Back to Journals » Substance Abuse and Rehabilitation » Volume 17
Effectiveness of the Functional-Cognitive and Sensory Treatment for Improving Daily Functioning of Individuals with Substance Use Disorder: A Randomized Controlled Trial
Authors Assayag N, Bachar Kirshenboim Y ![]() , Nemesh-Godin T, Zaude R, Rand D
, Nemesh-Godin T, Zaude R, Rand D ![]() , Bar Shalita T
, Bar Shalita T
Received 12 February 2026
Accepted for publication 5 May 2026
Published 3 June 2026 Volume 2026:17 598565
DOI https://doi.org/10.2147/SAR.S598565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Naama Assayag,1,* Yishai Bachar Kirshenboim,2,* Tom Nemesh-Godin,2 Raaya Zaude,2 Debbie Rand,2,3 Tami Bar Shalita2
1Department of Occupational Therapy, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel; 2Department of Occupational Therapy, School of Health Professions, Gray Faculty of Medical and Health Sciences, Tel-Aviv University, Tel-Aviv, Israel; 3Herczeg Institute on Aging, Tel Aviv University, Tel-Aviv, Israel
*These authors contributed equally to this work
Correspondence: Tami Bar Shalita, Department of Occupational Therapy, School of Health Professions and Gray Faculty of Medical and Health Sciences, Tel-Aviv University, Tel-Aviv, Israel, Tel +972-525437631, Fax +972-3-6409933, Email [email protected]
Purpose: To examine the effectiveness of the Functional-Cognitive and Sensory Treatment (F-CaST) for individuals with Substance Use Disorder (SUD), in supporting daily functioning and reducing dropout from the therapeutic community.
Patients and Methods: A single-blind randomized controlled trial was conducted in a therapeutic community. Participants were randomly allocated to either the F-CaST group or a control group receiving standard care. The F-CaST consisted of 16 sessions (eight group and eight individual sessions) delivered over eight weeks and focused on teaching strategies individually tailored for executive function deficits and sensory modulation dysfunction linked to participants’ personal occupational goals. Assessments were conducted at pre (T1), immediately post-intervention (T2), and at 1- and 3-month follow-ups (T3–T4). Primary outcomes included occupational performance and satisfaction measured by the Canadian Occupational Performance Measure (COPM), dropout rates, and length of stay in the therapeutic community.
Results: Thirty-three participants were randomized to F-CaST (n=20) or standard care (n=13). Both groups demonstrated significant improvements in COPM performance and satisfaction over time; however, the F-CaST group showed a more favorable pattern of improvement and higher rates of clinically meaningful change (72% vs. 39% at 3 months). Dropout rates were significantly lower in the F-CaST group at T2 (22% vs. 62%). No significant between-group differences were found in length of stay.
Conclusion: F-CaST appears to be a feasible and promising intervention that may support improvements in occupational performance, satisfaction, and early treatment retention among individuals with SUD in therapeutic communities.
Keywords: executive function, sensory processing, occupational performance, therapeutic community
Introduction
Rehabilitation of individuals with substance use disorder (SUD) is a complex and prolonged process that requires substantial personal and community resources,1 yet treatment outcomes remain modest. High rates of relapse and premature treatment discontinuation persist across rehabilitation settings,2–4 highlighting a gap between the extensive resources invested and the functional outcomes achieved.1,5 This gap underscores the need for more effective interventions that support sustained engagement and daily functioning beyond abstinence alone.6,7 SUD is defined as a chronic, relapsing pattern of substance use despite harmful consequences, leading to impairments in interpersonal, social, and occupational functioning, and characterized by a cluster of cognitive, behavioral, and physiological symptoms.8 Most alarmingly, SUD has emerged as a major global public health concern with recent reports indicating a worldwide increase in substance use, projected to rise by 43% by 2030.9 Nearly 49 million individuals in the United States aged 12 years and older, representing approximately 17% of the population, met diagnostic criteria for SUD in the past year.10 Therapeutic communities (TC) are a central treatment modality, offering drug-free residential settings based on a hierarchical model that emphasizes mutual self-help and promotes the gradual assumption of personal and social responsibility. Nevertheless, dropout rates remain high, with studies indicating that 20% to 70% of participants disengage before completion, and only about one-third successfully complete the program.2–4,11
Reports indicate that the low rate of intervention success is coupled with cognitive impairments often exhibited in this population,12 particularly in attention, memory, and executive function (EF).13,14 EF is an umbrella term referring to a set of interrelated abilities, including planning, inhibitory control, decision-making, and self-regulation, that are essential for adaptive functioning, persistence, and quality of life15–17 and associated with poorer treatment adherence, increased risk of dropout, and reduced rehabilitation success.12 High prevalence rates of EF impairments have been reported among individuals with SUD, affecting approximately 53–70% of the SUD population.12
Sensory modulation dysfunction (SMD) is linked to EF18–20 yet has been only scantily reported in SUD.21–23 SMD severely reduces daily-life participation, adaptation to life challenges, and quality of life,21,24–27 and may also contribute to the high dropout rate. Specifically, we previously found that 54% of individuals with SUD residing in a TC demonstrated co-occurring SMD, compared to only 12.7% in the general population.21 SMD, a neurodevelopmental condition, challenges the ability to grade and adapt the intensity and type of response to stimuli in one or more sensory modalities.28,29 In SUD it is mostly expressed as sensory over-responsiveness, behaviorally manifested as atypical negative responses to apparently innocuous sensory stimuli (eg., sounds, food textures, or clothing).21,30
Despite the high prevalence and clinical relevance of EF and sensory modulation difficulties in SUD impacting day-to-day living, interventions targeting both domains in therapeutic community settings remain lacking. Given the reported low intervention success along impaired EF and sensory modulation, the Functional-Cognitive and Sensory Treatment (F-CaST) was developed30 to improve occupational performance in daily tasks within TCs and reduce dropout rates. This intervention uniquely integrates strategies to address impairments in EF as well as sensory modulation. This study aimed to examine the effectiveness of the F-CaST compared to a control group to (1) improve occupational performance in daily tasks within a TC and (2) reduce dropout rates from the TC. We hypothesized that participants receiving the F-CaST would demonstrate greater improvements in occupational performance and satisfaction, as well as lower dropout rates, compared to the control group.
Materials and Methods
Study Design
A single-blind randomized controlled trial (RCT) was employed, comprising experimental and control groups, with assessments pre (T1) and post (T2) the F-CaST intervention, as well as follow-up at 1 (T3) and 3 (T4) months post T2, utilizing assessors (experienced occupational therapists) blind to group allocation. This trial followed the Consolidated Standards for Reporting Trials (CONSORT) statement for Randomized Trials31,32 and was registered at ClinicalTrials.gov (NCT05647863; study start date November 2022; end date December 2023). The study was approved by the University Ethics Committee of Tel Aviv University, Israel (Approval No. 0001484–5). Authorization to conduct the study was obtained from the Ministry of Welfare, Israel. All procedures were conducted in accordance with the Declaration of Helsinki and all participants provided written informed consent before their participation.
Participants
Participants were recruited from a men’s-only unit within the TC. Inclusion criteria were aged 18–45 years, with adequate language skills, abstained from substance use for at least 21 days (to minimize withdrawal effects), and had resided in the TC for no more than 21 days (ensuring initial adjustment to the facility’s framework). Exclusion criteria stipulated dual psychiatric diagnosis, other neurological conditions, or significant cognitive impairment [scoring<19 points on the Montreal Cognitive Assessment (MoCA)].33
Randomization
Given the high prevalence of attention deficit hyperactivity disorder (ADHD) in the SUD population and its potential impact on intervention compliance,34 this factor was controlled for in the randomization process. Following the pre-assessment (T1) and based on the Adult ADHD Self-Report Scale-Version 1.1 (ASRS),35,36 participants were stratified by ADHD status (Yes/No). Subsequently, participants were randomly allocated, using a simple block randomization method (block size = 4) with a 1:1 ratio, to either the experimental group (F-CaST) or the control group (standard care) by an independent researcher not involved in the intervention or the assessments. Allocation concealment was maintained, and participants were informed of their group assignment by a research assistant who did not take part in the assessments or intervention delivery.
Screening Tools
Montreal Cognitive Assessment (MoCA)33 is a brief, standardized, and validated screening tool for mild cognitive impairment (MCI). It includes 11 tasks assessing attention, visuospatial ability, executive function, language, memory, abstraction, and orientation. Score ranges between 0–30, with scores ≥26 indicating intact cognition. The MoCA has demonstrated strong reliability and validity33 and has been shown to be effective in populations with substance use disorders.37 In this study, a MoCA score above 19 was used as an inclusion criterion.
Adult Attention-Deficit/Hyperactivity Disorder (ADHD) Self-Report Scale (ASRS)38 is a standardized, reliable, and valid self-report screening tool developed with the World Health Organization (WHO) to identify suspected ADHD in adults.35,36 In the current study, only the six-item screener section was used, scored on a 5-point Likert scale (0 = never to 4 = very often), with a total score of ≥4 indicating a positive screen (yes for ADHD). The ASRS screener has demonstrated good sensitivity and specificity in individuals with substance use disorders.39
Outcome Measures
Primary Outcome Measures
Occupational Performance was assessed using the Canadian Occupational Performance Measure (COPM):40,41 Participants identified three personal occupational goals and rated performance and satisfaction on a 10-point scale. The same goals were rated at all four time-points and at each time-point were averaged for performance (0–10) and satisfaction (0–10) scales. A change of ≥2 points in performance scores is considered a minimal clinically important difference (MCID).42
Length of stay in therapeutic community (TC): Was determined by the total number of days until discharge or dropout. Dropout was defined as leaving the TC before completing the minimum rehabilitation period without formal discharge.
Secondary Outcome Measures
TC Performance was assessed using a 4-item questionnaire developed specifically for this study by the professional team at the TC, to reflect functioning within the TC. It was completed by the instructors (eg., “To what extent does the resident complete his required chores?”). The questions were rated on a scale from 1 (no difficulty) to 5 (great difficulty), and an average score of the four-items was calculated. A lower score indicates better functioning.
Session attendance in standard TC groups: Throughout the study, instructors systematically recorded participants’ late arrivals to daily scheduled treatment and group sessions. For each participant, the number of late arrivals was calculated; lower values indicate better punctuality.
Population Characterization
Color Trails Test (CTT)43 is a brief paper and pencil neuropsychological assessment to assess EF, specifically attention, speed processing and cognitive flexibility. Participants are instructed to draw a line in the correct order between colored numbers scattered on a page (1, 2, 3, 4) (Part A) and alternating between numbers in pink and yellow circles (1-yellow, 2-pink, 3-yellow, 4-pink) (Part B). Completion time for each part is recorded and compared to normative data using T-scores; higher scores indicate better EFs.
Behavior Rating Inventory of Executive Function–Adult Version (BRIEF-A).44 A 75-item self-report questionnaire assessing executive function in everyday life over the past 30 days. Items are rated on a three-point scale (1 = never, 2 = sometimes, 3 = always), and from nine subscales that yield two main indices: Behavior Regulation Index (BRI: Inhibit, Emotional Control, Self-Monitor, Shift) and the Metacognitive Index (MI: Initiate, Working Memory, Task Monitor, Organization/Planning) as well as an overall Global Executive Composite (GEC). Raw scores are converted to standard scores, with higher scores indicating greater executive dysfunction; scores ≥ 65 indicate clinical impairment. The BRIEF-A demonstrates high internal consistency (α = 0.93–0.94) and test–retest reliability (r = 0.93–0.96) for the three main indices,44 and is sensitive among individuals with SUD.45
The Sensory Responsiveness Questionnaire – Intensity Scale (SRQ-IS).46 A self-report questionnaire used to identify SMD based on cutoff scores for sensory over-responsiveness and under-responsiveness. The questionnaire consists of 58 items representing typical everyday situations, each involving stimulation in a single sensory modality and referring either to enjoyment or disturbance. The degree of enjoyment or disturbance is rated on a Likert scale ranging from (1) “not at all” to (5) “very much.” The questionnaire yields two final scores, which are the mean ratings (1–5). SMD was defined using established normative cutoff scores for the Sensory Responsiveness Questionnaire (SRQ). Cutoff values corresponding to two standard deviations above normative means were ≥2.76 for the Hedonic subscale and ≥2.39 for the Aversive subscale. The instrument has content and construct validity, high internal consistency (Cronbach’s α = 0.90–0.93), and test–retest reliability (r = 0.71–0.84, p = 0.001–0.005).46
Demographic and clinical information was collected at T1, including age, years of education, and SUD history.
Intervention
Both study groups received the standard care provided at the TC. In addition, the F-CaST (experimental) group received an intervention program delivered over eight weeks; each group session lasted 45 minutes, followed by an individual session. A licensed occupational therapist, trained to administer the F-CaST, led the group and individual sessions.
The group sessions were psychoeducational, focusing on the provision of theoretical knowledge regarding executive function and sensory modulation. The sessions addressed the influence of these domains on daily functioning in general and on the participants’ daily lives within the TC. Sessions incorporated structured discussions, experiential activities, and gamified simulations of everyday situations requiring sensory modulation and executive functioning.
The individual sessions focused on each participant’s sensory–executive profile and its implications for daily functioning within the TC. Based on the personal goals (COPM goals identified at T1), and together with the occupational therapist, conducted task analyses, identified specific difficulties, and selected appropriate cognitive and sensory strategies to improve performance of their personal occupational goals (eg., strategies related to planning, initiation, response inhibition, arousal regulation, and self-direction). Therapists guided participants in applying cognitive and sensory strategies to enhance functioning.
The intervention emphasized the use of personas (descriptions of other people with SUD with similar difficulties) with high or low self-efficacy to promote insight and reflection, as well as to strengthen self-efficacy.47 Each participant practiced implementing strategies in relation to their individual goals, with repetition and generalization to various real-life situations within the TC. More details regarding the intervention structure and rationale are available in the protocol for a RCT.30
Participants in the control group received the standard therapeutic community program, which includes structured daily routines, group-based activities, and ongoing staff support, but did not receive any additional individualized or structured occupational therapy intervention.
Statistical Analysis
All data were analyzed using IBM SPSS Statistics (v27). Descriptive statistics were used to summarize demographic, executive function, sensory modulation, and other baseline characteristics. Categorical baseline variables, including the presence of sensory modulation dysfunction (yes/no) based on established SRQ-IS cutoff scores and ASRS (yes/no for ADHD), were compared between groups using Fisher’s exact test. Non-parametric tests were used due to the small sample size and distributional characteristics of the data. Within-group differences across the four time points (T1–T4) in COPM performance and satisfaction, TC performance, and Session attendance were examined using Friedman tests followed by Wilcoxon signed-rank tests to assess pairwise comparisons between T1-T2, T1-T3 and T1-T4. Between-group differences (F-CaST vs. control) in COPM performance and satisfaction, TC performance, Session attendance and Dropout rates were examined at each time point (T1, T2, T3, and T4) using Mann–Whitney U-tests, while dropout rates were compared between groups using Chi-Square test. To understand the magnitude of the between-group differences, we calculated Cohen’s r effect-size as z/√n, where z was retrieved from the Wilcoxon/Mann–Whitney output and n is the sample size. The effect size values were considered small (0.1), moderate (0.3), and large (≥ 0.5).48,49 Statistical significance was set at p< 0.05.
A priori sample size calculation was conducted and published30 to detect a minimally clinically important difference in occupational performance (COPM) with 80% power and a significance level of 0.05, while accounting for an expected dropout rate of 40%, resulting in a required sample of 24 participants per group. Intention-to-treat analysis was conducted using the last observation carried forward (LOCF) method, as a pragmatic approach to retain all randomized participants in the analysis despite missing follow-up data and to preserve the intention-to-treat framework. LOCF has been used in clinical trial research for this purpose.50,51 All participants were included in the analysis based on their original group allocation, regardless of adherence to the intervention protocol or dropout.
Results
Thirty-three men (18–45 years) were randomly assigned to the F-CaST (n=20) or control (n=13) group. Two participants in the F-CaST group discontinued participation shortly after allocation, resulting in 31 participants who began the intervention (Figure 1). Groups were comparable in baseline demographics, substance use characteristics, age of onset, time in the TC, and ASRS scores (Table 1).
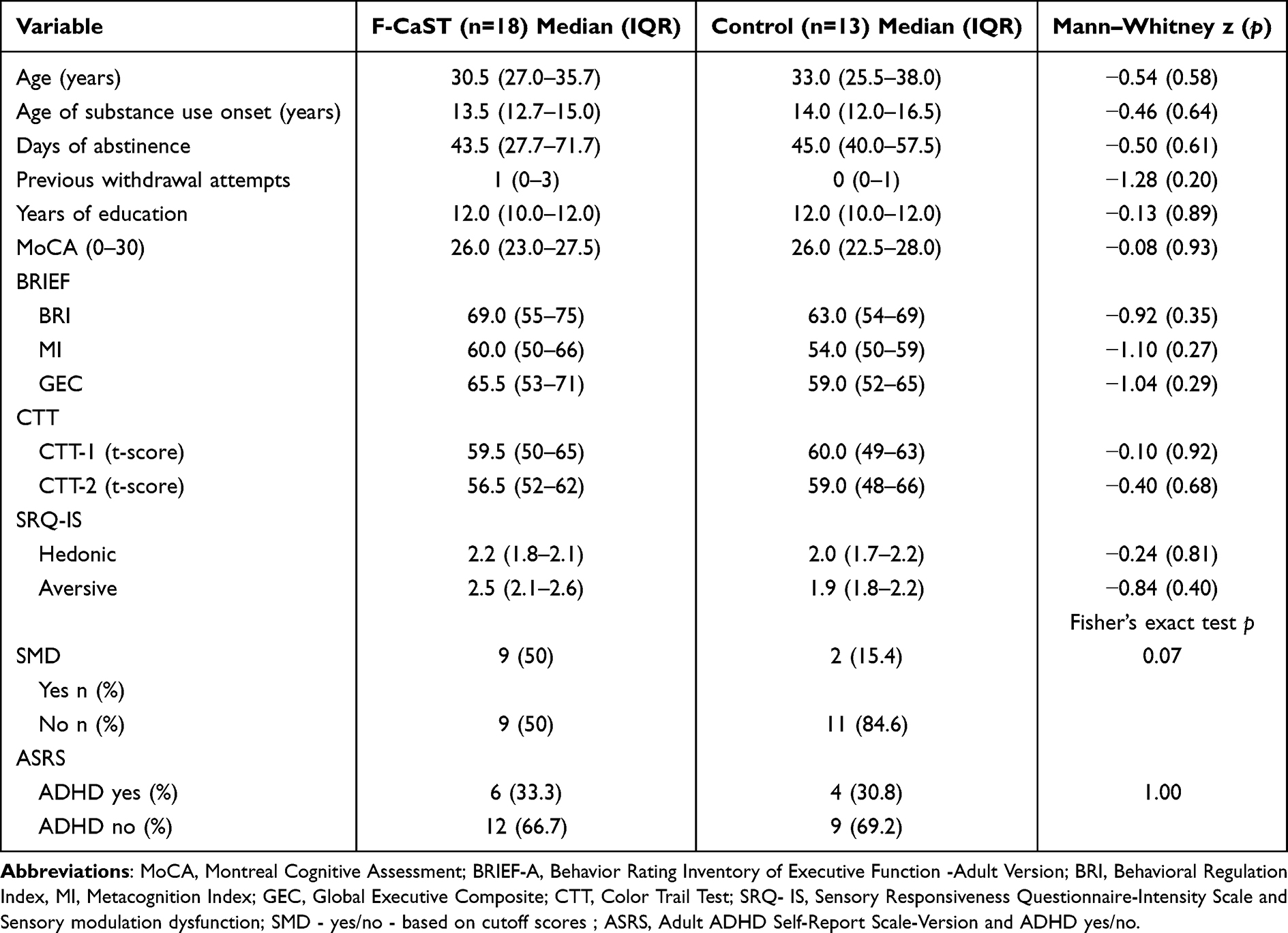 |
Table 1 Demographics, Substance Use, Impairments in EF and SMD; Characteristics of Participants in Both Groups and Comparisons |
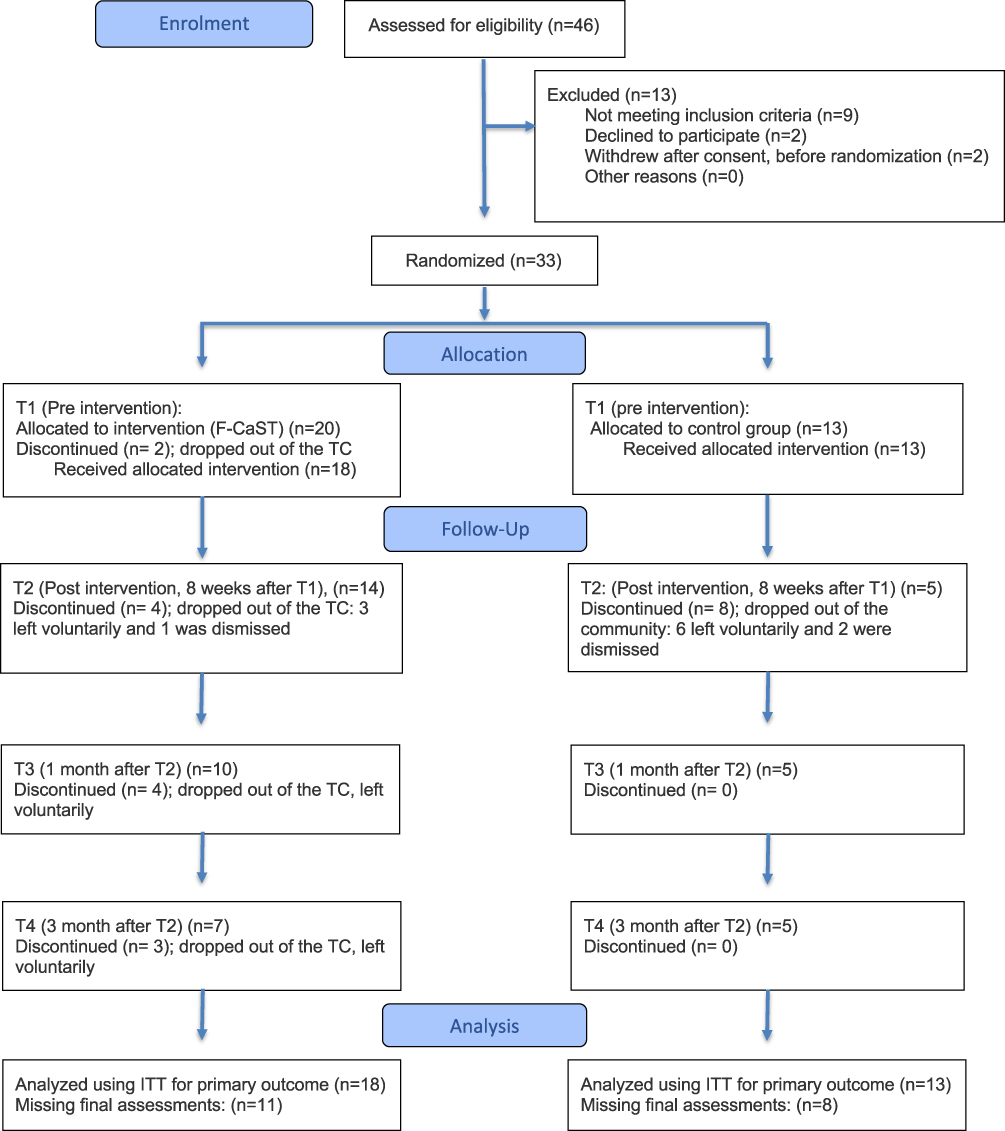 |
Figure 1 CONSORT 2025 flow diagram of participants through the study. |
Table 1 also characterizes the participants in terms of impairments in EF, CTT and SMD. BRIEF-A indicated greater EF difficulties in the F-CaST group (GEC >65), with BRI and MI scores within the clinical range, whereas the control group showed predominantly subclinical scores, yet the groups did not statistically differ. SMD, defined by SRQ-IS cutoff scores, was identified in 50% of participants in the F-CaST group and 15.4% in the control group; however, this difference did not reach statistical significance.
COPM – Performance and Satisfaction
At T1, no significant differences were found between groups in COPM Performance or Satisfaction, although the F-CaST group started slightly lower [Performance: 2.2 (1.5–3.0); Satisfaction: 2.2 (1.3–3.2)] compared with controls [Performance: 3.0 (2.0–3.7); Satisfaction: 3.0 (2.2–4.7)]. Within-group analyses showed significant improvements in both groups over time. In the F-CaST group, scores increased steadily from T1 to T4 [Performance: 5.7 (2.8–8.1); Satisfaction: 7.0 (2.7–9.2)], while the control group showed smaller gains that plateaued after T2 [Performance: 4.0 (3.0–8.2); Satisfaction: 5.5 (3.2–8.7)]. Between-group comparisons did not reveal statistically significant differences in COPM performance or satisfaction at any time point (Table 3). However, the F-CaST group demonstrated a more favorable pattern of improvement over time (Table 2). Both groups demonstrated progress, but the magnitude of change appeared greater in the F-CaST group, with larger effect sizes than those observed in the control group. A higher proportion of participants in the F-CaST group exceeded the MCID at each time point, with 55.6% at T2, 61.1% at T3, and 72.2% at T4, compared with 38.5% in the control group, whose rates remained stable over time. These findings suggest a potential advantage of F-CaST in terms of clinically meaningful improvements in occupational performance and satisfaction (Table 2).
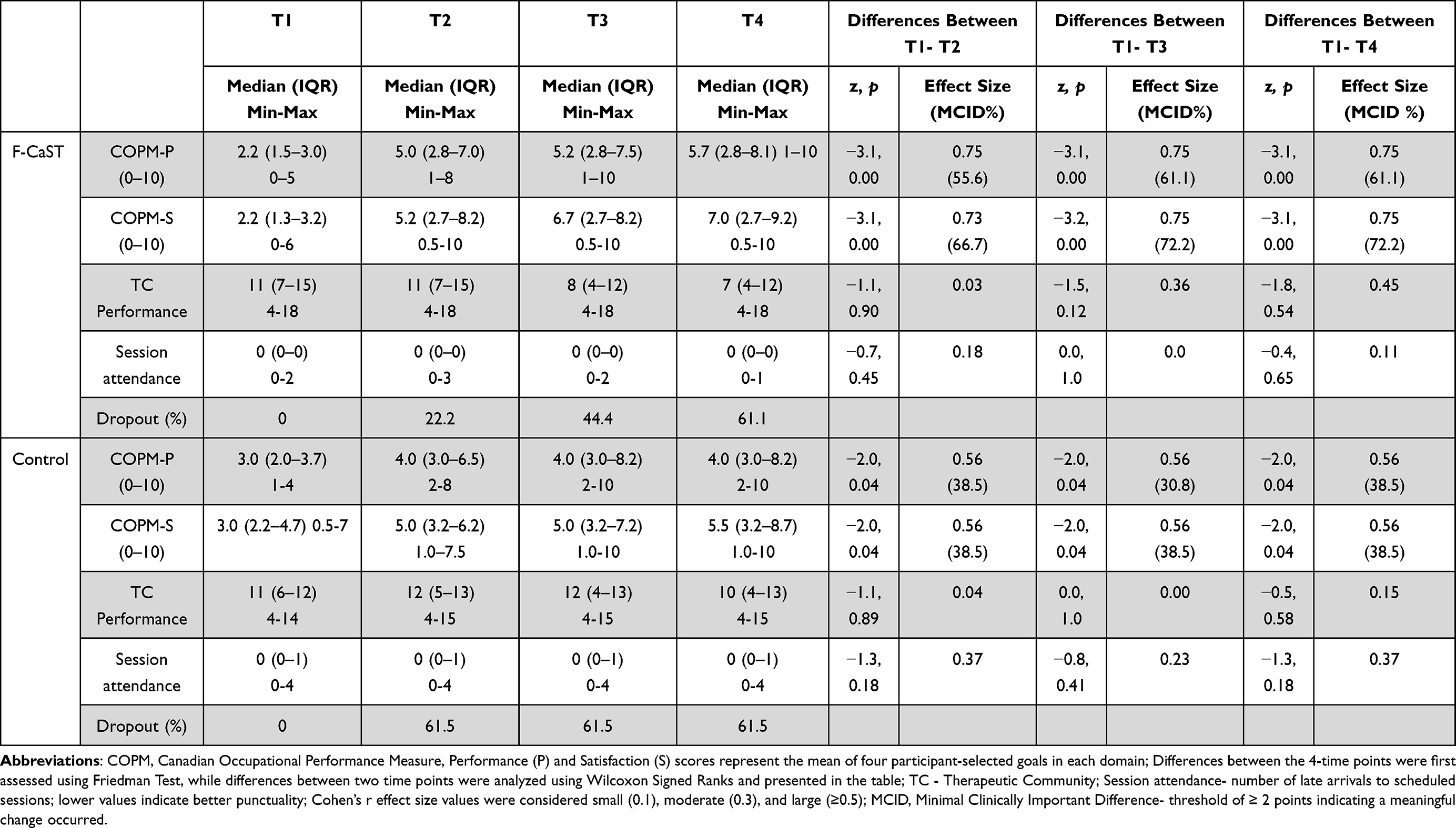 |
Table 2 Within-Group Comparison of COPM Performance and Satisfaction Scores Across Four Time-Points (T1, T2, T3, and T4) in F-CaST Group (n=18) and the Control Group (n=13) |
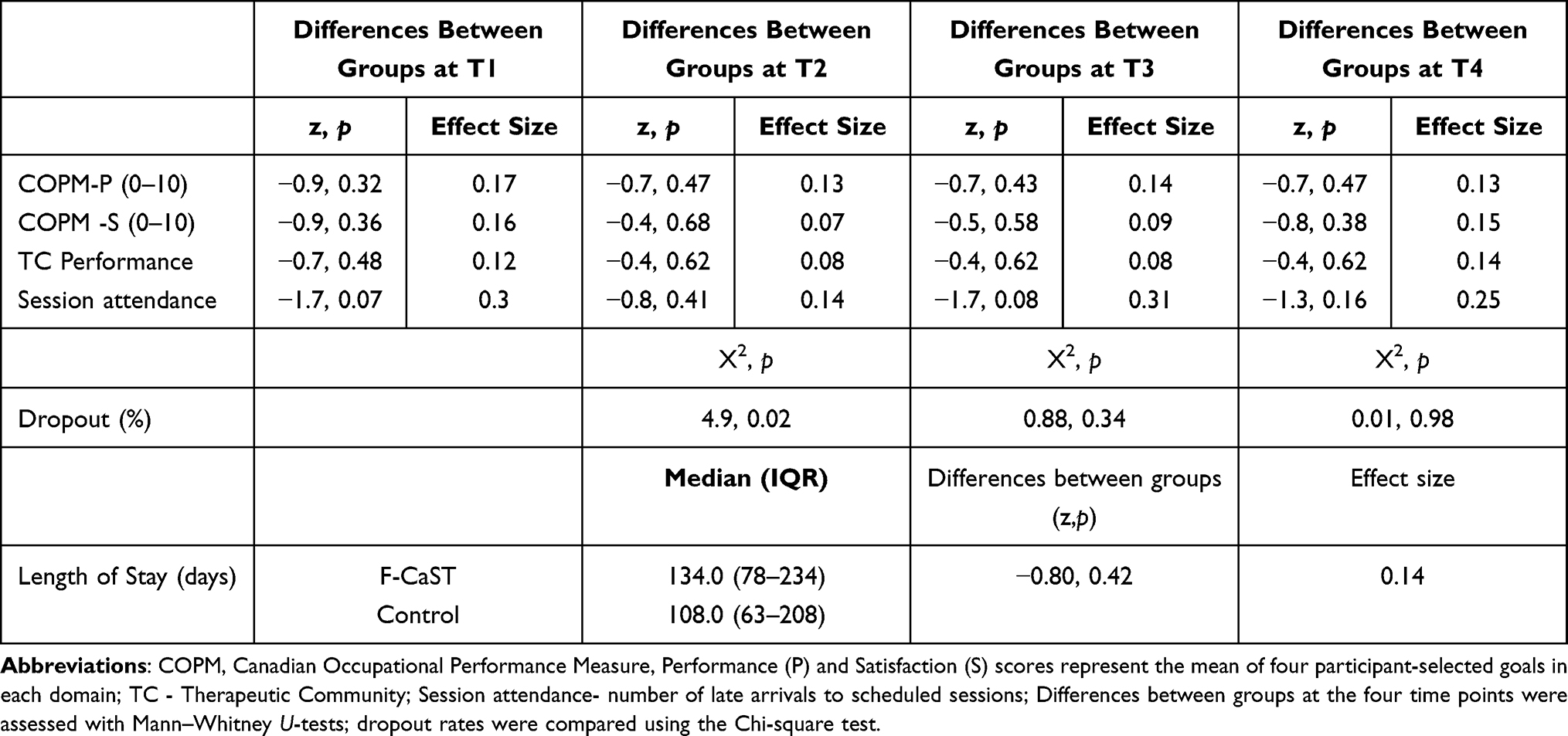 |
Table 3 Comparison of COPM Performance and Satisfaction Scores Across Four Time-Points (T1, T2, T3, and T4) Between Groups (F-CaST n=18; Control n=13) |
Dropout and Length of Stay in TC
No significant between-group differences were found in length of stay within the TC [F-CaST: 134 (78–234) days; control: 108 (63–208) days]. However, dropout rates differed over time. At T2, significantly fewer participants left the community in the F-CaST group (22.2%) compared with the control group (61.5%). By T3 and T4, dropout in the F-CaST group increased to 44.4% and 61.1%, respectively, while the control group remained unchanged at 61.5%, thus, between-group differences were no longer significant. Within-group analysis showed a gradual attrition pattern in F-CaST versus an early, stable dropout pattern in controls (Table 3).
TC Performance
No significant between-group differences were found in TC performance at any time point. Both groups improved over time, with a more pronounced change in the F-CaST group [median (IQR): 11 (7–15) to 7 (4–12)] compared with the control group [11 (6–12) to 10 (4–13)] (Table 3).
Session Attendance
No statistically significant between-group differences were observed in session attendance (number of late arrivals) at any time point (Table 3). However, a trend toward fewer late arrivals in the F-CaST group was observed at T1 and T3, with moderate effect sizes. The median number of late arrivals remained consistently low in the F-CaST group across all time points, and similarly low in the control group, although variability was lower in the F-CaST group. No significant within-group changes were observed over time.
Discussion
Findings from this randomized controlled trial suggest that F-CaST, a novel occupational therapy intervention for individuals with SUD, is feasible and may support improvements in daily functioning, satisfaction, and early treatment retention. These findings will be discussed below.
The COPM scores showed a more favorable pattern of improvement in the F-CaST group compared to the control group, although between-group differences were not statistically significant. Notably, over 70% of participants in the F-CaST group surpassed the MCID threshold at three months, compared with fewer than 40% in the control group, suggesting a potential for clinically meaningful functional gains. Exceeding the MCID reflects a meaningful improvement in daily functioning and participation, beyond statistical significance. As a patient-reported measure, COPM outcomes may also reflect participants’ perceptions and engagement with the intervention. In addition, given the non-double-blind design and the individualized nature of the intervention, COPM ratings may have been influenced by expectancy effects or social desirability. Notably, although not statistically significant, baseline trends indicated greater EF difficulties and a higher prevalence of SMD in the F-CaST group compared with the control group, which should be considered when interpreting the magnitude of change observed. These findings align with the FaCoT,47 an intervention for individuals with mild stroke, which the F-CaST was conceptually based on, and are consistent with prior studies showing that targeted cognitive and functional approaches can improve daily functioning in individuals with SUD.13,14,16 The psychoeducational format of the F-CaST, which combined theoretical instruction with practical application and reflection on daily challenges within the TC, may have contributed to these improvements by supporting the application of learned strategies in everyday contexts.52,53 The present findings, indicating improvements in functioning and reduced dropout during the early stages of the intervention, are consistent with recent research conducted in therapeutic community settings, suggesting that the most substantial improvements occur during the early phases of treatment and are associated with sustained engagement over time.54
F-CaST uniquely integrates strategies that target impairments in executive function as well as sensory modulation. These domains are rarely addressed together, not only in addiction rehabilitation. This dual focus may be one possible explanation for the higher rates of meaningful improvement observed, as regulating sensory responses alongside executive processes provides concrete tools for managing arousal, planning, and behavioral adaptation in daily life.22–24,27 Evidence from other populations, including ADHD, autism, and recent-onset mental illness, supports the link between atypical sensory modulation and impairments in EF, specifically in planning, inhibition, and emotion regulation.18,19,55 Taken together, these findings are consistent with theoretical models suggesting that interventions addressing both SMD and EF may support adaptive functioning by facilitating the coordination of sensory regulation, arousal, and executive control processes.20,56 Such integrative regulation has been proposed as a core component underlying adaptive behavior and cognitive–emotional regulation.
An additional finding of this study relates to treatment retention. Early dropout is a major challenge in SUD rehabilitation, typically occurring within the first 90 days.2,57 Participants who received the F-CaST showed lower dropout rates at T2, particularly immediately post-intervention, whereas no significant between-group differences were observed at the later follow-up points. This finding may indicate that a structured, goal-oriented, and functionally relevant program could support engagement and stability during the vulnerable early phase of treatment.58,59 It is possible that a longer intervention period may have yielded a more sustained retention effect. The lower dropout observed at T2 may reflect not only greater motivation but also improved self-efficacy and functional competence, core components of the F-CaST that promote autonomy and continuity in recovery. Taken together, these findings suggest the potential importance of addressing executive function–related difficulties in SUD rehabilitation as a potential lever for supporting engagement, adherence, and treatment outcomes,13,60 particularly during the early phase of treatment.
Our findings support the notion that strengthening daily functioning, establishing consistent routines, and enhancing engagement in meaningful activities may contribute to increased stability and involvement during the early stages of recovery. These findings are consistent with existing literature, which emphasizes that recovery from SUD extends beyond abstinence to include improvements in functioning, participation, and quality of life.6 Structured group-based interventions have similarly been shown to enhance discharge readiness and engagement in recovery routines.61 Recent conceptual reviews further highlight that daily structure, meaningful engagement, and participation in everyday activities are essential components of sustained recovery.5 Taken together, our results align with these perspectives and suggest that the F-CaST may contribute to enhanced engagement in treatment, considered an important foundation for recovery.
Improvements in both groups, particularly in the TC Performance, underscore the inherent therapeutic value of community-based rehabilitation. TC provides structured, occupation-rich environments that promote responsibility, social connection, and engagement in meaningful routines, key contributors to recovery and stability.1,62 Within this framework, the F-CaST may complement the community model by offering individualized strategies to help participants apply and generalize these experiences, leading to improved self-regulation and daily performance.
The F-CaST incorporated positive and negative personas to promote reflection, insight, and increase self-efficacy. This experiential approach may have facilitated the internalization of learned strategies and strengthened participants’ confidence in their ability to change. Consistent with Bandura’s social learning theory,63 observing adaptive and maladaptive behaviors through modeling reinforced both self-efficacy and the integration of intervention principles.
The study’s findings offer a unique perspective on mechanisms underlying participants’ perceived changes. The F-CaST combines individualized and group components, supporting both personal goal attainment and peer learning. In other words, individual sessions may have helped participants analyze their sensory and executive function profiles, set goals, and practice strategies for planning and behavioral regulation, likely enhancing self-efficacy and emotional control. Group sessions provided psychoeducation and shared experiential learning, fostering awareness and mutual reinforcement.47 Although no between-group differences were observed in objective indicators such as attendance (late arrivals), this may reflect contextual factors rather than a lack of progress. Consistent with prior research, subjective, client-centered measures such as the COPM are often more sensitive to meaningful functional change, whereas objective outcomes may require longer follow-up to capture effects.40–42,64
Study Limitations
This study has several limitations. The smaller-than-planned, homogeneous sample of men from a single TC enabled a more focused examination of the intervention but limited generalizability and may have reduced statistical power to detect between-group differences. Further, TC performance was assessed using an observational measure developed for this study, capturing context-specific relevance. Yet no psychometric validation was established, limiting the robustness of its findings. In addition, baseline trends indicating greater executive and sensory modulation dysfunction in the intervention group, although not statistically significant, may affect group comparability.
Given the modest and unequal group sizes (n=13, n=18), non-normal distributions, and four time points raising concerns about sphericity, non-parametric analyses were used; future studies with larger, balanced samples could apply repeated measures ANOVA. Missing data were handled using last observation carried forward, which may have influenced estimates, and dropout was analyzed at fixed time points rather than using time-to-event methods. The long-term impact of the findings remains unclear. Finally, as the intervention group received additional structured treatment, improvements may partly reflect increased therapeutic attention; future studies should include an active control condition to isolate intervention-specific effects.
Conclusion
The F-CaST is an innovative occupational therapy intervention for individuals with SUD residing in a TC. The F-CaST, which addressed impairments in executive function and sensory modulation, appears to support improvements in occupational performance, satisfaction, and early treatment retention. Further studies should aim to integrate the F-CaST in TC programs to enhance occupational performance and reduce dropout in early recovery of individuals with SUD.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions and protection of participant confidentiality but are available from the corresponding author on reasonable request.
Acknowledgments
The authors wish to thank the staff and residents of the therapeutic community for their cooperation and participation in this study, and Sigal Svorai for her assistance with data collection.
Funding
This trial has been funded by the Department of Justice, Estates Committee (grant number 20210605).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vanderplasschen W, Colpaert K, Autrique M, et al. Therapeutic communities for addictions: a review of their effectiveness from a recovery-oriented perspective. ScientificWorldJournal. 2013;2013:427817. doi:10.1155/2013/427817
2. Brorson HH, Ajo Arnevik E, Rand-Hendriksen K, Duckert F. Drop-out from addiction treatment: a systematic review of risk factors. Clinic Psychol Rev. 2013;33(8):1010–13. doi:10.1016/j.cpr.2013.07.007
3. Darke S, Campbell G, Popple G. Retention, early dropout and treatment completion among therapeutic community admissions. Drug and Alcohol Review. 2012;31(1):64–71. doi:10.1111/j.1465-3362.2011.00298.x
4. Lappan SN, Brown AW, Hendricks PS. Dropout rates of in-person psychosocial substance use disorder treatments: a systematic review and meta-analysis. Addiction. 2020;115(2):201–217. doi:10.1111/add.14793
5. Dogu SE, Ozkan E. The role of occupational therapy in substance use. Nordisk Alkohol Nark. 2023;40(4):406–413. doi:10.1177/14550725221149472
6. Gaumond P, Martin LA, Hagman BT, Davis MJ. Substance use disorder recovery research opportunities: perspectives from a federal interagency workgroup. Front Public Health. 2025;13:1585533. doi:10.3389/fpubh.2025.1585533
7. Ryan DA, Boland P. A scoping review of occupational therapy interventions in the treatment of people with substance use disorders. Irish J Occupat Ther. 2021;49(2):104–114. doi:10.1108/ijot-11-2020-0017
8. American Psychiatric Association. Understanding Mental Disorders: Your Guide to DSM-5-TR®. American Psychiatric Pub; 2023.
9. United Nations Office on Drugs and Crime. Outcome document of the 2016 United Nations General Assembly special session on the world drug problem. In: United Nations Office on Drugs and Crime. Vienna; 2016.
10. Key substance use and mental health indicators in the United States: results from the 2023 National Survey on Drug Use and Health (Center for behavioral health statistics and quality. Substance Abuse and Mental Health Services Administration). 2024.
11. Haviv N, Kaplan Harel G, Sternfeld M, Wolff M. Exploring the impact of coercion and voluntary entry on dropout rates in a therapeutic community for substance abuse rehabilitation: a survival analysis and logistic regression study. Probation Journal. 2024;71(3):275–293. doi:10.1177/02645505231221226
12. Fernández-Serrano MJ, Pérez-García M, Perales JC, Verdejo-García A. Prevalence of executive dysfunction in cocaine, heroin and alcohol users enrolled in therapeutic communities. Eur J Pharmacol. 2010;626(1):104–112. doi:10.1016/j.ejphar.2009.10.019
13. Nardo T, Batchelor J, Berry J, Francis H, Jafar D, Borchard T. Cognitive remediation as an adjunct treatment for substance use disorders: a systematic review. Neuropsychol Rev. 2022;32(1):161–191. doi:10.1007/s11065-021-09506-3
14. Verdejo-Garcia A, Garcia-Fernandez G, Dom G. Cognition and addiction. Dialogues Clin Neurosci. 2019;21(3):281–290. doi:10.31887/DCNS.2019.21.3/gdom
15. Zink N, Lenartowicz A, Markett S. A new era for executive function research: on the transition from centralized to distributed executive functioning. Neurosci Biobehav Rev. 2021;124:235–244. doi:10.1016/j.neubiorev.2021.02.011
16. Manning V, Verdejo-Garcia A, Lubman DI. Neurocognitive impairment in addiction and opportunities for intervention. Curr Opin Behav Sci. 2017;13:40–45. doi:10.1016/j.cobeha.2016.10.003
17. Toglia J, Katz N. Executive functioning: prevention and health promotion for at-risk populations and those with chronic disease. In: Cognition Occupation, and Participation Across the Lifespan: Neuroscience, Neurorehabilitation, and Models of Intervention in Occupational Therapy. 2018:129–142.
18. Engel-Yeger B, Mevorach Shimoni M. The contribution of atypical sensory processing to executive dysfunctions, anxiety and quality of life of children with ADHD. Occupat Ther Mental Health. 2024;40(2):103–122. doi:10.1080/0164212X.2023.2220975
19. Huang Z, Wang F, Xue L, Zhu H, Zou X. Relationships between sensory processing and Executive functions in children with combined ASD and ADHD compared to typically developing and single disorder groups. Brain Sci. 2024;14(6):566. doi:10.3390/brainsci14060566
20. Li J, Wang W, Cheng J, et al. Relationships between sensory integration and the core symptoms of attention-deficit/hyperactivity disorder: the mediating effect of executive function. Eur Child Adolesc Psychiatry. 2023;32(11):2235–2246. doi:10.1007/s00787-022-02069-5
21. Assayag N, Bonneh Y, Parush S, Mell H, Kaplan Neeman R, Bar-Shalita T. Perceived sensitivity to pain and responsiveness to non-noxious sensation in substance use disorder. Pain Med. 2020;21(9):1902–1912. doi:10.1093/pm/pnz292
22. Engel-Yeger B. Sensory processing disorders among substance dependents. Cadernos de Terapia Ocupacional da UFSCar. 2014;22(Especial):111–118. doi:10.4322/cto.2014.035
23. Kelly J, Meredith PJ, Taylor M, Morphett A, Wilson H. Substances and your senses: the sensory patterns of young people within an alcohol and drug treatment service. Subst Abus. 2021;42(4):998–1006. doi:10.1080/08897077.2021.1901177
24. Bar-Shalita T, Vatine JJ, Parush S. Sensory modulation disorder: a risk factor for participation in daily life activities. Dev Med Child Neurol. 2008;50(12):932–937. doi:10.1111/j.1469-8749.2008.03095.x
25. Lipskaya-Velikovsky L, Bar-Shalita T, Bart O. Sensory modulation and daily-life participation in people with schizophrenia. Compr Psychiatry. 2015;58:130–137. doi:10.1016/j.comppsych.2014.12.009
26. Kinnealey M, Koenig KP, Smith S. Relationships between sensory modulation and social supports and health-related quality of life. Am J Occup Ther. 2011;65(3):320–327. doi:10.5014/ajot.2011.001370
27. Costa-López B, Ferrer-Cascales R, Ruiz-Robledillo N, Albaladejo-Blázquez N, Baryła-Matejczuk M. Relationship between sensory processing and quality of life: a systematic review. J Clin Med. 2021;10(17):3961. doi:10.3390/jcm10173961
28. Miller LJ, Anzalone ME, Lane SJ, Cermak SA, Osten ET. Concept evolution in sensory integration: a proposed nosology for diagnosis. Am J Occup Ther. 2007;61(2):135–140. doi:10.5014/ajot.61.2.135
29. Interdisciplinary Council on Developmental and Learning Disorders. Diagnostic Manual for Infancy and Early Childhood: Mental Health Disorders, Developmental Disorders, Regulatory-Sensory Processing Disorders, Language Disorders, and Learning Challenges. ICDL-DMIC Work Groups; 2012.
30. Assayag N, Bar-Shalita T, Rand D. The Functional-Cognitive and Sensory Treatment (F-CaST) to improve rehabilitation outcomes of individuals with substance use disorder: a study protocol for a mixed-method randomized controlled trial. Addict Sci Clin Pract. 2024;19(1):28. doi:10.1186/s13722-024-00449-7
31. Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet. 2001;357(9263):1191–1194. doi:10.1016/S0140-6736(00)04337-3
32. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Obstet Gynecol. 2010;115(5):1063–1070. doi:10.1097/AOG.0b013e3181d9d421
33. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
34. Rohner H, Gaspar N, Philipsen A, Schulze M. Prevalence of Attention Deficit Hyperactivity Disorder (ADHD) among Substance Use Disorder (SUD) Populations: meta-Analysis. Int J Environ Res Public Health. 2023;20(2):1275. doi:10.3390/ijerph20021275
35. Daigre Blanco C, Ramos-Quiroga JA, Valero S, et al. Adult ADHD Self-Report Scale (ASRS-v1.1) symptom checklist in patients with substance use disorders. Actas Esp Psiquiatr. 2009;37(6):299–305.
36. Van de Glind G, Konstenius M, Koeter MWJ, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend. 2014;134:158–166. doi:10.1016/j.drugalcdep.2013.09.026
37. Copersino ML, Fals-Stewart W, Fitzmaurice G, Schretlen DJ, Sokoloff J, Weiss RD. Rapid cognitive screening of patients with substance use disorders. Exp Clin Psychopharmacol. 2009;17(5):337–344. doi:10.1037/a0017260
38. Kessler R, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol med. 2005;35:245–256. doi:10.1017/S0033291704002892
39. Van de Glind G, Van den Brink W, Koeter MWJ, et al. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend. 2013;132(3):587–596. doi:10.1016/j.drugalcdep.2013.04.010
40. Thyer L, Brown T, Roe D. The validity of the Canadian Occupational Performance Measure (COPM) when used in a sub-acute rehabilitation setting with older adults. Occupational Ther Health Care. 2018;32(2):137–153. doi:10.1080/07380577.2018.1446233
41. Law M, Baptiste S, Carswell A, McColl M, Polatajko H, Pollock N. Canadian Occupational Performance Measure Manual. Canada:Canadian Association of Occupational Therapy Publications; 1998.
42. Wressle E, Samuelsson K, Henriksson C. Responsiveness of the Swedish version of the Canadian occupational performance measure. Scandinavian J Occupat Ther. 1999;6(2):84–89. doi:10.1080/110381299443771
43. D’Elia LF, Satz P, Uchiyama CL, White T. Color Trails Test Professional manual. In: Psychological Assessment Resources. Odessa(FL.); 1996.
44. Roth RM, Gioia GA, Isquith PK. BRIEF-A: Behavior Rating Inventory of Executive Function--Adult Version. Psychological Assessment Resources; 2005.
45. Hagen E, Erga AH, Hagen KP, et al. Assessment of executive function in patients with substance use disorder: a comparison of inventory- and performance-based assessment. J Substance Abuse Treat. 2016;66:1–8. doi:10.1016/j.jsat.2016.02.010
46. Bar-Shalita T, Seltzer Z, Vatine -J-J, Yochman A, Parush S. Development and psychometric properties of the Sensory Responsiveness Questionnaire (SRQ). Disability Rehabil. 2009;31(3):189–201. doi:10.1080/09638280801903096
47. Adamit T, Shames J, Rand D. Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) intervention for improving daily functioning and participation of individuals with mild stroke: a randomized controlled trial. Int J Environ Res Public Health. 2021;18(15):7988. doi:10.3390/ijerph18157988
48. Cohen J. Statistical Power Analysis for the Behavioral Sciences. routledge; 2013.
49. Tomczak M, Tomczak E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trend Sport Sci. 2014;1(21):19–25.
50. Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res. 2011;2(3):109–112. doi:10.4103/2229-3485.83221
51. Zhang Y, Flórez ID, Colunga Lozano LE, et al. A systematic survey on reporting and methods for handling missing participant data for continuous outcomes in randomized controlled trials. J Clin Epidemiol. 2017;88:57–66. doi:10.1016/j.jclinepi.2017.05.017
52. Lukens EP, McFarlane WR. Psychoeducation as evidence-based practice: considerations for practice, research, and policy. Brief Treat Crisis Intervent. 2004;4(3):205–225. doi:10.1093/brief-treatment/mhh019
53. McFarlane WR, Dixon L, Lukens E, Lucksted A. Family psychoeducation and schizophrenia: a review of the literature. J Marital Fam Ther. 2003;29(2):223–245. doi:10.1111/j.1752-0606.2003.tb01202.x
54. Passam H, Miller RK, Rogers K, Babineau J, Newton-John TR. Effectiveness of a therapeutic community for substance use: stage completion and time in treatment as predictors of outcome. Clin Psychol. 2025;29(3):327–340. doi:10.1080/13284207.2025.2533128
55. Lipskaya-Velikovsky L, Hershkovitz A, Bukai M, Bar-Shalita T. Recent onset mental illness severity: pilot study on the role of cognition, sensory modulation, and daily life participation. Front Psych. 2024;15:1413635. doi:10.3389/fpsyt.2024.1413635
56. Menon V. Large-scale brain networks and psychopathology: a unifying triple network model. Trend Cognit Sci. 2011;15(10):483–506. doi:10.1016/j.tics.2011.08.003
57. Ehliasson K, Eriksson J, LoMartire R. Dropout from substance use disorder treatment at a swedish private care institution and its associated risk factors. Substance Use. 2025;19:1–7. doi:10.1177/29768357251332827
58. Lantz L, Chang Z, Virtanen S. Risk factors for dropout from psychological substance use disorder treatment programs in criminal justice settings. Drug Alcohol Depend. 2024;259:111314. doi:10.1016/j.drugalcdep.2024.111314
59. Fleury M-J, Cao Z, Grenier G, Huỳnh C. Predictors of dropout from treatment among patients using specialized addiction treatment centers. J Subst Use Addict Treat. 2023;150:209062. doi:10.1016/j.josat.2023.209062
60. McKowen J, Carrellas N, Zulauf C, Ward EN, Fried R, Wilens T. Factors associated with attrition in substance using patients enrolled in an intensive outpatient program. Am J Addict. 2017;26(8):780–787. doi:10.1111/ajad.12619
61. Alcala M, Esgro S. Group occupational therapy and substance use recovery. West Coast Univer J Health Wellness. 2025;2(1).
62. Malivert M, Fatséas M, Denis C, Langlois E, Auriacombe M. Effectiveness of therapeutic communities: a systematic review. Eur Addict Res. 2011;18(1):1–11. doi:10.1159/000331007
63. Bandura A. Self- Efficacy. In: Bandura A, editor. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs; 1986:390–453.
64. Malec JF, Ketchum JM. A standard method for determining the minimal clinically important difference for rehabilitation measures. Arch Phys Med Rehabil. 2020;101(6):1090–1094. doi:10.1016/j.apmr.2019.12.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.