Back to Journals » Clinical Interventions in Aging » Volume 20
Effects of a Comprehensive Intervention Program of Static-Dynamic Balance Training Combined with Reminiscence Therapy on the Level of Healthy Aging Among Older Adults in a Rural Community: A Randomized Controlled Trial
Authors Yang X, Li S, Xu LJ, Guo G, Song X, Ni Y, Ren C, Shi M, Sun Y ![]()
Received 1 May 2025
Accepted for publication 18 August 2025
Published 27 August 2025 Volume 2025:20 Pages 1381—1399
DOI https://doi.org/10.2147/CIA.S537889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Xinyu Yang,1,* Shasha Li,1,* Li Jun Xu,2,* Guojing Guo,1 Xiaofang Song,1 Yingyuan Ni,3 Canqi Ren,1 Mengxue Shi,1 Yashuang Sun1
1School of Medicine, Huzhou University, Huzhou, Zhejiang, People’s Republic of China; 2Medical College of Liaocheng University, Liaocheng, Shandong, People’s Republic of China; 3Yongkang Health School, Yongkang, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shasha Li, School of Medicine, Huzhou University, 759 Second Ring Road, Huzhou District, Huzhou, Zhejiang, 313000, People’s Republic of China, Email [email protected]
Purpose: Healthy aging levels are generally low among rural older adults, yet the effects of combined static-dynamic balance training and reminiscence therapy on this population remain underexplored. This study evaluated the efficacy of a combined static-dynamic balance training and reminiscence therapy (SDBT-RT) program in promoting healthy aging in rural communities, with emphasis on both immediate and sustained outcomes.
Patients and methods: A randomized, assessor-blinded, controlled trial with two parallel groups included 64 adults > 60 years from rural Huzhou, China, randomized to intervention (n=32) and control (n=32) groups. The intervention group received a 12-week SDBT-RT program, conducted twice weekly: 40-minute reminiscence therapy plus 50-minute balance training in odd weeks, and 50-minute balance training alone in even weeks; controls received health education and exercise instruction. Healthy Aging Instrument (HAI), satisfaction, and feasibility (adherence, safety) were assessed at baseline (T0), post-intervention (T1), and 1-month follow-up (T2). Data analysis used repeated measures analysis of variance and a simple effect test.
Results: The intervention group’s total HAI score significantly increased from 111.03 ± 11.36 at baseline to 129.80 ± 11.30 at T1 and 130.63 ± 12.01 at T2 (all P < 0.001). Significant between-group differences were observed in most domains at T1 and T2 (all P < 0.05), except “Being Self-Sufficient and Living Simply” (significant only at T1, P = 0.042) and “Making Merit and Good Deeds” (non-significant). Repeated measures showed significant within-group improvements across all domains in the intervention group (all P < 0.05). The intervention group had high adherence (88.8%), satisfaction (4.96 ± 0.18), and no adverse events. The control group improved only in self-care awareness (P = 0.042).
Conclusion: SDBT-RT effectively enhances healthy aging in rural older adults with high feasibility and sustained benefits, offering a promising intervention model in resource-limited rural settings.
Trial Registration: The Chinese Clinical Trial Registry, ChiCTR2300072132.
Plain Language Summary: Ensuring healthy aging is crucial, especially in rural areas where older adults often face challenges like limited physical activity, poor mental health, and weak social connections. This study aimed to see if combining physical exercise with emotional support could improve the well-being of older adults living in rural communities.
We designed a 12-week program that included balance training and reminiscence therapy, tested with a group of 64 adults aged 60 and above. Participants were randomly assigned to either the program or a control group that received standard health education.
The results showed that those who took part in the program experienced significant improvements in physical health, memory, social participation, and emotional well-being. These benefits continued for at least one month after the program ended. Participants were highly satisfied with the program and showed no serious side effects. In contrast, the control group showed only minor improvements. This suggests that the new program is more effective than regular health education. The program used low-cost materials and community spaces, making it easy to implement in rural settings.
By supporting both physical and emotional needs, this approach offers a practical and affordable strategy to help rural older adults stay active, socially connected, and mentally strong as they age.
Keywords: healthy aging, static-dynamic balance training, reminiscence therapy
Introduction
Global population aging has emerged as a significant public health challenge.1 To address this challenge, the World Health Organization (WHO) has prioritized healthy aging to ensure quality of life for older adults.2,3 Previous studies have shown that 36% (65–74 years) and 53% (>75 years) of older adults remain physically inactive,4 15.5% exhibit mild cognitive impairment,5 22% experience anxiety or depressive symptoms,6,7 and only 10.9% engage in weekly social activities.8 However, studies have shown that due to limited economic and medical resources in rural areas, insufficient social security coverage, and the influence of traditional beliefs, the level of healthy aging among rural older adults is relatively low.9,10
The World Health Organization defines healthy aging as “the process of maintaining functional capacity to enable well-being in older age” emphasizing the need for individuals to adapt dynamically to environmental demands.11 Regular physical activity is a key strategy for promoting healthy aging and preserving independence in older adults.12 Balance training improves functional capacity, proprioception, and cognitive performance, thereby reducing fall risk, mitigating frailty, and enhancing quality of life.13,14 Static-dynamic balance training (SDBT) integrates static postural control (eg, single-leg stance) with dynamic gait tasks (eg, narrow-base walking).15 Compared to the complex movements of Tai Chi or the equipment demands of resistance training,16 SDBT is space-efficient, easily adjustable through visual and vestibular perturbations, and adaptable to various functional levels. Moreover, by simulating real-life challenges (eg, uneven terrain, interfering movements), SDBT is particularly suitable for older adults in rural areas, where resources are limited and physical literacy is often low.17 However, physical training alone has limited effects on psychosocial outcomes,18 underscoring the need for integrated interventions that combine exercise with psychosocial support to promote holistic well-being in aging populations.
Reminiscence therapy (RT), also known as life review therapy, is a psychological intervention aimed at alleviating symptoms of cognitive decline. By activating the default mode network, RT enhances autobiographical memory19 and has been shown to improve emotional well-being,20 cognitive function,21 social engagement,22 quality of life, life satisfaction, and adaptability to aging.23 The World Health Organization’s Integrated Care for Older People (ICOPE) framework advocates the integration of physical activity with structured, group-based psychological interventions to promote healthy aging at the community level.24 Similarly, China’s 14th Five-Year Plan emphasizes the importance of precise, comprehensive, and personalized strategies for advancing healthy aging. Although previous studies on RT have primarily focused on cognitive and emotional outcomes, its potential to enhance social cohesion and promote exercise adherence through group-based nostalgic activities has received limited attention.20,21 In contrast, conventional standalone exercise programs often struggle to sustain long-term participation due to insufficient consideration of participant motivation, social context, and the absence of cognitive or social stimulation.13 Integrating RT with static-dynamic balance training (SDBT) presents a novel, synergistic approach that addresses both physical and psychosocial determinants of healthy aging. However, the effectiveness of this combined intervention warrants further investigation.
The Theory of Planned Behavior (TPB), an extension of the Theory of Reasoned Action, evaluates individuals’ intentions to engage in specific behaviors by considering both personal and social determinants of intention.25 TPB comprises four key constructs: attitude, subjective norm, perceived behavioral control, and behavioral intention. Previous studies have demonstrated that TPB has strong predictive validity for health behaviors requiring self-regulation, such as physical activity, making it a suitable framework for designing health interventions.26,27
This study aims to determine the impact of the SDBT-RT project based on TPB on rural older adults. The research hypotheses of this study are as follows: (1) The SDBT-RT intervention would have positive effects on healthy aging; (2) The SDBT-RT program is feasible and associated with high participant satisfaction.
Methods
Study Design and ethical Considerations
This single-blind, two-arm parallel-group, randomized controlled trial was conducted in accordance with the Declaration of Helsinki and registered on www.chictr.org.cn (No. ChiCTR2300072132), and ethical approval was granted by the Institutional Review Board of the Huzhou University, Huzhou, China (No. 20220607). All participants provided written informed consent, explicitly acknowledging their right to withdraw at any time. The intervention protocol adhered to the TIDieR Checklist (Template for Intervention Description and Replication), ensuring transparency and replicability.
Participants
Participants were recruited and received interventions between May and August 2023, with follow-up ending in September 2023. Inclusion Criteria: (1) Age ≥ 60 years; (2) Independent walking ability for ≥ 15 consecutive minutes (without assistive devices); (3) Long-term rural residency (≥ 1 year); (4) Provided informed consent and willingness to cooperate. Exclusion Criteria: (1) a diagnosis of severe pre-existing physical illnesses, defined as conditions that significantly impair physical functioning or require regular medical intervention (eg, advanced heart disease, cancer, or other major organ diseases); (2) cognitive impairment (Short Portable Mental Status Questionnaire score ≥ 3); (3) taking psychotropic medication; (4) participating in psychosocial /sports interventions and (5) severe visual or hearing impairment, as determined by the medical records.
Sample Size
A power analysis was conducted using G*Power version 3.1 to determine the required sample size for detecting significant differences between the intervention and control groups. Based on prior studies on reminiscence therapy and physical activity for older adults,28 and expected effect sizes, the following parameters were used for the calculation: Expected effect size (Cohen’s d) = 0.778; Statistical power = 0.80; Significance level (α) = 0.05. Based on these parameters, the power analysis indicated that a minimum sample size of 54 participants was required to detect significant effects. To account for a 20% attrition rate, 64 participants were recruited, with 32 participants randomly assigned to each group.
Randomization, Allocation Concealment, and Blinding
Two rural communities in Huzhou with comparable socio-economic levels, infrastructure, and population structures were selected. These communities were then randomly assigned to either the intervention or control group using a computer random number method, ensuring a distance of at least 5 kilometers between them to reduce the risk of infection. Within each of the randomly assigned communities, participants who met the inclusion criteria were consecutively enrolled. The allocation was hidden through sealed opaque envelopes containing labels of “intervention” or “control”, which were opened by the research assistants after randomization. Data collectors, outcome assessors and analysts were all unaware of the groupings. Participants could not be blinded due to the nature of the intervention. However, researchers minimized observer bias through standardized operation procedures and third-party evaluations. Moreover, each group of interventions was conducted at different locations, which could reduce the contamination of the trial caused by social interaction and communication among participants.
Intervention
Intervention Group
The Static-Dynamic Balance Training Combined with Reminiscence Therapy (SDBT-RT) program, grounded in the Theory of Planned Behavior, was designed to promote positive health behaviors. Guided by TPB, an SDBT-RT program was developed, taking into account the rural community context—including local policies, lifestyle habits, and social networks—as well as individual-level characteristics. The formulation of a research protocol that incorporates the model’s core constructs warrants further investigation. At the level of behavioral attitude, reminiscence therapy sessions are used to evoke positive memories, foster a constructive outlook on aging, and strengthen the belief that “participating in this program can enhance my well-being”.27 At the subjective norm level, the group-based intervention delivered in community centers helps establish supportive social norms. Peer observation and interaction reduce perceived barriers to participation. For perceived behavioral control, the SDBT component employs a progressive difficulty structure and real-time movement guidance to lower the perceived difficulty of performing the exercises.
The program was reviewed and revised by five experts in sports rehabilitation, medical psychology, geriatrics, health management, and nursing. Additionally, a pilot study was conducted prior to the main study to assess the feasibility of the intervention. The static-dynamic balance training component was derived from balancing postural control movements,17 with a gradual increase in intensity by varying sensory inputs and external distractions, and consisted of three parts: (1) a 10-minute warm-up phase (including range-of-motion exercises for the wrists, hips, shoulders, knees, and ankles); (2) a 15-minute static balance training session (standing on both feet; standing in parallel and tandem; standing in tandem; standing on one foot); and (3) a 25-minutes of dynamic balance training (normal gait; narrow gait; overlapping gait; tandem gait). RT is based on Erikson’s theory of psychosocial development, which states that recalling life experiences can help rural older adults resolve the psychological crisis of integration and despair in the final stages of life.29 Therefore, a structured procedure of reviewing the past, returning to the present, evaluating the past, and facing the present was set up and, combined with the temporal characteristics of older Chinese people’s lives, recreational activities, and traditional cultural practices; reminiscence therapy involves six themes:“Our Time”,“My Happy Times”, “Achievements in my life”, “Revisiting Traditional Festivals”, “My Hobbies”, and “Feeling the good old days”, promoting their self-integrity and optimism to face reality with positive goal orientation. Table 1 provides the content of the SDBT-RT.
 |
Table 1 Static-Dynamic Balance Training Combined with Reminiscence Therapy Program |
Each group of interveners consists of general practitioners, community health workers and medical postgraduate students who have undergone one month of specialized training. Thirty-two people in the intervention group were randomly divided into 8-person groups, and the appropriate time periods (8:00–10:00) were selected according to the activity habits of the elderly in the community. The intervention sites are fixed as community activity centers equipped with multimedia facilities and green rest areas. The intervention lasted for 12 weeks. In odd-numbered weeks, a dual intervention model of “40-minute RT + 50-minute SDBT” was adopted to establish behavioral intentions, and behavioral attitudes and subjective norms were strengthened through RT. Synchronous balance training enhances perceptual behavioral control through immediate improvement of physical functions. In even weeks, only 50 minutes of SDBT is conducted. A single training can reduce cognitive load and focus on the solidification of motor skills. To record engagement in reminiscence therapy, a standardized observation checklist and participant feedback forms were used after each session to assess participation and emotional responses. Facilitators were trained to recognize distress or fatigue, with activities adapted to individual conditions and emergency protocols in place for physical or psychological incidents.
The implementer is required to fill out the “Implementation Fidelity Checklist” immediately after each session, recording whether the RT theme is carried out as per the weekly plan, whether the SDBT training is upgraded in stages, and the duration of the core links. The project supervisor randomly selects 20% of the checklists every week for phone review. When deviations are found, the implementers are required to explain the reasons and formulate improvement measures at the weekly regular meeting. Meanwhile, the implemutors also need to record the physical and mental states of the participants and use resources such as unified theme audio and video, handicraft materials, festival decorations and life goal lists. During the intervention period, the intervention coordinator recorded the attendance of each participant in each course and promptly followed up on those who were absent to arrange make-up classes as much as possible. A “Behavior Log Form” was designed to record changes such as supplement use, recreational activities, and disease conditions. It was reviewed monthly by general practitioners to ensure that the intervention effect was not interfered with by confounding factors. During the 4-week follow-up, participants in the intervention group received four brief weekly phone calls (5–10 minutes each) to check on home practice adherence, provide encouragement, and answer basic questions. No new intervention content was introduced.
Control Group
The control group received standardized health education and general exercise guidance delivered by trained staff at community centers. Biweekly, 40-minute, 12-week group sessions cover six topics: Static Balance Training Principles, Dynamic Equilibrium Skill Development, Psychosocial Adaptation Techniques, Fall Risk Mitigation Strategies, Home Environment Optimization, and Lifestyle Behavior Internalization, focusing on knowledge transmission and fundamental movement instruction. A 1-month follow-up included four supervised telephone check-ins, which matched the intervention group in frequency and duration, and served only to monitor engagement and address basic questions, without introducing any new content.
Assessment
Sociodemographic Profile
A structured questionnaire developed by the research team collected demographic data (gender, age, education, marital status, residence, income), lifestyle factors (weekly exercise frequency, community engagement, sleep quality), and health status (chronic disease burden, self-rated health, emotional lowness).
Primary Outcomes
The Healthy Aging Instrument (HAI)
The Healthy Aging Instrument (HAI) was developed by Thiamwong et al30 and consists of 35 entries in 9 dimensions: Staying Cognitively Active, Staying Physically Active, Having Social Participation, Having Social Relationships and Support, Practicing Self-Care and Self-Awareness, Accepting Aging, Being Self-Sufficient and Living Simply, Making Merit and Good Deeds, and Managing Stress. A 5-point Likert scale was used (1 = not at all consistent, 2 = slightly consistent, 3 = not sure, 4 = moistening, physical functioning, social participation, social relationships and support, self-care, acceptance consistent, 5 = completely consistent). Total scores ranged from 35 to 175, with higher scores reflecting better levels of healthy aging, including more active engagement, stronger self-care, and greater psychosocial well-being. The Cronbach’s α in the Chinese version was 0.93, and the internal consistency was good.31,32
Secondary Outcomes
Satisfaction Evaluation
Satisfaction evaluation included five dimensions: (i) I like the atmosphere of the group intervention; (ii) I am active in the group intervention; (iii) I am willing to communicate and share with other group members; (iv) I am active in the integrated intervention; and (v) I actively refer to the manuals for exercise during the rest of the week. Five ratings on a Likert scale were used for the assessment, namely, “fully compliant”, “fairly compliant”, “fair”, “not quite compliant”, and ‘not at all compliant. Five experts assessed the content relevance of study items,33 resulting in a scale-level Content Validity Index of 0.90, showing high content validity. The satisfaction scale was pretested, achieving a Cronbach’s alpha of 0.92, indicating good reliability and validity. This was used as an indirect indicator of intervention acceptability.
Feasibility Assessment
The safety and adherence were selected as evaluation indicators for the feasibility of the comprehensive intervention program. The incidence of adverse events during the study period (eg, excessive physical fatigue, fall, mental abnormality) was used as the evaluation index for safety, ie, adverse event incidence (%) = (number of cases of adverse events in the intervention group/number of people in the intervention group)*100%; and adherence was evaluated by calculating the activity attendance rate of the older adults in the intervention group. Activity attendance rate (%) = total number of individual activity participation/total number of interventions* 100%.
Data Collection and Assessor Training
Data collection took place in rural community activity centers. Baseline data (with general information and primary measures) were collected at the end of screening to baseline (T0), a second collection (with primary and secondary measures) was carried out within one week after 12 weeks of the intervention (T1), and the primary measures were collected again within one week after 1 month of follow-up (T2). Assessors received structured training before the trial, including the use of evaluation tools, the practical operation of schemes, and the verification and maintenance of session consistency. Questionnaires were completed in person on paper, with assessor assistance when necessary.
Data Entry and Statistical Analysis
SPSS 25.0 was used for data processing in this study, setting α=0.05 as the significance level, with P<0.05 indicating a statistically significant difference. Two researchers entered and checked data to ensure accuracy. For demographic data, measures were expressed as mean ± standard deviation, and counts were expressed as frequency and constitutive ratio. Data normality was determined by the Shapiro–Wilk test, and accordingly, mean ± standard deviation or median (quartiles) were chosen to represent continuous variables. Balanced comparisons of baseline data were performed by t test Mann–Whitney U-test, or χ²-test. When both groups of outcome indicators met normal distribution and variance chi-square, two-factor repeated measures analysis of variance (ANOVA) was used to analyze the effects of time factors and treatment factors on the healthy aging scores of the two groups of study participants, as well as the interactions between time and groups. Generalized estimating equation analysis was used when the two groups’ outcome indicators did not conform to a normal distribution. The per-protocol analysis (PPA) was conducted by excluding subjects who withdrew from randomization to the end of the intervention, stopped the intervention, and/or participated in less than 70% of the prescribed exercise courses. Descriptive statistics were used for satisfaction assessment and program feasibility.
Results
Recruitment, Attrition, and Retention
As shown in the CONSORT flowchart in Figure 1, 64 participants who met the inclusion criteria and provided informed consent were allocated to two groups (32 in each group). Two participants in the intervention group withdrew due to health issues, and two participants in the control group withdrew due to time constraints. Neither of the health-related withdrawals was linked to adverse events caused by the SDBT-RT program. The final participants included in PPA were 30 people in each of the two groups (retention rate 94%).
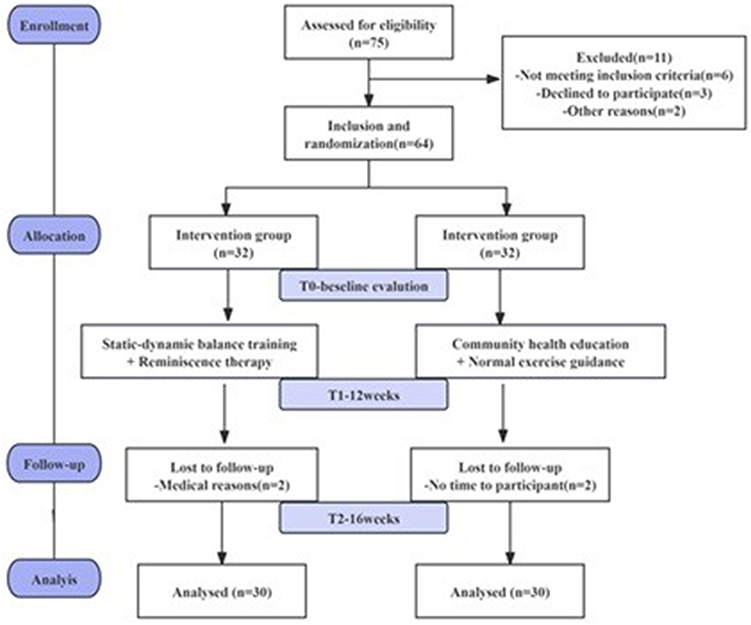 |
Figure 1 Study flow chart. |
Descriptive Data of Participant Characteristics
The largest percentage of the study was in the age group 70–79 years (61.7%, 37/60). Table 2 shows that there were no significant differences in baseline demographic characteristics (age, gender, education level) and health indicators (number of chronic diseases, sleep quality) between the intervention group and the control group analyzed by PPA (all P > 0.05), indicating good comparability.
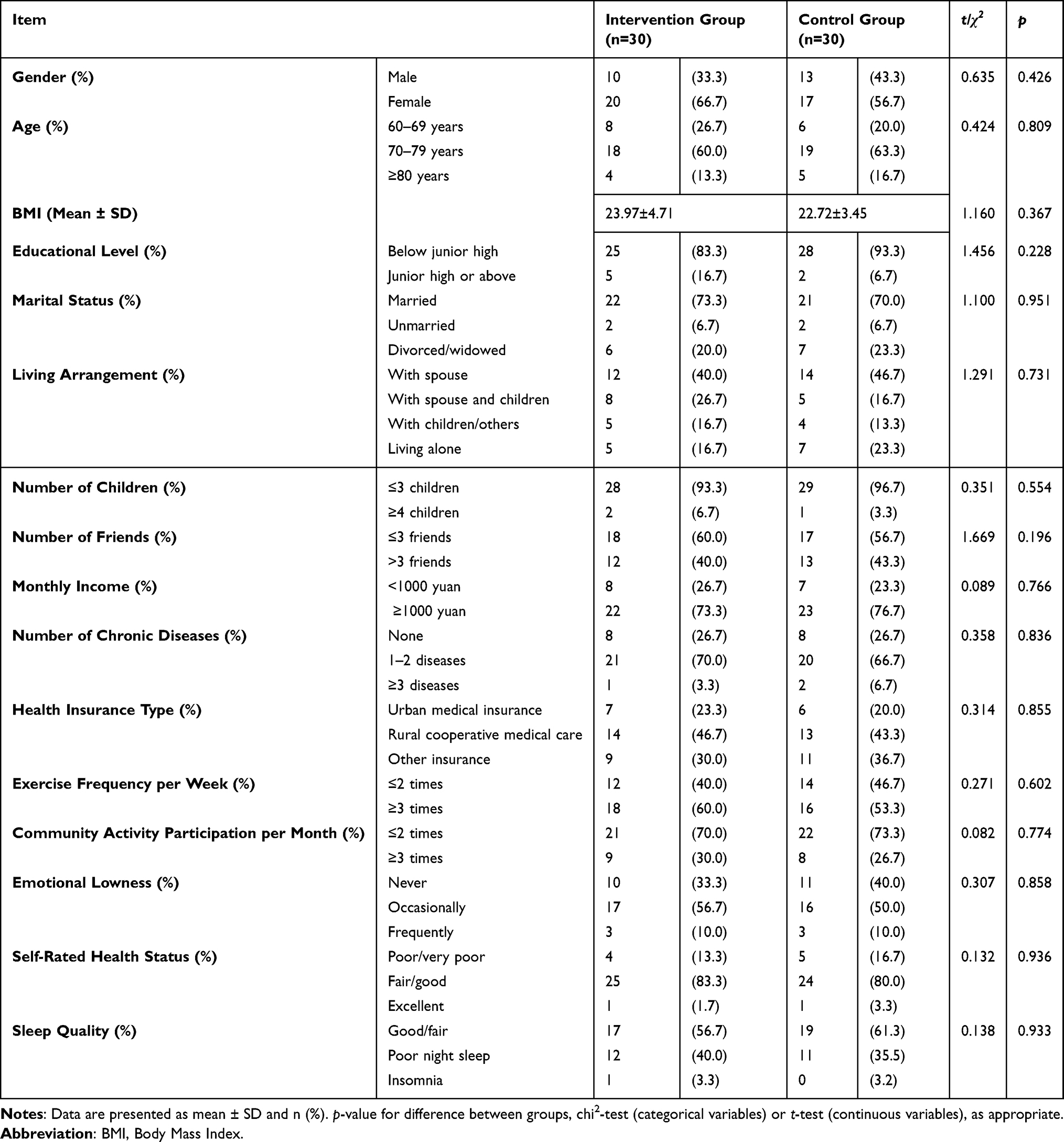 |
Table 2 Sociodemographic Characteristics of the Participants in the Two Groups |
Impact of the SDBT-RT Program on Primary Outcomes
As shown in Table 3, the time × group interaction was significant for total healthy aging score (18.8 point; P< 0.001), rising from 111.03 ± 11.36 at baseline to 129.80 ± 11.30 post-intervention and 130.63 ± 12.01 at follow-up. In contrast, the control group exhibited only a modest change (5.2 points; P > 0.05). Significant between-group differences were also observed across most domains at post-intervention and follow-up. In particular, the intervention group improved in “Staying Cognitively Active” (2.14 points; P= 0.002), “Staying Physically Active” (2.23 points; P= 0.002), and “Having Social Participation” (1.60 points; P= 0.042). Similar improvements were seen in “Having Social Relationships and Support” (3.63 points, P= 0.001), “Practicing Self-Care and Self-Awareness” (2.23 points; P= 0.010), “Accepting Aging” (1.57 points; P= 0.013), and “Managing Stress” (3.00 points, P < 0.001). No significant improvements were found in “Being Self-Sufficient and Living Simply” (18.95 ± 1.95 to 19.67 ± 1.60; P > 0.05) or “Making Merit and Good Deeds” (15.00 ± 2.00 to 15.90 ± 2.24; P > 0.05). Visualizations are provided in Figures 2–4.
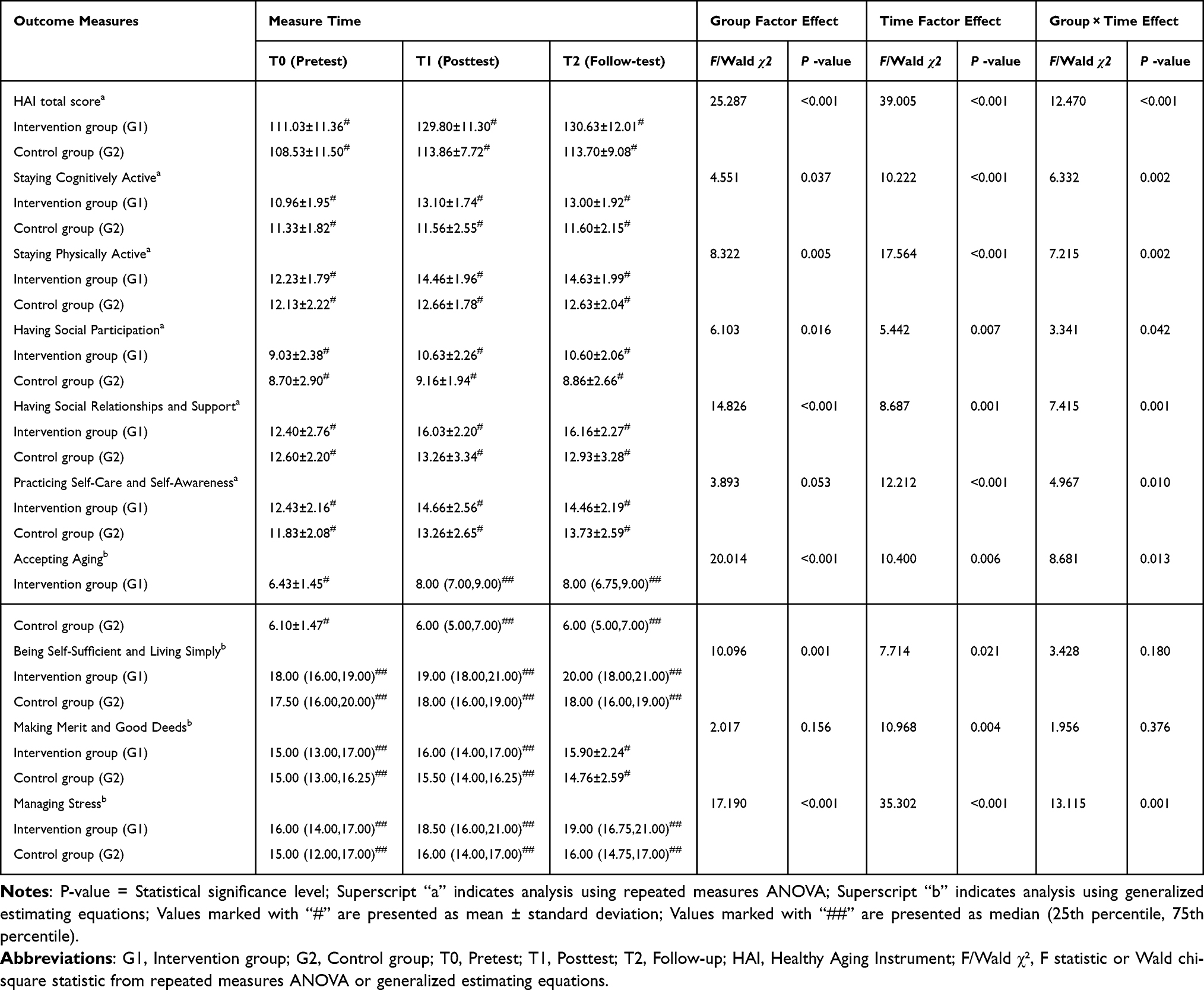 |
Table 3 Impact of the Intervention on Outcome Measures at Three Timepoints (Group × Time) Test (N = 60) |
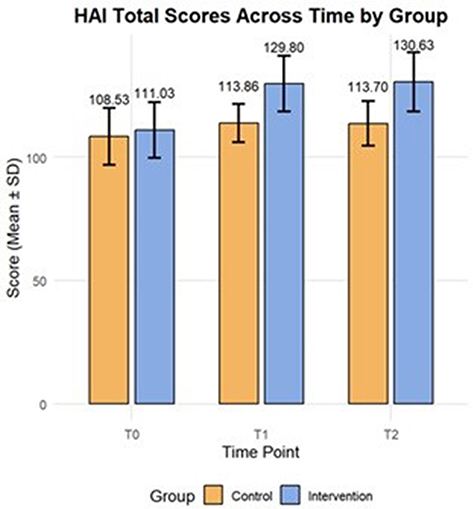 |
Figure 2 HAI total scores across time by group. |
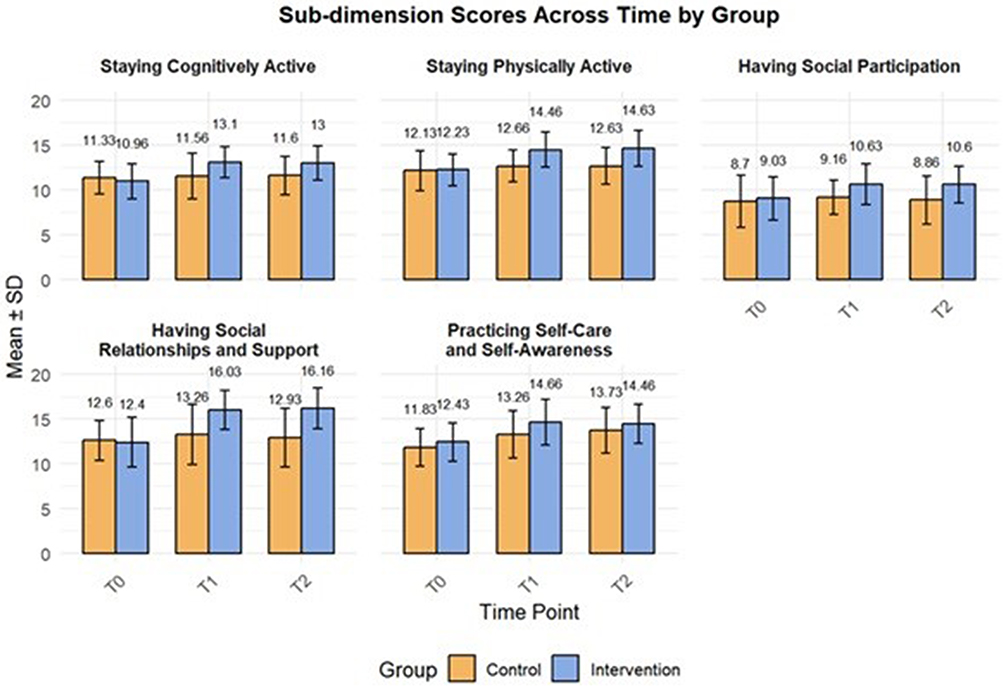 |
Figure 3 Bar chart of sub-dimension scores across time by group. |
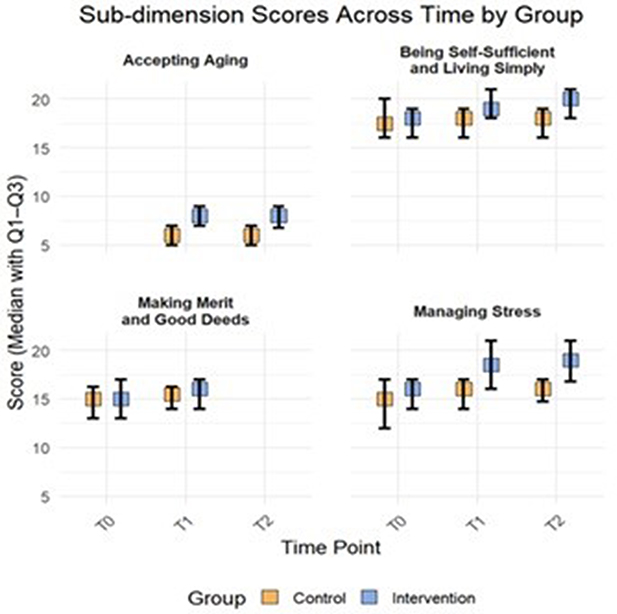 |
Figure 4 Box plot of sub-dimension scores across time by group. |
Table 4 shows the results of the comparison of variables between groups. There was no statistically significant difference (P > 0.05) between the intervention and control groups on all variables at T0. At the T1 time point, there was no statistically significant difference between groups in the dimension of “Making Merit and Good Deeds” (P = 0.233), and the differences in all other outcome indicators were statistically significant (P < 0.05). At the T2 time point, there were statistically significant differences (P < 0.05) between the intervention and control groups for all outcome indicators except for the “Practicing Self-Care and Self-Awareness” (P = 0.242) and “Making Merit and Good Deeds” (P = 0.076) dimensions, which did not show significant between-group differences.
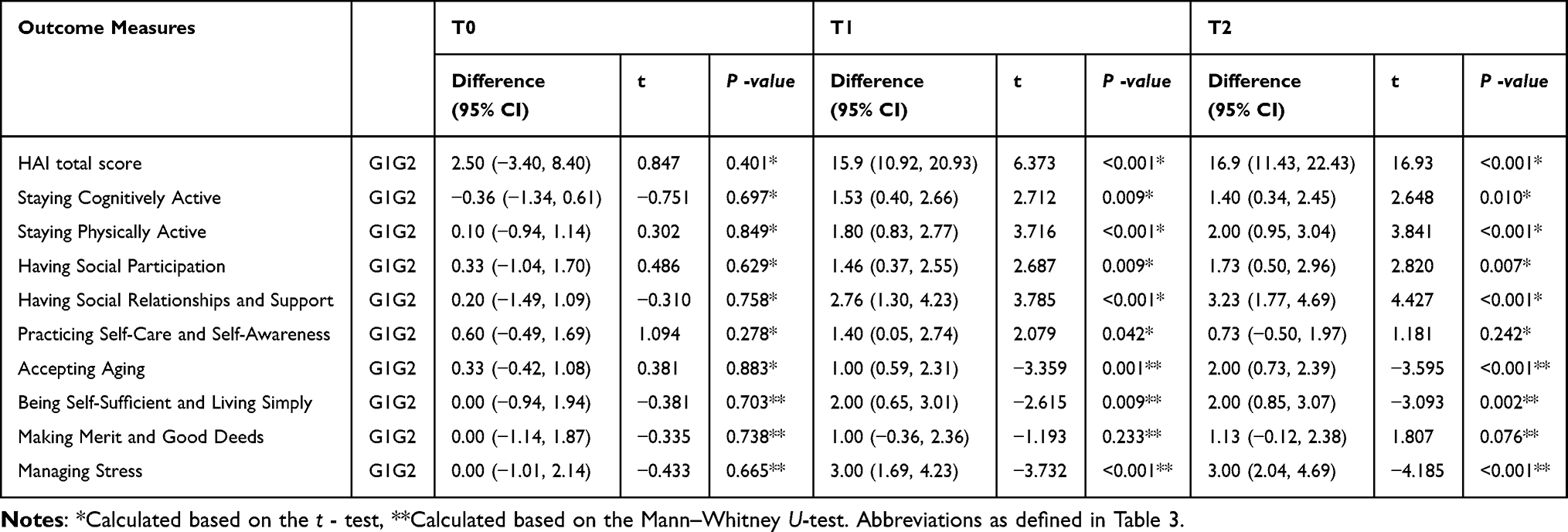 |
Table 4 Simple Effect Analysis and Multiple Comparisons of Group |
Table 5 Within-group time effect analyses show the results of all variables over time in both groups. Compared with baseline T0, there were statistically significant differences in the total healthy aging scores and scores for each dimension in the intervention group after the intervention (P < 0.05), and the effects persisted through the follow-up period. In the control group, statistically significant differences were observed at T1 in the total healthy aging score, “Practicing Self-Care and Self-Awareness” and “Making Merit and Good Deeds” dimensions (P < 0.05). However, only the total healthy aging score (P = 0.017) and “Practicing Self-Care and Self-Awareness” (P = 0.002) retained statistically significant differences at the T2 follow-up time point.
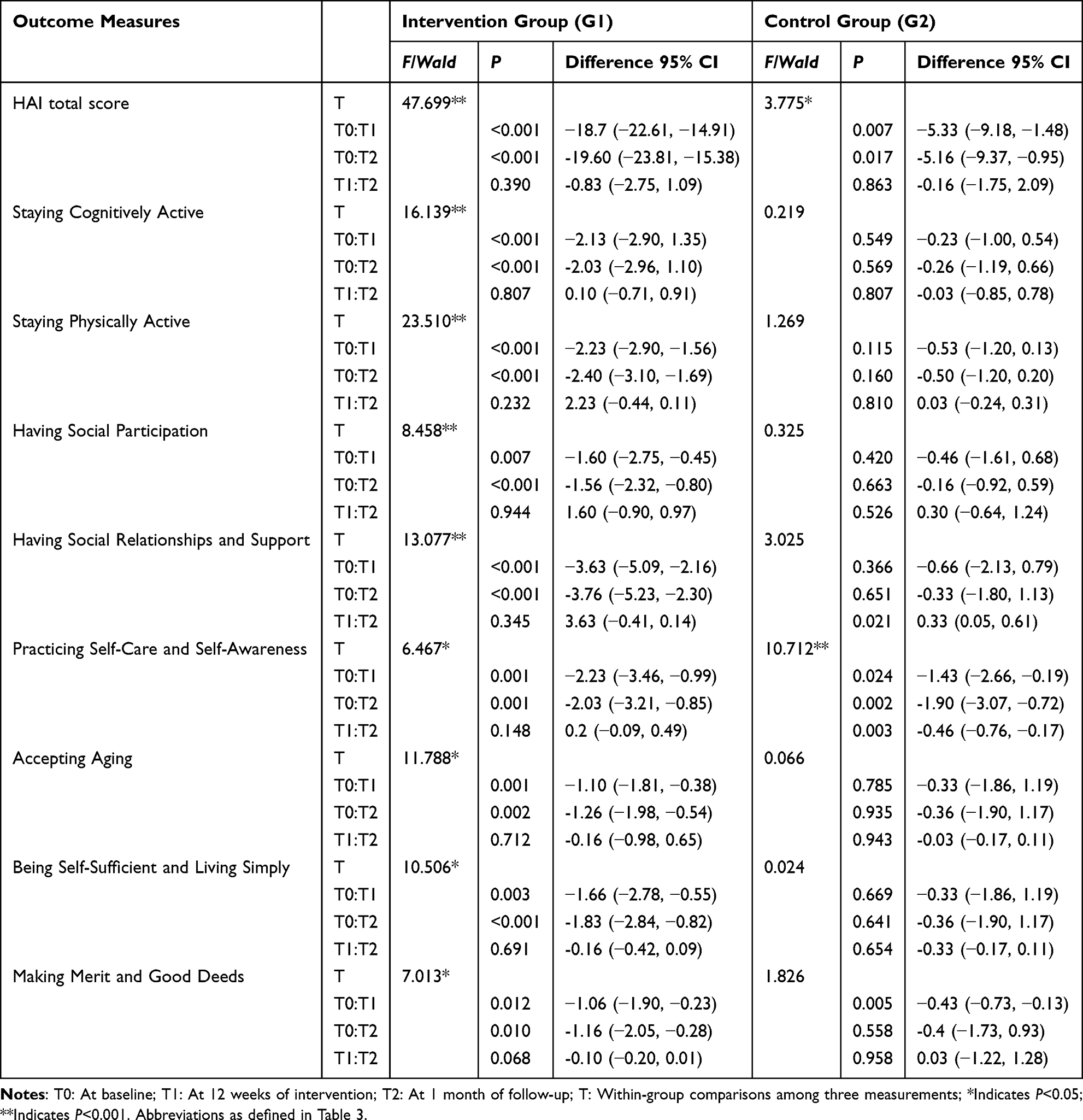 |
Table 5 Simple Effect Analysis and Multiple Comparisons of Time |
Impact of the SDBT-RT Program on Secondary Outcomes
The satisfaction survey results (mean score: 4.96 ± 0.18) indicated that a high level of participant satisfaction and 100% expressed willingness to recommend it to others. At the 12-week mark, the compliance rate was 88.8% in the intervention group and 85.0% in the control group, with no statistically significant difference between groups (P = 0.267). Adverse events were continuously monitored throughout both the intervention and follow-up periods, and no serious intervention-related adverse events were reported.
Discussion
To the best of our knowledge, this is the first randomized controlled trial to evaluate the impact of a 12-week SDBT-RT program on healthy aging in older adults in a rural community. Our findings indicate that SDBT-RT significantly enhanced healthy aging in rural older adults and maintained a significant effect one-month post-intervention. This can attributed to the fact that SDBT-RT was designed based on the Theory of Planned Behavior, which posits that a combination of behavioral attitudes, subjective norms, and perceived behavioral control determines behavioral intentions.26 Specifically, SDBT-RT fosters positive attitudes toward later life through group reminiscence therapy, thereby increasing willingness to perform; family and community support create a conducive environment for promoting subjective norms of healthy behaviors; and progressive balance training enhances perceptions of behavioral controllability and promotes exercise habits. The three elements synergistically promote the formation and sustainability of healthy aging behaviors in older adults.
Cognitive functioning is a core dimension in measuring healthy aging, often evaluated through daily activities, executive ability, and active thinking. This study found that SDBT-RT continuously improves cognitive function, which differs from the conclusions of some studies that only focus on a single intervention.34,35 The comparative study35 used a single multi-component exercise. After 12 weeks, there was no significant improvement in cognitive function in the Mini-Mental State Examination (MMSE) (P = 0.21), while this study showed continuous improvement in the “Staying Cognitively Active” dimension through the dual intervention model (P < 0.01). There are three possible reasons: First, recall therapy constructs a structured recall framework based on six major themes. Compared with unstructured interviews, it can more systematically activate the episodic memory retrieval function of the prefrontal cortex and the memory integration function of the hippocampus;36 Secondly, while a previous study involving a 6-month multicomponent physical exercise program did not yield significant improvements in cognitive function, neuropsychiatric symptoms, or quality of life among older adults with major neurocognitive disorder,34 the present intervention differs in its emphasis on dynamic balance training. In our study, dynamic balance training accounted for 60% of the total program, placing greater demands on real-time spatial orientation and rhythm control, which may provide more targeted stimulation of executive function. This highlights the growing need for rehabilitation strategies that go beyond basic physical activity and address cognitive stimulation through coordinated and sensorimotor-intensive exercises. Thirdly, multi-sensory interactive cognitive tasks like finger exercises and paper-cutting are integrated into RT to stimulate movement, emotion, and cognition, enhancing positive thinking. A recent meta-analysis including 16 randomized controlled trials demonstrated that multisensory stimulation reduces neuropsychiatric symptoms and improves cognitive function, supporting its therapeutic value in older adults.37
Additionally, physical function improvements were more pronounced in the intervention group. This aligns with evidence from a Vivifrail-based 12-week multicomponent exercise program, which included balance training and was shown to significantly enhance gait, balance, and muscle strength in older adults with functional decline.35 Building on this evidence, our intervention integrated both static and dynamic balance elements to further target physical function. On the one hand, dynamic balance training in SDBT-RT strengthens core muscle reaction speed, maintaining physical stability and reducing fall risks during daily life and exercise for rural older adults. On the other hand, intermittent visual/auditory deprivation and perturbation tasks (eg, shoulder tapping) in sandbags activated cortical-cerebellar network co-regulation, optimizing movement execution and coordination, thus systematically improving older adults’ physical function.38 These adaptations enhance sensory-motor stimulation while increasing reliance on proprioceptive and vestibular inputs, mimicking realistic challenges common in rural settings.39 Given the high prevalence and serious consequences of falls among older adults, particularly in rural environments, such balance-focused interventions are crucial. Addressing fall risk through progressive postural control exercises directly supports physical resilience and long-term functional independence.
Interestingly, SDBT-RT significantly promoted “Social Participation” and “Having Social Relationships and Support”. Older adults’ social participation and interpersonal interactions reflect older adults’ level of societal engagement, encompassing aspects such as family and friend interactions, group activities, and volunteering.40 As part of the SDBT-RT intervention, rural older adults participated in community group activities at least once a week, including reminiscing (loved ones, events, objects, and living conditions), nature activities (eg, planting trees, trekking), and handicrafts (eg, knitting, paper-cutting, and dumpling-making), and volunteer activities, which promotes the integration and interaction between older adults and the social environment and help to build social networks.41 Strong Social Participation and good social relationships and support are positively interrelated, as older adults who gain social relationships and a sense of support from participation are more willing to engage in SDBT-RT, further stimulating increased social participation.
SDBT-RT significantly enhances “Practicing Self-Care and Self-Awareness”, possibly because balance training improves balance and muscle strength, reduces the risk of falls in daily life,13,35 and enhances self-awareness. This is consistent with recent evidence emphasizing the role of physical activity and rehabilitation-based strategies in building self-efficacy and reducing fall-related anxiety among aging adults.42 Meanwhile, RT oriented towards positive life promotes dual improvements in mental and physical health by awakening pleasant experiences, enhancing enthusiasm and confidence in life, and enabling the elderly to respond more positively to aging and participate in social activities. This is particularly important for rural empty-nest elders.43 “Practicing Self-Care and Self-Awareness” becomes an essential strategy for sustaining healthy aging and improving quality of life. Surprisingly, there was a statistically significant difference in the change in scores on Practicing Self-Care and Self-Awareness in the control group during the follow-up period (P < 0.05), This may be attributed to peer interaction and professional guidance within the control group’s group health education, which grew knowledge and confidence in practicing Self-Care and Self-Awareness.
“Accepting aging” means that the elderly can admit their aging process and the decline of functional ability. There was a statistically significant difference in this dimension in the SDBT-RT scheme (P < 0.05). This is consistent with the mechanism of Siverova et al.44 Recall therapy is based on Erikson’s theory and is targeted at the “self-integration - despair” stage of old age (>65 years old). It helps the elderly reshape the meaning of life through peer sharing and empathy. Balance training combines four static standing postures and four progressive dynamic gaits, which is in line with the cognitive ability and learning habits of rural elderly people. It has a moderate intensity, is easy to master, and reduces the fear of functional decline.45 In addition, a positive attitude towards aging, good cognitive and physical functions, and greater social participation and support can help the elderly reshape their sense of meaning and achievement in life and identify with a simple lifestyle.40 The scores of the intervention group in terms of “Being Self-Sufficient and Living Simply” improved significantly at all three time points.
It is worth noting that although the intervention group showed significant time improvement in “Making Merit and Good Deeds” (P < 0.05), there was not statistically significant (P > 0.05), indicating that the SDBT-RT program was not superior to the control group in this aspect. Although the “My Happy Time” module elicited positive emotions and the “Achievements in a Lifetime” module reinforced a sense of moral identity through recalling virtuous actions, these effects were not easily internalized into consistent prosocial behavior in daily life. However, the multifactorial nature of “Making Merit and Good Deeds” (eg, personality, social environment) requires targeted interventions or longer duration,46 which implies that in the future, the cultural appropriateness and duration of SDBT-RT to explore the sustained effects of long-term comprehensive interventions on “Making Merit and Good Deeds” in older adults. Furthermore, structured health education received by the control group resulted in higher scores on the “Making Merit and Good Deeds” dimension at all three-time points, highlighting the value of knowledge sharing and social interaction in improving this dimension.
However, the present study demonstrated that SDBT-RT significantly improved “Managing Stress” among rural older adults (P < 0.001), with sustained improvement. This was primarily due to its dual pathways of action. First, group reminiscence therapy promotes social empathy, a sense of belonging and emotional venting by sharing pleasant experiences and life stories.47 Second, Balance training offers learning and exercise opportunities, enhancing physical abilities while achieving a sense of accomplishment, boosting confidence and stress resistance.48 Exercise itself, as a means of emotion regulation, stimulates the release of neurotransmitters such as endorphins, alleviating anxiety and depression.49 Consequently, the SDBT-RT program can function as a viable stress management strategy for older adults in rural areas.
Interestingly, the SDBT-RT program showed high adherence (88.8%) and satisfaction with no adverse events among older adults in rural communities. This aligns with the findings of Belogianni et al,50 who posited that comprehensive interventions surpass repetitive exercise programs in sustaining motivation. The SDBT-RT program effectively leveraged core elements of the Theory of Planned Behavior to foster positive group dynamics and intrinsic motivation, thereby promoting long-term exercise habituation and significantly enhancing adherence.51 In terms of resources and costs, it is crucial to provide specific implementation guidance for rural communities. Considering the resource limitations in rural areas, the existing activity venues and volunteer resources in the community can be utilized to reduce the implementation cost. For instance, community activity centers can serve as intervention sites, and trained community workers and volunteers can assist in implementing intervention programs, reducing reliance on professionals. In addition, low-cost materials and equipment, such as sandbags and handcrafted materials, can be adopted to reduce costs.
Several limitations of this study should be acknowledged. First, the intervention intensity was only adjusted gradually and the training parameters were not standardized. Future studies should implement stepwise randomized trials (8/12/16 weeks) and determine the optimal intervention cycle through cost-benefit analysis. Second, explore gender stratified analysis. Women may benefit more from the emotional support of RT, while men tend to take on the physical challenges of SDBT. Explore the intervention adaptation plans for the frail subgroups (such as living alone and chronic pain). Third, the single-blinded design of the study limits the ability to fully control for observer bias, and the potential for measurement error exists due to self-reported data. Future studies should focus on personalized intervention plans for these subgroups and explore the dose-effect relationship between individualized training parameters and long-term health benefits.
Conclusion
This study demonstrated that the Theory of Planned Behavior–based SDBT-RT program effectively promoted healthy aging among older adults in a rural community and yielded sustained benefits over time. The intervention was feasible, cost-effective, achieved high adherence rates, and was well accepted by participants. These findings offer a valuable reference for the design and implementation of future programs and policies aimed at advancing healthy aging in rural populations, especially in resource-limited settings.
Data Sharing Statement
The data of this study will be made available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Consent to Participate
All work was conducted in accordance with the provisions of the Helsinki Declaration. Our study adheres to CONSORT guidelines. It has been approved by the Medical Ethics Committee of Huzhou University (approval number: 20220607) and registered on the Chinese Clinical Trial Registry (Registration ID: ChiCTR2300072132). All participants will sign informedconsents prior to their participation. During implementation, the physical training component was adapted from the originally registered Vivifrail program to a static-dynamic balance training protocol, based on feasibility and safety considerations in the rural setting. This adjustment did not affect the study objectives, outcome measures, or overall intervention structure.
Acknowledgments
Xinyu Yang, Shasha Li, and Lijun Xu are co-first authors for this study. We would like to thank all participants and community workers in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 72204084), the Key Research And Development Program Of Zhejiang Province (2025C02106), and Graduate Scientific Research Innovation Project of Huzhou University (YJK30086).
Disclosure
The authors declare no competing interests.
References
1. Dzau VJ, Inouye SK, Rowe JW, Finkelman E, Yamada T. Enabling healthful aging for all - the national academy of medicine grand challenge in healthy longevity. N Engl J Med. 2019;381(18):1699–1701. doi:10.1056/NEJMp1912298
2. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
3. Maurice J. WHO puts healthy ageing on the front burner. Lancet. 2016;387(10014):109–110. doi:10.1016/S0140-6736(15)01365-3
4. Xu L, Shi H, Shen M, et al. The effects of mhealth-based gamification interventions on participation in physical activity: systematic review. JMIR Mhealth Uhealth. 2022;10(2):e27794. doi:10.2196/27794
5. Jia L, Du Y, Chu L, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. 2020;5(12):e661–e671. doi:10.1016/S2468-2667(20)30185-7
6. Spanakis M, Xylouri I, Patelarou E, Patelarou A. A literature review of high-tech physiotherapy interventions in the elderly with neurological disorders. Int J Environ Res Public Health. 2022;19(15):9233. doi:10.3390/ijerph19159233
7. Li CW, Yao YT, Hu YD. Current status and intervention suggestions for mental health of Chinese elderly. Chin Med Herald. 2021;18(15):192–196. doi:10.37155/2717-5650-0405-4
8. Zhang Y, Hu W, Feng Z. Social isolation and health outcomes among older people in China. BMC Geriatr. 2021;21(1):721. doi:10.1186/s12877-021-02681-1
9. Shi H, Hu FB, Huang T, et al. Sedentary behaviors, light-intensity physical activity, and healthy aging. JAMA Network Open. 2024;7(6):e2416300. doi:10.1001/jamanetworkopen.2024.16300
10. Schietzel S, Chocano-Bedoya PO, Sadlon A, et al. Prevalence of healthy aging among community dwelling adults age 70 and older from five European countries. BMC Geriatr. 2022;22(1):174. doi:10.1186/s12877-022-02755-8
11. Beard JR, Officer A, de Carvalho IA, et al. The world report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387(10033):2145–2154. doi:10.1016/S0140-6736(15)00516-4
12. Robinson S, Granic A, Cruz-Jentoft AJ, Sayer AA. The role of nutrition in the prevention of sarcopenia. Am J Clin Nutr. 2023;118(5):852–864. doi:10.1016/j.ajcnut.2023.08.015
13. Gómez-Redondo P, Valenzuela PL, Morales JS, Ara I, Mañas A. Supervised versus unsupervised exercise for the improvement of physical function and well-being outcomes in older adults: a systematic review and meta-analysis of randomized controlled trials. Sports Med. 2024;54(7):1877–1906. doi:10.1007/s40279-024-02024-1
14. Ni Y, Li S, Lv X, et al. Efficacy of sensory-based static balance training on the balance ability, aging attitude, and perceived stress of older adults in the community: a randomized controlled trial. BMC Geriatr. 2024;24(1):49. doi:10.1186/s12877-023-04596-5
15. Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis [published correction appears in sports med. Sports Med. 2016;46(3):457. doi:10.1007/s40279-016-0500-6
16. Cui Z, Xiong J, Li Z, Yang C. Tai chi improves balance performance in healthy older adults: a systematic review and meta-analysis. Front Public Health. 2024;12:1443168. doi:10.3389/fpubh.2024.1443168
17. Gschwind YJ, Kressig RW, Lacroix A, Muehlbauer T, Pfenninger B, Granacher U. A best practice fall prevention exercise program to improve balance, strength / power, and psychosocial health in older adults: study protocol for a randomized controlled trial. BMC Geriatr. 2013;13(1):105. doi:10.1186/1471-2318-13-105
18. Temprado JJ, Torre MM. Are conventional combined training interventions and exergames two facets of the same coin to improve brain and cognition in healthy older adults? Data-based viewpoint. JMIR Serious Games. 2022;10(4):e38192. doi:10.2196/38192
19. Pu Y, Zhang G, You S, et al. Reminiscence therapy delivery formats for older adults with dementia or mild cognitive impairment: a systematic review and network meta-analysis. Int J Nurs Stud. 2025. doi:10.1016/j.ijnurstu.2025.105085
20. Gonzalez-Senac NM, Somoza-Fernandez G, Ocaña Ramirez E, et al. Effects of reminiscence therapy on anxiety and depression during acute hospitalization in older patients: controlled study. J Am Geriatr Soc. 2023;71(1):36–45. doi:10.1111/jgs.18063
21. Saragih ID, Tonapa SI, Yao CT, Saragih IS, Lee BO. Effects of reminiscence therapy in people with dementia: a systematic review and meta-analysis. J Psychiatr Ment Health Nurs. 2022;29(6):883–903. doi:10.1111/jpm.12830
22. Cho E, Shin J, Seok JW, et al. The effectiveness of non-pharmacological interventions using information and communication technologies for behavioral and psychological symptoms of dementia: a systematic review and meta-analysis. Int J Nurs Stud. 2023;138:104392. doi:10.1016/j.ijnurstu.2022.104392
23. Wu Y, Zhang X, Yu T, et al. Effects of reminiscence therapy combined with memory specificity training (RT-MeST) on depressive symptoms in older adults: a randomized controlled trial protocol. BMC Geriatr. 2023;23(1):398. doi:10.1186/s12877-023-03967-2
24. Banerjee A, Sadana R. Editorial: Integrated Care for Older People (ICOPE): from guidelines to demonstrating feasibility. J Frailty Aging. 2021;10(2):84–85. doi:10.14283/jfa.2020.40
25. Fife-Schaw C, Sheeran P, Norman P. Simulating behaviour change interventions based on the theory of planned behaviour: impacts on intention and action. Br J Soc Psychol. 2007;46(Pt 1):43–68. doi:10.1348/014466605X85906
26. Bosnjak M, Ajzen I, Schmidt P. The theory of planned behavior: selected recent advances and applications. Eur J Psychol. 2020;16(3):352–356. doi:10.5964/ejop.v16i3.3107
27. Sanaeinasab H, Saffari M, Dashtaki MA, et al. A theory of planned behavior-based program to increase physical activity in overweight/obese military personnel: a randomised controlled trial. Appl Psychol Health Well Being. 2020;12(1):101–124. doi:10.1111/aphw.12175
28. Ren Y, Tang R, Sun H, Li X. Intervention Effect of Group Reminiscence Therapy in Combination with Physical Exercise in Improving Spiritual Well-Being of the Elderly. Iran J Public Health. 2021; 50. 3. 531–539. doi:10.18502/ijph.v50i3.5594
29. Erikson EH. Identity: Youth and Crisis. WW Norton & company; 1994.
30. Thiamwong L, Maneesriwongul W, Malathum P, Jitapunkul S, Vorapongsathorn T, Stewart AL. Development and psychometric testing of the healthy aging instrument. Pac Rim Int J Nurs Res. 2008;12(4):285–296.
31. Wu F, Sheng Y. The Chinese version and evaluation of the reliability and validity of the healthy aging scale. Chin Nurs res. 2019;33(8):1293–1297.doi:10.12102/j.issn.1009–6493.2019.08.004.
32. Chen JH, Mohd Zain N, Yusuf A, Ying BH. Prevalence and associated factors of healthy aging among community-dwelling older adults in Lishui city, China: a cross-sectional study. BMC Public Health. 2025;25(1):184. doi:10.1186/s12889-025-21420-4
33. Polit D, Beck C. Essentials of nursing research: appraising evidence for nursing practice. In: Wolters Kluwer Health - Lippincott Williams & Wilkins.
34. Borges-Machado F, Teixeira L, Carvalho J, Ribeiro O. Does multicomponent physical exercise training work for dementia? Exploring the effects on cognition, neuropsychiatric symptoms, and quality of Life. J Geriatr Psychiatry Neurol. 2023;36(5):376–385. doi:10.1177/08919887221149152
35. Chen B, Li M, Zhao H, et al. Effect of multicomponent intervention on functional decline in Chinese older adults: a multicenter randomized clinical trial. J Nutr Health Aging. 2023;27(11):1063–1075. doi:10.1007/s12603-023-2031-9
36. Anderson MC, Floresco SB. Prefrontal-hippocampal interactions supporting the extinction of emotional memories: the retrieval stopping model. Neuropsychopharmacology. 2022;47(1):180–195. doi:10.1038/s41386-021-01131-1
37. Octary T, Fajarini M, Arifin H, et al. Multisensory stimulation reduces neuropsychiatric symptoms and enhances cognitive function in older adults with dementia: a meta-analysis of randomized controlled trials. J Prev Alzheimers Dis. 2025;12(5):100091. doi:10.1016/j.tjpad.2025.100091
38. Gerards M, Marcellis R, Senden R, et al. The effect of perturbation-based balance training on balance control and fear of falling in older adults: a single-blind randomised controlled trial. BMC Geriatr. 2023;23(1):305. doi:10.1186/s12877-023-03988-x
39. Behm DG, Muehlbauer T, Kibele A, Granacher U. Effects of strength training using unstable surfaces on strength, power and balance performance across the lifespan: a systematic review and meta-analysis. Sports Med. 2015;45(12):1645–1669. doi:10.1007/s40279-015-0384-x
40. Duppen D, Lambotte D, Dury S, et al. Social participation in the daily lives of frail older adults: types of participation and influencing factors. J Gerontol B Psychol Sci Soc Sci. 2020;75(9):2062–2071. doi:10.1093/geronb/gbz045
41. Luxton D, Thorpe N, Crane E, et al. Systematic review of the efficacy of pharmacological and non-pharmacological interventions for improving quality of life of people with dementia. Br J Psychiatry. 2025:1–13. doi:10.1192/bjp.2025.11
42. Arkkukangas M, Bååthe KS, Hamilton J, Hassan A, Tonkonogi M. FallFitness exercise program provided using the train-the-trainer approach for community-dwelling older adults: a randomized controlled trial. BMC Geriatr. 2024;24(1):983. doi:10.1186/s12877-024-05575-0
43. Jia Y, Yue Y, Sheng Y. The mediating role of aging attitudes between social isolation and self-neglect: a cross-sectional study of older adults living alone in rural China. BMC Nurs. 2025;24(1):4. doi:10.1186/s12912-024-02637-x
44. Siverová J, Bužgová R. The effect of reminiscence therapy on quality of life, attitudes to ageing, and depressive symptoms in institutionalized elderly adults with cognitive impairment: a quasi-experimental study. Int J Ment Health Nurs. 2018;27(5):1430–1439. doi:10.1111/inm.12442
45. Tsai JL, Sims T, Qu Y, Thomas E, Jiang D, Fung HH. Valuing excitement makes people look forward to old age less and dread it more. Psychol Aging. 2018;33(7):975–992. doi:10.1037/pag0000295
46. Butovskaya M, Marczak M, Misiak M, Karelin D, Białek M, Sorokowski P. Approach to resource management and physical strength predict differences in helping: evidence from two small-scale societies. Front Psychol. 2020;11:373. doi:10.3389/fpsyg.2020.00373
47. Li S, Dai Y, Zhou Y, Zhang J, Zhou C. Efficacy of group reminiscence therapy based on Chinese traditional festival activities (CTFA-GRT) on loneliness and perceived stress of rural older adults living alone in China: a randomized controlled trial. Aging Mental Health. 2022;26(7):1377–1384. doi:10.1080/13607863.2021.1935457
48. Hernandez-Martinez J, Cid-Calfucura I, Chiguay C, et al. Effects of elastic band training on body composition and physical performance in older people: a systematic review with meta-analysis. Exp Gerontol. 2024;196:112553. doi:10.1016/j.exger.2024.112553
49. Zhang XY, Wu WX, Shen LP, et al. A role for the cerebellum in motor-triggered alleviation of anxiety. Neuron. 2024;112(7):1165–1181.e8. doi:10.1016/j.neuron.2024.01.007
50. Belogianni K, Baldwin C. Types of interventions targeting dietary, physical activity, and weight-related outcomes among university students: a systematic review of systematic reviews. Adv Nutr. 2019;10(5):848–863. doi:10.1093/advances/nmz027
51. André N, Grousset M, Audiffren M. A behavioral perspective for improving exercise adherence. Sports Med Open. 2024;10(1):56. doi:10.1186/s40798-024-00714-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.