Back to Journals » Clinical Interventions in Aging » Volume 15
Effectiveness of Neuromuscular Electrical Stimulation on Post-Stroke Dysphagia: A Systematic Review of Randomized Controlled Trials
Authors Alamer A ![]() , Melese H
, Melese H ![]() , Nigussie F
, Nigussie F ![]()
Received 23 May 2020
Accepted for publication 31 July 2020
Published 3 September 2020 Volume 2020:15 Pages 1521—1531
DOI https://doi.org/10.2147/CIA.S262596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Abayneh Alamer,1 Haimanot Melese,1 Fetene Nigussie2
1Department of Physiotherapy, School of Medicine, College of Health Sciences, Mekelle University, Mekelle, Ethiopia; 2Department Of Nursing Institute of Medicine, College of Health Sciences, DebreBerhan University, Debre Berhan, Ethiopia
Correspondence: Abayneh Alamer
Mekelle University, Ethiopia
Tel +251922276256
Fax +251344416681/9
Email [email protected]
Abstract: The purpose of this review was to summarize the latest best scientific evidence on the efficacy of neuromuscular electrical stimulation on swallowing function in dysphagic stroke patients. A comprehensive systematic search of literature published between November 2014 and May 2020 was performed using the following electronic databases: PubMed/Medline, CINAHL, PEDro, Science Direct, Google Scholar, EMBASE, and Scopus. Only randomized controlled trials (RCT) evaluating the effect of neuromuscular electrical stimulation on swallowing function in dysphagic stroke patients were included. Physiotherapy Evidence Database (PEDro) has been used to evaluate the risk of bias of included trials. This review was reported in accordance with PRISMA statement guideline. The methodological quality of the studies was determined using PEDro scale and GRADE approach. Evidence of overall quality was graded from moderate to high. Eleven RCTs involving 784 patients were analyzed. The primary outcome measures of this review were functional dysphagia scale (FDS) and standard swallowing assessment. This review found neuromuscular electrical stimulation (NMES) coupled with traditional swallowing therapy could be an optional intervention to improve swallowing function after stroke in rehabilitation department.
Keywords: swallowing dysfunction, stroke, neuromuscular electrical stimulation; NMES, systematic review
Introduction
Dysphagia is an irregular swallowing pattern or bolus flow disturbance from the mouth to esophagus and is a serious problem in various neurological conditions.1,2 Stroke is one of the most common neurological causes of dysphagia.1,3 After a stroke, dysphagia is a major health problem observed during the first 2–4 weeks with a prevalence of 29–81%.3–5 Dysphagia causes an increased risk of malnutrition, dehydration, aspiration pneumonia, and even death.3–7 These complications can delay functional recovery and reduce quality of life when patients are unable to eat or drink.
Treatment of dysphagia relies on traditional swallowing training, behavioral training and pharmacological therapies that focus on enhancing sensory feedback from the oropharynx to the central pattern generator, strengthening the disused or pharyngeal musculature, preventing atrophy and reduced motor output from the central pattern generator, and minimizing symptoms through the use of compensatory postural adjustments.8–11 Nowadays, numerous adjunctive treatment options have gained attention that may theoretically improve the recovery of dysphagia. These treatments include; repetitive transcranial magnetic stimulation and transcranial direct current stimulation, surface neuromuscular electrical stimulation (NMES), which is commonly used in rehabilitation department.12–15
(NMES is widely used for the treatment of pain management, muscle strengthening and sensorimotor recovery.16 NMES can be used to stimulate muscle contractions and/or activate sensory pathways through “motor”, and “sensory stimulation” that cause a depolarization of the peripheral motor nerve, usually in the neuromuscular junction or motor end plate.17–19 It also works peripherally on the neuromuscular system in an effort to reinforce damaged oropharyngeal musculature by using surface electrodes which trigger muscle contraction by depolarizing nerve fibers on neck muscles.19–21 While it has been presumed that NMES can enhance the strength of pharyngeal muscles after stroke, its clinical efficacy remains uncertain. Three meta-analysis studies that examined the efficacy of NMES for dysphagia have been reported and the findings confirmed its use.22–24 However, such meta-analysis included studies with different dysphagia etiologies and pooled data from studies with different outcomes. Conversely, two reviews reported that NMES alone was not preferable to swallowing therapy.23,25 As a result, it is difficult to interpret the efficacy of NMES for post-stroke dysphagia. In addition, prior reviews had included non-randomized controlled trials (RCTs), and limited number of articles which considerably, affect the strength of outcome. In view of these limitations in the previous studies, conclusive conclusions on NMES therapy could not be taken. Therefore, an updated review of recent and large numbers of RCTs should be conducted to evaluate the efficacy of NMES in the treatment of post-stroke dysphagia. The purpose of this review was to synthesize the efficacy of NMES on swallowing function in subjects with post-stroke dysphagia in a systematic manner on recent RCTs.
Methods
Study Design
This systematic review was performed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.26
Search Strategy
A literature review has been carried out to determine all qualifying RCTs. An online literature query was undertaken to recognize appropriate studies from the following databases; PubMed/MEDLINE, CINAHL, PEDro, Science Direct, Google Scholar, EMBASE, and Scopus. The keywords used to search journal articles were: “stroke/cerebrovascular accident/post-stroke”, “Dysphagia”, “swallowing difficulty”, “NMES”, and “RCTs”. The retrieval of the studies for the articles was carried out between November 2010 and May 2020. Manual searches were also performed from the reference list of included documents.
Eligibility Criteria
For inclusion the studies had to meet the following PICO criteria: All RCTs conducted to determine the efficacy of NMES on dysphagia in post-stroke patients. Only full-text articles published in English, in a peer reviewed journals have been included. Observational research, quasi-experimental studies and conference abstracts were excluded from this study. Studies involving patients in dysphagia with conditions other than stroke disorders have been eliminated from this review. Studies examined NMES, and/or NMES combined with conventional swallowing therapy irrespective of the duration of the intervention was provided or the outcome(s) measured were included. Comparison group of any conventional swallowing therapies (lingual-strengthening exercises, effortful swallowing training, laryngeal adduction-elevation exercises, pharmacological therapy, acupuncture therapy), placebo/sham stimulations or control were considered appropriate. Studies included were expected to declare an outcome indicator of swallowing functions and/or complication.
Study Selection
One reviewer (A.A.) performed the electronic database searches and screened the titles and abstracts. Two reviewers (A.A. and H.M.) have retrieved and independently reviewed the potential eligible articles. The studies were retrieved in detail through methodological quality and data extraction tools. The third reviewer (F.N.) was there to solve the disagreements between the two reviewers.
Risk of Bias in Individual Studies
The quality assessment of the individual studies was carried out by two independent reviewers on the basis of the Physiotherapy Evidence Database (PEDro) scale. This scale is valid and reliable tool which used to evaluate the methodological consistency of the 10-item studies and contains the first item to assess the external validity of the studies.27,28 The PEDro scale assesses the methodological quality of a study based on important criteria, such as concealed allocation, intention-to-treat analysis, and adequacy of follow up. These characteristics make the PEDro scale a useful tool to assess the methodological quality of physical therapy and rehabilitation trials. The overall quality of the evidence and the strength of recommendations have been evaluated using the GRADE approach.29 The GRADE approach defines four levels of quality (high, moderate, low and very low). The overall evidence was downgraded based on the existence of five factors: limitations (due to risk of bias); quality of results; directness (e.g., whether participants are similar to those about whom conclusions are drawn); precision (i.e., sufficient data to produce narrow confidence intervals); and other (e.g., publication bias).
Data Extraction
Data were extracted by using the PICO approach: 1) Participants; post-stroke dysphagia/difficulty of swallowing; 2) Interventions – NMES and/or combined with conventional swallowing therapy; 3) Comparison; conventional swallowing therapies (lingual-strengthening exercises, effortful swallowing training, laryngeal adduction-elevation exercises, pharmacological therapy, acupuncture therapy), placebo/sham stimulations were considered; and 4) Outcomes; swallowing functions and/or complication. Two reviewers (H.M. and A.A.) extracted the data independently and the extracted data were checked by the third author (F.N.). Disagreements were resolved by consensus between the three review authors. The following data were extracted from each RCT: Author's name and year of publication, stroke definition (Stroke and dysphagia severity measure, type and duration), number of participants in treatment and control group, types of treatments, both in experimental and control group, mean follow up time, mean age of the participants and treatment outcomes (baseline, follow-up and post-intervention). The effectiveness of interventions for each outcome, mean and standard deviations of the outcome measures at baseline, post- intervention, and during follow-ups were extracted.
Results
Study Selection
A total of 852 articles were recognized by the searching strategy. After adjusting for duplicates 600 were remained. After title and abstract screening of studies, 520 studies were expelled. After full content screening out of 40 articles, 11 RCTs were included in this review. (Figure 1.)
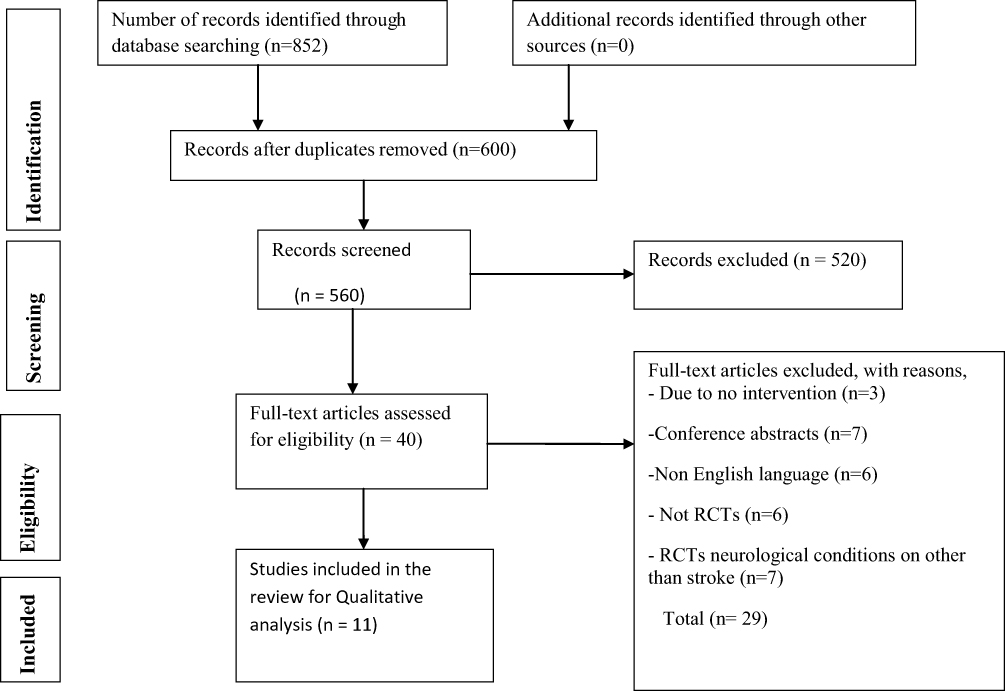 |
Figure 1 Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram. |
Characteristics of Included Studies
These studies have been published between 2014 through 2019. All eleven studies evaluated the efficacy of NMES on swallowing functions of subjects with post stroke dysphagia. The detailed descriptions on characteristics and results of the included trials were presented in Table 1. The synthesized characteristics and outline of the results about the included studies, based on PICO standard, are shown below.
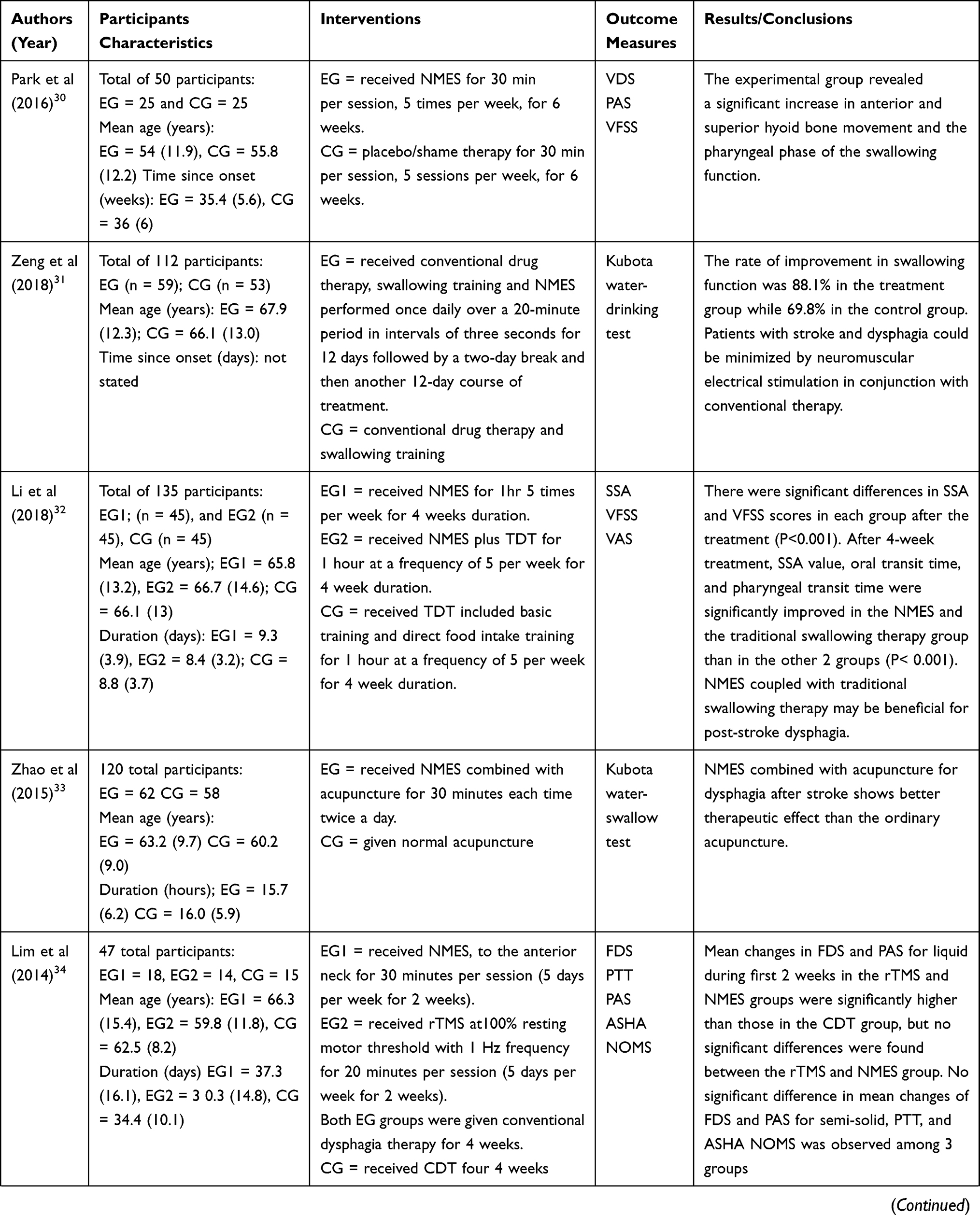 | 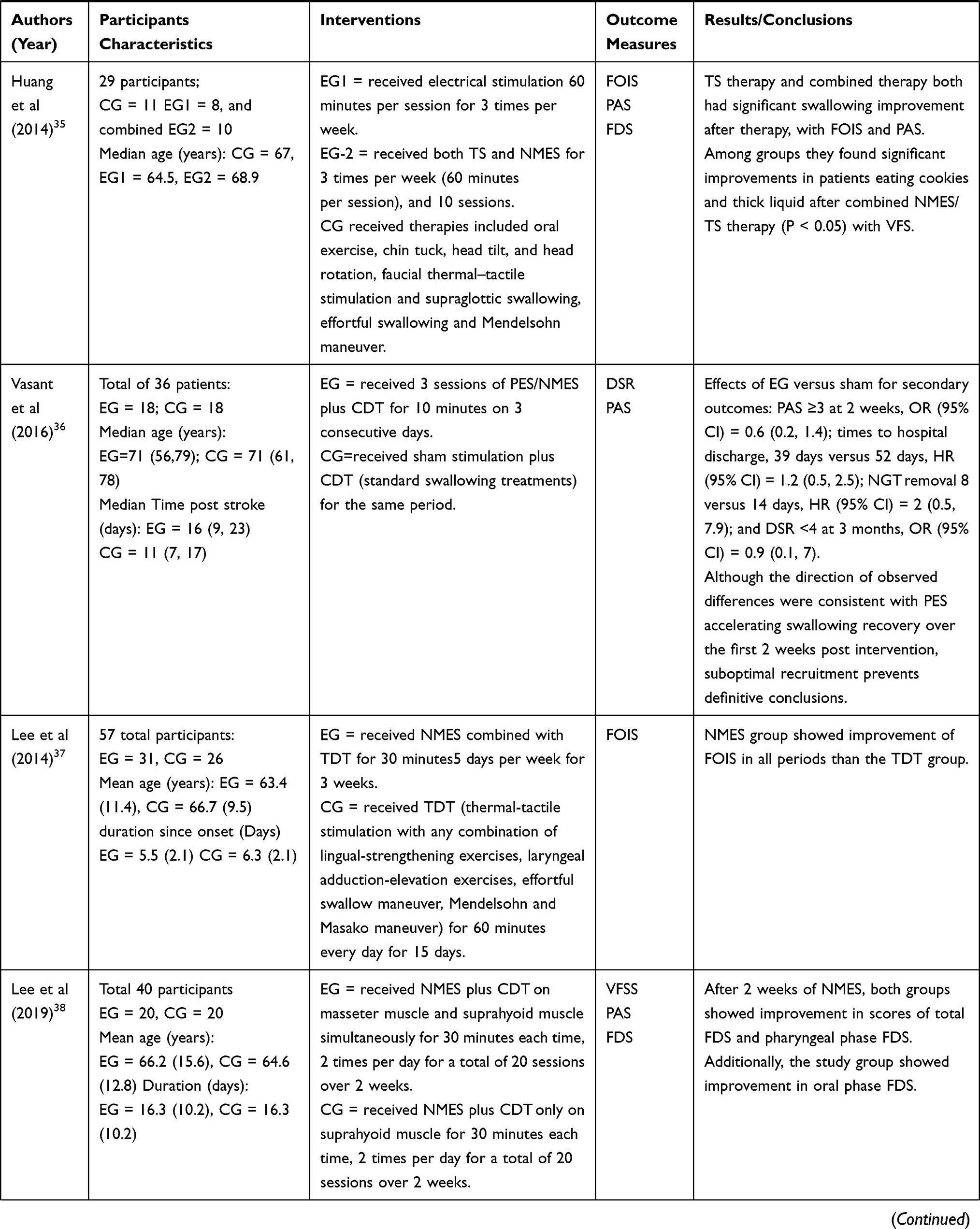 | 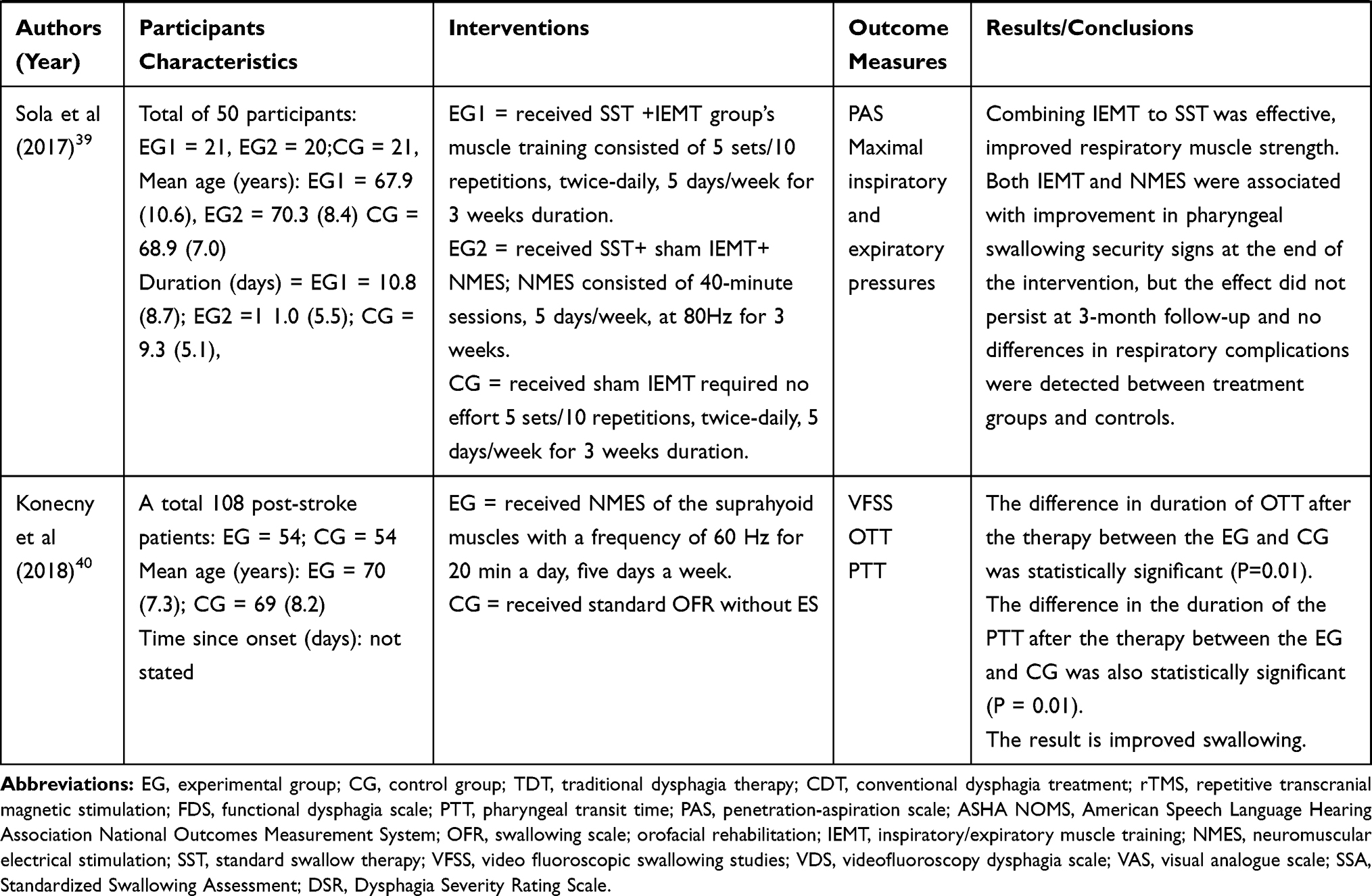 |
Table 1 Summary of Included Randomized Controlled Trials |
Participants
Eleven RCTs with a total of 784 individual participants were analyzed. The mean age of participants in the experimental groups ranged from 54 (11.9)30 to 66.2 (15.6)31 and 55.8 (12.2)30 to 66.1 (13.1)32 in controlled groups. The mean duration of the stroke ranges 15.7 (6.2) hours33 to 35.4 (5.4) weeks30 in the experimental groups and 16.0 (5.9) hours33 to 36 (6) weeks30 in the controlled groups. The sample size of the participants in the included studies was ranged from 29 to 135 individuals, both in the experimental and control groups.34,35
Interventions
Studies comparing the effectiveness of nNMES, and/or conventional swallowing therapy with controlled group; conventional swallowing therapies, and/or placebo/sham stimulations were considered. The treatment duration ranged from 10–60 minutes for each session,35,36 2–5 times per week33,34,37 for a 2–6 week period.30,38
Outcome Measures
Data were extracted for the following outcomes: swallowing function and/or complications. The primary outcome measures of this review were functional dysphagia scale (FDS), video fluoroscopy dysphagia scale (VFDS) and standardized swallowing assessments (SSA). Of all included studies, 6 studies evaluated swallowing function by using PAS.30,34–36,38,39 Four studies evaluated swallowing function by using VFDS,30,32,38,40 and only three studies used FDS.34,35,38
Risk of Bias Within Studies
The summary of risk of bias within individual studies and its score is presented in Table 2. The PEDro score of all included studies was ranged from 5 to 9, with the mean score of 7. The overall methodological quality of the evidence was ranged from moderate to high. All included studies randomized the participants to experimental and controlled groups. All included studies had been evaluated group comparisons and point measures variability for at least one key outcome. Only two studies blinded the participants and therapists36,39 whereas; four studies blinded the assessor.32,34,36,39 Five studies had lost to adequate follow up,30,32-35 and six studies were assessed using intention to treat analysis.30,31,34,39,40 For all included studies the potential source of bias was blinding the participant, therapist, and assessor.
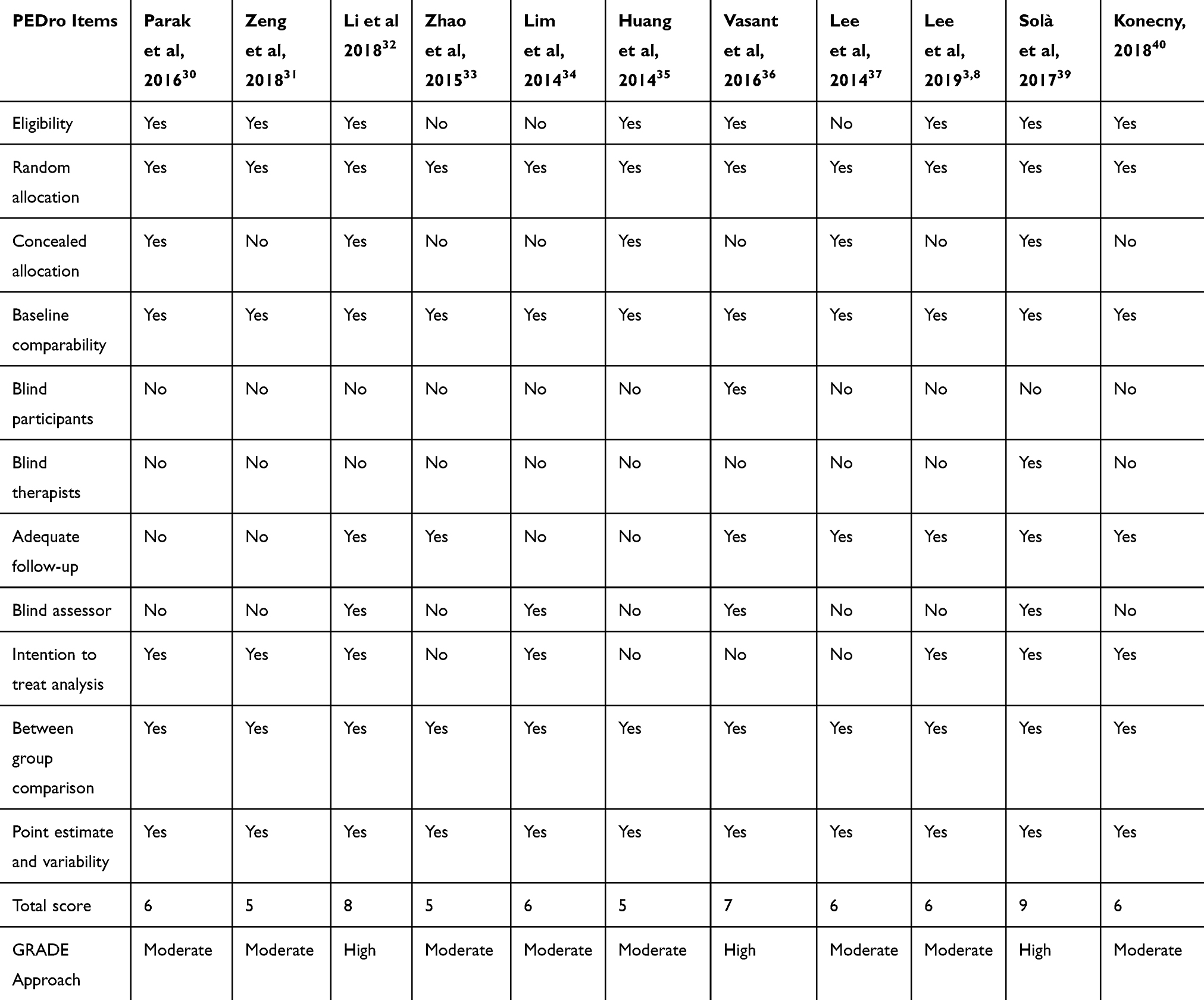 |
Table 2 Methodological Quality of Included Studies |
Effects of NMES on Swallowing Functions
Eleven RCTs; with a total of 784 individual participants were evaluated the post treatment effect of NMES on swallowing function in post-stroke dysphagia patients. Out of 11 studies, 10 of them (n=748) confirmed that NMES had increased swallowing function of post-stroke dysphagia patients compared to the control groups in all outcome measures.30,33–35,37–40 However, one study (n=36) indicated that the NMES had no observed differences between the experimental and control groups.36
Complications
On combining the results of all studies, no complications were reported.
Discussion
The purpose of this systematic review was to update and synthesize the most recent evidence on efficacy of NMES on swallowing function in subjects with post-stroke dysphagia. To the extent of our knowledge; there was lack of studies that investigated the effectiveness of the NMES on swallowing function in post-stroke dysphagia patients in systematic manner from recent high quality RCTs.
Most of the included studies confirmed that NMES was effective on swallowing function in post-stroke dysphagic patients. The overall methodological quality of included studies was rated moderate to high quality based on GRADE approach. The overall effects of NMES on the swallowing function of post-stroke dysphagic patients were evaluated for different durations of intervention.
The effect of NMES on swallowing functions was evaluated in eleven studies. Ten studies have confirmed that NMES helps to improve swallowing function in post-stroke dysphagic patients. A study conducted by Lee 2014,37 demonstrated that NMES showed a significant improvement on the FOIS after treatment. Both groups showed a significant improvement on the swallowing function following treatment on acute/sub acute dysphagic stroke patients. The FOIS score was significantly more improved at 3 and 6 weeks after baseline in the NMES/TDT group compared with the TDT group (p<0.05). Similarly, Huang et al's (2014)35 study observed substantial changes on swallowing functions in patients who had cookies and thick liquid after combined NMES/TS therapy (P<0.05) compared to TS therapy alone. In addition, the study done by Lim et al, 201434 stated that NMES could induce an early significant swallowing recovery from dysphagia relative to the conventional dysphagia treatment (CDT) groups. Moreover; the mean changes in FDS and PAS for liquid during first 2 weeks in the NMES and rTMS groups were significantly higher than those in CDT group, but no significant differences were found between the NMES and rTMS groups. Nevertheless; no significant difference in mean changes of FDS and PAS for semi-solid, pharyngeal transit time (PTT), and American Speech-Language Hearing Association National Outcomes Measurement System (ASHA NOMS) was observed among the three groups (rTMS, NMES, and CDT groups).
Zhao et al (2015)33 reported that NMES combined with acupuncture for dysphagia after stroke showed better therapeutic effect than the ordinary acupuncture. However, Vasant et al (2016)36 showed that NMES combined with standard swallowing treatment reported that no difference was observed between the interventional groups and control groups. This might be due to the fact that VFS measurement was not possible in all patients, given that a lack of a consistent test to determine dysphagia at baseline may have contributed to non-significant findings and difficulty of detecting clinically important treatment effect on the DSR. Similarly, a lack of a targeted number of participants in the final study (only reached 36% of its targeted number of patients), which led to a diminished ability of randomization to achieve balance on important prognostic factors. In contradiction to this, Jayasekeran et al (2010) study reported that pharyngeal electrical stimulation (PES) confirmed that it is a safe neurostimulation intervention that reverses swallowing disability after virtual lesion or stroke. This invariability might be due to the differences in the baseline characteristics of the participants between the trials.
A study by Park et al (2016)30 confirmed that NMES combined with effortful swallowing was effective in improving the pharyngeal phase of swallowing, and hyoid movement in stroke patients with dysphagia compared to effortful swallowing groups. Likewise, Park’s previous study (2012) confirmed its benefits for swallowing function of dysphagic stroke patients.41 The possible explanation might be the high-intensity NMES cause a strong depolarization of skeletal muscles and acts as a positive factor in the recovery of muscles required for swallowing. The muscles involved in swallowing consist of a greater number of type II muscle fibers than type I, and NMES is a strong stimulus for motor unit recruitment of type II fibers and evokes a contraction.42 A study done by Sola et al (2017)39 confirmed that NMES improved swallowing functions in sub acute stroke dysphagic patients, compared to standard swallow therapy, after 3-week intervention. But, no difference was observed at 3-month follow-up between the groups. This might be explained by the reversibility of the training effect and/or the natural evolution of dysphagia.43,44
A study done by Konecny et al (2018)40 showed that improvement of swallowing times (OTT and PTT) was significantly better in intervention group (NMES) compared to control groups. Despite this fact, the oral and PTTs improvement was observed in both groups after 4 weeks of therapy. Similar results were reported by two studies findings Permisirivanich et al45 and Ludlow et al.46 In contrast, Power et al47 found no changes in swallowing function were observed with NMES treatment. Likewise, Li et al (2018)32 suggested that NMES therapy combined with traditional swallowing therapy may be beneficial for post-stroke dysphagia. Similar findings were observed by two previous studies.48,49 The possible explanation might be electrical stimulation can increase pharyngeal and laryngeal activities by increasing the contraction force of hyoid bone muscle.50
A study done by Zeng et al (2018)31 reported that NMES and swallowing rehabilitation training together may significantly improve swallowing function which was consistent with the results of two similar studies conducted by Park et al,41 and Lim et al.51 A study done by Lee et al (2019)38 suggested that the application of NMES on masseter muscle had a therapeutic effect on oral dysfunction of patients after sub acute stroke. This might be due to chewing functional activities of this muscle might play an important role in stimulating the initiation of the swallowing process.
Taken together; the result of one study may indicate that NMES did not have a beneficial effect on swallowing. Nevertheless, based on the findings of 10 similar studies, a more plausible explanation noted that NMES combined with conventional swallowing therapy had a significant improvement on swallowing function of dysphagic stroke patients compared to the control groups.
Limitations
This review had the following limitations: this review was included only English language articles. Hence; there might be a chance of missing articles published in non-English languages. Due to heterogeneity of the interventions, to perform a meta-analysis was not possible.
Clinical Implication
This review suggests that NMES appears to result in improved outcomes swallowing function of dysphagia patients with stroke. Clinical decision making shall be based on the accessibility of NMES especially in resource-limited setting.
Conclusion
NMES has been found to improve the swallowing function of patients with dysphagia after stroke. Although this systematic review found that NMES is effective in improving swallowing function compared to other interventions, great attention is needed when NMES has been used for post- stroke dysphagic subjects such as; the course of disease duration and its severity. Further research should be conducted on NMES efficacy on chronic stroke patients with swallowing dysfunction.
Ethical Approval
Ethical approval or patient consent was not required since the present study was a review of previous published literature.
Disclosure
The authors declare there is no conflict of interest.
References
1. Lawrence ES, Coshall C, Dundas R, et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke. 2001;32(6):1279–1284. doi:10.1161/01.STR.32.6.1279
2. Youngs N. Effect of neuromuscular electrical stimulation on dysphagia in stroke patients; 2015.
3. Falsetti P, Acciai C, Palilla R, et al. Oropharyngeal dysphagia after stroke: incidence, diagnosis, and clinical predictors in patients admitted to a neurorehabilitation unit. J Stroke Cerebrovasc Dis. 2009;18(5):329–335. doi:10.1016/j.jstrokecerebrovasdis.2009.01.009
4. Mourão AM, Lemos SM, Almeida EO, et al. Frequency and factors associated with dysphagia in stroke. In: Codas. SciELO Brasil; 2016;28(1):66–70.
5. Cohen DL, Roffe C, Beavan J, et al. Post-stroke dysphagia: A review and design considerations for future trials. Int J Stroke. 2016;11(4):399–411. doi:10.1177/1747493016639057
6. Holas MA, DePippo KL, Reding MJ. Aspiration and relative risk of medical complications following stroke. Arch Neurol. 1994;51(10):1051–1053. doi:10.1001/archneur.1994.00540220099020
7. Finestone HM, Greene-Finestone LS, Wilson ES, et al. Malnutrition in stroke patients on the rehabilitation service and at follow-up: prevalence and predictors. Arch Phys Med Rehabil. 1995;76(4):310–316. doi:10.1016/S0003-9993(95)80655-5
8. Langmore SE. Efficacy of behavioral treatment for oropharyngeal dysphagia. Dysphagia. 1995;10(4):259–262. doi:10.1007/BF00431419
9. Miller RM, Langmore SE. Treatment efficacy for adults with oropharyngeal dysphagia. Arch Phys Med Rehabil. 1994;75(11):1256–1262. doi:10.1016/0003-9993(94)90015-9
10. Shapiro J. Oropharyngeal dysphagia: pathophysiology, clinical assessment and management. Rev Gastroenterol Mex. 1994;59(2):91–95.
11. Campbell-Taylor I. Oropharyngeal dysphagia in long-term care: misperceptions of treatment efficacy. J Am Med Dir Assoc. 2008;9(7):523–531. doi:10.1016/j.jamda.2008.06.001
12. Suiter DM, Leder SB, Ruark JL. Effects of neuromuscular electrical stimulation on submental muscle activity. Dysphagia. 2006;21(1):56–60. doi:10.1007/s00455-005-9010-7
13. Burnett TA, Mann EA, Stoklosa JB, et al. Self-triggered functional electrical stimulation during swallowing. J Neurophysiol. 2005;94(6):4011–4018. doi:10.1152/jn.00025.2005
14. Lefaucheur J-P, Antal A, Ayache SS, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. 2017;128(1):56–92. doi:10.1016/j.clinph.2016.10.087
15. Geeganage C, Beavan J, Ellender S, et al. Interventions for dysphagia and nutritional support in acute and subacute stroke. Cochrane Database Syst Rev. 2012;10.
16. Doucet BM, Lam A, Griffin L. Neuromuscular electrical stimulation for skeletal muscle function. Yale J Biol Med. 2012;85(2):201.
17. Bergquist A, Clair JM, Lagerquist O, et al. Neuromuscular electrical stimulation: implications of the electrically evoked sensory volley. Eur J Appl Physiol. 2011;111(10):2409. doi:10.1007/s00421-011-2087-9
18. Blumenfeld L, Hahn Y, LePage A, et al. Transcutaneous electrical stimulation versus traditional dysphagia therapy: a nonconcurrent cohort study. Otolaryngol Head Neck Surg. 2006;135(5):754–757. doi:10.1016/j.otohns.2006.04.016
19. Poorjavad M, Talebian Moghadam S, Nakhostin Ansari N, et al. Surface electrical stimulation for treating swallowing disorders after stroke: a review of the stimulation intensity levels and the electrode placements. Stroke Res Treat. 2014;2014:1–7. doi:10.1155/2014/918057
20. Park CL, O’Neill PA, Martin DF. A pilot exploratory study of oral electrical stimulation on swallow function following stroke: an innovative technique. Dysphagia. 1997;12(3):161–166. doi:10.1007/PL00009531
21. Shaw GY, Sechtem PR, Searl J, et al. Transcutaneous neuromuscular electrical stimulation (VitalStim) curative therapy for severe dysphagia: myth or reality? Ann Otol Rhinol Laryngol. 2007;116(1):36–44. doi:10.1177/000348940711600107
22. Carnaby-Mann GD, Crary MA. Examining the evidence on neuromuscular electrical stimulation for swallowing: a meta-analysis. Arch Otolaryngol Head Neck Surg. 2007;133(6):564–571. doi:10.1001/archotol.133.6.564
23. Tan C, Liu Y, Li W, et al. Transcutaneous neuromuscular electrical stimulation can improve swallowing function in patients with dysphagia caused by non‐stroke diseases: a meta‐analysis. J Oral Rehabil. 2013;40(6):472–480. doi:10.1111/joor.12057
24. Scutt P, Lee HS, Hamdy S, et al. Pharyngeal electrical stimulation for treatment of poststroke dysphagia: individual patient data meta-analysis of randomised controlled trials. Stroke Res Treat. 2015;2015:1–8. doi:10.1155/2015/429053
25. Chen Y-W, Chang K-H, Chen H-C, et al. The effects of surface neuromuscular electrical stimulation on post-stroke dysphagia: a systemic review and meta-analysis. Clin Rehabil. 2016;30(1):24–35. doi:10.1177/0269215515571681
26. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
27. Maher CG, Sherrington C, Herbert RD, et al. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
28. de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129–133. doi:10.1016/S0004-9514(09)70043-1
29. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 7. Rating the quality of evidence—inconsistency. J Clin Epidemiol. 2011;64(12):1294–1302. doi:10.1016/j.jclinepi.2011.03.017
30. Park JS, Oh D-H, Hwang N-K, et al. Effects of neuromuscular electrical stimulation combined with effortful swallowing on post‐stroke oropharyngeal dysphagia: a randomised controlled trial. J Oral Rehabil. 2016;43(6):426–434. doi:10.1111/joor.12390
31. Zeng Y, Yip J, Cui H, et al. Efficacy of neuromuscular electrical stimulation in improving the negative psychological state in patients with cerebral infarction and dysphagia. Neurol Res. 2018;40(6):473–479. doi:10.1080/01616412.2018.1451015
32. Li L, Li Y, Wu X, et al. The value of adding transcutaneous neuromuscular electrical stimulation (VitalStim) to traditional therapy for poststroke dysphagia: a randomized controlled trial. Top Geriatr Rehabil. 2018;34(3):200–206. doi:10.1097/TGR.0000000000000195
33. Zhao J-W, Wang Z-Y, Cao W-Z, et al. Therapeutic efficacy of swallowing neuromuscular electrical stimulation combined with acupuncture for post-stroke dysphagia. World J Acupunct Moxibustion. 2015;25(1):19–23. doi:10.1016/S1003-5257(15)30004-0
34. Lim K-B, Lee H-J, Yoo J, et al. Effect of low-frequency rTMS and NMES on subacute unilateral hemispheric stroke with dysphagia. Ann Rehabil Med. 2014;38(5):592. doi:10.5535/arm.2014.38.5.592
35. Huang K-L, Liu T-Y, Huang Y-C, et al. Functional outcome in acute stroke patients with oropharyngeal dysphagia after swallowing therapy. J Stroke Cerebrovasc Dis. 2014;23(10):2547–2553. doi:10.1016/j.jstrokecerebrovasdis.2014.05.031
36. Vasant DH, Michou E, O’Leary N, et al. Pharyngeal electrical stimulation in dysphagia poststroke: a prospective, randomized single-blinded interventional study. Neurorehabil Neural Repair. 2016;30(9):866–875. doi:10.1177/1545968316639129
37. Lee KW, Kim SB, Lee JH, et al. The effect of early neuromuscular electrical stimulation therapy in acute/subacute ischemic stroke patients with dysphagia. Ann Rehabil Med. 2014;38(2):153. doi:10.5535/arm.2014.38.2.153
38. Lee KW, Kim SB, Lee JH, et al. Effects of neuromuscular electrical stimulation for masseter muscle on oral dysfunction after stroke. Ann Rehabil Med. 2019;43(1):11. doi:10.5535/arm.2019.43.1.11
39. Guillén-Solà A, Messagi Sartor M, Bofill Soler N, et al. Respiratory muscle strength training and neuromuscular electrical stimulation in subacute dysphagic stroke patients: a randomized controlled trial. Clin Rehabil. 2017;31(6):761–771. doi:10.1177/0269215516652446
40. Konecny P, Elfmark M. Electrical stimulation of hyoid muscles in post-stroke dysphagia. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2018;162(1):40–42. doi:10.5507/bp.2017.043
41. Park J-W, Kim Y, Oh J-C, et al. Effortful swallowing training combined with electrical stimulation in post-stroke dysphagia: a randomized controlled study. Dysphagia. 2012;27(4):521–527. doi:10.1007/s00455-012-9403-3
42. Sella O, Jones RD, Huckabee M-L. Age and gender effects on submental motor-evoked potentials. Age. 2014;36(6):9735. doi:10.1007/s11357-014-9735-z
43. Smithard DG, O’Neill PA, England RE, et al. The natural history of dysphagia following a stroke. Dysphagia. 1997;12(4):188–193. doi:10.1007/PL00009535
44. Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30(4):744–748. doi:10.1161/01.STR.30.4.744
45. Permsirivanich W, Tipchatyotin S, Wongchai M, et al. Comparing the effects of rehabilitation swallowing therapy vs. neuromuscular electrical stimulation therapy among stroke patients with persistent pharyngeal dysphagia: a randomized controlled study. Med J Med Assoc Thai. 2009;92(2):259.
46. Ludlow CL, Humbert I, Saxon K, et al. Effects of surface electrical stimulation both at rest and during swallowing in chronic pharyngeal dysphagia. Dysphagia. 2007;22(1):1–10. doi:10.1007/s00455-006-9029-4
47. Power ML, Fraser CH, Hobson A, et al. Evaluating oral stimulation as a treatment for dysphagia after stroke. Dysphagia. 2006;21(1):49–55. doi:10.1007/s00455-005-9009-0
48. Li L, Yin J, Shen Y, et al. The value of adding transcutaneous neuromuscular electrical stimulation (Vitalstim) to traditional therapy for post-stroke dysphagia: a randomized controlled study. Rev Ecuatoriana de Neurol. 2012;21(43468):37.
49. Li L, Li Y, Huang R, et al. The value of adding transcutaneous neuromuscular electrical stimulation (VitalStim) to traditional therapy for post-stroke dysphagia: a randomized controlled trial. Eur J Phys Rehabil Med. 2015;51(1):71–78.
50. Christian M. Electrical stimulation for swallowing disorders caused by stroke. Respir Care. 2001;46:466–474.
51. Lim K-B, Lee HJ, Lim SS, et al. Neuromuscular electrical and thermal-tactile stimulation for dysphagia caused by stroke: a randomized controlled trial. J Rehabil Med. 2009;41(3):174–178. doi:10.2340/16501977-0317
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.