Back to Journals » Drug Design, Development and Therapy » Volume 19
Effectiveness of Sequential Treatment with Zoledronic Acid Following Discontinuation of Denosumab in Osteoporosis: A Narrative Review
Authors Ouyang H, Yang F, Wei W, Wang W
Received 23 June 2025
Accepted for publication 30 October 2025
Published 9 November 2025 Volume 2025:19 Pages 10013—10031
DOI https://doi.org/10.2147/DDDT.S549062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Georgios Panos
Hong Ouyang,1,* Fan Yang,1,* Wenzuo Wei,2 Wei Wang3
1Department of Endocrine and Metabolism, Geriatric Diseases Institute of Chengdu, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, 611137, People’s Republic of China; 2DXR Advanced Clinical Application and Collaboration Center, GE HealthCare, Shanghai, People’s Republic of China; 3Department of Endocrine and Metabolism, Chengdu Seven People’s hospital, Chengdu, 611137, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Ouyang, Email [email protected] Fan Yang, Email [email protected]
Abstract: Denosumab is a recently developed anti-osteoporosis agent widely applied in the treatment of osteoporosis in postmenopausal women. As a potent inhibitor of bone resorption, it significantly increases bone mineral density, lowers elevated bone turnover rates, and reduces fracture risk. Because denosumab does not bind to the bone matrix, its effects decrease rapidly after discontinuation, a process commonly known as the “rebound effect.” Research has shown that administering zoledronic acid after stopping denosumab can help preserve bone density and reduce the likelihood of vertebral fractures. However, the exact effectiveness of this sequential approach and the factors influencing it, including the duration of prior denosumab treatment, timing, and frequency of zoledronic acid administration, remain insufficiently understood. To address these uncertainties, this review evaluates the effects of sequential zoledronic acid therapy on subsequent changes in bone density, bone turnover markers, fracture risk, and adverse reactions. We also examined in detail the dosage strategies, administration intervals of zoledronic acid, and length of preceding denosumab use across studies, aiming to assist clinicians in designing more evidence-based and clinically relevant sequential treatment protocols.
Keywords: denosumab, zoledronic acid, bone mineral density, bone transformation markers, vertebral fractures
Introduction
Over recent decades, the incidence of osteoporosis has steadily risen, driven by an aging population, longer life expectancy, and widespread unhealthy dietary habits and sedentary lifestyles. Osteoporosis is a chronic skeletal condition characterized by disrupted bone metabolism. Its onset is often silent, and it typically presents as a reduction in both bone mass and structural integrity, resulting in a measurable decline in bone mineral density.1 According to the World Health Organization (WHO), osteoporosis is defined by a bone density that is 2.5 standard deviations or more below the average of young healthy adults (T-score ≤ −2.5).2 This decline in bone density sharply increases the risk of both vertebral and non-vertebral fragility fractures,3 and is strongly associated with elevated morbidity, mortality, healthcare utilization, medical expenses, and deterioration in quality of life.4–7
In recent years, notable progress has been made in pharmacological interventions for osteoporosis. These treatments primarily work by increasing bone density and regulating bone remodeling, which helps reduce the likelihood of osteoporotic fractures.8–10 Among these therapies, monoclonal antibodies that target the receptor activator of nuclear factor kappa-B ligand (RANKL), a key regulator of bone turnover, represent a major advancement. Denosumab (Dmab), a fully human monoclonal antibody against RANKL, is now widely prescribed for postmenopausal women with osteoporosis.11–14 As a potent anti-resorptive agent, Dmab is administered via subcutaneous injection every six months. It reversibly suppresses the formation, activity, and survival of osteoclasts, which substantially reduces bone resorption. Clinical studies have confirmed that Dmab can significantly increase bone density in postmenopausal women with osteoporosis, suppress elevated bone turnover, and reduce fracture risk.15,16 During the administration of Dmab, it is essential to dynamically monitor changes in blood calcium levels, vitamin D status, bone density, and other relevant indicators. Additionally, potential drug-related adverse reactions, such as allergic reactions, hypotension, and osteonecrosis of the jaw, should be closely observed. The corresponding management flowchart algorithm is presented in Figure 1. Moreover, long-term follow-up data indicate that Dmab continues to lower the incidence of new vertebral, non-vertebral, and hip fractures over treatment durations of up to 10 years.17–19
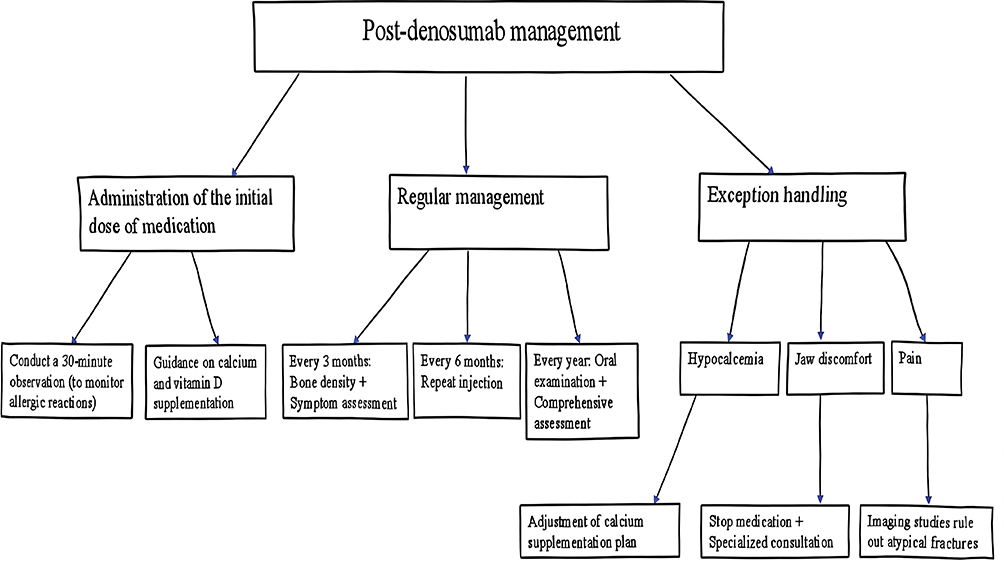 |
Figure 1 The guide of post-denosumab management. |
However, unlike bisphosphonates (BPs), Dmab does not bind to the bone matrix, and its effects are reversible. Following Dmab discontinuation, bone turnover markers (BTMs) rise rapidly, surpassing baseline levels within 9 months after the final injection and remaining elevated for approximately 2 years, before gradually returning to baseline around month 30. Consistent with this, bone mineral density (BMD) gained during treatment gradually declines after cessation, typically returning to pretreatment levels by 12 to 24 months.11,20 This process is commonly referred to as the “rebound effect”, likely resulting from increased osteoclastogenesis that drives bone turnover beyond baseline levels.20–22 During this phase of accelerated turnover, the risk of “rebound bone turnover-related vertebral fractures” increases substantially,by approximately 7%.23–25 The research revealed that among patients who discontinued Dmab treatment, 60.7% of vertebral fracture cases involved multiple fractures, compared to only 38.7% in the group that discontinued placebo treatment.26 Furthermore, another study indicated that delayed initiation of Dmab was associated with a fourfold increase in the risk of developing any vertebral fracture.27,28 In response to these concerns, clinical guidelines published in 2017 clarified that the concept of a “drug holiday” applies only to zoledronic acid (ZOL) and not to Dmab, for which sequential therapy is necessary.29 To reduce the risk associated with the rebound effect, it is recommended to initiate BPs therapy within 6–9 months of the final Dmab injection,30–32 with intravenous ZOL being the most extensively studied option.33–35 As a BP, ZOL also suppresses bone resorption. However, in contrast to Dmab, its effects can persist for years after treatment ends.36
At present, reported outcomes on the efficacy of ZOL in maintaining Dmab-induced BMD gains remain inconsistent. Some studies have indicated that most patients maintain stable BMD at one year post-treatment,33,37,38 while others suggest only partial preservation.39,40 The variation in outcomes is believed to depend mainly on two clinical factors: the timing of ZOL infusion and the length of prior Dmab use.34,40,41 Despite current knowledge, the optimal regimen for ZOL, regarding timing, frequency, and duration, after Dmab discontinuation is still under investigation. Therefore, we collected all relevant studies on the sequential treatment with ZOL after discontinuation of Dmab published up to May 2025 from the PubMed databases and conducted a comprehensive analysis. This review therefore aims to examine the effects of sequential ZOL therapy on subsequent BMD, BTMs, fracture risk, and adverse events. Additionally, it analyzes treatment intervals, ZOL dosing schedules, and duration of preceding Dmab use, with the goal of offering more practical guidance to clinicians. Table 1 provides a list of studies34,35,39,42–44 on on sequential ZOL treatment following Dmab discontinuation, which will be described in detail later in this review.
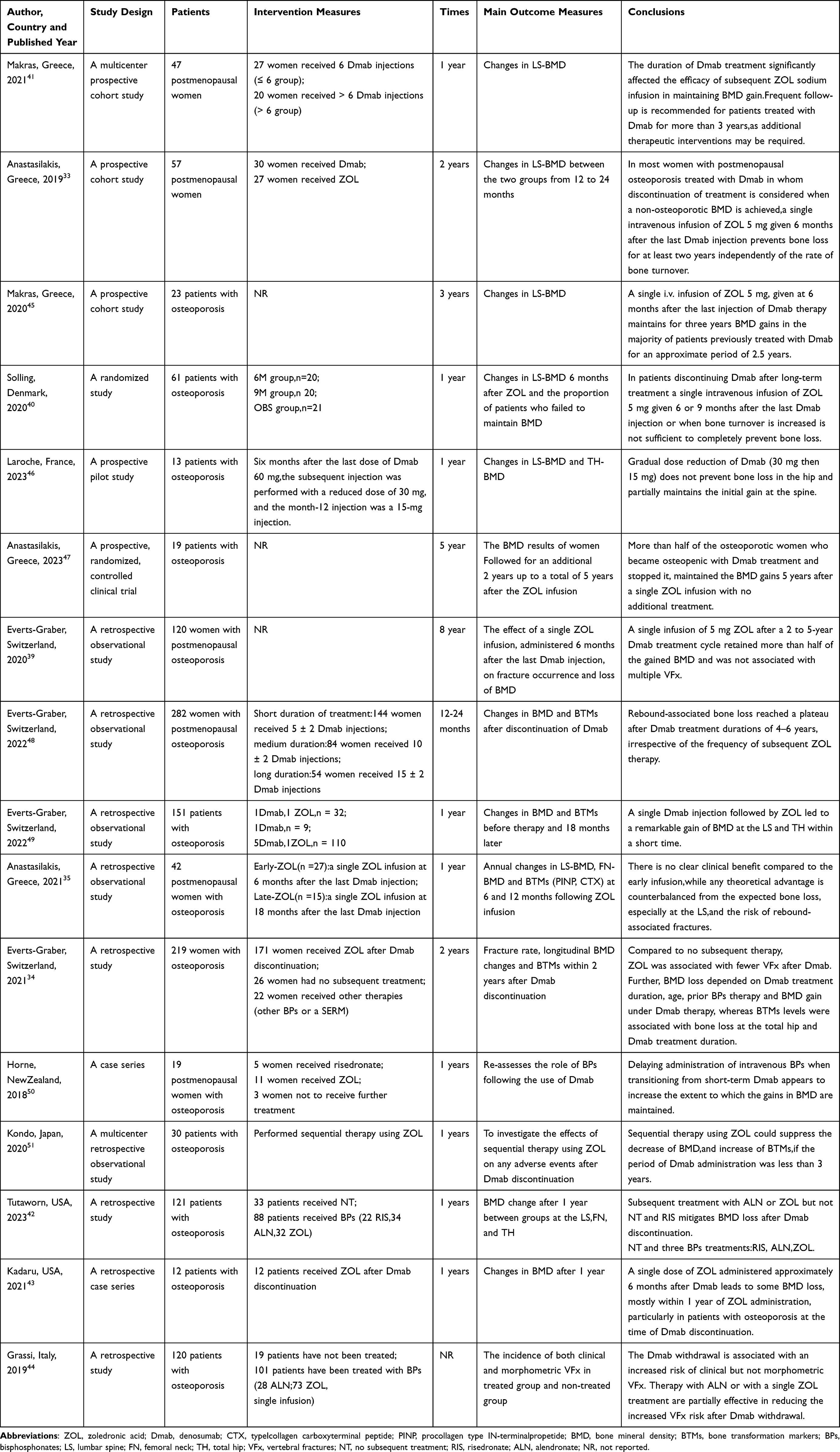 |
Table 1 Characteristics of Included Reports (N=16) |
The Efficacy of Sequential Zoledronic Acid Treatment After Discontinuation of Denosumab
We compiled and analyzed data on the effects of sequential ZOL on subsequent BMD, BTMs, fracture incidence, and adverse reactions, as presented in Table 2.
 |
Table 2 The Efficacy of Sequential Zoledronic Acid Treatment After Discontinuation of Denosumab |
The Influence on Bone Mineral Density
Following the discontinuation of Dmab, the BMD gained during treatment gradually declines, a process widely referred to as the “rebound effect.” Data from Table 2 suggest that sequential ZOL can partly maintain the BMD improvements achieved during Dmab therapy. In a study by Everts-Graber et al, 120 postmenopausal women with osteoporosis received a 5 mg dose of ZOL sodium 6 months after their final Dmab injection. Their findings showed that BMD decreased by 3.3% at the lumbar spine (following a 6.4% gain from baseline), by 2.2% at the total hip (after a 2.4% increase), and by 1.5% at the femoral neck (following a 2.0% gain). Despite these reductions, the BMD gains retained were 66%(95% CIs:57–75%) at the lumbar spine, 49%(95% CIs:31–67%) at the total hip, and 57%(95% CIs:25–89%) at the femoral neck, indicating that more than half of the improvement was preserved at most sites.39 Similar results were reported by Horne et al, who found that intravenous ZOL administered after Dmab preserved 73% ((95% CIs:61–85%) of the spinal BMD benefits achieved through the use of Dmab previously, and 87% (95% CIs:77–98%) of the total hip BMD benefits. In contrast, the corresponding spinal and hip bone densities of patients who did not receive treatment only retained 22% ((95% CIs:7–37%) and 8% ((95% CIs: −31-47%), respectively.50 Kadaru et al compared dual-energy X-ray absorptiometry (DXA) results taken at the end of Dmab treatment with those after the first ZOL infusion. Their findings showed a significant decrease in BMD at the femoral neck, while the lumbar spine and total hip showed a non-significant downward trend. Nevertheless, BMD at all three sites remained above the values recorded before initiating Dmab.43 Additionally, Everts-Graber et al compared BMD outcomes between women who received ZOL sodium after stopping Dmab and those who received no follow-up treatment. The results showed that patients given sequential ZOL had significantly higher BMD at all measured sites compared to those without subsequent therapy,34 a finding consistent with results reported by Tutaworn et al.42 Anastasilakis et al divided postmenopausal women previously treated with Dmab into two groups. One group received a single 5 mg ZOL infusion 6 months after the last Dmab dose, while the other group continued with two additional 60 mg Dmab injections. At 12 months, both groups had increased lumbar spine bone mineral density (LS-BMD) compared with baseline, with no statistically significant difference between them. However, by 24 months, LS-BMD in the ZOL group had returned to baseline, whereas the Dmab group experienced a significant decline from the 12-month value, dropping below baseline levels.33 In a 3-year follow-up of patients treated with ZOL, 82.6% maintained BMD within the osteopenia range, and only four patients had values below the osteoporosis threshold.45 At 5 years, 50% of the patients still had BMD in the osteopenia range, suggesting that more than half of postmenopausal women who transitioned from osteoporosis to osteopenia after Dmab treatment could sustain their BMD for up to 5 years with a single ZOL sodium infusion.47
The Influence on Bone Turnover Markers
BTMs change rapidly after Dmab is discontinued without follow-up treatment. Within 3–6 months after stopping Dmab, both C-terminal telopeptide of type I collagen (CTX) and type I procollagen N-terminal propeptide (PINP) exceed pretreatment levels, with median peak increases of 63% and 47% from baseline, respectively.11,20 These elevated levels persist for up to 2 years before gradually declining to pretreatment values by around 24 months. As shown in Table 2, sequential ZOL appears to lessen the rebound in BTMs to some degree. Studies report that when 5 mg of ZOL is given 6 months after the final Dmab injection, serum CTX and P1NP levels rise but remain below the upper limit of the postmenopausal range.39 In a study by Anastasilakis et al, BTMs in the ZOL group rose slightly in the first year and then stabilized. At 24 months, only 7.4% of patients had PINP levels above the postmenopausal reference range, and no patients had elevated CTX levels. In contrast, patients who remained on Dmab showed significant increases in both CTX and PINP by month 15 (9 months after their last injection), with levels significantly higher than those in the ZOL group. By month 24, only 6.6% of patients in the Dmab group had serum PINP within the premenopausal range, while 40% had CTX values within that range. These results suggest that although a single ZOL infusion can suppress the rebound in BTMs, it does not fully maintain BTMs levels within the reference range (either premenopausal or postmenopausal) 2 years after stopping Dmab.33 An extended follow-up of the same study found that, at 3 years after ZOL treatment, only one patient had a serum P1NP value above the postmenopausal reference range, and none had elevated CTX levels. This suggests that ZOL can effectively restrain the rebound in BTMs following Dmab discontinuation and may provide lasting control.45 Additionally, variation in BTMs levels was found to be associated with the duration of prior Dmab treatment.31 This finding aligns with the results reported by Everts-Graber et al, who observed that most patients with long-term Dmab use (5 to 9 years) experienced a ≥2-fold rise in CTX and/or PINP levels within 3 months of their first ZOL infusion. These patients required ongoing treatment with ZOL (≥2 infusions), in contrast to those with shorter Dmab exposure (≤5 years).48 However, other studies reported that serum CTX and P1NP levels increased significantly within 12 months after a single ZOL injection, regardless of whether prior Dmab treatment duration was ≤6 months or >6 months, yet these values remained within the postmenopausal reference range.41 In studies focusing on a single ZOL infusion following one course of Dmab, the average P1NP level before treatment was 53 ng/mL((95% CIs:28–78%), which declined to 36 ng/mL((95% CIs:22–49%) at 18 months, suggesting a significant reduction in P1NP concentration.49
The Impact on the Risk of Fractures and Other Adverse Reactions
The “rebound phenomenon” following Dmab discontinuation appears to be linked with an increased risk of clinical vertebral fractures (VFx). Several case reports and case series have documented VFx in patients who stopped Dmab, with most cases reported in women,52 though VFx in men53 and hip fractures54 have also been described. A population-based cohort study of 2594 patients showed a gradual rise in fracture risk corresponding to the time elapsed since the last Dmab injection.55 The cumulative fracture risk was 27.3 per 1000 within 4 weeks after discontinuation, increased to 32.2 per 1000 during weeks 4 to 16, and reached 42.4 per 1000 beyond 16 weeks. Evidence indicates that the risk of both clinical and multiple VFx increases significantly in patients who stop Dmab without follow-up BPs therapy. In contrast, BPs offer protection against VFx. Among the studies collected on sequential treatment with ZOL following the discontinuation of Dmab, a total of 5 prospective cohort studies33,40,41,45,47 and 9 retrospective observational studies34,35,39,42–44,48,49,51 assessed the risk of fractures, as presented in Table 2. In a 2-year cohort study on sequential ZOL treatment, three patients developed clinical VFx, one in the ZOL group (3.7%) and two in the Dmab group (6.7%).33 During a 3-year follow-up, no major non-vertebral fragility fractures were reported in the ZOL group, and only one patient sustained a metatarsal fracture.45 The follow-up was extended to 5 years, and no additional clinical or radiological VFx were observed in the ZOL group.47 However, in retrospective observational studies,Everts-Graber et al found that the incidence of VFx was lower in patients who received ZOL compared to those who received no follow-up treatment, with no significant difference between the ZOL group and those treated with other agents such as selective estrogen receptor modulators (SERMs) or different BPs.34 A retrospective study by Kadaru et al showed that the incidence of VFx was 5.5% in patients who received BPs after Dmab, significantly lower than the 21.1% observed in the untreated group. Notably, all cases of multiple VFx occurred in patients who did not receive follow-up treatment.43 This result aligns with findings from Tutaworn, Solling, and others,39–42 who reported no cases of multiple VFx in patients following sequential ZOL treatment. However, Everts-Graber et al observed a different pattern when analyzing patients by the number of prior Dmab injections. Among those who received ZOL after Dmab discontinuation, 9 patients developed VFx, including 4 cases involving multiple vertebrae. Of these, 1 patient had mid-term Dmab exposure (5 years), while the other 3 had undergone long-term treatment (7.5, 8, and 8.5 years).48 These findings suggest that the duration of Dmab use may influence the effectiveness of subsequent therapy and highlight a need for further investigation. Importantly, no cases of osteonecrosis of the jaw or atypical femoral fractures were reported among patients who received sequential ZOL. About half of the patients experienced symptoms resembling a transient acute-phase reaction, which were effectively relieved with symptomatic treatment using paracetamol.
The Related Factors Influencing the Efficacy of Sequential Zoledronic Acid Treatment After Discontinuation of Denosumab
One prevailing theory is that the “rebound phenomenon” observed after stopping Dmab may be caused by the reactivation of osteoclast precursors that remained dormant during treatment.56 Considering this rebound effect, long-term Dmab use is generally advised. However, there are specific situations in which discontinuation becomes necessary. These include the development of adverse drug reactions, cases where prolonged treatment has already raised bone density to a level where further reduction in fracture risk is unlikely,57 or when bone density reaches the upper half of the osteopenia range and the patient has a long life expectancy ahead. For patients who discontinue Dmab, follow-up anti-resorptive therapy should be initiated within the first year, along with close monitoring, as the majority of bone loss tends to occur within the initial 12 months post-discontinuation. Current evidence suggests that although sequential ZOL cannot fully preserve the BMD gains achieved with Dmab, it can retain more than half of the BMD increase at the lumbar spine, total hip, and femoral neck.34,39,42,43,50 Additionally, sequential treatment with ZOL appears to reduce the extent of rebound in BTMs to some degree.33,39,45 Still, variations exist among studies regarding the degree and duration of BMD preservation. These inconsistencies imply that certain underlying factors may influence the patient’s response to ZOL. To better understand these influences, we summarized the Dmab and ZOL treatment details from the included studies, as shown in Table 3.
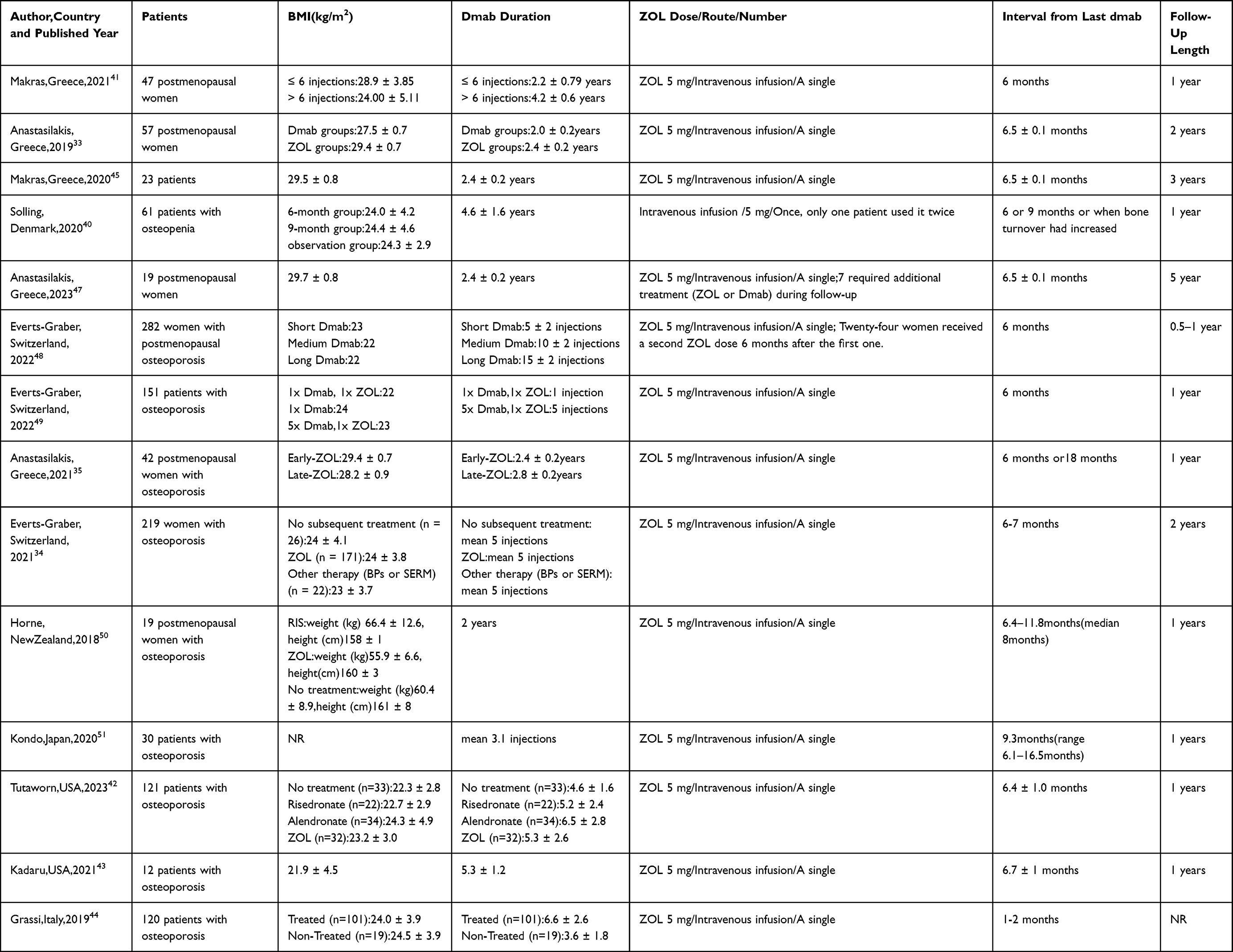 |
Table 3 Related Factors Affecting Curative Effect |
The Duration of Denosumab Use Before Sequential Zoledronic Acid Treatment
Makras et al divided postmenopausal women into two groups based on the number of prior Dmab infusions and administered a single ZOL infusion 6 months after the final Dmab dose. After one year, no significant changes in LS-BMD or femoral neck bone mineral density (FN-BMD) were observed in the ≤6 group (≤6 denosumab injections). In contrast, the >6 group (>6 injections) showed significant reductions in both LS-BMD and FN-BMD. These results suggest that the duration of Dmab therapy has a significant impact on the effectiveness of subsequent ZOL in maintaining BMD.41 Everts-Graber et al used more detailed groupings based on the number of Dmab injections: the “short-term” group (5±2 injections), the “medium-term” group (10±2), and the “long-term” group (15±2). Their findings showed that after Dmab discontinuation and sequential ZOL treatment, changes in BMD at the lumbar spine, total hip, and femoral neck differed significantly between the short-term and medium-term groups, with greater bone loss seen in the medium-term group. However, no significant difference in bone loss was found between the medium-term and long-term groups. The authors proposed that after 4–6 years of Dmab treatment, rebound-related bone loss may reach a plateau, regardless of how frequently ZOL is given afterward.48 Additionally, compared with patients who underwent short-term Dmab treatment (≤5 years), most individuals with longer treatment durations (5 to 9 years) required two or more ZOL infusions following Dmab discontinuation. The same study found that within 12 months after stopping Dmab, there were no significant differences in LS-BMD, total hip BMD(TH-BMD), or FN-BMD between women who received a single ZOL infusion and those who received two.48 In another study examining the effect of a single ZOL infusion following one Dmab injection, patients who received ZOL showed significant increases in LS-BMD, TH-BMD, and FN-BMD compared to those who received no BPs after Dmab. Furthermore, patients who had received only one Dmab injection before ZOL showed greater BMD increases at all measured sites than those who received five Dmab injections followed by ZOL.49 These findings suggest that the severity of the rebound phenomenon is closely linked to the duration of Dmab treatment. Long-term suppression of osteoclast differentiation by Dmab may lead to an expansion of the osteoclast precursor pool. Once Dmab is stopped, these precursors differentiate in a synchronized manner, triggering a sharp rise in BTMs and eventually resulting in the loss of BMD gains achieved during treatment.34 Therefore, a single 5 mg infusion of ZOL may not be sufficient to counter the bone resorption triggered by extended Dmab use.
Furthermore, related studies have shown that compared with placebo, patients treated with Dmab for 2–3 years exhibited a continued increase in matrix mineralization between years 2–3 and year 5, but no further increase was observed beyond the fifth year.58 This suggests that by year 5 of Dmab treatment, additional minerals had been incorporated into the bone matrix, contributing to a reduction in bone remodeling. However, when Dmab was discontinued and followed by ZOL infusion, the resulting changes in BTMs were sufficient to preserve the newly added mineral content in patients treated for 2–3 years, but not enough to fully retain the higher mineral loads in patients treated for more than 5 years. As a result, patients in the former group maintained bone density, while those in the latter experienced BMD loss.58 This finding was supported by other studies.41,48 Makras et al further confirmed that patients who received more than 6 Dmab injections experienced a significant decrease in LS-BMD compared to those who had 6 or fewer injections. A negative correlation was found between the duration of Dmab use and percentage change in LS-BMD.41 Similarly, Everts-Graber et al observed that patients who received 10±2 Dmab injections had greater BMD loss after transitioning to ZOL than those with 5±2 injections. Interestingly, those who received ≥15±2 injections did not show further bone loss, suggesting that rebound-related BMD decline may level off after 4–6 years of Dmab treatment.48 Additionally, one study found that patients who received a single Dmab injection followed by ZOL had greater increases in LS-BMD, TH-BMD, and FN-BMD than those who received five Dmab injections before switching to ZOL.49 This indirectly suggests that the duration of Dmab therapy can influence the effectiveness of subsequent ZOL treatment. The results also imply that if ZOL is administered at a time when a large number of bone multicellular units (BMUs) are active, it can achieve sufficient and sustained suppression of bone turnover.
The Time Points for Sequential Zoledronic Acid Treatment
Beyond the timing of the final Dmab injection, the timing of the subsequent ZOL infusion is also a key clinical consideration. Anastasilakis et al compared ZOL infusions administered 6 months and 18 months after the last Dmab dose over a one-year period. The study showed that delayed ZOL infusion at 18 months led to a notable overall decline in BMD, particularly at the lumbar spine.35 Solling et al conducted a more detailed subgroup analysis by administering ZOL at 6 months, 9 months, or at the time when BTMs were elevated. Although all groups experienced BMD loss, there were no significant differences in the average percentage changes in LS-BMD, TH-BMD, and FN-BMD across the different time points. However, the 6-month group generally had a slower rate of bone loss, while BMD reduction, especially at the hip, was more pronounced when ZOL infusion was delayed beyond 6 months.40 Earlier hypotheses suggested that the suppression of bone remodeling by the last Dmab injection could limit the number of active bone resorption surfaces available for intravenous BPs like ZOL to bind, potentially reducing their effectiveness. Based on this, it was proposed that administering ZOL when a greater number of BMUs were active, indicated by elevated BTMs, could lead to more effective and lasting inhibition of bone turnover.59 However, findings from two randomized trials showed that ZOL effectively suppressed bone turnover regardless of whether it was administered before or after the onset of the rebound phenomenon, with similar reductions in BTMs in both cases.33,40 Still, the 6-month group consistently showed a slower rate of BMD loss, while delays beyond 6 months were associated with more substantial reductions in BMD, particularly at the hip.40 Additionally, when ZOL was administered to patients experiencing rebound high bone turnover following Dmab discontinuation, its suppressive effect on BTMs lasted for at least 12 months, similar to the pattern observed in postmenopausal osteoporotic women receiving annual ZOL infusions.60 This suggests that administering ZOL during periods of abundant bone binding sites, such as when activated BMUs rebound fully, does not offer additional benefit for improving BMD. Current studies support the view that a 6-month interval between the last Dmab injection and the ZOL infusion is optimal, regardless of BTMs levels.61 This conclusion aligns with the findings of Anastasilakis et al, who reported that ZOL administered 6 months after the final Dmab dose effectively limited bone loss in many patients, making it a safer and more practical clinical choice.35 Makras et al further proposed that the severity of the patient’s disease might influence both the response to Dmab and the rebound risk. More advanced disease often requires longer treatment durations, and upon discontinuation, BMD tends to decline more significantly, often returning closer to baseline.41 In a prospective pilot study, Laroche et al investigated whether gradually tapering the Dmab dose could help prevent bone loss. After a final 60 mg injection, the dose was reduced to 30 mg at 6 months and to 15 mg at 12 months. One year after the last 15 mg dose, the initial LS-BMD gain was maintained at approximately 39%. However, BMD loss at the hip offset the initial gain. These findings indicate that while tapering the Dmab dose does not prevent hip bone loss, it can help preserve part of the initial spinal BMD increase.46 Currently, ZOL alone cannot fully retain the BMD gains following Dmab discontinuation. On the other hand, gradual dose reduction of Dmab retains around 40% of spinal BMD gain. This opens up the possibility that a combination strategy, ZOL paired with low-dose Dmab, may warrant further investigation.
Conclusion
Over the past few decades, as the population has gradually aged, the incidence of osteoporosis has steadily increased. The loss of bone strength raises the risk of brittle fractures in both spinal and non-spinal regions, accompanied by high mortality, greater healthcare service usage, rising medical costs, and a decline in quality of life. Dmab effectively suppresses BTMs, increases BMD, lowers fracture risk, and demonstrates a favorable safety profile. However, in certain cases, discontinuation of Dmab may be required. These include the occurrence of adverse effects, achievement of a BMD level at which further fracture risk reduction is unlikely, attainment of a high bone mass status following treatment with Dmab in patients with a long remaining life expectancy, and financial constraints. Nonetheless, stopping Dmab can result in a rapid loss of BMD and has been linked to multiple VFx in a subset of patients. This condition is referred to as the “rebound phenomenon.” To reduce the likelihood of this outcome, sequential administration of ZOL following Dmab discontinuation is recommended. This approach can partially preserve the BMD gains achieved with Dmab, dampen the rebound increase in BTMs, and offer some protection against VFx. Currently,there is no established consensus regarding the optimal timing for initiating ZOL following discontinuation of Dmab. Further validation through large-scale,rigorously designed randomized controlled trials is warranted. Nevertheless, based on existing evidence, we propose that it is important to monitor markers of bone metabolism, BMD, serum calcium, vitamin D, and other relevant parameters,within 3 to 6 months after ZOL administration. If BTMs rebound or BMD declines, further intervention with another dose of ZOL or alternative bone-protective agents (such as teriparatide) should be considered. The clinical pathway is illustrated in Figure 2.
 |
Figure 2 A clinical pathway figure of sequential treatment of zoledronic acid after denosumab discontinuation. Abbreviations: ZOL, zoledronic acid; Dmab, denosumab; BMD, bone mineral density; BTMs, bone transformation markers; BP, bisphosphonate. |
Although our review is the first to focus on the sequential use of BPs following Dmab discontinuation, it has certain limitations and presents challenges that call for further investigation. First, most studies examining ZOL after stopping Dmab are small-scale observational studies, often with limited participant numbers and variability in race, background, and age. Consequently, future research should include larger, regionally diverse, population-based randomized controlled trials to better analyze these observations. Second, existing studies offer limited data on the duration of Dmab use before discontinuation and on the optimal timing for initiating sequential ZOL. The grouping in these studies tends to be broad. Future investigations should widen the study scope, refine group classifications, and examine potential factors influencing patient response to ZOL, to increase both clinical applicability and therapeutic relevance of this regimen. Additionally, although ZOL has shown effects in maintaining BMD and reducing BTMs rebound, few studies have assessed parameters such as bone trabecular score(BTS), serum calcium, phosphorus, and vitamin D levels. Lastly, inconsistencies in measurement timing, indicator accuracy, and intervention timing across studies may also influence clinical outcomes. Despite these limitations, the findings and shortcomings outlined in this review may help guide the design of future clinical trials.
In conclusion, in most postmenopausal osteoporosis patients treated with Dmab, discontinuation of the drug leads to a “rebound phenomenon”, resulting in BMD loss and, in some cases, multiple fractures. Intravenous infusion of ZOL after the final Dmab injection can retain more than half of the BMD gain and has not been shown to be significantly associated with multiple VFx. However, the effectiveness of this sequential approach can be influenced by several factors, including the timing of the ZOL infusion, the duration of prior Dmab treatment, and the patient’s disease status. Therefore, patients transitioning from Dmab to ZOL should be managed with an individualized plan that includes regular assessment of BMD, monitoring of BTMs, and a comprehensive evaluation of clinical risk factors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Chin KY, Kamaruddin AA, Low NY, et al. Effects of age, sex, and ethnicity on bone health status of the elderly in KualaLumpur, Malaysia. Clin Interventions Aging. 2016;11:767–773. doi:10.2147/CIA.S108772
2. World Health Organization. WHO Scientific Group on the Assessment of Osteoporosis at Primary Health Care Level. Belgium May.Brussels. 2004. 5–7.
3. Blain H, Masud T, Dargent-Molina P, et al. A comprehensive fracture prevention strategy in older adults: the European Union Geriatric Medicine Society (EUGMS) statement. J Nutr Health Aging. 2016;20(6):647–652. doi:10.1007/s12603-016-0741-y
4. Migliaccio S, Falcone S, Spera G. Bone modeling and remodeling: from biology to clinical application. Aging Clin Exp Res. 2004;16(Suppl. S3):20–22.
5. Rousculp MD, Long SR, Wang SS, et al. Economic burden of osteoporosis‐related fractures in Medicaid. Value Health. 2007;10(2):144–152. doi:10.1111/j.1524-4733.2006.00161.x
6. De Vincentis AB, Bellelli G, Bravi M, et al. Management of Hip fracture in the older people: rationale and design of the Italian consensus on the orthogeriatric co‐management. Aging Clin Exp Res. 2020;32(7):1393–1399. doi:10.1007/s40520-020-01574-4
7. Cecere AB, Toro G, De CA, et al. How to improve the outcomes of surgically treated proximal humeral osteoporotic fractures? A narrative review. Orthop Rev. 2020;12(2):8529. doi:10.4081/or.2020.8529
8. McClung M, Harris ST, Miller PD, et al. Bisphosphonate therapy for osteoporosis: benefits, risks and drug holiday. Am J Med. 2013;126(1):13–20. doi:10.1016/j.amjmed.2012.06.023
9. Vescini F, Attanasio R, Balestrieri A, et al. Italian association of clinical endocrinologists (AME) position statement, drug therapy of osteoporosis. J Endocrinol Invest. 2016;39(7):807–834. doi:10.1007/s40618-016-0434-8
10. Iolascon G, Moretti AToro G, Toro G, et al. Pharmacological therapy of osteoporosis: whatʹs new? Clin Interv Aging. 2020;26(15):485–491. doi:10.2147/CIA.S242038
11. Miller PD, Bolognese MA, Lewiecki EM, et al. Effect of denosumab on bone density and turnover in postmenopausal women with low bone mass after long-term continued, discontinued, and restarting of therapy: a randomized blinded phase 2 clinical trial. Bone. 2008;43(2):222–229. doi:10.1016/j.bone.2008.04.007
12. Nakamura T, Matsumoto T, Sugimoto T, et al. Clinical trials express: fracture risk reduction with denosumab in Japanese postmenopausal women and men with osteoporosis: denosumab fracture intervention randomized placebo controlled Trial (DIRECT). J Clin Endocrinol Metab. 2014;99(7):2599–2607. doi:10.1210/jc.2013-4175
13. Kostenuik PJ, Nguyen HQ, McCabe J, et al. Denosumab, a fully human monoclonal antibody to RANKL, inhibits bone resorption and increases BMD in knock-in mice that express chimeric (murine/human) RANKL. J Bone Mineral Res. 2009;24(2):182–195. doi:10.1359/jbmr.081112
14. Kearns AE, Khosla S, Kostenuik PJ. Receptor activator of nuclear factor kappaB ligand and osteoprotegerin regulation of bone remodeling in health and disease. Endocr Rev. 2008;29(2):155–192. doi:10.1210/er.2007-0014
15. Sanchez A, Brun LR, Salerni H, et al. Effect of denosumab on bone mineral density and markers of bone turnover among postmenopausal women with osteoporosis. J Osteoporos. 2016;2016:8738959. doi:10.1155/2016/8738959
16. Deeks ED. Denosumab: a review in postmenopausal osteoporosis. Drugs Aging. 2018;35(2):163–173. doi:10.1007/s40266-018-0525-7
17. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–765. doi:10.1056/NEJMoa0809493
18. Hanley DA, Adachi JD, Bell A, Brown V. Denosumab: mechanism of action and clinical outcomes. Int J Clin Pract. 2012;66(12):1139–1146. doi:10.1111/ijcp.12022
19. Bone HG, Wagman RB, Brandi ML, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open‐label extension. Lancet Diabetes Endocrinol. 2017;5(7):513–523. doi:10.1016/S2213-8587(17)30138-9
20. Bone HG, Bolognese MA, Yuen CK, et al. Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. J Clin Endocrinol Metab. 2011;96(4):972–980. doi:10.1210/jc.2010-1502
21. McClung MR, Wagman RB, Miller PD, Wang A, Lewiecki EM. Observations following discontinuation of long-term denosumab therapy. Osteoporos Int. 2017;28(5):1723–1732. doi:10.1007/s00198-017-3919-1
22. Anastasilakis AD, Yavropoulou MP, Makras P, et al. Increased osteoclastogenesis in patients with vertebral fractures following discontinuation of denosumab treatment. Eur J Endocrinol. 2017;176(6):677–683. doi:10.1530/EJE-16-1027
23. Anastasilakis AD, Polyzos SA, Makras P, Aubry-Rozier B, Kaouri S, Lamy O. Clinical features of 24 patients with rebound associated vertebral fractures after denosumab discontinuation:systematic review and additional cases. J Bone Miner Res. 2017;32(6):1291–1296. doi:10.1002/jbmr.3110
24. Cummings SR, Ferrari S, Eastell R, et al. Vertebral fractures after discontinuation of denosumab: a post hoc analysis of the randomized placebo-controlled FREEDOM trial and its extension. J Bone Miner Res. 2018;33(2):190–198. doi:10.1002/jbmr.3337
25. Popp AW, Zysset PK, Lippuner K. Rebound-associated vertebral fractures after discontinuation of denosumab - from clinic and biomechanics. Osteoporos Int. 2016;27(5):1917–1921. doi:10.1007/s00198-015-3458-6
26. Cummings SR, Ferrari S, Eastell R, et al. Vertebral fractures after discontinuation of denosumab: a post hoc analysis of the randomized placebo-controlled FREEDOM trial and its extension. J Bone Miner Res. 2017;33(2):190–198. doi:10.1002/jbmr.3337
27. Lyu H, Yoshida K, Zhao SS, et al. Delayed denosumab injections and fracture risk among patients with osteoporosis: a population-based cohort study. Ann Intern Med. 2020;173(7):516–526. doi:10.7326/M20-0882
28. Cruchelow KR, Peter ME, Chakrabarti A, et al. Denosumab treatment lapses, discontinuation, and off-treatment fracture risk: a retrospective study of patients with osteoporosis in a real-world clinical setting. Bone. 2023;177:116925. doi:10.1016/j.bone.2023.116925
29. Cummings SR, Cosman F, Lewiecki EM, et al. Goaldirected treatment for osteoporosis: a progress report from the ASBMR-NOF working group on goal-directed treatment for osteoporosis. J Bone Miner Res. 2017;32(1):3–10. doi:10.1002/jbmr.3039
30. Tsourdi E, Langdahl B, Cohen-Solal M, et al. Discontinuation of denosumab therapy for osteoporosis: a systematic review and position statement by ECTS. Bone. 2017;105:11–17. doi:10.1016/j.bone.2017.08.003
31. Lewiecki EM. New and emerging concepts in the use of denosumab for the treatment of osteoporosis. Ther Adv Musculoskelet Dis. 2018;10(11):209–223. doi:10.1177/1759720X18805759
32. Meier C, Uebelhart B, Aubry-Rozier B, et al. Osteoporosis drug treatment: duration and management after discontinuation. A position statement from the Swiss Association against Osteoporosis (SVGO/ASCO). Swiss Med Wkly. 2017;147(3334):w14484. doi:10.4414/smw.2017.14484
33. Anastasilakis AD, Papapoulos SE, Polyzos SA, et al. Zoledronate for the prevention of bone loss in women discontinuing denosumab treatment. J Bone Miner Res. 2019;34(12):2220–2228. doi:10.1002/jbmr.3853
34. Everts-Graber J, Reichenbach S, Gahl B, et al. Risk factors for vertebral fractures and bone loss after denosumab discontinuation: a real-world observational study. Bone. 2021;144:115830. doi:10.1016/j.bone.2020.115830
35. Anastasilakis AD, Polyzos SA, Yavropoulou MP, et al. Comparative effect of zoledronate at 6 versus 18 months following denosumab discontinuation. Calcif Tissue Int. 2021;108. doi:10.1007/s00223-020-00785-1
36. Black DM, Reid IR, Boonen S, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res. 2012;27(2):243–254. doi:10.1002/jbmr.1494
37. Makras P, Papapoulos SE, Polyzos SA, et al. The three-year effect of a single zoledronate infusion on bone mineral density and bone turnover markers following denosumab discontinuation in women with postmenopausal osteoporosis. Bone. 2020;138:115478. doi:10.1016/j.bone.2020.115478
38. Kondo H, Okimoto N, Yoshioka T, et al. Zoledronic acid sequential therapy could avoid disadvantages due to the discontinuation of less than 3-year denosumab treatment. J Bone Miner Metab. 2020;38(6):894–902. doi:10.1007/s00774-020-01126-w
39. Everts-Graber J, Reichenbach S, Ziswiler HR, et al. A single infusion of zoledronate in postmenopausal women following denosumab discontinuation results in partial conservation of bone mass gains. J Bone Miner Res. 2020;35(7):1207–1215. doi:10.1002/jbmr.3962
40. Solling AS, Harslof T, Langdahl B. Langdahl B. treatment with zoledronate subsequent to denosumab in osteoporosis: a randomized trial. J Bone Miner Res. 2020;35(10):1858–1870. doi:10.1002/jbmr.4098
41. Makras P, Appelman-Dijkstra NM, Papapoulos SE. The duration of denosumab treatment and the efficacy of zoledronate to preserve bone mineral density after its discontinuation. J Clin Endocrinol Metab. 2021;106(10):e4155–e4162. doi:10.1210/clinem/dgab321
42. Tutaworn T, Nieves JW, Wang Z, Levin JE, Yoo JE, Lane JM. Bone loss after denosumab discontinuation is prevented by alendronate and zoledronic acid but not risedronate: a retrospective study. Osteoporos Int. 2023;34(3):573–584. doi:10.1007/s00198-022-06648-9
43. Kadaru T, Shibli-Rahhal A. Tarun Kadaru,Amal shibli-rahhal.zoledronic acid after treatment with denosumab is associated with bone loss within 1 year. J Bone Metab. 2021;28(1):51–58. doi:10.11005/jbm.2021.28.1.51
44. Grassi G, Chiodini I, Palmieri S, et al. Bisphosphonates after denosumab withdrawal reduce the vertebral fractures incidence. Eur J Endocrinol. 2021;185(3):387–396. doi:10.1530/EJE-21-0157
45. Makras P, Papapoulos SE, Polyzos SA, Appelman-Dijkstra NM, Anastasilakis AD, et al. The three-year effect of a single zoledronate infusion on bone mineral density and bone turnover markers following denosumab discontinuation in women with postmenopausal osteoporosis. Bone. 2020;138:115478. doi:10.1016/j.bone.2020.115478
46. Laroche M, Couture G, Degboé Y. Michel laroche,guillaume couture,yannick degboé.discontinuation of denosumab: gradual decrease in doses preserves half of the bone mineral density gain at the lumbar spine. JBMR Plus. 2023;7(7):e10731. doi:10.1002/jbm4.10731
47. Anastasilakis AD, Makras P, Polyzos SA, Papapoulos SE. The five-year effect of a single zoledronate infusion on bone mineral density following denosumab discontinuation in women with postmenopausal osteoporosis. Calcif Tissue Int. 2023;113(4):469–473. doi:10.1007/s00223-023-01119-7
48. Everts-Graber J, Reichenbach S, Gahl B. Effects of zoledronate on bone mineral density and bone turnover after long-term denosumab therapy: observations in a real-world setting. Bone. 2022;163:116498. doi:10.1016/j.bone.2022.116498
49. Everts-Graber J, Lehmann T. Bone Mass Gains After One Denosumab Injection Followed by Zoledronate. J Clin Densitom. 2022;25(3):293–298. doi:10.1016/j.jocd.2022.03.001
50. Horne AM, Mihov B, Reid IR. Bone loss after romosozumab/denosumab: effects of bisphosphonates. Calcif Tissue Int. 2018;103(1):55–61. doi:10.1007/s00223-018-0404-6
51. Kondo H, Okimoto N, Yoshioka T, et al. Zoledronic acid sequential therapy could avoid disadvantages due to the discontinuation of less than 3-year denosumab treatment. J Bone Miner Metab. 2020;38(6):894–902. doi:10.1007/s00774-020-01126-w
52. Aubry-Rozier B, Gonzalez-Rodriguez E, Stoll D, Lamy O. Severe spontaneous vertebral fractures after denosumab discontinuation: three case reports. Osteoporos Int. 2016;27(5):1923–1925. doi:10.1007/s00198-015-3380-y
53. Anagnostis P, Paschou SA, Gonzalez-Rodriguez E. Spontaneous vertebral fractures in males with osteoporosis after denosumab discontinuation: a report of two cases. J Clin Rheumatol. 2021;27(8S):S581–S584. doi:10.1097/RHU.0000000000000979
54. Sosa Henríquez M, Gómez de Tejada Romero MJ, Escudero-Socorro M, Torregrosa Suau O. Hip fractures following denosumab discontinuation: three clinical cases reports. J R Soc Med. 2019;112(11):472–475. doi:10.1177/0141076819861027
55. Lyu H, Yoshida K, Zhao SS, et al. Delayed denosumab injections and fracture risk among patients with osteoporosis. Ann Intern Med. 2020;173(7):516–526. doi:10.7326/M20-0882
56. McClung MR. Cancel the denosumab holiday. Osteoporos Int. 2016;27(5):1677–1682. doi:10.1007/s00198-016-3553-3
57. Ferrari S, Libanati C, Lin CJF. Relationship between bone mineral density t-score and nonvertebral fracture risk over 10 years of denosumab treatment. J Bone Miner Res. 2019;34(6):1033–1040. doi:10.1002/jbmr.3722
58. Dempster DW, Brown JP, Fahrleitner-Pammer A. Effects of long-term denosumab on bone histomorphometry and mineralization in women with postmenopausal osteoporosis. J Clin Endocrinol Metab. 2018;103(7):2498–2509. doi:10.1210/jc.2017-02669
59. Reid IR, Horne AM, Mihov B, Gamble GD. Bone loss after denosumab: only partial protection with zoledronate. Calcif Tissue Int. 2017;101(4):371–374. doi:10.1007/s00223-017-0288-x
60. Black DM, Delmas PD, Eastell R. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007;356(18):1809–1822. doi:10.1056/NEJMoa067312
61. Tsourdi E, Zillikens MC, Meier C. Fracture risk and management of discontinuation of denosumab therapy: a systematic review and positionstatement by ECTS. J Clin Endocrinol Metab. 2020;dgaa756. doi:10.1210/clinem/dgaa756
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impacts of Prior Anti-Osteoporosis Treatments on Sequential Denosumab Responses in BMD Changes Among Postmenopausal Osteoporosis Women in East China: Real-World Data Analysis
Guan G, Du Y, Tang W, Chen M, Yu W, Li H, Cheng Q
Clinical Interventions in Aging 2025, 20:573-586
Published Date: 8 May 2025
Synergistic Efficacy of Calcitriol Combined with Denosumab versus Calcitriol Alone in Postmenopausal Osteoporosis: A Retrospective Cohort Study
Li X, Hu M, Shen Y
International Journal of Women's Health 2026, 18:599348
Published Date: 22 May 2026