Back to Journals » International Journal of Women's Health » Volume 18
Effectiveness of a Health Belief Model-Based Educational Intervention on Iron-Folic Acid Supplement Intake Among Pregnant Women in Southern Afghanistan: A Quasi-Experimental Study
Authors Stanikzai MH ![]() , Le CN
, Le CN ![]() , Isaramalai SA
, Isaramalai SA ![]() , Punsawad C
, Punsawad C ![]() , Ezadi Z, Sayam H, Shohaimi S
, Ezadi Z, Sayam H, Shohaimi S ![]() , Dadras O
, Dadras O ![]() , Suwanbamrung C
, Suwanbamrung C ![]()
Received 1 April 2026
Accepted for publication 6 July 2026
Published 10 July 2026 Volume 2026:18 613759
DOI https://doi.org/10.2147/IJWH.S613759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Muhammad Haroon Stanikzai,1– 3 Cua Ngoc Le,1,2 Sang-Arun Isaramalai,4 Chuchard Punsawad,5 Zainab Ezadi,6 Hadia Sayam,7 Shamarina Shohaimi,8 Omid Dadras,9 Charuai Suwanbamrung1,2
1Public Health Research Program, School of Public Health, Walailak University, Tha Sala, Nakhon Si Thammarat, Thailand; 2Excellence Center for Public Health Research (EC-PHR), Walailak University, Tha Sala, Nakhon Si Thammarat, Thailand; 3Department of Public Health, Faculty of Medicine, Kandahar University, Kandahar, Afghanistan; 4Department of Community Health Nursing, Faculty of Nursing, Prince of Songkla University, Hat Yai, Songkla, Thailand; 5Department of Medical Science, School of Medicine, Walailak University, Tha Sala, Nakhon Si Thammarat, Thailand; 6Department of Midwifery, Master of Science in Midwifery, Reproductive Health, Kabul, Afghanistan; 7Department of Para-Clinic, Faculty of Medicine, Malalay University, Kandahar, Afghanistan; 8Department of Biology, Faculty of Science, Universiti Putra Malaysia, Serdang, Selangor, Darul Ehsan, Malaysia; 9Research Centre for Child Psychiatry, University of Turku, Turku, Finland
Correspondence: Charuai Suwanbamrung, Public Health Research Program, School of Public Health, Walailak University, Tha Sala, Nakhon Si Thammarat, 80160, Thailand, Email [email protected]
Background: Research indicates that educational interventions are effective in promoting adherence to iron-folic acid (IFA) supplementation during pregnancy. However, evidence from Afghanistan remains limited. This study aimed to assess the effect of a Health Belief Model (HBM)-based educational intervention on IFA supplement intake and related perceptions among pregnant women in Southern Afghanistan.
Methods: A quasi-experimental study was conducted among 182 pregnant women attending four purposively selected healthcare centers between 10 December 2025 and 10 March 2026. Participants were non-randomly assigned to the intervention (n = 91) or the control (n = 91) group. The intervention consisted of HBM-based educational sessions, while the control group received routine antenatal care. Outcomes included self-reported weekly IFA supplement intake, HBM construct scores, and hemoglobin level, measured at baseline and post-intervention. Data were analyzed using chi-square tests, t-tests, and Generalized Estimating Equations (GEE).
Results: After follow-up, 177 participants (intervention=89; control=88) were included in the analysis. The intervention was associated with a significant increase in weekly IFA supplement intake (β = 1.93, p < 0.001). Significant improvements were also observed in perceived benefits (β = 5.37), susceptibility (β = 3.16), severity (β = 2.18), self-efficacy (β = 3.61), and cues to action (β = 2.58) (all p < 0.001), while perceived barriers decreased significantly (β = − 5.99, p < 0.001). On the other hand, the intervention effect on hemoglobin levels was not statistically significant, but the mean hemoglobin concentration (g/dl) in the intervention group (11.23 ± 1.04) was higher than in the control group (10.88 ± 1.20).
Conclusion: The HBM-based educational intervention was associated with improved IFA supplement intake and favorable changes in health beliefs among pregnant women in Southern Afghanistan. These findings support the potential value of theory-driven educational interventions to promote maternal nutrition behaviors in low-resource settings.
Keywords: iron-folic acid supplementation, IFA, educational intervention, health-belief model, HBM, Afghanistan
Introduction
Iron deficiency is the most prevalent nutritional deficiency worldwide and the leading cause of anemia in pregnant women.1 During pregnancy, increased physiological demands for iron and other micronutrients place women at heightened risk of deficiency, making iron–folic acid (IFA) supplementation a critical intervention for the prevention and management of anemia.2 Despite global efforts, anemia continues to affect a substantial proportion of women of reproductive age, particularly in low- and middle-income countries (LMICs).3,4 In 2021, the prevalence of anemia among women of reproductive age was highest in sub-Saharan Africa and South Asia, reaching 47.4% in western sub-Saharan Africa and 35.7% in South Asia.4 Globally, an estimated 36.5% of pregnant women were anemic in 2019.3
Anemia in pregnant women is linked to poor birth outcomes, including low birth weight and preterm delivery, as well as increased maternal complications such as inadequate weight gain, placental issues, and a higher risk of maternal mortality.5–7 Additionally, it poses significant health risks for newborns, leading to premature birth, growth restrictions, and anemia, ultimately affecting cognitive development and productivity in adults.8 Anemia during pregnancy also plays a role in perpetuating cycles of inadequate growth and cognitive difficulties across generations in populations.1
To mitigate the effects of anemia, the World Health Organization (WHO) advises the adaptation of daily or intermittent oral IFA supplementation,9 and the promotion of essential nutrition actions.10 This should be complemented by multisectoral collaboration to implement both nutrition-sensitive and specific interventions, including health education. Such a holistic strategy is particularly suitable for LMICs in order to achieve the United Nations (UN) Sustainable Development Goals (SDGs) and global nutrition targets.11
Afghanistan faces a complex nutritional landscape shaped by decades of conflict, economic instability, food insecurity, and limitations in health service delivery. Evidence suggests that structural and policy-level factors, including poverty, gender inequality, limited access to education, and weaknesses in health and nutrition systems, contribute substantially to the high burden of malnutrition among Afghan women.12,13 These challenges increase women’s vulnerability to micronutrient deficiencies, particularly during pregnancy.
Although IFA supplementation programs are implemented in many countries, including Afghanistan, adherence to IFA supplementation during pregnancy remains suboptimal in several LMICs.14 According to the Afghanistan Health Survey 2018 (AHS 2018), 46.8% of women received IFA supplement during their most recent pregnancy.15 Evidence from southern Afghanistan identified multiple barriers to IFA adherence among pregnant women, including inadequate knowledge about anemia and IFA supplementation, fear of side effects, forgetfulness, inconsistent counseling, family influences, and challenges related to access to health services.16 These findings indicate that behavioral and informational barriers continue to impede optimal IFA utilization despite the availability of supplementation programs.
Nutrition education and counseling are commonly employed strategies to enhance maternal nutritional health during pregnancy.17 Research indicates that health education interventions are effective in increasing awareness about anemia and promoting adherence to IFA supplementation during pregnancy.18,19 Community-based programs in countries such as Cambodia, Vietnam, and Kenya have demonstrated improvements in knowledge and IFA-related practices.20,21 Furthermore, systematic reviews indicate that educational interventions are effective in promoting adherence to IFA supplementation in resource-limited settings.22
The health belief model (HBM) is a theoretical framework that examines how individual perceptions can influence health-related decision-making and behaviors. According to Rosenstock, the HBM includes several perceptual components, including perceived susceptibility, severity, cues to action, benefits, barriers, and self-efficacy. The model suggests that individuals who perceive themselves as vulnerable to a disease and recognize the seriousness of its consequences are more likely to adopt preventive health behaviors.23–26 In Afghanistan, these behavioral determinants are particularly relevant, as women’s limited knowledge and misconceptions about anemia and IFA use directly affect adherence.16,27 HBM-based interventions can therefore address these barriers by improving risk perception, reinforcing benefits, reducing perceived barriers, and strengthening self-efficacy through targeted education and counseling.
Access to antenatal care (ANC) services represents another important determinant of maternal health behaviors in Afghanistan.28 Recent studies from Kandahar province reported suboptimal utilization of ANC services and identified factors such as maternal education, socioeconomic status, awareness of pregnancy-related health issues, and accessibility of healthcare services as important determinants of ANC attendance.29,30 Because ANC visits provide a major platform for delivering nutrition education and IFA supplement, delayed initiation or inadequate utilization of ANC services may further reduce opportunities for promoting adherence to IFA supplementation.
Despite evidence on barriers to IFA use and ANC utilization in Afghanistan, research evaluating theory-based interventions remains limited. In particular, no published study has assessed an HBM-based educational intervention to improve IFA supplementation among pregnant women in southern Afghanistan. Existing studies have mainly focused on describing barriers rather than testing behavioral interventions.16,28 Therefore, this study aimed to evaluate the effect of an HBM-based educational intervention on IFA supplement intake and perceptions toward IFA supplements among pregnant women in southern Afghanistan.
Methods
Study Design and Settings
In this quasi-experimental study, we assessed the effectiveness of an HBM-based educational intervention on IFA supplement intake, perceptions related to IFA supplements, and hemoglobin level among pregnant women in Kandahar, Southern Afghanistan. The study was conducted from 10 December 2025 to 10 March 2026 at four purposively selected comprehensive healthcare centers (CHCs) in Kandahar, Southern Afghanistan. The CHCs provide free services in maternal and child health, communicable disease control, and other primary healthcare for the populations in their catchment areas. Moreover, all pregnant women are provided with free IFA supplements during their ANC visits at these health facilities. The selected CHCs represented both urban and rural populations and were chosen to ensure comparable levels of healthcare services, staffing, and implementation of ANC programs.
Study Population and Eligibility Criteria
The study population consisted of all pregnant women attending ANC services at pre-designated study sites. Eligibility criteria included being at least 18 years of age, below 16 weeks in their pregnancy gestation, and having received IFA supplements within 1 week prior to inclusion in the study. Women who were severely ill, experiencing acute mental distress, or unwilling to provide informed consent were excluded.
Sample Size and Sampling Procedures
The required sample size was computed using the formula for a two-group mean comparison,19,21,31 with the mean IFA supplement intake as the primary outcome. We assumed 1.5 tablets mean difference in IFA supplement intake between the two groups, with the standard deviation (SD) was assumed to be 2.75 in both groups.18 After adjusting for 10% non-response rate and 30% lost to follow-up, the final sample size was 182 (intervention=91; control=91) at 5% of significance level and 80% power. Taking these considerations into account, the sample size calculation was done using EPI-INFO Version 7.2.
Participants were recruited consecutively at each study site by trained data collectors after obtaining informed consent. All recruited participants were in the first trimester of their pregnancy. Baseline data were collected using a structured questionnaire. Following baseline assessment, participants were non-randomly assigned to either the intervention or control group based on study site (two CHCs served as the intervention sites and the other two as the control sites) to minimize contamination between groups. Endline data were collected one week after completion of the intervention (Figure 1).
 |
Figure 1 Flow diagram of participant enrollment, allocation, follow-up, and analysis. Notes: A total of 182 pregnant women were assessed for eligibility. After allocation was done non-randomly and by facility type, 91 participants were assigned to each group. During follow-up, 2 participants in the intervention group and 3 in the control group were lost. Final analysis included 89 and 88 participants in the intervention and control groups, respectively. |
Intervention
Development of Educational intervention
The health education intervention was conceptually grounded in the HBM model to enhance IFA supplement intake, foster a proactive and healthy behavior toward IFA supplement intake, and address common barriers and misconceptions surrounding IFA supplementation.16
The educational intervention was developed by a multidisciplinary team comprising the principal investigator, public health experts, senior midwives and nurses, and specialists in experimental studies. To ensure cultural relevance, the educational content was tailored by integrating local norms and practices. As shown in Table 1, the educational contents incorporated constructs such as perceived benefits, susceptibility, severity, self-efficacy, cues to action, and barriers to tailor intervention to the cultural context of Afghanistan.16 After the development phase, the educational materials were translated from English into Pashto (the national language) by bilingual public health translators. Prior to the study, the educational materials were pilot-tested among pregnant women at Kandahar Teaching Hospital to ensure their clarity and understandability. Feedback from the pilot testing was used to refine and finalize the educational materials.
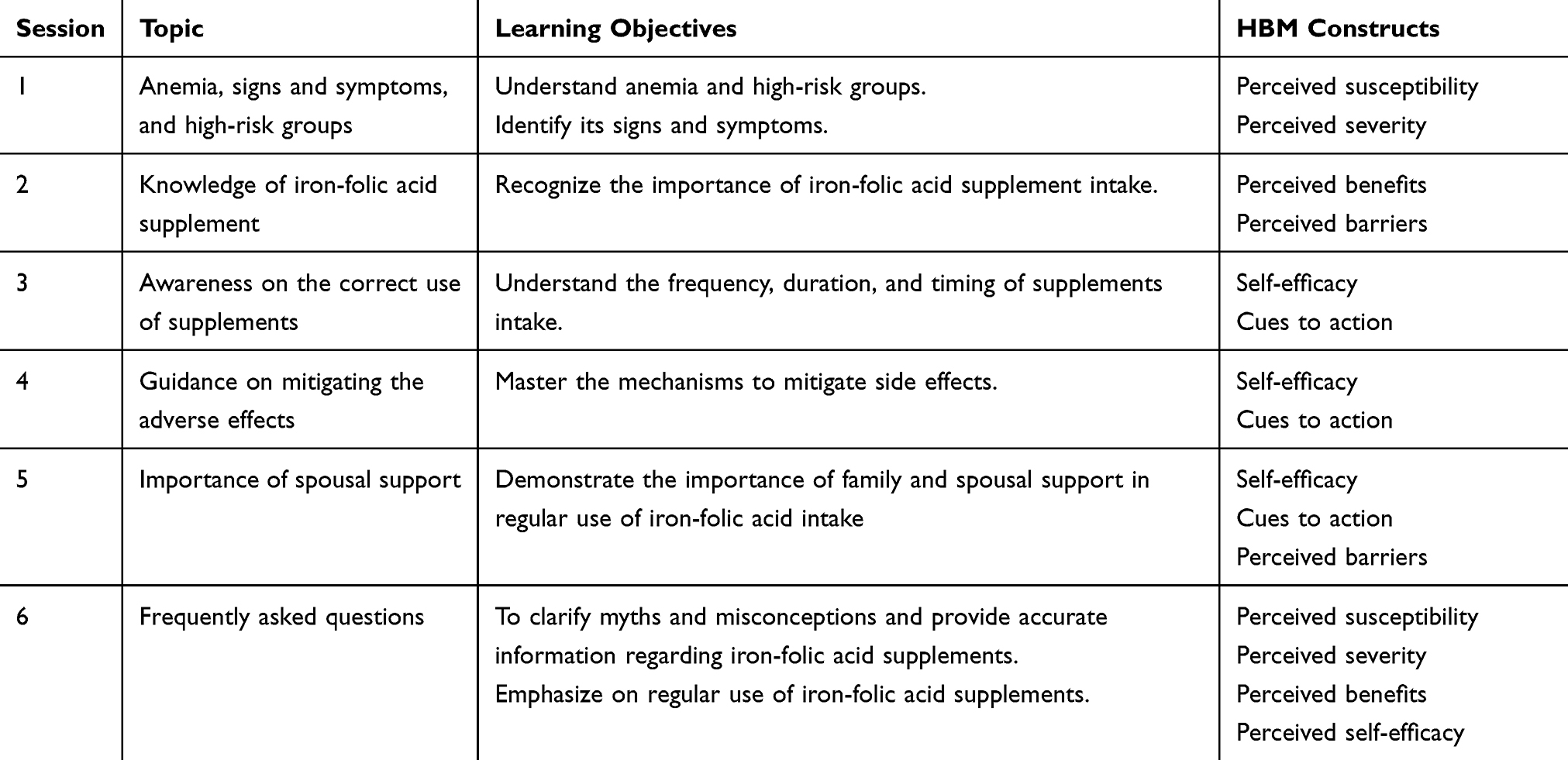 |
Table 1 Outline of the Educational Contents |
Delivery of the Intervention
The intervention was delivered by six qualified midwives as co-facilitators. Prior to the delivery of the intervention, the co-facilitators underwent rigorous training. The program, which lasted three months and included six sessions (pregnant women=5; spouses=1). The educational sessions were delivered face-to-face in a private setting in the health facility every 10 days. Sessions were delivered in a group format with an average of 10 participants per group (9 groups were set up).The intervention modules consisted of educational presentations, distribution of educational brochures, and interactive segments (question-and-answer session). Each session lasted 30 to 45 minutes.
To ensure intervention fidelity, all educational sessions were delivered by trained midwives who received standardized training before the intervention commenced. A structured intervention manual and standardized teaching materials were used to maintain consistency across facilitators. Attendance was recorded at each session, and the principal investigator regularly monitored session delivery through periodic supervision.
Control Group
We thoroughly informed participants in the control group about the study and their assignment. Participants in this group received routine ANC services from the health facilities.
Study Outcomes
Primary Outcomes
- Weekly IFA supplement intake: This primary outcome measures the number of IFA tablets pregnant women have taken in the past week. This is a proxy measure for the WHO recommendations of at least taking 90 IFA tablets during pregnancy and remains consistent with updated studies.26,32,33
- Perception toward IFA supplements: This outcome measured six perceptions using a 5-point Likert scale adopted from previous studies: benefits (5 statements), susceptibility (3 statements), severity (5 statements), self-efficacy (5 statements), cues to action (4 statements), and barriers (5 statements). The scores for each statement ranged from 1 (strongly disagree) to 5 (strongly agree). A higher score represented a higher perception. The statements were extracted from relevant literature and were validated by three experts.16,26,31,34–36
Secondary Outcomes
- Compliance with IFA supplementation: Pregnant women were classified as having good compliance if they consumed at least four IFA tablets in the past week, and as having poor compliance otherwise. This definition of compliance is aligned with most studies in LMICs.26,32,33,37
- Hemoglobin level: Hemoglobin level was measured using a portable device (Acon Mission Plus HB meter). Capillary blood samples were obtained by midwives using a sterile finger-prick technique following standard infection prevention procedures. The device was calibrated prior to usage.
Data Analysis
All analyses were carried out in Stata 18 (StataCorp, College Station, TX).38 Descriptive statistics were used to examine the distribution of baseline characteristics of pregnant women. The chi-square test was used to assess differences in the characteristics of pregnant women between the intervention and control groups. To compare mean changes in weekly IFA supplement intake, perception, and hemoglobin level, an independent t-test was used, and a paired t-test assessed changes within each group at baseline and endline. Generalized Estimating Equations (GEE) were used to examine the effect of intervention on repeated outcome measures while accounting for within-subject correlation over time. The model included group (0 = control, 1 = intervention), time (0 = baseline, 1 = post-intervention), and the group × time interaction. The model was adjusted for potential confounders, including age, residence, education level, parity, employment, and income). Robust standard errors were adjusted for clustering at the facility level. A two-sided p-value of <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 177 pregnant women were included in the final analysis (intervention: n = 89; control: n = 88). The sociodemographic characteristics of participants are presented in Table 2. There were no significant differences between pregnant women in the intervention and control groups in terms of age, women’s and husband’s educational level, residence, employment status, parity, and household monthly income. For instance, 7.9% of women in the intervention group had secondary or higher education compared with 9.1% in the control group.
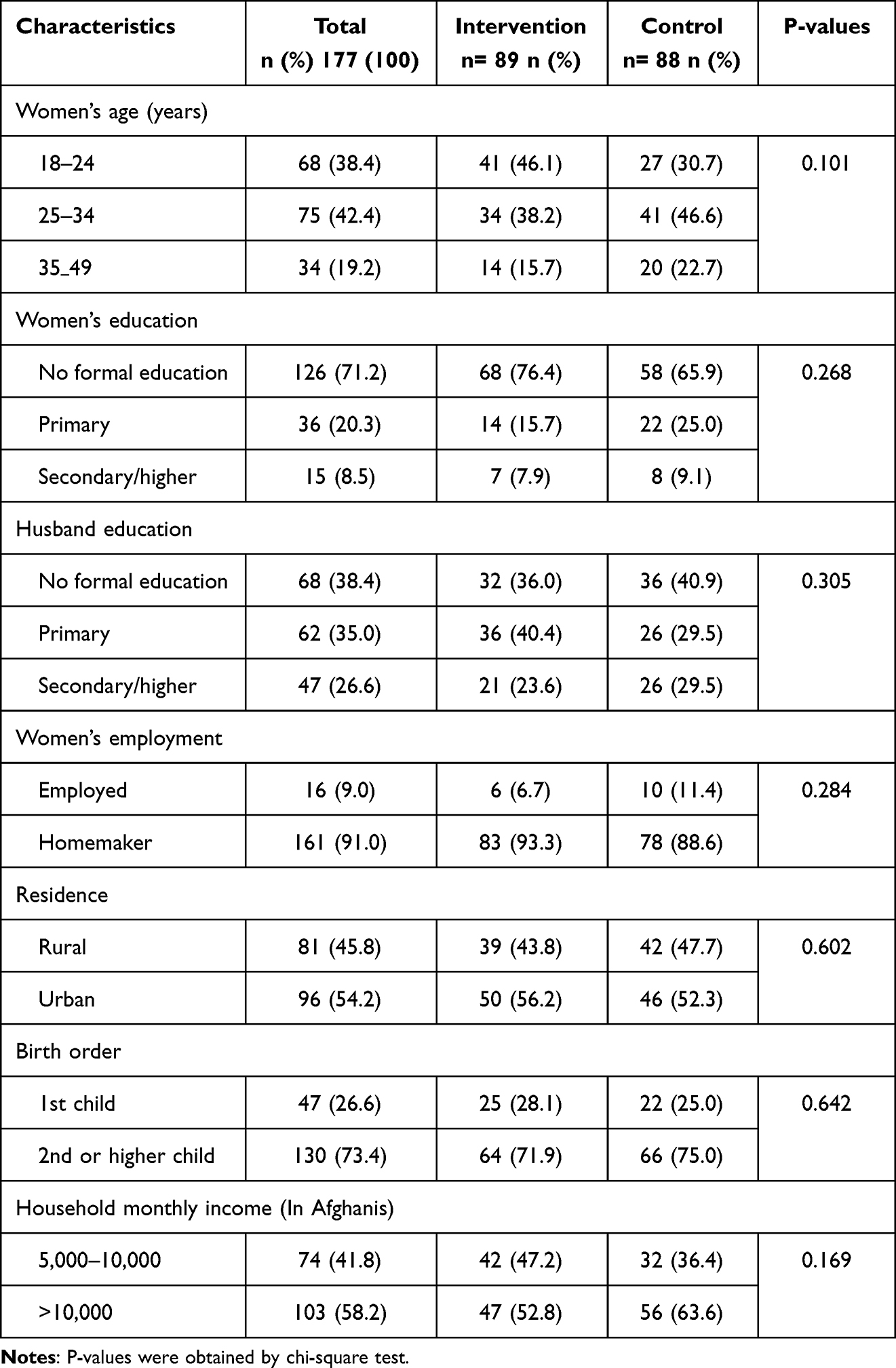 |
Table 2 Baseline Characteristics of Pregnant Women Across Intervention and Comparison Groups |
Changes in Weekly IFA Supplement Intake and HBM Perception Scores
As shown in Table 3, the average weekly intake of IFA supplement significantly increased in the intervention group compared with the control group following the intervention (p < 0.001). Perception scores for HBM constructs including benefits, severity, susceptibility, efficacy, barriers, and cues to action; also showed significant improvement post-intervention (p<0.001). Specifically, scores for benefits, severity, susceptibility, efficacy, and cues to action significantly increased in the intervention group (p < 0.001). In contrast, the scores for barriers significantly decreased in the intervention group (p < 0.001) (details in Table 3).
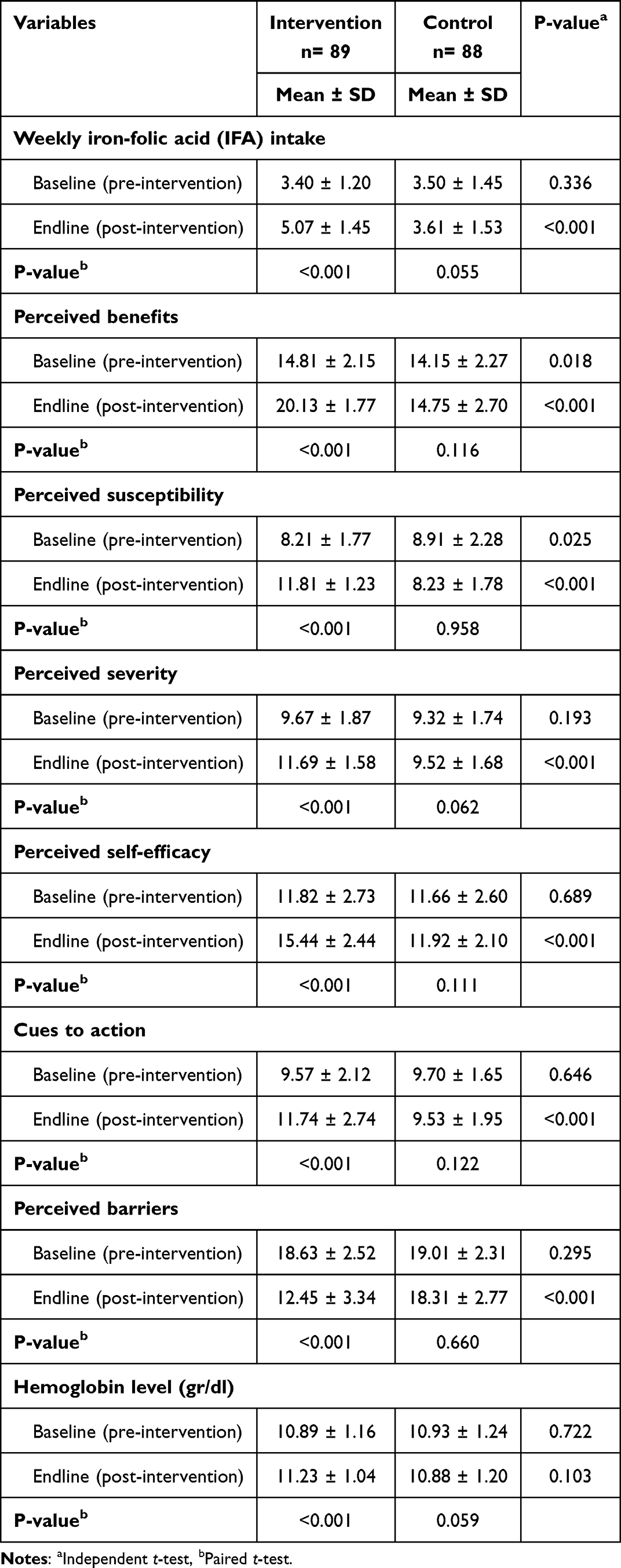 |
Table 3 Changes Over Time Between and Within Intervention and Control Groups on Weekly Iron-Folic Acid (IFA) Supplement Intake, Scores of Health-Belief Model (HBM) Constructs, and Hemoglobin Level |
At baseline, weekly IFA intake and most HBM construct scores were comparable between groups. However, perceived benefits and perceived susceptibility differed significantly at baseline (p = 0.018 and p = 0.025, respectively), and these imbalances were considered when interpreting the group-by-time estimates.
Effect of Educational Intervention on Weekly IFA Supplement Intake and Perception
The results of the Generalized Estimating Equations (GEE) analysis are presented in Table 4. After adjusting for age, residence, education, parity, employment, and household income, the group × time interaction term indicated that the intervention was associated with a significant increase in weekly IFA supplement intake compared with the control group (β = 1.93, p < 0.001).
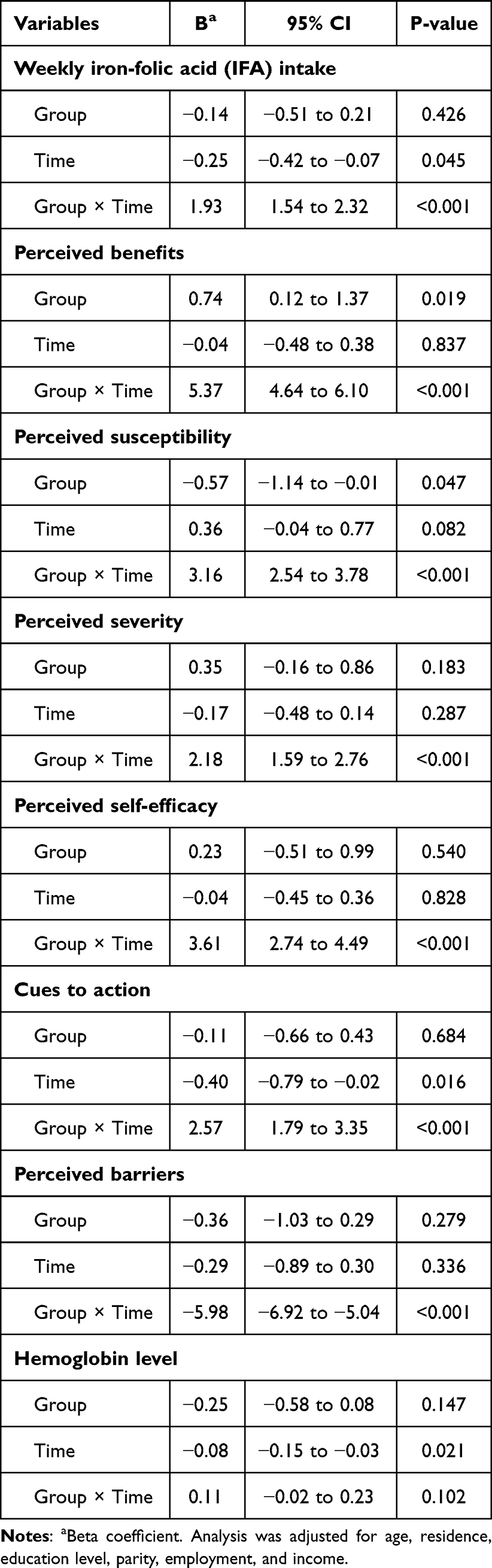 |
Table 4 Changes Over Time Between and Within the Intervention and Control Groups Using Generalized Estimating Equations (GEE) |
Significant intervention effects were also observed across all HBM constructs. Compared with the control group, the intervention group showed greater increases in perceived benefits (β = 5.37), susceptibility (β = 3.16), severity (β = 2.18), self-efficacy (β = 3.61), and cues to action (β = 2.58), along with a significant reduction in perceived barriers (β = −5.99) (all p < 0.001).
Compliance and Hemoglobin Levels in Intervention and Control Groups Following the Intervention
As shown in Figure 2, there was no significant difference in compliance levels between the intervention and control groups at baseline (48.3% vs. 47.6%, P=0.623). However, post-intervention, the intervention group reported markedly higher compliance levels compared to control group (71.9% vs. 50.3%, P= < 0.001).
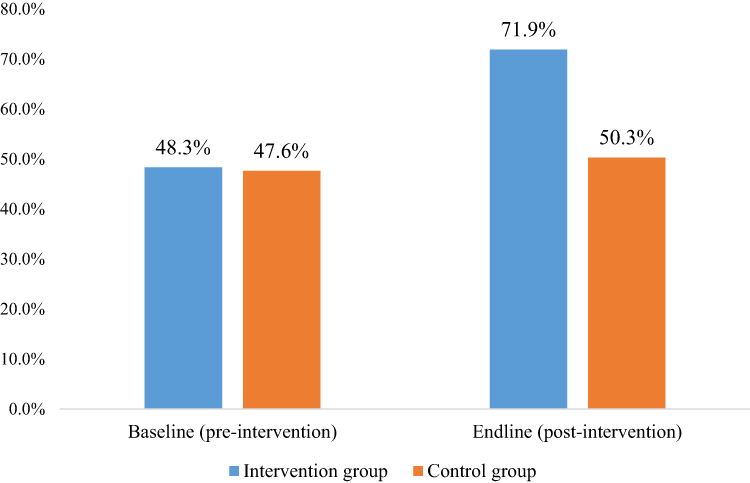 |
Figure 2 Iron-folic acid compliance levels at baseline and endline for intervention and control groups. |
The intervention effect on hemoglobin levels was not statistically significant (Table 4). However, the mean hemoglobin concentration (g/dl) in the intervention group (11.23 ± 1.04) was higher than in the control group (10.88 ± 1.20) (details in Table 3).
Discussion
This study examined the effects of an HBM-based educational intervention on IFA supplement intake, perceptions related to IFA supplements, and hemoglobin level among pregnant women in Southern Afghanistan. The findings indicate that the intervention was associated with a significant increase in weekly IFA supplement intake, along with improvements in multiple HBM constructs, including perceived benefits, susceptibility, severity, self-efficacy, and cues to action, and a reduction in perceived barriers. However, the hemoglobin level increased in the intervention group compared to the control group, but the effect was not statistically significant.
These findings are consistent with evidence from LMICs demonstrating the value of HBM-based educational interventions in promoting health-related behaviors.34,36 In this study, women in the intervention group reported higher weekly IFA supplement intake and greater compliance compared with those in the control group. The observed group-by-time interaction further supports the association between the intervention and improved outcomes. These results are in line with previous studies indicating that theory-based educational interventions can enhance knowledge and influence behavioral determinants, thereby supporting positive changes in health practices.31,35
The improvements observed in IFA supplement intake may be partly explained by changes in health beliefs targeted by the intervention. The HBM framework emphasizes the role of perceived susceptibility, severity, benefits, and barriers in shaping behavior, as well as the importance of self-efficacy and cues to action. The intervention addressed these constructs through interactive sessions, reinforcement, and engagement of spouses, which may have contributed to increased motivation and adherence. However, as this study did not formally assess mediation pathways, these mechanisms should be interpreted with caution. In contrast, the control group, which received routine ANC, showed relatively smaller changes in IFA supplement intake and compliance. While this may suggest limitations in the effectiveness of standard ANC counselling in this setting, the study did not directly assess the quality or content of ANC services. Therefore, these findings should be interpreted cautiously. Nonetheless, previous studies in Afghanistan have reported gaps in the quality of ANC services,39,40 which may contribute to suboptimal adherence to recommended maternal health practices. Overall, these findings suggest that theory-driven educational interventions may offer a promising approach to improving IFA supplementation behaviors among pregnant women in resource-constrained settings. Further research is needed to evaluate the effectiveness and scalability of such interventions across diverse populations and settings within Afghanistan.
An important contribution of this study is the examination of changes in health beliefs related to IFA supplementation. Following the intervention, perceived benefits increased significantly in the intervention group compared with the control group. This may be attributed to the educational content emphasizing the role of IFA supplementation in improving maternal and neonatal health outcomes, including prevention of anemia and support for safe pregnancy and childbirth. These findings are consistent with previous studies in LMICs demonstrating that HBM-based educational interventions can enhance awareness of the benefits of recommended health behaviors and support improved adherence.31,36
In addition, the intervention group demonstrated significantly higher perceived susceptibility and severity related to inadequate IFA supplementation compared with the control group. The educational sessions highlighted the risks and potential consequences of non-adherence, which may have contributed to increased awareness among participants. Prior research suggests that individuals who perceive greater susceptibility to health risks and recognize the seriousness of potential outcomes are more likely to adopt preventive behaviors, including adherence to supplementation.25,41 These findings underscore the importance of addressing risk perception as part of strategies to improve IFA supplementation practices.
The intervention was also associated with a significant improvement in perceived self-efficacy related to IFA supplementation in the intervention group compared with the control group. This may be attributed to the program’s emphasis on practical guidance, including strategies to manage common side effects and maintain regular supplement use.16 These findings are consistent with previous studies showing that educational interventions can enhance women’s confidence in managing their health during pregnancy and support improved utilization of maternal health services in LMICs.36,42 Strengthening self-efficacy may therefore be an important pathway through which educational interventions influence adherence to IFA supplementation.
Similarly, cues toward IFA supplement intake were significantly greater among pregnant women in the intervention group than in the control group. Research has shown that recommendations from healthcare workers and other experts involved in the educational sessions are important for enhancing cues to action.31 Additionally, involving spouses in one of the education sessions may have provided additional support and positive reinforcement, thereby strengthening cues to action for consistent IFA intake. While these findings suggest that incorporating multiple sources of cues may enhance adherence, further research is needed to better understand the relative contribution of different types of cues in promoting sustained supplementation behavior.
Pregnant women in LMICs often face multiple barriers to accessing and utilizing maternal healthcare services, including challenges related to knowledge, social norms, and health system constraints.43,44 Research has demonstrated that reproductive health interventions can effectively reduce these barriers and improve service uptake.45 In the current study, perceived barriers to IFA supplement adherence were significantly lower in the intervention group than in the control group. In justifying this finding, the educational intervention included efforts to identify obstacles to regular intake of IFA supplements among participants and allowed the team to discuss strategies to remove these barriers.16 This finding is consistent with earlier quasi-experimental evidence showing that educational interventions can reduce perceived barriers and improve adherence to recommended maternal health behaviors.36 There is also evidence that higher perceived barriers is a key predictor of poor compliance with IFA supplementation.14 While the findings suggest that targeted education may help reduce perceived barriers, further research is needed to better understand the broader structural, cultural, and contextual factors influencing adherence in this setting. In particular, qualitative studies could provide deeper insights into women’s experiences and inform the development of more contextually appropriate and acceptable interventions to promote sustained IFA supplementation in Afghanistan.
Although hemoglobin levels increased in the intervention group compared with the control group, the difference was not statistically significant. To elaborate on this finding, the following points may be worth considering. During the second trimester, plasma volume increases more than red blood cell volume, leading to physiological hemodilution and a lower hemoglobin level, even as iron status improves.46 Moreover, in women with low iron stores, the body may initially use the supplemented iron to replenish its reserves, resulting in a delayed increase in hemoglobin that may not be immediately observed.47
Limitations
Our study has some limitations. First, due to the quasi-experimental design and non-random allocation of participants, the findings may be subject to selection bias and residual confounding. Therefore, causal inferences should be made with caution, and further evaluation through randomized controlled trials is warranted. Second, data on IFA supplement intake and perceptions regarding IFA supplements were self-reported; therefore, they may be subject to information and social desirability biases. In addition, no objective measures (eg., pill counts) were used to validate self-reported intake. Third, the intervention was implemented at the facility level, and differences between study sites may have influenced the observed outcomes, limiting the ability to fully attribute effects to the intervention alone. Fourth, additional strategies such as community-based distribution, home visits, or mobile-based text messaging; which were not assessed in this study, could also influence IFA supplement intake and adherence. Therefore, future research should consider these interventional approaches. Fifth, although the intervention and control groups were comparable with respect to baseline demographic characteristics, differences were observed in baseline levels of perceived benefits and perceived susceptibility. These baseline imbalances may have introduced bias; however, their potential influence was minimized by adjusting for repeated measures and relevant covariates in the GEE analysis. Sixth, the duration of follow-up was relatively short, and the study did not assess the sustainability of behavioral changes over time or adherence throughout the full course of pregnancy. Lastly, the study was conducted in selected health facilities in Kandahar, Southern Afghanistan. Although sites were purposively selected to reflect contextual variation, findings may not be generalizable to other regions with different sociocultural, economic, or security contexts.
Despite these limitations, this study provides important evidence on the potential role of theory-based educational interventions in improving IFA supplementation behaviors in a fragile and resource-constrained setting.
Conclusion
This study found that an HBM-based educational intervention was associated with improved IFA supplement intake and compliance among pregnant women in Southern Afghanistan. The intervention was also associated with favorable changes in health beliefs, including increased perceived benefits, susceptibility, severity, self-efficacy, and cues to action, alongside reduced perceived barriers. These findings suggest that theory-driven educational approaches may be a promising strategy for improving maternal nutrition behaviors in resource-constrained and fragile settings. However, given the quasi-experimental design and short follow-up period, further research, particularly randomized controlled trials and longer-term studies, is needed to confirm effectiveness, assess sustainability, and evaluate scalability across diverse contexts within Afghanistan.
Data Sharing Statement
The primary data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The study was ethically approved by Human Research Ethics Committee at Walailak University (WUEC-25-371-01) and Department of Public Health, Faculty of Medicine, Kandahar University (PHMFKDRU-112-10-11-2025). Prior to participants’ recruitment into the study, we obtained informed consent from all participants. Participation was voluntary and had the right to withdraw at any time, for any reason. Moreover, the study was conducted in accordance with local ethical guidelines and in compliance with the Declaration of Helsinki.
Funding
This research work was financially supported by Walailak University Graduate Research Fund (No. CGS-RF-2024-17).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jouanne M, Oddoux S, Noël A, Voisin-Chiret AS. Nutrient requirements during pregnancy and lactation. Nutrients. 2021;13(2):692. doi:10.3390/nu13020692
2. World Health Organization. Nutritional anaemias: tools for effective prevention and control. Available from: https://www.who.int/publications/i/item/9789241513067.
3. World Health Organization. Anaemia in women and children: WHO Global Anaemia Estimates, 2021. 2023. Available from: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children.
4. Gardner WM, Razo C, McHugh TA, et al. Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990-2021: findings from the global burden of disease study 2021. Lancet Haematol. 2023;10(9):e713–14. doi:10.1016/S2352-3026(23)00160-6
5. Benson CS, Shah A, Stanworth SJ, et al. The effect of iron deficiency and anaemia on women’s health. Anaesthesia. 2021;76:84–95. doi:10.1111/anae.15405
6. Parks S, Hoffman M, Goudar S, et al. Maternal anaemia and maternal, fetal, and neonatal outcomes in a prospective cohort study in India and Pakistan. BJOG. 2019;126(6):737–743. doi:10.1111/1471-0528.15585
7. Hasan MM, Soares Magalhaes RJ, Garnett SP, et al. Anaemia in women of reproductive age in low- and middle-income countries: progress towards the 2025 global nutrition target. Bulletin of the World Health Organization. 2022;100(3):196–204. doi:10.2471/blt.20.280180
8. Wang X, Jing J, Huang S, et al. Relationship of early anemia with neurodevelopment and brain injury in very low birth weight preterm infants-a prospective cohort study. Nutrients. 2022;14(22):4931. doi:10.3390/nu14224931
9. World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience – highlights and Key Messages. Available from: https://www.who.int/publications/i/item/WHO-RHR-18.02.
10. World Health Organization. Essential nutrition actions: improving maternal, newborn, infant and young child health and nutrition. 2013. Available from: https://apps.who.int/iris/bitstream/handle/10665/84409/9789241505550_eng.pdf.
11. World Health Organization. Global Nutrition Targets 2025: policy Brief Series.
12. Stanikzai MH, Dadras O. Advancing breastfeeding research in Afghanistan: opportunities for policy and practice. Int. Breastfeed. J. 2025;20(1):68. doi:10.1186/s13006-025-00763-z
13. Fayez SM. Policy and structural drivers of malnutrition in afghan women: evidence and interventions. Int J Womens Health. 2026;18:604409. doi:10.2147/ijwh.S604409
14. Siekmans K, Roche M, Kung’u JK, Desrochers RE, De-Regil LM. Barriers and enablers for iron folic acid (IFA) supplementation in pregnant women. Maternal and Child Nutrition. 2018;14:e12532. doi:10.1111/mcn.12532
15. Afghanistan health survey. 2018. Available from: https://www.kit.nl/wp-content/uploads/2019/07/AHS-2018-report-FINAL-15-4-2019.pdf.
16. Stanikzai MH, Le CN, Isaramalai SA, et al. Barriers and facilitators of compliance with iron-folic acid supplementation among pregnant women in southern afghanistan: a qualitative study. Patient Prefer Adherence. 2026;20:606199. doi:10.2147/ppa.S606199
17. Engidaw MT, Lee P, Fekadu G, Mondal P, Ahmed F. Effect of nutrition education during pregnancy on iron-folic acid supplementation compliance and anemia in low- and middle-income countries: a systematic review and meta-analysis. Nutr Rev. 2025;83(7):e1472–e1487. doi:10.1093/nutrit/nuae170
18. Berhane A, TJJons B. Effect of Picture-based health education and counselling on knowledge and adherence to preconception Iron-folic acid supplementation among women planning to be pregnant in Eastern Ethiopia: a randomized controlled trial. J Nutr Sci. 2022;11e58. doi:10.1017/jns.2022.51
19. Abdisa DK, Jaleta DD, Tsegaye D, et al. Effect of community based nutritional education on knowledge, attitude and compliance to IFA supplementation among pregnant women in rural areas of southwest Ethiopia: a quasi experimental study. BMC Public Health. 2023;23(1):1923. doi:10.1186/s12889-023-16798-y
20. Kavle JA, Landry M. Community-based distribution of iron–folic acid supplementation in low-and middle-income countries: a review of evidence and programme implications. Public Health Nutr. 2018;21(2):346–354. doi:10.1017/S1368980017002828
21. Kamau M, Mirie W, Kimani S, IJPo M. Effect of community based health education on knowledge and attitude towards iron and folic acid supplementation among pregnant women in Kiambu County, Kenya: a quasi experimental study. PLoS One. 2019;14(11):e0224361. doi:10.1371/journal.pone.0224361
22. Girard AW, Olude OJP, Epidemiology p. Nutrition education and counselling provided during pregnancy: effects on maternal, neonatal and child health outcomes. Paediatr Perinat Epidemiol. 2012;26(Suppl 1):191–204. doi:10.1111/j.1365-3016.2012.01278.x
23. Khawwas HSM, El-Guindi FK, Farahat NH, Mohamed AT. Applying health belief model among mothers of children with thalassemia. Sci Rep. 2025;15(1):31219. doi:10.1038/s41598-025-15584-7
24. Alyafei A, Easton-Carr R.The health belief model of behavior change.StatPearls. Treasure Island (FL);StatPearls Publishing.
25. Yassin MA, Kumma WP, Haile DT, Elilo LT. Compliance to iron folic acid consumption and factors associated among antenatal care attendant mothers in southern Ethiopia. Sci Rep. 2024;14(1):27351. doi:10.1038/s41598-024-79066-y
26. Mekonnen A, Alemnew W, Abebe Z, Demissie GD. Adherence to iron with folic acid supplementation among pregnant women attending antenatal care in public health centers in simada district. Northwest Ethiopia. 2021;15:843–851. doi:10.2147/ppa.S299294
27. Anwary Z, Stanikzai MH, Wyar WM, Wasiq AW, Farooqi K. Anemia among women who visit Bost Hospital for delivery in Helmand Province, Afghanistan. Anemia. 2021;2021(1):9358464. doi:10.1155/2021/9358464
28. Naseri S, Durand MA, Arifi F, et al. Antenatal care interventions in Afghanistan from 2000 to 2024: a rapid realist review. BMJ Open. 2025;15(11):e102454. doi:10.1136/bmjopen-2025-102454
29. Samiah S, Stanikzai MH, Wasiq AW, Sayam H. Factors associated with late antenatal care initiation among pregnant women attending a comprehensive healthcare facility in Kandahar Province, Afghanistan. Indian J Public Health. 2021;65(3):298–301. doi:10.4103/ijph.IJPH_62_21
30. Stanikzai MH, Wafa MH, Wasiq AW, Sayam H. Magnitude and Determinants of Antenatal Care Utilization in Kandahar City, Afghanistan. Obstet Gynecol Int. 2021;2021:5201682. doi:10.1155/2021/5201682
31. Khani Jeihooni A, Razmjouie F, Jormand H, et al. Effectiveness of educational intervention in improving physical activity and nutritional performance among pregnant women: a pre-post quasi-experimental study using health belief model. Front Glob Womens Health. 2024;5:1471957. doi:10.3389/fgwh.2024.1471957
32. Fite MB, Roba KT, Oljira L, Tura AK, Yadeta TA. Compliance with Iron and Folic Acid Supplementation (IFAS) and associated factors among pregnant women in Sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. 2021;16(4):e0249789. doi:10.1371/journal.pone.0249789
33. Taye M, Mohammed T, Taye W, Glagn M, Yihune M. Compliance with iron-folate supplementation among pregnant women in Southern Ethiopia: a multi-center cross-sectional study. Reproductive Health. 2025;22(1):22. doi:10.1186/s12978-025-01944-z
34. Abed ASA, Garcia-Valdes L, Taha H, Amezcua-Prieto C. Health belief model-based educational interventions for knowledge, beliefs, and intentions on mammography: a systematic review. BMC Womens Health. 2025;26(1):48. doi:10.1186/s12905-025-04218-9
35. Mohammadkhah F, Kamyab A, Pezeshki B, Norouzrajabi S, Khani Jeihooni A. The effect of training intervention based on health belief model on self-care behaviors of women with gestational diabetes mellitus. Original Research Front Glob Womens Health. 2025;5:1490754. doi:10.3389/fgwh.2024
36. Rakhshani T, Poornavab S, Kashfi SM, Kamyab A, Jeihooni AK. The effect of educational intervention based on the health belief model on the domestic violence coping skills in women referring to comprehensive rural health service centers. BMC Women’s Health. 2024;24(1):596. doi:10.1186/s12905-024-03433-0
37. Kamau MW, Mirie W, Kimani S. Compliance with Iron and folic acid supplementation (IFAS) and associated factors among pregnant women: results from a cross-sectional study in Kiambu County, Kenya. BMC Public Health. 2018;18(1):580. doi:10.1186/s12889-018-5437-2
38. StataCorp. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC; 2023.
39. Tawfiq E, Stanikzai MH, Anwary Z, et al. Quality of antenatal care services in Afghanistan: findings from the national survey 2022–2023. BMC Pregnancy Childbirth. 2025;25(1):71. doi:10.1186/s12884-025-07206-x
40. Stanikzai MH, Tawfiq E, Jafari M, et al. Contents of antenatal care services in Afghanistan: findings from the national health survey 2018. BMC Public Health. 2023;23(1):2469. doi:10.1186/s12889-023-17411-y
41. Karki R, Khanal S, Joshi DR, Kaphle M. Compliance With Iron–Folic Acid Supplementation and Iron-Deficiency Anemia Among Pregnant Women in Kathmandu. Adv Public Health. 2025;2025(1):9964809. doi:10.1155/adph/9964809
42. Villardón-Gallego L, García-Cid A, Estévez A, García-Carrión R. Early educational interventions to prevent gender-based violence: a systematic review. Healthcare. 2023;11(1):142. doi:10.3390/healthcare11010142
43. Dahab R, Sakellariou D. Barriers to accessing maternal care in low income countries in africa: a systematic review. Int J Environ Res Public Health. 2020;17(12):4292. doi:10.3390/ijerph17124292
44. Belay DG, Tessema GA, Alemu MB, Kefale B, Dunne J, Norman R. Preferences of women for maternal healthcare services in low-income and middle-income countries: a systematic review of discrete choice experiments. BMJ Global Health. 2025;10(8):e017410. doi:10.1136/bmjgh-2024-017410
45. Meherali S, Rehmani M, Ali S, Lassi ZS. Interventions and strategies to improve sexual and reproductive health outcomes among adolescents living in low- and middle-income countries: a systematic review and meta-analysis. Adolescents. 2021;1(3):363–390. doi:10.3390/adolescents1030028
46. Aguree S, Gernand AD. Plasma volume expansion across healthy pregnancy: a systematic review and meta-analysis of longitudinal studies. BMC Pregnancy Childbirth. 2019;19(1):508. doi:10.1186/s12884-019-2619-6
47. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89–94. doi:10.5830/cvja-2016-021
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Barriers and Facilitators of Compliance with Iron-Folic Acid Supplementation Among Pregnant Women in Southern Afghanistan: A Qualitative Study
Stanikzai MH, Le CN, Isaramalai SA, Punsaward C, Ezadi Z, Sayam H, Shohaimi S, Dadras O, Suwanbamrung C
Patient Preference and Adherence 2026, 20:606199
Published Date: 13 May 2026