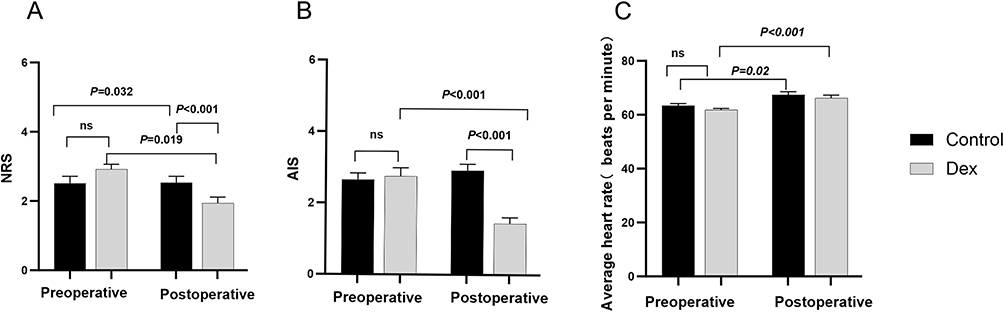 |
Figure 3 Dexmedetomidine nasal sprays improved postoperative sleep quality measured by Athens insomnia scale (AIS) and numerical rating scale (NRS) in patients undergoing gynecological laparoscopic operation. (A) Comparison of NRS between control and Dex group. (n=72, P = 0.032, vs preoperative group, Wilcoxon Signed Ranks Test, P = 0.019, vs preoperative group, Wilcoxon Signed Ranks Test, P < 0.001 vs control group, Mann–Whitney Test). (B) Comparison of AIS between control and DEX group. (n=72, P < 0.001, vs preoperative group, Wilcoxon Signed Ranks Test, P< 0.001 vs. control group, Mann–Whitney Test). (C) Comparison of average heart rate between control and DEX group. (n=72, P = 0.02, vs preoperative group, Wilcoxon Signed Ranks Test, P <0.001, vs preoperative group, Wilcoxon Signed Ranks Test). |
Secondary Outcomes
We measured the average heart rate of the patients to evaluate the impact of the dexmedetomidine nasal sprays on the heart rate. As shown in Figure 3C, there were no significant differences in the preoperative average heart rate between the control and Dex groups (P > 0.05). Compared with the preoperative heart rate, the postoperative average heart rate was greater in both the control and Dex groups (P = 0.02, P < 0.001). In addition, we recorded the occurrence of postoperative pain and postoperative nausea and vomiting. As shown in Table 2, there were no significant differences between the control group and the Dex group in terms of postoperative pain (P = 0.108) or postoperative nausea and vomiting (P = 0.065).
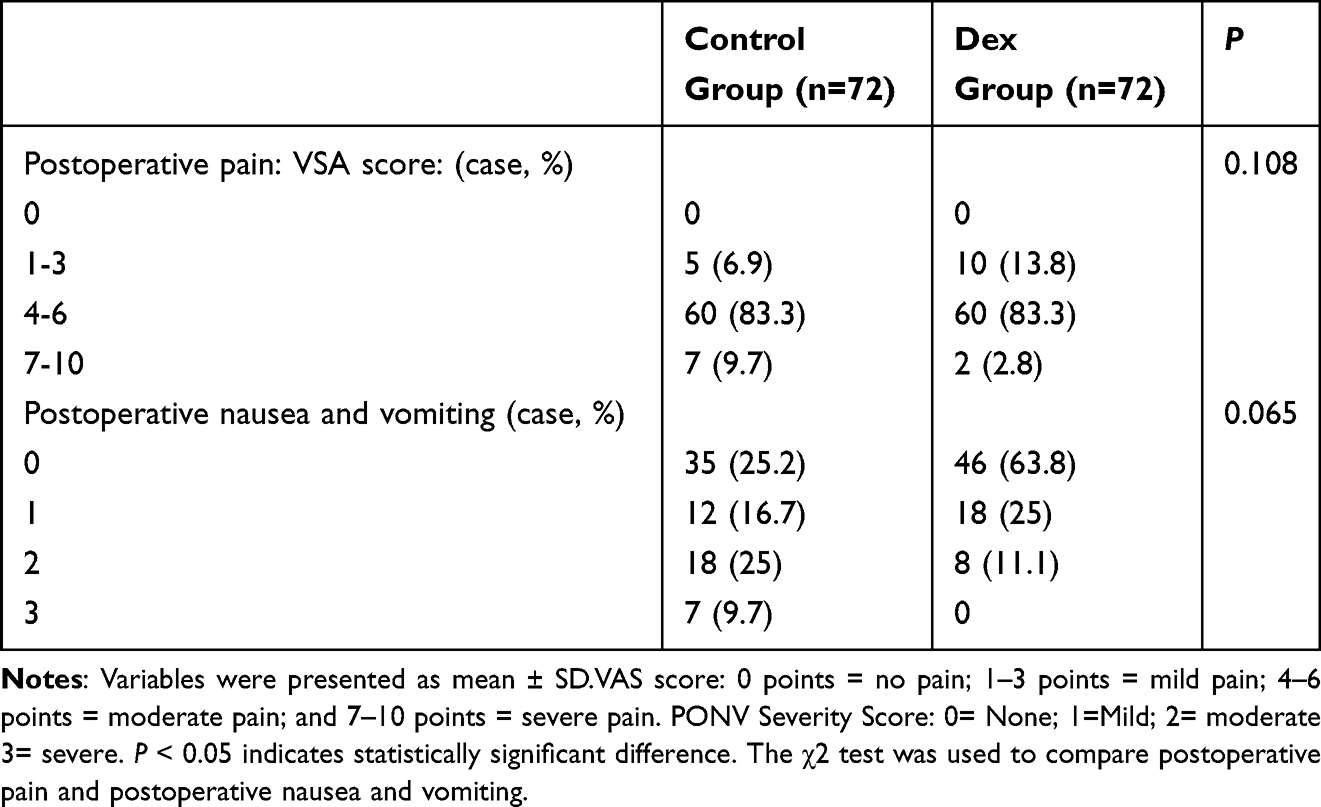 |
Table 2 The Occurrence of Postoperative Pain and Postoperative Nausea and Vomiting in Control Group and Dex Group |
Discussion
In this study, we evaluated the effects of dexmedetomidine nasal sprays on sleep quality in patients undergoing laparoscopic gynaecological surgery. The main results of this study were as follows. First, we found that, compared with those before surgery, the postoperative sleep duration, deep sleep duration and REM sleep duration were decreased, but the postoperative awakening duration and NRS score were increased in the control group, which means that postoperative sleep quality was decreased in the control patients who underwent laparoscopic gynaecological surgery. Second, compared with those in the control group, the postoperative sleep duration, deep sleep duration and REM sleep duration were longer in the Dex group, but the awakening duration, AIS score and NRS score were reduced. These findings indicate that the dexmedetomidine nasal sprays improved postoperative sleep quality in patients who underwent laparoscopic gynaecological surgery. In addition, we recorded the changes in the average heart rate before and after surgery. We found that the postoperative use of 50 µg of dexmedetomidine nasal sprays did not affect the average heart rate, which means that the dose used in this study is relatively safe for postoperative patients.
Previous studies have shown that most patients experience PSD characterized by a significant reduction in REM sleep duration, sleep duration and N3 sleep duration after major surgery.4,27,28 A total of 15% to 72% of patients experience PSD after major surgery, which is related to many factors, such as female sex, anxiety, age, postoperative pain, postoperative nausea and vomiting and the ward environment.27,29,30 Previous studies have shown that surgery and anaesthesia have adverse effects on sleep quality by altering sleep patterns. Patients who undergo surgery have significantly reduced REM and N3 sleep durations.31,32 Similarly, in our study, we observed a decrease in postoperative sleep quality among patients in the control group who underwent laparoscopic gynaecological surgery. This was evidenced by a significant reduction in REM sleep duration, sleep duration, and deep sleep duration, coupled with an increase in fragmented sleep duration. These results were consistent with those of previous studies.
Previous studies have shown that some drugs can treat PSD. Zolpidem can improve the proportion of REM and SWS sleep. However, there is an evidence that zolpidem prescription was associated with an increased risk of suicide attempts.8 Melatonin, synthesized, and secreted by the pineal gland, is an endogenous hormone that can regulate the circadian rhythm. The melatonin application in the perioperative period can improve sleep quality without apparent side effects.8 Also, Previous studies also have shown that intraoperative infusion of ketamine can improve postoperative sleep quality.26,33 Dexmedetomidine, a highly selective α2-adrenergic receptor (α2-AR) agonist, reduces the activity of locus coeruleus-noradrenergic system (LC-NE) neurons through the activation of α2-ARs on the central presynaptic membrane. This process results in disinhibition of the ventral lateral preoptic area of the hypothalamus, subsequently inducing sedative and hypnotic effects.34,35 Unlike these drugs, dexmedetomidine induces a sleep state that more closely resembles natural NREM sleep.35,36 Several studies have reported that dexmedetomidine can alleviate PSD symptoms by promoting the restoration of normal circadian sleep cycles, increasing sleep efficiency and optimizing sleep architecture in patients.15,37–39
Ye et al reported that postoperative sleep quality in patients who underwent maxillofacial surgery improved by intranasal administration of dexmedetomidine through a syringe (1.0 μg.kg−1 and 1.5 μg.kg−1).40 Research suggests that administering a low dose of dexmedetomidine intraoperatively, ranging from 1.0 to 2.0 μg.kg−1.h−1, improves the quality of sleep in elderly patients on the first night after surgery.16 Considering that intranasal administration via a syringe often fails to ensure precise dosing and optimal bioavailability, so, dexmedetomidine nasal sprays was used to ensure bioavailability and a precise dosage. Besides, the patients included in this study had normal preoperative sleep, so, low-dose dexmedetomidine nasal sprays (50 µg) was chosen to explore its impact on postoperative sleep quality. Nelson et al reported that during sleep induced by dexmedetomidine, the expression of the c-Fos protein in the brain is highly similar to that in the NREM phase, which suggested that dexmedetomidine could activate the NREM sleep pathway and induce sleep.35 Oluwaseun et al reported that dexmedetomidine could induce approximate natural sleep neurophysiology and promote NREM sleep.14 Similarly, in our study, we also found that dexmedetomidine improved postoperative sleep quality by prolonging sleep duration and N3 sleep duration, reducing the time to awakening and fragmented sleep duration. In addition, we also found that the average heart rate increased after surgery in the control and Dex groups, which may be due to postoperative pain and postoperative monitoring.
Polysomnography (PSG) has been the gold standard for evaluating sleep quality and diagnosing sleep-related diseases in the clinic. Physiological signal acquisition during sleep is usually conducted in the hospital since the acquisition process of vital signs is cumbersome. To obtain physiological signals, including electroencephalography (EEG), electrooculography (EOG), electromyography (EMG), electrocardiography (ECG), and respiratory rate data,41 many sensors are attached directly to patients’ skin,42 which is complex and can be uncomfortable for long-term monitoring. Therefore, a noncontact portable sleep monitor, which is a novel unperturbed sleep monitoring scheme based on a hidden Markov model in which the device is placed under the pillow, was used in our study. The noncontact vital sign monitoring system used in this study consists of a piezoelectric sensor, a circuit, and processing modules. The piezoelectric sensor module is placed under the pillow to perceive the vibration induced by the heartbeat, respiratory rate, and body movements. The effectiveness and accuracy of this module have been confirmed.43,44
The NRS and AIS have been commonly used to assess subjective sleep disorders in previous studies, indicating that their validity and reliability have been established. Previous studies have indicated that postoperative patients have elevated NRS and AIS scores, along with diminished sleep quality.16,23,24,45–47 In our study, we found that the AIS score and NRS score increased in the control group; however, they decreased after the administration of dexmedetomidine nasal sprays. These results were consistent with those of previous studies. PSD can increase the risk of postoperative infections and complications, even resulting in significant adverse outcomes, including adverse effects on the immune system and cardiovascular system and decreased physical and mental health.48–50 Consequently, treating PSD has significant benefits in accelerating the perioperative recovery of patients.
Previous studies have shown that a decreased heart rate is one of the common adverse effects of dexmedetomidine.51 In our study, we found that the postoperative use of 50 µg of dexmedetomidine not only did not affect the average heart rate of the patients but also improved the postoperative sleep quality of patients who underwent laparoscopic gynaecological surgery. Of course, we will further explore the effects of different doses of dexmedetomidine nasal sprays (100ug 150ug) on perioperative sleep quality in patients. Moreover, the convenience and safety of dexmedetomidine nasal sprays (50ug) may provide potential advantages for its use in treating insomnia at home, which is worth further research.
Many studies found that intravenous dexmedetomidine can lower the incidence of PONV compared to placebo.52,53 Previous studies have shown that intraoperative use of different doses of dexmedetomidine (0.2–0.5ug/kg, 0.2–0.7μg.kg−1.h−1) can effectively prevent PONV.54 However, dexmedetomidine nasal spray did not reduce the incidence of PONV in our study, which may be due to the fact that we used it 30 minutes before sleep on the first postoperative night and the dose was relatively small at 50ug. Another possible reason is that the incidence of PONV in the control group was not high in this study. So, although the DEX group reduced the incidence of PONV, there was no statistical difference. The effect of different doses of dexmedetomidine nasal spray (100ug,150ug) and medication time points on PONV is worth exploring in the future. Many previous studies have explored the relationship between postoperative pain and postoperative sleep disorders, and most research results indicate that postoperative pain is one of the risk factors for postoperative sleep disorders. Postoperative pain may lead to sleep disorders.8 Previous studies have confirmed that intraoperative use of dexmedetomidine can alleviate postoperative pain.55,56 But, dexmedetomidine nasal spray used 30 minutes before sleep on the first postoperative night did not reduce the postoperative pain in our study, which may be due to the fact that postoperative pain was controlled well in both group through patient-controlled intravenous analgesia (PCIA) with sufentanil (100ug) in our study. Besides, another reason maybe is that the low-dose (50ug) dexmedetomidine nasal spray was used in our study, which did not significantly improve postoperative pain, so there was no statistically significant difference in postoperative pain scores between the two groups. Of course, PONV and postoperative pain are important interfering factors that lead to fragmented sleep and changes in sleep structure,4,57 which need further exploration in future research.
Importantly, several limitations are present in this study. First, we only observed parameters of sleep structures during the first nights before and after surgery, and the long-term effect of dexmedetomidine nasal sprays on PSD needs further study. Second, the effects of different doses of dexmedetomidine nasal sprays on PSD have not been explored, and dose ranges within a safe clinical scope should be considered in more comprehensive studies on the prevention of postoperative sleep disturbances in patients who receive general anaesthesia. Third, Study data was only obtained through the female gender population due to enrolling patients who underwent gynecological laparoscopic surgery. We have no data in male gender population. Finally, we did not explore the effects of dexmedetomidine nasal sprays on postoperative recovery in patients, such as the incidence of postoperative delirium, the quality of postoperative recovery, and the length of hospital stay after surgery.
Conclusion
In conclusion, this clinical study reaffirmed the safety and efficacy of the dexmedetomidine nasal sprays in enhancing postoperative sleep quality, which not only provides clinical evidence for the use of dexmedetomidine nasal sprays in patients with sleep disorders but also ensures the safety of the use of the nasal spray in the treatment of insomnia at home.
Data Sharing Statements
Data are available from the corresponding author by email [email protected].
Statement of Ethics
The study protocol was approved by the Research Ethics Committee of Guangzhou Women and Children’s Medical Center on November 10, 2023 and was registered in the Chinese Clinical Trial Register (ChiCTR2400080181, http://www.chictr.org.cn). All participants signed informed consent forms before inclusion.
Funding
This study was supported by the Guangdong Province Yiyang Health Charity Foundation (Grant No. JZ2024024) and Guangzhou Science and Technology Program Project (Grant No. 2025A03J4381).
Disclosure
The authors have no competing interests to declare.
References
1. Wang J-P, Lu S-F, Guo L-N, Ren C-G, Zhang Z-W. Poor preoperative sleep quality is a risk factor for severe postoperative pain after breast cancer surgery: a prospective cohort study. Medicine. 2019;98(44):e17708. doi:10.1097/MD.0000000000017708
2. Ida M, Onodera H, Yamauchi M, Kawaguchi M. Preoperative sleep disruption and postoperative functional disability in lung surgery patients: a prospective observational study. J Anesthesia. 2019;33:501–508. doi:10.1007/s00540-019-02656-y
3. Halle IH, Westgaard TK, Wahba A, Oksholm T, Rustøen T, Gjeilo KH. Trajectory of sleep disturbances in patients undergoing lung cancer surgery: a prospective study. Int Cardiovasc Thoracic Surg. 2017;25(2):285–291. doi:10.1093/icvts/ivx076
4. Rosenberg-Adamsen S, Kehlet H, Dodds C, Rosenberg J. Postoperative sleep disturbances: mechanisms and clinical implications. Brit J Anaesthesia. 1996;76(4):552–559. doi:10.1093/bja/76.4.552
5. Ayuse T, Kurata S, Mishima G, et al. Influence of general anesthesia on the postoperative sleep cycle in patients undergoing surgery and dental treatment: a scoping review on the incidence of postoperative sleep disturbance. J Dental Anesthesia Pain Med. 2023;23(2):59. doi:10.17245/jdapm.2023.23.2.59
6. Kim SH, Kim N, Min KT, Kim EH, Oh H, Choi SH. Sleep disturbance and delirium in patients with acromegaly in the early postoperative period after transsphenoidal pituitary surgery. Medicine. 2020;99(45):e23157. doi:10.1097/MD.0000000000023157
7. Rampes S, Ma K, Divecha YA, Alam A, Ma D. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2020;34(4):271. doi:10.7555/JBR.33.20190054
8. Lin D, Huang X, Sun Y, Wei C, Wu A. Perioperative sleep disorder: a review. Front Med. 2021;8:640416. doi:10.3389/fmed.2021.640416
9. Aldecoa C, Bettelli G, Bilotta F, et al. European society of anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214 doi:10.1097/EJA.0000000000000594.
10. Huang B-H, Duncan MJ, Cistulli PA, Nassar N, Hamer M, Stamatakis E. Sleep and physical activity in relation to all-cause, cardiovascular disease and cancer mortality risk. Brit J Sports Med. 2022;56(13):718–724. doi:10.1136/bjsports-2021-104046
11. Weerink MA, Struys MM, Hannivoort LN, Barends CR, Absalom AR, Colin P. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
12. Ramaswamy SM, Weerink MA, Struys MM, Nagaraj SB. Dexmedetomidine-induced deep sedation mimics non-rapid eye movement stage 3 sleep: large-scale validation using machine learning. Sleep. 2021;44(2):zsaa167. doi:10.1093/sleep/zsaa167
13. Akeju O, Pavone KJ, Westover MB, et al. A comparison of propofol-and dexmedetomidine-induced electroencephalogram dynamics using spectral and coherence analysis. Anesthesiology. 2014;121(5):978–989. doi:10.1097/ALN.0000000000000419
14. Akeju O, Hobbs LE, Gao L, et al. Dexmedetomidine promotes biomimetic non-rapid eye movement stage 3 sleep in humans: a pilot study. Clin Neurophysiol. 2018;129(1):69–78. doi:10.1016/j.clinph.2017.10.005
15. Oto J, Yamamoto K, Koike S, Onodera M, Imanaka H, Nishimura M. Sleep quality of mechanically ventilated patients sedated with dexmedetomidine. Int Care Med. 2012;38:1982–1989. doi:10.1007/s00134-012-2685-y
16. Cai J, Chen Y, Hao X, et al. Effect of intraoperative dexmedetomidine dose on postoperative first night sleep quality in elderly surgery patients: a retrospective study with propensity score-matched analysis. Front Med. 2020;7:528. doi:10.3389/fmed.2020.00528
17. Lu C, Zhang L-M, Zhang Y, et al. Intranasal dexmedetomidine as a sedative premedication for patients undergoing suspension laryngoscopy: a randomized double-blind study. PLoS One. 2016;11(5):e0154192. doi:10.1371/journal.pone.0154192
18. Liu H, Wei H, Qian S, et al. Effects of dexmedetomidine on postoperative sleep quality: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023;23(1):88. doi:10.1186/s12871-023-02048-6
19. Wang Y, Shuai Y, Qiu F, He J, Zhuang S. Dexmedetomidine-soaked nasal packing can reduce pain and improve sleep quality after nasal endoscopic surgery: a double-blind, randomized, controlled clinical trial. Sleep Breathing. 2021;25:2045–2052. doi:10.1007/s11325-021-02342-y
20. Baier NM, Mendez SS, Kimm D, Velazquez AE, Schroeder AR. Intranasal dexmedetomidine: an effective sedative agent for electroencephalogram and auditory brain response testing. Pediatric Anesthesia. 2016;26(3):280–285. doi:10.1111/pan.12851
21. Wu Z-F, He L, Lai Y, Li S-J, Zhang Y-P. Observation of the sedative effect of dexmedetomidine combined with midazolam nasal drops before a pediatric craniocerebral MRI. J Craniofacial Surg. 2020;31(6):1796–1799. doi:10.1097/SCS.0000000000006657
22. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh Sleep Quality Index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
23. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. The diagnostic validity of the Athens insomnia scale. J Psychosomatic Res. 2003;55(3):263–267. doi:10.1016/S0022-3999(02)00604-9
24. Duan G, Wang K, Peng T, Wu Z, Li H. The effects of intraoperative dexmedetomidine use and its different dose on postoperative sleep disturbance in patients who have undergone non-cardiac major surgery: a real-world cohort study. Nat Sci Sleep. 2020;Volume 12:209–219. doi:10.2147/NSS.S239706
25. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesthesia Analgesia. 2020;131(2):411–448 doi:10.1213/ANE.0000000000004833.
26. Qiu D, Wang X-M, Yang J-J, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514–e2244514. doi:10.1001/jamanetworkopen.2022.44514
27. Gögenur I, Wildschiøtz G, Rosenberg J. Circadian distribution of sleep phases after major abdominal surgery. Brit J Anaesthesia. 2008;100(1):45–49. doi:10.1093/bja/aem340
28. Krenk L, Jennum P, Kehlet H. Sleep disturbances after fast-track hip and knee arthroplasty. Brit J Anaesthesia. 2012;109(5):769–775. doi:10.1093/bja/aes252
29. Chouchou F, Khoury S, Chauny J-M, Denis R, Lavigne GJ. Postoperative sleep disruptions: a potential catalyst of acute pain? Sleep Med Rev. 2014;18(3):273–282. doi:10.1016/j.smrv.2013.07.002
30. Su X, Wang D-X. Improve postoperative sleep: what can we do? Current Opin Anesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
31. Gehlbach BK, Chapotot F, Leproult R, et al. Temporal disorganization of circadian rhythmicity and sleep-wake regulation in mechanically ventilated patients receiving continuous intravenous sedation. Sleep. 2012;35(8):1105–1114. doi:10.5665/sleep.1998
32. Elliott R, McKinley S, Cistulli P, Fien M. Characterisation of sleep in intensive care using 24-hour polysomnography: anobservational study. Crit Care. 2013;17:1–10. doi:10.1186/cc12565
33. Zhang T, Song N, Li S, et al. S-ketamine improves slow wave sleep and the associated changes in serum protein among gynecological abdominal surgery patients: a randomized controlled trial. Nat Sci Sleep. 2023;2023:903–913 doi:10.2147/NSS.S430453.
34. McCall JG, Al-Hasani R, Siuda ER, et al. CRH engagement of the locus coeruleus noradrenergic system mediates stress-induced anxiety. Neuron. 2015;87(3):605–620. doi:10.1016/j.neuron.2015.07.002
35. Nelson LE, Lu J, Guo T, Saper CB, Franks NP, Maze M. The α2-adrenoceptor agonist dexmedetomidine converges on an endogenous sleep-promoting pathway to exert its sedative effects. J Am Soc Anesthesiolog. 2003;98(2):428–436 doi:10.1097/00000542-200302000-00024.
36. Coull JT, Jones ME, Egan TD, Frith CD, Maze M. Attentional effects of noradrenaline vary with arousal level: selective activation of thalamic pulvinar in humans. Neuroimage. 2004;22(1):315–322. doi:10.1016/j.neuroimage.2003.12.022
37. Brito RA, Do Nascimento Rebouças Viana SM, Beltrão BA, de Araújo Magalhães CB, de Bruin VMS, de Bruin PFC. Pharmacological and non-pharmacological interventions to promote sleep in intensive care units: a critical review. Sleep Breathing. 2020;24:25–35. doi:10.1007/s11325-019-01902-7
38. Wu X-H, Cui F, Zhang C, et al. Low-dose dexmedetomidine improves sleep quality pattern in elderly patients after noncardiac surgery in the intensive care unit: a pilot randomized controlled trial. Anesthesiology. 2016;125(5):979–991. doi:10.1097/ALN.0000000000001325
39. Chen Z, Tang R, Zhang R, Jiang Y, Liu Y. Effects of dexmedetomidine administered for postoperative analgesia on sleep quality in patients undergoing abdominal hysterectomy. J Clin Anesthesia. 2017;36:118–122. doi:10.1016/j.jclinane.2016.10.022
40. Wang Y, Jin Z, Xu W, et al. Clinical observation of dexmedetomidine nasal spray in the treatment of sleep disorders on the first night after undergoing maxillofacial surgery: a single-center double-blind randomized controlled study. J Pharm Pharmaceut Sci. 2023;26:11699. doi:10.3389/jpps.2023.11699
41. Chien Y-R, Wu C-H, Tsao H-W. Automatic sleep-arousal detection with single-lead EEG using stacking ensemble learning. Sensors. 2021;21(18):6049. doi:10.3390/s21186049
42. Penzel T, Conradt R. Computer based sleep recording and analysis. Sleep Med Rev. 2000;4(2):131–148. doi:10.1053/smrv.1999.0087
43. Wang Z, Zha S, Yu B, Chen P, Pang Z, Zhang H. Sleep staging using noncontact‐measured vital signs. J Healthcare Eng. 2022;2022(1):2016598. doi:10.1155/2022/2016598
44. Song B, Li Y, Teng X, Li X, Yang Y, Zhu J. The effect of intraoperative use of dexmedetomidine during the daytime operation vs the nighttime operation on postoperative sleep quality and pain under general anesthesia. Nat Sci Sleep. 2019;Volume 11:207–215. doi:10.2147/NSS.S225041
45. Gu X, Zhang Y, Wei W, Zhu J. Effects of preoperative anxiety on postoperative outcomes and sleep quality in patients undergoing laparoscopic gynecological surgery. J Clin Med. 2023;12(5):1835. doi:10.3390/jcm12051835
46. Okajima I, Nakajima S, Kobayashi M, Inoue Y. Development and validation of the J apanese version of the A thens I nsomnia S cale. Psych Clin Neurosci. 2013;67(6):420–425. doi:10.1111/pcn.12073
47. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosomatic Res. 2000;48(6):555–560. doi:10.1016/S0022-3999(00)00095-7
48. Campo FR, Drouot X, Thille AW, et al. Poor sleep quality is associated with late noninvasive ventilation failure in patients with acute hypercapnic respiratory failure. Crit Care Med. 2010;38(2):477–485. doi:10.1097/CCM.0b013e3181bc8243
49. Kamdar BB, Needham DM, Collop NA. Sleep deprivation in critical illness: its role in physical and psychological recovery. J Intensive Care Med. 2012;27(2):97–111. doi:10.1177/0885066610394322
50. Boyko Y, Ørding H, Jennum P. Sleep disturbances in critically ill patients in ICU: how much do we know? Acta Anaesthesiolog Scand. 2012;56(8):950–958. doi:10.1111/j.1399-6576.2012.02672.x
51. Lee S. Dexmedetomidine: present and future directions. Kor J Anesthesiol. 2019;72(4):323–330. doi:10.4097/kja.19259
52. Lee J, Hwang HW, Jeong J-Y, Kim YM, Park C, Kim JY. The effect of low-dose dexmedetomidine on pain and inflammation in patients undergoing laparoscopic hysterectomy. J Clin Med. 2022;11(10):2802. doi:10.3390/jcm11102802
53. Xie C, Zhang C, Sun H, Lu Y. Effects of dexmedetomidine on postoperative nausea and vomiting in adult patients undergoing ambulatory thyroidectomy: a randomized clinical trial. Front Med. 2021;8:781689. doi:10.3389/fmed.2021.781689
54. Li HJ, Liu S, Geng ZY, Li XY. Adding dexmedetomidine to morphine-based analgesia reduces early postoperative nausea in patients undergoing gynecological laparoscopic surgery: a randomized controlled trial. BMC Anesthesiol. 2020;20(1):11. doi:10.1186/s12871-019-0928-y
55. Schnabel A, Meyer-Frießem C, Reichl S, Zahn P, Pogatzki-Zahn E. Is intraoperative dexmedetomidine a new option for postoperative pain treatment? A meta-analysis of randomized controlled trials. Pain®. 2013;154(7):1140–1149. doi:10.1016/j.pain.2013.03.029
56. Bellon M, Le Bot A, Michelet D, et al. Efficacy of intraoperative dexmedetomidine compared with placebo for postoperative pain management: a meta-analysis of published studies. Pain Ther. 2016;5(1):63–80. doi:10.1007/s40122-016-0045-2
57. Roehrs T, Roth T. Sleep and pain: interaction of two vital functions. Seminars in neurology. 2005;25(1);106–116. doi:10.1055/s-2005-867079.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.