Back to Journals » International Journal of Women's Health » Volume 15
Effectiveness of Training Program on Improving Health Care Providers’ Readiness for Managing Domestic Violence in Jimma Medical Center: Pre-Experimental Study
Authors Negessa EH, Joseph SA ![]() , Kitaba KA
, Kitaba KA ![]() , Negesa MG
, Negesa MG ![]()
Received 10 September 2022
Accepted for publication 12 January 2023
Published 17 January 2023 Volume 2023:15 Pages 71—77
DOI https://doi.org/10.2147/IJWH.S389433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Endalew Hailu Negessa,1 Susan Anand Joseph,1 Kebenesa Angasu Kitaba,2 Melkamu Gelan Negesa2
1Department of Nursing, Jimma University, Jimma, Ethiopia; 2Department of Midwifery, Jimma University, Jimma, Ethiopia
Correspondence: Kebenesa Angasu Kitaba, Jimma University Main Campus, PO Box: 378, Tel +251919841766, Email [email protected]
Background: Domestic violence (DV) is a pervasive human-right violation and is an impediment to the achievement of Sustainable Development Goals by 2030. Although they may not often disclose their violence, survivors of DV are most likely to be treated by health care providers. Thus, this study aimed to assess the effectiveness of training intervention in improving the readiness of health care providers for managing domestic violence in Jimma Medical Center.
Methods: Pre-experimental study design was undertaken among 64 health care providers of Jimma Medical Center on two rounds from March 16 to 19 and from May 18 to 21/2022. Data were collected by using a structured self-administered questionnaire and entered into Epi-data version 4.6 and exported to SPSS version 23 for analysis. To test the difference in the participants’ readiness to manage DV in terms of knowledge and attitude; a Paired-samples t-test analysis was done at 95%-confidence-interval and p-value < 0.05. To quantify the magnitude of the intervention’s effect, Eta-squared was computed as an effect size statistic.
Results: The overall knowledge score was improved from pre-intervention (M= 12.44, SD=4.55) to post-intervention (M=15.66, SD= 5.48, t(4.29), p< 0.0005). The overall attitude score was improved from pre-intervention (M= 156.4, SD= 15.68) to post-intervention (M=169.1, SD=20.67, t(3.8), p< 0.0005). The Eta-squared value for the knowledge was 0.23 and for the attitude was 0.19 both indicating a large effect size.
Conclusion: Significant improvement in the study participants’ readiness for managing DV was a result in this study with a large effect size. Thus, different concerned stakeholders should provide training intervention for health care providers of Jimma Medical center to improve their readiness to manage survivors of domestic violence thereby contributing to the reduction of the negative consequences that can be resulted from poor management of domestic violence.
Keywords: domestic violence, Jimma Medical Center, pre-experimental study
A Letter to the Editor has been published for this article.
Introduction
Worth of any civilization can be judged from the position it gives to women.1 The Judeo-Christian cultural beliefs, Greek philosophy, and the western legal code are the three major propagators of the patriarchal society where expression of male superiority has become manifested in the form of violence towards women.2 Domestic violence or intimate partner violence has been defined by World Health Organization (WHO) as “behavior by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviors”.3 Anyone could be a victim and it is all-pervasive irrespective of race, age, sexual orientation, religion, or gender.3
Women, especially the young and pregnant, are at high risk of DV.4 World Health Organization estimated that globally 30% of women had been physically or sexually abused mostly by an intimate partner.5 In Ethiopia, 34.1% of reproductive-age women ever experienced physical, sexual, and/or emotional abuse,6 while 20% of the ever-married women experienced physical and/or sexual violence within a year.7
Domestic violence, which is a social evil, negatively impacts psychological, physical health, and lowers the quality of life and productivity, results in mortality, is largely concealed and difficult to identify. But almost every healthcare professional is likely to provide care for a patient who has survived a DV.8 The existing evidence indicates that even though healthcare providers’ positive interaction with the survivors of DV can result in the survivors’ increased safety, support, and self-efficacy; screening rates for DV are low among most health care providers.9 The readiness of health professionals to diagnose and manage DV determines the success of care given to the survivors.10 Thus, committing to addressing DV cases; being advocator for the survivors; establishing a trustful professional relationships with survivors; collaborating with the health care team; and being supported by the health system enhances the readiness of healthcare providers for screening and managing DV.11
A study conducted in the United Kingdom indicated that lack of training leads to the reluctance of health care providers to screen women for DV.12 In contrast, another study pointed out that educational intervention improves clinicians’ readiness for managing domestic violence.13 But since such a study was not conducted in the Ethiopian context, this study aimed to assess the effectiveness of training intervention on improving readiness for managing domestic violence among healthcare providers of Jimma Medical Center. Thus, it is believed that this study had dual benefits concerning updating the study participants’ competence for managing domestic violence and revealing the effectiveness of the training intervention in improving the readiness of the respondents for managing domestic violence.
Methods and Materials
Study Area, Design, and Period
This study was conducted among front-line health care providers (medical doctors, nurses, and midwives) and social workers of Jimma Medical Center (JMC). JMC is the only tertiary hospital in the southwest part of Ethiopia serving more than 15 million people in its catchment area. The hospital had 64 medical doctors (general practitioners), 671 nurses, 76 midwives, 26 social workers and other health professionals such as pharmacists, laboratory technicians, radiologists, and others. Also, since the hospital serves as the teaching hospital for Jimma University, specialist doctors from different departments of the university serve the hospital. Pre-experimental (single group pre and post-training intervention test) study design was used to undertake this study from March 16 to 19 and May 18 to 21/2022.
Study Population
The study population was the front-line healthcare providers of JMC who are directly involved in the healthcare provision for the survivors of domestic violence including medical doctors (general practitioners), nurses, midwives, and social workers of JMC.
Inclusion and Exclusion Criteria
The inclusion criteria were being frontline health care providers in JMC and getting deployment from the service director of their respective unit head.
Sample Size Determination and Sampling Techniques
The sample size was determined by taking the study design’s minimum required sample size which is greater than or equal to 30 participants and the resource we had to undertake the training intervention we gave for the study participants. Thus, we gave training to 32 participants in two rounds for a total of 64 participants.
Data Collection Tool and Methods
The data were collected through a self-administered structured validated questionnaire named “Physician Readiness to Manage Intimate Partner Violence Survey (PREMIS)” adapted from literature.14 The data were collected both before starting the training and after finishing the training. The data collectors were two MSc holder midwifery educators at Jimma University. The training intervention was focused on the concepts of DV, how to screen the survivors of DV, clinical response for survivors of DV, psychosocial support, and a multi-sectorial approach for managing DV. Thus, we gave four days of training to the health care providers of JMC with the hope that the training intervention can result in the improvement of the study participants’ knowledge and attitude toward the management of DV. The training was provided by five specialist doctors who had training trainer certificates in the area of domestic violence. The training manual was a standardized manual prepared by the Ethiopian Federal Ministry of Health.
Operational Definition
Knowledge of Domestic Violence Management
The respondents’ knowledge of management of domestic violence was measured by thirty-eight items that include multiple choice and true/false items with only one correct answer. The correct response was coded “1” and the incorrect response was coded “0”. Then the total knowledge score was summed up giving rise to the maximum possible score equal to 38 and the minimum possible score of 0. Finally, the mean score was used to compare the results of pre-intervention with the result obtained after the intervention.
Attitude Towards Domestic Violence Management
The respondents’ attitude towards management of domestic violence was measured by thirty-two seven points Likert scale items. The negatively constructed items were recoded and finally, the responses of the respondents were summed up giving rise to 224 as the maximum possible score and 32 as the minimum possible score. Finally, the mean score was used to compare the results of pre-intervention with the result obtained after the intervention.
Data Analysis and Presentation
Data entered into Epi-data software version 4.6 was transported to SPSS version 23 for analysis. Paired sample t-test was used to see the mean difference in the mean score of the study participants’ knowledge and attitude toward managing domestic violence. P-value less than 0.05 was used to ascertain the statistical significance and eta squared was used to show the effect size of the intervention on the mean score of the study participants’ knowledge and attitude towards managing survivors of domestic violence.
Data Quality Control
To assure the quality of the data, we used a standardized tool for data collection. The data collectors have experienced personnel in data collection and had one day training on the data collection tool, the content of the questionnaire, and the way to approach the study participants. Moreover, to minimize encountering an error during data entry, we used Epi-data software version 4.6 with its check-file. Finally, the analysis was done by SPSS version 23.
Ethical Consideration
This study was done as per the declaration of Helsinki. Ethical approval was obtained from the institutional review board of the Institute of Health, Jimma University. Written informed consent was taken from each study participant. The anonymity and confidentiality of the collected data were assured by using the data for this research purpose only.
Results
Socio-Demographic Characteristics
The response rate for this study was 100% (64 participants). Three-fourths 48 (75%) of the respondents were less than or equal to thirty years old while the median age was 28 years. More than three-fourths 49 (76.6%) of the respondents were married. Also, a higher proportion 52 (81.2%) of the respondents were Bachelor of Science degree holders. Less than half 30 (46.8%) of the respondents were nurse professionals. Moreover, around one-fourth 17 (26.6%) of the respondents have been working in the maternity and gynecology ward. In addition, just less than two-thirds 41 (64.1%) of the respondents had two to five years of working experience. Lastly, around three-fourths of the respondents had 5000–9000 Ethiopian birr monthly income (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Health Care Providers of Jimma Medical Center, 2022, (n=64) |
The Knowledge and Attitude Improvement
The paired sample t-test analysis result revealed that the overall knowledge score was improved from pre-intervention (M= 12.44, SD=4.55) to post-intervention (M=15.66, SD= 5.48, t(4.29), at p<0.0005). The overall attitude score was improved from pre-intervention (M= 156.4, SD= 15.68) to post-intervention (M=169.1, SD=20.67, t(3.8), at p<0.0005). The eta squared value for the knowledge was 0.23 and for the attitude was 0.19 both indicating a large effect size (Tables 2 and 3). This means that provision of in-service training can better result in health care providers’ knowledge and attitude improvement thereby leading to improved detection, diagnosis and management of domestic violence which is at very minimal stage at the current level.
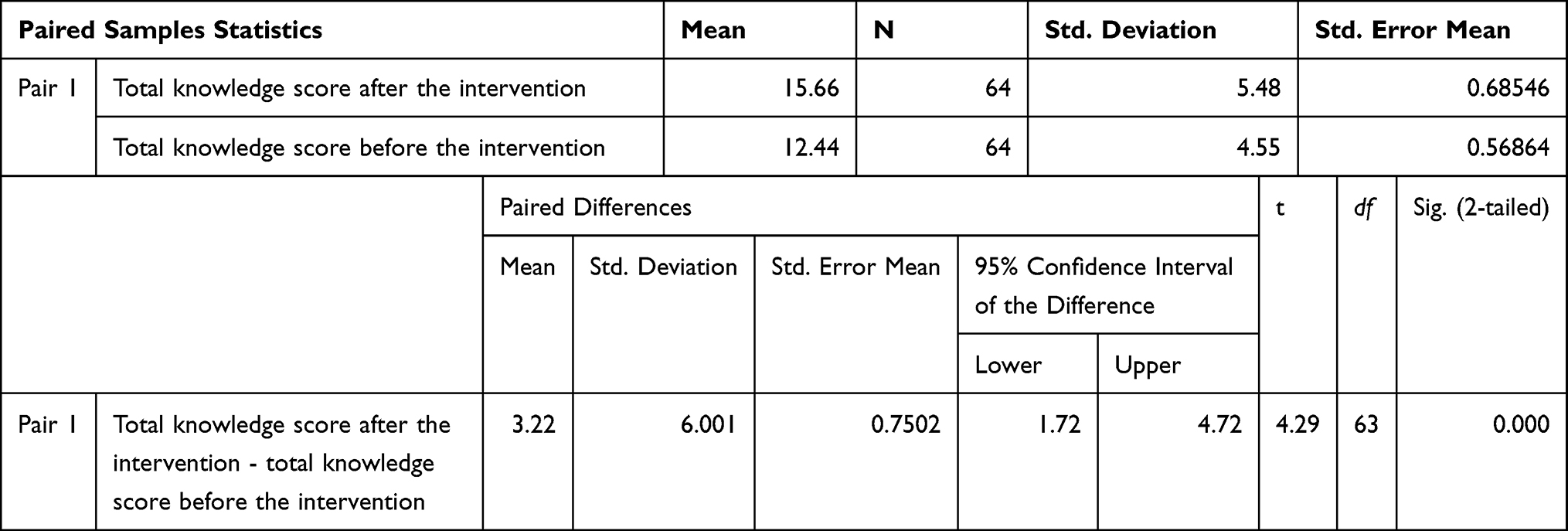 |
Table 2 The Paired Sample t-test Output Shows the Mean Difference in the Overall Knowledge Toward Domestic Violence Management Before and After Four Days of Training Intervention Among Frontline Health Care Providers of JMC, 2022, (n=64) |
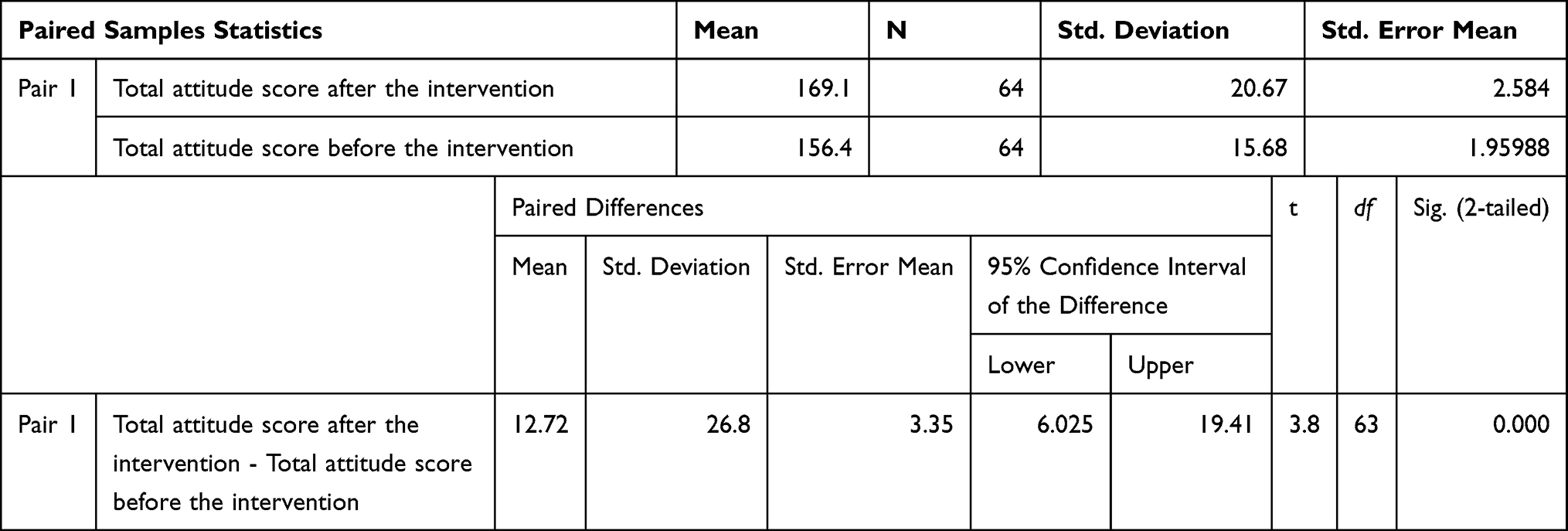 |
Table 3 The Paired Sample t-test Output Shows the Mean Difference in the Overall Attitude Toward Domestic Violence Management Before and After Four Days of Training Intervention Among Frontline Health Care Providers of JMC, 2022, (n=64) |
Discussion
The objective of this study was to assess the effectiveness of training intervention on improving readiness for managing domestic violence among health care providers of Jimma Medical Center. As a result, the training intervention resulted in a significant improvement in the knowledge and attitude of the study participants.
The finding of this study is in line with the result of a study done in the west side of Chicago where educational intervention resulted in better improvement in health care providers’ readiness for identifying and managing DV.13 Also, the finding of the current study is in line with the result of a systematic review study conducted in 2021 where training intervention resulted in an improvement in the knowledge and attitude of health care providers towards screening and management of DV.10 The possible reason behind the consistency of the results of the studies can be the fact that training/educational intervention leads to a better understanding of the areas of concern and that will lead to the improvement in the healthcare provider’s knowledge and attitude thereby improving their commitment for solving the existing problems leading into improving the effectiveness of their work.
The implication behind this study is that relevant stakeholders including non-government organizations should help the JMC by providing training for all of its health care providers to improve their readiness to manage DV which is a very devastating and prevalent problem in Ethiopia as well as the world. Also, the training interventions can have multiple improvement effects refreshing and improving the commitment of health care professionals as it provides the opportunity by which they can share their experience with their colleagues and relevant others.11
Strength and Limitation
This study was conducted by using practical intervention on the issue of global concern that contributes to effective improvement for the achievement of Sustainable Development Goals in terms of women empowerment. Also, this study paves the way for concerned stakeholders to undertake training intervention by revealing the effectiveness of training intervention in improving the health care providers’ readiness to manage DV. Also, since there is a lack of published studies with the same title in Ethiopia, this study contributes to filling the existing literature gap in the Ethiopian context. The possible limitation of this study can be attributed to the nature of the study design that it lacks a comparative group. So, it is better if the future study is done by using a randomized controlled trial on the same topic to result in more robust findings.
Conclusions
This study revealed that four days of training intervention resulted in significant improvement of the study participants’ knowledge and attitude toward managing domestic violence with a large effect size. So, different concerned stakeholders should provide training intervention for health care providers of Jimma Medical Center to improve their readiness to manage domestic violence thereby contributing to better health care provision for the survivors of domestic violence.
Abbreviations
DV, Domestic Violence; JMC, Jimma Medical Center; SPSS, Statistical Package for Social Science.
Acknowledgments
We would like to express our heartfelt acknowledgment to the funder of this research and to our data collectors. Also, we acknowledge our study participants for providing their genuine responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The fund to undertake this study was given to us by the Jimma University Institute of Health Research and Innovation director’s office. But the fund they gave us was only for data collection and for the logistics required for providing the training intervention. Otherwise, the funder has no contribution to any aspect of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sumitra M. 131st Assembly of the Inter-Parliamentary Union (IPU) in Geneva on ‘Achieving Gender Equality, Ending Violence Against Women’, Geneva (Switzerland), 13 October, 2014. 2014.
2. Fox VC. Historical perspectives on violence against women. J Int Womens Stud. 2002;4(1):15–34.
3. WHO. Addressing violence against women in health and multisectoral policies: a global status report; 2021. Available from: https://www.who.int/publications/i/item/9789240040458.
4. Welfare. AIoHa. Family, Domestic and Sexual Violence in Australia 2018.Cat. No. FDV 2. Canberra: AIHW; 2018.
5. WHO. COVID-19 and violence against women: what the health sector/system can do? Available from: https://apps.who.int/iris/handle/10665/331699.
6. Tiruye TY, Harris ML, Chojenta C, Holliday E, Loxton D. Determinants of intimate partner violence against women in Ethiopia: a multi-level analysis. PLoS One. 2020;15(4):e0232217. doi:10.1371/journal.pone.0232217
7. ICF. CSACEa. Ethiopia demographic and health survey 2016: key indicators report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.
8. World Health Organization. Strengthening the health system response to violence against women in Uganda: lessons learned from adapting and implementing WHO guidelines and tools. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO. Available from: 9789240010543-eng.pdf.
9. Renner LM, Wang Q, Logeais ME, Clark CJ. Health care providers’ readiness to identify and respond to intimate partner violence. J Interpers Violence. 2021;36(19–20):9507–9534. doi:10.1177/0886260519867705
10. Kalra N, Hooker L, Reisenhofer S, Di Tanna GL, García-Moreno C. Training healthcare providers to respond to intimate partner violence against women. Cochrane Database Syst Rev. 2021;5(5):CD012423. doi:10.1002/14651858.CD012423.pub2
11. Hegarty K, McKibbin G, Hameed M, et al. Health practitioners’ readiness to address domestic violence and abuse: a qualitative meta-synthesis. PLoS One. 2020;15(6):e0234067. doi:10.1371/journal.pone.0234067
12. Ramsay J, Rutterford C, Gregory A, et al. Domestic violence: knowledge, attitudes, and clinical practice of selected UK primary healthcare clinicians. Br J General Pract. 2012;62(602):e647–55. doi:10.3399/bjgp12X654623
13. Martin-Engel L, Allen J, Alencar A, et al. Improving readiness to manage intimate partner violence in family medicine clinics by collaboration with a community organization. PRiMER. 2021;5:20. doi:10.22454/PRiMER.2021.717020
14. Lynn MEA, Harris JM, Zita J, Surprenant ZJ. A tool for measuring physician readiness to manage intimate partner violence. Am J Prev Med. 2006;30(2):173–180. doi:10.1016/j.amepre.2005.10.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.