Back to Journals » Psychology Research and Behavior Management » Volume 19
Effects of Cognitive Reappraisal Training on Psychological Resilience, Depression Symptoms, and Emotional State
Received 29 June 2025
Accepted for publication 8 March 2026
Published 27 March 2026 Volume 2026:19 550385
DOI https://doi.org/10.2147/PRBM.S550385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Chong Gao, Xiaolong Zhao, Shuang Li
School of Design and Architecture, Zhejiang University of Technology, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Shuang Li, School of Design and Architecture, Zhejiang University of Technology, Hangzhou, 310023, People’s Republic of China, Tel +86 571 85290827, Email [email protected]
Purpose: Cognitive reappraisal can improve mental state by reinterpreting events and thoughts. This study investigated the effects of a five-day cognitive reappraisal training program on mental resilience, depression level, and emotional state in 63 Chinese individuals with depressive disorder.
Patients and Methods: This pre–post intervention study recruited participants through verified online depression support groups. Training was conducted daily over five consecutive days (each session lasting 60 minutes). A total of 63 individuals participated (age range 16– 42 years, M=24, SD=5), including 26 males and 37 females. Based on baseline SDS scores, 27.0% met criteria for minor depression, 31.7% for moderate depression, and 41.3% for major depression. A 5-day intervention comprising daily 30– 40-minute sessions of cognitive reappraisal training using IAPS images was implemented. Patient-generated reappraisal strategies were collected as written responses and systematically coded by researchers for analysis. Participants completed the Reappraisal Inventiveness Test (RIT), Brief Resilience Scale (BRS), Self-Rating Depression Scale (SDS), and Positive and Negative Affect Scale (PANAS) before training, on day 2 and day 5 during training, and 10 days post-training. Data were analyzed using SPSS 27.0, including paired-sample t-tests, Wilcoxon signed-rank tests, Spearman correlation, and independent-sample t-tests with Bonferroni correction.
Results: Cognitive reappraisal ability (CR1: mean increase from 2.349 to 3.365, P< 0.05), mental resilience (mean increase from 12.333 to 13.540, P< 0.05), and emotional state improved during training (ES: mean increase from 29.825 to 40.095, P< 0.05), while depression level declined, though changes in depression were not statistically significant. Improvements persisted to 10 days after training, albeit slightly diminished. Cognitive reappraisal ability correlated positively with mental resilience (P< 0.05) and negatively with depression level (P< 0.05). The strategy of “humor interpretation” significantly enhanced mental resilience and reduced depression (P< 0.05), while “generating positive aspects” only significantly enhanced mental resilience (P< 0.05). The differences in emotional state across strategies were not significant. Demographic analyses indicated a larger reduction in depression levels among younger participants (16– 25 years)(P< 0.05) and those with minor depression (p< 0.01), while gender and regional differences were nonsignificant.
Conclusion: Cognitive reappraisal training can improve mental well-being in the short-term in individuals with depressive disorder. Extended training may enhance these effects.
Keywords: reappraisal, depressive disorder, mental health, emotion, pre-post intervention
Introduction
Cognitive reappraisal is an emotional management strategy for handling emergencies by changing one’s perception of situations and altering emotional reactions.1 According to Gross’s2 emotion regulation model, cognitive reappraisal is an antecedent-focused emotion management strategy for self-regulating emotions before emotional feedback. Compared to expressive suppression, cognitive reappraisal acts earlier in emotion generation, using fewer cognitive resources and better reducing negative emotions.3,4
Depending on its emotional coping effect, positive cognitive reappraisal can improve mental health across various psychological variables. Cognitive reappraisal is positively associated with trait resilience,5 which is the maintenance or speed of mental health recovery in adversity.6 Cognitive reappraisal also positively correlates with positive notions, including self-acceptance7 self-efficacy,8 and life satisfaction.9
Recent research suggests a potential dynamic interplay among cognitive reappraisal, resilience, emotional state, and depression, underpinned by specific psychological mechanisms. Resilience enables individuals to maintain emotional stability under stress, reducing vulnerability to depressive symptoms.10,11 Cognitive reappraisal functions as an adaptive emotion regulation strategy that actively modifies the interpretation of stressors, leading to increased positive affect and decreased negative affect.12 This modulation of emotional state is a key mechanism through which reappraisal enhances resilience: by experiencing more adaptive emotional responses, individuals strengthen their capacity to cope with adversity.13 In turn, higher resilience amplifies the effectiveness of reappraisal, enabling individuals to buffer negative emotional reactions more efficiently and thereby attenuate depressive symptoms.14 Taken together, these findings suggest a reciprocal mechanism in which cognitive reappraisal and resilience interact to stabilize emotional states, and this interaction underlies their protective effect against depression. The emotional modulation and reinforcement of coping capacity represent the central pathways through which reappraisal exerts its beneficial impact.
However, while theoretical models suggest that cognitive reappraisal should consistently reduce depressive symptoms, empirical findings in clinical populations indicate considerable variability in its effectiveness. Depression is a clinically heterogeneous condition—characterized by variations in affective, cognitive, and somatic symptoms.15 Cognitive reappraisal has been shown to have small-to-medium associations with depressive symptoms, although results are heterogeneous between studies.16–18 Some studies have found no correlation,19 while others report that it is only associated with more severe depressive symptoms.20 Such inconsistencies may stem from variations in methodology, differences in cultural context, and the duration of training or testing. Therefore, cognitive reappraisal’s relation to depressive symptoms must be examined further.
Some studies further emphasize that the relationships between cognitive reappraisal and other psychological variables are dynamic and context-dependent. It is emphasized that the effectiveness of reappraisal interventions depends on the interaction between individual traits, intervention design, and emotional context.21 Therefore, investigating the interaction of cognitive reappraisal ability with psychological outcomes across individuals with diverse demographic and clinical characteristics is essential.
Different reappraisal strategies may relate to overall cognitive reappraisal ability. Previous research has distinguished cognitive reappraisal based on the self-reference effect into situation-focused and self-focused types,22,23 which differ in brain activation patterns, emotional regulation effectiveness, and associations with other cognitive abilities.22 Building on this framework, Weber et al24 further classified cognitive reappraisal into four types and 17 categories, using the number of categories participants generated as a measure of reappraisal ability. Similarly, Samson et al25 divided reappraisal strategies into “humorous” and “serious” categories based on processing attitude, finding that humorous reappraisal was more effective at down-regulating negative emotions. These classifications informed the assessment of reappraisal ability in the present study, integrating previous findings into a comprehensive framework for evaluating strategy effectiveness.
Furthermore, longitudinal studies have investigated the effects of cognitive reappraisal training on mental health. A 10-day study on cognitive reappraisal training showed increased trait reappraisal, which mediated the promotion of well-being and reduced negative emotions,26 while other intervention studies have found that reappraisal trainings’ duration, intensity, and participant characteristics may influence the effectiveness of interventions designed to enhance cognitive reappraisal.27,28 While structured reappraisal training elicits rapid improvements in reappraisal competence via short-duration interventions, it lacks robust longitudinal support for long-term efficacy;29 in contrast, mindfulness-based cognitive therapy delivers sustained emotional regulation benefits, albeit requiring prolonged engagement.30,31 Emotion regulation workshops offer practical benefits but vary in effectiveness due to differences in training design.31 Other methods promoting trait cognitive reappraisal through mutual social support, mantra, and mindfulness-based management have been shown to reduce depression, stress, and anger, respectively.32–34 However, few studies have directly analyzed the impact of cognitive reappraisal training on cognitive reappraisal ability, mental resilience, depression level, and emotional state.
Although cognitive reappraisal is well supported theoretically, empirical studies have not fully addressed how specific reappraisal strategies operate in practice, how their effects change over time, or how individual characteristics influence training outcomes. Prior research has focused mainly on overall effectiveness rather than strategy-specific processes and effect magnitudes. Therefore, the present study examines the effects of short-term cognitive reappraisal training in people with depressive disorders, by analyzing temporal changes of mental resilience, depression level, and emotional state, as well as strategy-specific differences, and individual variability.
Accordingly, we hypothesized that cognitive reappraisal training would improve cognitive reappraisal ability, which leads to a significant enhancement in mental resilience and emotional state, and a reduction in depressive symptoms. More specifically, it was expected that (H1) mental resilience would show a moderate increase following training (estimated effect size d=0.5–0.6), (H2) depression level would decrease to a small-to-moderate degree (d=0.3–0.5), and (H3) positive emotional state would increase (d=0.4–0.6). (H4) Certain strategy types would yield more robust improvements compared to other strategies (d=0.3–0.5). We further expected that (H5) demographic characteristics would be associated with differential training outcomes (d=0.4–0.6).
Materials and Methods
Participants
This study was conducted from April 2 to April 24, 2024, among individuals with depressive disorder in China, recruited through the social media platform “QQ groups”. A QQ group is a popular online platform in China for users with shared interests to interact. This study selected four widely used QQ groups for individuals with depressive disorder, with membership strictly verified by medical certification. These groups reflect a specific subgroup of individuals with depressive symptoms, demonstrating some degree of representativeness in terms of age, gender, severity of illness, and regional distribution, making the sample relatively representative. Stratified random sampling was used to select participants from within the groups, ensuring proportional representation from each level of depression severity. This method minimizes selection bias and enhances the validity of participant selection, improving the generalizability of the study’s findings to the broader population of individuals with depressive disorders. Participants were first divided into three strata based on their diagnosed depression severity—minor, moderate, and major depression—according to their medical certifications. From each stratum, we randomly selected participants using a computer-generated random number table In this process, each participant was assigned a unique number within their stratum, and the selection was made by randomly choosing numbers, ensuring an unbiased and representative sample. A proportional number of participants were chosen from each group to reflect the overall distribution of depression severity.
A total of 121 individuals initially expressed interest and were screened for eligibility. Figure 1 illustrates the selection criteria and steps for participant inclusion and exclusion. During the first screening stage, participants were asked to report whether they were currently receiving psychological therapy or taking psychotropic medication, in order to reduce the influence of potential confounding variables. Individuals undergoing concurrent structured psychotherapy or pharmacological treatment were excluded. Low adherence to the training protocol.
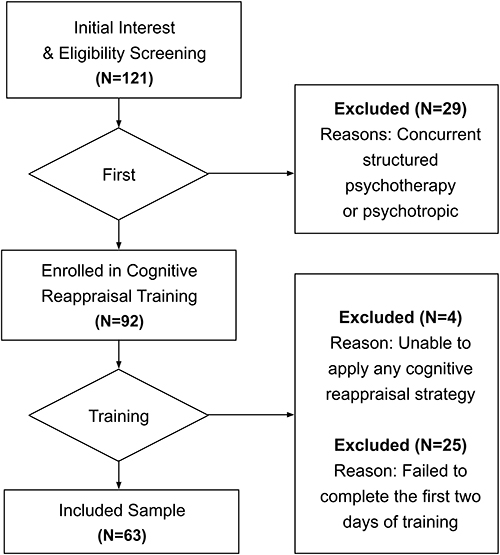 |
Figure 1 Participant Inclusion and Exclusion. |
After this screening process, 92 participants were recruited to participate in the cognitive reappraisal training. During the training phase, 29 participants were further excluded, including four participants who were unable to apply any cognitive reappraisal strategy and 25 participants who failed to complete the first two days of training. Consequently, the final sample consisted of 63 participants. The sample size was determined based on a power analysis, achieving a power value of 0.8, which is considered sufficient to detect meaningful effects in the study. As shown in Table 1, the sample consisted of 26 men (41.3%) and 37 women (58.7%), aged 16–42, with an average age of 24±5years. The sample had a balanced gender ratio, with age distribution following a normal distribution as confirmed by the One-Sample Kolmogorov–Smirnov test (P=0.200) and the Quantile-Quantile Plot. Geographically, the participants were distributed across China, with the largest proportion from Southern China (n=25), followed by Northern China (n=19), Central China (n=11), and Western China (n=8). In terms of clinical severity based on medical certifications, 17 participants had minor depression, 20 had moderate depression, and 26 had major depression.
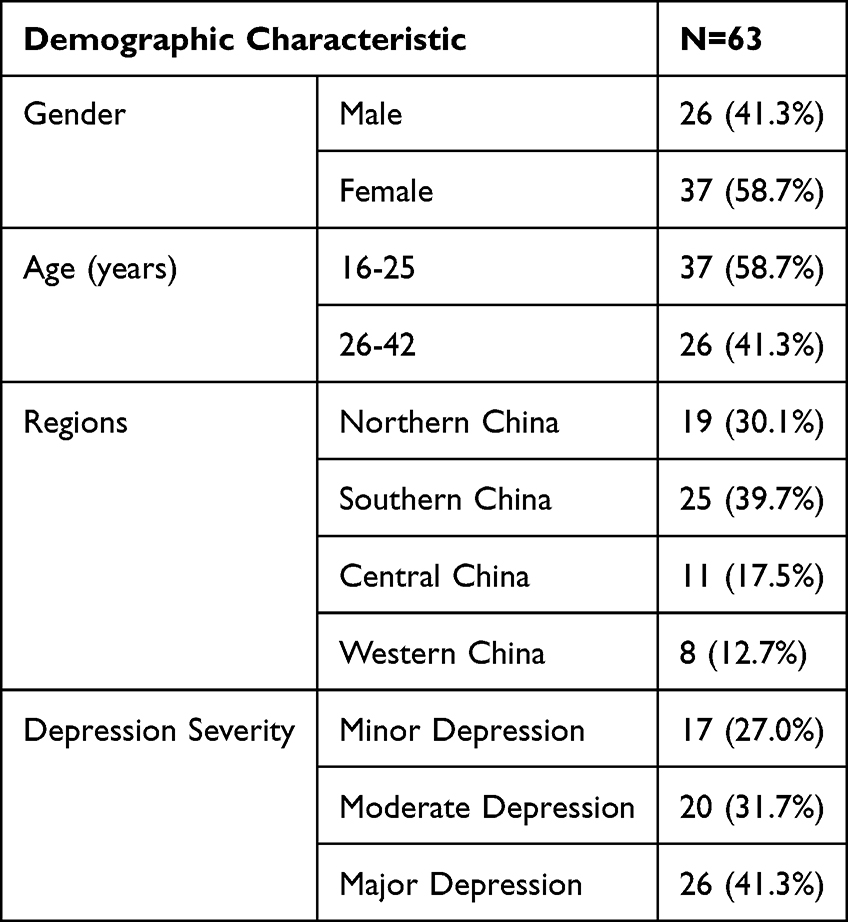 |
Table 1 Socio-Demographic Characteristics and Depression Severity of Participants |
To reduce the influence of potential confounding variables, although participants completed the training within QQ groups, interactions were restricted to task-related instructions, and no peer discussion or emotional support exchange was encouraged during the training period.
Instruments
Cognitive Reappraisal
Cognitive reappraisal has traditionally been assessed through self-report measures,35 which are prone to bias and may not accurately capture individuals’ actual processing abilities. For example, Troy et al36 reported that changes in sympathetic activation during a sad film clip were unrelated to participants’ self-reported frequency of reappraisal use. To address this limitation, Weber et al24 developed the Reappraisal Inventiveness Test (RIT), an objective tool measuring both the fluency (CR1) and flexibility (CR2) with which individuals generate reappraisal strategies. The RIT has demonstrated strong construct validity and operates independently of self-reported measures, providing a more precise assessment of reappraisal capacity. In the present study, the RIT was adopted to evaluate participants’ cognitive reappraisal ability, ensuring that the measurement accurately reflects actual cognitive performance rather than subjective perceptions.
Currently, no validated Chinese version of the Reappraisal Inventiveness Test (RIT) exists. Therefore, a Chinese translation of the RIT was used in this study. The translation followed standard cross-cultural adaptation procedures, and its psychometric properties have been validated, showing good reliability (Cronbach’s alpha>0.80), ensuring its suitability for the Chinese sample.
Mental Resilience
Mental resilience was measured using the Brief Resilience Scale (BRS), a self-report measure developed to assess an individual’s ability to recover or “bounce back” from stress and adversity.37 The BRS consists of six items that assess how easily individuals can overcome challenging situations. Each item is rated on a 5-point Likert scale, where 1 indicates strong disagreement (“completely disagree”) and 5 indicates strong agreement (“completely agree”).
The study used the Chinese version of the Brief Resilience Scale (BRS),38 a culturally validated tool with strong psychometric properties, including excellent internal consistency (Cronbach’s alpha > 0.80). Its concise nature and proven effectiveness in assessing resilience make it well-suited for evaluating the impact of cognitive reappraisal training on mental resilience in Chinese populations.
Depression Level
Depression level was measured using the Self-Rating Depression Scale (SDS),39 a widely-used tool for evaluating the severity of depressive symptoms. The SDS consists of 20 items that assess the frequency of depression-related thoughts and feelings, including mood, sleep, and concentration. Each item is rated on a 4-point Likert scale, where 0 indicates “some of the time” and 4 indicates “most of the time”. The SDS was selected due to its strong psychometric properties and its proven effectiveness in detecting depressive symptoms across different populations.
The Chinese version of the scale used in this study was developed by Cheung S.K. (1996),40 demonstrating good internal consistency (Cronbach’s alpha>0.80) and has been widely validated in both clinical and non-clinical settings, making it a reliable instrument for measuring depression level in this study.
Emotional State
The Positive and Negative Emotion Scale (PANAS) measured the participants’ emotional state,41 a well-established scale for measuring both positive and negative emotions. The PANAS consists of 20 adjectives, 10 describing positive emotions (eg, “enthusiastic”, “interested”) and 10 describing negative emotions (eg, “angry”, “nervous”). Participants rated the extent to which they experienced each emotion on a 5-point Likert scale, where 1 represents “not at all” and 5 represents “very much”.
The Chinese version of the International Positive and Negative Affect Schedule Short Form (I-PANAS-SF),42 was used to assess positive and negative emotions in this study. The version has been shown to have excellent internal consistency (Cronbach’s alpha > 0.80) and good nomological validity in a sample of Chinese adolescents in Hong Kong. Factor structure analysis supported the 9-item, two-factor model, making it suitable for measuring affective states in Chinese populations.
Procedure
Before data collection, participants were instructed on the study’s purpose and procedures. The research was conducted according to the principles of the Declaration of Helsinki, which was adopted by the World Medical Association. The study was approved by the ethical committee of Zhejiang University of Technology (Approval No.20240105DA1). Written and oral explanations were provided to the participants, and written informed consent was obtained from all subjects before the experiments. Data were collected anonymously. As an illustration, one example stimulus presented to participants was an image depicting a “patient in a hospital bed receiving infusion therapy”. They were instructed to write down multiple positive interpretations of the situation. Sample answers were then provided (Appendix 1). The first four reappraisal types were generated from 17 RIT categories.24 The “humor interpretation” type was added for this study, as evidence suggests that, in addition to serious reappraisal, humorous coping can be an effective reappraisal strategy.25
The training materials included 20 images from the International Affective Picture System selected as cognitive arousal tools.43 The system contains 64 negative images (injured animals, people carrying weapons, garbage piles, crashed cars, etc) and 16 neutral images (spoons, chessboards, etc).
As shown in Table 2, each day, each participant was shown four different pictures (three negative, one neutral) for cognitive reappraisal training, each displayed on a screen for 10 seconds. Participants had 10 minutes to think of as many cognitive reappraisal strategies as possible and were instructed to type out their coping responses. After this, they were given sample answers. Binary coding was employed to record the application of each strategy type, with a “1” denoting its use and a “0” indicating its absence.
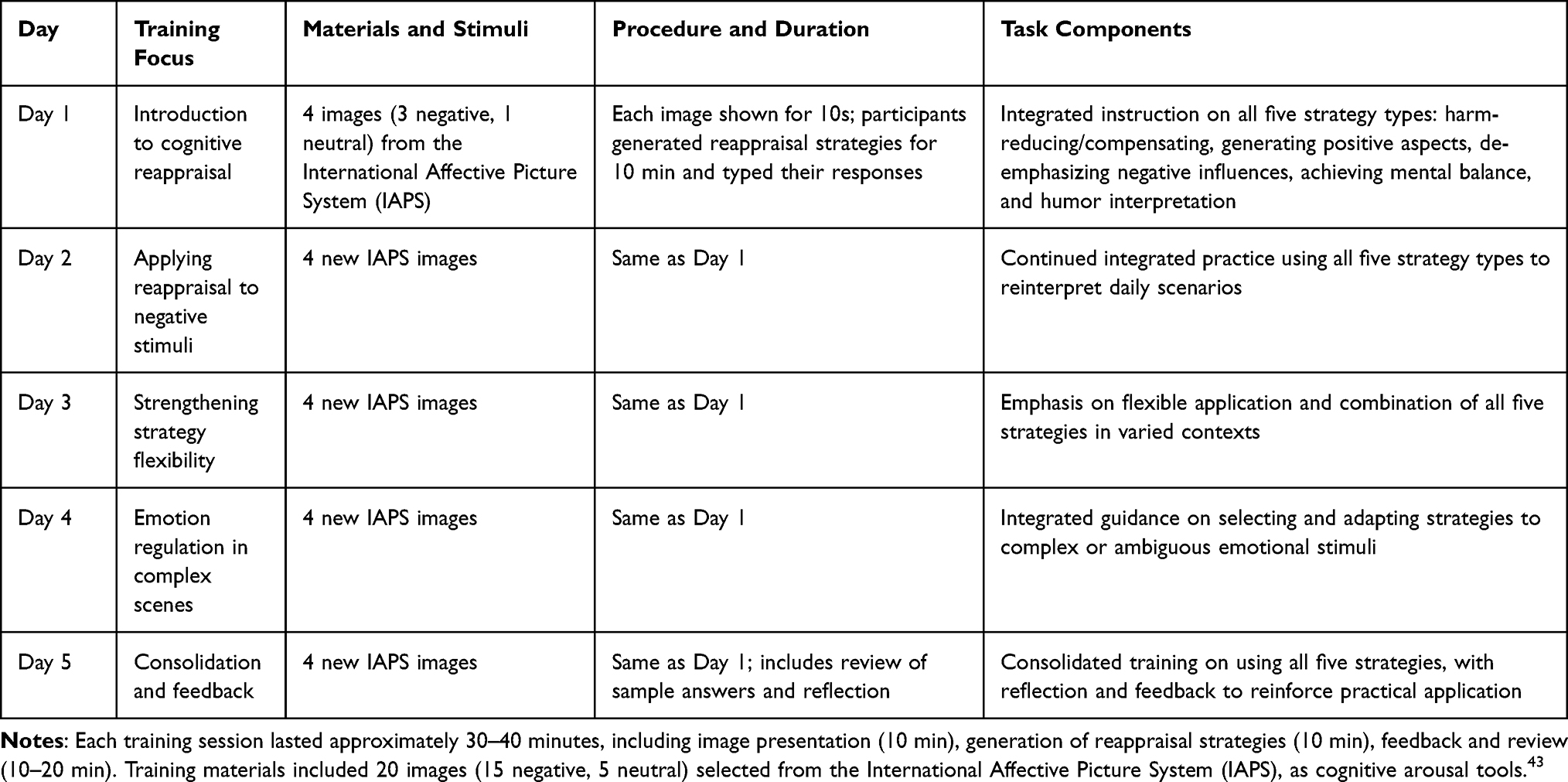 |
Table 2 Summary of the 5-Day Cognitive Reappraisal Training Procedure |
The training lasted five consecutive days, a duration consistent with established standards for short-term psychological and behavioral interventions and prior empirical studies.29,36 Participants’ cognitive reappraisal, mental resilience, depression level, and emotional state were assessed before the training, on the second day of training, on the fifth day of training, and on the 10th day after the training. A self-contrast method was adopted to test for differences before and after training.
Statistical Analysis
The data were analyzed using SPSS 27.0. software (IBM Corp., Armonk, NY, USA). Paired sample t-tests and Wilcoxon signed-rank tests were used to identify significant differences between paired groups and whether there were mental improvements following the training. The raw data of this study are available in the Appendix 2.
Correlation analysis was used to examine the relationships between cognitive reappraisal and various mental health indicators, such as resilience, emotional state, and depression. This approach helped assess the effectiveness of the training and identify the mechanisms through which cognitive reappraisal influences mental well-being.
To examine the potential psychological benefits of different emotion regulation strategies, each participant’s response was binary-coded for each strategy: “1” indicated that the strategy was applied, and “0” indicated that it was not applied. This coding enabled classification of participants into two groups for each specific strategy: strategy users and non-users. Pared-samples T tests were conducted to compare psychological outcome measures—including emotional state, depressive symptoms, and resilience—between the two groups. This approach allowed assessment of the effects of individual strategies on participants’ psychological outcomes while clearly distinguishing between strategy application and non-application.
To examine the potential influence of demographic characteristics on training outcomes, participants were grouped by age, gender, regional distribution, and Depression Severity. Independent-samples t-tests were used when parametric assumptions were satisfied. For variables with more than two subgroups, including regional distribution and depression severity, one-way ANOVA was applied. These analyses allowed assessment of whether the effectiveness of cognitive reappraisal training varied across demographic subgroups while ensuring statistical robustness.
Prior to conducting t-tests, Levene’s test was used to assess homogeneity of variances. In cases where the assumption of equal variances was not met, Welch-adjusted t-tests or non-parametric alternatives were applied to ensure the robustness of statistical inference.
Bonferroni correction was applied across all analyses, which is a commonly used correction method in multiple comparisons.43 Effect sizes were calculated using Cohen’s d for t-tests, r for non-parametric tests and correlation analyses, and η2 for ANOVA, following conventional guidelines for psychological research.
Results
Data Type and Processing
Descriptive statistical analysis was conducted to determine the normality of mental health sub-factors before analyzing the relationship between pre- and post-training data. The results showed that the mental resilience and depression level data followed a normal distribution. The changes were analyzed using a paired sample t-test. Cognitive reappraisal and emotional state data did not follow a normal distribution, and the data changes were analyzed using the Wilcoxon matched-pairs signed-rank test. Due to the abnormal distribution of cognitive reappraisal data, Spearman correlation analysis was used to explore the relationship between cognitive reappraisal and other mental reactions.
Changes in Cognitive Reappraisal Ability
Table 3 shows the changes in cognitive reappraisal ability. The Wilcoxon signed-rank tests were used for the analysis of CR1 and CR2. For CR1, it revealed significant differences between baseline and the second day (P<0.01), the fifth day (P<0.01), and the tenth day after training (P<0.01). For CR2, significant increases were observed from baseline to the second day (P<0.05), the fifth day (P<0.01), and the tenth day (P<0.05). Although the values of CR1 and CR2 on the tenth day was lower than on the second and fifth days, it remained significantly higher than baseline.
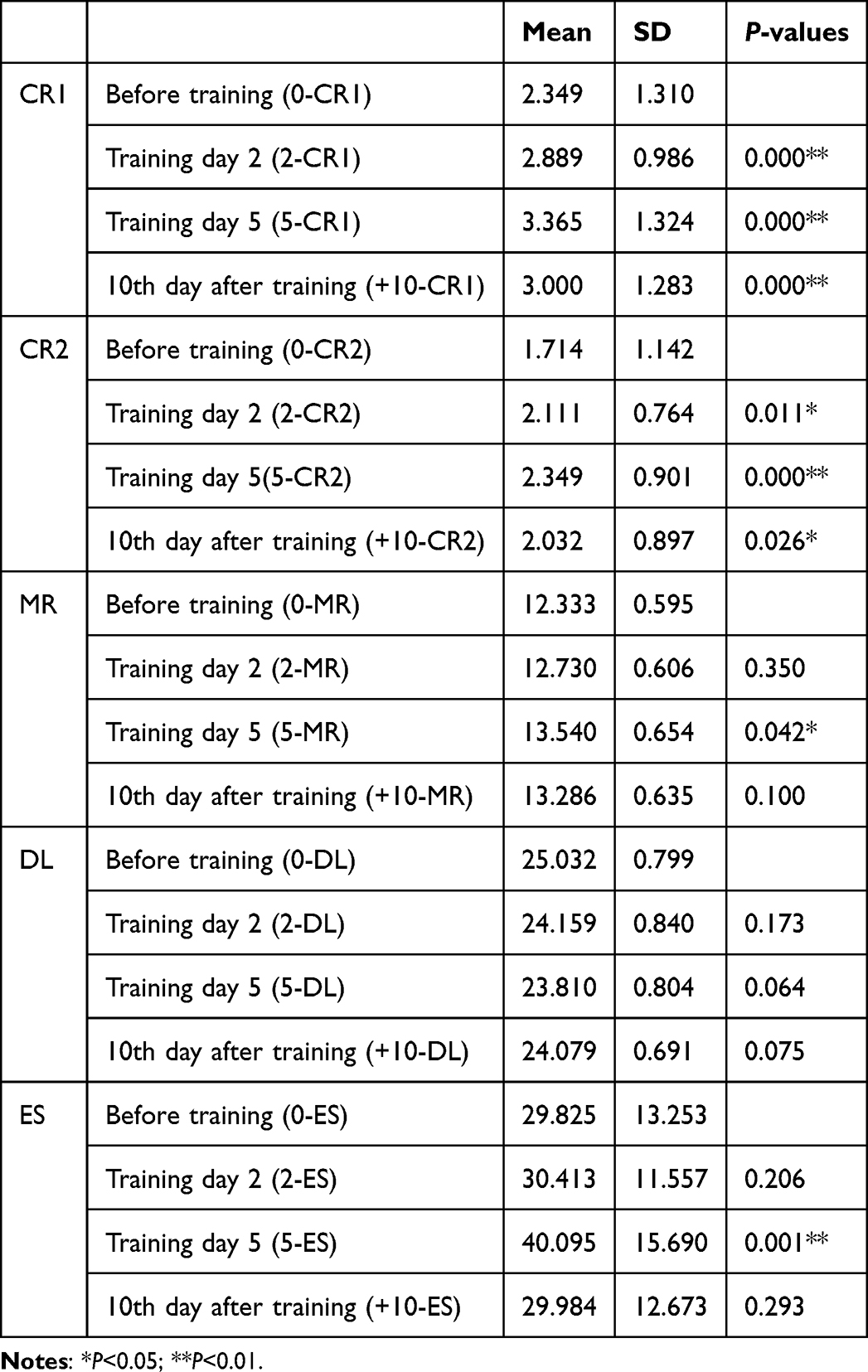 |
Table 3 Descriptive Statistics of Cognitive Reappraisal (CR), Mental Resilience (MR), Depression Level (DL), Emotional State (ES) (n=63) |
Changes in Mental Resilience
Paired sample t-tests showed changes in mental resilience. After two days of training, the mean mental resilience score increased from 12.333 to 12.730, and by the fifth day, it rose to 13.540. On the tenth day after training, the mean mental resilience score decreased compared to the fifth day but remained higher than before training. The improvement in mental resilience was only significant on the fifth day compared to pre-training scores (P<0.05).
Changes in Depression Level
Paired sample t-tests showed that depression level decreased during training but increased again after training (Table 3); however, the changes were not significant. The mean depression level dropped from 25.032 before training to 24.159 on the second day and 23.810 on the fifth day. Ten days after training, the mean increased to 24.079. However, these changes in depression level were not significant compared to pre-training levels (P>0.05).
Changes in Emotional State
The Wilcoxon signed-rank tests showed changes in emotional state. Higher scores for emotional state score represent more positive emotions. Table 3 shows that the mean of emotional state increased from the start of the training to the second day and further increased by the fifth day. On the tenth day after training, the emotional state mean decreased but remained slightly higher than that before training. The emotional state mean difference was significant only between the fifth day and the beginning (P<0.01). Despite emotional state improvements on the second day and the tenth day after training, they were not significant (P>0.05).
Relationship Between Cognitive Reappraisal and Mental Reactions
Table 4 shows the results of the Spearman correlation analysis. Before training, CR1 and CR2 were positively and significantly correlated with mental resilience (P<0.05) and significantly negatively correlated with depression level (P<0.01) but not significantly correlated with emotional state (P>0.05). On the second and fifth training days, cognitive reappraisal values were not significantly correlated with mental resilience, depression level, or emotional state (P>0.05). Ten days after training, CR1 and CR2 had a significant positive correlation with mental resilience (P<0.01) and a significant negative correlation with depression level (P<0.05). No significant correlation was found between cognitive reappraisal and emotional state (P>0.05).
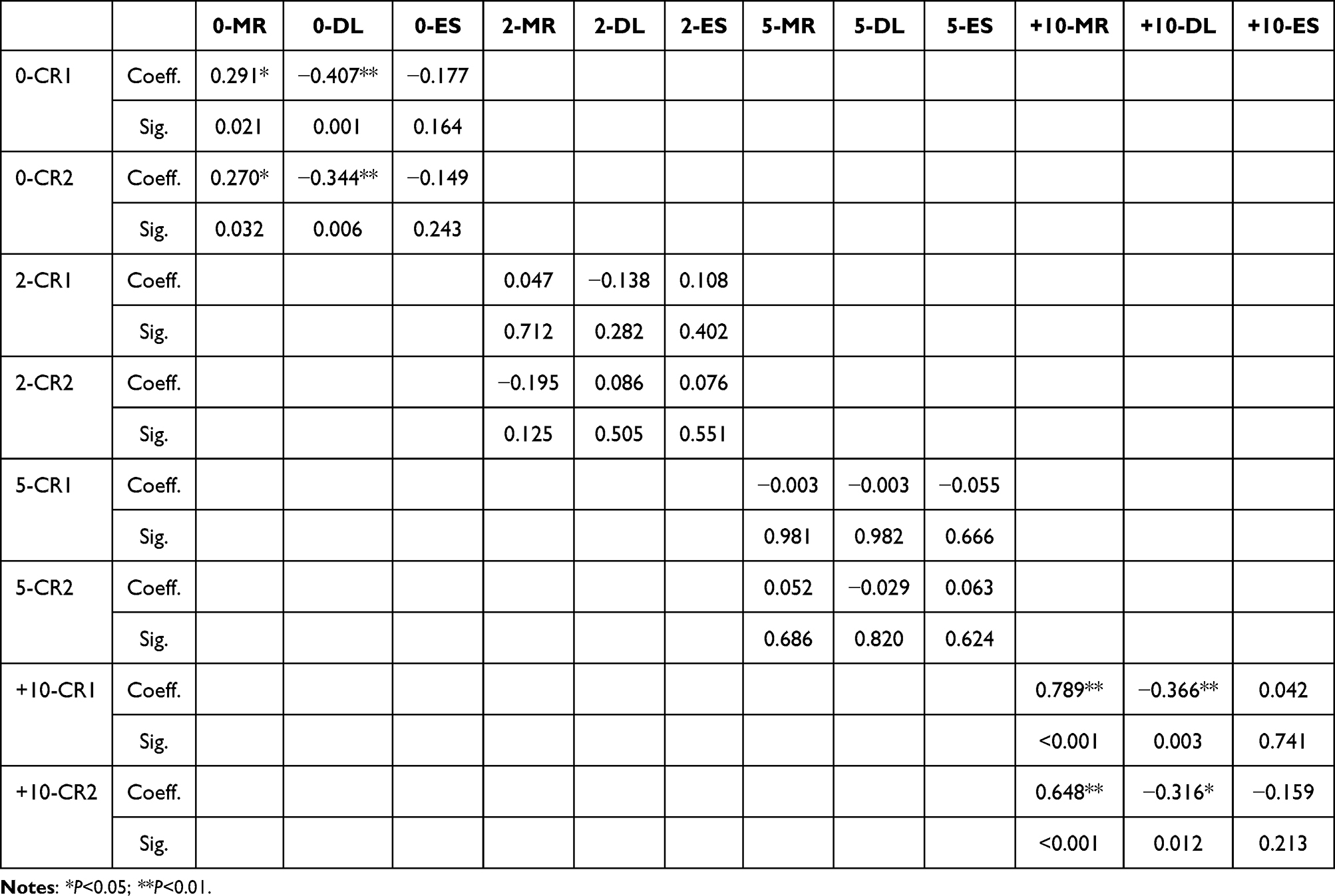 |
Table 4 Correlations Between Cognitive Reappraisal (CR) and Mental Resilience (MR), Depression Level (DL), and Emotional State (ES) |
Mental Well-Being Promotion Effects of Different Strategies
The results of the pared-samples T tests displayed in Table 5 indicate that the reappraisal strategies’ mental well-being promotion effects measured by CR1 showed significant differences for Strategy 1 (mean increased from 2.476 to 3.143, P<0.05) and Strategy 4 (mean increased from 1.714 to 2.238, P<0.01). The differences in CR2 were observed across Strategy 1 (mean increased from 2.105 to 3.105, P<0.05).
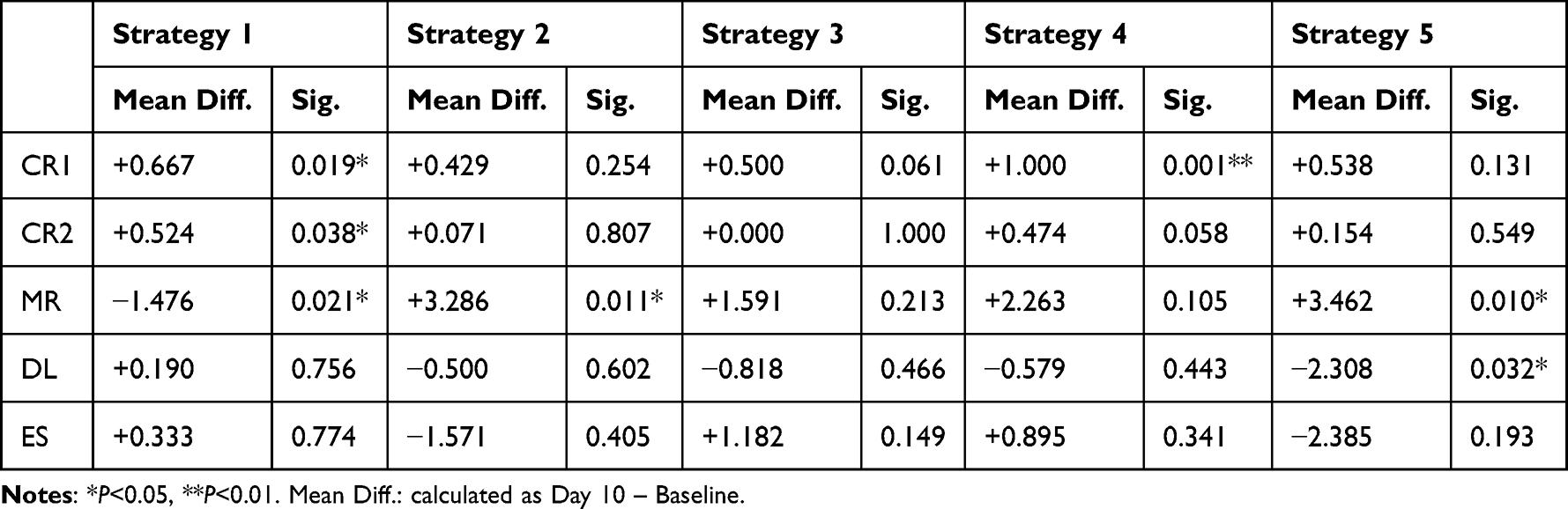 |
Table 5 Pre- Vs. Post-Training Comparisons of Cognitive Reappraisal (CR), Mental Resilience (MR), Depression Level (DL), and Emotional State (ES) Across Reappraisal Strategies |
Mental resilience were significantly different across Strategy 1, Strategy 2, and Strategy 5. After analyzing the changes in the means of mental resilience from baseline to the tenth day after training for each reappraisal strategy, mental resilience was found to be lower when participants utilized Strategy 1 (mean decreased from 13.048 to 11.571) during cognitive reappraisal training (P<0.05). Conversely, mental resilience increased when Strategy 2 (mean increased from 10.929 to 14.214, P<0.05) and Strategy 5 (mean increased from 10.385 to 13.846) were applied (P<0.05).
The mental well-being promotion effects of the reappraisal strategies, as measured by depression level, showed significant differences for Strategy 5. After comparing the mean depression level between the present and absent groups for each reappraisal strategy, depression level was significantly lower when participants utilized Strategy 5 (mean decreased from 26.692 to 24.384) during cognitive reappraisal training (P<0.05).
No significant differences in emotional state were observed across the various reappraisal strategies.
Mental Well-Being Promotion Effects of Different Demographic Groups
To examine the influence of demographic characteristics on training outcomes, participants were grouped by age, gender, regional distribution, and depression severity. Changes from baseline to Day 10 in cognitive reappraisal (CR1, CR2), mental resilience (MR), depression level (DL), and emotional state (ES) were calculated for each subgroup (Table 6).
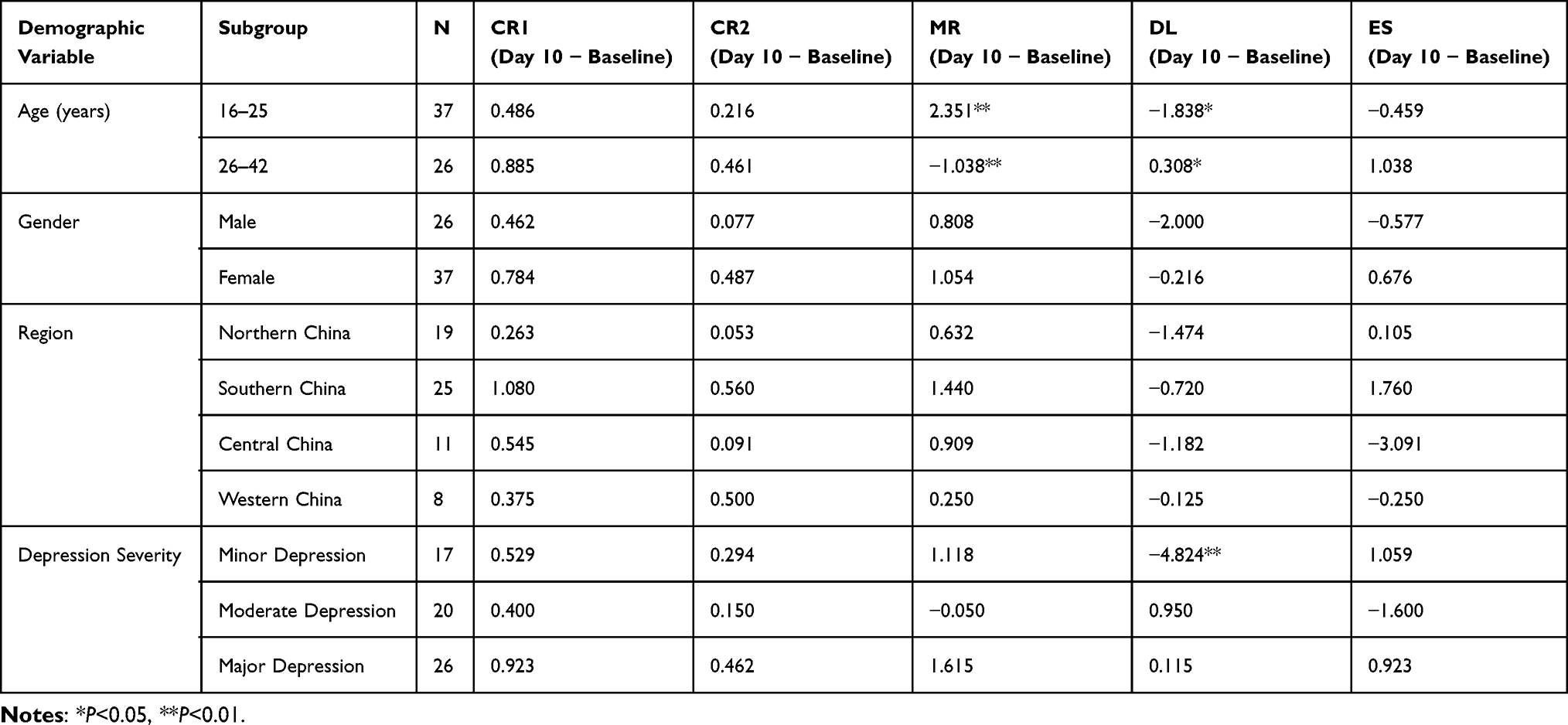 |
Table 6 Between-Group Differences in Cognitive Reappraisal (CR), Mental Resilience (MR), Depression Level (DL), and Emotional State (ES) Across Demographic Groups |
Independent-samples t-tests revealed significant differences between younger (16–25 years) and older participants (26–42 years) in MR (+2.351 vs. −1.038, P<0.01), and DL (−1.838 vs. +0.308, P<0.05), indicating larger improvements in mental resilience and and a greater reduction in depression levels among younger participants. No significant age-related differences were observed in CR1, CR2, or ES (P>0.05).
Comparisons between males and females showed no significant differences for any outcome measure (all P>0.05, Independent-samples t-tests). Regional comparisons across four areas (Northern, Southern, Central, Western China) revealed no significant differences in CR1, CR2, MR, DL, or ES (all P>0.05, one-way ANOVA).
Significant differences were observed across depression severity levels for DL (F=14.823, P<0.01), with participants with minor depression showing the greatest reductions in DL (−4.824). No significant differences were found in CR1, CR2, MR, or ES across depression severity levels (P>0.05, one-way ANOVA).
Effect Size Calculation and Hypotheses Testing
Overall, the results partially supported the proposed hypotheses.Consistent with H1, paired-sample comparisons showed that mental resilience increased significantly after cognitive reappraisal training, with a moderate effect size (Cohen’s d=0.56).In partial support of H2, depression levels showed a non-significant decreasing trend following training, with an observed effect size (Cohen’s d=0.38) that fell within the predicted small-to-moderate range. Supporting H3, participants’ positive emotional state improved significantly, with a moderate effect size (Cohen’s d=0.49).
Analysis of different cognitive reappraisal strategies revealed that Strategy 2 (generating positive aspects) and Strategy 5 (humor interpretation) produced significant improvements in mental resilience or reductions in depression. The effect sizes for these strategies were Cohen’s d=0.44 and Cohen’s d=0.52, respectively.
As for H5, age and depression severity significantly moderated the effectiveness of cognitive reappraisal training. Younger participants (16–25 years) showed larger improvements in mental resilience (Cohen’s d=0.45) and depression level (Cohen’s d=0.55) compared to older participants (26–42 years). Regarding depression severity, participants with minor depression exhibited the greatest reduction in depression (Cohen’s d=0.62).
Discussion
Effects of Cognitive Reappraisal
This study verified the impact of cognitive reappraisal training on mental health promotion and the relationship between cognitive reappraisal ability and psychological reactions. After training, mental resilience and emotional state improved while depression level decreased compared to before training. The changes in these values continued as the training progressed, indicating continuous mental improvement. These findings contribute to the growing body of research on cognitive reappraisal and its effects on mental well-being, consistent with recent studies.44,45
Significant changes in cognitive reappraisal scores during and after the training suggest the effectiveness and reliability of the training. This finding aligns with Ng and Diener (2013),46 who reported increased trait cognitive reappraisal after a 10-day program. Moreover, our results highlight the role of cognitive reappraisal as a modifiable trait that can be enhanced through targeted interventions, with potential for long-term mental health benefits.
The changes in depression level were not statistically significant, likely due in part to the limitations of the SDS tool, which provides a subjective assessment based on mental conditions over a previous period rather than real-time feedback on depressive states. Consequently, the tool may lack sufficient sensitivity to detect recent changes. This is an important consideration, as real-time assessments may offer more precise insights into the effects of cognitive reappraisal on depressive symptoms, as suggested by recent advancements in real-time affective reporting.47,48 Nevertheless, depression level evidently declined during training but rose again after training. This trend aligns with the finding that cognitive reappraisal training boosts well-being, reduces psychological distress, and mitigates negative emotional reactivity in stressful situations.26,47
The findings indicate that while mental resilience remained significantly higher than pre-training levels—suggesting a lasting cognitive reappraisal effect consistent with Samson et al25—both resilience and emotional state deteriorated from the fifth training day to 10 days post-training, accompanied by an increase in depression. This pattern implies that the benefits of training weaken after the intervention ends, though the only statistically significant changes were observed on the fifth day, pointing to an initial increase in effect strength over time. The post-training decline aligns with theories of psychological flexibility, which posit that sustained practice of adaptive strategies leads to enduring benefits that may diminish once practice ceases.49,50 Consequently, as noted by Goldberg SBi et al,51 ongoing practice or booster sessions may be necessary to maintain effects. Longer or repeated training periods could enhance and sustain the positive outcomes, and future studies should explore how extended interventions might mitigate the observed post-training decline.
The results further indicated that cognitive reappraisal ability (fluency and flexibility) were positively correlated with mental resilience and negatively correlated with depression level over the long term. This aligns with previous findings that trait cognitive reappraisal is positively associated with resilience and negatively correlated with depression.9,17,18 Notably, the correlations varied across different time points during and after training, which may reflect temporal fluctuations in participants’ engagement with reappraisal strategies, the limited sample size, and inherent variability in the measurement tools.
The correlations between cognitive reappraisal (CR) indices and psychological outcomes (mood recovery [MR], depressive levels [DL], and emotional state [ES]) varied across time points, reflecting the dynamic nature of short-term emotion regulation training. Significant baseline correlations indicate that initial reappraisal tendencies were closely linked to mental resilience and depression level, consistent with prior findings that higher dispositional reappraisal predicts better psychological outcomes.52 During the mid-phase of the intervention (Days 2 and 5), these associations largely disappeared, likely reflecting a transitional period in which participants were still integrating new strategies, resulting in more variable responses, as observed in early-stage reappraisal training.53 By the follow-up session (+10 days), correlations between CR and MR, as well as CR and DL, re-emerged, suggesting a delayed consolidation effect as strategies were internalized.54 Additional factors, including small sample size, inter-individual variability, and short-term measurement fluctuations, may have contributed to intermediate instability.55 These temporal dynamics indicate a non-linear trajectory of cognitive-emotional adaptation during and after short-term training.29
Regarding the types of cognitive reappraisal strategies, it was observed that when participants employed Strategy 5 (humor interpretation) during cognitive reappraisal training, depression level was significantly lower and mental resilience significantly higher. These findings suggest that the “humor interpretation” strategy is more effective in promoting mental well-being. This is consistent with previous research suggesting that humor-based cognitive reappraisal is effective in reducing negative emotions.43 Humor interpretation, by reframing stressful situations in a lighthearted way, may be particularly effective in mitigating negative emotional reactivity and promoting positive psychological outcomes.
Conversely, when participants utilized Strategy 1, mental resilience was significantly lower, indicating that the “harm-reducing or compensating” strategy may inhibit the promotion of mental-wellbeing, although it corresponds with an increase in Cognitive Reappraisal scores. One possible explanation is that although Strategy 1 emphasizes mitigating negative impacts, the mere presence of negative information can serve as a cue, directing individuals’ thoughts toward negative emotions. In contrast, Strategy 2, which emphasizes “generating positive aspects”, effectively promotes mental resilience by reinforcing only positive information rather than introducing and countering negative information. This aligns with theories of cognitive bias, which suggests that when negative information is introduced and subsequently countered, it may still leave a residual negative impression despite the rebuttal.35
The results of this study must also be understood in the context of the specific demographic characteristics of the participants. Previous research suggests that individual differences such as age, gender, and baseline mental health status may influence the effectiveness of cognitive reappraisal training.56,57
Impacts of Demographic Characteristics
In this study, participants ranged from 16 to 42 years old, with a fairly balanced gender distribution. The findings revealed significant variability in the effectiveness of cognitive reappraisal strategies across different age groups. Younger participants (ages 16–25) demonstrated more pronounced improvements in mental resilience and psychological health outcomes compared to older participants (ages 26–42). This suggests that cognitive reappraisal may be more effective for younger individuals, likely due to their greater cognitive flexibility and neuroplasticity. In contrast, older participants showed more gradual changes, with smaller improvements in resilience and depression, despite the overall positive trend in the sample.
These results are consistent with the hypothesis that younger individuals may adapt more quickly to emotion regulation strategies such as cognitive reappraisal. This may be because younger adults tend to exhibit more flexible cognitive processes, allowing them to more easily integrate and apply new emotion regulation techniques. Nolen-Hoeksema et al56 similarly found that younger individuals show stronger emotional regulation improvements following cognitive reappraisal training, possibly due to their more adaptable neural circuitry. In contrast, older adults, who tend to have more stable, habitual ways of responding to emotional challenges, may require additional time or tailored interventions to experience similar benefits. This observation aligns with findings from Ochsner et al,58 who found that aging is associated with slower changes in brain activity related to emotion regulation.
Results indicate that baseline depression severity significantly moderated the psychological benefits of cognitive reappraisal training. Participants with minor depression showed the the greatest reduction in depressive symptoms, whereas improvements were progressively smaller among those with moderate and major depression. This pattern is consistent with prior work suggesting that lighter symptom burden is associated with greater cognitive flexibility and more effective uptake of emotion regulation strategies.56,59 In contrast, more severe depression is often characterized by impaired cognitive control and entrenched negative appraisal habits, which may limit the translation of trained skills into clinical improvements.60
Overall, these findings support stepped or tailored intervention approaches, whereby cognitive reappraisal training may be most suitable as a low-intensity, preventive strategy for those with mild symptoms, whereas individuals with more severe depression may require additional therapeutic support to experience comparable emotional benefits.
Limitations
This study has some limitations due to the small sample size and limited training time.
First, the study employed a within-subject pre–post design without the inclusion of a separate control group, which constrains the ability to establish causal inferences. Although changes were observed across assessment points, it remains uncertain whether these improvements in cognitive reappraisal, resilience, and emotional state can be attributed solely to the intervention, as they may also reflect spontaneous recovery, expectancy effects, or time-related factors. To enhance causal validity and rule out alternative explanations, Future research should strengthen the evidence base by employing randomized controlled trial (RCT) designs, in which participants are randomly assigned to a cognitive reappraisal training group and an active or waitlist control group.
Second, this study’s sample was self-selected from digitally active communities, which may introduce selection bias. Participants’ willingness to discuss mental health online may not reflect the broader population with depression, limiting the generalizability of the findings, especially to less digitally engaged individuals.
Third, the reliance on self-report measures introduces potential demand characteristics and social desirability bias. Participants may have been inclined to provide responses consistent with expected outcomes rather than their actual experiences, which could influence the accuracy of the findings. Incorporating behavioral, physiological, or third-party assessments in future research would help mitigate these biases and yield more objective evidence.
Fourth, to operationalize participants’ use of cognitive reappraisal strategies, responses were initially coded in a binary format (“1”=strategy used, “0”=strategy not used). It is acknowledged that this binary coding does not capture frequency or intensity of strategy use, and future studies may adopt more nuanced coding schemes to assess strategy strength and combination effects.
Fifth, the study did not provide an in-depth examination of Chinese cultural factors that might have shaped participants’ emotion regulation patterns and the effectiveness of cognitive reappraisal. Cultural norms regarding emotional expression, interpersonal harmony, and self-restraint may have influenced how individuals engaged with and benefited from reappraisal training. Moreover, the exclusive focus on a Chinese sample, combined with constraints related to online access and financial resources, limited the possibility of cross-cultural comparison. As a result, the regional cultural context was not sufficiently reviewed, and the generalizability of the findings beyond the Chinese setting remains uncertain. Future research should incorporate culturally sensitive frameworks and comparative samples to better understand how sociocultural factors mediate cognitive-emotional processes across contexts.
Moreover, the relatively brief duration of the intervention may have limited the extent of observed improvements in certain psychological responses. Extending the training period to several weeks or months (eg, 8–24 weeks) would allow participants more time to practice, consolidate, and internalize cognitive reappraisal techniques, facilitating more stable behavioral and emotional changes. In addition, incorporating structured booster sessions (eg, brief refresher trainings delivered weekly or monthly after the core intervention) may help reinforce learned strategies and prevent skill decay. Such designs would allow for clearer causal inference regarding training effects and provide more robust evidence on the sustainability of cognitive reappraisal interventions. Furthermore, incorporating additional follow-up assessments—such as at one, three, and six months post-intervention—would enable evaluation of both short-term and long-term effects, providing clearer evidence regarding the persistence and reinforcement of training benefits.
Conclusion
This study explored the effects of cognitive reappraisal training on mental resilience, depression level, and emotional state among Chinese individuals with depressive disorders. Results showed that the training promoted psychological well-being, reduced distress (with cumulative and persistent effects), and cognitive reappraisal ability significantly predicted mental health; among strategies, “humor interpretation” was most effective, followed by “generating positive aspects”; younger participants (16–25) and those with minor depression showed the largest gains, while gender and region showed no significant differences. These findings offer empirical insights for clinicians and mental health professionals, applicable in clinical, educational, and workplace settings—providing actionable emotional regulation strategies for depressed individuals and supporting resilience-building in general populations.
Nevertheless, the findings should be interpreted cautiously due to a relatively small, culturally specific Chinese sample, limiting generalizability to other populations/cultures. Future studies should replicate with larger, more diverse samples, employ randomized controlled designs to verify causality, and extend training/follow-up durations to clarify long-term intervention stability. Overall, this study provides evidence-based, culturally grounded insights into cognitive reappraisal training’s practical value for enhancing emotional regulation and psychological resilience in Chinese contexts.
Acknowledgments
We gratefully acknowledge the guidance of Dr. Manlin Qi, a qualified physician at the College of Medicine, Jilin University, who provided professional input regarding the clinical appropriateness of the study design and contributed valuable advice throughout the research process. We also sincerely thank all the participants who generously took part in this study.
Funding
This work was supported by the Routine Project of Philosophy and Social Science Planning, Hangzhou, China (grant number Z24JC001); the Department of Education of Zhejiang Province, China (grant number 2024GH062); Chinese Fund for the Humanities and Social Science (grant number 20WYSB002); and the Annual Project of the Humanities and Social Sciences Research Fund, Zhejiang University of Technology (grant number SKY-ZX-20240023).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Gross JJ, Thompson RA. Emotional regulation: conceptual foundations. In: Gross JJ, editor. Handbook of Emotion Regulation. Guilford Press; 2007:3–16.
2. Gross JJ. Emotion regulation in adulthood: timing is everything. Curr Dir Psychol Sci. 2001;10(6):214–219. doi:10.1111/1467-8721.00152
3. Brans K, Koval P, Verduyn P, Lim YL, Kuppens P. The regulation of negative and positive affect in daily life. Emotion. 2013;13(5):926–939. doi:10.1037/a0032400
4. Hayes JP, Morey RA, Petty CM, et al. Staying cool when things get hot: emotion regulation modulates neural mechanisms of memory encoding. Front Hum Neurosci. 2010;4:230. doi:10.3389/fnhum.2010.00230
5. Hong F, Tarullo AR, Mercurio AE, Liu S, Cai Q, Malley-Morrison K. Childhood maltreatment and perceived stress in young adults: the role of emotion regulation strategies, self-efficacy, and resilience. Child Abuse Negl. 2018;86:136–146. doi:10.1016/j.chiabu.2018.09.014
6. Kalisch R, Baker DG, Basten U, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Hum Behav. 2017;1(11):784–790. doi:10.1038/s41562-017-0200-8
7. Schanowitz JY, Nicassio PM. Predictors of positive psychosocial functioning of older adults in residential care facilities. J Behav Med. 2006;29(2):191–201. doi:10.1007/s10865-005-9034-3
8. Hanley AW, Palejwala MH, Hanley RT, Canto AI, Garland EL. A failure in mind: dispositional mindfulness and positive reappraisal as predictors of academic self-efficacy following failure. Pers Individ Dif. 2015;86:332–337. doi:10.1016/j.paid.2015.06.033
9. Aliche JC, Onyishi IE. Mindfulness and wellbeing in older adults’ survivors of herdsmen attack. The mediating effect of positive reappraisal. Aging Mental Health. 2020;24(7):1132–1140. doi:10.1080/13607863.2019.1602592
10. Yan M, Zhang L, Qin D, et al. Examining the effects of psychological resilience and wellbeing on perceived stress and depressive symptoms among undergraduate nursing interns: testing a moderated mediation model. Front Public Health. 2024;12:1497076. doi:10.3389/fpubh.2024.1497076
11. Zhu Z, Sang B, Liu J, et al. Associations between emotional resilience and mental health among Chinese adolescents in the school context: the mediating role of positive emotions. Behav Sci. 2025;15(5):567. doi:10.3390/bs15050567
12. Dawel A, Mewton P, Gulliver A, et al. For whom and what does cognitive reappraisal help? A prospective study. Cognit Ther Res. 2024;48(4):687–703. doi:10.1007/s10608-023-10407-3
13. Hu J, Wu X, Yu T. How does cognitive reappraisal longitudinally contribute to psychological resilience among adolescents: evidence based on the affect-regulation framework. Psychol Rep. 2025. doi:10.1177/00332941251397333
14. Wang J, Wang T, Cheng Y. Resilience as a moderator of the relationship between stress and different symptom dimensions of depression in adolescents with a history of childhood maltreatment: a multi-wave longitudinal study. Child Abuse Negl. 2024;154:106888. doi:10.1016/j.chiabu.2024.106888
15. Fried EI, Nesse RM. Depression is not a consistent syndrome: an investigation of unique symptom patterns in the STAR*D study. J Affect Disord. 2015;172:96–102. doi:10.1016/j.jad.2014.10.010
16. Everaert J, Joormann J. Emotion regulation difficulties related to depression and anxiety: a network approach to model relations among symptoms, positive reappraisal, and repetitive negative thinking. Clin Psychol Sci. 2019;7(6):1304–1318. doi:10.1177/2167702619859342
17. Mahali SC, Beshai S, Wolfe WL. The associations of dispositional mindfulness, self-compassion, and reappraisal with symptoms of depression and anxiety among a sample of Indigenous students in Canada. J Am Coll Health. 2020;69(8):872–880. doi:10.1080/07448481.2020.1711764
18. Plate AJ, Dunn EJ, Christensen K, Aldao A. When are worry and rumination negatively associated with resting respiratory sinus arrhythmia? It depends: the moderating role of cognitive reappraisal. Cognit Ther Res. 2020;44(4):874–884. doi:10.1007/s10608-020-10099-z
19. Mahali SC, Beshai S, Feeney JR, Mishra S. Associations of negative cognitions, emotional regulation, and depression symptoms across four continents: international support for the cognitive model of depression. BMC Psychiatry. 2020;20(1):18. doi:10.1186/s12888-019-2423-x
20. Folkman S, Lazarus RS, Gruen RJ, DeLongis A. Appraisal, coping, health status, and psychological symptoms. J Pers Soc Psychol. 1986;50(3):571–579. doi:10.1037//0022-3514.50.3.571
21. Kobylińska D, Kusev P. Flexible emotion regulation: how situational demands and individual differences influence the effectiveness of regulatory strategies. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.00072
22. Ochsner KN, Gross JJ. The cognitive control of emotion. Trends Cognit Sci. 2005;9(5):242–249. doi:10.1016/j.tics.2005.03.010
23. Shiota MN, Levenson RW. Turn down the volume or change the channel? Emotional effects of detached versus positive reappraisal. J Pers Soc Psychol. 2012;103(3):416–429. doi:10.1037/a0029208
24. Weber H, Loureiro de Assunção VL, Martin C, Westmeyer H, Geisler FC. Reappraisal inventiveness: the ability to create different reappraisals of critical situations. Cogn Emot. 2014;28(2):345–360. doi:10.1080/02699931.2013.832152
25. Samson AC, Glassco AL, Lee IA, Gross JJ. Humorous coping and serious reappraisal: short-term and longer-term effects. Eur J Psychol. 2014;10(3):571–581. doi:10.5964/ejop.v10i3.730
26. Ranney RM, Bruehlman-Senecal E, Ayduk O. Comparing the effects of three online cognitive Reappraisal trainings on well-being. J Happiness Stud. 2017;18(5):1319–1338. doi:10.1007/s10902-016-9779-0
27. Pogrebtsova E, Son Hing L, González-Morales MG. Effectiveness of an emotion regulation intervention versus an active control on daily well-being and cognitive reappraisal: an experience sampling randomized controlled trial. Int J Stress Manag. 2022;29(4):400–412. doi:10.1037/str0000259
28. Salazar Kämpf M, Adam L, Rohr MK, et al. A meta-analysis of the relationship between emotion regulation and social affect and cognition. Clin Psychol Sci. 2023;11(1):1159–1189. doi:10.1177/21677026221149953
29. Denny BT, Ochsner KN. Behavioral effects of longitudinal training in cognitive reappraisal. Emotion. 2014;14(2):425–433. doi:10.1037/a0035276
30. Pruessner L, Timm C, Kalmar J, Bents H, Barnow S, Mander J. Emotion regulation as a mechanism of mindfulness in individual cognitive-behavioral therapy for depression and anxiety disorders. Depress Anxiety. 2024;41(8):725–737. doi:10.1155/2024/9081139
31. Sharma N, Agrawal M, Rushi AS, Rai D, Rai D. Mindfulness-based interventions for emotional dysregulation in adolescents: a systematic review. Ann Neurosci. 2025. doi:10.1177/09727531251355311
32. Bormann JE, Carrico AW. Increases in positive reappraisal coping during a group-based mantram intervention mediate sustained reductions in anger in HIV-positive persons. Int J Behav Med. 2009;16(1):74–80. doi:10.1007/s12529-008-9007-3
33. Doré BP, Morris RR, Burr DA, Picard RW, Ochsner KN. Helping others regulate emotion predicts increased regulation of one’s own emotions and decreased symptoms of depression. Pers Soc Psychol Bull. 2017;43(5):729–739. doi:10.1177/0146167217695558
34. Garland EL, Gaylord SA, Fredrickson BL. Positive reappraisal mediates the stress-reductive effects of mindfulness: an upward spiral process. Mindfulness. 2011;2(1):59–67. doi:10.1007/s12671-011-0043-8
35. Garnefski N, Kraaij V. Cognitive emotion regulation questionnaire—development of a short 18-item version (CERQ-short). Pers Individ Dif. 2006;41(6):1045–1053. doi:10.1016/j.paid.2006.04.010
36. Troy AS, Wilhelm FH, Shallcross AJ, Mauss IB. Seeing the silver lining: cognitive reappraisal ability moderates the relationship between stress and depressive symptoms. Emotion. 2010;10(6):783–795. doi:10.1037/a0020262
37. Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008;15(3):194–200. doi:10.1080/10705500802222972
38. Chen W, Liu J, Luo J, Liu GQ. Reliability and validity of the Chinese version of brief resilience scale. Chin J Clin Psychol. 2020;28(1):24–28.
39. Sepehry AA. Self-rating depression scale (SDS). In: Encyclopedia of Quality of Life and Well-Being Research. Cham: Springer International Publishing; 2021:1–9.
40. Cheung SK. Reliability and factor structure of the Chinese version of the depression self-rating scale. Educ Psychol Meas. 1996;56(1):142–154. doi:10.1177/0013164496056001011
41. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the Panas scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037//0022-3514.54.6.1063
42. Liu JD, You RH, Liu H, Chung PK. Chinese version of the international positive and negative affect schedule short form: factor structure and measurement invariance. Health Qual Life Outcomes. 2020;18(1):285. doi:10.1186/s12955-020-01526-6
43. Lang PJ, Bradley MM, Cuthbert BN. International Affective Picture System (IAPS): Technical Manual and Affective Ratings. University of Florida, Center for Research in Psychophysiology; 1995.
44. Hofmann SG, Hayes SC, Lorscheid DN. Learning Process-Based Therapy: A Skills Training Manual for Targeting the Core Processes of Psychological Change in Clinical Practice. Oakland (CA): New Harbinger Publications; 2021.
45. Lu T, Liu K, Feng X, Zhang X, She Z. The impact of cognitive reappraisal intervention on depressive tendencies in Chinese college students: the mediating role of regulatory emotional self-efficacy. Behav Sci. 2025;15(5):562. doi:10.3390/bs15050562
46. Ng W, Diener E. Daily use of reappraisal decreases negative emotions toward daily unpleasant events. J Soc Clin Psychol. 2013;32(5):530–545. doi:10.1521/jscp.2013.32.5.530
47. Trull TJ, Ebner-Priemer UW. Ambulatory assessment in psychopathology research: a review of recommended reporting guidelines and current practices. J Abnorm Psychol. 2020;129(1):56–63. doi:10.1037/abn0000473
48. Kuppens P, Verduyn P. Emotion dynamics. Curr Opin Psychol. 2017;17:22–26. doi:10.1016/j.copsyc.2017.06.004
49. Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change.
50. Roemer L, Orsillo SM. Mindfulness- and Acceptance-Based Behavioral Therapies in Practice. New York: Guilford Press; 2008.
51. Goldberg SB, Riordan KM, Sun S, Davidson RJ. The empirical status of mindfulness-based interventions: a systematic review of 44 meta-analyses of randomized controlled trials. Perspect Psychol Sci. 2022;17(1):108–130. doi:10.1177/1745691620968771
52. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348–362. doi:10.1037/0022-3514.85.2.348
53. O’Toole MS, Renna ME, Mennin DS, Fresco DM. Changes in decentering and reappraisal temporally precede symptom reduction during emotion regulation therapy for generalized anxiety disorder with and without co-occurring depression. Behav Ther. 2019;50(6):1042–1052. doi:10.1016/j.beth.2018.12.005
54. Wang YX, Yin B. A new understanding of the cognitive reappraisal technique: an extension based on the schema theory. Front Behav Neurosci. 2023;17:1174585. doi:10.3389/fnbeh.2023.1174585
55. Hu D, Tamir M. Variability in emotion regulation strategy use in major depressive disorder: flexibility or volatility? J Affect Disord. 2025;372:306–313. doi:10.1016/j.jad.2024.12.027
56. Nolen-Hoeksema S. Emotion regulation and psychopathology: the role of gender. Annu Rev Clin Psychol. 2012;8(1):161–187. doi:10.1146/annurev-clinpsy-032511-143109
57. Goldin PR, McRae K, Ramel W, Gross JJ. The neural bases of emotion regulation: reappraisal and suppression of negative emotion. Biol Psychiatry. 2008;63(6):577–586. doi:10.1016/j.biopsych.2007.05.031
58. Ochsner KN, Ray RD, Cooper JC, et al. For better or for worse: neural systems supporting the cognitive down-and up-regulation of negative emotion. Neuroimage. 2004;23(2):483–499. doi:10.1016/j.neuroimage.2004.06.030
59. Joormann J, Stanton CH. Examining emotion regulation in depression: a review and future directions. Behav Res Ther. 2016;86:35–49. doi:10.1016/j.brat.2016.07.007
60. Joormann J, Gotlib IH. Emotion regulation in depression: relation to cognitive inhibition. Cogn Emot. 2010;24(2):281–298. doi:10.1080/02699930903407948
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.