Back to Journals » Risk Management and Healthcare Policy » Volume 15
Effectiveness of a Nurse-Led Support Programme Using a Mobile Application versus Phone Advice on Patients at Risk of Coronary Heart Disease – A Pilot Randomized Controlled Trial
Authors Wong EML, Leung DYP ![]() , Tam HL
, Tam HL ![]() , Ko SY
, Ko SY ![]() , Leung AYM
, Leung AYM ![]() , Lam SC, Cheung KC, Cheung ASP
, Lam SC, Cheung KC, Cheung ASP
Received 6 January 2022
Accepted for publication 27 March 2022
Published 8 April 2022 Volume 2022:15 Pages 597—610
DOI https://doi.org/10.2147/RMHP.S355554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Eliza Mi Ling Wong,1 Doris Yin Ping Leung,2 Hon Lon Tam,2 Shuk Yee Ko,3 Angela Yee Man Leung,2 Simon Ching Lam,1 Ka Ching Cheung,2 Alice Siu Ping Cheung2
1School of Nursing, Tung Wah College, Hong Kong SAR, People’s Republic of China; 2School of Nursing, The Hong Kong Polytechnic University, Hong Kong SAR, People’s Republic of China; 3Accident and Emergency Department, Tuen Mun Hospital, Hong Kong SAR, People’s Republic of China
Correspondence: Eliza Mi Ling Wong, School of Nursing, Tung Wah College, 16/F, Ma Kam Chan Memorial Building, 31 Wylie Road, Homantin, Kowloon, Hong Kong SAR, People’s Republic of China, Tel +852 3468 6803, Fax +852 2782 1566, Email [email protected]
Purpose: Coronary heart disease (CHD) is the leading cause of morbidity and mortality globally. This study aimed to examine the preliminary effect of a nurse-led support programme using a mobile application versus nursing telephone advice on patients at risk of CHD living in the community.
Patients and Methods: A prospective randomized controlled trial was adopted. Sixty eligible CHD participants were randomized into the app group (App) or the nursing telephone advice (NTA) group to support their own health care and exercise. Data were collected at baseline (T0), 1 month (T1), and 3 months (T2). Outcomes were total amount of exercise, self-efficacy of chronic disease management, total time of exercise, blood pressure, and lipid concentrations. Data were analyzed using the generalized estimating equation models.
Results: Ninety-two individuals were screened for eligibility and 60 were randomized into the app group (n = 30) or NTA group (n = 30). The mean age of the participants was 60.92. The total attrition rate at T2 was 1.66%. The app group showed a moderate effect (Cohen’s d =0.43) in significant increase in exercise amount, and reduction of lipid concentration (total cholesterol d=− 0.43, triglyceride d=− 0.39) respectively. Other outcomes showed improvement trend but non-significant between group.
Conclusion: The CHD app is effective to motivate CHD patients for maintaining exercise amount which will be beneficial to their lipid control.
Keywords: coronary heart disease, nurse-led, mobile application, exercise, blood lipid
Introduction
Coronary heart disease (CHD) is the leading cause of both morbidity and mortality in the world.1 In Hong Kong, 4032 deaths were caused by CHD, accounting for 8.6% of all registered deaths in 2016.2 CHD refers to an atherosclerotic condition in which narrowed coronary arteries lead to reduced blood flow, consequently leading to angina (ie, chest pain) or myocardial infarction and even death.3 If an individual’s atherosclerotic condition is not well controlled, the progressive deterioration of his/her cardiac functions will lead to a weakened physical condition, poor psychological well-being, and poor health-related quality of life.1–4
The American Heart Association Guideline (2018) emphasizes the importance of early awareness of symptoms and timely action and treatment upon experiencing angina; and the importance of lifestyle modifications to prevent further deterioration in CHD status over the long term.5 Preventive strategies to decrease modifiable CHD risks include greater awareness and self-efficacy in managing one’s health; effective communication with healthcare professionals; and lifestyle modifications such as regularly engaging in physical activity/exercise, healthy dietary choices, and smoking cessation.1,3,4 CHD modifiable risk factors include smoking; a sedentary lifestyle (< 150 minutes a week of moderate aerobic physical activity); Body Mass Index (BMI) > 25Kg/m2; hypertension (> 140/90 mmHg); abnormal low-density lipoprotein (LDL) > 3mmol/L; and diabetes (hemoglobin A1c, HbA1c) > 7%.4
Regular professional support and the provision of self-care information are important to motivate and promote self-management of health for patients with chronic conditions. Regarding professional support, a systematic review of 25 studies indicated that telephone counselling/advice by healthcare professionals was effective.6 Those who received a telephone advice or counselling intervention experienced significantly fewer hospitalizations, higher rates of quitting smoking, better blood pressure control, and less anxiety than the comparison group. However, additional resources such as professional support time and manpower were required to achieve such improvements.6
With the rapid growth of smart phone ownership and advancing technologies, e-health or mHealth has been integrated into cardiovascular healthcare in recent decades.7–21 “eHealth” or mHealth refers to the use of mobile computing and communication technologies to improve access to health information and to routine and emergency health services, and to provide diagnostic services and other functions.8 Many studies have demonstrated that e-health interventions (including web-based and mobile phone-based interventions) can be successfully used to support the self-management of chronic diseases such as CHD and heart failure.7,9–20 Studies have reported significant positive effects on physical activity and psychological health outcomes from using website support,9,12,20 or providing phone text messages10–18 or phone advice support for cardiac patients.6 These positive effects include reductions in some modifiable cardiac risk factors (body weight) and improvements in engagement in physical activity, medication adherence, and CHD self-management.6,10–17 There have been only a limited number of studies providing comprehensive reports of the concentration of lipids such as total cholesterol, LDL, high-density lipoprotein (HDL), triglyceride, and glucose levels, although it is an important biomarker for coronary heart disease.1,4 Therefore, more empirical studies need to be conducted. There is great potential for professional support to be better performed, and more feasibly, using the advanced features of a mobile application embedded in a smart phone. This study was conducted after considering the high prevalence of CHD, the proven effect of using phone advice to support patients in taking care of their own health problems,6,12,15,19 the advantages of mobile applications (interactive, accessible, and individualized) compared to websites, and the widespread use of smart phones in Hong Kong.
Materials and Methods
Aims and Hypotheses
The aim of this study was to examine the preliminary effects on the outcomes of total exercise, self-efficacy and self-management behaviour, emergency department attendance and hospitalizations, and the CHD risk factor profile of a nurse-led support programme for patients who are at risk of CHD. Patients who are at risk of CHD are those who possess at least two CHD risk factors.2–4 We hypothesized that patients receiving a nurse-led support programme with a tailor-made app (App group) would be likely to access the knowledge platform and app features easily, and therefore perform better than those in the NTA group, who would receive nursing telephone advice only in terms of changes in lifestyle, such as more engagement in exercise, greater self-efficacy in CHD self-care leading to better control of their CHD risk factor profile, and fewer visits to the emergency department and hospitalizations. Over 3 months, we examined the effect on the App group as compared to the NTA group regarding:
1.Total amount of exercise (Primary outcome).
2.Self-efficacy in chronic disease management.
3.Emergency department attendance and hospitalization frequency.
4.CHD risk factor profile (smoking, blood pressure, body weight, blood lipid level).
Design
A prospective multi-centre, parallel, randomized controlled trial (RCT) with two arms – an app support programme (App) group versus a Nursing Telephone advice (NTA) group – was adopted. This design was guided by the Consolidated Standards of Reporting Trials checklist.22 The study was conducted from November 2019 to October 2020.
Study Setting, Subjects, and Sample Size
Community centres regularly hold various health talks and activities for members living nearby. Patients could voluntarily register for our project. Subject recruitment was held by appointment in the community centres or in a university research laboratory.
Subjects
The criteria for inclusion in this study were: i) Chinese adults with coronary cardiac risk factors (at least two from below); ii) those able to perform a brisk walking exercise; and iii) those who possessed a smart phone and could use it.
Coronary heart disease risk factors:2,4 i) current regular smoker, ii) over 50 years of age; iii) has a medical diagnosis of diabetes or hypertension; iv) has a family history of ischaemic heart disease or hyperlipaemia; v) has hyperlipidaemia or is regularly taking drugs for hyperlipidaemia; vi) is obese (BMI>25); vii) has had a Percutaneous Coronary Intervention performed; and viii) has been diagnosed with stable angina and prescribed with TNG drugs.
The exclusion criteria were a) those with mental, visual, hearing, or cognitive impairments that caused them to be unable to perform a brisk walking exercise or communicate using a smart phone; b) those who were on a waiting list for cardiac angiography within 6 months, and c) who had a medical diagnosis of unstable angina.
Randomization
Randomization was 1:1 to each treatment arm. We used a computer-generated randomizer to generate the random allocation list. To ensure allocation concealment, each generated sequence was put in a sequentially numbered, opaque sealed envelope. The envelope was opened by the research assistant after the participant had completed the baseline questionnaire. In this study, the outcome assessors were blinded to the allocation sequence. However, given its type, the intervention was unmasked to the participants and the research nurse performing the intervention.
Sample Size
Hertzog suggested that at least 30 participants should be recruited per group for a pilot study.23 We successfully recruited 30 participants in the App group and 30 participants in the NTA group after taking into consideration a minimal attrition rate at the 3-month follow-up, as reported by our study in a similar setting.24
Intervention Material
The design of the app was grounded in self-efficacy theories and literature related to good mobile app designs.19,25–28
The front page of the app (Figure 1) is comprised of colourful icons to direct the participant to i) the educational area, which defines CHD and provides tips on a healthy diet, exercise, and medications; ii) a health member area, with data on blood pressure, cholesterol, body weight, and glycaemic levels; iii) a Chest Pain—Thing to Do list; and iv) a record of daily exercises and set goals. The table of contents for the educational component of the App group is illustrated in Table 1.
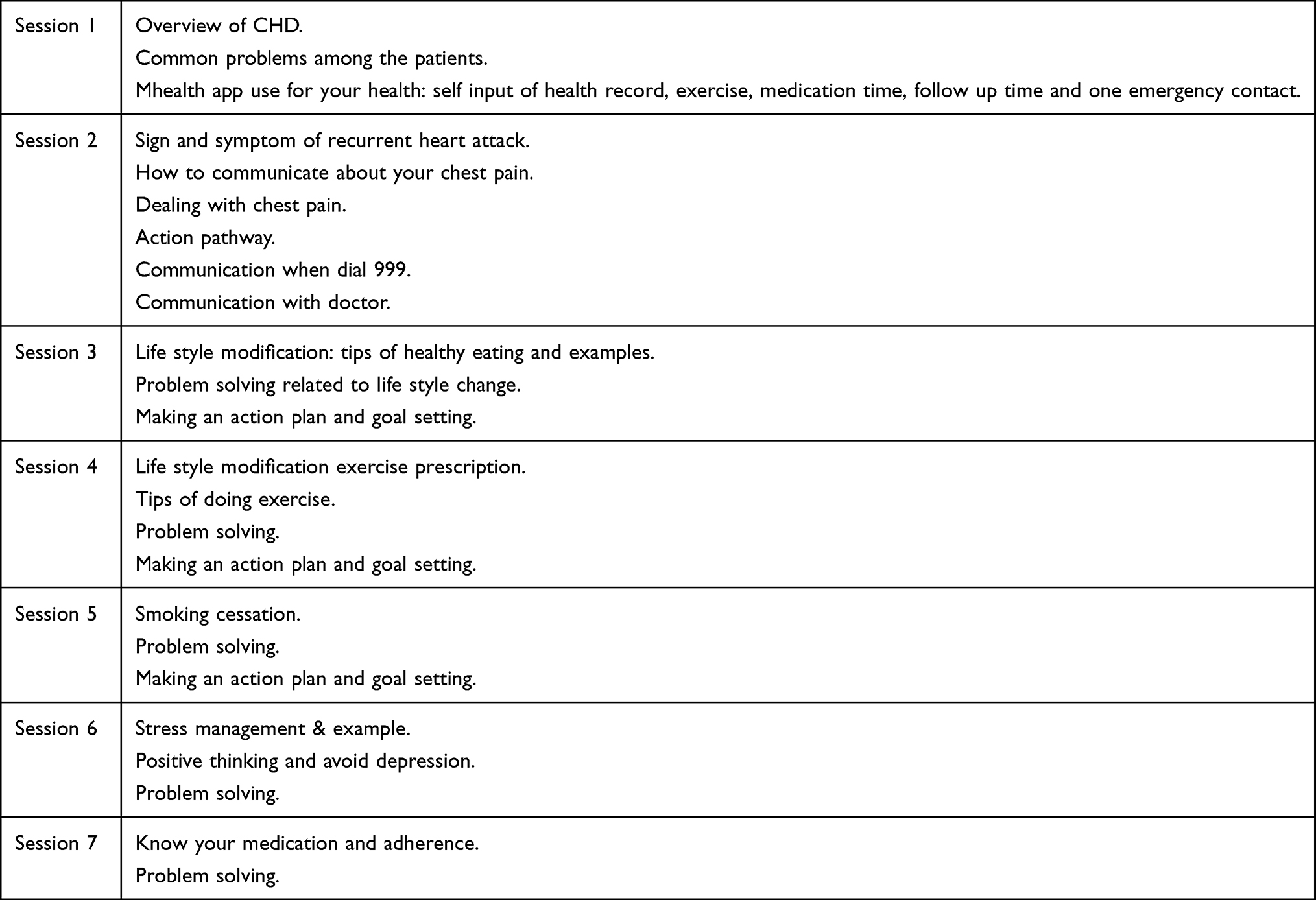 |
Table 1 Overview of the mhealth Educational Content Installed in the App |
 |
Figure 1 Front Page of the App. |
Usual Care
All the subjects continued to receive their usual care with prescribed medical treatments and follow-ups if any. By appointment, a trained nurse provided an individual briefing related to the CHD care. The participants were asked to quit smoking, adhere to their prescribed medications, lead a healthy lifestyle, and regularly perform a brisk walking exercise with moderate intensity at a rate of 5 to 6 km/h for at least 30 minutes per day, 5 days per week, as far as they were able to. Regular brisk walking has been reported to be a safe exercise that can strengthen a person’s cardiovascular function and muscles and mood.29 The App group and NTA group interventions both lasted for only 3 months. A systematic review reported that a programme of at least 3 months significantly improves outcomes.30
App Group
In addition to the usual care, the participant received a CHD app and a briefing from a trained research nurse. The app provided features such as structured e-educational contents and supportive features, which are described in the simple supplementary leaflet which were provided to the participants to take home. Only participants of the App group were able to use the membership area of the app, as it was restricted to individual member with the first time log in and password with own’s smart phone. To arouse interest in engagement in and fidelity to the app interaction by using their smart phone, the participants are encouraged to input own daily exercise time and type of exercise there. Weekly blood pressure input is also encouraged. If they forget to input their exercise daily with their smart phone, they can input it back within one week. An alert/feedback message in red was provided if the self-inputted health data, such as blood pressure, were found to be abnormal or they did not perform exercise for 2 weeks. In addition, two automatic messages (randomly generated from a pool of fifteen automatic messages) with encouraging words to sustain their exercise maintenance were provided weekly to all participants. Furthermore, the participants could easily read their health and exercise records, with trends shown in line charts. In summary, the app could help alert patients to their CHD risks (chest pain episodes, blood pressure) and provide support for their efforts to monitor their health and keep exercise records.
Nursing Telephone Advice (NTA) Group
In addition to the above usual care, three monthly 20-minute telephone follow-ups supplemented twice weekly by phone text messages were provided by a trained research nurse for up to 3 months. Participants could ask about their related health problems, if any. The nurse, who was experienced in cardiac nursing, might provide advice, or refer them to the emergency department if necessary. The team had set up a telephone advice guide to support the research nurse in giving phone advice and text messages. The contents of the phone text messages were similar to the WhatsApp messages sent to the App group.
In summary, both groups received similar nursing educational content relating to their CHD and care. The only difference was the reinforcement and continual support of the app feature such as CHD knowledge platform, exercise record and blood pressure record that was provided through an app for the App group or the regular nursing advice for the NTA group.
Data Collection Procedure
The collecting of follow-up data was held at baseline (T0), 1 month (T1), and 3 months (T2) by a trained research assistant (RA1) who was blinded to the group allocations. The research assistant performed physical assessments on the participants at the community centres or at a university research laboratory. The project was promoted through Facebook promotions and web postings at websites such as https://www.happy-retired.com/ (which has 50,000 members) and the Institute of Active Ageing (http://iaa.apss.polyu.edu.hk/), as well as at community centres (by means of web postings, poster displays, and health talks). Potential participants were approached via web link for a quick cardiac health screening using a simple e-survey form. The potential participants were further screened and approached by the RA1 via email or phone and invited to join the study. At an appointment with the RA1, participants signed the written consent form after receiving an explanation of the project. A survey form with baseline data (T0) was given to participants for self-administration. The survey form was then placed in a locked box. Individual participants were randomly allocated to one of the two groups (the App group, NTA group) and received their respective intervention according to the intervention protocol.
To ensure the quality of the participant recruitment, intervention, and data collection processes and to minimize subject contamination, the different groups were assigned different follow-up dates. The research assistant who was responsible for collecting data was blinded to the group allocations. That research assistant had received training on collecting data, taking blood using the finger-stick method, and using the auto blood analysers. Questionnaires measuring the primary outcome of total amount of physical exercise and the secondary outcomes including self-efficacy in illness management and numbers of emergency admission and hospitalization were distributed to the individual participants, who were asked to place their own completed survey forms in a locked box. The other secondary outcomes including systolic blood pressure, diastolic blood pressure, and body weight were obtained by using standardized and calibrated devices and blood lipid profile was taken using a finger stick with auto-analyser by RA1. The participants were asked to fast for 8 hours before the health assessment.
Ethical Considerations
Ethical approval and permission were obtained from the study university and the selected community centres (Departmental Research Committee, the Hong Kong Polytechnic University, reference number: HSEARS20190228001). RCT registration was obtained from the ClinicalTrials.gov Protocol Registration system (https://clinicaltrials.gov/). The registration number is ClinicalTrials.gov ID: NCT04054258. To ensure the rights of the participants, and the anonymity and confidentiality of the data, we followed the principles of the Declaration of Helsinki and ethical principles in designing the study. Written consent forms were obtained from all participants.
Regarding the safety of the subjects during the intervention, the PI and the research assistant monitored their progress for any problems that might occur during the intervention period, such as chest discomfort during brisk walking. No problems or complaints were raised by the participants in the study.
Outcome Measures
Two consecutive (1-, and 3-month) follow-ups were conducted for all participants. The primary outcome and the secondary outcomes are listed below.
Primary Outcome
Total amount of physical exercise: This outcome was measured using the Godin–Shephard Leisure Time Physical Activity Questionnaire (GSLTPA). This scale measures the frequency and duration with which the respondent has performed strenuous, moderate, and mild exercise outside of work duties. The respondent’s total weekly leisure activity is calculated in arbitrary units as a sum of the products of the separate components. This approach has been widely used in empirical studies and has been shown to exhibit good psychometric properties.31,32 Total exercise time per week was also recorded.
Secondary Outcomes
1. Self-efficacy in illness management: This is a six-item subscale of the Self-Management Behaviour Questionnaire. The Self-Management Behaviour Questionnaire was originally developed by Lorig, and the Chinese language version was translated and validated by Siu et al in Hong Kong.33,34 It includes a subscale using a Likert scale, namely the subscale of self-efficacy in illness management (six items), which was adopted, and the final sum of the score was calculated. The questionnaire was shown to have internal consistency, with Cronbach’s alpha values ranging from 0.72 to 0.91, and a retest reliability value, r, of 0.62–0.80.33,34
2. Clinical and Cardiovascular risk factors profile: The clinical and cardiovascular risk factors profile consisted of the number of emergency department attendances, the number of hospitalizations, participant’s systolic blood pressure, diastolic blood pressure, body weight, and blood lipid profile (LDL cholesterol, HDL cholesterol, triglycerides, and blood glucose). The systolic blood pressure, diastolic blood pressure, and body weight were obtained by using standardized and calibrated devices at baseline, 1 month, and 3 months by RA1. Blood lipid profile was taken at baseline and 3 months by using a finger stick with auto-analyser, and the participants were asked to fast for 8 hours.
3. Demographic and health profiles: Demographic data (age, gender, occupation, level of education) and information on medical problems (health problems, drug use, recent hospitalizations) were collected at baseline.
Process Evaluation
Process evaluation was conducted to evaluate the acceptability, strength, and weakness of the intervention. Three open-ended questions were asked regarding the acceptability and usefulness of the programme support. Process evaluation data were used to explain or supplement the RCT data.
Data Analysis
Data were analysed using SPSS version 26. The intention-to-treat principle was applied. The baseline characteristics of the groups was compared using a Chi-square or Fisher’s exact test for categorical variables, and a t-test or Mann–Whitney test for continuous variables, to examine the comparability of the groups by randomization. Con-founding variables were accounted for in subsequent analyses. The effectiveness of the App group versus the NTA group was evaluated by comparing the study outcomes using Generalized Estimating Equations (GEE) models. The GEE model was chosen because the GEE model could accommodate missing data caused by dropouts, if data were missing at random (which was particularly suitable for an ITT analysis), without the need to impute missing data.35 The between-group Cohen’s d was calculated to estimate the effect sizes of the app as compared to the booklet on each separate outcome measure. All statistical tests were two-sided and a p-value of <0.05 was considered an indicator of statistical significance.
Results
Eighty-two adults were assessed for eligibility via phone contact. Eighteen people were excluded for not meeting the eligibility criteria for CHD after a physical assessment and four declined to participate in the study after its purpose was explained. Sixty participants (30 in the App group and 30 in the NTA group) completed the study (Figure 2).
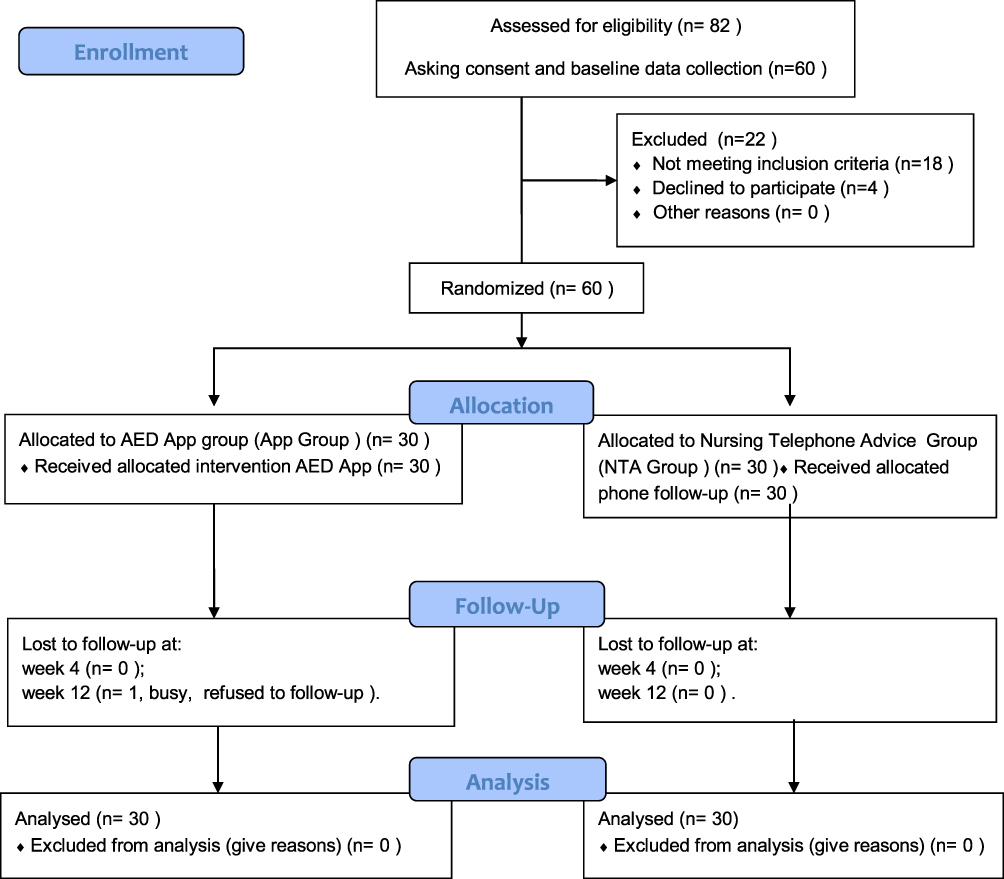 |
Figure 2 Study Flow Chart. |
Participant Outcomes
The mean age was 58.83 (SD 9.11) and 63 (SD 7.38) for the App group and the control group, respectively. Males comprised 56.7% (n=17) of the App group and only 30% (n=9) of the control group. Attrition rates of 3.33% (n=1) and 0% at T1 (1 month), and 3.33% (n=1) and 0% at T2 were observed for the App and NTA groups, respectively. The total attrition rate for all participants was 1.6% at T2. No significant difference was found in demo-graphic data between those who dropped out and those who completed the study. Moreover, no significant differences were found in baseline demographic or outcome data between the groups (Table 1). Most participants were obese, with a mean body mass index (BMI) of 25.63 (SD 3.23). Their mean systolic blood pressure was 138.85mmHg (SD 17.7 mmHg) and their mean diastolic blood pressure was 83.07 mmHg (SD, 10.95 mmHg). Most participants had completed secondary education or higher (85%, n=51), were married (65%, n=39), retired (46.7%, n=28), and were not currently smoking regularly (93.3% n=56). Less than half of them had a regular exercise habit (48.3%, n=29) and their mean exercise time was 195 min (SD, 154.01 min). Their self-efficacy chronic disease management score (SES) was about 7.36; SD=1.4. Their LDL cholesterol and triglyceride levels were abnormal, while their blood glucose level belonged to the at-risk group, with a blood glucose level of 5.67 for the App group and 5.61 for the NTA group. No significant differences were found between the two groups with respect to demographic or clinical characteristics (Table 2).
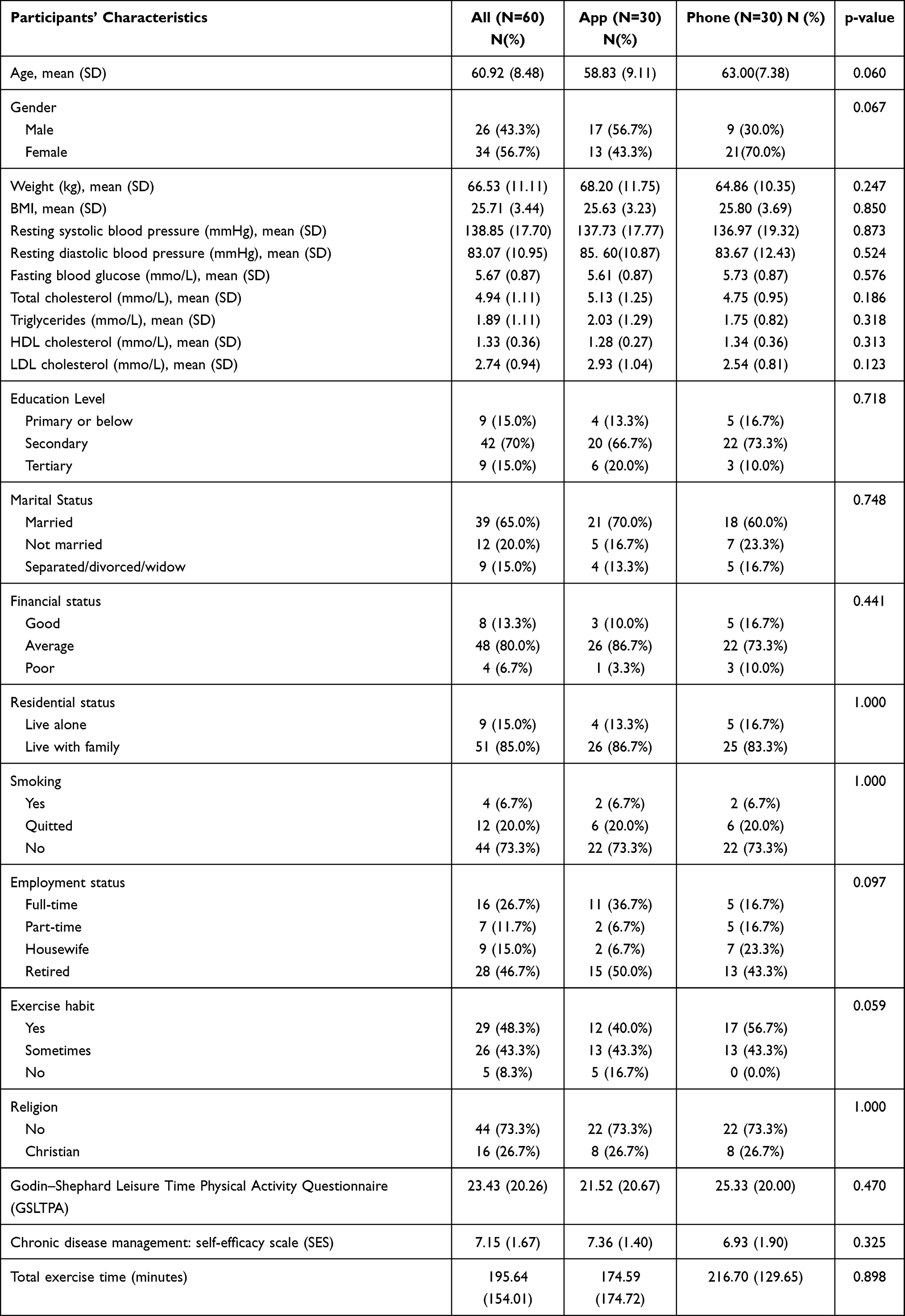 |
Table 2 Characteristics of the Participants |
Regarding ED attendance within the study period, only one patient from the App group and one patient from the NTA group admitted to the emergency department hospital only due to recurrent chest pain. Both were discharged home after doctor consultation. Table 3 summarizes the mean, the SD of the outcomes, and the effect size of the GEE results of the outcomes (SES score, body weight, BMI, lipid and fasting blood glucose concentrations, blood pressure, total exercise time, GSLTPA (total exercise amount)) within 3 months between the two groups. Compared to the NTA group, the App group performed better with a medium effect size, as seen in a greater improvement in the total amount of exercise (Cohen’s d 0.43) and greater reductions in total cholesterol level (Cohen’s d −0.43), triglycerides level (Cohen’s d −0.39), and diastolic blood pressure (Cohen’s d 0.32); although there was only a small effect on the reduction in body weight (Cohen’s d −0.1) and LDL cholesterol Cohen’s d −0.19). On the other hand, the NTA group resulted in greater increment in self-efficacy of chronic disease management than the app group, with Cohen’s d = −0.50 at 1 month and −0.03 at 3 months. Significant improvement was found on self- efficacy of chronic disease management at 1 month only (B −0.793, p=0.037), but not at T2 (3 months).
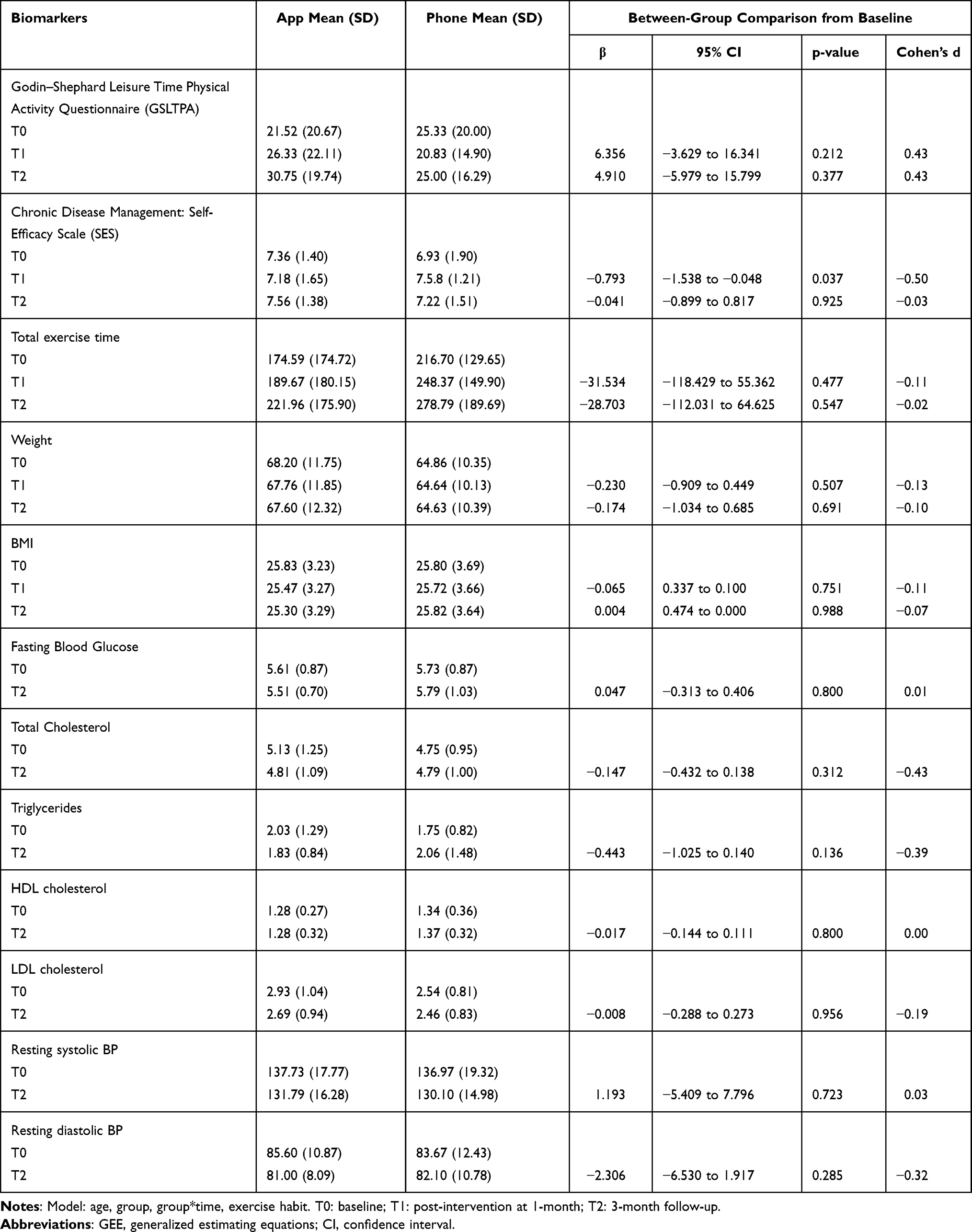 |
Table 3 Mean and Standard Deviation of Outcomes and Results of Generalized Estimation Equation (GEE) Models for the Comparison of the Repeated Measures Outcome Variables Between the Two Groups |
Process Evaluation
We assessed the feasibility of the programme by examining the recruitment rate, which was good at 1.67%, (n=1) at T2. Acceptability was assessed through a qualitative analysis of the perceptions of the participants. Most of the participants (93.3% n=28) in the App group and 96.6% (n=29) of the group advice group appreciated the intervention programme. The App group found that the app was useful, easily accessible for exercise maintenance, and that the information platform was particularly useful for their CHD care and for alerting them to the importance of making lifestyle modifications, such as the importance of exercise maintenance. They appreciated the user-friendly features, easy accessibility, and the ability to view or input their exercise time at their own pace and time. One drawback of the app was that the speed was slow if they had an older smartphone. The NTA groups also expressed great appreciation for the nursing advice, although five participants claimed that the contact time with nurses might not be convenient at times due to their work commitments or other scheduling conflicts. The mean number of successful contacts with advice given to a participant ranged from two to five times. Suggestions of ways to further improve the app included providing such features as automatic step counts and more frequent reminders (n=2). Overall, these findings indicated that the proposed intervention was feasible and well appreciated by the participants.
Discussion
The overall aim of this study was to examine the preliminary effects of a nurse-led support programme for patients who were at risk of developing CHD on outcomes of total exercise, self-efficacy of chronic disease management, emergency department attendance and hospitalizations, CHD risk factor profile, and acceptability as perceived by the patients. Before the intervention, only 48% of the participants had an exercise habit, although the majority (61.6%) did not work either full time or part time. Compared to the NTA group, the App group performed better, with a small to moderate effect on total cholesterol level, tri-glycerides level, diastolic blood pressure, and total amount of exercise (GSLTPA), against a small effect on body weight and LDL cholesterol. These results indicate that the app effectively promoted regular aerobic physical exercise, such as brisk walking, leading to a reduction in total cholesterol, triglycerides, LDL and cholesterol, and better blood pressure control within 3 months.
The results showed that the App group engaged in a greater total amount of physical exercise, as measured by their GSLTPA score, than did the NTA group, who showed little improvement in their total amount of exercise. The result indicates that the app was effective at promoting the performance of more moderate-intensity exercise.
The result also showed a small-to-moderate effect, with more greater reductions of in total cholesterol concentrations, the triglyceride concentrations, and systolic blood pressure in the App group compared to the NTA group. A possible explanation for these results is that the App group increased the total amount of physical exercise that they engaged in, which led to better blood pressure control, and to a reduction in total cholesterol and LDL cholesterol reduction over the 3-month study period. Exercise was proven proved to be effective in controlling blood pressure and lipids control (Carlson et al, 2001). In this study, our intervention likely elicited positive effects on lipid control, blood pressure controls up to 3 months. The findings were consistent with a previous study in Hong Kong that participants in the intervention group (with more e-health support for exercise maintenance) demonstrated continuous improvements in body weight, total exercise amount and self-efficacy for exercise, and lipid level as well.21 A significant interaction effect was observed on the self-efficacy of chronic disease management (SES) at T1 (1 month) only, but not at T2 (3 months). A possible explanation for this is that nursing counselling via phone contact still had a superior impact on supporting patients’ self-care in the short term, which is consistent with the findings in the literature.16 A significant improvement was found in SES at 1 month only, not at T2 (3 months). The result highlights the importance of providing professional support via phone contact as this might lead to more interactions with the nurse and might make the patients feel that they are being cared for. With encouragement from the nurse, patients might have more confidence in performing the exercise tasks, leading to a change in their behaviours, (ie, spending more exercising). The participants in the NTA group performed better in self-care via the professional nursing support within 1 month. But this only resulted in an increase in their total exercise time, not in the intensity of the exercise, which would be needed to achieve an improvement in clinical outcomes such as lipid profiles.
Given that the same information on CHD care was provided to both the NTA and App groups, the members’ area and interactive platform and other features of the CHD app may have further motivated the participants to self-monitor their health and record details of their exercise, body weight, blood pressure, and blood glucose, thereby enhancing the participants’ SES within 3 months. A positive trend was observed in the App group with the improvement in their SES score of 7.36 to 7.56, while the phone group also showed improvement of 6.93 to 7.22, although a non-significant result was observed between groups. The success of the NTA group may be due to their labour-intensive components, such as individual nursing phone counselling for dietary and exercise advice. However, the App group relied solely on the App support to improve their knowledge of CHD care and modification of exercise behaviour. Consistent with the preliminary RCT data, our qualitative findings on the process evaluation also showed that the participants in the both the App and NTA groups mostly accepted and appreciated the support that they received on exercise maintenance. However, the app group could be more beneficial due to easy accessibility to the app at any time. In the NTA group, they are waiting for the nurse to call them which might be at an inconvenient time. Furthermore, NTA group required more human resources in terms of nursing time and effort.
In summary, the study adds more evidence that a small-to-moderate effect, with more greater reductions of in total cholesterol concentrations, the triglyceride concentrations, and systolic blood pressure in the App group compared to the NTA group. This app might have helped the participants to improve their level of knowledge regarding self-management in CHD care, adhere to positive lifestyle modifications (eg, engaging in exercise), and self-monitor their blood pressure, body weight, and lipid measures. Accordingly, the participants also experienced good nursing support via either phone advice or the CHD app. The CHD app might be superior to phone contact because it consumes less in terms of manpower resources, is easily accessible, and could be sustainable within 3 months. Our CHD app could be incorporated in the programme and promoted to the population on a larger scale to reduce cardiovascular risks using limited human resources.
Limitations
This study has several limitations. First, the sample size was small and only two websites, one Facebook site, and two community centres were used for promotion, which might affect the generalizability of the results. More motivated people than average might have joined the study. Second, the Hawthorne effect might have been present for the NTA group, which might have affected the results. Third, the data relied on the participants’ self-inputted exercise records, and some participants might have forgotten to input their data. An objective tool for measuring exercise might be used in future studies if funding permits. Lastly, the older mean age of participants could mean that this group of people might have a harder time using technology. They are perhaps more used to speaking on the phone rather than navigating through an app. A large-scale multi-centre RCT is needed to confirm the results observed in this pilot study. A sustainable, longer-term effect (6 months or longer) or an e-health intervention with a stronger dose in terms of features designed to engage the patients so that they exercise in a sustainable manner might be explored in the future.
Conclusion
At-risk CHD is a common health problem associated with a heightened risk of developing cardiovascular disease. The risks could be reduced through lifestyle interventions and the provision of appropriate professional support for self-care. This pilot study showed that the use of a CHD app was better to increase the participant’s total amount of exercise and improve their clinical and cardiovascular risk factors profile in terms of blood pressure, body weight, and blood lipid profile. With a good recruitment rate and high satisfaction from the participants, it might be feasible in the future to incorporate this app into a larger-scale health promotion programme to test its effectiveness.
Data Sharing Statement
The authors do not intend to share individual deidentified participant data.
Acknowledgments
Sincere thanks to the grant support by Nam Kee Noodle Foundations Ltd and UGC matching grant of Hong Kong SAR (Grant number ZJM9) to support our research work. Special thanks to the patients who participate in our project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Cardiovascular diseases (CVDs); 2021. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/.
2. The Government of the Hong Kong Special Administrative Region. Coronary heart diseases; 2021. Available from: https://www.healthyhk.gov.hk/phisweb/en/chart_detail/24/.
3. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18:109–114. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
4. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the management of patients with Non–ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014;64:e139–e228. doi:10.1016/j.jacc.2014.09.017
5. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: executive Summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines, and the heart rhythm society. J Am Coll Cardiol. 2019;74:932–987. doi:10.1016/j.jacc.2018.10.043
6. Artinian NT, Fletcher GF, Mozaffarian D, et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults: a scientific statement from the American Heart Association. Circulation. 2010;122:406–441. doi:10.1161/CIR.0b013e3181e8edf1
7. Kotb A, Hsieh S, Wells GA, Guo Y. The effect of telephone support interventions on coronary artery disease (CAD) patient outcomes during cardiac rehabilitation: a systematic review and meta-analysis. PLoS One. 2014;9:e96581. doi:10.1371/journal.pone.0096581
8. Chow CK, Ariyarathna N, Islam SMS, et al. mHealth in cardiovascular health care. Heart Lung Circ. 2016;25:802–807. doi:10.1016/j.hlc.2016.04.009
9. World Health Organization. mHealth, New horizons for health through mobile technologies. Available from: http://www.who.int/goe/publications/goe_mhealth_web.pdf.
10. Antypas K, Wangberg SC. An Internet- and mobile-based tailored intervention to enhance maintenance of physical activity after cardiac rehabilitation: short-term results of a randomized controlled trial. J Med Internet Res. 2014;16:e77. doi:10.2196/jmir.3132
11. Chow CK, Redfern J, Hillis GS, et al. Effect of lifestyle-focused text messaging on risk factor modification in patients with coronary heart disease: a Randomized Clinical Trial. JAMA. 2015;314:1255–1263. doi:10.1001/jama.2015.10945
12. Khonsari S, Subramanian P, Chinna K, et al. Effect of a reminder system using an automated short message service on medication adherence following acute coronary syndrome. Eur J Cardiovasc Nurs. 2015;14:170–179. doi:10.1177/1474515114521910
13. Maddison R, Pfaeffli L, Whittaker R, et al. A mobile phone intervention increases physical activity in people with cardiovascular disease: results from the HEART randomized controlled trial. Eur J Prev Cardiol. 2015;22:701–709. doi:10.1177/2047487314535076
14. Kassavou A, Sutton S. Automated telecommunication interventions to promote adherence to cardio-metabolic medications: meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychol Rev. 2018;12:25–42. doi:10.1080/17437199.2017.1365617
15. Islam SM, Farmer AJ, Bobrow K, et al. Mobile phone text-messaging interventions aimed to prevent cardiovascular diseases (Text2PreventCVD): systematic review and individual patient data meta-analysis. Open Heart. 2019;6:e001017. doi:10.1136/openhrt-2019-001017
16. Park LG, Beatty A, Stafford Z, et al. Mobile phone interventions for the secondary prevention of cardiovascular disease. Prog Cardiovasc Dis. 2016;58:639–650. doi:10.1016/j.pcad.2016.03.002
17. Adler AJ, Martin N, Mariani J, et al. Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;4:CD011851. doi:10.1002/14651858.CD011851.pub2
18. Tam HL, Wong EML, Cheung K, et al. Effectiveness of text messaging interventions on blood pressure control among patients with hypertension: systematic Review of Randomized Controlled Trials. JMIR mHealth and uHealth. 2021;9:e27347. doi:10.2196/24527
19. Doupis J, Festas G, Tsilivigos C, et al. Smartphone-based technology in diabetes management. Diabetes Ther. 2020;11:607–619. doi:10.1007/s13300-020-00768-3
20. Dorje T, Zhao G, Tso K, et al. Smartphone and social media-based cardiac rehabilitation and secondary prevention in china (SMART-CR/SP): a parallel-group, single-blind, Randomised Controlled Trial. Lancet Digit Health. 2019;1:e363–e374. doi:10.1016/S2589-7500(19)30151-7
21. Wong EML, Leung DYP, Chair SY, et al. Effects of a web-based educational support intervention on total exercise and cardiovascular risk markers in adults with coronary heart disease. Worldviews Evid Based Nurs. 2020;17:283–292. doi:10.1111/wvn.12456
22. Schulz KF, Altman DG, Moher D, et al. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7:e1000251. doi:10.1371/journal.pmed.1000251
23. Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008;31:180–191. doi:10.1002/nur.20247
24. Wong EML, Leung DYP, Tam HL, et al. The effect of a lifestyle intervention program using a mobile application for adults with metabolic syndrome, versus the effect of a program using a booklet: a Pilot Randomized Controlled Trial. Clin Interv Aging. 2021;16:633–644. doi:10.2147/CIA.S303920
25. Wong EML, Leung DYP, Wang Q, et al. A nurse-led lifestyle intervention using mobile application versus booklet for adults with metabolic syndrome-Protocol for a randomized controlled trial. J Adv Nurs. 2020;76:364–372. doi:10.1111/jan.14241
26. Bandura A. Self-Efficacy: The Exercise of Control. New York: W.H. Freeman; 1997.
27. Carlson JJ, Norman GJ, Feltz DL, et al. Self-efficacy, psychosocial factors, and exercise behavior in traditional versus modified cardiac rehabilitation. J Cardiopulm Rehabil. 2001;21:363–373. doi:10.1097/00008483-200111000-00004
28. Laplante C, Peng W. A systematic review of e-health interventions for physical activity: an analysis of study design, intervention characteristics, and outcomes. Telemed J E Health. 2011;17:509–523. doi:10.1089/tmj.2011.0013
29. Centers for Disease Control and Prevention. Benefits of physical activity. Available from: https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm.
30. Lin CH, Chiang SL, Tseng WC, et al. Systematic review of impact of lifestyle-modification programs on metabolic risks and patient-reported outcomes in adults with metabolic syndrome. Worldviews Evid Based Nurs. 2014;11:361–368. doi:10.1111/wvn.12069
31. Godin G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fit J Canada. 2011;4:18–22.
32. Godin G, Shephard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci. 1985;10:141–146.
33. Siu AM, Chui DY. Evaluation of a community rehabilitation service for people with rheumatoid arthritis. Patient Educ Couns. 2004;55:62–69. doi:10.1016/j.pec.2003.08.001
34. Siu AMH, Chan CCH, Poon PKK, et al. Evaluation of the chronic disease self-management program in a Chinese population. Patient Educ Couns. 2007;65:42–50. doi:10.1016/j.pec.2006.04.013
35. Sawilowsky S. New effect size rules of thumb. J Mod Appl Stat Methods. 2009;8:597–599. doi:10.22237/jmasm/1257035100
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.