Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Effectiveness of CYP2C19 Genotype-Guided Antiplatelet Therapy Following Neurovascular Endovascular Procedures: A Prospective Non-Randomized Controlled Study
Authors Xu S, Wang X, Cui G, Li M, Chen G, Hu J, Zhang Q
Received 10 April 2026
Accepted for publication 19 June 2026
Published 9 July 2026 Volume 2026:22 615918
DOI https://doi.org/10.2147/TCRM.S615918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandeep Ajoy Saha
Shaowen Xu,1,2 Xinxin Wang,2 Guangjun Cui,3 Miaomiao Li,2 Guoning Chen,2 Jinhua Hu,4 Qizhi Zhang2
1Department of Neurology, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 2Department of Neurology, The Fifth People’s Hospital of Jinan, Shandong Second Medical University, Jinan, Shandong, People’s Republic of China; 3The Fifth People’s Hospital of Jinan, Shandong Second Medical University, Shandong, People’s Republic of China; 4Department of Gastroenterology, Shandong Provincial Hospital, Shandong First Medical University, Jinan, Shandong, People’s Republic of China
Correspondence: Jinhua Hu, Department of Gastroenterology, Shandong Provincial Hospital, Shandong First Medical University, Jinan, Shandong, People’s Republic of China, Email [email protected] Qizhi Zhang, Department of Neurology, The Fifth People’s Hospital of Jinan, Shandong Second Medical University, Jinan, Shandong, People’s Republic of China, Email [email protected]
Background: CYP2C19 loss-of-function alleles are highly prevalent in Asian populations and may reduce the effectiveness of clopidogrel. This study aimed to evaluate the efficacy and safety of CYP2C19 genotype-guided antiplatelet therapy in patients with symptomatic severe intracranial atherosclerotic stenosis undergoing neurovascular endovascular treatment (EVT).
Methods: This prospective non-randomized controlled study enrolled 175 patients who underwent neurovascular intervention. Patients in the genotype-guided group (n=100) received individualized antiplatelet therapy according to CYP2C19 genotyping results, whereas patients in the conventional therapy group (n=75) received routine dual antiplatelet therapy with aspirin and clopidogrel. Safety events, 90-day neurological outcomes, and the cumulative incidence of ischemic events within one year were compared between groups.
Results: The incidence of bleeding events did not differ significantly between the genotype-guided group and the conventional therapy group (1.0% vs 4.0%, P> 0.05). At 90 days, a significantly higher proportion of patients achieved a favorable functional outcome (modified Rankin Scale score 0– 1) in the genotype-guided group than in the conventional therapy group (84.0% vs 65.3%, P=0.004). At one year, the proportion of patients experiencing at least one ischemic event was significantly lower in the genotype-guided group than in the conventional therapy group (12.0% vs 26.7%, P=0.013). Multivariable Cox regression analysis demonstrated that patients in the conventional therapy group had a significantly higher risk of ischemic events during follow-up than those in the genotype-guided therapy group (HR: 2.723, 95% CI: 1.259– 5.888, P = 0.011). Interaction analysis suggested that treatment effects differed according to device type, with a numerically greater benefit observed in the stent subgroup, although this finding should be considered exploratory.
Conclusion: CYP2C19 genotype-guided antiplatelet therapy following neurovascular EVT was associated with improved neurological outcomes and a lower incidence of ischemic events without increasing bleeding risk. However, because ticagrelor exposure differed between treatment groups, the independent contribution of pharmacogenetic testing requires further confirmation in larger randomized studies.
Keywords: intracranial atherosclerotic severe stenosis, endovascular treatment, CYP2C19 genotyping, pharmacogenetics, antiplatelet therapy
Introduction
More than 65% of ischemic strokes in Asian populations are caused by intracranial atherosclerotic disease, which contrasts sharply with Caucasian populations.1,2 Endovascular treatment (EVT) has become an important therapeutic approach for severe symptomatic intracranial stenosis.3 However, despite continuous advances in endovascular devices and techniques, the risk of recurrent ischemic events after EVT remains substantial, with reported one-year event rates ranging from 4.4% to 36.2%.4–8 Optimizing post-procedural antiplatelet therapy therefore remains a major clinical challenge. Current guidelines and expert consensus generally recommend dual antiplatelet therapy (DAPT) with aspirin and clopidogrel following neurovascular intervention, particularly in patients receiving intracranial stents.9 Clopidogrel is a prodrug whose antiplatelet activity depends on hepatic bioactivation mediated primarily by the CYP2C19 enzyme.10 The prevalence of CYP2C19 loss-of-function (LOF) alleles, including *2 and *3, is considerably higher in East Asian populations than in Western populations, affecting approximately 30–60% of individuals.11 Consequently, a substantial proportion of patients may experience reduced responsiveness to clopidogrel and remain at increased risk of thromboembolic events despite standard DAPT.
Ticagrelor is a direct-acting P2Y12 receptor inhibitor that does not require CYP2C19-mediated metabolic activation and therefore provides more consistent platelet inhibition in LOF allele carriers.10 In the cardiovascular field, individualized selection of P2Y12 inhibitors has increasingly been adopted to optimize antiplatelet efficacy and clinical outcomes.12 Furthermore, the CHANCE-2 trial demonstrated that ticagrelor plus aspirin significantly reduced recurrent stroke risk among CYP2C19 LOF carriers with minor stroke or transient ischemic attack compared with clopidogrel plus aspirin, without increasing severe bleeding risk.13 Previous neurointerventional studies have also suggested that CYP2C19 polymorphisms and clopidogrel hyporesponsiveness may be associated with thromboembolic complications after cerebral endovascular procedures and carotid artery stenting.14,15 These findings provide a rationale for considering genotype-guided antiplatelet therapy in neurovascular intervention.
However, an important distinction should be made between the benefit of genotype-guided treatment selection and the pharmacological effect of ticagrelor itself. The value of a genotype-guided strategy lies in identifying patients who are less likely to respond adequately to clopidogrel and selecting a more appropriate P2Y12 inhibitor. Nevertheless, any observed clinical benefit may also reflect the intrinsically stronger and more consistent platelet inhibition provided by ticagrelor. This distinction remains insufficiently explored in the neurointerventional setting. In addition, different endovascular devices may confer distinct thrombotic risks. Intracranial stent implantation introduces a permanent metallic scaffold and may result in prolonged platelet activation and delayed endothelialization, whereas balloon angioplasty does not leave a permanent implant and may therefore have a different thrombogenic profile. These mechanistic differences provide a biological rationale for evaluating whether the effectiveness of genotype-guided antiplatelet therapy varies according to device type. Therefore, this prospective non-randomized controlled study aimed to evaluate the efficacy and safety of CYP2C19 genotype-guided antiplatelet therapy after neurovascular EVT and to explore whether its potential benefits differ according to interventional device type.
Methods
Study Population
This study was designed as a single-center, prospective, non-randomized controlled trial. The project approval number is MR-37-24-055021. The study was approved by the Ethics Review Committee of the Fifth People’s Hospital of Jinan, Shandong Province (Approval No.: 23-1-05). Written informed consent was obtained from all patients or their legally authorized representatives, in accordance with the Declaration of Helsinki. Each neurointerventional physician involved in the study performed more than 40 interventional procedures annually.
Patients who underwent EVT (including stent implantation and drug-coated balloon, DCB) for symptomatic intracranial atherosclerotic severe stenosis from January 2022 to June 2024 were consecutively enrolled. Because this was a prospective non-randomized study, treatment allocation was not determined by randomization. Eligible patients were consecutively enrolled during the study period. Patients managed according to CYP2C19 genotyping results were assigned to the genotype-guided treatment group, whereas patients receiving standard dual antiplatelet therapy irrespective of genotype results were assigned to the conventional treatment group. No formal matching procedure was performed. To reduce potential confounding, baseline characteristics were compared between groups and multivariable Cox regression analyses were conducted to adjust for relevant clinical variables.Inclusion criteria: Age ≥ 18 years; Severe stenosis confirmed by digital subtraction angiography (DSA). According to the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) measurement method, severe stenosis was defined as 70–99%; Symptomatic intracranial atherosclerotic stenosis, defined as neurological deficits due to TIA or ischemic cerebral infarction diagnosed by MRI; Postoperative standard dual antiplatelet therapy (aspirin + clopidogrel/ticagrelor); Successful EVT was defined as residual stenosis ≤ 50% after endovascular treatment; Signed informed consent. CYP2C19 genotyping was offered to all eligible patients as part of routine clinical evaluation; however, treatment decisions were made according to the antiplatelet strategy selected by the treating physician and patient preference.
Exclusion criteria: Concomitant anticoagulation therapy such as atrial fibrillation; Severe hepatic or renal dysfunction; Allergy to aspirin or P2Y12 inhibitors; Concomitant intracranial tumors, aneurysms, or arteriovenous malformations; Any hemorrhagic disorder within 90 days; Inability to participate in follow-up (Figure 1).
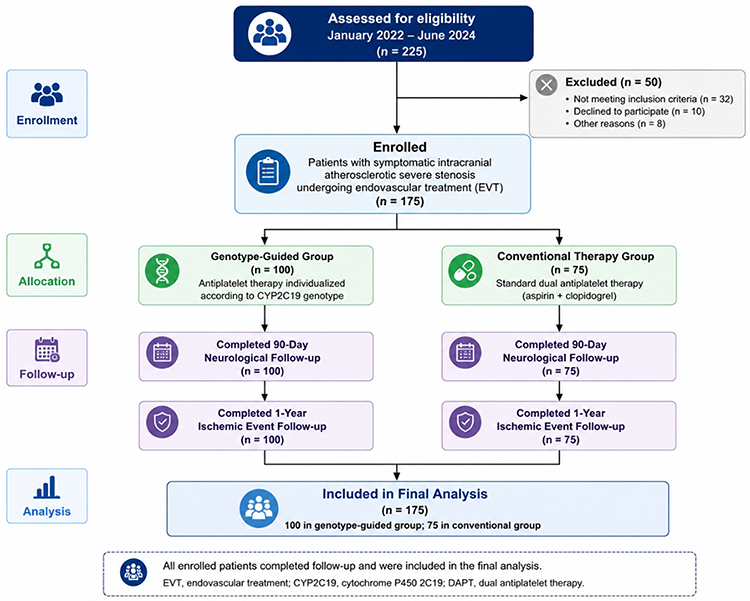 |
Figure 1 Flow Diagram of Patient Enrollment, Treatment Allocation, Follow-up, and Analysis. |
Genetic Analysis
We used nucleic acid mass spectrometry (Zhejiang Dipo Diagnostic Technology Co., Ltd., Zhejiang, China) to rapidly and efficiently detect whole blood DNA samples and identify gene variants in enrolled patients. The main genotypes included: CYP2C191, CYP2C192, CYP2C193, CYP2C1917. The workflow of nucleic acid mass spectrometry included: PCR amplification of target fragments using Shrimp Alkaline Phosphatase (PCR), followed by removal of deoxynucleotide triphosphates (dNTPs) with Shrimp Alkaline Phosphatase (SAP); subsequently, single-base extension was performed, purified, and spotted. Finally, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) was used to analyze the generated spectra, and genotypes were directly identified by peak position interpretation.
CYP2C19 Phenotype and Grouping
CYP2C19 Phenotypes Were Classified as LOF and Non-LOF
LOF included intermediate metabolizers (IM): *1/*2, *1/*3, *2/*17, *3/*17, and poor metabolizers (PM): *2/*2, *2/*3, *3/*3. Non-LOF included rapid metabolizers (RM): *1/*17 and normal metabolizers (NM): *1/*1. Genotype testing of CYP2C19 (*2, *3, *17 alleles) was performed at the Jinan Dian Pharmacogenetic Testing Center. This classification followed the recommendations of the Clinical Pharmacogenetics Implementation Consortium (CPIC).16
Grouping Criteria
Experimental group (n=100): Patients with IM or PM received aspirin (100 mg once daily) plus ticagrelor (90 mg twice daily); RM or NM continued aspirin plus clopidogrel. Conventional group (n=75): Empirically treated with aspirin (100 mg once daily) plus clopidogrel (75 mg once daily).
All patients received loading doses of aspirin (300 mg) and clopidogrel (300 mg) before the interventional procedure. Genotyping results were available before or shortly after the procedure, and antiplatelet therapy was adjusted as early as clinically feasible, generally within 24 hours. Duration of DAPT was 6 months after stenting and 3 months after DCB. After completing the prescribed course, aspirin was continued lifelong. Patients with hypertension, diabetes, or hyperlipidemia received long-term management.
Outcome Measures
All patients received outpatient or inpatient follow-up at 3 months, 6 months, and 1 year. Follow-up assessments were conducted through scheduled outpatient visits whenever possible. For patients who were unable to attend in person, structured telephone interviews were performed by trained investigators. Neuroimaging examinations, including CT, MRI, or vascular imaging, were reviewed when clinically indicated to verify suspected ischemic or thrombotic events. Clinical outcome events were independently adjudicated by two neurologists who were not involved in treatment allocation. During each follow-up contact, information regarding medication use, treatment discontinuation, and adherence to prescribed antiplatelet therapy was collected. Patients were considered adherent if they reported continuous use of the prescribed antiplatelet regimen throughout the recommended treatment period. The primary ischemic events were composite adverse cerebrovascular events, including cerebrovascular-related death, ischemic stroke, TIA, and thrombotic events.
Ischemic stroke was defined as sudden onset of neurological deficits lasting more than 24 hours, with CT/MRI excluding hemorrhage or confirming ischemia. TIA was defined as transient neurological deficits resolving within 24 hours, with no acute infarction on DWI-MRI. Thrombotic events included in-stent thrombosis and target-vessel thrombosis (DCB procedures did not involve implants). Myocardial infarction was defined as elevated troponin levels with ischemic symptoms or ischemic ECG changes, or new regional wall-motion abnormalities unrelated to surgery.
Neurological function at 90 days after surgery was assessed via the modified Rankin Scale (mRS). Ischemic events such as stroke or TIA occurring during follow-up were included in the mRS outcome. Neurological outcomes were dichotomized: mRS 0–1 = good, mRS 2–6 = poor.
Safety events were defined according to the Bleeding Academic Research Consortium (BARC) class 2 or higher bleeding events:17 Type 2: actionable bleeding requiring non-surgical intervention, hospitalization, or physician evaluation; Type 3: 3a: hemoglobin drop 3–5 g/dL or transfusion; 3b: hemoglobin drop ≥5 g/dL, surgical intervention; 3c: intracranial hemorrhage; Type 4: unrelated to coronary bypass surgery; Type 5: 5a: probable fatal bleeding without documentation; 5b: definite fatal bleeding. All events were verified by at least two neurologists. Follow-up ended upon the occurrence of the first clinical event.
Data Analysis
Statistical analysis was performed using SPSS 29.0 (IBM, Armonk, New York), and figures were generated using GraphPad Prism (version 10.1.2). The Shapiro–Wilk test was used to assess normality of variable distribution. Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR), and compared using Student’s t-test, one-way analysis of variance (ANOVA), the Kruskal–Wallis test, or the Mann–Whitney U-test as appropriate. Categorical variables were presented as frequencies and percentages, and compared using the chi-square test or Fisher’s exact test. Differences in baseline characteristics and outcomes were analyzed using McNemar’s test for categorical variables and the Wilcoxon signed-rank test. Kaplan–Meier curves and Log rank tests were used to compare ischemic events. Age, sex, smoking, alcohol consumption, diabetes, hypertension, postoperative residual stenosis rate, lesion length, and device type were included in univariate Cox regression analysis. Based on previous prospective research and clinical importance, age, sex, and diabetes were pre-specified prognostic factors. Variables with P < 0.05 in univariate analysis were included in the multivariate model to assess the independent effect of genotype-guided therapy. To examine whether the benefit of genotype-guided therapy varied by device type, an interaction term “group × device type” was introduced into the Cox model. All probability values were two-sided, and P < 0.05 was considered statistically significant.
Results
Baseline Characteristics
Baseline characteristics are shown in Table 1. The mean age of the 175 patients included in the study was 65.9 ± 8.37 years, of whom 119 (68.0%) were male. No significant differences were observed between the two groups in demographic data, cerebrovascular risk factors, or laboratory findings. There were no statistically significant differences in etiology (P = 0.573), NIHSS at admission (P = 0.057), or ABCD2 score (P = 0.143). In the experimental group, 46% of patients were IM and 16% were PM. We subsequently calculated the allele frequencies of *2 and *3 according to genotype distribution. The *2 allele frequency was 35%, and the *3 allele frequency was 4%.
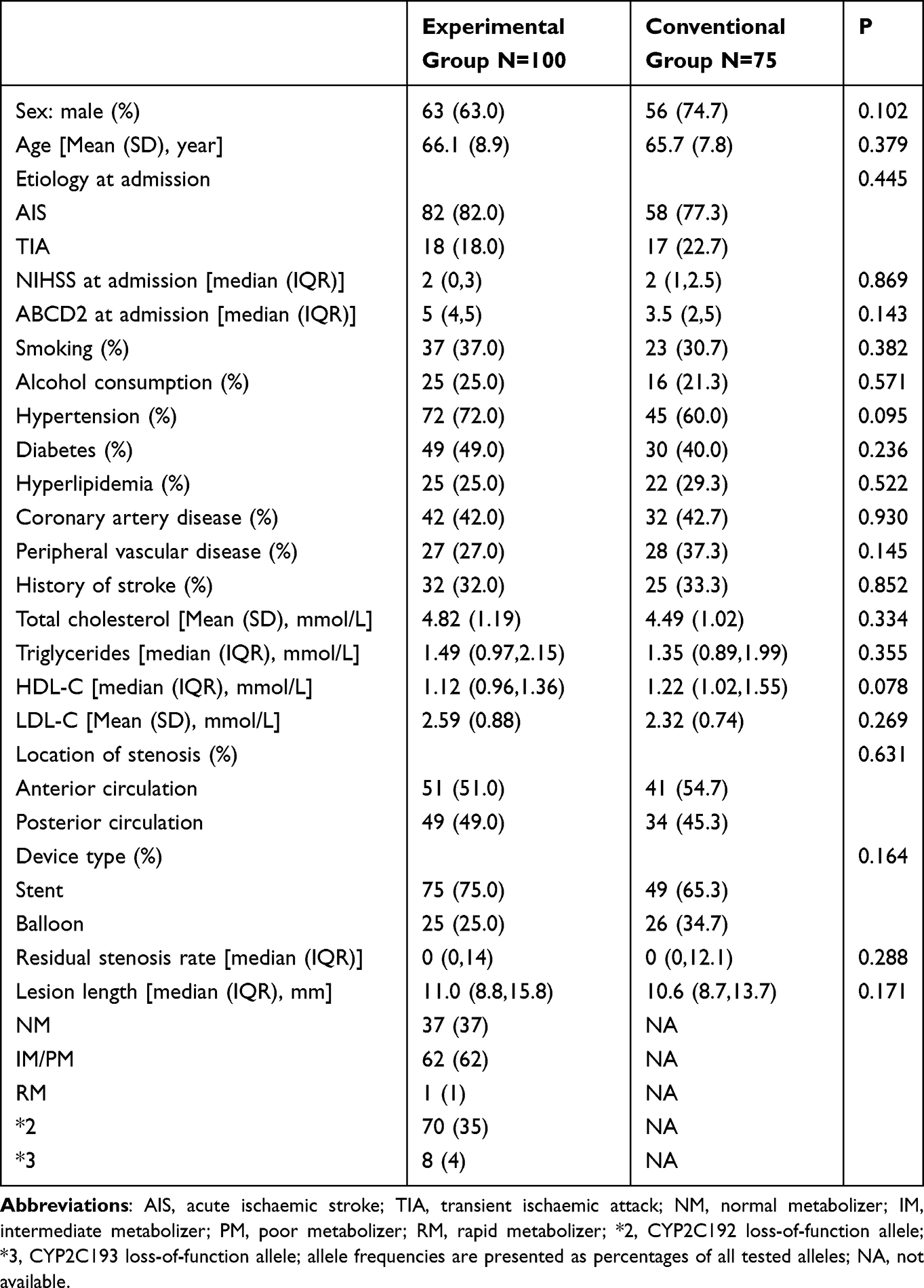 |
Table 1 Baseline Characteristics of the Two Groups |
Clinical Outcomes
At 1 year after EVT, the cumulative incidence of cerebrovascular death, ischemic stroke, TIA, and thrombotic events was significantly lower in the experimental group compared with the conventional group (12% vs 26.7%, P = 0.013) (Table 2). We then divided the 175 patients into two subgroups based on device type: stent implantation and balloon angioplasty. Kaplan–Meier curves were generated to compare the 1-year cumulative incidence of ischemic events. Kaplan–Meier analysis demonstrated a significantly lower cumulative incidence of ischemic events in the genotype-guided therapy group compared with the conventional therapy group in the overall study population (HR=0.393, 95% CI: 0.193–0.797, P=0.008; Figure 2A). In the stent subgroup, genotype-guided therapy showed a trend toward reduced ischemic event risk compared with conventional therapy (HR=0.405, 95% CI: 0.163–1.009, P=0.052; Figure 2B). In the drug-coated balloon subgroup, no statistically significant difference was observed between treatment groups (HR=0.462, 95% CI: 0.128–1.418, P=0.164; Figure 2C).
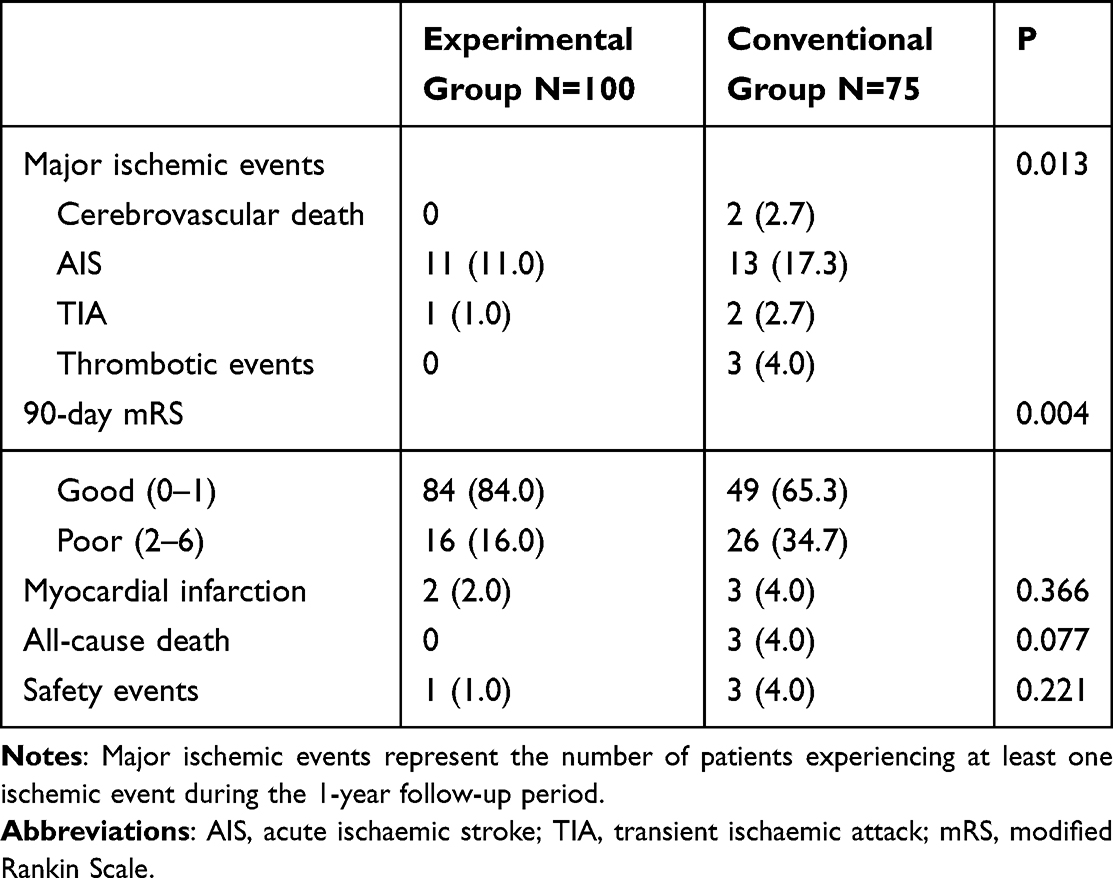 |
Table 2 Comparison of Outcomes Between Groups |
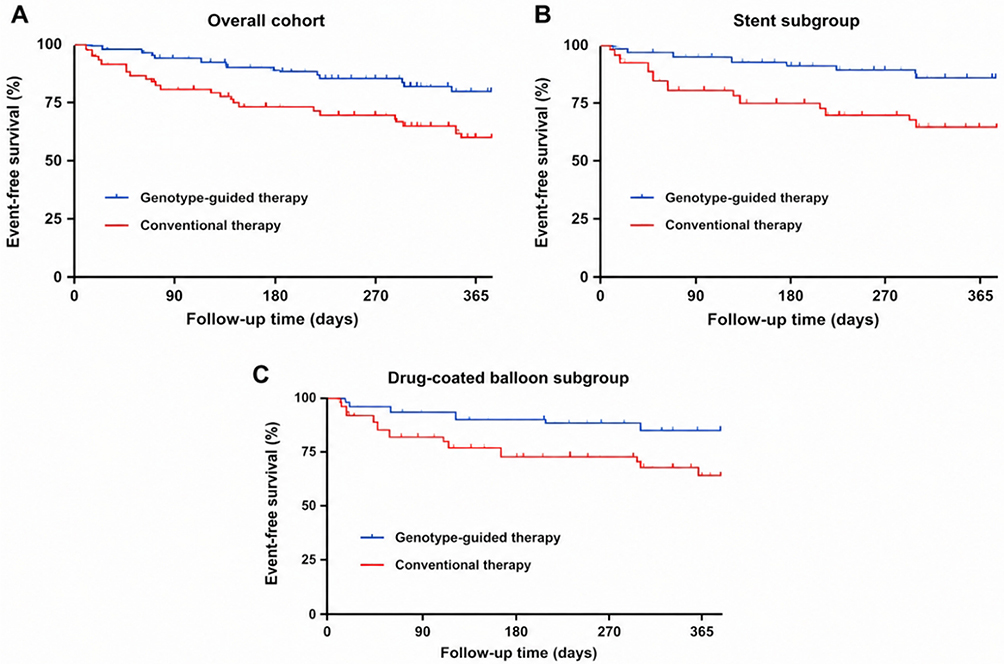 |
Figure 2 Kaplan–Meier curves for 1-year ischemic-event-free survival according to treatment strategy. Notes: The primary endpoint was the occurrence of at least one ischemic event during the 1-year follow-up period, including cerebrovascular death, ischemic stroke, transient ischemic attack, or thrombotic events. (A) Overall study population. (B) Patients treated with intracranial stent implantation. (C) Patients treated with drug-coated balloon angioplasty. Subgroup analyses were exploratory and should be interpreted with caution because of the limited number of events. |
The subsequent univariate Cox regression confirmed this association (HR:2.565, 95% CI:1.251–5.259, P = 0.010, Figure 3). To evaluate whether the genotype-guided treatment strategy was an independently associated with ischemic event risk and eliminate potential confounders, we included age, sex, smoking, alcohol consumption, hypertension, diabetes, device type, residual stenosis rate, and lesion length in the multivariate Cox regression model. After adjustment for potential confounders, treatment strategy remained significantly associated with the risk of ischemic events during follow-up (HR: 2.723, 95% CI: 1.259–5.888, P = 0.011). Patients in the conventional treatment group had a significantly higher risk of ischemic events than those in the genotype-guided treatment group. (Figure 3).
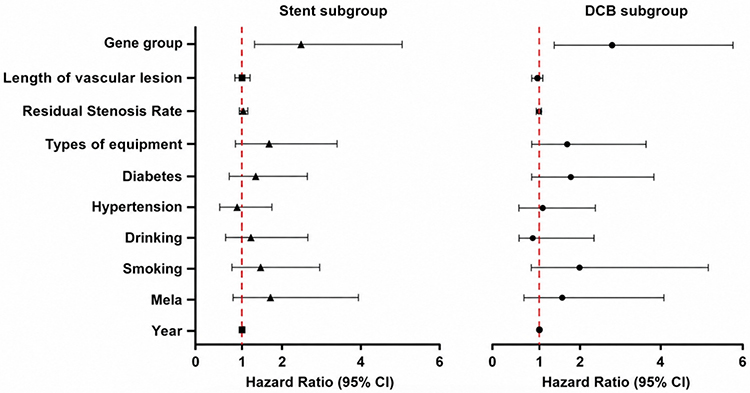 |
Figure 3 Forest plot of risk factors for ischemic events. Note: ▲Univariate Cox regression; ●Multivariate Cox regression. |
In the Kaplan–Meier analysis, a numerically greater survival benefit was observed in stent-treated patients receiving genotype-guided therapy compared with conventional therapy. To rigorously examine this heterogeneity, we introduced an interaction term “treatment group × device type” into the model. The interaction analysis suggested a potential difference in treatment effect according to device type (P for interaction = 0.004), although the subgroup findings should be interpreted cautiously because of the limited number of events. In the stent subgroup, genotype-guided therapy showed the strongest trend toward benefit, reaching marginal significance compared with the conventional group (HR:0.405, 95% CI:0.163–1.009, P = 0.052). No significant benefit was observed in the DCB subgroup (HR:0.462, 95% CI:0.128–1.419, P = 0.164, Table 3).
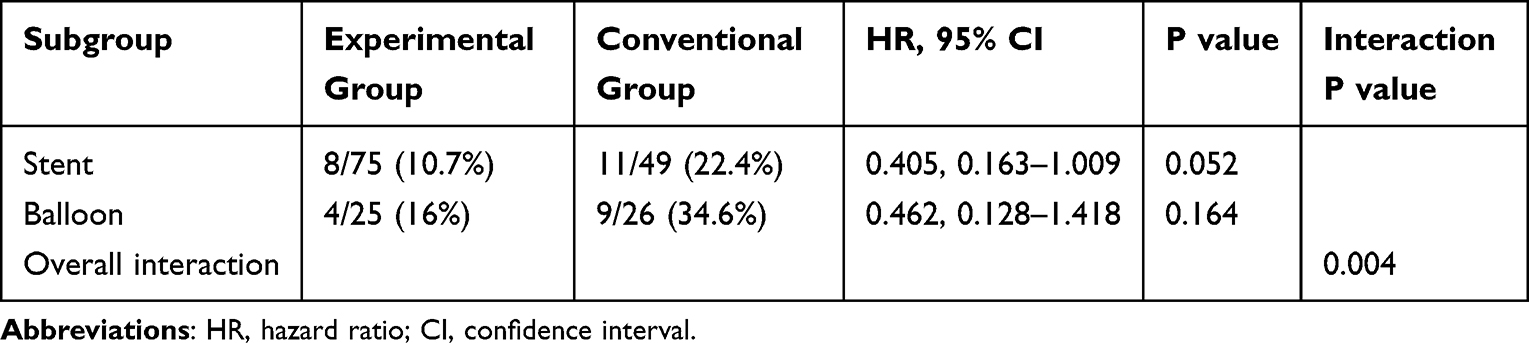 |
Table 3 Subgroup Analysis and Interaction Effects Across Device Types |
Neurological recovery differed significantly between groups (16% vs 34.7%, P = 0.004). Among all-cause deaths in the conventional group, 4% died from severe gastrointestinal bleeding. Of the thrombotic events, two occurred within stents and one at the distal segment of a balloon-dilated vessel. The experimental group had lower rates of myocardial infarction (2% vs 4%, P = 0.336), all-cause death (0 vs 4%, P = 0.077), and safety events (1% vs 4%, P = 0.221), although none reached statistical significance (Table 2).
Discussion
This study investigated the efficacy of CYP2C19 genotype-guided antiplatelet therapy after EVT in a prospective, non-randomized controlled trial. The genotype-guided strategy was associated with improved neurological recovery and a lower incidence of ischemic events without increasing bleeding risk. However, the observed clinical benefit should be interpreted cautiously. In the genotype-guided group, intermediate and poor metabolizers received ticagrelor, whereas all patients in the conventional group received clopidogrel. Therefore, part of the observed benefit may have resulted from the greater and more consistent antiplatelet effect of ticagrelor itself rather than the pharmacogenetic testing strategy alone. We found that the experimental group did not show an increased risk of moderate-to-severe bleeding (1% vs 4.0%, P=0.221). At 90 days postoperatively, patients in the experimental group demonstrated significantly improved neurological recovery (16% vs 34.7%, P=0.004). Compared with conventional DAPT therapy, genotype-guided antiplatelet treatment significantly reduced the proportion of patients experiencing at least one ischemic event within 1 year after EVT (12.0% vs 26.7%, P=0.013). Multivariate COX regression analysis indicated that conventional therapy was a prognostic risk factor after EVT. Kaplan–Meier analysis demonstrated a significantly lower cumulative incidence of ischemic events in the genotype-guided therapy group in the overall cohort. Interaction analysis further suggested that the treatment effect differed according to device type (P for interaction = 0.004).
Among the 175 patients in this study, the frequencies of CYP2C19*2 and *3 were 35% and 4%, respectively, consistent with previous reports in East Asian populations.18,19 The observed clinical benefit may be attributable to both the genotype-guided treatment strategy and the pharmacological differences between ticagrelor and clopidogrel. Because CYP2C19 loss-of-function carriers in the genotype-guided group were preferentially treated with ticagrelor, the present study cannot fully separate the effect of pharmacogenetic-guided treatment selection from the intrinsic antiplatelet superiority of ticagrelor in this patient population. Studies exploring the relationship between CYP2C19 polymorphisms and postoperative outcomes after EVT showed that *2 and *3 significantly influenced postoperative outcomes among clopidogrel users, and ticagrelor was recommended as an alternative.20,21 One study reported that in LOF allele carriers, clopidogrel combined with aspirin did not reduce 90-day stroke risk compared with aspirin monotherapy (9.4% vs 10.8%; HR:0.93, 95% CI:0.69–1.26, p=0.64),22 while non-LOF carriers experienced a significant risk reduction (6.7% vs 12.4%; HR:0.51; 95% CI:0.35–0.75; p<0.01).21 Another study using genotyping to assess clopidogrel treatment found that compared with normal metabolizers, IM or PM patients receiving clopidogrel had more than double the risk of vascular events (HR:2.16, 95% CI:1.31–3.56, p=0.003).23 Our study observed a significant reduction in ischemic events in the experimental group compared with the conventional group (P=0.013), and Kaplan-Meier analysis (P=0.008) together with multivariate COX regression (P=0.011) demonstrated a sustained survival advantage throughout the follow-up period. Overall, we found that clopidogrel failed to provide strong platelet inhibition for IM or PM patients, consistent with a meta-analysis including seven studies showing that LOF patients had increased thromboembolic complications after neurointerventional procedures.14 In this study, thrombotic events occurred in only three cases, and although the number was too small for definitive conclusions, all occurred in the conventional group.
In the conventional group, three cases of moderate-to-severe bleeding were confirmed; all were related to gastrointestinal bleeding, and subsequent genetic testing revealed no UM. A retrospective study reported that after percutaneous neurointerventional procedures, UM patients exhibited a higher bleeding risk.15 Given the limited sample size of this study, further investigation is required. Another randomized controlled trial found that ticagrelor combined with aspirin did not increase bleeding risk compared with clopidogrel plus aspirin, consistent with our findings. Neurological function assessed by mRS showed better recovery in the experimental group, consistent with results from a single-blind trial.24,25
From the perspective of device type, interaction analysis suggested that treatment effects may differ between stent implantation and drug-coated balloon procedures. Although a larger numerical risk reduction was observed in the stent subgroup, the result did not reach conventional statistical significance (P=0.052) and should therefore be considered exploratory. This observation is biologically plausible because stents, as permanent implants, create an environment with prolonged platelet activation and a potentially higher thrombotic burden. Under these conditions, differences in antiplatelet responsiveness may have a greater clinical impact. Therefore, CYP2C19-guided antiplatelet selection may be particularly relevant in patients receiving stent implantation.26,27 However, these findings require confirmation in larger studies with adequate statistical power. Avoiding clopidogrel resistance via genotyping allows ticagrelor to provide strong and consistent platelet inhibition, which was most evident in our study. From a practical perspective, implementation of CYP2C19 genotyping in neurointerventional practice is becoming increasingly feasible because testing can now be completed within a relatively short time frame and at a modest cost in many centers. Early identification of CYP2C19 loss-of-function carriers may facilitate individualized antiplatelet selection before or shortly after EVT, potentially reducing thromboembolic complications in high-risk patients. Nevertheless, the cost-effectiveness of routine pharmacogenetic testing in neurovascular intervention remains uncertain and may vary across healthcare systems. Future prospective studies should evaluate not only clinical outcomes but also economic impact and optimal timing of genotyping in relation to the procedure. Compared with stents, DCB avoids permanent implants, reduces chronic inflammation, and lowers long-term thrombotic risk.28 However, antiproliferative drugs such as paclitaxel, while preventing restenosis, may delay functional endothelial healing, creating a surface prone to platelet adhesion and activation during the mid-to-late postoperative period, thereby potentially increasing thrombotic risk.29 As drug effects diminish, the vessel achieves near-complete endothelialization, and the thrombosis risk window is relatively short. This mechanism helps explain why genotype-guided therapy still trends toward benefit in the DCB subgroup, although its absolute value is less pronounced than in the stent subgroup. From another angle, the relatively lower thrombogenic burden associated with DCB procedures may provide a rationale for future studies investigating de-escalation antiplatelet strategies in selected patients at high bleeding risk. However, the present study was not designed to evaluate DAPT duration, and therefore no conclusions regarding de-escalation strategies can be drawn from our findings.
Limitations
Our study has several limitations. First, this was a single-center study. All enrolled patients were Han Chinese from northern China, which may introduce selection bias. Multi-center studies with larger sample sizes are required to validate our findings. Second, no formal sample size calculation was performed before study initiation. Although 175 patients were enrolled, the absolute number of ischemic events was relatively small, particularly within individual device subgroups. Consequently, the statistical power for exploratory subgroup and interaction analyses may have been limited. The observed trend toward benefit in the stent subgroup did not reach conventional statistical significance, which may partly reflect insufficient sample size rather than the absence of a true treatment effect. Therefore, subgroup findings should be interpreted cautiously and regarded as hypothesis-generating until confirmed in larger adequately powered studies. Third, an important source of potential confounding should be acknowledged. The genotype-guided group did not simply undergo pharmacogenetic testing; rather, intermediate and poor metabolizers were switched to ticagrelor, whereas patients in the conventional group uniformly received clopidogrel. Consequently, the observed reduction in ischemic events may partly reflect the stronger antiplatelet efficacy of ticagrelor rather than the effect of genotyping alone. Fourth, although genotype results were available before or shortly after EVT and antiplatelet therapy was adjusted within 24 hours whenever feasible, all patients initially received a clopidogrel loading dose before the procedure. Consequently, some CYP2C19 loss-of-function carriers may have experienced suboptimal platelet inhibition during the peri-procedural period before treatment adjustment. This could have influenced the risk of early thrombotic events and may have attenuated the potential benefit of genotype-guided therapy. Because platelet function testing was not routinely performed during this early phase, the impact of this temporary exposure to clopidogrel cannot be fully quantified and warrants further investigation.
Conclusion
In patients undergoing EVT, CYP2C19 genotype-guided dual antiplatelet therapy was associated with improved neurological outcomes at 90 days and a lower incidence of ischemic events during 1-year follow-up without increasing bleeding risk. Interaction analysis suggested that treatment effects may vary according to device type; however, these subgroup findings should be considered exploratory and interpreted with caution. Given the non-randomized design and the potential confounding effect of differential ticagrelor exposure between groups, the independent contribution of pharmacogenetic-guided treatment selection requires further confirmation in larger multicenter randomized studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Jinan Science and Technology Innovation Development Project in 2026 (No. 202512032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu L, Wang D, Wong KS, et al. Stroke and stroke care in China: huge burden, significant workload, and a national priority. Stroke. 2011;42(12):3651–11. doi:10.1161/STROKEAHA.111.635755
2. Hurford R, Rothwell PM. Prevalence, prognosis, and treatment of atherosclerotic intracranial stenosis in Caucasians. Int J Stroke. 2021;16(3):248–264. doi:10.1177/1747493020974461
3. Yang L, Du H, Zhang D, et al. Complications and long-term in-stent restenosis of endovascular treatment of severe symptomatic intracranial atherosclerotic stenosis and relevant risk factors. Medicine. 2023;102(38):e34697. doi:10.1097/MD.0000000000034697
4. Sun X, Deng Y, Zhang Y, et al. Balloon angioplasty vs medical management for intracranial artery stenosis: the BASIS randomized clinical trial. JAMA. 2024;332(13):1059–1069. doi:10.1001/jama.2024.12829
5. Compter A, Van Der Worp HB, Schonewille WJ, et al. Stenting versus medical treatment in patients with symptomatic vertebral artery stenosis: a randomised open-label phase 2 trial. Lancet Neurol. 2015;14(6):606–614. doi:10.1016/S1474-4422(15)00017-4
6. Miao Z, Jiang L, Wu H, et al. Randomized controlled trial of symptomatic middle cerebral artery stenosis: endovascular versus medical therapy in a Chinese population. Stroke. 2012;43(12):3284–3290. doi:10.1161/STROKEAHA.112.662270
7. Gao P, Wang T, Wang D, et al. Effect of stenting plus medical therapy vs medical therapy alone on risk of stroke and death in patients with symptomatic intracranial stenosis: the CASSISS randomized clinical trial. JAMA. 2022;328(6):534–542. doi:10.1001/jama.2022.12000
8. Zaidat OO, Fitzsimmons BF, Woodward BK, et al. Effect of a balloon-expandable intracranial stent vs medical therapy on risk of stroke in patients with symptomatic intracranial stenosis: the VISSIT randomized clinical trial. JAMA. 2015;313(12):1240–1248. doi:10.1001/jama.2015.1693
9. Meyer BM, Campos JK, Collard De Beaufort JC, et al. Trends in dual antiplatelet therapy use for neurointerventional procedures for the management of intracranial aneurysms. Biomedicines. 2023;11(8):2234. doi:10.3390/biomedicines11082234
10. Rocca B, Patrono C. Precision antiplatelet therapy. Res Pract Thromb Haemost. 2023;7(3):100138. doi:10.1016/j.rpth.2023.100138
11. Gower MN, Ratner LR, Williams AK, et al. Clinical utility of CYP2C19 genotype-guided antiplatelet therapy in patients at risk of adverse cardiovascular and cerebrovascular events: a review of emerging evidence. Pharmgenomics Pers Med. 2020;13:239–252. doi:10.2147/PGPM.S231475
12. Kumar A, Lutsey PL, St Peter WL, et al. Prescription patterns of P2Y12 inhibitors following revascularization in the United States: 2013-2018. Clin Transl Sci. 2023;16(10):1886–1897. doi:10.1111/cts.13596
13. Wang Y, Johnston C, Bath PM, et al. Clopidogrel with aspirin in high-risk patients with acute non-disabling cerebrovascular events II (CHANCE-2): rationale and design of a multicentre randomised trial. Stroke Vasc Neurol. 2021;6(2):280–285. doi:10.1136/svn-2020-000791
14. Duconge J, Hernandez-Suarez DF. Potential usefulness of clopidogrel pharmacogenetics in cerebral endovascular procedures and carotid artery stenting. Curr Clin Pharmacol. 2017;12(1):11–17. doi:10.2174/1574884712666170227154654
15. Saiz-Rodríguez M, Romero-Palacián D, Villalobos-Vilda C, et al. Influence of CYP2C19 phenotype on the effect of clopidogrel in patients undergoing a percutaneous neurointervention procedure. Clin Pharmacol Ther. 2019;105(3):661–671. doi:10.1002/cpt.1067
16. Zhang Y, Shi XJ, Peng WX, et al. Impact of implementing CYP2C19 genotype-guided antiplatelet therapy on P2Y(12) inhibitor selection and clinical outcomes in acute coronary syndrome patients after percutaneous coronary intervention: a Real-World Study in China. Front Pharmacol. 2020;11:582929. doi:10.3389/fphar.2020.582929
17. Ndrepepa G, Schuster T, Hadamitzky M, et al. Validation of the bleeding academic research consortium definition of bleeding in patients with coronary artery disease undergoing percutaneous coronary intervention. Circulation. 2012;125(11):1424–1431. doi:10.1161/CIRCULATIONAHA.111.060871
18. Yuan XW, Yuan SY, Wu GX, et al. Genetic polymorphism of clopidogrel metabolism related gene CYP2C19 gene in Chinese from Foshan area of Guangdong Province. Hematology. 2022;27(1):1056–1061. doi:10.1080/16078454.2022.2121899
19. Lee SH, Jeong YH, Hong D, et al. Clinical impact of CYP2C19 genotype on clopidogrel-based antiplatelet therapy after percutaneous coronary intervention. JACC. 2023;16(7):829–843. doi:10.1016/j.jcin.2023.01.363
20. Zhu WY, Zhao T, Xiong XY, et al. Association of CYP2C19 polymorphisms with the clinical efficacy of clopidogrel therapy in patients undergoing carotid artery stenting in Asia. Sci Rep. 2016;6:25478. doi:10.1038/srep25478
21. Wang Y, Zhao X, Lin J, et al. Association between CYP2C19 loss-of-function allele status and efficacy of clopidogrel for risk reduction among patients with minor stroke or transient ischemic attack. JAMA. 2016;316(1):70–78. doi:10.1001/jama.2016.8662
22. Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. 2013;369(1):11–19. doi:10.1056/NEJMoa1215340
23. Sun W, Li Y, Li J, et al. Variant recurrent risk among stroke patients with different CYP2C19 phenotypes and treated with clopidogrel. Platelets. 2015;26(6):558–562. doi:10.3109/09537104.2014.953044
24. Wang Y, Chen W, Lin Y, et al. Ticagrelor plus aspirin versus clopidogrel plus aspirin for platelet reactivity in patients with minor stroke or transient ischaemic attack: open label, blinded endpoint, randomised controlled Phase II trial. BMJ. 2019;365:l2211. doi:10.1136/bmj.l2211
25. Zeinhom MG, Elbassiouny A, Mohamed AM, et al. Ticagrelor versus clopidogrel in acute large-vessel ischemic stroke: a randomized controlled single-blinded trial. CNS Drugs. 2024;38(5):387–398. doi:10.1007/s40263-024-01080-5
26. Baber U, Leisman DE, Cohen DJ, et al. Tailoring antiplatelet therapy intensity to ischemic and bleeding risk. Circ Cardiovasc Qual Outcomes. 2019;12(1):e004945. doi:10.1161/CIRCOUTCOMES.118.004945
27. Scorpiglione L, Pizzicannella J, Bacigalupi E, et al. Therapeutic strategies aiming at the reduction of the antiplatelet intensity should not overlook the ischemic risk in patients with coronary syndromes. Cardiovasc Revasc Med. 2025;70:78–84. doi:10.1016/j.carrev.2024.06.015
28. Ma G, Sun D, Jia B, et al. Comparison of drug-coated balloon with bare-metal stent in patients with symptomatic intracranial atherosclerotic stenosis: the AcoArt sICAS randomized clinical trial. J Neurointerv Surg. 2025;18(1):248–256. doi:10.1136/jnis-2024-022650
29. Park HM, Kim CL, Kong D, et al. Innovations in vascular repair from mechanical intervention to regenerative therapies. Tissue Eng Regen Med. 2025;22(4):551–567. doi:10.1007/s13770-024-00700-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.