Back to Journals » Clinical Interventions in Aging » Volume 15
Effects of Arch Support Insoles on Single- and Dual-Task Gait Performance Among Community-Dwelling Older Adults
Authors Peng HT, Lin CH, Kuo YC, Song CY ![]()
Received 18 March 2020
Accepted for publication 12 July 2020
Published 10 August 2020 Volume 2020:15 Pages 1325—1332
DOI https://doi.org/10.2147/CIA.S254474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Hsien-Te Peng,1 Chueh-Ho Lin,2,3 Yu-Chi Kuo,4 Chen-Yi Song5
1Department of Physical Education, Chinese Culture University, Taipei, Taiwan; 2Master Program in Long-Term Care, College of Nursing, Taipei Medical University, Taipei, Taiwan; 3Center for Nursing and Healthcare Research in Clinical Practice Application, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 4Department of Exercise and Health Science, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan; 5Department of Long-Term Care, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan
Correspondence: Chen-Yi Song
Department of Long-Term Care, National Taipei University of Nursing and Health Sciences, 365 Ming-Te Road, Taipei 11219, Taiwan
Tel +886 2 28227101 Ext 6136
Fax +886 2 23891464
Email [email protected]
Purpose: To explore the immediate and prolonged effects of arch support insoles on single- and dual-task gait performance among community-dwelling older adults.
Methods: Twenty women performed single- and dual-task walking for 10 m at self-selected comfortable and fast paces while performing serial subtractions (cognitive interference) or carrying a tray (motor interference). Spatiotemporal gait parameters were measured and compared with measurements without arch support immediately after the insertion of the insoles and at 1-week follow-up.
Results: Some effects were noted, with small-to-medium effect sizes. During comfortable-paced single-task walking, stride length and walk ratio (step length/cadence) increased after arch support use. During comfortable-paced motor dual-task walking, arch support use increased cadence, stride length, and speed and decreased dual-task costs (DTCs) on cadence and speed. During fast-paced motor dual-task walking, cadence increased and the DTC on cadence decreased after arch support use at the 1-week follow-up. During comfortable-paced cognitive dual-task walking, cadence increased and the walk ratio decreased following arch support use. At the 1-week follow-up, DTCs on cadence reduced, but those on stride length and speed increased. During fast-paced cognitive dual-task walking, the speed and stride length demonstrated immediate decreases followed by increases at the 1-week follow-up.
Conclusion: The study results indicate that the use of arch support improves single- and motor dual-task gait performance, which may contribute to gait and balance training in older adults.
Keywords: gait, dual-task, insole, elderly
Introduction
Gait and balance deficits are among the most common risk factors for falls among older adults.1 Approximately 32–35% of community-dwelling older adults have impaired gait.2,3 Age-related gait changes include decreased step length, increased double-support stance time, and decreased gait speed,4,5 with maximum gait speed declining more steeply than comfortable gait speed.4 A study reported that older adults who experience falls have lower gait speed, lower cadence, shorter step and stride length, and longer double-support stance time during comfortable walking than those who do not experience falls; in addition, older fallers’ gait speed, cadence, and stride length are lower during fast-paced walking.6
Walking involves several cognitive domains, including executive/attentional function, visuospatial ability, and memory resources;7 therefore, the gait performance of older adults is affected by the addition of a dual task. Reduced gait velocity has been reported among older adults performing concurrent functional motor tasks, including carrying an object.8 Studies have also demonstrated the negative effect of cognitive dual-task performance on gait speed, cadence, and stride length.9,10 Assessment of walking under attention-demanding, dual-task conditions improves the detection of walking disorders.11 Gait deterioration during cognitive and/or motor dual tasks is significantly associated with an increase in the risk of falling among older adults.12,13 By contrast, studies have reported that single- and dual-task tests measuring simple gait speed have equivalent accuracy in the prediction of falls among older adults.14 Nevertheless, dual-task gait paradigms might be of value because such multitasking abilities are required in many real-life situations, and the results of the paradigms may assist in guiding interventions.14
Footwear, insoles, and orthoses are gaining popularity as integral components of fall-prevention strategies.15 Shoe insoles enhance balance control and gait, possibly preventing falls among older adults through sensorimotor and mechanical mechanisms.16,17 Arch support insoles may enhance somatosensory stimulation by increasing the base of support and stimulating the plantar aspect of the foot over a larger contact area, thereby providing greater sensory input that can be used to make adjustments for changes in the center of pressure perceived through the plantar aspect of the foot.18 In addition, arch support insoles can optimize kinematics, including foot and lower-limb alignment, thus providing mechanical stability.16 Therefore, it is likely that the insole use has positive mechanical and sensory influences on walking performance.
Although various insoles have been used in previous studies, evidence for the effect of arch support insoles on balance and gait in the elderly population is lacking. Chen et al17 designed a heel cup with an arch support insole for healthy older adults but investigated its effectiveness only for improving balance while standing. Mulford et al19 demonstrated the ability of arch support to improve both balance (Berg Balance Scale) and functional mobility (timed up and go test) in older adults; however, its effect on gait was unclear. Gross et al18 investigated the effects of semirigid custom foot orthoses on dynamic balance during a tandem gait test in older fallers; however, tandem walking is less functionally relevant because it does not emulate real-life mobility. Understanding how arch support influences gait is critical because falls among community-dwelling elderly people occur most frequently while walking.20 Furthermore, elderly people’s balance control during walking is perturbed when changing walking speeds from preferred speeds to fast speeds21 and from single to dual tasks.9,10 Arch support insoles may benefit all these types of gait. Once the effects of insole interventions on dual-task gait are determined, such interventions may be applied as treatment strategies or in conjunction with exercise interventions to improve balance and gait in older adults.22
The purpose of the current study was to investigate the immediate and prolonged effects of arch support insoles on single- and dual-task gait performance among community-dwelling older adults. Both comfortable and fast walking speeds were evaluated. We hypothesized that arch support insoles improve single- and dual-task walking performance at both comfortable and fast speeds.
Materials and Methods
Participants
Twenty female older adults were recruited from a local senior center in New Taipei City. Only women were recruited in the present study because female older adults tend to have a higher risk of falling and fall incidence rate.23,24 Other inclusion criteria were community-dwelling adults aged ≥65 years capable of independent ambulation without any assistive devices. Participants who had severe lower-extremity joint pain or deformity, cognitive impairment (defined as a Montreal Cognitive Assessment score of <26),25 or a self-reported history of falls in the preceding year were excluded. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board of the Antai-Tian-Sheng Memorial Hospital. All participants provided signed informed consent prior to participating in this study.
Procedure
Gait performance was measured under three conditions in a random order based on a random number table: (1) walking (single task); (2) walking while verbally counting backward in decrements of three from a random number between 90 and 100 (cognitive dual-task walking); and (3) walking while carrying a tray (size: 38 × 28 × 5 cm3) that was 80% full of water (motor dual-task walking). In line with a previous study,26 our dual-task walking testing protocol comprised cognitive and motor dual-tasks because in their daily life, people tend to combine walking and executing a cognitive or motor task.
The primary task was a 10-m walk, and the secondary task was executing serial subtractions or carrying a tray while keeping it as steady as possible. The participants were randomly asked to walk at a self-selected comfortable or fast pace for each of the three testing conditions. A researcher walked alongside the participants to ensure their safety. Each test condition was performed twice with 1-min intervals, and the results were averaged for further statistical analysis. If a participant stopped walking or stopped performing the cognitive task, the trial was repeated. Gait performance assessments were conducted randomly with or without an insole, and an additional 5-min rest interval was provided to prevent fatigue. The participants were then asked to wear the insoles for at least 6-h every day for 1 week, and follow-up gait assessment (with insole) was conducted after 1 week of habitual wear.
Gait Assessment
The inertial measurement unit–based shoe-worn GAIT Up system (Gait Up, Lausanne, Switzerland) was used to evaluate spatiotemporal gait performance. The system is lightweight (weight, 36 g; dimensions, 50 × 40 × 16 mm3), easy to wear and use, and suitable for clinical application in situations requiring the objective evaluation of gait among older adults outside a laboratory environment.27,28
In the current study, the spatiotemporal parameters of gait recorded during each trial included gait speed (m/s), stride length (m), and cadence (step/s). Test–retest reliability was good (intraclass correlation coefficient [ICC] = 0.82–0.98).
To quantify the interference of performing a dual task on gait, dual-task costs (DTCs) of walking are expressed as percentage of loss relative to single-task walking performance according to the following formula:29
DTC (%) = 100 × (single-task gait parameter − dual-task gait parameter)/single-task gait parameter.
In addition, the walk ratio (mm/step/min), which is a good representation of the gait pattern among older people,30 was used to explore the strategies adopted to adjust cadence or stride length with arch support use. In this study, the walk ratio was calculated using the corrected step length and the corrected cadence, where30
Corrected step length = (stride length/2) × (height/mean height of all participants)−1
Corrected cadence = cadence × (height/mean height of all participants)−0.5
Intervention
The FootDisc insole (Global Action Inc., Taipei, Taiwan) with the patented dynamic technology of arch cradle support was used (Figure 1). The insole was designed with curEVA for shock absorption and motion reduction, poron for secondary heel and metatarsal protection, and dynamic arch support for returning energy for propulsion.
 |
Figure 1 The arch support insole used in the present study. |
Data Analysis
Statistical analyses were performed using SPSS version 23.0 (IBM, Armonk, NY, USA). Descriptive statistics were used to evaluate the participants’ gait performance, and all variables are expressed as mean ± standard deviation. One-way repeated-measures analysis of variance was used to determine the effects of arch support on the gait variables of interest. The P value was adjusted (0.008) for multiple comparisons. In addition, effect sizes (Cohen’s d) were calculated and classified as small (d = 0.2), medium (d = 0.5), and large (d = 0.8).31
Results
The mean age of the participants was 77.1 ± 5.1 years, mean height was 153.0 ± 5.0 cm, and mean weight was 59.6 ± 9.6 kg. Figure 2 shows single-task and dual-task walking gait performance with and without arch support insoles. DTCs on walking and the walk ratios are summarized in Tables 1 and 2, respectively.
 |
Figure 2 Single-task and dual-task gait performance with and without arch support. |
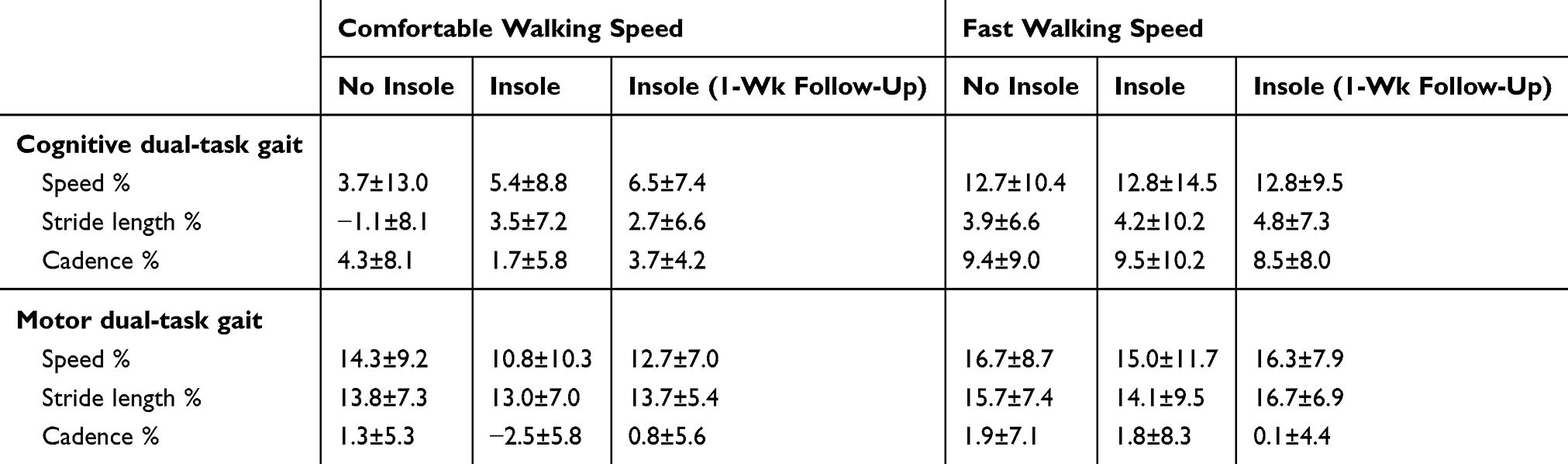 |
Table 1 Dual-Task Costs on Various Gait Parameters with and without Arch Support |
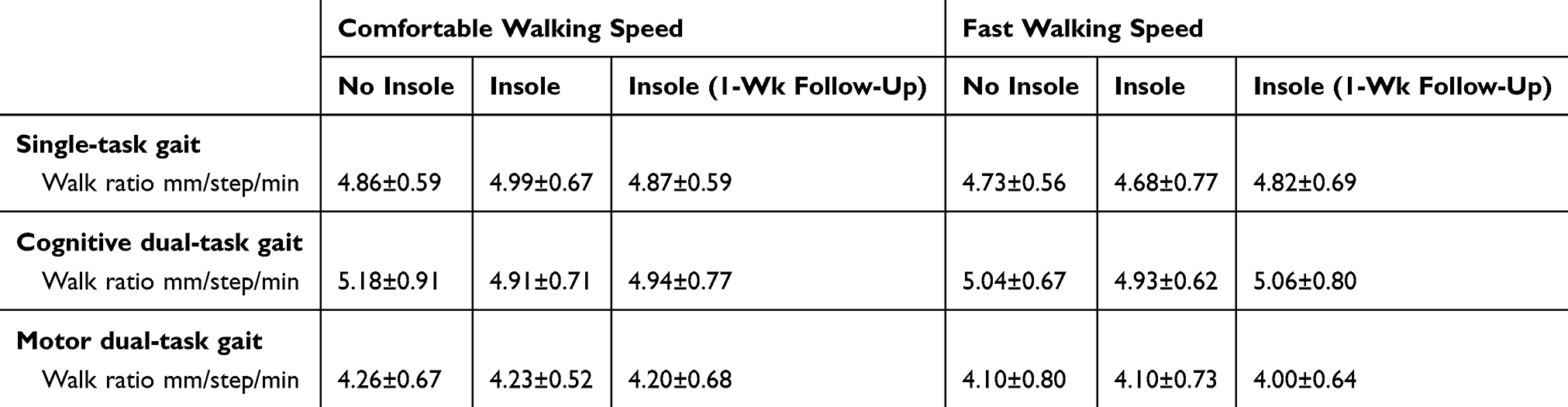 |
Table 2 Single-Task and Dual-Task Walk Ratios with and without Arch Support |
Single-Task Gait
At a comfortable pace, arch support immediately increased the stride length (d = 0.21, Figure 2) and walk ratio (d = 0.21, Table 2). At a fast pace, no significant difference was noted in stride length (P = 0.074) before and after adopting arch support; however, stride length increased at the 1-week follow-up compared with the measurements taken immediately after insertion of the insoles (d = 0.24, Figure 2). No significant differences were observed in the walk ratios before and after adopting arch support.
Cognitive Dual-Task Gait
At a comfortable speed, the immediate effects of arch support were evident in cadence (d = 0.22, Figure 2); the DTC on cadence (d = 0.37) decreased, but that on stride length increased (d = 0.60, Table 1). At the 1-week follow-up, the stride length decreased (d = 0.28), whereas DTCs on stride length (d = 0.51) and speed (d = 0.26) increased (Table 1). A difference in the walk ratio was observed (P = 0.040). Pairwise comparison revealed a decrease in the walk ratio both immediately after the insertion of the insoles (P = 0.037, d = 0.33) and at the 1-week follow-up (P = 0.026, d = 0.29, Table 2).
At a fast pace, speed (d = 0.28) and stride length (d = 0.22) immediately decreased after adopting arch support but increased (d = 0.46 and 0.36, respectively) at the 1-week follow-up (Figure 2). Furthermore, cadence increased at the 1-week follow-up compared with that immediately after insole insertion (d = 0.22). No significant differences were observed in walk ratios before and after adopting arch support.
Motor Dual-Task Gait
At a comfortable speed, the immediate effects of arch support were evident in cadence (P = 0.014; d = 0.47), speed (d = 0.32), and stride length (d = 0.21, Figure 2); DTCs on cadence (d = 0.68) and speed (d = 0.36) decreased (Table 1). At the 1-week follow-up, the sustained effects of arch support were evidenced by increases in both cadence (d = 0.24) and speed (d = 0.20).
At a fast pace, adopting arch support increased cadence (d = 0.26) and reduced the DTC on cadence (d = 0.30) at the 1-week follow-up. No significant differences were observed in walk ratios before and after adopting arch support.
Discussion
This study investigated the immediate and prolonged effects of arch support insoles on single- and dual-task gait performance among community-dwelling older adults. Our results indicate that arch support improves single-task gait by increasing the stride length and walk ratio. Older adults who experience falls have higher cadence and smaller steps.32 The risk of multiple falls is increased in those with smaller walk ratios (shorter steps and higher cadence).33 Furthermore, those with a gait speed of ≥1.0 m/s and a smaller walk ratio had higher fall rates and risk of falling.30 The findings of the present study corroborate the notion that footwear interventions can enhance balance control and gait in older adults.16,17
Arch support insoles may exert beneficial effects on walking in older adults by improving postural stability. Chen et al17 reported that the use of a heel cup with an arch support insole effectively enhanced the standing balance of healthy older adults. Qu34 compared four commercially available insoles and found that cupped insoles improved older adults’ dynamic postural stability, as measured using the anterior-posterior margin of stability during treadmill walking at a self-selected comfortable speed. Postural stability can also be affected by insole material hardness. Iglesias et al35 suggested that compared with softer insoles, more rigid insoles are more likely to place the foot in a more neutral position, leading to greater postural stability.
To the best of our knowledge, the present study is the first to examine the effect of arch support insoles on dual-task gait performance among community-dwelling older adults. The effects of insoles differed between motor and cognitive dual-task gait performance. During motor dual-task walking at a comfortable speed, arch support use led to increases in cadence, stride length, and speed, whereas during cognitive dual-task walking, arch support use led to increased cadence and a decreased walk ratio. During fast-paced motor dual-task walking, arch support use increased cadence at the 1-week follow-up, whereas during cognitive dual-task walking, gait speed and stride length decreased immediately after adopting arch support but increased at the 1-week follow-up.
The addition of a motor or cognitive task to the task of walking (dual task) reduces gait speed, stride length, and cadence.8–10 Older adults adapt their gait for increased safety and stability. Generally, arch support use demonstrated benefits in mitigating the deterioration of motor dual-task gait performance. However, the immediate effect of arch support use on cadence and the walk ratio during comfortable-paced cognitive dual-task walking should be assessed because the gait pattern of short steps with high cadence may increase the likelihood of tripping and falling.30,36 Gait deterioration following arch support use during fast-paced cognitive dual-task walking was indicated by decreased gait speed and stride length in older adults. Decreased gait velocity can be a strategy for maintaining balance when walking under challenging circumstances.37 By contrast, Huijben et al38 indicated that a lower walking speed results in lower gait quality among older adults. Fan et al39 also demonstrated a decrease in lateral variability with an increase in walking speed. Taken together, these results suggest that the interference of secondary cognitive challenges and walking speed on gait performance should be considered when prescribing arch support insoles for gait and balance training in older adults.
In this study, we used DTCs to quantify the dual-task interference (ie, the relative change in gait performance associated with performing a dual task) and to elucidate the effects of arch support. A study revealed that the difficulty level associated with walking while carrying a glass of water on a tray with one hand (a manual motor task) was the same as that associated with walking with the usual gait at a preferred walking speed in cognitively healthy adults.40 Because gait velocity decrements during a dual task are related to the difficulty of the task,40 we used a more challenging motor dual task (ie, carrying a tray of water with two hands); as expected, a decrease in gait speed was observed. With arch support, DTCs on both cadence and speed decreased, indicating a decrease in the percentage of loss in motor dual-task performance relative to single-task walking performance. We speculate that arch support improved dynamic balance during standing and walking in older people through a combination of sensorimotor and mechanical mechanisms,16–19 thereby reducing DTCs. During cognitive dual-task walking, the DTC on cadence decreased, but DTCs on stride length and speed increased following arch support use. This may be attributed to the high level of difficulty and high cognitive cost associated with walking while performing serial subtractions compared with those associated with walking while carrying a glass of water among cognitively healthy adults.37 Multicomponent exercise and combined physical–cognitive training can positively affect gait performance,41,42 and incorporating arch support insoles into such interventions for longer durations may have some additional benefit on cognitive dual-task gait performance.
The single-task gait and dual-task gait in this study were measured both immediately after wearing the insole and at the 1-week follow-up to explore the effects of immediate and habitual wear of arch support insoles. Sustained effects of arch support on increasing cadence and speed were found during comfortable-paced motor dual-task walking. Additionally, the insoles’ effects were more evident after a habitual wear period under the more complicated condition of the fast-paced dual-task. Similarly, the stride length during single-task fast-paced walking increased at the 1-week follow-up compared with that immediately after insole insertion. Thus, future studies should investigate the long-term effects of the arch support intervention (eg, 4–12 weeks) on gait performance.
This study has some limitations. First, our participants comprised only cognitively healthy female older adults; hence, the results may not be generalizable to men. Future investigations involving older adults with mild cognitive impairment and more pronounced gait dysfunction43 are warranted. Second, only a few gait parameters were measured in this study. Comprehensive gait assessment, including gait variability and stride time, may detect gait improvement following the application of arch support insoles. Third, we did not measure the number of errors during the cognitive dual task and the amount of water remaining inside the tray during the motor dual task; thus, whether arch support insoles lead to better dual-task performance requires further investigation. Finally, prospective studies are required to determine whether arch support reduces the incidence of falls in older adults.
Conclusions
The study results indicate that the use of arch support improves single- and motor dual-task gait performance, which may contribute to gait and balance training in older adults.
Acknowledgment
The authors thank Global Action Inc., Taipei, Taiwan, for sponsoring the arch support insoles used in this study.
Disclosure
The authors report no conflicts of interest associated with this work.
References
1. Guideline for the prevention of falls in older persons. Guideline for the prevention of falls in older persons. American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on falls prevention. J Am Geriatr Soc. 2001;49(5):664–672.
2. Mahlknecht P, Kiechl S, Bloem BR, et al. Prevalence and burden of gait disorders in elderly men and women aged 60–97 years: a population-based study. PLoS One. 2013;8:e69627. doi:10.1371/journal.pone.0069627
3. Verghese J, LeValley A, Hall CB, et al. Epidemiology of gait disorders in community-residing older adults. J Am Geriatr Soc. 2006;54:255–261. doi:10.1111/j.1532-5415.2005.00580.x
4. Bohannon R. Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants. Age Ageing. 1997;26:15–19. doi:10.1093/ageing/26.1.15
5. Winter DA, Patla AE, Frank JS, et al. Biomechanical walking pattern changes in the fit and healthy elderly. Phys Ther. 1990;70:340–347. doi:10.1093/ptj/70.6.340
6. Newstead AH, Walden JG, Gitter AJ. Gait variables differentiating fallers from nonfallers. J Geriatr Phys Ther. 2007;30:93–101. doi:10.1519/00139143-200712000-00003
7. Amboni M, Barone P, Hausdorff JM. Cognitive contributions to gait and falls: evidence and implications. Mov Disord. 2013;28(11):1520–1533. doi:10.1002/mds.25674
8. Oh-Park M, Holtzer R, Mahoney J, et al. Motor dual-task effect on gait and task of upper limbs in older adults under specific task prioritization: pilot study. Aging Clin Exp Res. 2013;25(1):99–106. doi:10.1007/s40520-013-0014-0
9. Smith E, Cusack T, Blake C. The effect of a dual task on gait speed in community dwelling older adults: a systematic review and meta-analysis. Gait Posture. 2016;44:250–258. doi:10.1016/j.gaitpost.2015.12.017
10. Smith E, Cusack T, Cunningham C, et al. The influence of a cognitive dual task on the gait parameters of healthy older adults: a systematic review and meta-analysis. J Aging Phys Act. 2017;25:671–686. doi:10.1123/japa.2016-0265
11. Lamoth CJ, van Deudekom FJ, van Campen JP, et al. Gait stability and variability measures show effects of impaired cognition and dual tasking in frail people. J Neuroeng Rehabil. 2011;8:2. doi:10.1186/1743-0003-8-2
12. Beauchet O, Annweiler C, Dubost V, et al. Stops walking when talking: a predictor of falls in older adults? Eur J Neurol. 2009;16:786–795. doi:10.1111/j.1468-1331.2009.02612.x
13. Muir-Hunter SW, Wittwer JE. Dual-task testing to predict falls in community-dwelling older adults: a systematic review. Physiotherapy. 2016;102:29–40. doi:10.1016/j.physio.2015.04.011
14. Menant JC, Schoenea D, Sarofimc M, et al. Single and dual task tests of gait speed are equivalent in the prediction of falls in older people: a systematic review and meta-analysis. Ageing Res Rev. 2014;16:83–104. doi:10.1016/j.arr.2014.06.001
15. Hatton AL, Rome K. Falls, footwear, and podiatric interventions in older adults. Clin Geriatr Med. 2019;35(2):161–171. doi:10.1016/j.cger.2018.12.001
16. Hatton AL, Rome K, Dixon J, et al. Footwear interventions: a review of their sensorimotor and mechanical effects on balance performance and gait in older adults. J Am Podiatr Med Assoc. 2013;103:516–533. doi:10.7547/1030516
17. Chen TH, Chou LW, Tsai MW, et al. Effectiveness of a heel cup with an arch support insole on the standing balance of the elderly. Clin Interv Aging. 2014;20:351–356.
18. Gross MT, Mercer VS, Lin FC. Effects of foot orthoses on balance in older adults. J Orthop Sports Phys Ther. 2012;42(7):649–657. doi:10.2519/jospt.2012.3944
19. Mulford D, Taggart HM, Nivens A, et al. Arch support for improving balance and reducing pain in older adults. Appl Nurs Res. 2008;21:153–158. doi:10.1016/j.apnr.2006.08.006
20. Niino N, Tsuzuku S, Ando F, et al. Frequencies and circumstances of falls in the National Institute for Longevity Sciences, Longitudinal Study of Aging. J Epidemiol. 2000;10:S90. doi:10.2188/jea.10.1sup_90
21. Shkuratova N, Morris ME, Huxham F. Effects of age on balance control during walking. Arch Phys Med Rehabil. 2004;85:582–588. doi:10.1016/j.apmr.2003.06.021
22. Gobbo S, Bergamin M, Sieverdes JC, et al. Effects of exercise on dual-task ability and balance in older adults: a systematic review. Arch Gerontol Geriatr. 2014;58:177–187. doi:10.1016/j.archger.2013.10.001
23. Burns ER, Stevens JA, Lee R. The direct costs of fatal and non-fatal falls among older adults - United States. J Safety Res. 2016;58:99–103. doi:10.1016/j.jsr.2016.05.001
24. Hsu HC, Jhan LJ. Risk factors of falling among the elderly in Taiwan. TW Geriatr Gerontol. 2008;3:141–154.
25. Tsai CF, Lee WJ, Wang SJ, et al. Psychometrics of the montreal cognitive assessment (MoCA) and its subscales: validation of the taiwanese version of the MoCA and an item response theory analysis. Int Psychogeriatr. 2012;24:651–658. doi:10.1017/S1041610211002298
26. Peng HT, Tien CW, Lin PS, Peng HY, Song CY. Novel mat exergaming to improve the physical performance, cognitive function, and dual-task walking and decrease the fall risk of community-dwelling older adults. Front Psychol. 2020;11:1620. doi:10.3389/fpsyg.2020.01620
27. Dadashi F, Mariani B, Rochat S, et al. Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sensors. 2014;14:443–457. doi:10.3390/s140100443
28. Mariani B, Hoskovec C, Rochat S, et al. 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J Biomech. 2010;43:2999–3006. doi:10.1016/j.jbiomech.2010.07.003
29. McDowd JM. The effects of age and extended practice on divided attention performance. J Gerontol. 1986;41:764–769. doi:10.1093/geronj/41.6.764
30. Nakakubo S, Doi T, Makizako H, et al. Association of walk ratio during normal gait speed and fall in community-dwelling elderly people. Gait Posture. 2018;66:151–154. doi:10.1016/j.gaitpost.2018.08.030
31. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
32. Barak Y, Wagenaar RC, Holt KG. Gait characteristics of elderly people with a history of falls: a dynamic approach. Phys Ther. 2006;86(11):1501–1510. doi:10.2522/ptj.20050387
33. Callisaya ML, Blizzard L, McGinley JL, et al. Risk of falls in older people during fast-walking–the TASCOG study. Gait Posture. 2012;36(3):510–515. doi:10.1016/j.gaitpost.2012.05.003
34. Qu X. Impacts of different types of insoles on postural stability in older adults. Appl Ergon. 2015;46:38–43. doi:10.1016/j.apergo.2014.06.005
35. Iglesias MEL, de Bengoa Vallejo RB, Pena DP. Impact of soft and hard insole density on postural stability in older adults. Geriatr Nurs. 2012;33:264–271. doi:10.1016/j.gerinurse.2012.01.007
36. Pavol MJ, Owings TM, Foley KT, et al. Gait characteristics as risk factors for falling from trips induced in older adults. J Gerontol a Biol Sci Med Sci. 1999;54(11):M583–590. doi:10.1093/gerona/54.11.M583
37. Van Iersel MB, Ribbers H, Munneke M, et al. The effect of cognitive dual tasks on balance during walking in physically fit elderly people. Arch Phys Med Rehabil. 2007;88:187–191. doi:10.1016/j.apmr.2006.10.031
38. Huijben B, van Schooten KS, van Dieën JH, Pijnappels M. The effect of walking speed on quality of gait in older adults. Gait Posture. 2018;65:112–116. doi:10.1016/j.gaitpost.2018.07.004
39. Fan Y, Li Z, Han S, Lv C, Zhang B. The influence of gait speed on the stability of walking. Gait Posture. 2016;47:31–36. doi:10.1016/j.gaitpost.2016.02.018
40. Hunter SW, Divine A, Frengopoulos C, et al. A framework for secondary cognitive and motor tasks in dual-task gait testing in people with mild cognitive impairment. BMC Geriatr. 2018;18:202. doi:10.1186/s12877-018-0894-0
41. Wang RY, Wang YL, Cheng FY, et al. Effects of a multicomponent exercise on dual-task performance and executive function among older adults. Int J Gerontol. 2018;12:133–138. doi:10.1016/j.ijge.2018.01.004
42. Falbo S, Condello G, Capranica L, et al. Effects of physical-cognitive dual task training on executive function and gait performance in older adults: a randomized controlled trial. Biomed Res Int. 2016;2016:5812092. doi:10.1155/2016/5812092
43. Bahureska L, Najafi B, Saleh A, et al. The impact of mild cognitive impairment on gait and balance: a systematic review and meta-analysis of studies using instrumented assessment. Gerontology. 2017;63:67–83. doi:10.1159/000445831
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.