Back to Journals » Risk Management and Healthcare Policy » Volume 13
Effectiveness of a Health Talk Education Program on Human Papillomavirus (HPV) Knowledge, Attitudes, and Intentions to Vaccinate Children Among Mothers of Secondary School Boys in Thua Thien Hue Province, Vietnam
Authors Nguyen Minh D ![]() , Taneepanichskul N, Hajek R
, Taneepanichskul N, Hajek R ![]()
Received 24 April 2020
Accepted for publication 14 July 2020
Published 18 August 2020 Volume 2020:13 Pages 1207—1214
DOI https://doi.org/10.2147/RMHP.S259097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Video abstract presented by Nguyen Minh Duc.
Views: 437
Duc Nguyen Minh,1,2 Nutta Taneepanichskul,1 Richard Hajek3
1Colleges of Public Health Sciences, Chulalongkorn University, Bangkok, Thailand; 2Hue Central Hospital, Hue City, Vietnam; 3MD Anderson Cancer Center, Houston, TX, USA
Correspondence: Nutta Taneepanichskul Colleges of Public Health Sciences
Chulalongkorn University, Bangkok, Thailand
Tel +66 02-218-8197
Email [email protected]
Background: The incidence of cancer related to human papillomavirus (HPV) that affects males is rising throughout the world. Currently, Vietnamese boys are typically not vaccinated against HPV while girls are. There are only a few studies pertaining to HPV vaccination among boys in Asian countries where parents play the most important role in deciding on such vaccination. We present here the first study to assess the effectiveness of a health talk education program on HPV knowledge, attitudes and intention to vaccinate children among mothers of secondary school students in the Thua Thien Hue province, Vietnam.
Methods: This was a quasi-experimental study. Two secondary schools in the Thua Thien Hue province, Vietnam were selected by purposive sampling. A total of 288 mothers of male students of two secondary schools were selected to participate, n=144 as controls and n=144 for the intervention arm for every school. Mothers of male students were invited to answer interview questions. The questionnaires covered social demographics, health history, HPV knowledge and HPV vaccination perception and intention. The study ran from September 2019 to January 2020.
Results: In total, 279 mothers finished the questionnaires. At the baseline, HPV knowledge in both groups was at the same level (p> 0.05). One month after receiving the HPV health talk education, mothers of male students had much higher HPV knowledge than those who did not receive such HPV health talk education. The intervention group also had a much higher HPV vaccination intention than the control group (p< 0.05).
Conclusion: Health education was shown in this study to be an effective method to increase HPV knowledge and vaccination intention among mothers of boys in Vietnam.
Keywords: health talk education, human papillomavirus (HPV) vaccination, perception, intention, Vietnam
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted disease and a significant contributor to the global cancer burden.1 This virus can cause several types of cancer including cervical, vulvar, vaginal, and anal cancer in women, and penis and certain head and neck cancers in men, the latter being the most frequently occurring HPV-related cancer.2–6 It is well known that the incidence of cancers relating to HPV in males is rising. HPV is also the main cause of cervical cancer. In the US, 90% of patients suffering from cervical cancer are affected by HPV. It is estimated that roughly 70% oropharyngeal cancers, 90% anal cancers, and 60% of penile cancers are HPV-associated.7
Between 2009 and 2013, there were about 9,600 cases in males and about 2,000 cases in females in the US.8,9 Rates of oropharyngeal SCC among females were lower than for males (1.7% vs. 7.6%), while the rates of anal SCC in females were higher than for males (1.8% vs. 1.1%).9 Globally, 38,000 new cases (85%) of head and neck cancers, 35,000 (87%) cases of anal cancers and 90% of cervical cancer are caused by HPV.1
Fighting HPV in males is a very important public health issue. In 2006, the FDA approved the Gardasil vaccine that can protect against four types of HPV (6, 11, 16, 18) for females aged 9–2610 and approved it for males aged 9–26 3 years later in 2009.11 There are two available and approved HPV vaccines in Vietnam (Gardasil and Cervarix) for girls aged 11–26.12 In contrast to girls, Vietnamese boys are not vaccinated against HPV13 and there is no specific age recommendation for them.
For Vietnamese women aged 15 to 44, the second most common cancer is cervical cancer with most cases related to HPV infection.14
The uptake rate of HPV immunization in developing countries remains comparatively low.15,16 The HPV vaccine uptake rate in Vietnam (31.8%)17 was higher than previously reported (2.3%),18 however lower than China (47.2%) and for European countries such as Germany (53%)19 and the Netherlands (49.9%).20 A three-shot series of the vaccine in Vietnam costs from $150–$195 which is comparatively low compared to the global average of $400.21
At nearly once-tenth of the 2016 average per capita income of $2,170, this remains out of the reach of most Vietnamese citizens.21 Next to high costs22,23 reasons include lack of knowledge24 and negative attitudes towards the HPV vaccine.25
Although most health care providers in Vietnamese private clinics recommend giving boys a HPV vaccination, it is not recommended for them at government health centers.
In Vietnamese families, mothers spend more time taking care of children’s health, encouraging their self-care, as well as monitoring nutrition, than fathers do.26 It is therefore usually easier for mothers to talk to teenagers about sensitive issues such as reproductive or sexual health than it is for fathers.27
In order to understand whether parents of boys have any plans for HPV vaccination if it is available, we wanted to investigate if they have the required knowledge about HPV and the intentions to have their male children HPV-vaccinated.
As far as we know, no study about HPV knowledge, attitudes and intention to vaccinate among parents of boys in any Asian country has been conducted as of yet. This study assesses attitudes and rates of HPV knowledge and vaccination intention, and measures whether a health talk education intervention affects these factors among mothers of male students in Thua Thien Hue province of Vietnam.
Methods and Participants
This study was conducted from September 2019 through January 2020 in secondary schools in Thua Thien Hue province, which is in the central region of Vietnam. In this exploratory phase of the study, inclusion criteria included: 1) Mothers of male students aged 11–14 years; 2) Mothers of these students who provided written consent; 3) Mothers of these students who were 31 to 60 years of age; 4) Mothers who were able to take responsibility for their children’s vaccinations; and 5) Exploratory phases were selected to capture data on mothers eligible to attend HPV education intervention. Exclusion criteria included: 1) Mothers who were not sure they could participate throughout the whole study; 2) Mothers of secondary school male students who already received a HPV vaccination; and 3) Secondary school male students who already received HPV vaccinations.
According to previous studies28 having change intention of HPV vaccination intention among mothers in the intervention group and control group. Using the G power application testing two proportions, researchers have a sample size with a 5% significance level and 80% statistical power.
The sample size was increased by 10% in case someone decided not to participate or was absent during the collection period. With these calculations, we arrived at 144 mothers for each arm.
Those arms included mothers of male students from two secondary schools. The male students were adolescents aged 11–14 years. The two secondary schools were selected by using purposive sampling, both are urban schools and have similar characteristics regarding the education level, number of classes, and male to female student ratios. These two secondary schools are located in two districts and these districts have citizens with a similar social-economic status, age, and education.
In the years 2019 and 2020, mothers of male students from these two schools were invited to participate in this study. Two hundred eighty-eight mothers were informed of the study’s purpose, the potential benefits and any known risks. Participants who wanted to join the study signed the Informed Consent Forms written in Vietnamese. This study was approved by the Ethical Committee of Hue University of Medicine and Pharmacy, Vietnam.
Before the intervention, 279 mothers in both the control group (138 mothers) and the intervention group (141 mothers) completed the pre-intervention questionnaires after a detailed explanation by the researchers. The pre-intervention questionnaire included socio-demographic characteristics (including age of the mothers, marital status, religion, ages of the children, personal income, level of education, and residence) and following questions: 1) Do you know anything about HPV; 2) Have you ever heard of HPV vaccines; 3) Have you ever heard of penile cancer, or anal cancer in men; and 4) Have you ever heard of genital warts in men?29,30 The research team collected and checked all completed questionnaires.
One hundred forty-one mothers of the intervention group attended the HPV health talk education which took place at the secondary school every Saturday and Sunday mornings for one month. It consisted of PowerPoint presentations and two-way communications – in general, many interactions with the audience of 10 people at a time and one research assistant. The small group discussed the HPV education content that researcher presented. The content of the education was guided by information from the WHO, CDC, and other reputable health-based websites, and from input of experts from the US and Vietnam.
After the education intervention, the mothers were asked to complete the post-intervention questionnaires. Research assistants included three medical doctors and 6 assistants to collect data, talk with mothers of the male students and take notes during the education intervention. The questionnaire included questions regarding knowledge of HPV in males30,31 attitudes of HPV vaccination for sons32 and intentions to give males HPV vaccination.33 The study flowchart is shown in Figure 1.
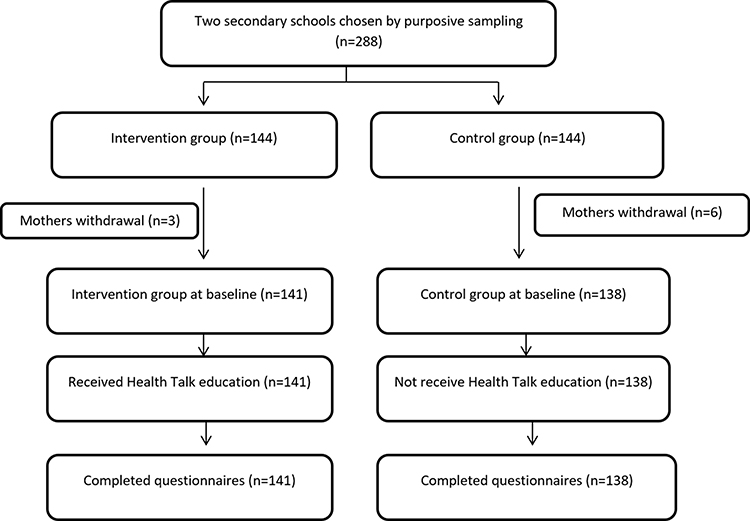 |
Figure 1 Flowchart of study design. |
The KR 20 of HPV knowledge was found to be 0.8. Cronbach’s Alpha of perceived barriers and benefits was 0.828. The IOC score for HPV knowledge was found to be 0.917, for perceived barriers and benefits 0.917 and for HPV vaccination intention 1.00. Content validity was checked by three experts through pilot testing of 30 mothers using IOC scores.
Statistical analysis: We used frequency and percentages to describe the characteristics of mothers and their HPV knowledge and attitudes towards HPV vaccination (Table 1). To analyze the differences in both groups at baseline and to compare the mothers’ knowledge, we used contingency tables and a Chi-squared test. Those were also used to compare the knowledge and vaccination intention in both groups. A Mann–Whitney U-test was used to assess different median scores of HPV knowledge of the control and intervention group. Data were analyzed using SPSS software (version 18.0). A p-value <0.05 was considered statistically significant.
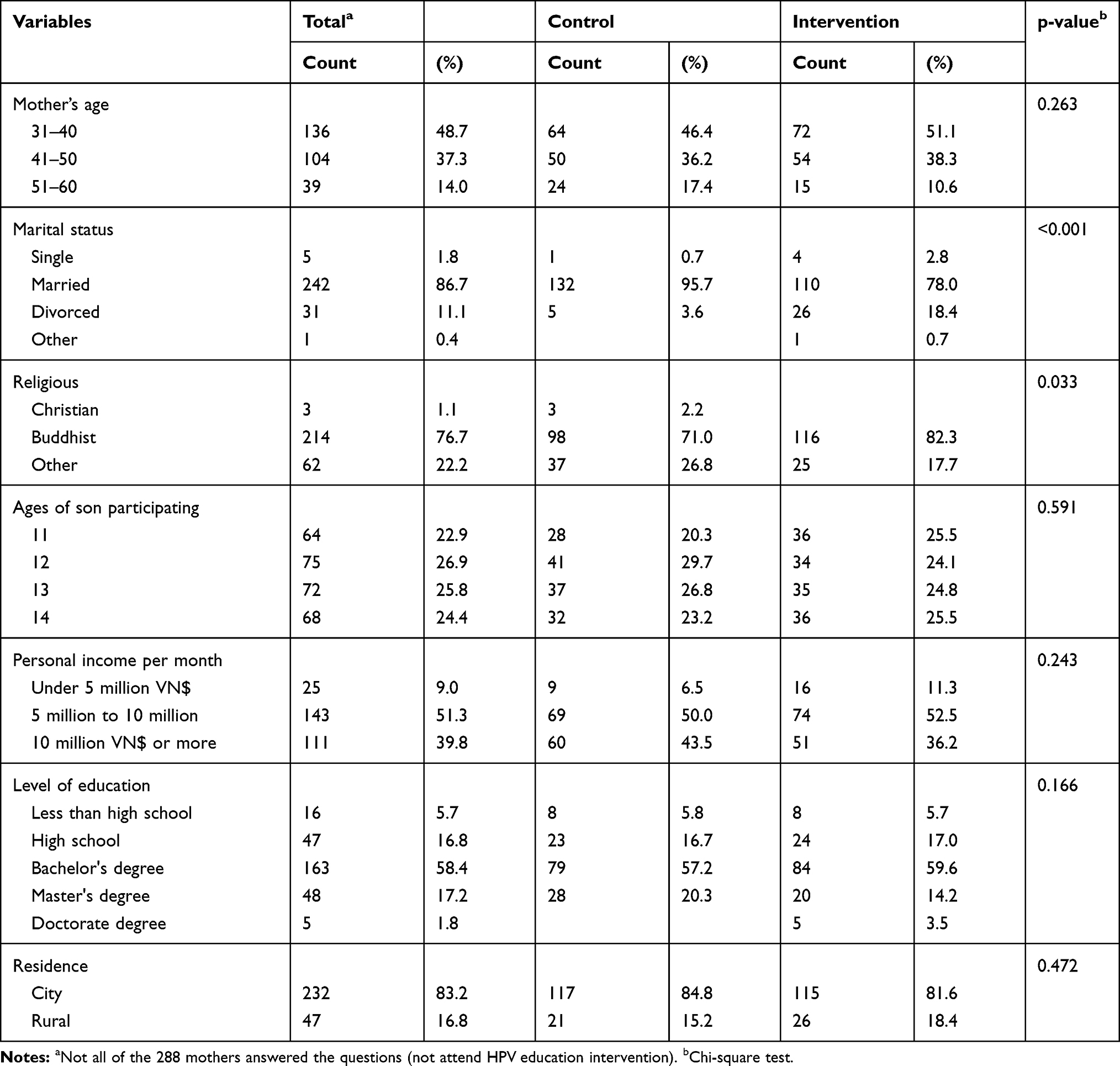 |
Table 1 Sample Characteristics |
Results
Two hundred seventy-nine mothers attended the study and all of them finished the questionnaires (9 mothers withdrew without reasons) (Table 1).
At baseline, there were no significant differences found in both groups regarding their reports of having heard about HPV (p=0.448), HPV vaccine (p=0.380), penile and anal cancer in males (p=0.111), and genital warts in males (p=0.679) (Table 2).
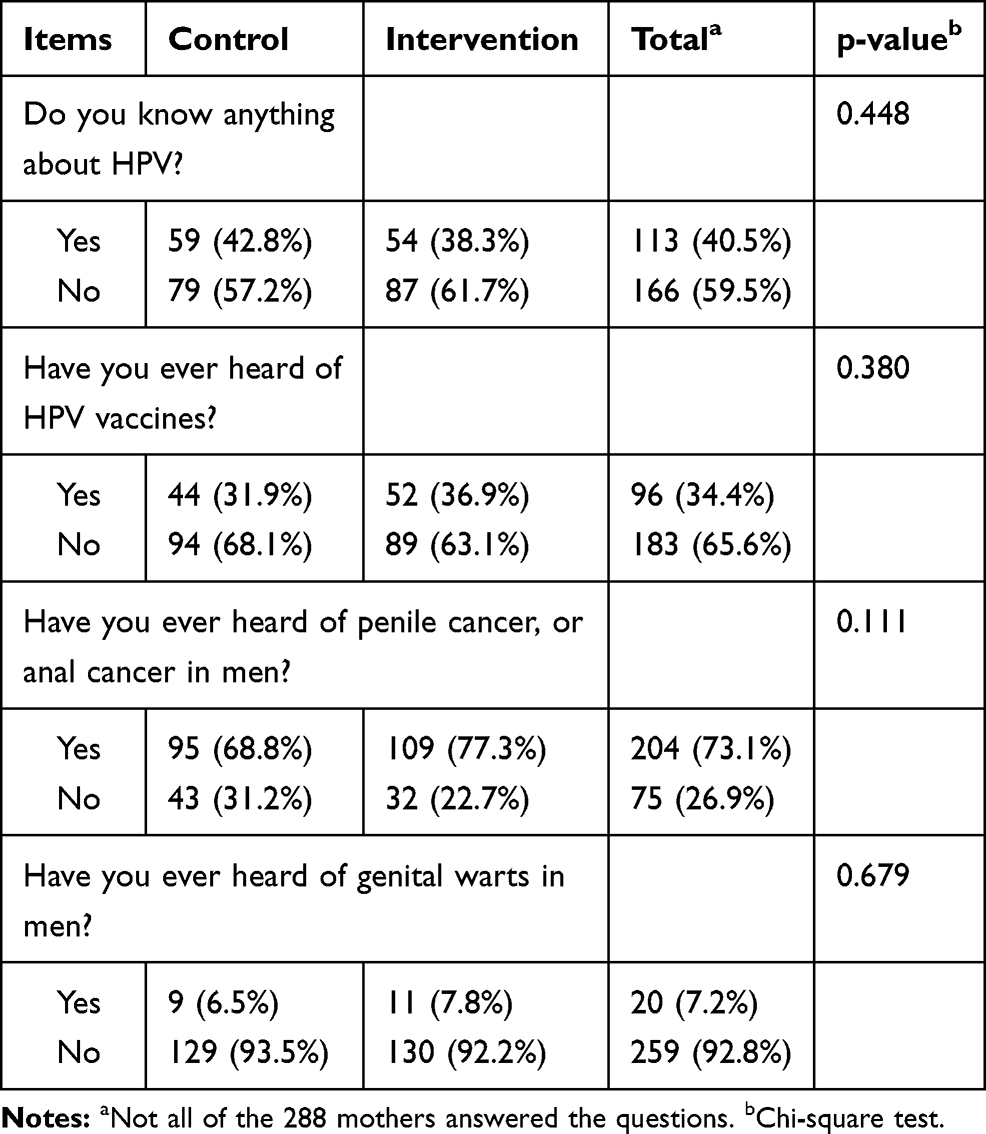 |
Table 2 HPV Awareness and Attitudes at Baseline |
After the intervention, the number of mothers who gave correct answers were much higher in the intervention group than those in the control group, answeting questions such as whether HPV is a sexually transmitted infection (92.9% vs. 81.9%), men cannot get HPV (90.1% vs. 27.5%), types of HPV (95% vs. 68.8%), HPV can be transmitted through oral sex (86.5% vs. 41.6%), HPV infection can cause oropharyngeal cancer (92.2% vs. 26.8%), HPV infection can cause genital warts in boys (92.2% vs. 26.8%), HPV infection can cause penile cancer in boys (90.8% vs. 28.3%), HPV vaccine protects you from some types of HPV (89.4% vs. 71.7%), HPV vaccine is most effective for those who have not had sexual intercourse (83.7% vs. 65.2%). All HPV knowledge between intervention group and control group are different (p<0.05) (Table 3).
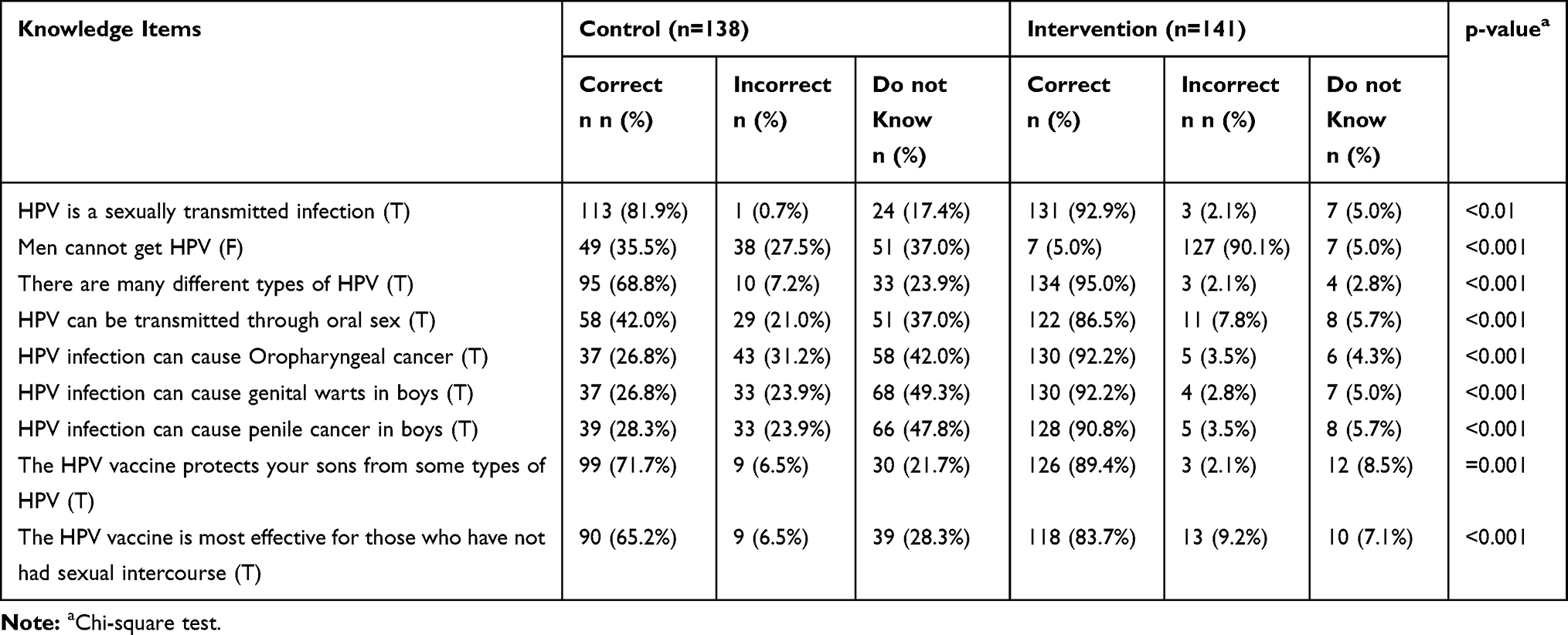 |
Table 3 Comparison of HPV Knowledge After Receiving Education Intervention Between Two Groups |
HPV knowledge scores were much higher for mothers who joined health talk education intervention (MDN = 8.0) than those who did not receive HPV health talk education (MDN = 4.0). A Mann–Whitney U-test showed that mean scores of both groups HPV knowledge are different (p<0.001) (Table 4)
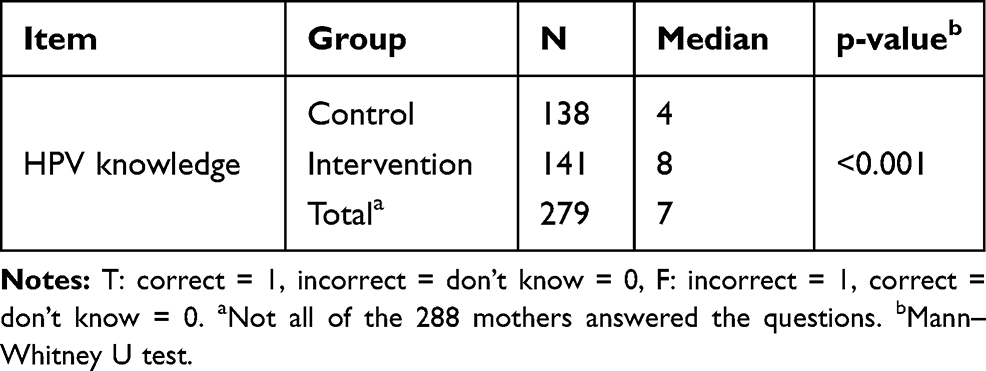 |
Table 4 Median Score of HPV Knowledge of Control and Intervention Group |
Regarding the attitudes towards benefit and barriers of HPV vaccine, there are significant differences between the control and intervention group (P<0.001) (Table 5).
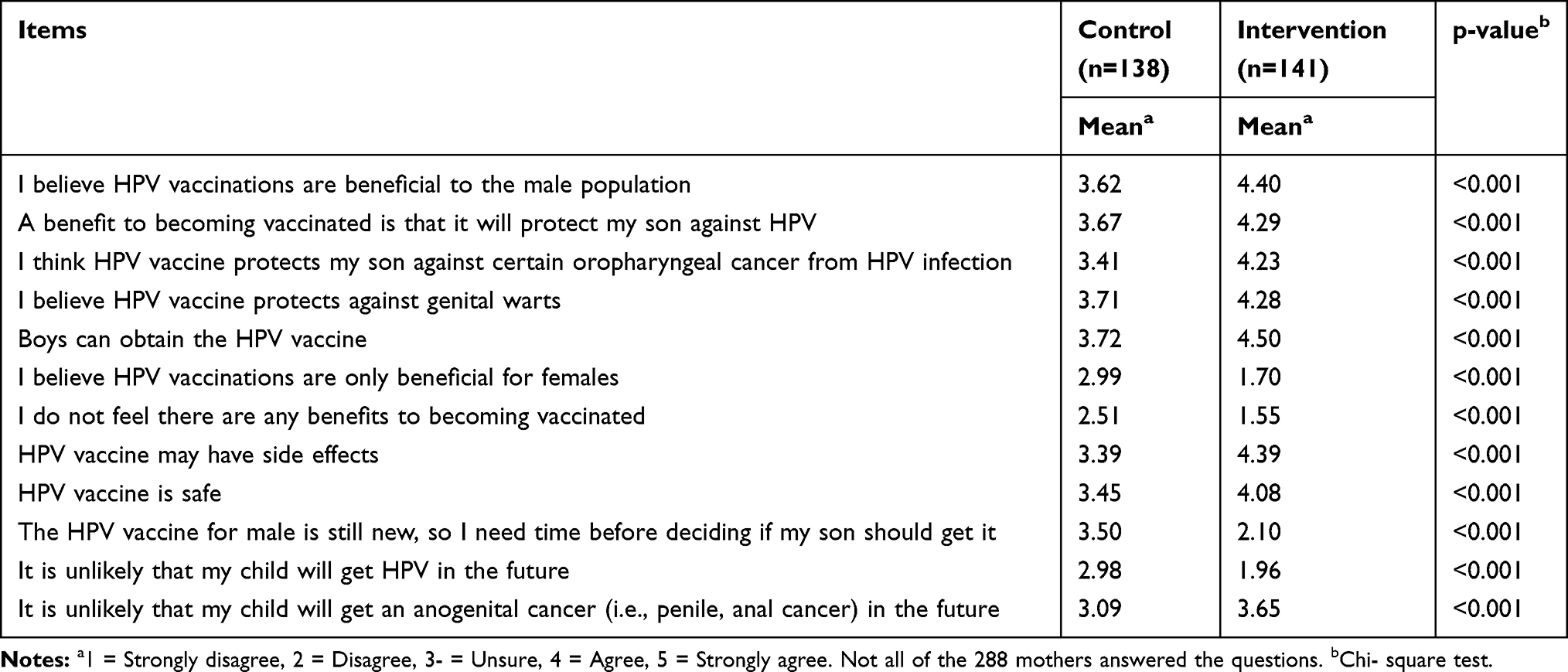 |
Table 5 Attitudes Towards Benefit and Barriers of HPV Vaccine |
The HPV vaccination intention was found to differ significantly in both groups (p<0.001), with the HPV vaccination intention in the intervention group being much higher (89.4%) than in the control group (53.6%) (Table 6).
 |
Table 6 HPV Vaccine Intention |
Discussion
To our knowledge, this is the first study in an Asian country which has evaluated the effect of HPV health talk education on the knowledge and perception towards HPV vaccination intention in males. Less than half of the mothers of male students in our survey had heard about HPV prior to the survey. After receiving the education, most of the mothers thought their sons should be vaccinated against HPV in the future. The detailed findings in depth are as follows:
HPV Awareness and Knowledge
After receiving the health talk education, the knowledge on HPV of the intervention group was much higher than for the control group. In the control group, very few mothers had the right answers for the questions related to HPV in males. In a study by Radisic et al, knowledge has been identified as an important factor in vaccine acceptability.34 Our study supports this view since the HPV knowledge scores were much higher for mothers of male students in the intervention group who were willing to vaccinate their sons than for mothers in the control group.
We found that lack of information about HPV is a significant barrier for HPV vaccination intention and uptake. This is confirmed in the Health Belief Model mentioned in the Radisic study stating that “constructs of perceived benefits, cues to action, and perceived barriers are all related to vaccine acceptability of male vaccination among parents.”34 The research done by Krawcyzk et al has also showed that “these theoretically motivated constructs are very useful for targeting interventions to increase vaccination intention and uptake among a male population.”35
With their approval of vaccinating their sons, most parents thought that it would bring them benefits and believed that the vaccine is safe and that “without the HPV vaccine their son would be at risk of diseases related to HPV.”35
While we explored the attitudes of the mothers of male students before the vaccination becomes widely available, previous studies on the vaccine acceptability among mothers of male students conducted in other countries took place at a time when the vaccine was already widely available for boys. What we found in our study is similar to the findings of Zimet and Rosenthal that almost all studies about parents’ attitudes towards HPV vaccination for their sons conducted before it was widely available reported that a majority of parents endorsed male vaccination.36
This study is similar to the research by Schuler37 who concluded that efforts to improve HPV vaccination intention and uptake in males should bring many benefits for female partners because they can protect HPV infection transmission. When such cancers as anal and head and neck cause suffering to women and men due to HPV, the traditional belief that women are responsible for sexual and reproductive health must be reconsidered.38–40
In 2009, Holman conducted research to explore the barriers to HPV intention and uptake of boys due to the lack of HPV knowledge of the parents.41 Several studies point out the high cost of the HPV vaccine acts as a barrier to HPV vaccine recommendation.42,43
Similarly, A study conducted in Binh Dinh, Vietnam also suggests that high cost is a major barrier to HPV vaccination uptake.18
Some studies in Asian countries, and particularly Vietnam have reported low levels of knowledge about cervical cancer, HPV, and HPV vaccination.44–46 In our study, we found that mothers of male students were more likely interested in HPV vaccination education by doctors and nurses. Most of them were very curious about a male HPV program by their trusted health care providers.
From our perspective, it would be beneficial for boys to be vaccinated against HPV to achieve good health on equal terms for males and females. This is also the general overall aim of global public health. Furthermore, our results highlight the need for an HPV education program.
Limitations of the study
A limitation was that participants were not queried specifically about how much parents could pay for an HPV vaccination if an HPV vaccine would be available for boys, when cost was sometimes identified as a barrier and the vaccine costs for girls are still high, especially when compared to personal incomes in Vietnam.17 HPV vaccination for men also faces some issues from a communication perspective with low levels of public health awareness, lack of proven effectiveness, and stigmatized perceptions of many people regarding the HPV vaccine.17
Strengths of the Study
This is the first study to assess the effectiveness of a health talk education program on HPV knowledge, perception, and vaccination intention among mothers of teenage boys in an Asian country. This study is expected to provide important information to policymakers and health professionals on how important HPV health talk education is, and that HPV vaccination is not only justified for girls, but also for boys. In addition, this study provides insights that could lead to effective strategies in education and health policy which can ultimately lead to better health behaviors and outcomes.
Conclusion
Currently, HPV vaccinations are routinely available to all women in Vietnam, but only to few men on request. Our hope is that our education program can be used more widely to encourage mothers to request the HPV vaccination for their male children as well. We further hope that the findings of our study will encourage the inclusion of HPV vaccinations for males in the Vietnamese National Vaccination Programs.
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. Human papilloma virus vaccines: WHO position paper. Wkly Epidemiol Rec. 2017;92(19):241–268.
2. American Cancer Society. Cancer facts and figures; 2008. Available from: http://www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf.
3. Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev. 2005;14(2):467–475. doi:10.1158/1055-9965.EPI-04-0551
4. Ryan DP, Mayer RJ. Anal carcinoma: histology, staging, epidemiology, treatment. CurrOpinOncol. 2000;12:345–352.
5. Daling JR, Madeleine MM, Johnson LG, et al. Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005;116(4):606–616. doi:10.1002/ijc.21009
6. Parkin DM, Bray F. The burden of HPV-related cancers. Vaccine. 2006;21(24):S11–25. doi:10.1016/j.vaccine.2006.05.111
7. Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015;107(6):djv086. doi:10.1093/jnci/djv086
8. HPV and cancer. HPV-Associated Cancer Diagnosis by Age. Atlanta, GA: CDC; 2017.
9. Viens LJ, Henley SJ, Watson M, et al. Human papillomavirus-associated cancers— United States, 2008–2012. MMWR Morb Mortal Wkly Rep. 2016;65(26):661–666. doi:10.15585/mmwr.mm6526a1
10. Centers for Disease Control and Prevention (CDC). Recommendations on the use of quadrivalent human papillomavirus vaccine in males—advisory committee on immunizations practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60(50):1705–1708.
11. Centers for Disease Control and Prevention (CDC). FDA licensure of quadrivalent human papillomavirus vaccine (HPV4, Gardasil) for use in males and guidance from the advisory committee on immunizations practices (ACIP). MMWR Morb Mortal Wkly Rep. 2010;59(20):630–632.
12. Bruni L, Barrionuevo-Rosas L, Albero G. ICO information centre on HPV and cancer (HPV information centre). Hum Papillomavirus Relat Dis Viet Nam. 2014;202:12–18.
13. NationalInstitute of Hygiene and Epidemiology. Evaluating HPV vaccine delivery strategies in Vietnam. Available from: https://www.path.org/publications/files/CPVietnam_eval_hpv_vacc_deliv.pdf.
14. Bruni L, Barrionuevo-Rosas L, Albero G, et al. Human Papillomavirus and Related Diseases Report; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Barcelona, Spain; 2017.
15. Vu LT, Bui D, Le HT. Prevalence of cervical infection with HPV type 16 and 18 in Vietnam: implications for vaccine campaign. BMC Cancer. 2013;13(1):53. doi:10.1186/1471-2407-13-53
16. Chow SN, Soon R, Park JS, et al. Knowledge, attitudes, and communication around human papillomavirus (HPV) vaccination amongst urban Asian mothers and physicians. Vaccine. 2010;28(22):3809–3817. doi:10.1016/j.vaccine.2010.03.027
17. Tran B, Quoc Than PT, Doan T. Knowledge, attitude, and practice on and willingness to pay for human papillomavirus vaccine: a cross-sectional study in Hanoi, Vietnam. Patient Prefer Adherence. 2018;12:945–954. doi:10.2147/PPA.S165357
18. Nguyen TNT, Phan TL, Ngo VT, Nguyen TTD, Vo HP, Nguyen T. Knowledge and practices of HPV vaccination to prevent cervical cancer among women aged 15–49 in Binh Dinh province, 2017. Vietnam J Prevent Med. 2017;27(8):246.
19. Remschmidt C, Walter D, Schmich P, Wetzstein M, Deleré Y, Wichmann O. Knowledge, attitude, and uptake related to human papillomavirus vaccination among young women in Germany recruited via a social media site. Hum Vacc Immunother. 2014;10(9):2527–2535. doi:10.4161/21645515.2014.970920
20. Rondy M, van Lier A, van de Kassteele J, Rust L, de Melker H. Determinants for HPV vaccine uptake in the Netherlands: a multilevel study. Vaccine. 2010;28(9):2070–2075. doi:10.1016/j.vaccine.2009.12.042
21. Thanh Le XT, Ngoc Nguyen PT, Thanh Do TT. Intention to pay for HPV vaccination among women of childbearing age in Vietnam. Environ Res Public Health. 2020;17(9):3144. doi:10.3390/ijerph17093144
22. Agosti JM, Goldie SJ. Introducing HPV vaccine in developing countries – key challenges and issues. N Engl J Med. 2007;356(19):1908–1910. doi:10.1056/NEJMp078053
23. Rajiah K, Maharajan MK, Chin NS, Num KS. Awareness and acceptance of human papillomavirus vaccination among health sciences students in Malaysia. Virus disease. 2015;26(4):297–303. doi:10.1007/s13337-015-0287-3
24. Al-Nuaimi NS, Al-Ghas YS, Al-Owais AH, et al. Human papillomavirus vaccination uptake and factors related to uptake in a traditional desert city in the United Arab Emirates. Int J STD AIDS. 2011;22(7):400–404. doi:10.1258/ijsa.2009.009380
25. Ritten CJ, Breunig IM. Willingness to pay for programs for the human papillomavirus vaccine on a rocky mountain west college campus. West Econ Forum. 2013;12(1):15.
26. Locke C, NganHoa NT, Thanh Tam NT. Visiting marriages and remote parenting: changing strategies of rural-urban migrants to Hanoi, Vietnam. J Dev Stud. 2012;48(1):10–25. doi:10.1080/00220388.2011.629650
27. LanAnhThi Do LAT, Boonmongkon P, Paek SC, Guadamuz TE. ‘Hu Hong’ (bad thing): parental perceptions of teenagers’ sexuality in urban Vietnam. BMC Public Health. 2017;17(1):226. doi:10.1186/s12889-017-4133-y
28. Chan SS, Cheung TH, Lo WK, Chung TK. Women’s attitudes on human papillomavirus vaccination to their daughters. J Adolesc Health. 2007;41(2):204–207. doi:10.1016/j.jadohealth.2007.04.011
29. Sherman SM, Nailer E, Minshall C, Coombes R, Cooper J, Redman CW. Awareness and knowledge of HPV and cervical cancer in female students: a survey (with a cautionary note). J Obstet Gynaecol. 2016;36(1):76–80. doi:10.3109/01443615.2015.1041886
30. Perez S, Tatar O, Ostini R, et al. Extending and validating a human papilloma virus (HPV) knowledge measure in a national sample of Canadian parents of boys. Preventive medicine. 2016;91:43–49.
31. Waller JO, Ostini R, Marlow LA, McCaffery K, Zimet G. Validation of a measure of knowledge about human papillomavirus (HPV) using item response theory and classical test theory. Prev Med. 2013;56(1):35–40. doi:10.1016/j.ypmed.2012.10.028
32. Fua LY, Bonhommea L-A, Cooperb SC, Joseph JG, Zimetd GD. Educational interventions to increase HPV vaccination acceptance: a systematic review. Vaccine. 2014;32(17):1901–1920. doi:10.1016/j.vaccine.2014.01.091
33. Katz ML, Kam JA, Krieger JL, Roberto AJ. Predicting human papillomavirus vaccine intentions of college- aged males: an examination of parents’ and son’s perceptions. J Am Coll Health. 2012;60(6):449–459. doi:10.1080/07448481.2012.673523
34. Radisic G, Chapman J, Flight I, Wilson C. Factors associated with parents’ attitudes to the HPV vaccination of their adolescent sons: a systematic review. Prev Med. 2017;95:26–37. doi:10.1016/j.ypmed.2016.11.019
35. Krawczyk A, Knäuper B, Gilca V, et al. Parents’ decision-making about the human papillomavirus vaccine for their daughters: I. quantitative results. Hum Vaccin Immunother. 2015;11(2):322–329. doi:10.1080/21645515.2014.1004030
36. Zimet GD, Rosenthal SL. HPV vaccine and males: issues and challenges. Gynecol Oncol. 2010;117(2Suppl):S26–31.
37. Schuler CL, DeSousa NS, Coyne-Beasley T. Parents’ decisions about HPV vaccine for sons: the importance of protecting sons’ future female partners. J Community Health. 2014;39(5):842–848. doi:10.1007/s10900-014-9859-1
38. Du J, Nordfors C, Ahrlund-Richter A, et al. Prevalence of oral human papillomavirus infections among youth, Sweden. Emerg Infect Dis. 2012;18(9):1468–1471. doi:10.3201/eid1809.111731
39. Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Onco1. 2011;29(32):4294–4301. doi:10.1200/JCO.2011.36.4596
40. Machalek DA, Grulich AE, Jin F, et al. The epidemiology and natural history of anal human papillomavirus infection in men who have sex with men. Sex Health. 2012;9(6):527–537. doi:10.1071/SH12043
41. Holman DM, Benard V, Roland KB, Watson M, Liddon N, Stokley S. Barriers to human papillomavirus vaccination among US adolescents: a systematic review of the literature. JAMA Pediatr. 2014;168(1):76–82. doi:10.1001/jamapediatrics.2013.2752
42. Farias AJ, Savas LS, Fernandez ME, et al. Association of physicians perceived barriers with human papillomavirus vaccination initiation. Prev Med. 2017;105:219–225. doi:10.1016/j.ypmed.2017.07.016
43. Wong LP. Issues surrounding HPV vaccine delivery in a multi-ethnic country in Asia: the physician’s perspective. J Community Health. 2011;36(1):14–22. doi:10.1007/s10900-010-9275-0
44. Loi TT, Nhung BTH. Screening cervical cancer of perimenopausal women in Ho Chi Minh City. HCMH J Med. 2004;8:116–119.
45. Dinh TA, Rosenthal SL, Doan ED. Attitudes of mothers in Da Nang, Vietnam toward a human papillomavirus vaccine. J Adolesc Health. 2007;40(6):559–563. doi:10.1016/j.jadohealth.2007.02.003
46. Nghi NQ, LaMontagne DS, Bingham A, et al. Human papillomavirus vaccine introduction in Vietnam: formative research findings. Sex Health. 2010;7(3):262–270. doi:10.1071/SH09123
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.