Back to Journals » Clinical Interventions in Aging » Volume 21
Effect of the Center Bridge-Type Knee Orthosis on the External Knee Adduction Moment During Gait in Patients with Knee Osteoarthritis
Authors Nakano K, Mine Y ![]() , Katsuhira J, Yamauchi K, Kitashiro M, Nomoto S, Asano N
, Katsuhira J, Yamauchi K, Kitashiro M, Nomoto S, Asano N
Received 11 August 2025
Accepted for publication 2 December 2025
Published 3 February 2026 Volume 2026:21 558427
DOI https://doi.org/10.2147/CIA.S558427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Kosuke Nakano,1,2 Yasuhiro Mine,3 Junji Katsuhira,3 Kantaro Yamauchi,2 Masateru Kitashiro,4 So Nomoto,4 Nobuhiro Asano5
1School of Information-Oriented Management, SANNO University, Isehara, Kanagawa, Japan; 2Graduate School of Human Life Design, Toyo University, Kita, Tokyo, Japan; 3Faculty of Design for Welfare Society, Toyo University, Kita, Tokyo, Japan; 4Keiyu Orthopedic Group, Adachi, Tokyo, Japan; 5IZUMI Orthopedics, Kita, Tokyo, Japan
Correspondence: Kosuke Nakano, School of Information-Oriented Management, SANNO University, 1573 Kamikasuya, Isehara, Kanagawa, 259-1197, Japan, Tel +81-80-4206-2692, Fax +81-463-93-0554, Email [email protected]
Purpose: This study aimed to investigate the biomechanical effects of a center bridge-type knee orthosis prescribed for patients with knee osteoarthritis (OA) based on real-time, direct quantification of external knee adduction moment (EKAM), a key mechanical indicator associated with progression of knee OA.
Patients and Methods: To evaluate the effect of the center bridge-type knee orthosis, 17 patients with knee OA performed level-ground walking under two conditions: with and without the orthosis. Each participant completed gait trials in both conditions in a randomized order. Additionally, 18 healthy older individuals were assessed during free walking for comparisons. The analysis focused on the gait stance phase, during which substantial mechanical loading was exerted on the knee joint. Gait data were obtained using a six-axis force-torque sensor.
Results: In patients with knee OA, wearing the orthosis significantly reduced EKAM during the loading response compared with that in the no-orthosis condition. Furthermore, EKAM values in patients wearing the orthosis became comparable to those in healthy participants during the loading response and pre-swing phases. No significant differences in gait parameters, such as walking speed or stride length, were observed between groups or conditions.
Conclusion: These findings suggest that in patients with OA, achieving EKAM values comparable to those in healthy individuals would require a valgus corrective moment at least 5.34 times greater than that produced by the center bridge-type knee orthosis. Clinically, this indicates that current orthotic designs may provide insufficient mechanical offloading, and that further structural refinements are required to enhance valgus correction and achieve more effective reduction of medial knee loading during gait.
Plain Language Summary: In knee osteoarthritis, the joint cartilage breaks down, resulting in knee pain, swelling, and stiffness. External knee adduction moment (EKAM) is a biomechanical indicator of medial knee loading during walking. Measuring EKAM is useful for assessing disease progression. In this study, we evaluated a center bridge-type knee orthosis designed to reduce medial knee load and improve gait. A total of 17 patients with knee osteoarthritis and 18 healthy adults participated. Each participant performed level-ground walking with and without the orthosis, while the support provided by the device was quantified in real time using a built-in six-axis force sensor. The orthosis significantly reduced EKAM during the loading response, with values approaching those of healthy individuals. Furthermore, during pre-swing, when the foot prepares to leave the ground for the next step, medial knee loading was also close to healthy levels. However, gait parameters such as walking speed and stride length showed no significant differences between groups or conditions. These findings indicate that the orthosis provides substantial mechanical support during the early stance phase and continues to reduce medial knee loading even during the transition to swing. Nevertheless, to fully normalize EKAM throughout the stance phase, a corrective force that gently pushes the knee outward and is approximately five-fold stronger than what the current orthosis can generate would be required. These insights will guide the development of future knee orthoses capable of adjusting support dynamically throughout walking.
Keywords: valgus corrective moment, walking biomechanics, force-torque sensor, loading response, stance phase
Introduction
Osteoarthritis (OA) of the knee is a chronic disorder characterized by gradual degeneration of the joint, eventually leading to swelling and pain. In 2019, approximately 528 million people worldwide were affected by knee OA, representing a 113% increase since 1990.1 Both systemic factors, such as age, sex, and genetic predisposition, as well as local factors, such as excessive mechanical stress due to obesity and muscle weakness, contribute to the onset and progression of knee OA.2–5 Various treatment options are available for knee OA.6 When conservative therapies, such as physiotherapy, fail to alleviate symptoms, surgical interventions, such as total knee arthroplasty, may become necessary.6–8
However, although total knee arthroplasty generally results in significant pain relief and improvements in joint mobility and overall function, persistent postoperative pain and reduced patient satisfaction are still frequently reported.9 For example, postoperative satisfaction surveys indicate that approximately 13% of patients remain dissatisfied, even under favorable clinical and radiological conditions.10
Poor postoperative outcomes may be associated with misalignment and uneven load distribution, which deviate from the natural kinematics of the knee joint.11–13 Therefore, whether through conservative or surgical treatment, reducing the mechanical load on the knee is crucial for preventing the progression and exacerbation of OA.14–16 The external knee adduction moment (EKAM) is a key parameter that helps track the progression of knee OA. In clinical practice, knee orthoses designed to reduce EKAM are often prescribed in addition to physiotherapy.17–21
Several studies have investigated the effects of knee orthoses on EKAM.20,21 A study comparing EKAM values in individuals with varus alignment during walking and running showed that the use of a valgus orthosis significantly decreased EKAM.20 However, the corrective force exerted by the knee orthosis was not directly measured in that study, as the effectiveness of the orthosis was inferred from gait analysis.
The structural aspects of knee orthoses have been extensively researched. Previous studies have estimated the structural characteristics and corrective forces of knee orthoses by attaching strain gauges, pressure sensors, or load sensors to specific parts of the orthotic structure.18,20–23 However, these measurements were indirect and inherently limited in terms of accuracy, complicating precise evaluations of the mechanical properties of orthoses. Indirect evidence of the effectiveness of knee orthoses has been obtained through analyses of gait patterns recorded with and without orthotic use.20,24 In a recent study, attempts were made to directly assess the corrective forces of knee orthoses by incorporating sensors capable of measuring force and moment into the orthotic structure.25 However, that study included only five healthy participants and was limited to sports-related movements. Consequently, the extent to which knee orthoses can reduce mechanical stress in patients with knee OA remained unresolved.25 Furthermore, previous studies primarily compared gait with and without orthotic use, and it remained unclear how much of the corrective moment was generated by the orthotic structure itself—specifically, the valgus moment produced at the interface between the thigh and shank segments. To address this gap, it is necessary to directly quantify the extent by which EKAM values could be reduced by wearing a knee orthosis.
The results of previous studies, which compared EKAM values in individuals with and without knee orthoses, may reflect not only the valgus corrective moment generated by the orthosis but also changes in gait patterns induced by orthotic use.26 Therefore, it is also necessary to clarify whether the observed reduction in EKAM was attributable to the mechanical effects of the orthosis itself or to secondary gait adaptations.
In the present study, we directly measured the valgus corrective moment generated by a knee orthosis during gait using a six-axis force sensor and evaluated the effect of the orthosis on EKAM. A key strength of this approach was that it allowed for real-time, direct quantification of the corrective moment produced by the structural interaction between the thigh and shank components of the orthosis, an element that had previously been inferred only indirectly. In addition, we estimated the magnitude of the corrective force required to reduce EKAM in patients with knee OA to a level comparable to that in healthy individuals.
We hypothesized that applying a valgus corrective moment using a knee orthosis would reduce EKAM in patients with knee OA and that achieving EKAM values comparable to those in healthy individuals would require a greater magnitude of valgus correction than that produced by existing orthotic designs.
Materials and Methods
Participants and Ethical Approval
This study included 17 patients with left knee OA (8 men and 9 women) and 18 healthy participants (11 men and 7 women). The demographic characteristics, including age, sex, height, and weight, of both groups are summarized in Table 1. No significant differences were noted between patients with OA and healthy participants in terms of age, sex, height, and weight (p > 0.05). Knee OA was diagnosed by a physician. Eligible patients included those who were either using a knee orthosis for the first time or those wearing a flexible orthosis regularly. None of the patients had a history of knee surgery, and all were diagnosed with grade II (n = 10) or grade III (n = 7) OA according to the Kellgren–Lawrence (KL) grading system, as determined by an experienced orthopedic surgeon based on radiographic findings.27 Among the 10 patients diagnosed with KL grade II OA in the left knee, two also had KL grade III OA in the right knee. The left limb was chosen as the test limb for orthosis application and analysis to ensure consistency in orthosis fitting, sensor alignment, and gait data acquisition. Accordingly, although two participants had more severe OA in the right knee (KL grade III), the analysis was limited to the left side to maintain methodological consistency. Corresponding gait data from the left limb of healthy participants were analyzed for comparison.
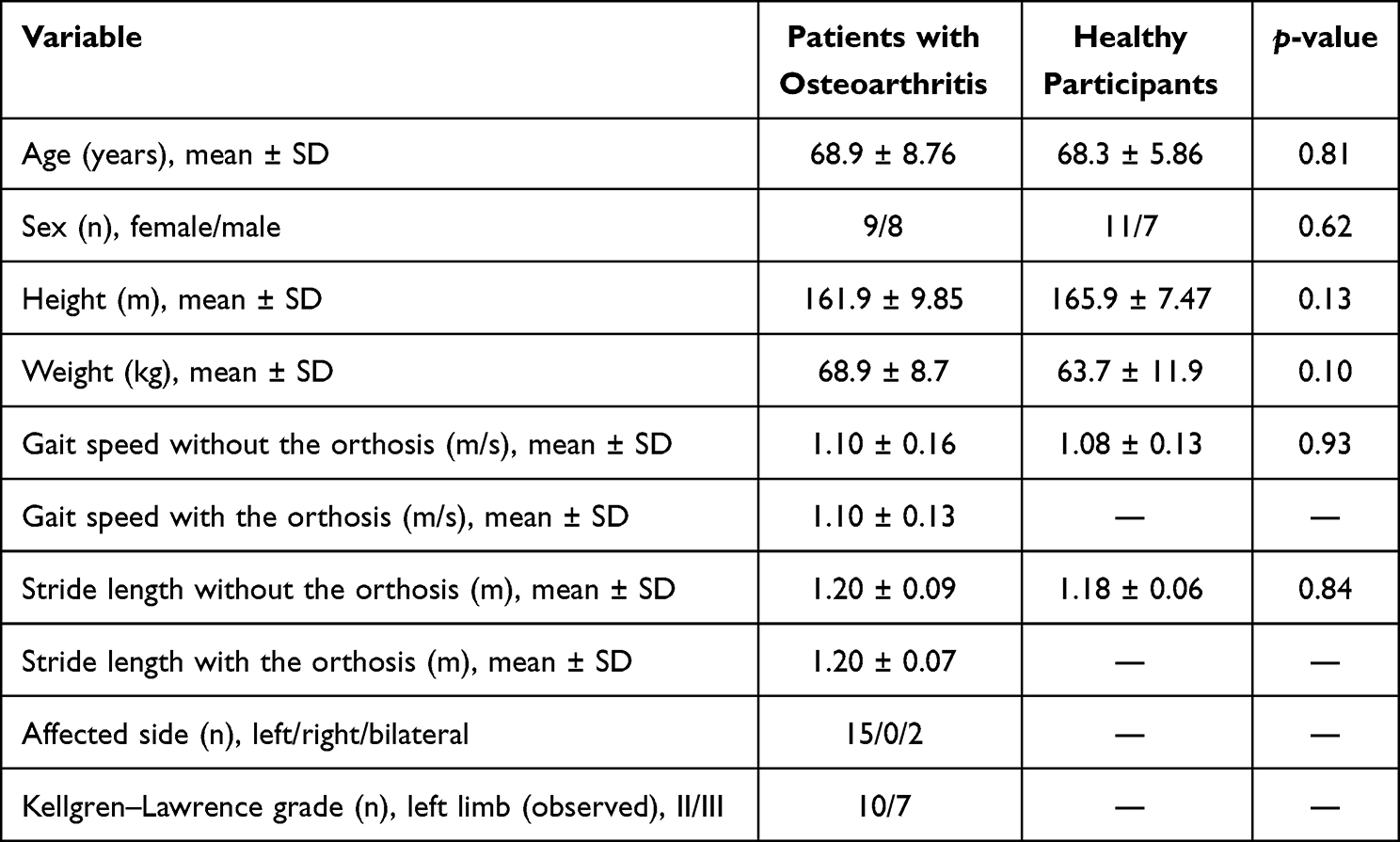 |
Table 1 Demographic Characteristics, Clinical Characteristics, and Kinematic Parameters of Study Participants |
We excluded individuals who were unable to walk independently indoors without a cane, presented with other orthopedic or central nervous system disorders, were unable to communicate, had epilepsy or fever, consumed alcohol, or showed significant symptoms, such as pain or swelling, on the day of measurement. Healthy participants included those without a history of orthopedic or central nervous system disorders. As the patients with knee OA were generally older, we adopted an age-based recruitment strategy to minimize age-related differences and potential confounding effects. Although sex was not strictly matched, healthy participants were recruited selectively to achieve comparable age distribution between groups.
The required sample size for this pilot study was estimated using G*Power 3.1.9.7 (Heinrich Heine University, Düsseldorf). Based on an effect size of 0.3, statistical power of 0.9, alpha level of 0.05, correlation among repeated measures of 0.7, and four measurement sessions, the minimum required sample size was 14 participants.28–30 For pilot studies, in which only limited data are available to calculate the formal sample size, approximately 12 participants per group should be recruited.31 In the present study, the estimated sample size met both the necessary statistical requirements and minimum recommended sample size for a pilot study.
All participants were provided with a written document approved by the Research Ethics Committee of the Graduate School of Life Design, Toyo University (approval Nos.: 2023-A14 and 2024-A6S). Prior to data collection, the experimental protocol was explained both in writing and verbally, and informed consent was obtained from all participants. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Experimental Setup
A knee orthosis measurement system was used to assess the corrective moment exerted by a center bridge-type knee orthosis (Sakima Prosthetics and Orthotics Co., Ltd., Okinawa, Japan). This system was designed to apply valgus correction by supporting the knee at three points on the thigh and lower leg to reduce EKAM (Figure 1).
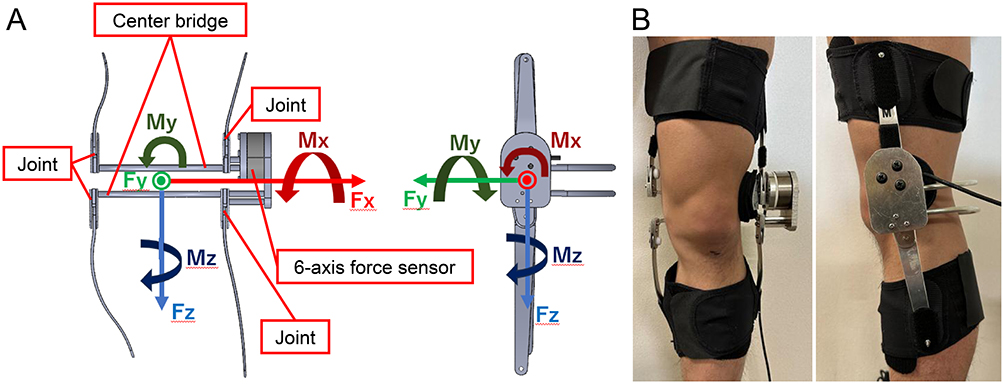 |
Figure 1 Coordinate system of the knee orthosis measurements and knee orthosis-wearing conditions. (A) Schematic diagram of the force and moment axes of the measurement knee orthosis. (B) Wearing of the knee orthosis. |
A center bridge-type knee orthosis was selected for this study, as its structure enables stable three-point support during gait and allows for accurate measurement of the corrective moment. To measure the varus–valgus corrective moment generated between the thigh and lower leg, a six-axis force sensor (model: SAN050102200A00, Leptrino Co., Ltd., Saku City, Nagano, Japan) was integrated into the relatively rigid joint section of the knee orthosis structure. The sensor was installed at an intermediate position between the thigh and lower leg sections, allowing for precise measurements of the corrective forces and moments. This six-axis force sensor detects translational forces (Fx, Fy, Fz) and moments (Mx, My, Mz) using strain gauges and converts them into digital signals via an integrated amplifier board. The sensor provides both analog output (16-bit D/A conversion, ±2.0 V range, low-pass filter at 300 Hz) and USB digital output (resolution ±1/4,000 DC) at a sampling rate of 1.2 kHz. The rated capacities were ±1000 N for Fx, Fy, and Fz, and ±20 Nm for Mx, My, and Mz, with nonlinearity within ±1.0% of rated output (R.O.) and cross-axis interference within ±2.0% R.O. Before data collection, the sensor was calibrated according to the manufacturer’s standard procedure using reference loads to ensure measurement accuracy, and all sensor outputs were verified for linearity and zero-drift stability before each experimental session. Specifications of the six-axis force sensor were based on the manufacturer’s technical documentation (Specification No. SSAN050002C, Leptrino Co., Ltd).
The six-axis force sensor enables measurements of forces and moments along three orthogonal axes, thereby capturing the complex dynamic interactions between forces and moments that occur between the thigh and lower leg due to the knee orthosis. This approach enables the direct mechanical evaluation of the corrective function of the orthosis, which is difficult to achieve using indirect methods, such as gait analysis alone.25
The forces and moments measured using the six-axis force sensor were defined according to a right-handed coordinate system, in which the x-axis pointed outward, the y-axis aligned with the direction of movement, and the z-axis corresponded to the direction of body weight. The analysis focused on the y-axis moment, which represents the varus–valgus corrective moment generated by the knee orthosis. When the orthosis applied a valgus (abduction) correction to the lower leg relative to the thigh, the moment was assigned a negative (−) sign. When the orthosis applied a varus (adduction) correction, the moment was assigned a positive (+) sign. The sensor coordinate system was aligned with the orthosis frame and transformed into the global coordinate system during the analysis to maintain consistency in moment interpretation.
Three force plates (AMTI, Watertown, MA, USA) and seven infrared cameras (MX T-series, sampling rate: 960 Hz; Vicon Motion System Ltd., Oxford, UK) were used for data acquisition. Infrared reflective markers (diameter: 14 mm, based on the Helen Hayes marker set) were attached to the parietal, forehead, occipital regions; both acromion processes; both elbow joints, wrist joints, and C7 cervical vertebra; anterior and posterior superior iliac spines; both thighs; medial and lateral knee joints; bilateral lower legs; both medial and lateral malleoli of the ankle joints; and both second metatarsal heads. For the left leg, which was fitted with a knee orthosis, two additional infrared reflective markers were attached to the thigh and lower leg, resulting in a total of 34 markers (Figure 2). All markers were captured using an optical three-dimensional motion capture system (ViconNexus2; Vicon Motion System Ltd.) in a reference stationary standing position for 30s.
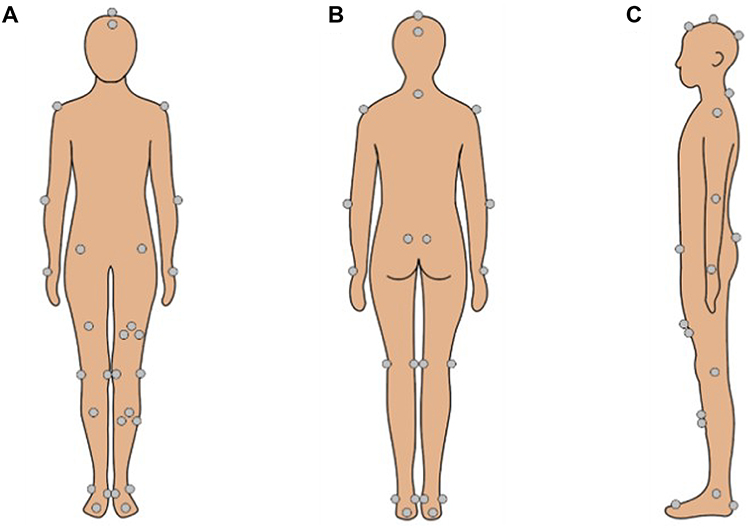 |
Figure 2 Positions of reflective markers. (A) Anterior surface, (B) posterior surface, and (C) lateral surface. |
Healthy participants were instructed to walk four times along a flat 10 m walking path in the laboratory for measurements. Patients with knee OA were instructed to walk along the same walkway under two conditions: four times while wearing the measurement knee orthosis and four times without it, for a total of eight trials. Measurements were performed under both conditions.
To facilitate acclimation to the knee orthosis, a 5-min practice period was provided prior to the measurement trials. Before initiating gait measurement, the medial and lateral markers on the left knee joint were removed to prevent interference with the orthosis. The data from the removed markers were compensated using baseline static standing posture. The corrective moment exerted by the knee orthosis during gait in patients with knee OA was measured in real time using a Leptrino six-axis force sensor integrated into the orthosis. Prior to measurements, the initial value was set to 0 Nm by recording data during a period when the measurement orthosis was not worn by the participant.
Data Analysis
Kinematic and kinetic data were processed using Visual3D software (version 3.6, C-Motion, Germantown, MD, USA). The raw marker data collected from the participants were filtered using a low-pass Butterworth filter with a cutoff frequency of 6 Hz. Similarly, raw data obtained from the ground reaction force and Leptrino six-axis force sensor embedded in the knee orthosis measurement system were filtered using a low-pass Butterworth filter with a cutoff frequency of 15 Hz. All gait data were time-normalized to 100% of the stance phase before further analyses. Knee joint moments and gait performance metrics, including walking speed and stride length, were subsequently calculated. Both knee joint moments and the corrective moment exerted by the knee orthosis derived from the six-axis force sensor were normalized to the participants’ body weight. For the analysis, data were extracted with a focus on the stance phase of gait, during which substantial mechanical stress was applied to the knee joint.
Based on the vertical component of the ground reaction force, the stance phase of the gait cycle was divided into three phases: loading response, mid and terminal stance, and pre-swing. The loading response was defined as the interval from the initial contact of the affected left lower limb to the toe-off of the contralateral right limb. The mid and terminal stance phase was defined as the period from the toe-off to the subsequent initial contact of the unaffected right lower limb. The pre-swing phase was defined as the interval from initial contact of the unaffected right lower limb to the toe-off of the affected left lower limb. The same data collection protocol was applied to healthy participants, with the left lower limb designated as the reference for phase definitions, consistent with the affected side in patients with knee OA.
To determine whether EKAM value depended on the use of a knee orthosis in patients with knee OA, the integral value of EKAM during the stance phase was calculated for each scenario. Additionally, to compare EKAM values in healthy participants with those in patients with knee OA under both orthosis and no-orthosis conditions, the same integration procedure was applied. Furthermore, gait parameters indicating spatiotemporal characteristics, namely walking speed and stride length, were calculated for each participant. Finally, the integral value of the valgus corrective moment generated by the knee orthosis was computed.
Statistical Analysis
The normality of each parameter was assessed using the Shapiro–Wilk test, with a p-value of < 0.05 indicating a significant deviation from normal distribution. Parametric statistical methods were applied when the assumption of normality was met; otherwise, nonparametric methods were used.
Before the main analysis, we examined group differences in demographic variables, including age, sex, height, and weight. For the categorical variable of sex, the χ2-test was conducted after confirming that the expected cell frequencies satisfied test assumptions. As age, height, and weight data satisfied the normality assumption, between-group comparisons for these variables were performed using the t-test for independent samples.
EKAM values obtained with and without the orthosis in both healthy participants and patients with knee OA were analyzed using the integral values for the affected left lower limb obtained from each gait cycle in the four walking trials. EKAM values for patients with knee OA were compared between the orthosis and no-orthosis conditions using the Wilcoxon signed-rank test. Next, differences in EKAM values under both conditions between patients with knee OA and healthy participants were evaluated using the Mann–Whitney U-test. Furthermore, gait parameters, including gait speed and stride length, were evaluated and compared between the orthosis and no-orthosis conditions in patients with knee OA using the Wilcoxon signed-rank test. Comparisons between the OA patients (with and without the orthosis) and healthy participants were performed using the Mann–Whitney U-test.
Effect sizes (r, based on z-scores: r = z/√n) were calculated for the Mann–Whitney U and Wilcoxon signed-rank tests and interpreted according to Cohen’s criteria (small: 0.10–0.29, medium: 0.30–0.49, large: ≥0.50).32 To address the potential issue of type I error inflation associated with multiple comparisons across stance sub-phases, the Holm’s correction was applied to post hoc analyses within the stance-phase subdivisions (loading response, mid and terminal stance, and pre-swing). The main analysis focused on the entire stance phase without the correction, whereas Holm-adjusted p-values were used for the sub-phase analyses. Although multiple statistical tests were conducted, each comparison addressed a distinct analytical objective. To minimize type I error inflation, the application of the Holm’s correction ensured that the analyses did not involve uncontrolled multiple testing.
All statistical analyses were conducted using SPSS Statistics version 27 (International Business Machines Corp., Armonk, NY, USA) and Python (version 3.11; https://www.python.org). Differences were considered statistically significant if the null hypothesis could be rejected at the 0.05 probability level.
Results
Participants and Gait Performance
Table 1 presents baseline characteristics of the participants, including age, sex, height, weight, and the KL grade for patients with knee OA, as well as walking speed and stride length. No significant differences were observed in age, sex distribution, height, weight, walking speed, or stride length between patients with knee OA and healthy participants (p > 0.05). Within the OA group, walking speed and stride length were comparable between trials with and without the orthosis (p > 0.05). These results confirm that the orthosis did not alter walking speed or stride length, ensuring that any changes in EKAM would reflect the mechanical effect of the orthosis rather than differences in walking conditions.
Effect of the Orthosis on EKAM in Patients with Knee OA
Figure 3 illustrates the time-normalized EKAM during the stance phase in the left lower limb of patients with OA and healthy participants. EKAM in patients with OA was significantly higher than that in healthy participants (p < 0.05), regardless of orthosis use. Wearing the orthosis reduced EKAM, reflecting the valgus corrective moment generated by the orthosis. However, even after the reduction, EKAM remained above the levels observed in healthy participants, suggesting partial mechanical unloading rather than complete normalization.
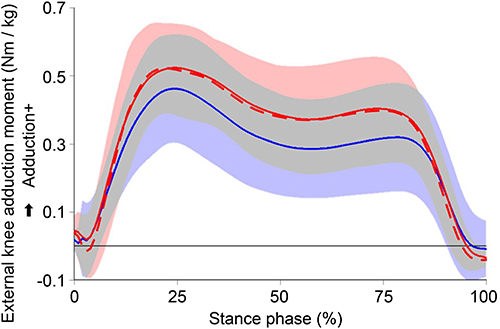 |
Figure 3 External knee adduction moment during the stance phase in patients with knee osteoarthritis (with and without an orthosis) and healthy controls. Solid red line: patients with orthosis; dashed red line: patients without orthosis; solid blue line: healthy participants. |
Table 2 presents the integrated EKAM values for the entire stance phase under the orthosis and no-orthosis conditions. The mean EKAM during the stance phase decreased by 2.6% with orthosis use; however, this reduction was not statistically significant (Wilcoxon signed-rank test, p > 0.05). Importantly, during the loading response, EKAM was significantly reduced by 11.8% (p < 0.05).
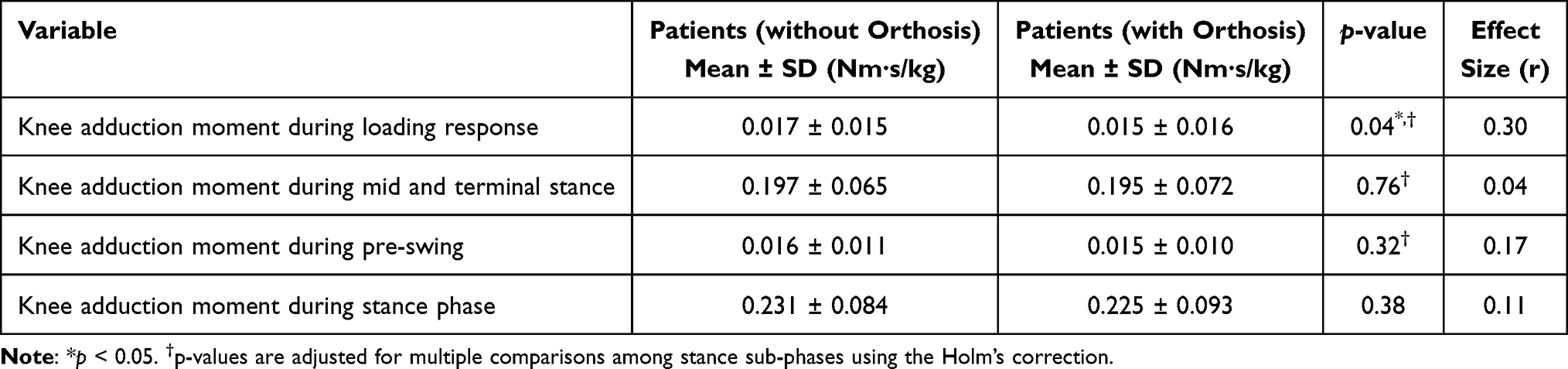 |
Table 2 Comparison of External Knee Adduction Moment Values in Patients with Osteoarthritis with and without a Knee Orthosis |
The effect size indicated a moderate effect (r = 0.30), suggesting that the orthosis effectively reduced medial knee loading during the early stance phase. In contrast, the reductions observed during the mid and terminal stance (1.0%) and pre-swing (6.3%) phases were not statistically significant (p > 0.05).
Table 3 compares the integrated EKAM values between patients with OA (without orthosis) and healthy participants. Without orthotic assistance, patients with OA showed significantly higher integrated EKAM throughout the entire stance phase and in all sub-phases (p < 0.05). Table 4 compares the integrated EKAM values between patients with OA (with orthosis) and healthy participants. Wearing the orthosis reduced the integrated EKAM during the loading response and pre-swing phases to levels comparable to those in healthy participants, whereas significant differences persisted during mid- and terminal stance and overall stance (p < 0.05), indicating that the corrective effect of the orthosis was phase-specific and primarily limited to the early stance and late transition phases of gait.
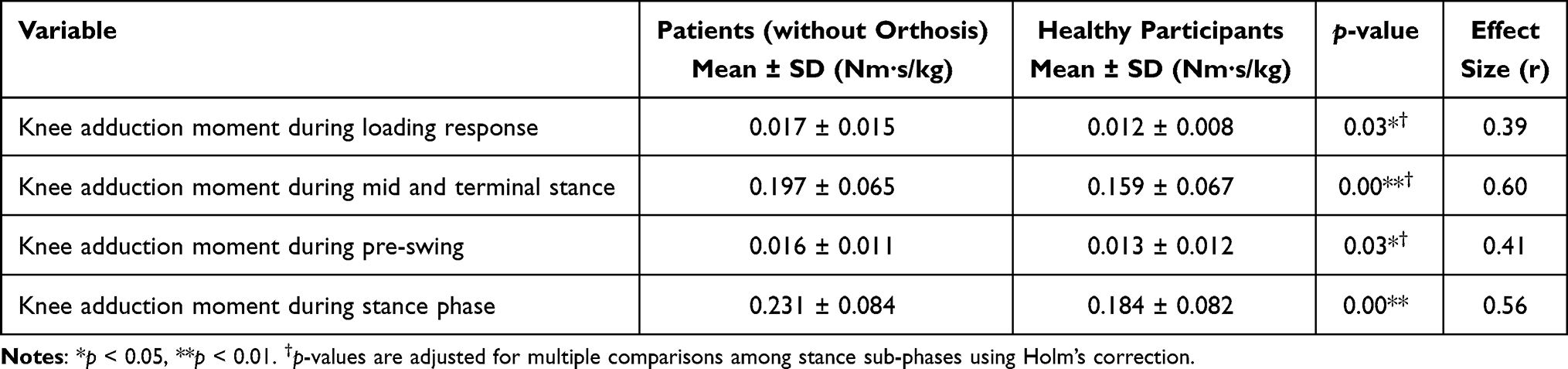 |
Table 3 Comparison of External Knee Adduction Moment in Patients with Knee Osteoarthritis without an Orthosis and Healthy Individuals |
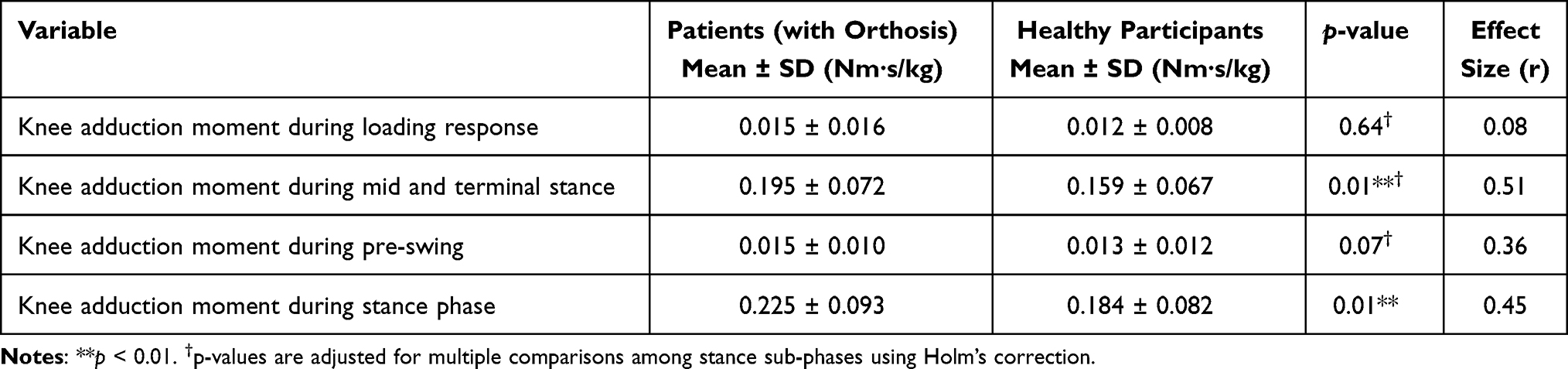 |
Table 4 Comparison of External Knee Adduction Moment in Patients with Knee Osteoarthritis with an Orthosis and Healthy Individuals |
Direct Quantification of the Valgus Corrective Moment Using a Six-Axis Force/Torque Sensor-Embedded Knee Orthosis
Figure 4 illustrates the valgus corrective moment generated by the knee orthosis during the stance phase in the left leg of patients with knee OA. The orthosis consistently produced a valgus corrective moment throughout all stance sub-phases — loading response, mid and terminal stance, and pre-swing — causing abduction of the shank relative to the thigh and reflecting the intended corrective function. Quantitative analysis showed that this corrective moment peaked during the mid and terminal stance phases, with an average magnitude of 0.0088 ± 0.0074 Nm·s/kg (Table 5). This finding indicates that the orthosis provided the greatest valgus corrective assistance, particularly during the mid and terminal stance phases. In contrast, the integrated EKAM during the entire stance phase was 0.184 ± 0.082 Nm·s/kg in healthy participants, but 0.231 ± 0.084 Nm·s/kg in patients with knee OA without the orthosis. These findings suggest that the valgus corrective moment generated by the orthosis alone, with an average magnitude of 0.0088 ± 0.0074 Nm·s/kg, was insufficient to reduce EKAM during gait in patients with knee OA to the level observed in healthy individuals.
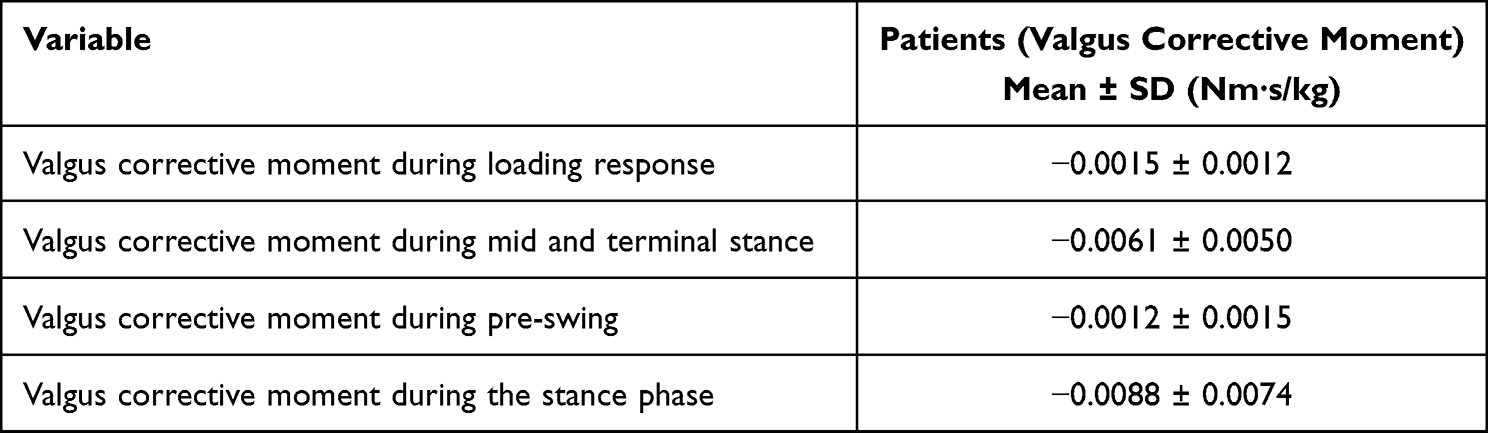 |
Table 5 Integrated Valgus Corrective Moment Generated by the Knee Orthosis in Patients with Knee Osteoarthritis |
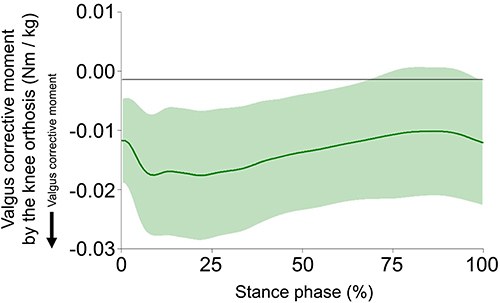 |
Figure 4 Valgus corrective moment generated by the knee orthosis during the stance phase. A positive value (“+”) indicates an orthosis-generated corrective moment acting to adduct the shank relative to the thigh, whereas a negative value (“−”) represents a moment acting to abduct the shank relative to the thigh. |
Discussion
In this study, we examined the biomechanical effects of a center bridge-type knee orthosis prescribed for patients with knee OA using real-time, direct quantification of EKAM. The main finding of this study is as follows: to reduce EKAM in patients with knee OA to a level comparable to that of healthy individuals, the corrective moment produced by the current center bridge-type knee orthosis would need to be increased by approximately 5.34 times, which provides a quantitative indicator.
In this study, we established and tested two hypotheses based on previous reports that knee orthosis reduces EKAM by approximately 10–13%.18,24 The first hypothesis proposed that wearing a knee orthosis would generate a valgus corrective moment and thereby decrease EKAM. The second hypothesis purported that to achieve an EKAM value comparable to that of healthy individuals, patients with knee OA would require a stronger valgus corrective moment than that generated by existing knee orthoses. The results partially supported both hypotheses: a significant reduction in EKAM during the loading response and a trend toward healthy levels during the pre-swing phase were observed when the orthosis was worn.
Before testing these hypotheses, we confirmed that no significant differences were observed in gait speed and stride length either between the orthosis and no-orthosis conditions in patients with knee OA, or between patients with OA and healthy participants.
Although patients with knee OA have been reported to generally exhibit slower gait speed and shorter stride length than healthy individuals,33 this pattern was not observed in this present study: patients with knee OA were recruited based on the criteria that they were able to walk independently indoors without a walking stick and capable of visiting the hospital. In addition, age-matched healthy adults were recruited as the control group. Furthermore, most patients with knee OA included in this study had mild to moderate symptoms, without marked gait impairment. Consequently, no significant differences in gait speed or stride length were observed between patients with knee OA and healthy participants, thereby minimizing potential confounding influence of gait speed and stride length on the comparison of EKAM.
In validating the first hypothesis, the reduction in EKAM observed during the loading response is considered to result from the floor reaction force vector passing medial to the knee joint center, thereby increasing the moment arm relative to the medial lower leg strut of the orthosis structure. This enabled the valgus corrective moment generated by the orthosis to act effectively.23,34 These results are also consistent with previous findings. For instance, a study reported that the use of a knee orthosis reduced EKAM by approximately 7% in the early stance phase, demonstrating effective valgus corrective assistance.35 Furthermore, the moderate effect size associated with the reduction in EKAM with orthosis observed in this study indicates that its effectiveness was not only statistically significant but also clinically meaningful.
Regarding the second hypothesis, when knee OA patients wore the knee orthosis, EKAM was reduced to a level comparable to that of healthy participants during the loading response and pre-swing phases, whereas in the mid and terminal stance phases, EKAM remained higher than that in healthy participants.
EKAM approached the level comparable to that of healthy participants during pre-swing likely because as the knee flexes and the load shifts toward the forefoot, the ground reaction force decreases and its line of action approaches the center of the knee joint, which biomechanically contributes to a natural reduction in EKAM. Moreover, because knee flexion increases the moment arm between the medial strut of the orthosis and the ground reaction force vector, the valgus corrective moment generated by the orthosis can be more effectively transmitted. These biomechanical conditions are considered to have contributed to the increased corrective effect of the orthosis during pre-swing, resulting in a reduction in EKAM to a level comparable to that of healthy participants, consistent with previous findings.36
In validating the first hypothesis, no statistically significant difference in EKAM was observed between the orthosis and no-orthosis conditions during the pre-swing phase within the OA group. Although knee flexion increases and the center of pressure shifts anteriorly during pre-swing, creating favorable mechanical conditions for transmitting the corrective moment generated by the orthosis, individual differences in lower limb alignment and gait strategies among knee OA patients likely caused variability in orthotic effects, resulting in the absence of statistically significant differences.
During the mid and terminal stance phases, knee extension predominates, and the line of action of the ground reaction force continues to pass medial to the knee joint center, making it difficult to maintain a sufficient moment arm for the orthosis to effectively exert valgus corrective moment. Consequently, although the integrated valgus corrective moment directly measured in this study was relatively large in the mid and terminal stance compared with that during other phases, EKAM in these phases remained higher than that in other phases, implying that the corrective moment was relatively small. The between-group difference in EKAM therefore persisted. These results are consistent with the findings of previous phantom model experiments, which indicated that the corrective force generated by current knee orthoses is insufficient, thus supporting the validity of the present findings.22
In many previous studies, the effects of knee orthoses have been evaluated using inverse dynamics based on gait analysis. This approach makes it difficult to determine whether the reduction in EKAM reflects the direct effect of the orthosis itself or is due to changes in lower limb alignment or gait patterns induced by the orthosis. To overcome these limitations, attempts have been made to directly quantify the corrective force generated by knee orthoses. For example, some studies estimated the valgus moment by attaching strain gauges to the medial strut of the orthosis,18 and others measured the orthosis moment throughout the gait cycle using pressure sensors attached to the medial side of the lower leg.21 However, when estimating the total corrective moment produced by the orthosis based on these methods, which only capture partial load measurements from strain gauges or pressure sensors, measurement accuracy and reliability are limited, because the contact between the orthosis and the body is not fully controlled. Therefore, to avoid uncertainty in contact conditions, a previous study incorporated sensors capable of simultaneously measuring three-axis forces and moments into a double-strut knee orthosis.25 However, that study examined the assistive effects of the orthosis during a jumping task in five healthy participants, and its purpose differed from that of the present study, which focused on changes during normal walking.
Based on these considerations, in the present study, we achieved real-time quantification of the valgus corrective moment exerted during walking using a knee orthosis equipped with a six-axis force/torque sensor. The novelty of this study lies in the demonstration of the quantitative magnitude of the corrective moment required to reduce EKAM in patients with knee OA to the level of healthy individuals. In addition, the results showed that the corrective force generation was relatively insufficient during mid and terminal stance, providing specific implications for improving future orthosis design. These findings not only contribute to clarifying the mechanism underlying orthosis effects but also offer evidence-based guidance for future orthosis development.
This study has some limitations. First, although the sample size was calculated using G*Power, this was a pilot study, and the number of participants was insufficient to fully reflect individual differences in the valgus corrective moment and EKAM generated by the orthosis. To obtain more precise and generalizable results, future studies with a larger sample size are required. Second, only one type of center bridge knee orthosis was investigated in this study, and comparisons with other orthotic designs were not conducted. In addition, the orthosis used in this study was modified for measurement purposes and was approximately 293 g heavier than orthoses prescribed clinically. Although the sensors and related components were positioned near the orthotic frame to minimize inertia effects during walking, some influence of the increased weight cannot be eliminated. Therefore, future research should compare the characteristics of corrective moment generation among multiple orthosis designs and examine lighter structures that more closely replicate clinical orthoses. Finally, this study employed a short-term experimental design and did not account for long-term adaptation to orthosis use or changes in gait patterns over time. Evaluating how gait dynamics and knee joint load distribution evolve with long-term orthosis use would provide a more comprehensive understanding of the clinical efficacy and practicality of the orthosis.
Conclusion
This study demonstrated that the use of a center bridge-type knee orthosis effectively reduced the EKAM during the loading response in patients with medial knee OA. Wearing the orthosis enabled patients to achieve EKAM values comparable to those of healthy individuals during the loading response and pre-swing, whereas EKAM during the mid- and terminal stance remained significantly higher than that in healthy individuals, indicating that the corrective moment provided by the current orthosis was insufficient. Quantitative analyses further revealed that, to reduce EKAM to a level equivalent to that of healthy individuals throughout the stance phase, the valgus corrective moment generated by the orthosis would need to be increased by approximately 5.34 times. These findings may serve as valuable indicators for clinicians and orthotists in establishing appropriate corrective force settings in knee orthosis design. Future improvements in structural design that allow selective generation of corrective torque at the required phases of gait could contribute to improved load distribution and knee joint biomechanics. Such selective torque generation may also reduce discomfort and pain associated with excessive corrective forces. Therefore, future research should focus on optimizing orthosis design to balance mechanical effectiveness and user comfort.
Abbreviations
EKAM, external knee adduction moment; KL, Kellgren–Lawrence; OA, osteoarthritis; RO, rated output.
Data Sharing Statement
The data for the participants were obtained under the precondition that no personally identifiable information would be disclosed. Therefore, only anonymized datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request, and any data that could potentially compromise participant privacy cannot be shared for ethical reasons.
Ethics Approval and Informed Consent
This experiment was conducted with the approval of the Research Ethics Committee of the Graduate School of Life Design, Toyo University (approval Nos: 2023-A14 and 2024-A6S). All measurements were performed after obtaining written informed consent.
Acknowledgments
We are grateful to Tamotsu Sakima (Chairman) and Ichiro Sakima (President) of Sakima Prosthetics and Orthotics Co. for providing materials to develop the knee orthosis measurement system used in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by JSPS KAKENHI (grant number: JP22K11350) and partly funded by the Precise Measurement Technology Promotion Foundation. The funders had no role in the design, conduct, or reporting of the study.
Disclosure
The center bridge knee orthosis was provided by Sakima Prosthetics and Orthotics Co., Japan. J.K. received research grants from JSPS KAKENHI. J.K. is an advisor and shareholder (unlisted) of Trunk Solution Co., Ltd., obtains patent royalties, and and reports non-financial support from Inter Reha Co., Ltd., during the conduct of the study. Trunk Solution Co. Ltd. was not included in this study. The authors report no other conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–13. doi:10.1016/S0140-6736(20)30925-9
2. Muraki S, Oka H, Akune T, et al. Prevalence of radiographic knee osteoarthritis and its association with knee pain in the elderly of Japanese population-based cohorts: the ROAD study. Osteoarthr Cartil. 2009;17(9):1137–1143. doi:10.1016/j.joca.2009.04.005
3. Yoshimura N, Muraki S, Oka H, et al. Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab. 2009;27(5):620–628. doi:10.1007/s00774-009-0080-8
4. Knecht S, Vanwanseele B, Stüssi E. A review on the mechanical quality of articular cartilage — implications for the diagnosis of osteoarthritis. Clin Biomech. 2006;21(10):999–1012. doi:10.1016/j.clinbiomech.2006.07.001
5. Englund M. The role of biomechanics in the initiation and progression of OA of the knee. Best Pract Res Clin Rheumatol. 2010;24(1):39–46. doi:10.1016/j.berh.2009.08.008
6. American Academy of Orthopaedic Surgeons. Management of osteoarthritis of the knee (non-arthroplasty) evidence-based clinical practice guideline; 2021. Available from: https://www.aaos.org/oak3cpg.
7. Lim WB, Al-Dadah O. Conservative treatment of knee osteoarthritis: a review of the literature. World J Orthop. 2022;13(3):212–229. doi:10.5312/wjo.v13.i3.212
8. Onu I, Matei D, Sardaru DP, et al. Rehabilitation of patients with moderate knee osteoarthritis using hyaluronic acid viscosupplementation and physiotherapy. Appl Sci. 2022;12(6):3165. doi:10.3390/app12063165
9. Baker PN, van der Meulen JH, Lewsey J, Gregg PJ. National joint registry for England and Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the national joint registry for England and Wales. J Bone Joint Surg Br. 2007;89(7):893–900. doi:10.1302/0301-620X.89B7.19091
10. Rissolio L, Sabatini L, Risitano S, et al. Is it the surgeon, the patient, or the device? A comprehensive clinical and radiological evaluation of factors influencing patient satisfaction in 648 total knee arthroplasties. J Clin Med. 2021;10(12):2599. doi:10.3390/jcm10122599
11. Vessely MB, Whaley AL, Harmsen WS, Schleck CD, Berry DJ. The Chitranjan Ranawat Award: long-term survivorship and failure modes of 1000 cemented condylar total knee arthroplasties. Clin Orthop Relat Res. 2006;452:28–34. doi:10.1097/01.blo.0000229356.81749.11
12. Fang DM, Ritter MA, Davis KE. Coronal alignment in total knee arthroplasty: just how important is it? J Arthroplasty. 2009;24(6):39–43. doi:10.1016/j.arth.2009.04.034
13. Ritter MA, Davis KE, Davis P, et al. Preoperative malalignment increases risk of failure after total knee arthroplasty. J Bone Joint Surg Am. 2013;95(2):126–131. doi:10.2106/JBJS.K.00607
14. Bennell KL, Bowles KA, Wang Y, Cicuttini F, Davies-Tuck M, Hinman RS. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Ann Rheum Dis. 2011;70(10):1770–1774. doi:10.1136/ard.2010.147082
15. Nakajima A, Murata K, Morishita Y, Kokubun T, Oka Y, Kanemura N. Improvement in joint instability reduces inflammatory pain of early knee osteoarthritis. Ann Phys Rehabil Med. 2018;
16. Takahashi I, Takeda K, Matsuzaki T, Kuroki H, Hoso M. Reduction of knee joint load suppresses cartilage degeneration, osteophyte formation, and synovitis in early-stage osteoarthritis using a post-traumatic rat model. PLoS One. 2021;16(7):e0254383. doi:10.1371/journal.pone.0254383
17. Lindenfeld TN, Hewett TE, Andriacchi TP. Joint loading with valgus bracing in patients with varus gonarthrosis. Clin Orthop Relat Res. 1997;344:290–297. doi:10.1097/00003086-199711000-00029
18. Pollo FE, Otis JC, Backus SI, Warren RF, Wickiewicz TL. Reduction of medial compartment loads with valgus bracing of the osteoarthritic knee. Am J Sports Med. 2002;30(3):414–421. doi:10.1177/03635465020300031801
19. Gaasbeek RDA, Groen BE, Hampsink B, van Heerwaarden RJ, Duysens J. Valgus bracing in patients with medial compartment osteoarthritis of the knee. A gait analysis study of a new brace. Gait Posture. 2007;26(1):3–10. doi:10.1016/j.gaitpost.2006.07.007
20. Fantini Pagani CH, Potthast W, Brüggemann GP. The effect of valgus bracing on the knee adduction moment during gait and running in male subjects with varus alignment. Clin Biomech. 2010;25(1):70–76. doi:10.1016/j.clinbiomech.2009.08.010
21. Cusin E, Honeine JL, Schieppati M, Rougier PR. A simple method for measuring the changeable mechanical action of unloader knee braces for osteoarthritis. IRBM. 2018;39(2):136–142. doi:10.1016/j.irbm.2018.02.003
22. Kon K, Fukushi K, Tsuji T, Sato K. Comparison of corrective forces of knee orthoses for osteoarthritis. J Jpn Acad Prosthetists Orthotists. 2021;29(2):107–114. doi:10.32193/jjapo.29.2_107
23. Nakano K, Mine Y, Katsuhira J, Sakima T. Measuring the load acting on a knee brace of Center bridge type during walking. J Life Support Eng. 2022;34(4):129–135. doi:10.5136/lifesupport.34.129
24. Schmalz T, Knopf E, Drewitz H, Blumentritt S. Analysis of biomechanical effectiveness of valgus-inducing knee brace for osteoarthritis of knee. J Rehabil Res Dev. 2010;47(5):419–429. doi:10.1682/jrrd.2009.05.0067
25. Lee H, Ha D, Kang YS, Park HS. Biomechanical analysis of the effects of bilateral hinged knee bracing. Front Bioeng Biotechnol. 2016;4:50. doi:10.3389/fbioe.2016.00050
26. Moyer R, Birmingham T, Dombroski C, Walsh R, Giffin JR. Combined versus individual effects of a valgus knee brace and lateral wedge foot orthotic during stair use in patients with knee osteoarthritis. Gait Posture. 2017;54:160–166. doi:10.1016/j.gaitpost.2017.02.030
27. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
28. Moyer RF, Birmingham TB, Dombroski CE, et al. Combined effects of a valgus knee brace and lateral wedge foot orthotic on the external knee adduction moment in patients with varus gonarthrosis. Arch Phys Med Rehabil. 2013;94(1):103–112. doi:10.1016/j.apmr.2012.09.004
29. Robbins SM, Astephen Wilson JL, Rutherford DJ, Hubley-Kozey CL. Reliability of principal components and discrete parameters of knee angle and moment gait waveforms in individuals with moderate knee osteoarthritis. Gait Posture. 2013;38(3):421–427. doi:10.1016/j.gaitpost.2013.01.001
30. Robert-Lachaine X, Dessery Y, Belzile ÉL, Corbeil P. Knee braces and foot orthoses multimodal 3-month treatment of medial knee osteoarthritis in a randomised crossover trial. Knee Surg Sports Traumatol Arthrosc. 2024;32(11):2919–2930. doi:10.1002/ksa.12312
31. Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Stat. 2005;4(4):287–291. doi:10.1002/pst.185
32. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
33. Boekesteijn RJ, van Gerven J, Geurts ACH, Smulders K. Objective gait assessment in individuals with knee osteoarthritis using inertial sensors: a systematic review and meta-analysis. Gait Posture. 2022;98:109–120. doi:10.1016/j.gaitpost.2022.09.002
34. Shelburne KB, Torry MR, Steadman JR, Pandy MG. Effects of foot orthoses and valgus bracing on the knee adduction moment and medial joint load during gait. Clin Biomech. 2008;23(6):814–821. doi:10.1016/j.clinbiomech.2008.03.004
35. Jones RK, Nester CJ, Richards JD, et al. A comparison of the biomechanical effects of valgus knee braces and lateral wedged insoles in patients with knee osteoarthritis. Gait Posture. 2013;37(3):368–372. doi:10.1016/j.gaitpost.2012.08.002
36. Fantini Pagani CH, Hinrichs M, Brüggemann GP. Kinetic and kinematic changes with the use of valgus knee brace and lateral wedge insoles in patients with medial knee osteoarthritis. J Orthop Res. 2012;30(7):1125–1132. doi:10.1002/jor.22031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.