Back to Journals » Clinical Ophthalmology » Volume 16
Effects of Bilateral Medial Rectus Resection on Motor Outcomes in Infantile Exotropia
Authors Yagasaki T ![]() , Yokoyama Y
, Yokoyama Y ![]() , Yagasaki A
, Yagasaki A ![]() , Tsukui M
, Tsukui M
Received 11 April 2022
Accepted for publication 8 June 2022
Published 21 June 2022 Volume 2022:16 Pages 2047—2056
DOI https://doi.org/10.2147/OPTH.S370266
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Teiji Yagasaki,1,2 Yoshimi Yokoyama,2 Ayaka Yagasaki,2,3 Makiko Tsukui2
1Yagasaki Eye Clinic, Ichinomiya, Aichi, Japan; 2Department of Ophthalmology, Japan Community Health Care Organization Chukyo Hospital, Nagoya, Aichi, Japan; 3Department of Ophthalmology, Gifu Prefectural General Medical Center, Gifu, Gifu, Japan
Correspondence: Teiji Yagasaki, Yagasaki Eye Clinic, 62-6 Gonaka, Kaimei, Ichinomiya, Aichi, 494-0001, Japan, Tel +81-586-61-8787, Fax +81-586-61-9210, Email [email protected]
Purpose: To evaluate the effects of bilateral medial rectus resection (BMRres) on motor outcomes in infantile exotropia.
Methods: We evaluated 19 cases of infantile exotropia surgery. The mean age at surgical alignment was 4.8± 3.4 years (range, 1.5– 11.8 years). The surgical procedures included BMRres (5 cases), BMRres with unilateral lateral rectus recession (ULRR) (3 cases), bilateral lateral rectus recession (BLRR) (8 cases), unilateral lateral rectus recession and medial rectus resection (uniRandR) with contralateral lateral rectus recession (2 cases), and uniRandR (1 case). After dividing the cases into two groups (BMRres group, n=8; other group, n=11), the outcomes at 1 day and at 1, 3, and 6 months after surgery were compared. Surgical outcomes were defined as (1) success: distant esotropia ≤ 5 prism diopters (Δ) or exotropia ≤ 10Δ, (2) recurrence: exotropia > 10Δ, or (3) overcorrection: esotropia > 5Δ.
Results: Although postoperative distant deviations at 1 day were not different between the two groups, the BMRres group showed smaller distant deviations at 1, 3, and 6 months than the other group (p=0.015, 0.019, and 0.006, respectively). Success rates of the BMRres and other groups were 88% and 73% at 1 day, 100% and 36% at 1 month, 88% and 27% at 3 months, 88% and 18% at 6 months, respectively. Although there were no significant differences between the two groups within 3 months after surgery, surgical outcomes in the BMRres group 6 months after surgery were significantly better than those in the other group (p=0.003).
Conclusion: BMRres is a better procedure than others for infantile exotropia to achieve desirable motor outcomes after surgery.
Keywords: infantile exotropia, strabismus surgery, bilateral medial rectus resection, motor outcome
Introduction
Infantile exotropia is a rare motility disorder that appears before the first year of age and has been defined as idiopathic, large-angle, intermittent, or constant exotropia without any other ocular or neurological disorder.1 Surgical intervention for infantile exotropia before the age of 24 months is recommended to obtain optimal motor and sensory results.2–8 However, in most infantile exotropia cases, the outcomes of long-term ocular alignment after surgery have been disappointing, with the major reason for unsuccessful postoperative results yet to be determined.1
Recently, the most common procedure for infantile exotropia has been the use of bilateral lateral rectus recession (BLRR),2–8,11–15 unilateral lateral rectus recession (ULRR), or unilateral lateral rectus recession and medial rectus resection (uniRandR).13–16 However, the surgical results of these procedures for infantile exotropia are yet to be definitively proven. Another procedure used for exotropia is bilateral medial rectus resection (BMRres), which is indicated for convergence-insufficiency exotropia.17,18 To our knowledge, there have been few reports on the surgical results of BMRres as a basic procedure for infantile exotropia.19 Although the number of cases treated with BMRres is small, we also have impressions that better results have been obtained by performing this procedure for infantile exotropia.
The purpose of this study was to compare postoperative motor outcomes in patients treated for infantile exotropia with BMRres and other procedures.
Subjects and Methods
This study prospectively recruited all patients diagnosed with infantile exotropia with onset prior to 12 months of age and who were undergoing surgical alignment between 2010 and 2019. Patients with any other ocular or neurologic disorder, mental retardation, or systemic disease (including prematurity defined as a gestational age of <37 weeks), or who had undergone previous eye muscle surgery were excluded. Patients with craniosynostosis were excluded from this study. Age at onset was confirmed by both the first observation of an ocular misalignment by either a parent or guardian and evidence of these changes in previous photographs of the patients. Nineteen patients met the inclusion criteria.
All patients underwent complete ophthalmologic and orthoptic examinations at their first visit. Full cycloplegic hyperopic refraction was performed using 1% atropine sulfate eye drops, and all recorded deviations were verified using appropriate spectacle correction. In most patients, the alternate prism cover test for fixation at 1, 3, and 6 months was performed to measure the angle of infantile exotropia. The Krimsky method was used in cases of poor cooperation during the alternate prism cover test. To differentiate between the clinical characteristics according to the type of exotropia present at the time of onset, the patients were divided into those with constant or intermittent exotropia (CXT and IXT, respectively).
Infantile exotropia is a specific type of strabismus and some cases have systemic complications. Therefore, we performed a routine diagnostic imaging test for infantile exotropia, if possible. Biorbital angle measurements were obtained using axial magnetic resonance imaging (MRI) or computed tomography (CT) of the orbit in the transverse plane of the horizontal extraocular muscle. The biorbital angle is defined as the angle formed by the intersection of both lines running tangentially along the deep lateral wall.9,10
The surgical procedure details for the 19 patients were as follows: BMRres (5 cases), BMRres with ULRR (3 cases), BLRR (8 cases), uniRandR with contralateral lateral rectus recession (2 cases) and uniRandR (1 case). After dividing the patients who underwent exotropia surgery into two groups, we compared the postoperative outcomes and clinical features. The BMRres group consisted of 8 patients with resected bilateral medial rectus muscle, while the other group consisted of 11 patients who underwent other procedures. The selection of surgical procedure did not reflect the results of diagnostic imaging and was decided at random.
Postoperative alignments at distance and at near were measured at 1 day after surgery; 1, 3, and 6 months after surgery; and at the final visit. All study patients were assigned to one of the following postsurgical criteria: (1) success, defined as ocular distant alignment with esotropia of ≤5 prism diopters (Δ) or exotropia of ≤10Δ; (2) recurrence, defined as exotropia of >10Δ; or (3) overcorrection, defined as esotropia of >5Δ.
This study was conducted in accordance with ethical approval for the study obtained from the Clinical Research Ethics Committee of the Japan Community Health Care Organization Chukyo Hospital (approval no. 2,010,031). All data collection conformed to local laws, and informed consent was obtained from all parents or guardians of the patients. All medical procedures were performed in accordance with the tenets of the Declaration of Helsinki.
Where appropriate, the Mann–Whitney U-test, Fisher’s exact test, or chi-squared test was used to compare the angle of deviations and the biorbital angle. One-way ANOVA, the Kruskal–Wallis test, or the Dunn test were also used to compare the outcomes of exodeviation at 1 day and at 1, 3, and 6 months after surgery. The independent t-test or Welch’s t-test were also used to compare the other mean values, with two-tailed p-values of <0.05 considered statistically significant.
Results
All Study Patients
Table 1 shows the characteristics and preoperative and postoperative results of all study patients. The mean age at the first visit was 3.1±2.9 years. All 19 patients exhibited basic-type exotropia, with 12 (63%) presenting with constant deviation (CXT group) and 7 (37%) with intermittent deviation (IXT group). The mean age at the time of MRI or CT examination was 3.8±3.5 years. The mean biorbital angle was 108.2±9.5°, which was significantly larger than the 94.3±5.1° previously found in 129 normal infants.11 The mean exodeviation before surgery was 48.2±14.3Δ (range, 30–80Δ) at distance and 48.7±14.1Δ (range, 25–80Δ) at near. Significant differences were found in the postoperative alignment at 1 day and at the other visits (at distance: 1 month, p=0.015; 3 months, p<0.001; 6 months, p<0.001; at near: 1 month, p=0.004; 3 months, p<0.001; 6 months, p<0.001). Moreover, the means for distant and near exodeviations at 6 months after surgery were significantly larger than those observed at 1 month after surgery (Figures 1 and 2). The success, overcorrection, and recurrence rates 1 day after surgery were 78% (15 cases), 11% (2 cases), and 11% (2 cases), respectively. The distribution of success, overcorrection, and recurrence worsened during the postoperative follow-up with these rates at 6 months after surgery, which were calculated to be 47% (9 cases), 0.0% (0 cases), and 53% (10 cases), respectively (1 day vs 6 months: p=0.044).
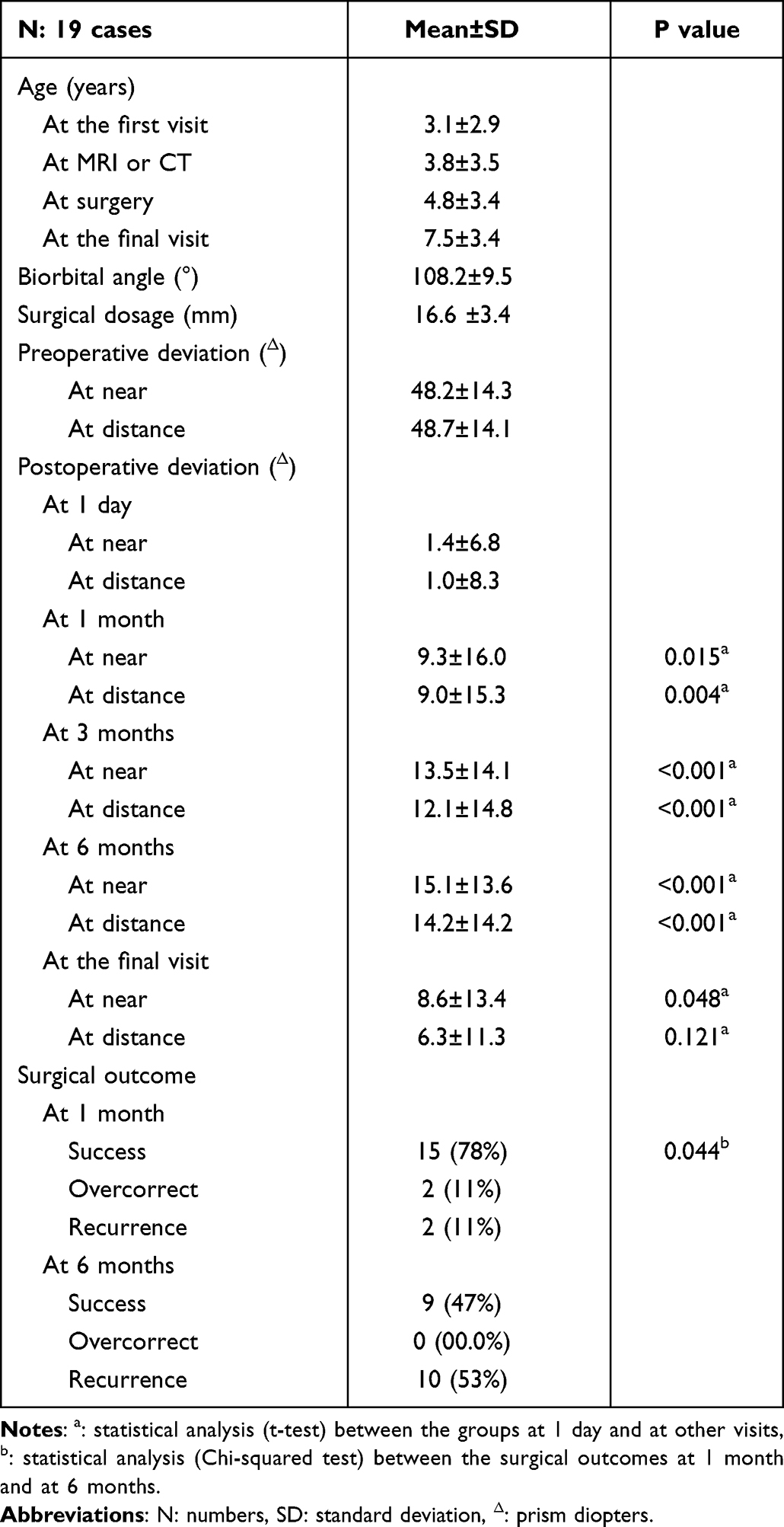 |
Table 1 Basic Characteristics and Postoperative Alignments of All Patients |
 |
Figure 1 Motor outcomes at distance (D) in the two groups undergoing the bilateral medial rectus resection procedure (BMRres; left) and other procedures (Others; right). |
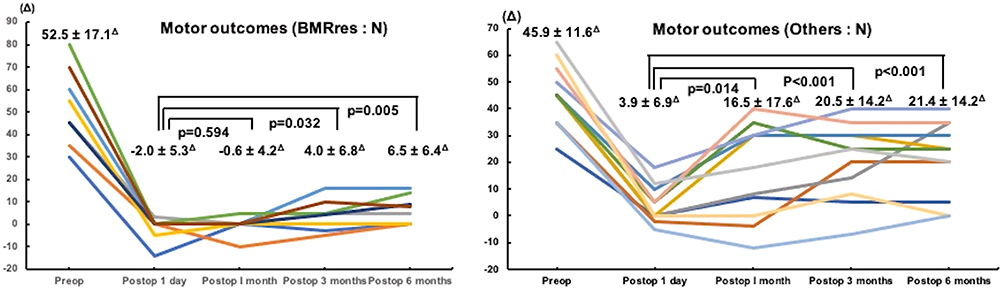 |
Figure 2 Motor outcomes at near (N) in the two groups undergoing the bilateral medial rectus resection procedure (BMRres; left) and other procedures (Others; right). |
At the initial visit, four patients were diagnosed with hyperopic ametropic amblyopia and one patient with hyperopic anisometropic amblyopia. With appropriate amblyopia treatment, all patients showed 20/20 or better best-corrected visual acuity.
Constant Exotropia and Intermittent Exotropia
Comparisons between CXT and IXT are shown in Table 2. There were no differences in baseline characteristics, except preoperative deviations and surgical dosage, between the CXT and IXT groups. There were significantly larger angles in the CXT group than in the IXT group (at distant, p=0.018; at near, p=0.014). Surgical types in the CXT group included 3 cases of BMEres, 3 cases of BMRres with ULRR, 4 cases of BLRR, and 2 cases of uniRandR with contralateral lateral rectus recession. In the IXT group, BMEres was performed for 2 cases, BLRR for 4 cases, and uniRandR for 1 case. The distribution of surgical types between groups was not significantly different (p=0.190). Although the mean surgical dosage was 16.6±3.4 mm in all patients, there was a significant difference found between the IXT and CXT groups (14.6±2.2 mm vs 17.8±3.5 mm, p=0.027).
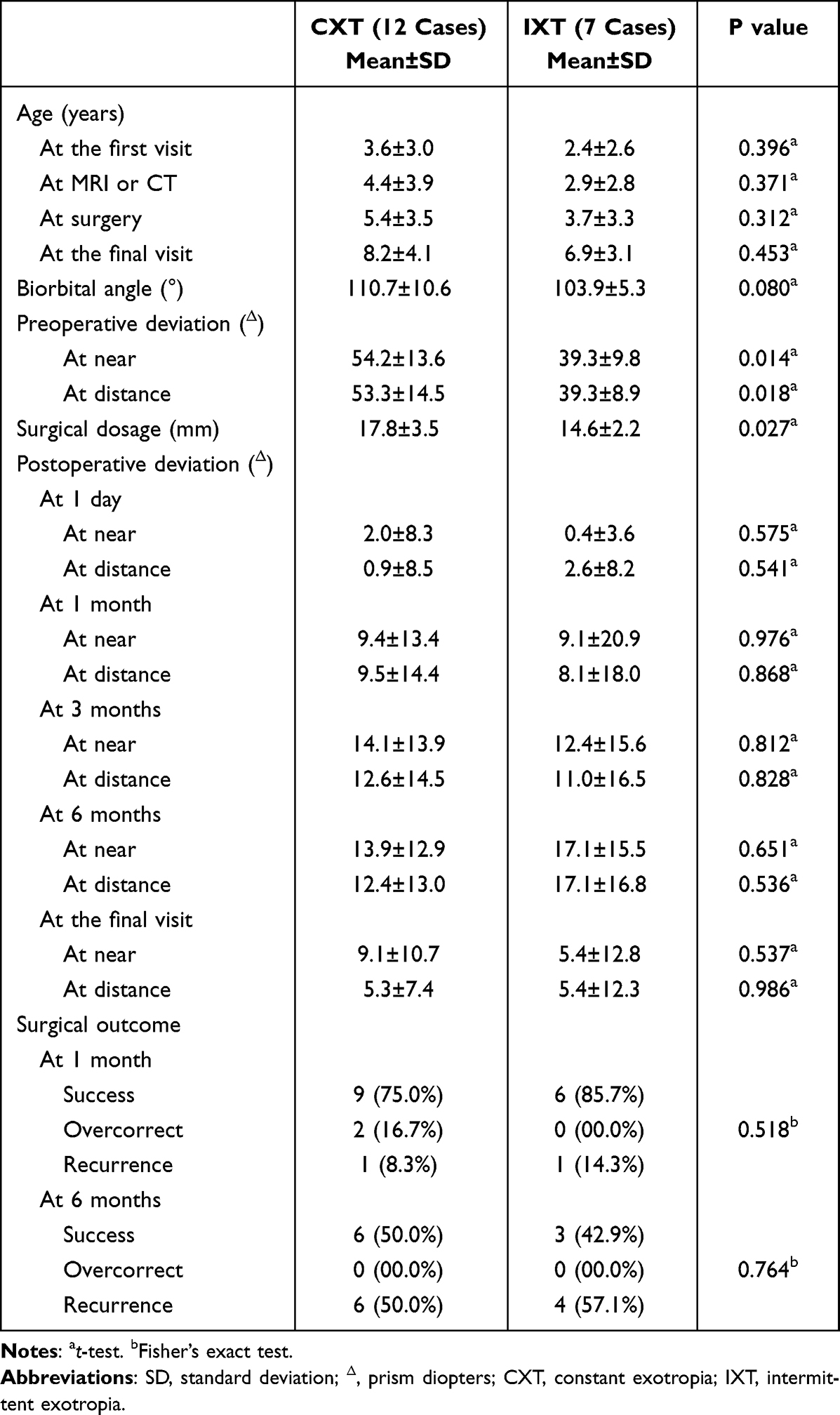 |
Table 2 Comparison of Basic Characteristics and Surgical Outcomes Between the Constant and Intermittent Infantile Exotropia Groups |
There was no significant difference in the mean age at the time of the surgical alignments in the CXT and IXT groups (5.4±3.5 years and 3.7±3.3 years, p=0.312). Although the mean surgical dosage was 16.6 ±3.4 mm in all patients, there was a significant difference between the IXT and CXT groups (14.6±2.2 mm and 17.8±3.5 mm, p=0.027). There were no significant differences in the postoperative alignment between the CXT and IXT groups.
Postoperative distant and near exodeviation angles in the CXT and IXT groups at 1 day and at 1, 3, and 6 months are shown in Table 2. There were no significant differences in postoperative alignment between the CXT and IXT groups within 6 months after surgery.
In the IXT group, there were no differences in the postoperative angles at distance and at near between the 1-day visit and other visits, with the exception at 6 months, while the postoperative exotropic angles of deviation at 6 months were significantly larger than those observed at 1 day (p=0.022 and 0.025, respectively; one-way ANOVA). In contrast, in the CXT group, the postoperative distant and near exotropic angles at 1, 3, and 6 months were significantly larger than those observed at 1 day (p<0.001 and <0.001, respectively; one-way ANOVA).
Successful surgical outcomes showed no significant differences between the two groups within 6 months after surgery. However, the distribution of success, overcorrection, and recurrence in the two groups deteriorated during the postoperative follow-up.
BMRres Procedure and Other Procedures
Comparisons between the BMRres procedure and the other procedures are presented in Table 3. There were no differences in the mean age at the first visit and at surgery between the BMRres group (8 cases) and the other group (11 cases). There were also no significant differences in the biorbital angle between the BMRres group and the other group (108.1±6.4° vs 103.8±4.5°, p=0.129). The mean exodeviation at near before surgery was 52.5±17.1Δ (range, 30–80Δ) in the BMRres group and 45.9±11.6Δ (range, 25–60Δ) in the other group, while at distance it was 50.1±18.8Δ (range, 30–80Δ) in the BMRres group and 46.4±10.5Δ (range, 30–65Δ) in the other group. There were no significant differences in exodeviation before surgery at distance and at near between these two groups.
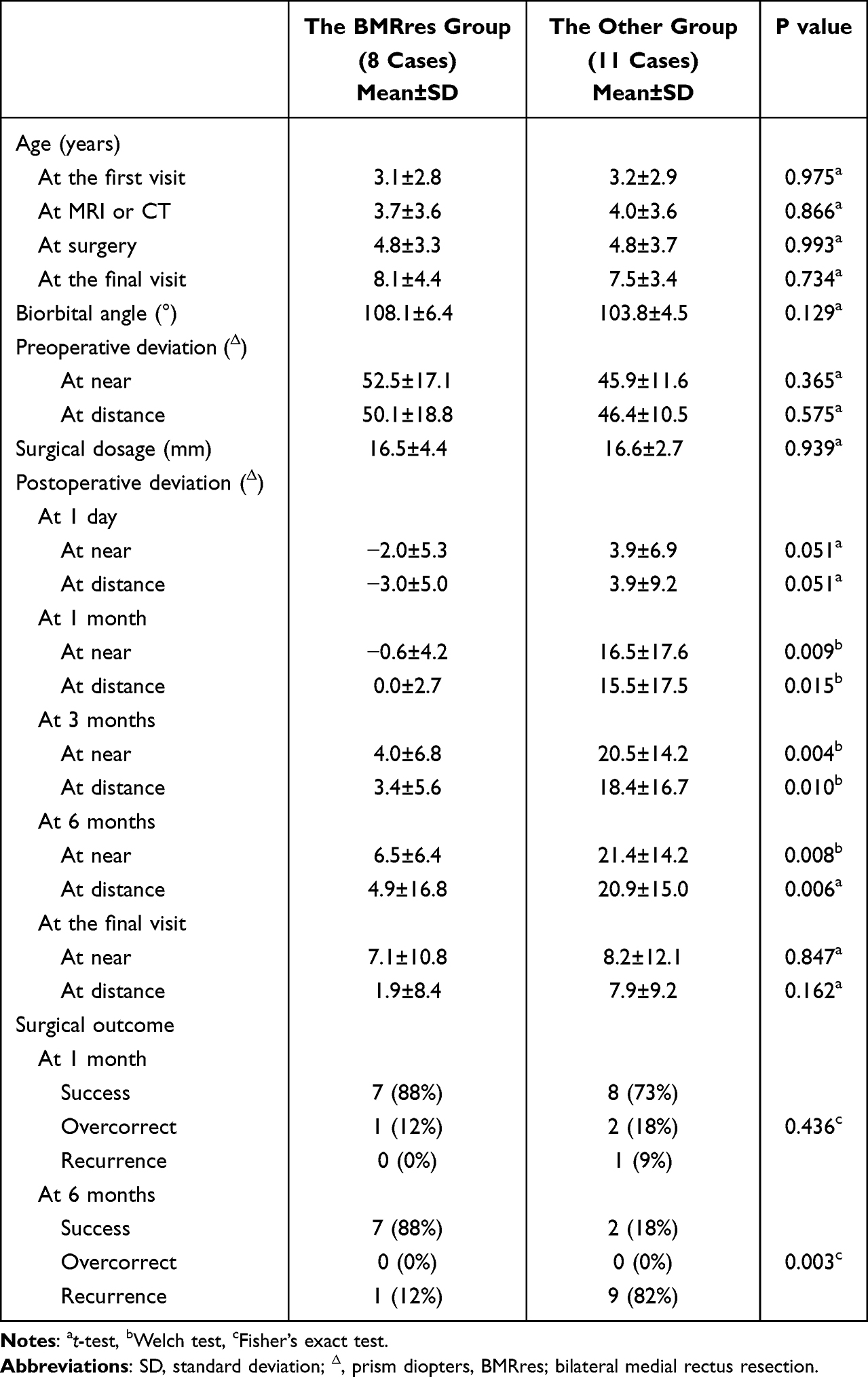 |
Table 3 Comparison of Basic Characteristics and Surgical Outcomes Between the Two Groups Undergoing the Bilateral Medial Rectus Resection Procedure and the Other Procedures |
The mean age at the time of surgical alignment was not significantly different between the BMRres group and the other group. There was also no significant difference in the mean surgical dosage between the two groups.
Postoperative distant and near exodeviation angles in the BMRres group and the other group at 1 day, and at 1, 3, and 6 months are shown in Figures 1 and 2. In the BMRres group, although no differences were found in postoperative distant and near angles between 1 day and 1 month, postoperative exotropic angles of deviation at 3 and 6 months were significantly larger than those observed at 1 day (p=0.004 and 0.032, p=0.002 and 0.005, respectively). Moreover, in the other group, the postoperative distant and near angles at 1, 3, and 6 months were significantly larger than those observed at 1 day (p=0.008 and p=0.014, p=0.002 and p<0.001, p<0.001 and p<0.001, respectively; one-way ANOVA) (Table 4).
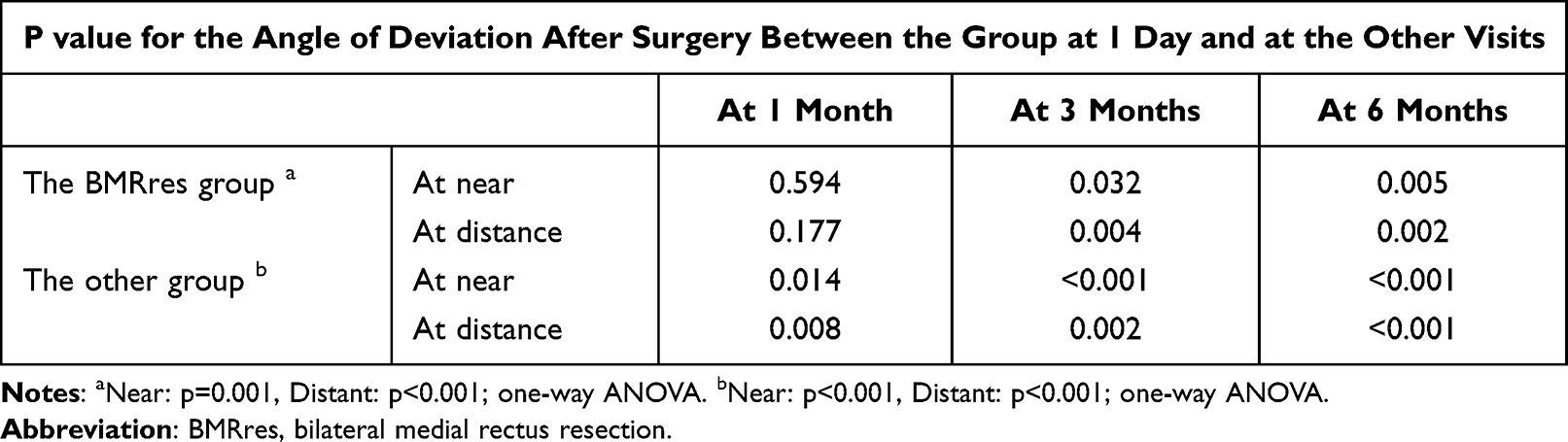 |
Table 4 P value for the Angle of Deviation After Surgery at 1 Day and at the Other Visits in the Two Groups Undergoing the Bilateral Medial Rectus Resection Procedure and the Other Procedures |
Although the postoperative distant and near exodeviation angles at 1 day in both groups were not significantly different, the postoperative distant and near exodeviation angles at 1, 3, and 6 months in the BMRres group were significantly smaller than those observed in the other group (at distance and at near; p=0.015 and p=0.009 at 1 month, p=0.010 and p=0.004 at 3 months, p=0.006 and p=0.008 at 6 months, respectively) (Table 3).
The successful surgical outcomes of the BMRres group and the other group were 88% and 73% at 1 day, 100% and 36% at 1 month, 88% and 27% at 3 months, and 88% and 18% at 6 months, respectively. Although there were no significant differences found in the distribution of success, overcorrection, and recurrence between the two groups within 3 months after surgery (at 1 month: p=0.435), the distribution of these in the BMRres group at 6 months after surgery was significantly better than that observed in the other group (p=0.003) (Table 3).
Reoperation
Although only 1 patient (13%) in the BMRres group required a second procedure to correct recurrence after the initial surgery, 8 patients (73%) in the other group underwent significantly more surgeries (p=0.020). The details of the additional surgeries included bilateral medial rectus resection in 4 cases and unilateral medial rectus resection in 4 cases of the other group, and unilateral lateral rectus recession in 1 case of the BMRres group. The mean age at the additional surgical alignments was 5.6±1.5 years.
The mean age at the final visit was 7.5±3.4 years. The mean final exodeviations were 6.3±11.3Δ at distance and 8.6±13.4Δ at near. Although the mean final exodeviation at near was significantly larger than that observed 1 day after the initial surgery (p=0.048), there were no significant differences found in the postoperative alignment at distance between 1 day and the final visit (p=0.121). There were also no significant differences in the distribution of success, overcorrection, or recurrence between 1 day after the initial surgery and the final visit (p=0.446).
Discussion
Most long-term outcomes for infantile exotropia after ocular alignment surgery are disappointing.2–8 Biglan et al reported that reoperations were required in 4 (40%) of 10 patients who underwent initial surgery for infantile exotropia.3 Hunter et al also reported a 67% success rate for the initial surgery in 12 cases of infantile exotropia.4 The success rates of initial surgery for infantile exotropia in other reports ranged from 41% to 67%.12,13
Furthermore, the recurrence of infantile exotropia generally appears immediately after the initial surgery. Biglan et al reported that 4 patients exhibited recurrence of exodeviation within the first few months after their initial surgery,3 and that if the surgical alignment was found to be satisfactory at 1 and 6 weeks after the surgery, there was less chance that any additional surgery would be required.4 Park and Kim examined 20 patients with infantile exotropia and reported the clinical features and risk factors for infantile exotropia recurrence.17 The authors divided these patients into two groups: those who underwent successful BLRR and those in the recurrence group that exhibited exodeviation at 1 year after surgery. They found that there was no significant difference in the postoperative deviations between the two groups 1 day after surgery. However, at 1 month after the surgery, the recurrence of exotropia was already present, and by 3 months after the surgery, significant postoperative deviations were observed between the two groups. This difference was still present 12 months after surgery. The authors then investigated the differences in clinical features between these two groups in an attempt to identify factors that could affect surgical outcomes. They concluded that there was no significant association with the recurrence of infantile exotropia after surgery, despite their finding of ideal initial overcorrection during the immediate postoperative period. Suh et al also evaluated the clinical characteristics and surgical outcomes of 45 patients with infantile exotropia to compare differences between CXT and IXT.13 The results indicated that there were no significant differences in surgical success rates or binocularities between CXT and IXT. Hunter et al also reported similar clinical outcomes after surgical intervention between patients with CXT and IXT.4 Taken together with our results, these findings demonstrate that the phase of infantile exotropia (constant or intermittent) has no influence on surgical effects in infantile exotropia.
Although the characteristics of this disease have been investigated in detail, its pathology remains unclear.1 Several small-scale studies have attempted to analyze the parameters required to achieve successful surgery for infantile exotropia.1,19 While a single factor has yet to be determined that can affect the surgical outcome in infantile exotropia, recurrence is very apparent starting from the first postoperative month.20 Therefore, further investigations focusing on the pathogenic factors of infantile exotropia need to be carried out.
In our previous study,9 we demonstrated for the first time that there is a larger biorbital angle between the lateral walls of the orbit in patients with infantile exotropia. However, the relationship between the configuration of the orbit and the presence of strabismus has yet to be definitively established. Rates of strabismus in craniosynostosis have been shown to range from 39% to 91%, with exotropia being the most common type of strabismus reported in Crouzon and Apert syndrome.21 Morax reported changes in the eye position from exotropic to orthophoric in 8 of 9 patients with Crouzon syndrome after sagittal expansion of the orbit.22 In Crouzon syndrome, there is a significant increase in both the inner and outer interorbital distances compared with normal subjects.23 These findings suggest that there may be the creation of a large biorbital angle. Successful craniosynostosis treatments include sagittal expansion of the orbit (such as fronto-orbital advancement), Le Fort III advancement, or monobloc advancement (which can decrease the biorbital angle). Based on these previous treatments and findings, our results clearly show a relationship between the decrease in the biorbital angle and orthophoric changes in ocular alignment. In Apert syndrome, the same ocular alignment findings have been reported in exotropic-to-esotropic patients after craniofacial surgery.24,25 These previous reports seem to suggest that the greater the increase in the biorbital angle, the more frequent the existence of exotropia due to the extraocular muscles being in contact with the orbital bone by a pulley system.
The question that remains to be answered is whether the larger opening angle of the orbit is a major factor in the pathogenesis of infantile exotropia, and why immediate recurrence after surgery is frequently seen. Moreover, it is unknown as to which procedure would be the most effective for correcting infantile exotropia. We speculate that the principle of surgical correction of infantile exotropia is similar to that involved in raising the upper body on a reclining seat. To achieve this positional change, the abdominal muscles, and not the back muscles, are used to generate the force needed to complete this action. Thus, strengthening the abdominal muscles makes it easier for an individual to raise their upper body. Likewise, weakening of the lateral rectus muscle can not generate enough adductor power to raise the reclined globe, because the lateral rectus muscle is in contact with the wider open lateral orbital bone by a pulley system. This speculation might be confirmed by the disappointing results reported for the correction of exodeviation in infantile exotropia after performing BLRR or uniRandR.1–7,11–16 In our current study, the successful surgical outcomes of the BMRres and other groups were not significantly different within 3 months after surgery. Furthermore, the distributions of success, overcorrection, and recurrence in the BMRres group at 6 months after surgery was significantly better than those in the other group. Although there was no difference in the opening angle of the orbit between patients who did and did not undergo BMRres, we found that there was a better outcome in patients undergoing BMRres. In previous reports, the main surgical procedure for infantile exotropia was BLRR.1–7,11,12 In addition, only two reports have detailed the use of uniRandR as the first surgical procedure for infantile exotropia.13,16 According to one of these reports by Rajavi et al, uniRandR exhibited significantly better outcomes than BLRR.16 However, the authors classified the success or failure of their 82 cases based on an angle of deviation of 10Δ or less at only 3 months after the first surgery. Therefore, recommendations as to whether uniRandR should be the primary procedure will remain unclear until further postoperative outcome results after 3 months become available.
In general, BMRres is indicated for exotropia with convergence insufficiency.17,18 All cases in this report involved basic exotropia, in which BMRres is not considered to be indicated according to our principles. Despite this, our results revealed that there were no undesirable outcomes noted in any of the patients who underwent BMRres, suggesting that BMRres might be beneficial as an initial intervention when treating infantile exotropia, as reported by Farias et al.19
The biggest limitation of our study was the small number of recruited patients that were examined. Because the incidence of infantile exotropia is only 0.003% of births in the general population,1 this makes it difficult to recruit a large number of patients with infantile exotropia. However, since MRI or CT examinations can be used to detect a larger opening angle of the orbit in patients with infantile exotropia, the use of these procedures may help determine the surgical procedure that needs to be performed in order to correct exodeviation with less recurrence of exotropia.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Funding
The authors declare no funding sources, including financial support, for the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kraft SP. Infantile exotropia. In: Rosenbaum AL, Santiago AP, editors. Clinical Strabismus Management: Principles and Surgical Techniques. Philadelphia: WB Saunders; 1993:176–181.
2. Rubin SE, Nelson LB, Wagner RS, Simon JW, Catalano RA. Infantile exotropia in healthy children. Ophthalmic Surg. 1988;19:792–794. doi:10.3928/0090-4481-19881101-07
3. Biglan AW, Davis JS, Cheng KP, Pettapiece MC. Infantile exotropia. J Pediatric Ophthalmol Strabismus. 1996;33(2):79–84. doi:10.3928/0191-3913-19960301-04
4. Hunter DG, Kelly JB, Buffenn AN, Ellis FJ. Long-term outcome of uncomplicated infantile exotropia. J AAPOS. 2001;5(6):352–356. doi:10.1067/mpa.2001.120175
5. Paik HJ, Yim HB. Clinical effect of early surgery in infantile exotropia. Korean J Ophthalmol. 2002;16(2):97–102. doi:10.3341/kjo.2002.16.2.97
6. Na KH, Kim SH. Early versus late surgery for infantile exotropia. J AAPOS. 2018;22:3–6. doi:10.1016/j.jaapos.2017.08.006
7. Lee HW, Park SE, Oh SY. The clinical feature and surgical outcome of infantile exotropia. J Korean Ophthalmol Soc. 2004;45:1899–1905.KMID: 2337177
8. Hiles DA, Biglan AW. Early surgery of infantile exotropia. Trans Pa Acad Ophthalmol Otolaryngol. 1983;36:161–168. PMID: 6659036
9. Tsukui M, Yagasaki Y, Yokoyama Y. Abnormal biorbital angle in children with infantile exotropia. Jpn J Ophthalmol. 2022;66:81–86. doi:10.1007/s10384-021-00881-1
10. Yagasaki T, Yokoyama Y, Tsukui M. Developmental change of the biorbital angle in normal Japanese infants. Clin Ophthalmol. 2018;12:2047–2051. doi:10.2147/OPTH.S180306
11. Yam JC, Chong GS, Wu PK, Wong US, Chan CW, Ko ST. Preoperative factors predicting the surgical response of bilateral lateral rectus recession surgery in patients with infantile exotropia. J Pediatr Ophthalmol Strabismus. 2013;50:245–250. doi:10.3928/01913913-20130507-01
12. Yam JC, Chong GS, Wu PK, et al. Long-term ocular alignment after bilateral lateral rectus recession in children with infantile and intermittent exotropia. J AAPOS. 2012;16:274–279. doi:10.1016/j.jaapos.2012.01.005
13. Suh SY, Kim MJ, Choi J, Kim SJ. Outcomes of surgery in children with early-onset exotropia. Eye. 2013;27:836–840. doi:10.1038/eye.2013.75
14. Bagheri M, Farvardin M. The clinical effect of surgical timing in infantile exotropia. J AAPOS. 2018;22(3):167–169. doi:10.1016/j.jaapos.2017.12.004
15. Rajavi Z, Sabbaghi H, Behradfar N, et al. Motor and sensory outcomes of infantile exotropia: a 10-year study (2008–2017). Korean J Ophthalmol. 2020;34:143–149. doi:10.3341/kjo.2019.0090
16. Rajavi Z, Lashgari A, Sabbaghi H, Behradfar N, Yaseri M. The Incidence of Reoperation and related risk factors among patients with infantile exotropia. J Pediatr Ophthalmol Strabismus. 2017;54(1):22–30. doi:10.3928/01913913-20160926-02
17. von Noorden GK. Resection of both medial rectus muscles in organic convergence insufficiency. Am J Ophthalmol. 1976;81(2):223–226. doi:10.1016/0002-9394(76)90735-2
18. Hermann JS. Surgical therapy of convergence insufficiency. J Pediatr Ophthalmol Strabismus. 1981;18:28–31. doi:10.3928/0191-3913-19810101-08
19. Farias LB, Barham R, Costa AL, Wang S, Weakley JDR. Dose-response of primary bilateral medial rectus resection in infantile exotropia. J Pediatr Ophthalmol Strabismus. 2022;59(1):24–27. doi:10.3928/01913913-20210706-02
20. Park JH, Kim SH. Clinical features and the risk factors of infantile exotropia recurrence. Am J Ophthalmol. 2010;150:464–467. doi:10.1016/j.ajo.2010.05.004
21. Rosenberg JB, Tepper OM, Medow NB. Strabismus in craniosynostosis. J Pediatr Ophthalmol Strabismus. 2013;50(3):140–148. doi:10.3928/01913913-20121113-02
22. Morax S. Change in eye position after cranio-facial surgery. J Maxillofac Surg. 1984;12:47–55. doi:10.1016/S0301-0503(84)80211-8
23. Kreiborg S, Cohen MM
24. Khong JJ, Anderson P, Gray TL, Hammerton M, Selva D, David D. Ophthalmic findings in Apert syndrome prior to craniofacial surgery. Am J Ophthalmol. 2006;142(2):328–330. doi:10.1016/j.ajo.2006.02.046
25. Khong JJ, Anderson P, Gray TL, Hammerton M, Selva D, David D. Ophthalmic findings in Apert’s syndrome after craniofacial surgery: twenty-nine years’ experience. Ophthalmology. 2006;113:347–352. doi:10.1016/j.ophtha.2005.10.011
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.