Back to Journals » Drug Design, Development and Therapy » Volume 20
Effects of Desflurane and Propofol General Anesthesia on Postoperative Recovery Quality in Elderly Patients Undergoing Spinal Surgery: A Randomized Non-Inferiority Trial
Authors Shi D, Liang X, Xi C, Pei C, Wang G ![]()
Received 4 February 2026
Accepted for publication 23 April 2026
Published 30 April 2026 Volume 2026:20 601299
DOI https://doi.org/10.2147/DDDT.S601299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Dongjing Shi, Xuan Liang, Chunhua Xi, Chunming Pei, Guyan Wang
Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, 1 Dongjiaominxiang Road, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-10-58268101, Email [email protected]
Purpose: Postoperative recovery quality is a key concern for elderly patients undergoing spinal surgery, yet evidence comparing different anesthetic techniques in this population remain limited. This study aimed to compare the quality of recovery between desflurane-based inhalational anesthesia and propofol-based total intravenous anesthesia in this population.
Patients and Methods: This randomized non-inferiority trial was conducted from July 1 to October 31, 2025. A total of 109 elderly patients scheduled for spinal surgery were randomly assigned to two groups: the desflurane group (group D), which received desflurane at a maintenance dose of 0.7 to 1.0 MAC, and the propofol group (group P), which received propofol at 4 to 6 mg/kg/h. Both groups received standard monitoring and invasive arterial blood pressure measurement. The primary outcome was the quality of recovery (QoR-15) scores on postoperative day 1 (POD1). Secondary outcomes include intraoperative remifentanil and vasopressors requirements, fluid volume, hemodynamic parameters, emergence profiles, duration of post-anesthesia care unit (PACU) stay, postoperative hospital length of stay, Activities of Daily Living (ADL) scale, Mini Montreal Cognitive Assessment (Mini-MoCA), Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), incidence of postoperative nausea and vomiting (PONV), Numeric Rating Scale (NRS) of postoperative pain and subjective sleep quality on POD1 and POD2.
Results: The total QoR-15 score on POD1 in group D was non-inferior to that in group P (117.0 ± 10.6 vs. 118.4 ± 12.0; mean difference: − 1.4; 95% CI: − 5.6– 2.4; one-sided P=0.017 for non-inferiority). Compared with group P, group D had significantly shorter times to extubation, eye opening, limb movement, orientation recovery, and ability to state one’s name, as well as significantly higher Riker Sedation-Agitation Scale scores. Intraoperative phenylephrine consumption and fluid volume were lower in group D than in group P. No significant differences were observed between the two groups in PACU stay duration, postoperative hospital length of stay, ADL scale, Mini-MoCA, CAM-ICU, PONV incidence, NRS pain scores, or subjective sleep quality.
Conclusion: Desflurane-based inhalational anesthesia provided a non-inferior quality of recovery compared with propofol. Additionally, desflurane was associated with faster emergence and lower vasopressor requirements. Desflurane and propofol can be considered interchangeable for general anesthesia in elderly patients undergoing spinal surgery.
Keywords: desflurane, aged, vertebra, postsurgical recovery
Introduction
China’s growing geriatric population is driving an increase in age-related degenerative pathologies of the lumbar and cervical spine. For patients with significant symptoms refractory to conservative management, surgery remains the most effective therapeutic option. Consequently, modern perioperative care, facilitated by advances in surgical techniques, has shifted its focus from solely mitigating morbidity to actively enhancing patient-reported postoperative experiences.1
The choice of an appropriate anesthetic regimen is crucial for ensuring successful surgical outcomes and optimizing postoperative recovery. Despite the variety of available sedatives and hypnotic drugs, identifying an ideal general anesthetic remains challenging. Even widely used intravenous anesthetics like propofol are associated with adverse effects such as injection pain, cardiorespiratory depression, metabolic acidosis, hyperlipidemia, and hepatomegaly.2,3 In addition, propofol-based total intravenous anesthesia (TIVA) may elevate the risk of intraoperative awareness.4
Desflurane, a volatile halogenated anesthetic characterized by low blood-gas solubility, exhibits rapid pharmacokinetics that facilitate quick emergence from anesthesia, a property particularly advantageous in elderly patients undergoing major spinal surgery.5–7 In addition, desflurane has been shown to provide greater intraoperative hemodynamic stability, with reduced ephedrine and fluid requirements, in elderly patients undergoing emergency abdominal surgery.8 Furthermore, in elderly orthopedic surgery, desflurane anesthesia was associated with a higher quality of recovery and greater patient and surgeon satisfaction.9 Within the framework of enhanced recovery after surgery (ERAS), this rapid washout and emergence not only permit early neurological assessment, which is particularly valuable in spine surgery where prompt evaluation of motor and sensory function can guide timely intervention if complications arise,10 but also promotes hemodynamic stability which helps reduce the need for vasopressors and the risk of fluid overload,11 both of which are independent risk factors for postoperative complications in elderly patients.
By facilitating a rapid recovery to baseline physical function and potentially shortening the length of stay in PACU, desflurane could support early mobilization,12 a core measure of ERAS. This approach effectively alleviates muscle atrophy and lowers the incidence of postoperative complications, including respiratory depression, cardiovascular instability, cognitive disturbances, and thromboembolic events, which are of heightened concern in the geriatric population, while also reducing hospitalization costs. Therefore, verifying the non-inferiority of desflurane to propofol in terms of holistic recovery metrics will further clarify its value in optimizing perioperative care pathways for the growing geriatric surgical cohort. However, comprehensive studies evaluating the overall impact of desflurane on postoperative recovery quality remain limited.
We hypothesize that the recovery quality on postoperative day 1 (POD1) following desflurane anesthesia would be non-inferior to that after propofol-based TIVA. This hypothesis was evaluated using the Quality of Recovery-15 (QoR-15) questionnaire to assess postoperative recovery quality in elderly patients undergoing spine surgery.
Material and Methods
Ethics and Registration
This prospective, double-blind, randomized trial was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Beijing Tongren Hospital (Approval No. TREC2025-KY052) and was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2500104947). Written informed consent was obtained from all individual participants.
Participants
Eligible participants were patients aged 65 or above, scheduled for elective spine surgery under general anesthesia, with an American Society of Anesthesiologists (ASA) physical status I–III.
The exclusion criteria were as follow:
- Known allergy or contraindications to propofol or desflurane;
- History of neuromuscular disorders (eg., malignant hyperthermia);
- Conditions potentially, interfering with the completion of the preoperative questionnaire (eg., severe hearing impairment, mental disorders, or cognitive dysfunction);
- Anticipated duration of the operation exceeding six hours;
- Planned postoperative admission to ICU or inability to adhere to the study anesthesia protocol;
- Concurrent enrollment in another clinical trial.
Randomization and Blinding
Eligible Patients were randomly allocated in a 1:1 ratio to either the desflurane group (Group D) or the propofol-based total intravenous anesthesia group (Group P). A computer-generated randomization sequence was prepared by an independent medical statistician, and allocation was concealed using the sealed envelope method. Patients, attending surgeons, and outcome assessors were all blinded to the group allocation. However, the attending anesthesiologist responsible for administering the anesthesia could not be blinded due to the distinct properties of the inhaled and intravenous anesthetics.
Anesthesia Protocol
All patients received standardized surgical and anesthetic care, except for the choice of general anesthetic agent used. No premedication was administered. Upon arrival in the operating room, standard monitoring was established, including pulse oxygen saturation (SpO2), electrocardiography (ECG), invasive arterial blood pressure, and Bispectral Index (BIS) monitoring.
Anesthesia was induced with etomidate (0.2–0.5 mg/kg), sufentanil (0.2–0.5μg/kg), and cisatracurium (0.15mg/kg). Tracheal intubation was performed using a video laryngoscope with a 7.0mm internal diameter tracheal tube after BIS values decreased below 60.
For maintenance, Group D received desflurane, starting at an initial vaporizer concentration of 2%, which was increased by 1% every three breaths until an end-tidal concentration of 0.7 to 1.0 MAC was achieved. Group P, received a continuous intravenous infusion of propofol at 4–6 mg/kg/h. Both groups received remifentanil infusion (0.1–0.3 μg/kg/min), and BIS was maintained between 40 and 60.
Mechanical ventilation was set to a tidal volume of 6–8 mL/kg based on predicted body weight, with 5 cmH2O positive end-expiratory pressure (PEEP). The respiratory rate was adjusted to maintain end-tidal carbon dioxide (ETCO2) of 30–35 mmHg, using a fractional inspired oxygen (FiO2) of 0.5 at a fresh gas flow of 2 L/min. Hypotension (mean arterial pressure <65 mmHg or a >20% decrease from baseline) was treated with ephedrine (6 mg) or phenylephrine (20 μg), provided depth of anesthesia was adequate.
30 minutes before the end of surgery, all patients received sufentanil (0.1μg/kg) and ondansetron (4mg) for analgesia and antiemetic prophylaxis, respectively. Local infiltration with 0.375% ropivacaine was performed at the surgical site. Anesthetics were discontinued at the end of surgery, and neuromuscular blockade was reversed with of neostigmine (1mg) and with atropine (0.5mg). Extubation was performed after the return of consciousness and adequate spontaneous breathing (tidal volume≥5 mL/kg). Subsequently, patients were transferred to the post-anesthesia care unit (PACU).
In the PACU, sufentanil (5μg) and ondansetron (4mg) were administered for pain numerical rating scale (NRS) >3 or nausea/vomiting. Patients were discharged to the ward upon achieving a modified Aldrete score of ≥9. Postoperative analgesia in the ward include intravenous flurbiprofen axetil (50mg twice daily), with supplemental oxycodone/acetaminophen tablets for NRS scores exceeding 4.
Outcome Measurement
The primary outcome was the quality of recovery (QoR) assessed using the QoR-15 questionnaire. This instrument evaluates postoperative recovery across five distinct domains: physical comfort (5 items), physical independence (2 items), emotional state (4 items), psychological support (2 items), and pain (2 items). Each item is rated on an 11-point numerical scale, with higher scores reflecting better outcomes. The total score ranges from 0 (poorest recovery) to 150 (optimal recovery). Patients completed the QoR-15 questionnaire preoperatively (the day before surgery) and on postoperative day 1 (POD1) and 2 (POD2) between 4:00 PM and 6:00 PM. The POD1 score served as the primary outcome measure.
Second outcomes included intraoperative remifentanil consumption, use of vasoactive drugs, time to extubation (from anesthetic discontinuation to tracheal extubation), and the Riker sedation-agitation scores at extubation. Additional recovery metrics were time to follow verbal command (eg., limb movement), time to state their name, time to orientation to place, duration of PACU stay, postoperative length of hospitalization, and time to ambulation. Adverse events were also recorded. Hemodynamic parameters (mean arterial pressure and heart rate) were recorded at predefined intervals: before general anesthesia induction (T0), after intubation (T1), at the time of skin incision (T2), 30min after incision (T3), 60min after incision (T4), at the end of the operation (T5), after extubation (T6) and at the time of leaving the operation room (T7). On POD1 and POD2, patients were also assessed using the Activities of Daily Living (ADL) scale, the Mini Montreal Cognitive Assessment (Mini-MoCA), the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), and Numeric Rating Scale (NRS) for postoperative pain, PONV, and subjective sleep quality.
Sample Size Calculation
Based on the recent update on the minimal clinically important difference (MCID) of the Quality of Recovery-15 (QoR-15) scores, the non-inferiority margin was set as 6.13 We considered desflurane inhalation anesthesia to be non-inferior to propofol-based total intravenous anesthesia (TIVA) if the lower bound of the 95% confidence interval (CI) for the difference in QoR-15 scores was greater than −6. A preliminary study was conducted with 10 participants in each group (desflurane and propofol). Group D had a mean QoR-15 score of 114.9 [standard deviation (SD) = 11.3], while Group P had a mean score of 110.4 (SD = 10.1). Sample size calculations for the non-inferiority test based on the primary outcome were performed with a one-sided significance level of 2.5%, a power of 80%, and an equal allocation ratio between the two groups. Using PASS 15 software, the required sample size was estimated to be 52 participants per group. Considering a potential dropout rate of 5%, the final sample size was adjusted to 55 participants per group, resulting in a total of 110 participants.
Statistical Analysis
Statistical analysis was conducted using SPSS version 29.0. Continuous data are presented as mean (SD) or median (interquartile range), as appropriate, with comparisons performed using Student’s t-test or the Wilcoxon rank-sum test, depending on whether the data followed a normal distribution. Categorical variables were described using frequencies and percentages, with comparisons conducted using the chi-square test or Fisher’s exact test, as appropriate. Standardized differences were calculated to assess the balance of demographic and operative characteristics between groups. Hemodynamic measurements and assessment scales across time points were analyzed using repeated measures analysis of variance (ANOVA). Non-inferiority was assessed using a one-sided test with a significance level of 0.025. Other statistical tests were two-tailed, with P< 0.05 considered statistically significant. For the five dimensions of the QoR-15, a Bonferroni correction was applied to control for multiple comparisons, with the significance threshold set at P < 0.01 for each postoperative day. The overall QoR-15 scores at POD1 and POD2 were analyzed without correction as the primary and key secondary endpoints, respectively.
Results
From July 1 to October 31, 2025, a total of 116 patients were assessed for eligibility. Four patients were excluded due to not meeting the inclusion criteria, and two patients declined to participate. Consequently, 110 patients who provided informed consent were enrolled and randomly assigned to receive either desflurane or propofol-based anesthesia. One patient in group P was withdrawn from the study after inclusion due to an unplanned postoperative ICU admission. Therefore, the final analysis included 109 patients, with 55 assigned to group D and 54 to group P (Figure 1). Demographic and clinical characteristics were comparable between the groups, with no statistically significant differences in gender, age, BMI, education level, ASA physical status classification, surgery time, anesthesia time, surgical type, surgical segment, or preoperative QoR-15 scores (Table 1).
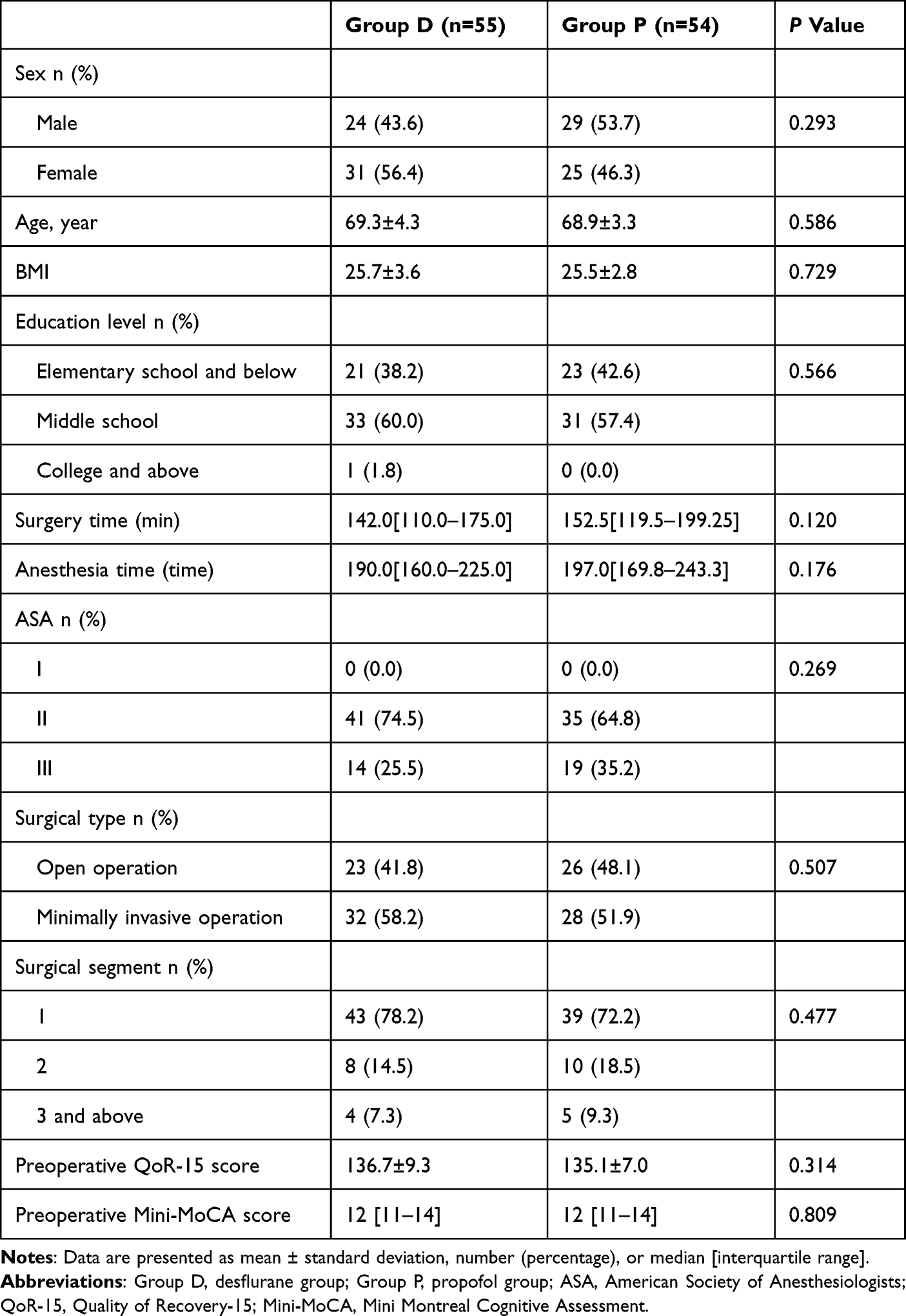 |
Table 1 The Characteristic of Patients, Surgery, and Anesthesia |
 |
Figure 1 Flowchart of the study design. |
The overall and dimensional QoR-15 scores for both groups are presented in Table 2. On POD1, the overall QoR-15 score in group D was non-inferior to that in group P (117.0 ± 10.6 vs. 118.4 ± 12.0; mean difference, −1.4; 95% CI, −5.6–2.4). The lower limit of the confidence interval was above the pre-specified non-inferiority margin of −6 (one-sided P=0.017 for non-inferiority; Figure 2). No significant differences were observed in the total QoR-15 scores between the two groups on POD2. Furthermore, analyses of the five individual dimensions, including pain, physical comfort, physical independence, psychological support, or emotional state, revealed no significant differences on either POD1 or POD2.
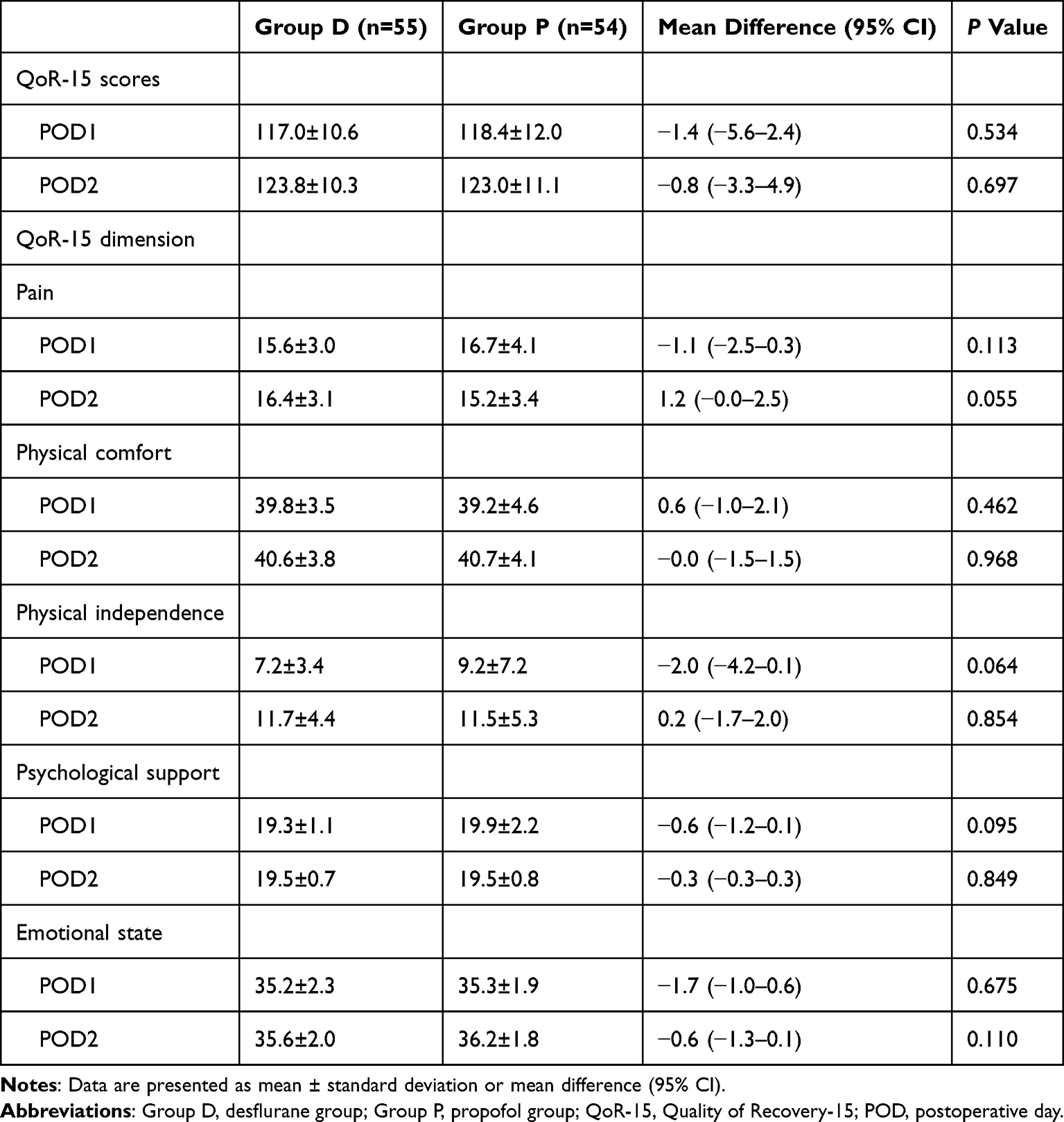 |
Table 2 Postoperative QoR-15 Scores |
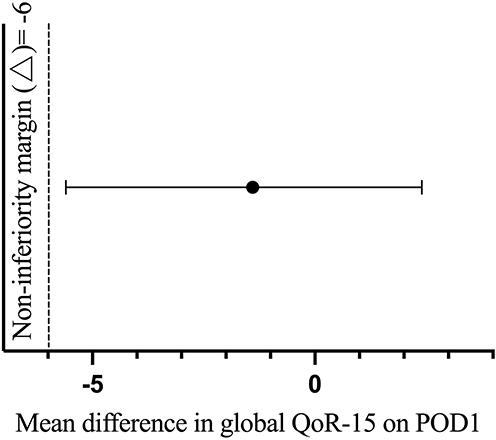 |
Figure 2 Mean difference in global QoR-15 on POD1. |
The emergence profiles showed significant differences between the two groups (Table 3). Patients in group D exhibited markedly shorter times from anesthetic discontinuation to extubation, eye opening, limb movement, regaining orientation, and the ability to state one’s name (P<0.01). Riker sedation-agitation scores were also significantly higher in group D (P<0.01). However, the length of PACU stay did not differ significantly between the two groups.
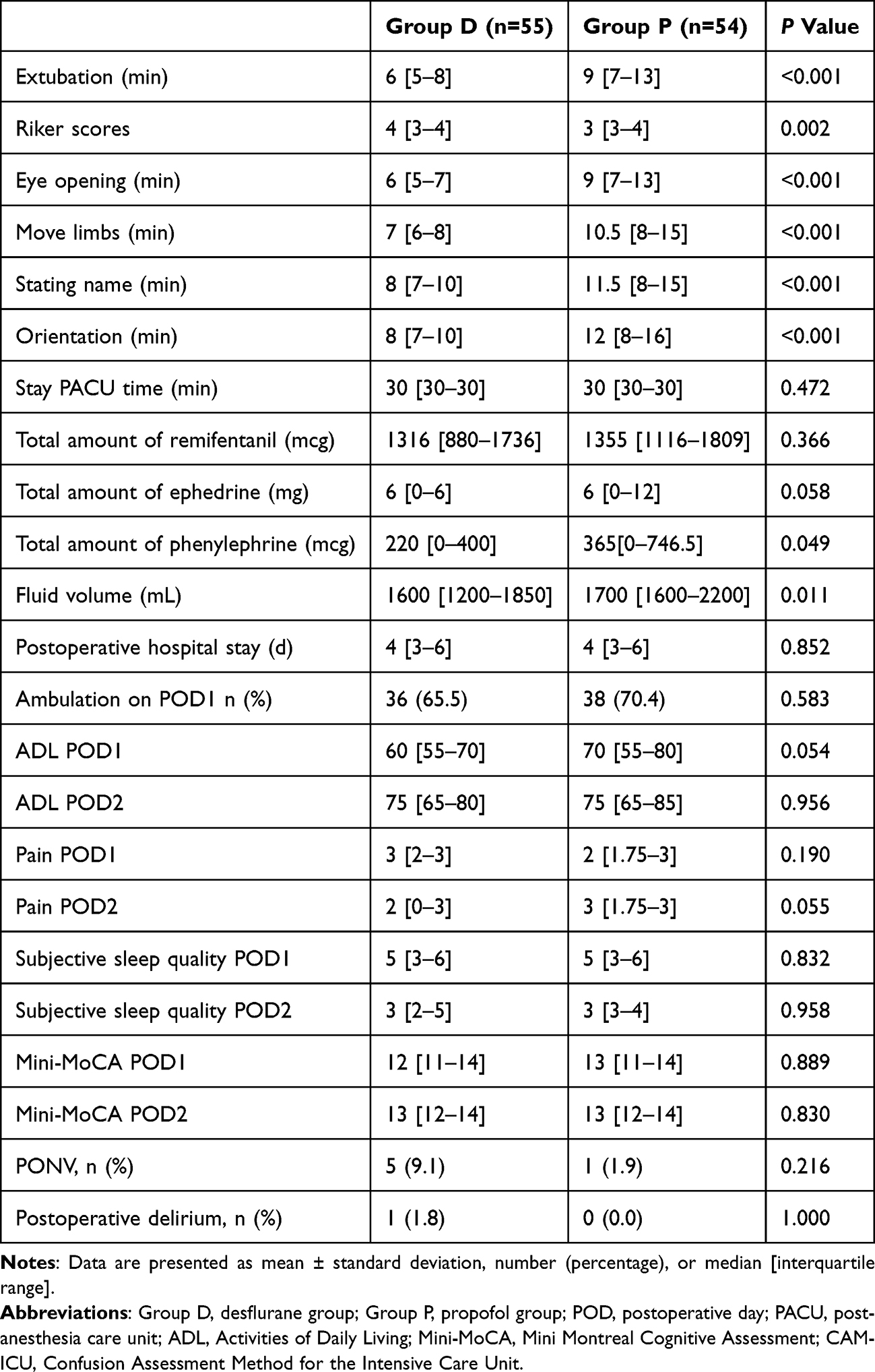 |
Table 3 The Secondary Outcomes |
Perioperative hemodynamic data are summarized in Figure 3. There were no significant differences observed in remifentanil or ephedrine consumption in the two groups. But both phenylephrine requirement and total fluid volume were significantly lower in group D than in group P (P<0.05; Table 3).
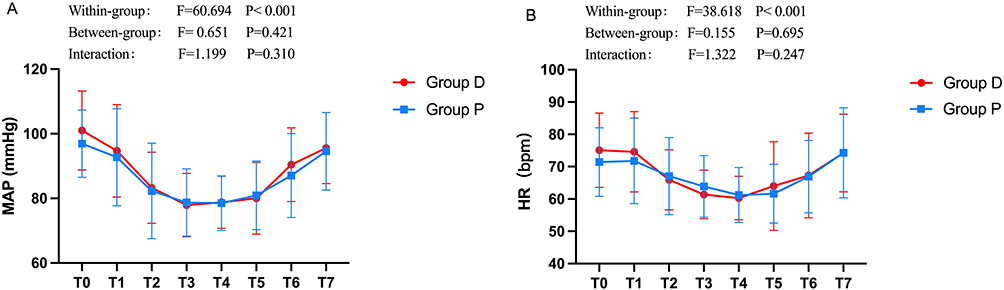 |
Figure 3 Comparison of hemodynamic parameters between the two groups. (A) MAP; (B) HR. Abbreviations: Group D, desflurane group; Group P, propofol group; MAP, mean arterial pressure; HR, heart rate. Notes: (T0) before general anesthesia induction, (T1) after intubation, (T2) at the time of skin incision, (T3) 30min after incision, (T4) 60min after incision, (T5) at the end of the operation, (T6) after extubation, (T7) at the time of leaving the operation room. |
There was no significant difference in postoperative hospital stay (P>0.05). Similarly, early ambulation, ADL scores, pain levels, PONV, and subjective sleep quality on POD1 and POD2 were all comparable (P> 0.05). Additionally, no significant differences were found in the incidence of postoperative cognitive function changes or delirium (Table 3).
Discussion
In this randomized non-inferiority trial, desflurane provides a quality of recovery on POD 1 that was non-inferior to propofol-based TIVA in elderly patients undergoing spinal surgery. This finding supports the integration of desflurane into enhanced recovery protocols for this growing patient population. Beyond the primary outcome, desflurane demonstrated a more rapid emergence profile, as evidenced by significantly shorter times to extubation and recovery of consciousness. During surgery, patients receiving desflurane required less phenylephrine and lower volumes of fluid. No significant differences were found in pain level, delirium, or cognitive function changes between the two groups. This comprehensive evaluation underscores that desflurane is a non-inferior alternative to propofol, with a distinct set of clinical considerations.
The assessment of postoperative recovery extends beyond conventional morbidity and mortality metrics, with growing recognition of the importance of patient-reported outcome measures (PROM).14 In this study, we employed the QoR-15 questionnaire, a well-validated PROM specifically designed to evaluate quality of recovery after surgery.15 This instrument has demonstrated high reliability, broad applicability in perioperative care, and strong acceptance in clinical practice.16 It encompasses five major dimensions: physical comfort, emotional state, physical independence, psychological support, and pain.17 Compared with the longer QoR-40 scale, the QoR-15 exhibits superior validity and reliability, while offering the advantage of reduced patient burden to complete the assessment.18,19
Previous studies have confirmed that propofol has the potential to alleviate body’s stress response and inhibit the excessive activation of pro-inflammatory cytokines. These effects help enhance the quality of patients’ postoperative recovery.20,21 However, a number of studies in recent years have shown that propofol-based TIVA does not yield superior overall postoperative QoR scores compared with desflurane-based inhalational anesthesia.22,23 Consistent with these findings, our study indicates that for elderly patients undergoing spinal surgery, general anesthesia with desflurane provides a comparable quality of recovery to that achieved with propofol.
It is noteworthy that the postoperative overall QoR-15 scores in our study population were lower than those reported in a previous study involving patients undergoing ureteroscopy.24 This discrepancy may be attributable to the advanced age of our participants and the substantial tissue trauma associated with spine surgery, both of which can predispose patients to a slower and more challenging recovery. Studies have shown that patients receiving propofol-based TIVA experience less pain during coughing and have lower analgesics consumption after lumbar spine surgery.25 No significant differences were observed between the two groups throughout the entire course of the present study. We suppose that the absence of obvious differences in the pain levels between the two groups may be associated with the multimodal analgesia regimen adopted in this study, which includes ropivacaine infiltration at the incision site and postoperative flurbiprofen axetil patient-controlled analgesia (PCA). This regimen may have “masked” the potential differences in the intrinsic analgesic properties between the two anesthetic agents themselves.
The results of this study revealed a statistically significant difference in anesthetic emergence profiles between the desflurane and propofol groups. Patients under desflurane-based inhalational anesthesia experienced a shorter time to extubation than those under propofol-based TIVA. The variances can be attributed to the pharmacokinetic characteristic of the two agents: the rapid “washout” of the poorly soluble desflurane upon discontinuation, in contrast to the potential for accumulation of propofol caused by continuous infusion during surgery.26,27 In group D, the time intervals from discontinuation of the anesthetic agent to eye opening, voluntary limbs movement on command, stating one’s name, and accurate completion of orientation tests were all significantly shorten at a statistical level of P<0.001 level. The findings of this study are consistent with those reported by La Colla et al.28
Such differences in emergence time might not have significant clinical value in the general population of surgical patients; however, in patients undergoing spine surgery, these differences can assist clinicians in rapidly identifying those with symptoms of nerve compression, thereby enabling targeted diagnostic examinations and even emergent reintervention for such patients. Moreover, the operating room is a labor-intensive department. Reducing procedural time can directly cut down the time that surgeons, anesthesiologists, nurses, and other staff devote to a single operation. The human resources saved in this way can be allocated to other clinical diagnosis and treatment activities. Prior analyses suggest that each minute saved can reduce scheduled labor costs by 1.0 to 1.2 minutes.29 It is noteworthy that despite the difference in emergence speed, the incidence of postoperative delirium and cognitive dysfunction was comparable between the two groups. In summary, the consistent and rapid emergence profile of desflurane thus contributes to operating room efficiency without increasing the risk of these specific neurocognitive complications.
The hemodynamic parameters (MAP and HR) were essentially consistent between the two groups, but the total dose of phenylephrine required was lower in group D compared with group P. This finding suggests that desflurane is conducive to maintaining intraoperative circulatory stability, which is consistent with the findings of a published study on other surgical procedures.30 Propofol can induce excessive vasodilation and reduce cardiac output, leading to arterial hypotension.31,32 Our result can be explained by the potent sympatholytic suppressive effects of propofol and remifentanil administered intraoperatively.33 In addition, patients in Group D received a lower volume of intraoperative fluid than those in Group P. Excessive intraoperative fluid administration is correlated with an increased incidence of postoperative complications,34,35 which impairs postoperative recovery in patients, especially in elderly patients. Therefore, desflurane is more beneficial for maintaining intraoperative circulatory stability and promoting postoperative recovery in this vulnerable population. We acknowledge that desflurane has been associated with sympathetic activation, tachycardia, and airway irritation in some studies, particularly in elderly patients. However, in the present study, no significant differences in heart rate were observed between groups at any time point (Figure 3), likely due to our slow, breath-by-breath incremental increase of desflurane concentration. Nevertheless, the potential for these adverse effects should not be overlooked, especially in patients with cardiovascular or airway disease.
There are some limitations in this study. First, the study relied on patient-reported questionnaires, which are inherently and lack objective biomarkers. Incorporating physiological measures, such as cortisol levels or inflammation markers, could strengthen future assessments. Second, as a single-center trial involving exclusively elderly patients undergoing spinal surgery, the generalizability of our findings to other populations or clinical settings may be limited. Third, excluding patients with prolonged surgery (>6 hours) or postoperative ICU admission introduced selection bias. Our findings are primarily generalizable to elderly patients undergoing elective spinal surgery with an uncomplicated course. Whether desflurane is non-inferior to propofol in higher-risk patients remains unknown and warrants further investigation. Fourth, the follow‑up period was limited to POD2. Given that recovery in elderly patients often extends beyond this early phase, future studies with longer follow‑up are needed to capture recovery trajectories fully. Because the study was powered for the primary outcome, it may be underpowered for secondary neurocognitive outcomes (eg., Mini-MoCA, delirium), which are relatively rare events. Consequently, the null findings for these outcomes should not be overinterpreted as evidence of equivalence. Therefore, further multicenter studies including broader surgical cohorts and incorporating objective outcome measures are warranted.
Conclusion
We found that desflurane-based inhalational anesthesia was noninferior to propofol-based TIVA in terms of QoR among elderly patients undergoing spinal surgery. Compared with propofol, desflurane offered improved emergence profiles and greater hemodynamic stability. These secondary benefits may facilitate early neurological assessment and reduce the risk of hemodynamic instability in this vulnerable population. Therefore, desflurane represents a viable anesthetic choice for optimizing postoperative recovery in this population.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. After the article is published, readers can contact the corresponding author to obtain data by email.
Acknowledgments
Assistance with the study: We gratefully acknowledge Shaofei Su, PhD (Department of Epidemiology and Health Statistics, Beijing Obstetrics and Gynecology Hospital, Capital Medical University) for statistical consultation.
Funding
This study was supported by Beijing Hospitals Authority’s Ascent Plan (DFL20220203). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wessels E, Perrie H, Scribante J. et al. Quality of recovery in the perioperative setting: a narrative review. J Clin Anesth. 2022;78:110685. doi:10.1016/j.jclinane.2022.110685
2. Liolios A, Guérit JM, Scholtes JL, et al. Propofol infusion syndrome associated with short-term large-dose infusion during surgical anesthesia in an adult. Anesth Analg. 2005;100(6):1804–12. doi:10.1213/01.ANE.0000153017.93666.BF
3. Lundström S, Twycross R, Mihalyo M, et al. Propofol. J Pain Symptom Manage. 2010;40(3):466–470. doi:10.1016/j.jpainsymman.2010.07.001
4. Yu H, Wu D. Effects of different methods of general anesthesia on intraoperative awareness in surgical patients. Medicine. 2017;96(42):e6428. doi:10.1097/MD.0000000000006428
5. Magni G, Rosa IL, Melillo G, et al. A comparison between sevoflurane and desflurane anesthesia in patients undergoing craniotomy for supratentorial intracranial surgery. Anesth Analg. 2009;109(2):567–571. doi:10.1213/ane.0b013e3181ac1265
6. Boisson-Bertrand D, Laxenaire MC, Mertes PM. Recovery after prolonged anaesthesia for acoustic neuroma surgery: desflurane versus isoflurane. Anaesth Intensive Care. 2006;34(3):338–342. doi:10.1177/0310057X0603400302
7. Yasuda N, Lockhart SH, Eger II EI, et al. Kinetics of desflurane, isoflurane, and halothane in humans. Anesthesiology. 1991;74(3):489–498. doi:10.1097/00000542-199103000-00017
8. Varvat C, Passot S, Beauchesne B, et al. Optimization of anesthesia for emergency abdominal surgery in the elderly. Ann Fr Anesth Reanim. 2009;28(7–8):634–639. doi:10.1016/j.annfar.2009.05.006
9. Dong R, Song C, Li J, et al. Comparison of the safety and efficacy of desflurane versus sevoflurane on postoperative cognitive function and early recovery quality in elderly orthopedic patients: a prospective, randomized controlled trial. Front Med Lausanne. 2025;12:1707107. doi:10.3389/fmed.2025.1707107
10. Pavankumar M, Sunil BV, Bhat S. Comparison of Sevoflurane and Desflurane with Dexmedetomidine for Recovery in Neurosurgical Patients Undergoing Supratentorial Tumor Surgery. Ann Afr Med. 2026. doi:10.4103/aam.aam_314_25
11. Weiskopf RB, Cahalan MK, Eger II EI, et al. Cardiovascular actions of desflurane in normocarbic volunteers. Anesth Analg. 1991;73(2):143–156.
12. White PF. Studies of desflurane in outpatient anesthesia. Anesth Analg. 1992;75(4 Suppl):S47–53.
13. Myles PS, Myles DB. An Updated Minimal Clinically Important Difference for the QoR-15 Scale. Anesthesiology. 2021;135(5):934–935. doi:10.1097/ALN.0000000000003977
14. Myles PS. More than just morbidity and mortality - quality of recovery and long-term functional recovery after surgery. Anaesthesia. 2020;75(Suppl 1):e143–e150. doi:10.1111/anae.14786
15. Kleif J, Waage J, Christensen KB, et al. Systematic review of the QoR-15 score, a patient- reported outcome measure measuring quality of recovery after surgery and anaesthesia. Br J Anaesth. 2018;120(1):28–36. doi:10.1016/j.bja.2017.11.013
16. Myles PS, Shulman MA, Reilly J, et al. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. Br J Anaesth. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
17. Kleif J, Gögenur I. Severity classification of the quality of recovery-15 score-An observational study. J Surg Res. 2018;225:101–107. doi:10.1016/j.jss.2017.12.040
18. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
19. Myles PS, Weitkamp B, Jones K, et al. Validity and reliability of a postoperative quality of recovery score: the QoR-40. Br J Anaesth. 2000;84(1):11–15. doi:10.1093/oxfordjournals.bja.a013366
20. Liu T, Gu Y, Chen K, et al. Quality of recovery in patients undergoing endoscopic sinus surgery after general anesthesia: total intravenous anesthesia vs desflurane anesthesia. Int Forum Allergy Rhinol. 2019;9(3):248–254. doi:10.1002/alr.22246
21. Lee WK, Kim MS, Kang SW, et al. Type of anaesthesia and patient quality of recovery: a randomized trial comparing propofol-remifentanil total i.v. anaesthesia with desflurane anaesthesia. Br J Anaesth. 2015;114(4):663–668. doi:10.1093/bja/aeu405
22. Zaballos M, Reyes A, Etulain J, et al. Desflurane versus propofol in post-operative quality of recovery of patients undergoing day laparoscopic cholecystectomy. Prospective, comparative, non-inferiority study. Rev Esp Anestesiol Reanim. 2018;65(2):96–102. doi:10.1016/j.redar.2017.09.010
23. Kim SH, Ju HM, Choi CH, et al. Inhalational versus intravenous maintenance of anesthesia for quality of recovery in patients undergoing corrective lower limb osteotomy: a randomized controlled trial. PLoS One. 2021;16(2):e0247089. doi:10.1371/journal.pone.0247089
24. Shi S, Wu J, Wu Y, et al. Effects of Ciprofol and Propofol General Anesthesia on Postoperative Recovery Quality in Patients Undergoing Ureteroscopy: a Randomized, Controlled, Double-Blind Clinical Trial. Drug Des Devel Ther. 2025;19:931–943. doi:10.2147/DDDT.S497554
25. Lin WL, Lee MS, Wong CS, et al. Effects of intraoperative propofol-based total intravenous anesthesia on postoperative pain in spine surgery: comparison with desflurane anesthesia - a randomised trial. Medicine. 2019;98(13):e15074. doi:10.1097/MD.0000000000015074
26. Levitt DG, Schnider TW. Human physiologically based pharmacokinetic model for propofol. BMC Anesthesiol. 2005;5(1):4. doi:10.1186/1471-2253-5-4
27. Gökçek E, Kaydu A, Akdemir MS, et al. Early postoperative recovery after intracranial surgical procedures. Comparison of the effects of sevoflurane and desflurane. Acta Cir Bras. 2016;31(9):638–644. doi:10.1590/S0102-865020160090000010
28. La Colla L, Albertin A, La Colla G, et al. Faster wash-out and recovery for desflurane vs sevoflurane in morbidly obese patients when no premedication is used. Br J Anaesth. 2007;99(3):353–358. doi:10.1093/bja/aem197
29. Dexter F, Epstein RH. Typical savings from each minute reduction in tardy first case of the day starts. Anesth Analg. 2009;108(4):1262–1267. doi:10.1213/ane.0b013e31819775cd
30. Zhu YL, Shen WH, Chen QR, et al. Desflurane anesthesia compared with total intravenous anesthesia on anesthesia-controlled operating room time in ambulatory surgery following strabotomy: a randomized controlled study. Chin Med J. 2020;133(7):779–785. doi:10.1097/CM9.0000000000000728
31. Sundt TM, Jneid H. Guideline Update on Indications for Transcatheter Aortic Valve Implantation Based on the 2020 American College of Cardiology/American Heart Association Guidelines for Management of Valvular Heart Disease. JAMA Cardiol. 2021;6(9):1088–1089. doi:10.1001/jamacardio.2021.2534
32. Fassl J. Pro: transcatheter aortic valve implantation should be performed with general anesthesia. J Cardiothorac Vasc Anesth. 2012;26(4):733–735. doi:10.1053/j.jvca.2012.02.010
33. El Dib R, Guimarães Pereira JE, Agarwal A, et al. Inhalation versus intravenous anaesthesia for adults undergoing on-pump or off-pump coronary artery bypass grafting: a systematic review and meta-analysis of randomized controlled trials. J Clin Anesth. 2017;40:127–138. doi:10.1016/j.jclinane.2017.05.010
34. Gill P, Chua TC, Huang Y, et al. Pancreatoduodenectomy and the risk of complications from perioperative fluid administration. ANZ J Surg. 2018;88(4):E318–e323. doi:10.1111/ans.13913
35. Arslantas MK, Kara HV, Tuncer BB, et al. Effect of the amount of intraoperative fluid administration on postoperative pulmonary complications following anatomic lung resections. J Thorac Cardiovasc Surg. 2015;149(1):314–320. doi:10.1016/j.jtcvs.2014.08.071
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.