Back to Journals » Drug Design, Development and Therapy » Volume 14
Effective Tacrolimus Treatment for Patients with Non-Severe Aplastic Anemia That is Refractory/Intolerant to Cyclosporine A: A Retrospective Study
Authors Du Y, Huang Y, Zhou W, Liu X, Chen F ![]() , Yang C, Chen M, Ruan J
, Yang C, Chen M, Ruan J ![]() , Han B
, Han B
Received 18 August 2020
Accepted for publication 10 November 2020
Published 30 December 2020 Volume 2020:14 Pages 5711—5719
DOI https://doi.org/10.2147/DDDT.S275975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Yali Du,1 Yuzhou Huang,1 Wenzhe Zhou,1 Xinjian Liu,2 Fangfei Chen,1 Chen Yang,1 Miao Chen,1 Jing Ruan,1 Bing Han1
1Department of Hematology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, People’s Republic of China; 2Department of Hematology, Affiliated Cancer Hospital of Zhengzhou University, Henan Cancer Hospital, Institute of Hematology of Henan Province, Zhengzhou, People’s Republic of China
Correspondence: Bing Han
Department of Hematology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, People’s Republic of China
Email [email protected]
Background: For symptomatic non-severe aplastic anemia (NSAA) patients who cannot afford anti-thymocyte globulin (ATG) or allogeneic hematopoietic stem cell transplantation (HSCT), tacrolimus (FK) may be an option if these patients do not respond or become tolerant to cyclosporine A (CsA).
Methods: We enrolled 101 NSAA patients who were refractory or intolerant to CsA with no chance of HSCT or ATG treatment and treated these patients with tacrolimus for at least 6 months, with follow-up for at least one year.
Results: The overall response rate (ORR) was 38.6% (complete response: 9.9%; partial response: 28.7%), and the median time to optimal response was 6 (3~10) months. Thirty-two (31.7%) cases had elevated creatinine levels. Eight (7.9%) cases had elevations in AST/ALT. A total of 25.6% (10/39) of patients relapsed at the end of follow-up. Age (P=0.0005), FK concentration (4.0∼ 12 ng/mL, P=0.0005) and intolerance to CsA (P=0.012) were the independent risk factors for ORR. Treg cell levels pre-FK treatment were much lower than those of healthy controls (3.7± 0.6% vs 6.8± 0.7%, P=0.0004) but increased significantly after FK treatment (3.7± 0.6% vs 7.1± 0.8%, P=0.0039).
Conclusion: Our data suggest that tacrolimus is a salvage treatment for patients with NSAA that is refractory or intolerant to CsA.
Keywords: non-severe aplastic anemia, tacrolimus, cyclosporine A
Introduction
Aplastic anemia (AA) is a syndrome of hematopoietic failure due to various reasons that leads to diminished or absent hematopoietic precursors in the bone marrow and attendant pancytopenia. For patients who need treatment, age, disease severity, donor availability, and performance status play important roles in the decision-making process.1,2 For patients with acquired severe AA (SAA), young patients (≤50 years) with an HLA-matched sibling donor should undergo allogeneic hematopoietic stem cell transplantation (HSCT), and older patients (50 years or older) and young patients without a matched donor may receive full-dose immunosuppressive therapy (IST), such as horse/rabbit anti-thymocyte globulin (ATG) combined with cyclosporine A (CsA), as the first-line choice.
For patients who do not reach severe criteria (non-severe aplastic anemia, NSAA) and become transfusion-dependent, ATG + cyclosporine A may be the first-line therapy.1 The combination of ATG and CSA is superior to CSA alone for patients with NSAA,2 but patients with NSAA are often treated with CsA alone in the real world due to the high cost and potential risks of ATG, especially in developing countries. However, some patients do not respond to CsA or relapse at a later stage of follow-up.3,4 Patients may also withdraw from CsA due to some severe side effects, especially kidney impairment.
Tacrolimus (FK)5 is an immunosuppressive agent that is similar to cyclosporine A, and it inhibits the production and release of TNF-α, IFN-γ, and interleukin-2 (IL-2) and the IL-2-induced activation of resting T-lymphocytes. FK is used to prevent graft-versus-host disease (GVHD) and other autoimmune diseases.6 Tacrolimus exhibits 10~100 times the immunosuppressive effect of cyclosporine A and has fewer side effects, and it is occasionally used to treat AA patients who are refractory to CsA.7–10
The present study analyzed data from 101 patients with NSAA who were refractory or intolerant to CsA and were switched to FK treatment for at least 6 months. The efficacy and safety of FK were evaluated.
Materials and Methods
Patient Selection
From January 2017 to January 2019, all patients diagnosed with NSAA11 and treated with FK for at least 6 months in the Peking Union Medical College Hospital (PUMCH), and the relatively integrated clinical data were reviewed retrospectively. Included patients met the following criteria: 1) 12 years or older; 2) with confirmed diagnoses of NSAA; 3) were excluded for inherited bone marrow failure syndrome; 4) did not respond after at least 6 months of standard CsA (3~5 mg/kg/d) treatment or did not tolerate CsA due to side effects before FK; 5) met at least one of the following criteria but not reach the criteria for SAA before FK treatment: hemoglobin ≤90 g/L, or neutrophil (ANC) ≤0.8 × 109/L, or platelet counts ≤30 × 109/L; 6) with no history of HSCT; 7) not a candidate for ATG (could not afford or were not willing) or allo-HSCT; and 8) Serum creatinine (Scr) <200 μmol/L prior to FK treatment. Patients refractory to CsA were defined as those did not respond after at least 6 months of standard CsA (3~5mg/kg/d). Patients intolerant to CsA were defined as those who suffered from grade III to IV side effects according to National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE, version 4.0).
Treatment Regimen
All patients were treated with tacrolimus (Cyfokei, Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd., Hangzhou, Zhejiang, China) at initial dose of 1 mg b.i.d., and the dose was adjusted to maintain a plasma concentration of 4~10 ng/mL for at least 6 months. Patients with renal insufficiency before or after FK received a reduced drug dose and may not have reached the standard plasma concentration. Patients who reacted positively to FK continued the treatment for at least 1.5 years, and it was tapered gradually afterwards. The longest exposure time to FK was 30 months. The effectiveness of FK was evaluated after at least 6 months of treatment. Patients who did not reach PR after 6 months were recognized as no response (NR), and FK treatment was stopped, but the follow-up continued until the end of the study. Patients received transfusions as supportive care to maintain platelets at a level above 10 × 109/L and hemoglobin at a level above 60 g/L.
Clinical Evaluations
Patient symptoms (including side effects), signs and laboratory assessments (complete blood count with differential and serum chemistry profile, ECG or other tests if needed) and plasma FK concentrations were recorded at one month, three months, six months, and twelve months after treatment and at the end of follow-up. All medical records were taken from the official documents from our hospital. RBC or platelet transfusion requirements were also checked before and after FK treatment.
The following criteria were used for effectiveness. Complete response (CR): ANC >1.5 × 109/L, hemoglobin >110 g/L and platelet counts > 100 × 109/L for 2 months. Partial response (PR): patients who met the response criteria for one or more lineages at 12 weeks but did not meet the criteria of CR. Platelet response was defined as an increase of 20 × 109/L or more above the baseline value or independence from platelet transfusions for a minimum of eight weeks in patients who were previously transfusion-dependent. The erythroid response was defined as an increase in hemoglobin level of 15 g/L or more without transfusion of packed red cells or a reduction in the number of units of packed red cells transfused by at least four units for eight consecutive weeks compared to transfusion requirements during the eight weeks preceding FK treatment. The neutrophil response was defined as an absolute increase in neutrophil count of greater than 0.5 × 109/L in patients with a pretreatment count less than 0.5 × 109/L or at least a 100% increase over the baseline neutrophil count. NR: did not have any of the above responses.
Patients were followed up for at least one year or until the time of death. The final outcome was recorded from the medical documents or telephone interview of the patients or their relatives. Adverse events (AEs) were evaluated according to the CTCAE 4.0.
Examination of Regulatory T Cells
Anti-CD4 conjugated to FITC, anti-foxP3 conjugated to APC and anti-CD25 conjugated to PE antibodies were obtained from BD Biosciences (New Jersey, USA). Regulatory T (Treg) cells were determined via staining with markers of CD4-FITC, CD25-PE and foxP3-APC and subsequently analyzed using a Beckman Coulter FC500 flow cytometry (California, USA). Total events of 50,000 were gated based on forward (FSC) and side-scatter (SSC) characteristics, and dot plots for Treg cells were gated on CD4+cells. Treg cells were defined as CD4+CD25+foxP3+ co-expression and expressed as a percentage of the total CD4+ T population.12,13 Only 31 patients gave consent for the measurement of Treg cells before and after FK treatment. We recruited eight age- and gender-matched healthy volunteers and tested their Treg cells as normal controls.
Statistical Analysis
Proportions are given for categorical variables, means ± standard deviation are given for continuous variables, and medians (minimum, maximum) are given for variables that were not normally distributed. Chi-squared tests and Fisher’s exact test were used for categorical measures. Logistic regression models were used to estimate the odds ratio (OR) and 95% confidence interval (CI) for the association between potential risk factors and ORR. All analyses were performed using SAS version 9.4 (SAS Institute, Inc, Cary, NC, USA). A P-value <0.05 was considered statistically significant.
The median values and frequencies for the categorical data were described using descriptive analyses. SPSS 24.0 software (IBM, NY, USA) was used for statistical analyses. Data were analyzed using Fisher’s exact test and Pearson’s chi-squared test. P<0.05 was considered statistically significant.
Results
Patient Characteristics
From January 2017 to January 2019, there were 156 NSAA patients treated with FK. Fifty-five patients were excluded due to loss to follow-up (32 patients), withdrawal of FK (12 patients) within 6 months after FK, follow-up less than 12 months (10 patients) or denying consent (3 patients). There were 101 patients enrolled in the final analysis, including 49 males (48.5%) and 52 females (51.5%), with a median age of 46 (range 14~83) years. Fifty-eight (57.4%) patients were under the age of 50 years old. PUMCH is known for the treatment of difficult and complicated cases, so most refractory NSAA patients are referred to our clinic, which makes our cohort highly selective. Approximately 20% of younger patients discontinued CsA due to renal disfunction after repeated use for a long period of time. Table 1 shows the patients’ hematological and biochemistry parameters before FK treatment. For chromosome abnormalities, +8 was found in 5 patients, -Y in 3 patients, 20q- in 2 patients and monosomy 7 in 1 patient. Seven patients had notable PNH clone (paroxysmal nocturnal hemoglobinuria, PNH; percentage of FLAER-negative neutrophils from 3.5%~18.3%). Fifty (48.1%) patients were red blood cell transfusion-dependent, and the median transfusion requirements were 6 (range 4~10) units/eight weeks. Twenty-six (25.0%) patients were platelet transfusion-dependent, and the median transfusion requirements were 4 (range 1~5) units/eight weeks before FK treatment (Table 1).
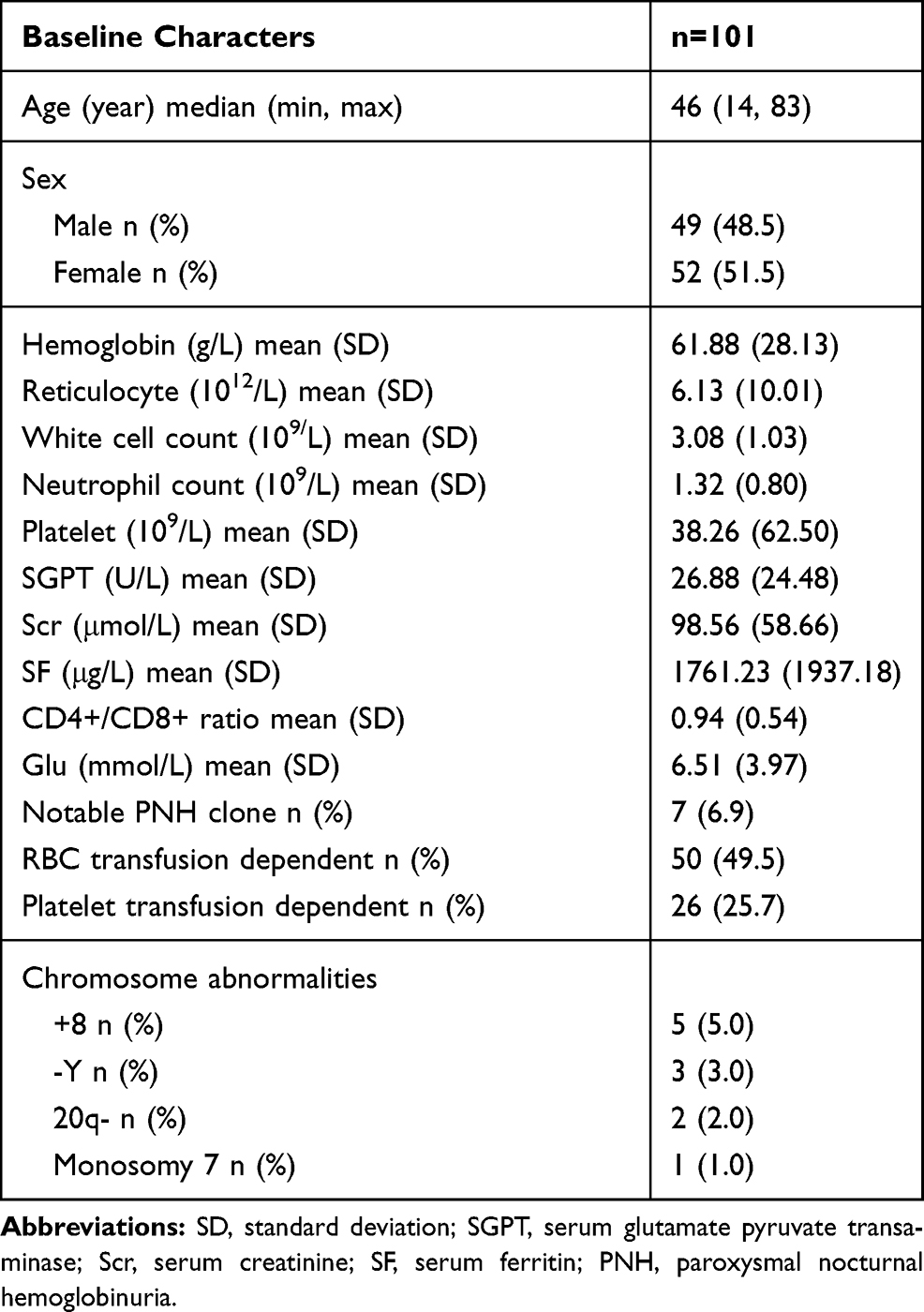 |
Table 1 Patients’ Baseline Demographic and Clinical Characters |
Patients were treated with CsA alone before FK treatment. Forty-five patients (refractory patients) had no response, and the median time for CsA treatment was 8 (6~10) months. Thirty-six patients (relapsed patients) relapsed when CsA was tapered or stopped but did not respond when CsA was added again or the dose was increased, and the median time for CsA treatment was 18 (12~60) months. Twenty patients (intolerant patients) did not tolerate CsA due to severe side effects, like gingival hyperplasia, muscle tremor, kidney impairment, and gastrointestinal disturbances. The median time of CsA exposure for these patients was 4 (3~7) months. None of these patients reached PR before FK treatment. Of all patients, 50 (53.2%) patients had FK concentrations of 4~12 ng/mL within three months of tacrolimus treatment, and the other patients did not reach the target concentration due to kidney limitations.
Efficacy
The median follow-up time was 19 (14~36) months from the start of FK treatment. At the end of follow-up, the median time of FK treatment was 14 (6~30) months. For all 101 patients, the median time to respond (at least PR) was 4 (1~6) months, and the medium time to optimal response was 6 (3~10) months. There were 10 (9.9%) CR, 29 (28.7%) PR, and 62 (61.4%) NR, for an OR (CR+PR) rate of 38.6%.
Of the 39 patients who achieved OR, 9 (23.1%) patients were solely an erythroid response (6 of them became transfusion-independent), 11 (28.2%) patients were solely a platelet response, 3 (7.7%) patients had a neutrophil response, 9 (23.1%) patients had bilineage responses, and 7 (17.9%) patients had trilineage responses.
Fourteen patients with liver or kidney impairment showed improved liver and kidney function after FK treatment. Ten of the patients with elevated creatinine levels and the other 4 patients with abnormal bilirubin levels prior to FK treatment returned to normal after 6 months of medication. Gingival hyperplasia and gastrointestinal symptoms improved significantly in 10 patients.
Subgroup analyses showed that the OR rate (ORR) for patients younger than 50 years old was 50.0%, which was significantly higher than patients over 50 years old (23.3%, P=0.004). Patients with FK concentrations 4.0~12.0 ng/mL had higher ORR (49.2%) compared to patients with concentrations <4.0 ng/mL (22.7%, P=0005). Females had a higher ORR than males (P= 0.0442). There was no significant difference in ORR between patients with refractory/relapsed and intolerant to CsA (35.8% vs 50.0%, P=0.2429, Table 2). However, multiple logistic regression results indicated that age (P=0.0005), FK concentration (4.0~12 ng/mL) (P=0.0005) and intolerance to CsA (P=0.0142) were independent risk factors for ORR (Table 3).
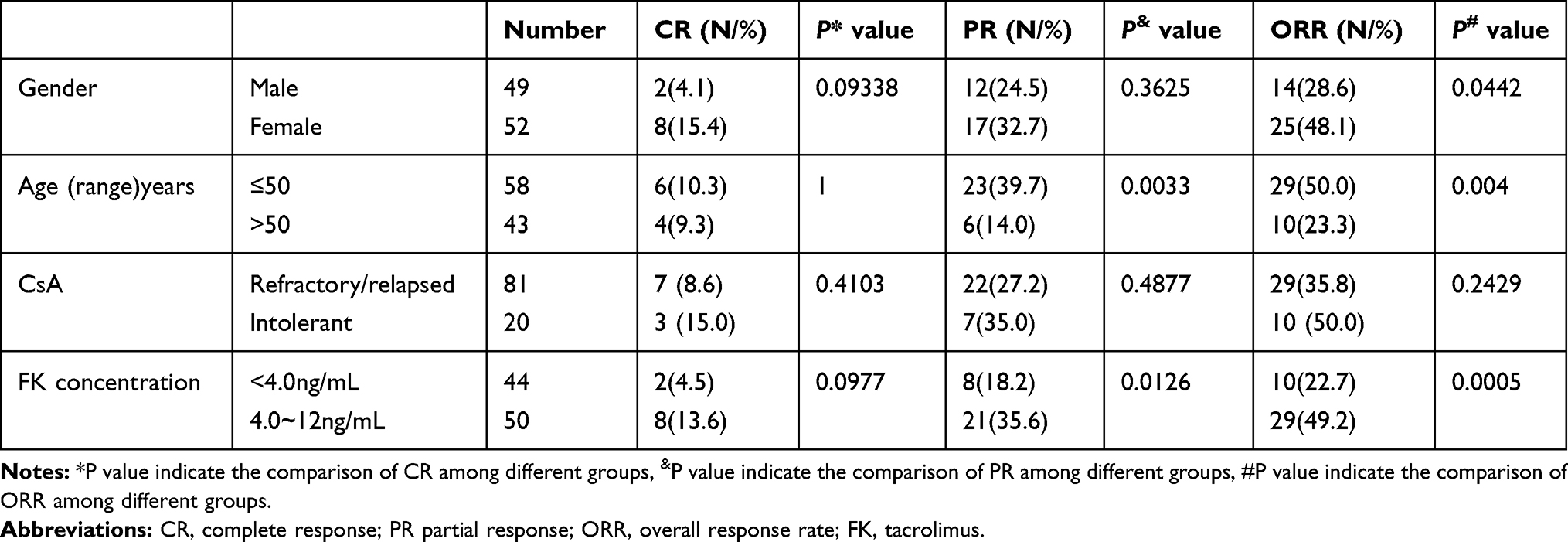 |
Table 2 Patients’ Response in Different Groups |
 |
Table 3 Multivariate Analysis for the Factors Associated with ORR |
Safety
Of the 101 total patients, there were 32 (31.7%) cases of elevated creatinine (9 of them had increased Scr level before FK treatment), 8 cases (7.9%) with elevated aspartate transaminase (AST)/alanine transaminase (ALT), 6 (5.9%) cases of hypertension, 5 (5.0%) cases of elevated bilirubin, and 2 (2.0%) cases of drug allergy. Most of them were grade I–II in CTCAE criteria 4.0 and recovered after symptomatic treatment. The following severe adverse events resulted in drug withdraw or hospitalization: 4 cases of grade III creatinine increase; 4 episodes of fever with grade III~IV neutropenia, one of which was linked to culture-confirmed infection; and one patient who did not have a response.
Relapse, Survival and Clonal Evolution
Of the 39 patients who reached CR or PR, 25.6% (10/39) of these patients relapsed at a median of 12 (10~16) months before FK tapering. Clonal evolution to acute myeloid leukemia (AML) was observed in one patient with monosomy 7 who did not response to FK. Two patients who did not respond evolved into myelodysplastic syndrome (MDS) one year after treatment and lived with supportive care. No increase in PNH clone or clonal evolution to MDS or AML developed in other patients in our cohort. Four young patients who did not respond underwent HSCT and achieved CR.
There were two deaths during the follow-up period in the no response cohort. One death was due to severe infections, as mentioned above, and the other death was the patient who transformed to AML and died of infections 2 months after chemotherapy. Other patients with no response lived with supportive care. No other deaths were observed in the cohort.
Regulatory T Cells in the Peripheral Blood Before and After FK
Treg cells were measured in 31 patients before and six months after FK, and they all achieved at least PR. The level of Treg cells from eight age- and sex-matched normal volunteers were used as controls. The level of Treg cells pre-FK was much lower than healthy controls (Treg/CD4+ T: 3.7±0.6% vs 6.8±0.7%, P=0.0004). As expected, the level of Treg cells increased significantly after FK treatment (Treg/CD4+ T, before: 3.7±0.6% vs after: 7.1±0.8%, P=0.0039, Figure 1).
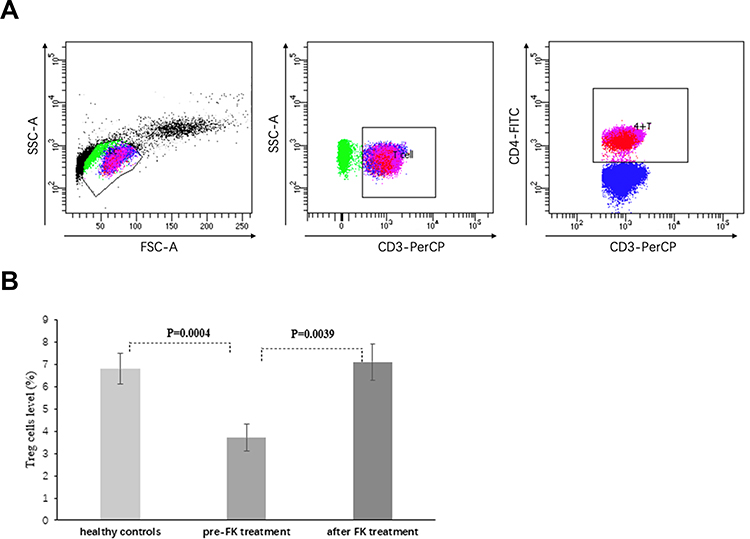 |
Figure 1 Regulatory T cells in peripheral blood before and after FK. (A) Total events of 50,000 were gated based on FSC and SSC characteristics, and dot plots for Treg cells were gated on CD4+ cells. Treg cells were defined as CD4+CD25+foxP3+ co-expression and expressed as a percentage of the total CD4+ T population. (B) The expression of Treg cells from 31 patients who achieved at least PR was tested before and 6 months after FK treatment. Eight age- and sex-matched normal volunteers were used as controls. Levels of Treg cells pre-FK were much lower compared to healthy controls, but increased significantly after FK treatment. FSC, forward-scatter characteristics; SSC, side-scatter characteristics; Treg cells, T regular cells; FK, tacrolimus; PR, partial response. |
The CD4+/CD8+ Ratio in the Peripheral Blood Before and After FK
The mean CD4+/CD8+ ratio for 81 patients (0.94±0.54) was significantly decreased in AA patients before tacrolimus in comparison with that of 21 normal controls (2.18±0.47, P<0.0001). Fifteen patients evaluated CD4+/CD8+ ratio after hematopoietic improvement following tacrolimus, and showed an increase of the CD4/CD8 ratio (0.92±0.44 vs 1.57±0.76, P=0.0078), whereas 3 patients with no response to tacrolimus showed no change of CD4/CD8 ratio (0.98±0.58 vs 1.03±0.56, P=0.92).
Discussion
Although CsA achieved a 40~50% response rate and has long-term effects on the maintenance and survival of patients with non-severe aplastic anemia,2,3 an unmet need remains when patients do not response, relapse, or are intolerant to CsA.8,14 Although intensive immunosuppressive therapy with ATG and HSCT further improve the response rate, these treatments are relatively expensive, risky, sometimes unavailable, and not suitable to older and weak patients.15 The oral thrombopoietin receptor agonist Eltrombopag16 was launched in China recently, and it has emerged as a promising new drug for the treatment of aplastic anemia.17,18 However, the price is too high for regular use in most patients.
Our study examined a large cohort with relatively long term follow-up for the second-line use of tacrolimus in NSAA. Many patients in our study were referred from local hospitals and were refractory or intolerant to CsA treatment. Our study showed that at the median time of 4 (1~6) months, 38.6% of patients achieved a response to varying degrees, with 9.9% CR and 28.7% PR. Of the patients who achieved CR and PR, most had a monolineage reaction, and a few had a bilineage or trilineage response. For these patients, FK produced some reaction, but primarily PR rather than CR. Patients reached optimal effects at a median of 6 months, and 25.6% of patients who responded relapsed at a median of 12 months before FK tapering. Although patients gained some benefit from the hematology improvement and elimination of transfusion, FK provided a different choice with an acceptable response because most of the patients in our study were CsA resistant or intolerant.
Most of the studies on tacrolimus were case reports or focused on the replacement of CsA in ATG or bone marrow transplantation (BMT) regimens.6–8,14 However, these studies verified our results to some extent. Matched-pair analysis by Yagasaki et al6 to compare FK/methotrexate (MTX) with CsA/MTX in patients with SAA who received U-BMT (unrelated BMT) indicated that the 5-year survival rate was higher in the FK group compared to the CsA group. These results show the superiority of FK/MTX over CsA/MTX in overall survival because of the lower incidence of transplantation-related deaths. Zhu et al7 showed that 54% of 13 patients with SAA in the tacrolimus + rabbit-ATG group and 42% of 24 cases in the ATG + CsA group achieved the criteria for CR, and the PR rate was similar between the two groups, which suggests the use of tacrolimus as part of the IST regimen. The effects of tacrolimus are further manifested in some case reports that FK improved the hematopoiesis of some AA patients who were refractory to CsA, and a pediatric study demonstrated the use of tacrolimus in the maintenance phase of IST with 88% of CR in SAA.8
Notably, tacrolimus seemed safer and more tolerable compared to CsA. A large number of patients with SAA treated with CsA showed hirsutism and gingival hyperplasia, and kidney injury was very commonly seen.14 A total of 31.7% of cases had elevated creatinine levels in our cohort, which was likely due to the long-term use of CsA before FK treatment, but most of them were mild and controllable (four patients withdrew FK treatment due to grade III creatinine increase). Very few cases of elevated AST/ALT, hypertension, elevated bilirubin and drug allergy were observed. No hirsutism or gingival hyperplasia was noted. Fourteen patients with liver or kidney impairment exhibited improved liver and kidney function after FK treatment. These results are consistent with previous reports that tacrolimus exhibited much greater safety and lower impact on renal function and blood pressure than cyclosporine A.19,20
We further analyzed the possible influencing factors for FK response. Older patients seemed to have poorer reactions compared with younger patients, and similar findings were reported in patients with SAA who received ATG+CsA or allo-BMT.2 Older patients may have less remaining hematopoiesis and do not have a sufficient storage of kidney function to achieve proper FK concentration, which may contribute to the poorer response. Notably, patients with different FK concentrations had different ORRs. Patients with enough plasma concentration (>4.0ng/l) got better OR rate compared those with insufficient plasma concentration (ORR 49.2% vs 22.7%, P=0.0005), which indicates the importance of maintaining sufficient drug exposure. Some patients with renal insufficiency did not receive the full dose of FK and stayed at a low concentration, and the ORR was lower for these patients accordingly. Patients who were refractory/relapsed to CsA had inferior ORRs in our cohort compared to patients who were intolerant to CsA in multiple logistic regression analysis. It is easily understood that patients who stopped CsA due to side effects may have more chance of response if they are treated continuously with FK compared to patients who had no response to CsA. Although female gender played a role in the univariate analysis, logistic regression indicated that it was not an independent risk factor.
Previous research demonstrated that IL-2 enhanced the proliferation and expression of TNF-α in CD8(+)HLA-DR(+) T cells from AA patients, and tacrolimus may inhibit this effect, which is also true for CsA.21,22 However, tacrolimus may have a different mechanism of action from CsA because we observed that the decreased level of Treg cells after CsA treatment significantly improved after a full dose of tacrolimus in patients who responded.13,23 Treg cells, identified as CD4+CD25+ and Foxp3+, were obviously lower in patients with untreated AA compared to normal people and increased significantly after effective treatment with IST.24,25 Besides, CD4+/CD8+ ratio decreased in AA patients and got a recovery after hematopoietic improvement by tacrolimus treatment.
Three patients had clonal evolution to MDS or AML, which was similar to patients who were refractory to CsA.26 Patients who did not react to immunosuppressive agents had greater pressure of clonal selection under bone marrow failure environment or more clonal hematopoiesis at the very beginning. For patients who had no response, infection and bleeding were common, and 1 patient died of infection 12 months after FK treatment, which was also seen in patients who failed other treatments.
There are some limitations of the present study. One-third of patients were excluded from analysis due to the short period of treatment or follow-up time, which may cause bias because some of these patients may have a less positive response to FK. Follow-up time was limited for long-term efficacy, survival and clone evolution. No regular molecular tests were done in our cohort before or after FK treatment, which may limit the prediction of clone evolution.
Conclusion
We summarized the second-line use of FK in the real world for the first time. FK may be an alternative treatment option for patients who are refractory or intolerant to CsA with an acceptable price and tolerance. Further investigation with larger patient numbers and proper controls are needed.
Abbreviations
NSAA, non-severe aplastic anemia; SAA, severe aplastic anemia; AA, aplastic anemia; ATG, anti-thymocyte globulin; HSCT, hematopoietic stem cell transplantation; FK, tacrolimus; CsA, cyclosporine A; ORR, overall response rate; CR, complete response; PR, partial response; NR, no response; OR, odds ratio; IST, immunosuppression therapy; GVHD, graft-versus-host disease; PUMCH, Peking Union Medical College Hospital; AE, adverse events; CTCAE, common toxicity criteria for adverse events; Treg cells, regulatory T cells; CI, confidence interval; AML, acute myeloid leukemia; MDS, myelodysplastic syndrome; PNH, paroxysmal nocturnal hemoglobinuria.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained from all patients over 18 years old and patients or legal guardian for patients under the age of 18 years old. Before data collected, and all clinical procedures were performed in accordance with the Declaration of Helsinki.
Consent for Publication
Consent for publication was obtained from all patients and accompanied by informed consent at the beginning of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Beijing Natural Science Foundation (7192168), the Chinese Academy of Medical Sciences (CAMS) innovation fund for medical sciences (2016-I2M-3-004) and the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2019XK 320047).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Pierri F, Dufour C. Management of aplastic anemia after failure of frontline immunosuppression. Expert Rev Hematol. 2019;12(10):809–819. doi:10.1080/17474086.2019.1645003
2. Marsh J, Schrezenmeier H, Marin P, et al. Prospective randomized multicenter study comparing cyclosporin alone versus the combination of antithymocyte globulin and cyclosporin for treatment of patients with nonsevere aplastic anemia: a report from the European Blood and Marrow Transplant (EBMT) Severe Aplastic Anaemia Working Party. Blood. 1999;93(7):2191–2195.
3. Zhu XF, He HL, Wang SQ, et al. Current treatment patterns of aplastic anemia in China: a prospective cohort registry study. Acta Haematol. 2019;142(3):162–170. doi:10.1159/000499065
4. Alashkar F, Oelmuller M, Herich-Terhurne D, et al. Immunosuppressive therapy (IST) in adult patients with acquired aplastic anemia (AA): A single-center experience over the past 15 years. Eur J Haematol. 2019;103(1):18–25. doi:10.1111/ejh.13235
5. Tong J, Viale M, Bacigalupo A, Esposito M. Effect of FK-506 and cyclosporin A on in vitro CFU-GM growth in severe aplastic anemia patients. Haematologica. 1992;77(4):369–370.
6. Yagasaki H, Kojima S, Yabe H, et al. Tacrolimus/Methotrexate versus cyclosporine/methotrexate as graft-versus-host disease prophylaxis in patients with severe aplastic anemia who received bone marrow transplantation from unrelated donors: results of matched pair analysis. Biol Blood Marrow Transplant. 2009;15(12):1603–1608. doi:10.1016/j.bbmt.2009.08.012
7. Zhu X, Guan J, Xu J, et al. Pilot study using tacrolimus rather than cyclosporine plus antithymocyte globulin as an immunosuppressive therapy regimen option for severe aplastic anemia in adults. Blood Cells Mol Dis. 2014;53(3):157–160. doi:10.1016/j.bcmd.2014.04.008
8. Alsultan A, Goldenberg NA, Kaiser N, Graham DK, Hays T. Tacrolimus as an alternative to cyclosporine in the maintenance phase of immunosuppressive therapy for severe aplastic anemia in children. Pediatr Blood Cancer. 2009;52(5):626–630. doi:10.1002/pbc.21926
9. Inamoto Y, Flowers ME, Wang T, et al. Tacrolimus versus cyclosporine after hematopoietic cell transplantation for acquired aplastic anemia. Biol Blood Marrow Transplant. 2015;21(10):1776–1782. doi:10.1016/j.bbmt.2015.05.023
10. Macartney C, Freilich M, Odame I, Charpentier K, Dror Y. Complete response to tacrolimus in a child with severe aplastic anemia resistant to cyclosporin A. Pediatr Blood Cancer. 2009;52(4):525–527. doi:10.1002/pbc.21751
11. Camitta BM, Storb R, Thomas ED. Aplastic anemia (second of two parts): pathogenesis, diagnosis, treatment, and prognosis. N Engl J Med. 1982;306(12):712–718. doi:10.1056/NEJM198203253061204
12. Lin S, Hou L, Liu S, et al. Roles of regulatory T cells in the pathogenesis of pediatric aplastic anemia. Pediatr Hematol Oncol. 2019;36(4):198–210. doi:10.1080/08880018.2019.1621968
13. Dong QE, Fu R, Liu CY, et al. [Inhibitory effects of tacrolimus on effector T cells from patients with severe aplastic anemia]. Zhonghua Yi Xue Za Zhi. 2013;93(20):1541–1545. Chinese.
14. Vallejo C, Iniesta P, Moraleda JM. Resolution of cyclosporine-induced gingival hyperplasia resistant to azithromycin by switching to tacrolimus. Haematologica. 2001;86(1):110.
15. Tisdale JF, Dunn DE, Maciejewski J. Cyclophosphamide and other new agents for the treatment of severe aplastic anemia. Semin Hematol. 2000;37(1):102–109. doi:10.1016/S0037-1963(00)90034-9
16. Fattizzo B, Levati G, Cassin R, Barcellini W. Eltrombopag in immune thrombocytopenia, aplastic anemia, and myelodysplastic syndrome: from megakaryopoiesis to immunomodulation. Drugs. 2019;79(12):1305–1319. doi:10.1007/s40265-019-01159-0
17. Ecsedi M, Lengline E, Knol-Bout C, et al. Use of eltrombopag in aplastic anemia in Europe. Ann Hematol. 2019;98(6):1341–1350. doi:10.1007/s00277-019-03652-8
18. Cheng H, Wang X, Zhou D, Cao J, Larochelle A, Xu KL. Eltrombopag combined with cyclosporine may have an effect on very severe aplastic anemia. Ann Hematol. 2019;98(8):2009–2011. doi:10.1007/s00277-019-03658-2
19. Liu JY, You RX, Guo M, et al. Tacrolimus versus cyclosporine as primary immunosuppressant after renal transplantation: a meta-analysis and economics evaluation. Am J Ther. 2016;23(3):e810–824. doi:10.1097/MJT.0000000000000150
20. Muduma G, Saunders R, Odeyemi I, Pollock RF. Systematic review and meta-analysis of tacrolimus versus ciclosporin as primary immunosuppression after liver transplant. PLoS One. 2016;11(11):e0160421.
21. Halloran PF, Madrenas J. The mechanism of action of cyclosporine: a perspective for the 90’s. Clin Biochem. 1991;24(1):3–7. doi:10.1016/0009-9120(91)90063-K
22. Bai YJ, Wang LL, Cai B, Zou YG, Feng WH, Yan LN. [Regulatory function of tacrolimus and CsA on CD4/CD8 T lymphocyte subgroups and costimulators on them in allo-liver recipients]. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2008;24(10):989–992. Chinese.
23. Miroux C, Morales O, Ghazal K, et al. In vitro effects of cyclosporine A and tacrolimus on regulatory T-cell proliferation and function. Transplantation. 2012;94(2):123–131. doi:10.1097/TP.0b013e3182590d8f
24. Solomou EE, Rezvani K, Mielke S, et al. Deficient CD4+ CD25+ FOXP3+ T regulatory cells in acquired aplastic anemia. Blood. 2007;110(5):1603–1606.
25. Kordasti S, Costantini B, Seidl T, et al. Deep phenotyping of Tregs identifies an immune signature for idiopathic aplastic anemia and predicts response to treatment. Blood. 2016;128(9):1193–1205. doi:10.1182/blood-2016-03-703702
26. Hama A, Takahashi Y, Muramatsu H, et al. Comparison of long-term outcomes between children with aplastic anemia and refractory cytopenia of childhood who received immunosuppressive therapy with antithymocyte globulin and cyclosporine. Haematologica. 2015;100(11):1426–1433. doi:10.3324/haematol.2015.128553
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.