Back to Journals » Drug Design, Development and Therapy » Volume 20
Effect of Remimazolam on Postoperative Cough in Patients Undergoing Thyroid Surgery: A Randomized Double-Blind Controlled Clinical Trial
Authors Liu X, Zhang T, Zhao L ![]() , Zhou X, Zhang L, Mao W, Chen L, Xie Y, Li L
, Zhou X, Zhang L, Mao W, Chen L, Xie Y, Li L
Received 19 October 2025
Accepted for publication 5 February 2026
Published 13 February 2026 Volume 2026:20 575369
DOI https://doi.org/10.2147/DDDT.S575369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Xianchun Liu, Ting Zhang, Li Zhao, Xuelei Zhou, Longyi Zhang, Wei Mao, Linlin Chen, Ying Xie, Linji Li
Department of Anesthesiology, Beijing Anzhen Hospital, Capital Medical University, Nanchong Branch, The Second Clinical Medical College of North Sichuan Medical College, Nanchong, People’s Republic of China
Correspondence: Linji Li, Email [email protected]
Purpose: This study aimed to evaluate the inhibitory effect of remimazolam on coughing during emergence from general anesthesia in patients undergoing thyroid surgery.
Methods: Sixty-eight patients were randomly assigned to two groups (n = 34 each). After anesthesia induction, the remimazolam group (R group) received a continuous infusion of 0.4 mg/kg/h remimazolam, while the control group (C group) received an equal volume of saline until the end of surgery. Both groups were maintained with remifentanil and sevoflurane. The incidence and severity of coughing during emergence, awakening time, extubation time, and sedation scores were recorded. Heart rate and mean arterial pressure were measured at five time points: admission (T0), 2 min before intubation (T1), 2 min after intubation (T2), end of surgery (T3), and extubation (T4). Adverse events were also documented.
Results: The incidence of coughing was significantly lower in the R group (38.24%) than in the C group (76.47%) (risk difference [RD], − 38.2%; 95% CI, − 59.9% to − 16.6%; relative risk [RR], 0.50; 95% CI, 0.30– 0.82; P < 0.005). Moderate to severe coughing occurred less frequently in the R group (14.71% vs 35.29%, P = 0.029), and overall coughing severity was lower (P < 0.001). Awakening and extubation times were longer in the R group (P < 0.0001), and sedation scores were higher at response and extubation (P < 0.0001, P = 0.002). Heart rate and mean arterial pressure decreased in both groups without significant intergroup differences.
Conclusion: Remimazolam significantly reduces the incidence of coughing during emergence from general anesthesia in thyroid surgery.
Keywords: remimazolam, thyroid surgery, emergence phase of general anesthesia, coughing
Background
Reports estimate that cough may occur in 76%–98% of patients during extubation and the immediate awakening period.1–3 Coughing during the extubation phase increases the risk of postoperative bleeding in thyroid surgery. Once bleeding occurs postoperatively, it can lead to tracheal compression and suffocation, making it a severe and life-threatening complication after thyroidectomy.4 In recent years, specialized endotracheal tubes have been widely used in thyroid surgery for recurrent laryngeal nerve monitoring to reduce the risk of perioperative nerve injury; however, these tubes are characterized by exposed monitoring electrode wires on their surface.5 During emergence, such structural features may result in increased irritation of the tracheal surface and vocal cords compared with conventional endotracheal tubes, thereby increasing the likelihood of coughing or poor tolerance. In addition, recurrent laryngeal nerve monitoring tubes with the same nominal internal diameter are generally thicker than regular tubes, and the use of local anesthetic gel for lubrication is contraindicated to avoid interference with nerve monitoring. Furthermore, thyroid surgery is typically performed in a supine position with neck extension, and intraoperative neck manipulation may cause slight displacement of the endotracheal tube, which has been associated with postoperative airway-related symptoms such as sore throat and hoarseness.6 Given these factors, identifying a simple, safe, and effective strategy to reduce coughing and improve tolerance during extubation, while preserving the reliability of recurrent laryngeal nerve monitoring, is of particular clinical importance in thyroid surgery.
Various pharmacological approaches, including opioids, dexmedetomidine, and lidocaine have been investigated to suppress emergence coughing, but their use may be limited by adverse effects such as respiratory depression, delayed recovery, or bradycardia.7–9 Remimazolam is a novel ultra–short-acting benzodiazepine that produces rapid-onset sedation with predictable recovery and minimal drug accumulation. As a positive allosteric modulator of the GABA-A receptor, it enhances inhibitory neurotransmission in the central nervous system. Because it is metabolized by non-specific tissue esterases, remimazolam enables precise titration of sedation depth and rapid emergence even after prolonged infusion.g thyroidectomy.10 Beyond its favorable pharmacokinetics, remimazolam may blunt airway reflexes during emergence. Benzodiazepine-mediated enhancement of GABAergic inhibition in brainstem reflex pathways can reduce cough sensitivity and attenuate sympathetic responses to tracheal stimulation. Clinical studies across different surgical settings have reported that remimazolam decreases emergence agitation and coughing and provides more stable hemodynamics compared with placebo or conventional anesthetics.11 In nasal surgery, intraoperative remimazolam infusion has been shown to reduce movement and coughing during tracheal extubation. In pediatric flexible bronchoscopy, remimazolam-based anesthesia effectively suppresses coughing and body movement while allowing prompt recovery.12,13 Furthermore, studies have shown that remimazolam has minimal impact on nerve stimulators and does not affect the effectiveness of recurrent laryngeal nerve monitoring.
Although remimazolam has shown benefits in improving hemodynamic stability and emergence quality in other surgical settings, it remains uncertain whether these advantages translate to patients undergoing thyroidectomy under sevoflurane-based anesthesia, where cough suppression and smooth extubation are particularly critical.Therefore, this randomized controlled trial aimed to evaluate whether remimazolam infusion during anesthesia maintenance could reduce the incidence and severity of coughing during emergence, while assessing its effects on recovery profiles, sedation characteristics, and adverse events in patients undergoing thyroidectomy.
Materials and Methods
Study Design
This randomized controlled trial has been approved by the Ethics Committee of Beijing Anzhen Hospital Nanchong Branch (Ethical Approval No.: 2025106) and has been registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR2500105311, Registration Date: July 1, 2025). All participants or their legally authorized representatives signed a written informed consent form prior to surgery. The study was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki.
Study Participants
Sample Size Calculation
This study is a parallel-design randomized double-blinded controlled trial. The initial sample size calculation was based on the report by Lee et al, which stated that the incidence of coughing in patients undergoing thyroidectomy under anesthesia maintenance with sevoflurane and remifentanil was as high as 91%.14 Based on a clinically relevant reduction of 40% in this incidence and an α level of 0.025, a total sample size of 56 was required to achieve 95% power. Considering a 20% dropout rate, the total sample size required for this study was 70, with 35 patients in each group. This study included 70 patients who underwent elective thyroidectomy under general anesthesia at Beijing Anzhen Hospital Nanchong Branch from July to August 2025.
Eligibility Criteria
Patients were eligible for inclusion if they met the following criteria: undergoing thyroid surgery under general anesthesia with endotracheal intubation, aged 18–65 years, classified as American Society of Anesthesiologists (ASA) physical status I–III, with a body mass index (BMI) between 18.5 and 30 kg m2, and having provided written informed consent to participate in this study.
Patients were excluded if they had acute heart failure, unstable angina, myocardial infarction within the past 6 months, or resting heart rate <50 beats/min; poorly controlled hypertension (systolic blood pressure ≥160 mmHg or diastolic blood pressure ≥100 mmHg); acute respiratory tract infection, acute exacerbation of chronic obstructive pulmonary disease (COPD), or poorly controlled asthma; end-stage renal failure or decompensated hepatic dysfunction; psychiatric disorders (schizophrenia, mania, bipolar disorder, or cognitive impairment); known allergy to benzodiazepines; use of benzodiazepines or history of general anesthesia within the past 3 months; pregnancy or lactation; refusal to participate by the patient or their legal guardian; or psychosocial problems or other conditions preventing cooperation.
Patients were withdrawn from the study if their surgical plan changed, if unexpected adverse events occurred, or if the surgical duration exceeded 3 hours or was shorter than 1 hour.
Randomization and Blinding
Seventy patients who met the eligibility criteria were randomly assigned into two equal groups using a random number table, with a 1:1 allocation ratio. The allocation results were prepared by an independent investigator and placed in sealed, opaque envelopes. After surgical confirmation, an anesthesia nurse who was not involved in patient management or data collection opened the envelope to determine group assignment and prepared the study drugs.
Patients in the remimazolam group (R group) received remimazolam at a dose of 0.4 mg/kg/h, while those in the control group (C group) received an equal volume of normal saline administered at the same infusion rate. The study drugs were prepared in identical syringes to ensure blinding.
Both the anesthesiologists responsible for intraoperative management and the patients were blinded to group allocation. Outcome measures, including coughing incidence, coughing severity, awakening time, extubation time, sedation scores, and hemodynamic parameters, were collected by a separate investigator who was also blinded to group assignment. The study was organized and supervised by the trial designers.
Methods
Standard Anesthesia Procedure
All patients fasted for 8 hours and abstained from drinking for 6 hours before surgery. Upon entering the operating room, intravenous access was established, and compound sodium chloride solution was infused at a rate of approximately 5 mL/kg/h. Standard monitoring was initiated, including electrocardiogram, pulse oximetry, heart rate, and blood pressure. Patients were placed in the supine position and received 100% oxygen via a face mask at a flow rate of 5 L/min.
During anesthesia induction, both groups received sufentanil 0.5 μg/kg, propofol 2.5 mg/kg, and cisatracurium 0.2 mg/kg, followed by endotracheal intubation with a specialized tube for recurrent laryngeal nerve monitoring under direct laryngoscopy. Electrode needles were inserted into the shoulder muscles and secured. After connection to the nerve monitoring device and confirmation of appropriate electrode positioning, the endotracheal tube was fixed. Mechanical ventilation was initiated with a tidal volume of 8–10 mL/kg, an inspiratory-to-expiratory ratio of 1:2, and a respiratory rate of 10–12 breaths/min. Ventilation parameters were adjusted intraoperatively to maintain end-tidal carbon dioxide (ETCO2) between 35 and 45 mmHg.
During the maintenance phase, both groups received remifentanil at 0.1–0.2 μg/(kg min) and sevoflurane at 1.5%–2% until the end of surgery. The intervention group received remimazolam at 0.4 mg/(kg h), while the control group received normal saline infusion. The bispectral index (BIS) was maintained between 40 and 60, and mean arterial pressure (MAP) fluctuations were kept within 20% of baseline values. When skin closure began, sevoflurane concentration was reduced to 0.5%. At the end of surgery, sevoflurane and remifentanil were discontinued, and the oxygen flow was increased to 6 L/min to accelerate elimination of sevoflurane until the minimum alveolar concentration (MAC) reached 0. No postoperative analgesic devices were used. All patients were transferred to the post-anesthesia care unit (PACU), and the specialized endotracheal tube for recurrent laryngeal nerve monitoring was removed once the patients opened their eyes in response to stimulation and recovered adequate spontaneous respiration.
If hemodynamic instability occurred intraoperatively, adjustments were made as follows: when systolic blood pressure (SBP) or diastolic blood pressure (DBP) increased by more than 30% from baseline, anesthetic depth was adjusted or urapidil was administered for blood pressure control. Hypotension, defined as a decrease of SBP or DBP >30% from baseline or an absolute blood pressure <85/50 mmHg, was treated with ephedrine or phenylephrine. If heart rate (HR) fell below 45 beats/min, atropine 0.2–0.5 mg was administered.
Outcome Measures
The primary outcome was the incidence of coughing within 5 minutes after extubation following discontinuation of sevoflurane.
Secondary outcomes included the severity of coughing, hemodynamic parameters, sedation level, postoperative sore throat, emergence characteristics, anesthetic consumption, and adverse events.The severity of coughing was assessed using a 4-point scale: 0 = no coughing; 1 = single cough; 2 = more than one episode of non-persistent coughing; 3 = persistent and repetitive coughing accompanied by head lifting. Coughing graded at level 2 or above was defined as moderate-to-severe coughing.15 Hemodynamic parameters, including heart rate and mean arterial pressure, were recorded at the following time points: T0, upon entering the operating room; T1, 2 minutes before intubation; T2, 2 minutes after intubation; T3, at the end of surgery; and T4, at extubation. Sedation level was assessed using the Ramsay Sedation Scale:16 1 = anxious, agitated, or both; 2 = awake, calm, and cooperative; 3 = drowsy, but responsive to commands; 4 = asleep, with a brisk response to loud auditory stimulus or light glabellar tap; 5 = asleep, with a sluggish response to loud auditory stimulus or glabellar tap; 6 = asleep, with no response. Assessments were performed when patients first opened their eyes or responded to stimulation, at extubation, and 5 minutes after extubation. Post-extubation sore throat was evaluated at 1 hour and 24 hours using a modified 4-point scale:17 Grade 1 = no sore throat; Grade 2 = mild sore throat (reported only when asked); Grade 3 = moderate sore throat (reported spontaneously by the patient); Grade 4 = severe sore throat (sore throat accompanied by voice change or hoarseness).
Additional recorded parameters included operation time, anesthesia duration, emergence time (defined as the time from discontinuation of sevoflurane or remimazolam to the first eye opening or execution of a simple command) extubation time (defined as the time from discontinuation of sevoflurane or remimazolam to removal of the endotracheal tube2), intraoperative remifentanil dosage, and adverse events (such as nausea and vomiting, hypotension, and bradycardia). In addition, demographic and clinical data were collected, including comorbidities, age, sex, BMI, and ASA classification. These data were used to evaluate the effects of anesthesia on patients’ vital signs and to explore their association with the incidence of adverse events.
Statistical Analysis
Statistical analyses were performed in SPSS (version 26.0, IBM, Armonk, NY, USA). Normality of continuous variables was assessed by the Shapiro–Wilk test. Continuous data are presented as mean ± SD or median (IQR), as appropriate; categorical data as counts (percentages). Between-group comparisons for single-time-point continuous outcomes used the independent-samples t test or Mann–Whitney U-test; categorical outcomes used the χ2-test or Fisher’s exact test.
For hemodynamic outcomes repeatedly measured across time points (heart rate [HR] and mean arterial pressure [MAP] at T0–T4), we conducted two-way repeated-measures ANOVA with time (within-subject factor: 5 levels, T0–T4) and group (between-subject factor: remimazolam vs control). Mauchly’s test assessed sphericity; when violated, Greenhouse–Geisser or Huynh–Feldt corrections were applied. Where omnibus tests were significant, Bonferroni-adjusted post-hoc comparisons (simple main effects) were performed across time within group and between groups at each time point. Effect sizes were summarized using partial eta-squared (ηp2) for ANOVA and risk ratios with 95% CIs for binary outcomes. A two-tailed p < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 76 patients were screened for eligibility, of whom 6 were excluded: 2 declined participation, 1 had poorly controlled asthma, 2 had systolic blood pressure exceeding 160 mmHg, and 1 had abnormal renal function. Ultimately, 70 patients were enrolled. During the study, 1 patient withdrew due to a change in surgical plan and 1 patient withdrew because the surgery lasted longer than 3 hours. Therefore, 68 patients completed the study (Figure 1). The baseline characteristics of the participants are presented in Table 1. No statistically significant differences were observed between the two groups in terms of age, sex, BMI, ASA classification, operation time, anesthesia duration, or intraoperative remifentanil dosage.
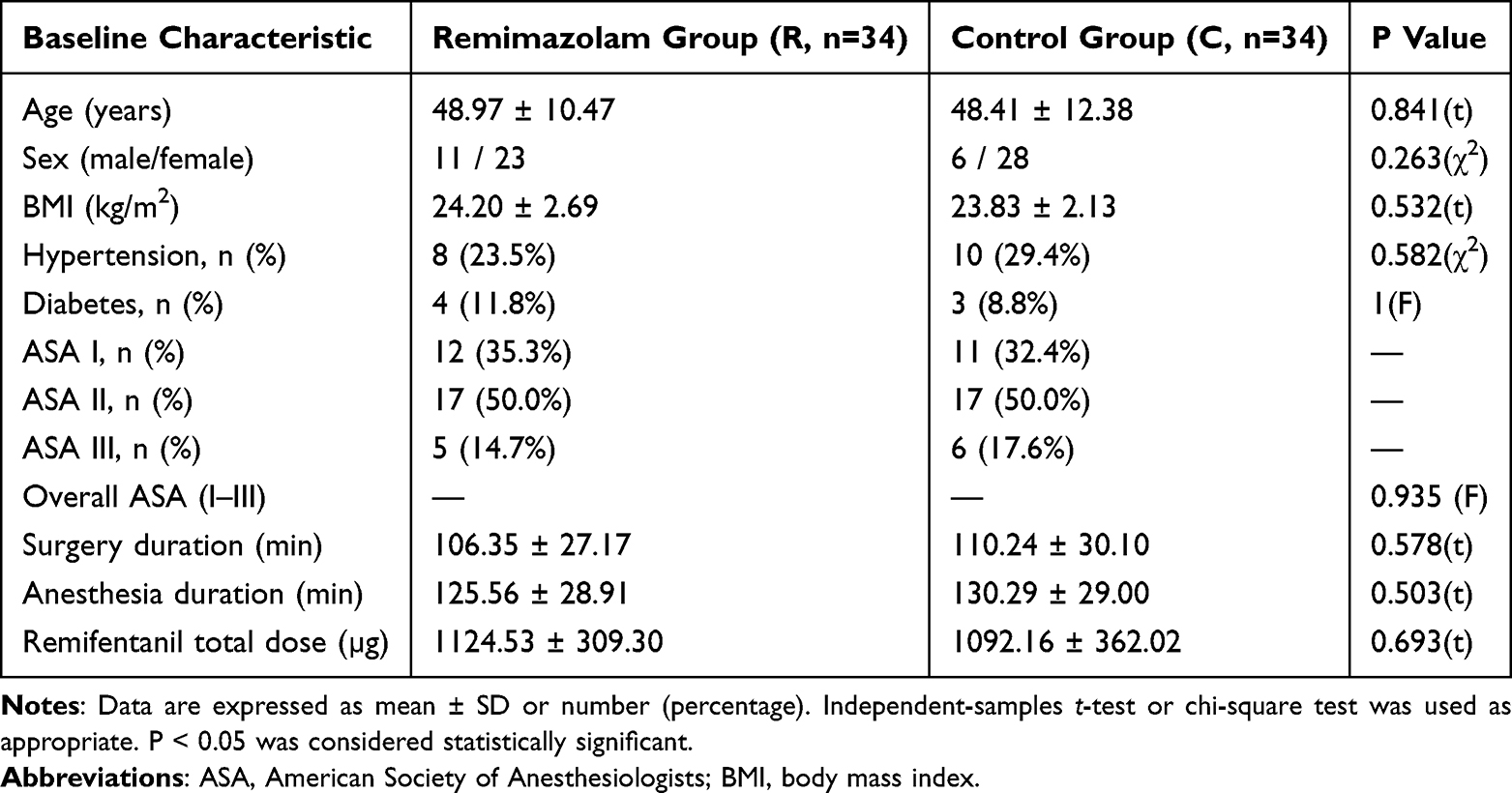 |
Table 1 Comparison of Baseline Characteristics Between the Two Groups |
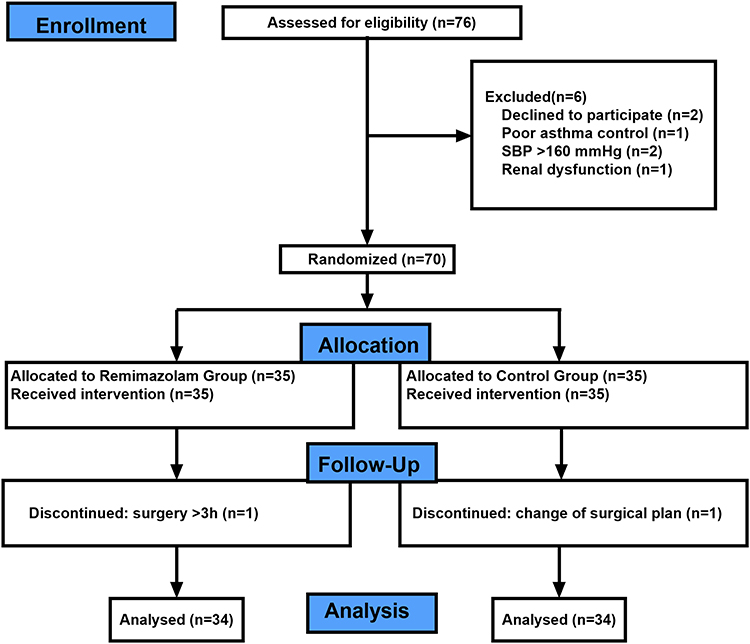 |
Figure 1 Participant Flow Diagram. |
Effect on Coughing
In this study, the incidence of coughing was 38.24% in the remimazolam group (R group), which was significantly lower than 76.47% in the control group (C group) (risk difference [RD], −38.2%; 95% CI, −59.9% to −16.6%; relative risk [RR], 0.50; 95% CI, 0.30–0.82; P < 0.005), indicating that remimazolam markedly reduced the risk of coughing during emergence from general anesthesia in patients undergoing thyroid surgery (Figure 2). Further analysis of cough severity showed that in the remimazolam group, 8 patients experienced mild coughing, 5 experienced moderate coughing, and none experienced severe coughing, whereas in the control group, the corresponding numbers were 14, 6, and 6, respectively. The total number of patients with moderate-to-severe coughing was significantly lower in the remimazolam group (5 cases) compared with the control group (12 cases, P = 0.029). The median (interquartile range) cough severity score was 0 (0–1) in the remimazolam group, significantly lower than 1 (0.75–2) in the control group (P = 0.001) (Figure 3 and Table 2). Comparisons by grade revealed significant differences between groups in the incidence of moderate coughing (P = 0.041) and severe coughing (P = 0.011), whereas no significant difference was observed in mild coughing (P = 0.162). Taken together, these findings demonstrate that remimazolam not only significantly reduced the overall incidence of coughing during emergence from general anesthesia in thyroid surgery but also effectively alleviated its severity.
 |
Table 2 Comparison of Cough Severity and Scores Between the Two Groups |
 |
Figure 2 Incidence of coughing during emergence in the two groups. The incidence of coughing was significantly lower in the remimazolam group (38.24%) than in the control group (76.47%) (P < 0.005). Data are expressed as percentages. |
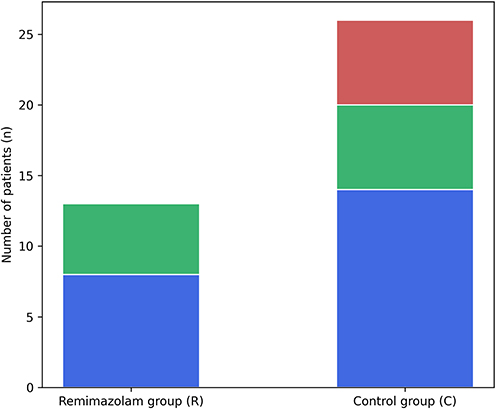 |
Figure 3 Severity distribution of coughing during emergence. Stacked bar chart showing the number of patients with mild, moderate, and severe coughing. The incidence of moderate-to-severe coughing was significantly lower in the remimazolam group (14.7%) than in the control group (35.3%) (P = 0.029). |
Hemodynamic Changes
For heart rate, there was a significant main effect of time (P < 0.001) and a significant group × time interaction (P = 0.029), indicating different heart rate change trends between the two groups.
For mean arterial pressure, there was a significant main effect of time (P < 0.001) and a significant group × time interaction (P = 0.016). Post hoc Bonferroni-adjusted tests revealed that MAP was significantly lower in the Remimazolam group than in the Control group at T2 and T4, while no significant differences were observed at other time points. Detailed hemodynamic parameters and trends at each time point are presented in Tables 3, 4 and Figure 4.
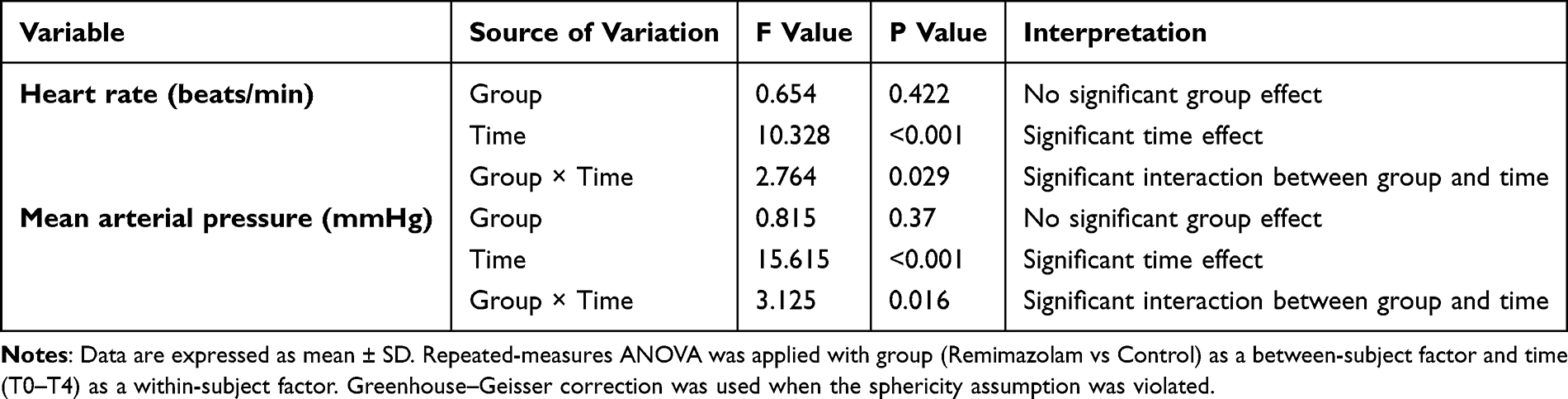 |
Table 3 Changes in Heart Rate and Mean Arterial Pressure Between the Two Groups Analyzed by Repeated-Measures ANOVA |
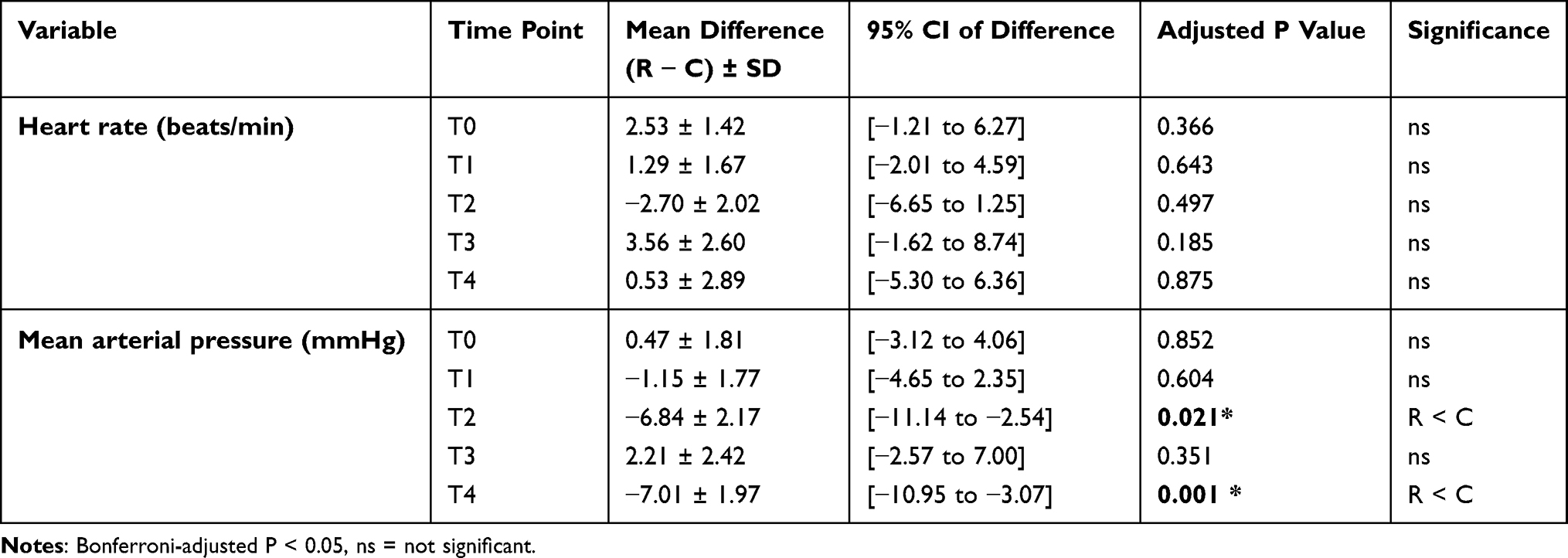 |
Table 4 Post Hoc Pairwise Comparisons (Bonferroni-Adjusted) for Heart Rate and Mean Arterial Pressure |
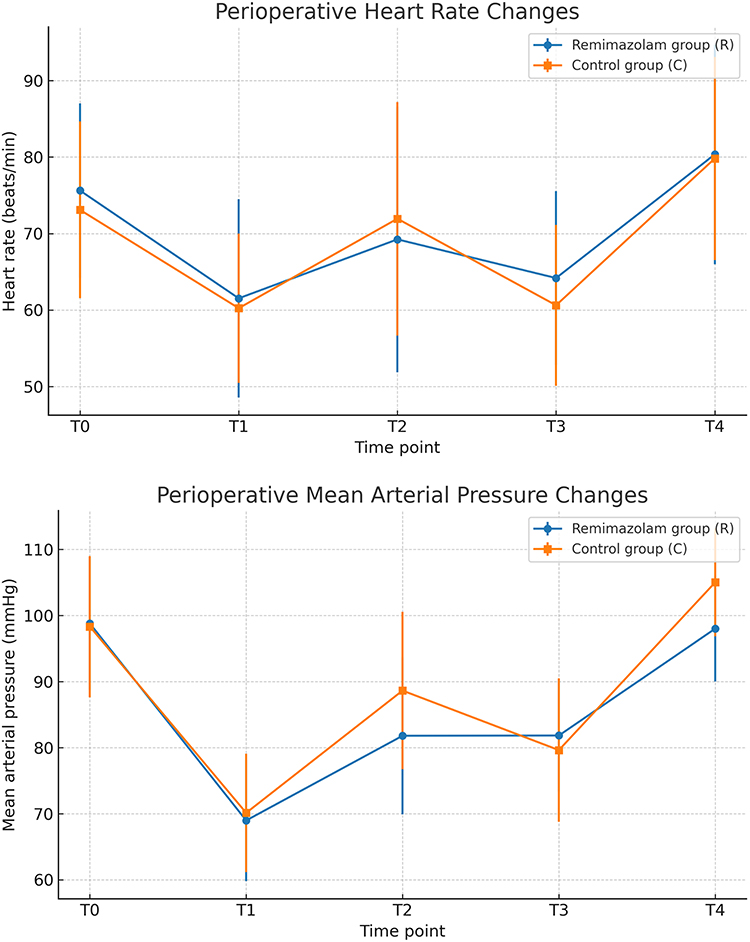 |
Figure 4 Changes in Vital Signs. |
Ramsay Sedation Scores
At the time of eye opening or first response, the median (interquartile range) Ramsay score was 3 (2–4) in the remimazolam group, significantly higher than 2 (2–2) in the control group (P < 0.001). Further analysis of the score distribution revealed an overall significant difference between groups (P = 0.0066): the proportion of patients with a score of 4 was significantly higher in the remimazolam group compared with the control group (17.6% vs 0%, P = 0.0246), whereas a score of 2 was more common in the control group (70.6% vs 44.1%, P = 0.049). Differences in other score levels were not statistically significant (P > 0.05).
At extubation, the median Ramsay score was 2 (2–3) in the remimazolam group and 2 (2–2) in the control group, with a statistically significant difference (P = 0.002). Distributional comparison also indicated a significant overall difference (P = 0.0187): a score of 2 was more frequent in the control group (91.2% vs 64.7%, P = 0.0174), whereas a score of 3 was more common in the remimazolam group (26.5% vs 5.9%, P = 0.0446). No significant differences were observed for the other levels.
At 5 minutes after extubation, the median Ramsay scores were 2 (2–3) in both groups, with no significant difference (P = 0.562). Similarly, the distribution of scores did not differ significantly (P = 0.5664), with comparable proportions in each category (eg, score of 2: 55.9% vs 61.8%; score of 3: 41.2% vs 38.2%; all P > 0.05). Detailed Ramsay sedation scores at different time points are summarized in Tables 5–8.
 |
Table 5 Ramsay Scores at First Response |
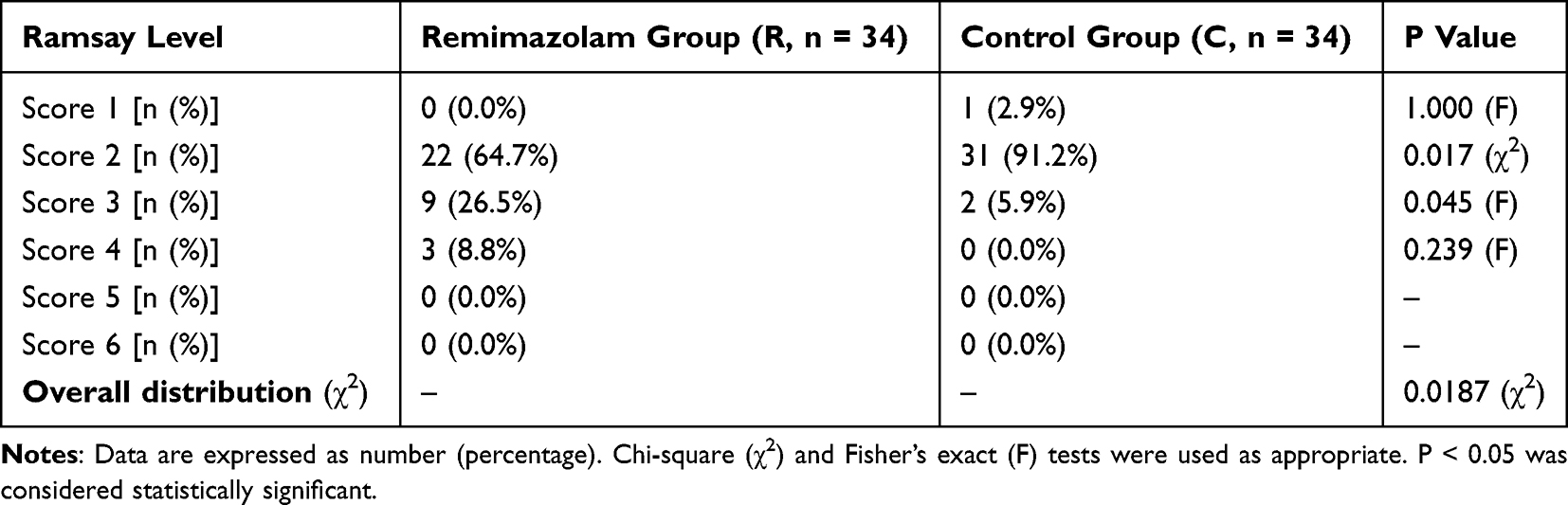 |
Table 6 Ramsay Scores at Extubation |
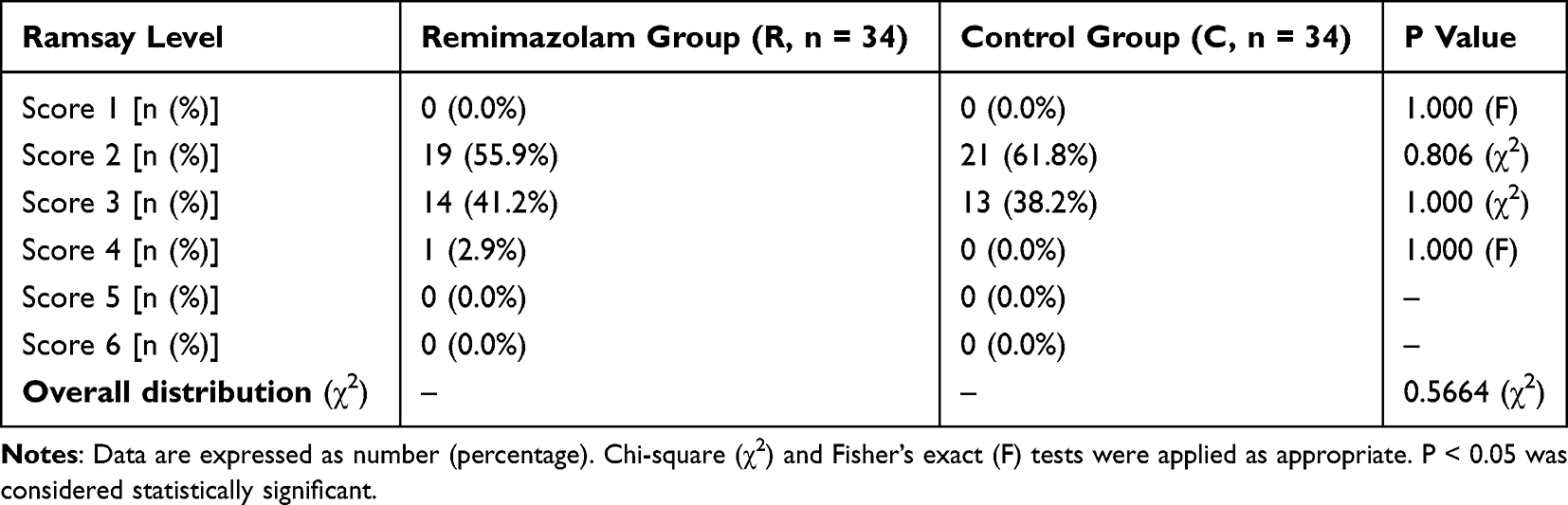 |
Table 7 Ramsay Scores 5 min After Extubation |
 |
Table 8 Summary of Ramsay Scores (Median [IQR]) at Different Time Points |
Adverse Events
The emergence time was significantly longer in the remimazolam group compared with the control group (12.21 ± 9.52 min vs 5.12 ± 4.80 min, P < 0.001). Similarly, extubation time was prolonged in the remimazolam group (15.18 ± 11.85 min vs 6.09 ± 5.78 min, P < 0.001). At 1 hour postoperatively, the median sore throat score was 1 (1–2) in the remimazolam group and 1.5 (1–2.25) in the control group, with no significant difference (P = 0.356). At 24 hours, the corresponding scores were 1 (1–2) and 1.5 (1–2), also without significant difference (P = 0.335).
Comparisons of postoperative adverse events showed no statistically significant differences between the remimazolam and control groups in the incidence of bradycardia [5.9% (2/34) vs 2.9% (1/34), P = 1.000], nausea and vomiting [0% (0/34) vs 2.9% (1/34), P = 1.000], hypotension [14.7% (5/34) vs 20.6% (7/34), P = 0.755], or postoperative bleeding [0% (0/34) vs 2.9% (1/34), P = 1.000] (Table 9).
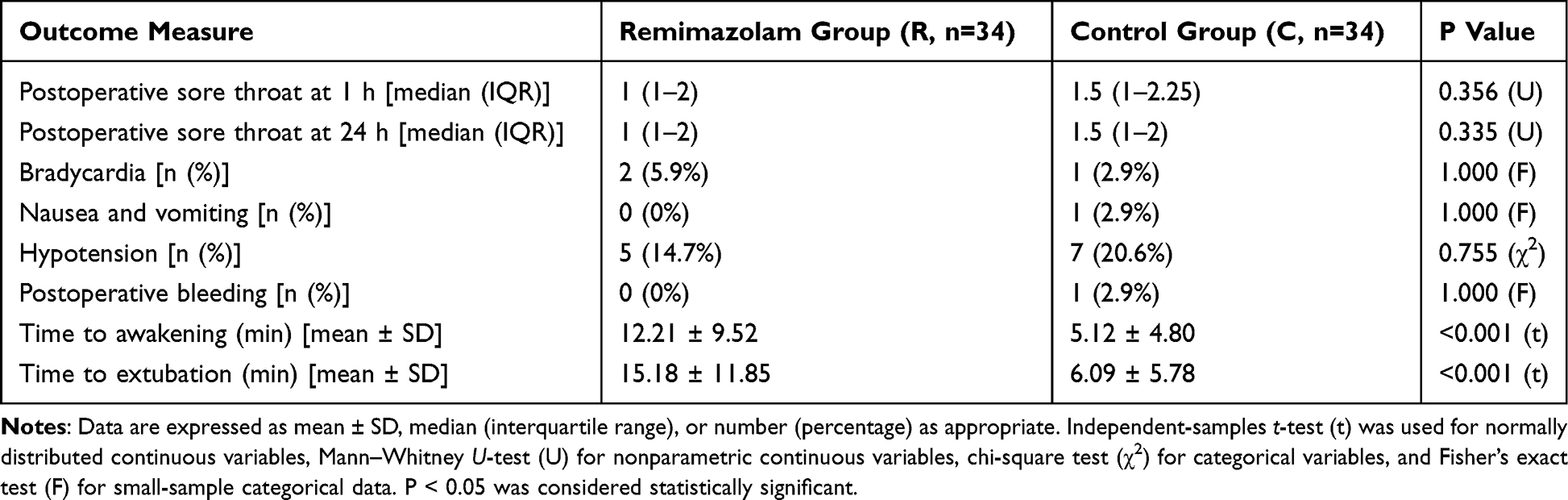 |
Table 9 Comparison of Adverse Events Between the Two Groups |
Discussion
The present randomized controlled trial demonstrated that remimazolam infusion during sevoflurane-based anesthesia significantly reduced the incidence of postoperative coughing during emergence in patients undergoing thyroidectomy. In addition, patients receiving remimazolam exhibited more stable hemodynamic responses during tracheal extubation. Although awakening and extubation times were significantly prolonged in the remimazolam group, the extent of this prolongation was clinically acceptable and was accompanied by improved sedation quality and a smoother emergence process, without an increase in adverse events.
The reduced incidence of coughing observed with remimazolam may be attributed to its central pharmacological effects on airway reflex control. As an ultra–short-acting benzodiazepine, remimazolam enhances GABA-A receptor–mediated inhibitory neurotransmission in the central nervous system, including brainstem pathways involved in cough generation. Increased GABAergic inhibition has been shown to elevate the cough reflex threshold and reduce the excitability of airway reflex arcs, thereby attenuating cough responses to tracheal stimulation during emergence from anesthesia.18,19
In addition to direct suppression of airway reflex sensitivity, remimazolam may indirectly reduce coughing by providing a smoother and more stable emergence profile. Previous studies have demonstrated that remimazolam is associated with reduced emergence agitation, lower cough grades, and improved hemodynamic stability compared with control anesthetic regimens. Attenuation of sympathetic activation and abrupt arousal during emergence may further limit cough-triggering stimuli, particularly during tracheal extubation.11,20,21
Taken together, the combined effects of central cough reflex inhibition and smoother emergence with reduced agitation and sympathetic fluctuations likely account for the lower incidence and severity of coughing observed with remimazolam in the present study.Several clinical studies have shown that remimazolam administration is associated with decreased emergence agitation, lower cough grades, and more stable blood pressure and heart rate during recovery compared with control conditions.13,22,23
In our study, one patient in the placebo group developed active bleeding in the drainage bag after returning to the ward and required emergency reoperation. Notably, this patient experienced severe coughing at extubation, supporting the hypothesis that vigorous emergence coughing may serve as a triggering factor for post-thyroidectomy hemorrhage. Previous studies have likewise reported that extubation-related coughing and hemodynamic changes are major contributors to postoperative bleeding after thyroid surgery.24
Accordingly, multiple pharmacological strategies have been investigated to suppress coughing during emergence. Lidocaine, administered intravenously or topically to the airway, can blunt airway reflexes and has been supported by systematic evidence for reducing extubation-related cough. Dexmedetomidine has also been widely studied for achieving smoother emergence;7,25 randomized trials in thyroidectomy patients have shown that low-dose dexmedetomidine reduces emergence coughing and agitation and may decrease postoperative bleeding by attenuating sympathetic responses.26 Opioid-based approaches have similarly been explored, including continuous remifentanil infusion and the use of potent opioids such as sufentanil, which can suppress coughing more effectively;8,27 however, these regimens may increase the risk of delayed awakening, postoperative nausea and vomiting, respiratory depression, or bradycardia, thereby limiting their routine use.
In the present study, the incidence of coughing after thyroidectomy under sevoflurane–remifentanil anesthesia was 76.47%, lower than the 91% reported by Lee et al. This discrepancy may be attributable to differences in opioid dosing. Lee’s study used remifentanil at a target-controlled infusion of 1 ng/mL (approximately 0.05 μg/kg/min), whereas our infusion rate was 0.1–0.2 μg/kg/min. Higher opioid doses may reduce coughing but at the expense of more opioid-related adverse effects. Therefore, strategies that enhance cough suppression without further increasing opioid exposure are clinically desirable. In this context, adjunctive remimazolam may represent a more balanced approach by attenuating airway reflexes and sympathetic activation while maintaining favorable safety. Importantly, unlike dexmedetomidine or opioids, remimazolam has the unique advantage of being rapidly antagonized by flumazenil when rapid emergence is required, which may further improve its clinical applicability.28
It is noteworthy that remimazolam was associated with significantly prolonged awakening and extubation times. However, the absolute prolongation was modest and remained within clinically acceptable limits. Importantly, this delay was accompanied by improved sedation quality during emergence, reduced coughing, and more stable cardiovascular responses. In the context of thyroid surgery, where excessive coughing and hemodynamic surges may increase the risk of postoperative bleeding, such a trade-off may be clinically advantageous. Our findings suggest that a slightly prolonged emergence may be an acceptable cost for enhanced safety and patient comfort.
Although continuous remimazolam infusion reduced the intraoperative requirement for sevoflurane, this was unlikely to have confounded the primary outcomes. In our protocol, end-tidal sevoflurane concentration was washed out to zero before outcome assessment, minimizing any residual pharmacodynamic effects. Therefore, the observed effects are more likely attributable to remimazolam rather than differential sevoflurane exposure.
Several limitations of this study should be acknowledged. First, this was a single-center study with a relatively limited sample size, which may affect the generalizability of the results. Second, coughing severity was assessed using a clinical grading scale, which, although commonly used, remains subjective. Third, the optimal dose and infusion duration of remimazolam for minimizing coughing while avoiding excessive sedation were not explored. However, sevoflurane was fully washed out at the end of anesthesia (MAC reduced to 0) to minimize its residual influence on emergence outcomes. Future multicenter studies with larger sample sizes and dose-finding designs are warranted to further refine the clinical application of remimazolam during emergence.
Conclusion
In conclusion, remimazolam infusion during sevoflurane-based anesthesia reduces emergence coughing and stabilizes hemodynamic responses during extubation in patients undergoing thyroidectomy, while providing a deeper but controlled level of sedation during emergence. Despite slightly prolonged awakening and extubation times, no increase in postoperative adverse events was observed, indicating clinically acceptable safety.
Data Sharing Statement
The data that support the findings of this study are not publicly available due to patient confidentiality and institutional policy restrictions. Deidentified participant data may be made available from the corresponding author upon reasonable request for academic purposes only.
Acknowledgment
The authors would like to thank all the authors who participated in this study for their contributions to this study.
Funding
This study was supported by research funds from Nanchong Science and Technology Bureau (22SXQT0293).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wang X, Zhu G, Tan J. et al. Effects of continuous and slow tracheal tube cuff deflation on cough reflex during extubation in noncardiac surgery patients: a randomised clinical trial. BMC Anesthesiol. 2023;23(1):45. doi:10.1186/s12871-023-02003-5
2. Xu J, Sun P, Ma J-H, et al. Multimodal prevention of emergence cough following nasal endoscopic surgery under general anesthesia: a double-blind randomized trial. Front Med Lausanne. 2024;11:1288978. doi:10.3389/fmed.2024.1288978
3. Min K, Wang Y, Feng D, et al. The Influence of Piriform Recess Instillation with Lidocaine Before Bronchoscopy on Post-General Anesthesia Cough: a Randomized Controlled Trial. Drug Des Devel Ther. 2024;18:2883–13. doi:10.2147/DDDT.S458058
4. Edafe O, Cochrane E, Balasubramanian SP. Reoperation for Bleeding After Thyroid and Parathyroid Surgery: incidence, Risk Factors, Prevention, and Management. World J Surg. 2020;44(4):1156–1162. doi:10.1007/s00268-019-05322-2
5. Nakagawa S, Shakuo T, Matsudo S, et al. Remimazolam Anesthesia for Thyroid Surgery. Case Rep Anesthesiol. 2023;2023:2352693. doi:10.1155/2023/2352693
6. Randolph GW, Dralle H, Abdullah H, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011;121(Suppl S1):S1–16. doi:10.1002/lary.21119
7. Shroff PP, Patil V. Efficacy of cuff inflation media to prevent postintubation-related emergence phenomenon: air, saline and alkalinized lignocaine. Eur J Anaesthesiol. 2009;26(6):458–462. doi:10.1097/EJA.0b013e32832403fa
8. Egan TD, Minto CF, Hermann DJ, et al. Remifentanil versus alfentanil: comparative pharmacokinetics and pharmacodynamics in healthy adult male volunteers. Anesthesiology. 1996;84(4):821–833. doi:10.1097/00000542-199604000-00009
9. Kim SY, Kim JM, Lee JH, et al. Efficacy of intraoperative dexmedetomidine infusion on emergence agitation and quality of recovery after nasal surgery. Br J Anaesth. 2013;111(2):222–228. doi:10.1093/bja/aet056
10. Sneyd JR, Rigby-Jones AE. Remimazolam for anaesthesia or sedation. Curr Opin Anaesthesiol. 2020;33(4):506–511. doi:10.1097/ACO.0000000000000877
11. Cinelli E, Iovino L, Bongianni F, et al. GABA A - and glycine-mediated inhibitory modulation of the cough reflex in the caudal nucleus tractus solitarii of the rabbit. Am J Physiol Lung Cell Mol Physiol. 2016;311(3):L570–80. doi:10.1152/ajplung.00205.2016
12. Chen W, Bao W, Shi J, et al. Investigation into the application of remimazolamin conjunction with low-dose propofolfor pediatricfiberoptic bronchoscopy. Sci Rep. 2024;14(1):11671. doi:10.1038/s41598-024-62181-1
13. Lu Y, Xu Q, Dai H, et al. Remimazolam for the prevention of emergence agitation in adults following nasal surgery under general anesthesia: a prospective randomized clinical controlled trial. BMC Anesthesiol. 2025;25(1):8. doi:10.1186/s12871-024-02875-1
14. Kim JH, Lee GY, Lee HS, et al. The Effect of Ramosetron on Remifentanil in Preventing Emergence Cough from Sevoflurane Anesthesia in Female Patients. Curr Pharm Des. 2022;28(16):1359–1366. doi:10.2174/1381612828666220412101447
15. Minogue SC, Ralph J, Lampa MJ. Laryngotracheal topicalization with lidocaine before intubation decreases the incidence of coughing on emergence from general anesthesia. Anesth Analg. 2004;99(4):1253–1257. doi:10.1213/01.ANE.0000132779.27085.52
16. Ramsay MA, Savege TM, Simpson BRJ, et al. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2(5920):656–659. doi:10.1136/bmj.2.5920.656
17. Hung NK, Wu C-T, Chan S-M, et al. Effect on postoperative sore throat of spraying the endotracheal tube cuff with benzydamine hydrochloride, 10% lidocaine, and 2% lidocaine. Anesth Analg. 2010;111(4):882–886. doi:10.1213/ANE.0b013e3181d4854e
18. Kilpatrick GJ, McIntyre MS, Cox RF, et al. CNS 7056: a novel ultra-short-acting Benzodiazepine. Anesthesiology. 2007;107(1):60–66. doi:10.1097/01.anes.0000267503.85085.c0
19. Freyer N, Knöspel F, Damm G, et al. Metabolism of remimazolam in primary human hepatocytes during continuous long-term infusion in a 3-D bioreactor system. Drug Des Devel Ther. 2019;13:1033–1047. doi:10.2147/DDDT.S186759
20. Tung A, Fergusson NA, Ng N, et al. Medications to reduce emergence coughing after general anaesthesia with trachealintubation: a systematic review and network meta-analysis. Br J Anaesth. 2020;124(4):480–495. doi:10.1016/j.bja.2019.12.041
21. Zhang J, Wang X, Zhang Q, et al. Application effects of remimazolam and propofol on elderly patients undergoing Hip replacement. BMC Anesthesiol. 2022;22(1):118. doi:10.1186/s12871-022-01641-5
22. Kim SH, Cho JY, Kim M, et al. Safety and efficacy of remimazolam compared with midazolam during bronchoscopy: a single-center, randomized controlled study. Sci Rep. 2023;13(1):20498. doi:10.1038/s41598-023-47271-w
23. Pastis NJ, Yarmus LB, Schippers F, et al. Safety and Efficacy of Remimazolam Compared With Placebo and Midazolam for Moderate Sedation During Bronchoscopy. Chest. 2019;155(1):137–146. doi:10.1016/j.chest.2018.09.015
24. Bacuzzi A, Dionigi G, Del Bosco A, et al. Anaesthesia for thyroid surgery: perioperative management. Int J Surg. 2008;6(1):S82–5. doi:10.1016/j.ijsu.2008.12.013
25. Chang CH, Lee JW, Choi JR, et al. Effect-site concentration of remifentanil to prevent cough after laryngomicrosurgery. Laryngoscope. 2013;123(12):3105–3109. doi:10.1002/lary.24199
26. D Spina, I McFadzean, FKR Bertram, et al. Peripheral mechanisms II: the pharmacology of peripherally active antitussive drugs. Handb Exp Pharmacol. 2009;187(187):155–186.
27. Lee JY, Lim BG, Park HY, et al. Sufentanil infusion before extubation suppresses coughing on emergence without delaying extubation time and reduces postoperative analgesic requirement without increasing nausea and vomiting after desflurane anesthesia. Korean J Anesthesiol. 2012;62(6):512–517. doi:10.4097/kjae.2012.62.6.512
28. Jeon S, Kim J, Karm M-H, et al. Effect of converting from propofol to remimazolam with flumazenil reversal on recovery from anesthesia in outpatients with mental disabilities: a randomized controlled trial. BMC Anesthesiol. 2024;24(1):151. doi:10.1186/s12871-024-02526-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.