Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 9
Effect of preheating and light-curing unit on physicochemical properties of a bulk fill composite
Authors Theobaldo JD, Aguiar FH ![]() , Pini NI, Lima DA
, Pini NI, Lima DA ![]() , Liporoni PC
, Liporoni PC ![]() , Catelan A
, Catelan A
Received 21 December 2016
Accepted for publication 5 April 2017
Published 16 May 2017 Volume 2017:9 Pages 39—43
DOI https://doi.org/10.2147/CCIDE.S130803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Jéssica Dias Theobaldo,1 Flávio Henrique Baggio Aguiar,1 Núbia Inocencya Pavesi Pini,2 Débora Alves Nunes Leite Lima,1 Priscila Christiane Suzy Liporoni,3 Anderson Catelan3
1Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Piracicaba, 2Ingá University Center, Maringá, 3Departament of Dentistry, University of Taubaté, Taubaté, Brazil
Objective: The aim of this study is to evaluate the effect of composite preheating and polymerization mode on degree of conversion (DC), microhardness (KHN), plasticization (P), and depth of polymerization (DP) of a bulk fill composite.
Methods: Forty disc-shaped samples (n = 5) of a bulk fill composite were prepared (5 × 4 mm thick) and randomly divided into 4 groups according to light-curing unit (quartz–tungsten–halogen [QTH] or light-emitting diode [LED]) and preheating temperature (23 or 54 °C). A control group was prepared with a flowable composite at room temperature. DC was determined using a Fourier transform infrared spectrometer, KHN was measured with a Knoop indenter, P was evaluated by percentage reduction of hardness after 24 h of ethanol storage, and DP was obtained by bottom/top ratio. Data were statistically analyzed by analysis of variance and Tukey’s test (α = 0.05).
Results: Regardless of light-curing, the highest preheating temperature increased DC compared to room temperature on bottom surface. LED showed a higher DC compared to QTH. Overall, DC was higher on top surface than bottom. KHN, P, and DP were not affected by curing mode and temperature, and flowable composite showed similar KHN, and lower DC and P, compared to bulk fill.
Conclusion: Composite preheating increased the polymerization degree of 4-mm-increment bulk fill, but it led to a higher plasticization compared to the conventional flowable composite evaluated.
Keywords: composite resins, physicochemical phenomena, polymerization, hardness, heating
Introduction
Nowadays, composite resins have been used successfully as an alternative material to amalgam in posterior restorations.1,2 In an attempt to speed up the restoration process, bulk fill composites were introduced on dental market, enabling build increments up to 4- to 5-mm thickness to be cured in 1 step, skipping the time required for layering technique.3,4 Clinically, large and deep cavities could be restored easily and faster using these materials.5
Polymerization effectiveness of light-activated materials is related to improved mechanical properties; however, it is affected by several factors, such as exposure time, light power intensity, distance between the guide tip of light-curing unit (LCU) and restorative material surface, and others.6 Quartz–tungsten–halogen (QTH) curing unit has been extensively used for a long time; however, light-emitting diode (LED) device shows lower degradation over time and blue light emission without requiring filter, is becoming popular in dental practice.7
The degree of conversion (DC) of resinous materials can be improved with composite preheating prior to light curing.8 Increased temperature results in a higher molecular mobility due to lower viscosity,8,9 but this reaction is self-limited and imposed by rapid formation of a highly cross-linked polymeric structure during conversion of monomer into polymer.8
Mechanical properties are related to conversion rate, but a similar DC value may display distinct cross-link density content due to differences in polymer network, since linear chains are more susceptible to softening than cross-linked polymer,10 affecting the clinical durability of composite restorations.
Therefore, this study aimed to assess the effect of preheating composite and LCU on DC, microhardness, and plasticization of bulk fill composites. Two research hypotheses were tested: (1) the highest preheating temperature and (2) LED curing would increase the physicochemical properties tested.
Materials and methods
The experimental design of this study constituted 2 factors (LCU in 2 levels: QTH and LED; and preheating temperature in 2 levels: 23 and 54 °C) and 1 sub-factor (in 2 levels: top and bottom surfaces).
In this study, one light-cured low-stress posterior bulk fill flowable base composite (Surefil SDR, shade universal, Lot 651073E; Dentsply Caulk, Milford, DE, USA) was used. The material was kept in an incubator (model 502; Fanem Ltda, Guarulhos, Brazil) with respective preheating temperature (23 and 54 °C) for 1 h before use. Disc-shaped samples (5 mm in diameter and 4 mm in thickness) were prepared (n = 5) at room temperature (23 °C) and controlled humidity (30%). A Teflon mold was filled with the composite, and then covered with a polyester strip and microscope slide. A 500-g load was used to compress the material and prevent bubble formation, removing excess of the material. A control group was prepared with a flowable composite (Filtek Z350 XT Flow, shade A3, Lot N531664; 3M Espe, St. Paul, MN, USA) at room temperature in same dimensions, except thickness (2 mm).
Composites were cured for 20 s at a distance of 2 mm from the material surface (the objective was to simulate the space for after placement with traditional resin composite, indicated by the manufacturer (2mm).), using a QTH (Optilux 501; Kerr Corp., Orange, CA, USA) or a third-generation LED (Valo; Ultradent Inc., South Jordan, UT, USA) according to the manufacturer’s recommendation. The light optical power (mW) delivered by devices was measured using a power meter (Ophir Optronics, Jerusalem, Israel). The tip diameter was measured with a digital caliper (Mitutoyo Sul Americana, Suzano, Brazil), and the tip area was determined in square centimeters. Irradiance (mW/cm2) was calculated by dividing the optical power by tip area. Positioning a spacer device of 2-mm height between the light guide tip of curing unit and the power meter surface, the irradiance was calculated to be 450 and 630 mW/cm2 for QTH and LED, respectively (an output irradiance of 650 and 800 mW/cm2 at 0 mm). Samples were dry-stored for 24 h in light-proofed containers at 37 °C, and polished with a 1200-grit silicon carbide abrasive paper (CarbiMet 2 Abrasive Discs; Buehler, Lake Bluff, IL, USA).
DC was recorded in scattering mode using a Fourier transform infrared (FT-IR) spectrometer (Spectrum 100 Optica; PerkinElmer, Waltham, MA, USA) equipped with an attenuated total reflectance (ATR) accessory. The sample was placed on the horizontal face of ZnSe crystal (Pike Technologies, Madison, WI, USA) of ATR cell, and an absorption spectrum was obtained with 16 scans at a resolution of 4 cm−1 in region between 1800 and 1400 cm−1 by baseline technique.11 To calculate DC, the ratio (R) between the peak heights of C=C aliphatic (1637 cm−1) and internal standard (1608 and 1602 cm−1 for Filtek Z350 XT Flow and Surefil SDR, respectively) band absorptions for cured and uncured composite was used, according to the formula: DC (%) = (1 – [Rpolymer/Rmonomer]) × 100.
Initial microhardness (MHi) was assessed on the top and bottom surfaces of each sample using a microhardness tester (HMV-2T E; Shimadzu Corporation, Kyoto, Japan) with a Knoop diamond indenter under a 10-g load for 10 s. Five indentations were carried out on the surface of each sample, one at the center and the other four at a distance of approximately 100 μm from the central location. The average of 5 values was calculated as KHN (Knoop hardness number) value for each sample.
Plasticization (P) was determined by the percentage reduction of microhardness (%MHred) after storage in absolute ethanol (100%) at 37 °C for 24 h.10 After storage in alcohol, a second microhardness measurement (MHf) was carried out as previously described. The same operator performed KHN measurements, before and after immersion in alcohol. The P was calculated using the following formula: %MHred = 100 – [(MHf × 100)/MHi]. Depth of polymerization (DP) was calculated by the hardness ratio between the bottom and top surfaces for each sample.
Normality of DC, KHN, P, and DP data was confirmed by Shapiro–Wilk test. After that, DC, KHN, and DP data were analyzed by split-plot analysis of variance (ANOVA) and Tukey’s test at a preset α of 0.05. The factors LCU and preheating temperature were considered in parcels, and the sub-factor surface was considered in sub-parcel. DP was analyzed by 2-way ANOVA and Tukey’s test (α = 0.05). Dunnett test was used to compare experimental groups with control group at 5% level of significance.
Results
The DC results are presented in Table 1. ANOVA showed significant difference for factors (LCU: p < 0.001 and surface: p < 0.001), as well as for interactions of factors (LCU × surface: p = 0.0078 and temperature × surface: p = 0.0417). Regardless of preheating temperature, LED presented a higher DC compared to QTH, and top surface showed a higher conversion rate compared to bottom for LED unit. Regardless of LCU, the highest preheating temperature (54 °C) increased the DC of bottom surface compared to room temperature (23 °C), and top surface presented a higher monomer conversion than bottom at 23 °C. Bulk fill composite (Surefil SDR) resulted in a higher DC compared to control group (Filtek Z350 XT Flow) at all experimental conditions (p ≤ 0.05).
 | Table 1 Means (SD) of degree of conversion (%) of composites in terms of light-curing unit, preheating temperature, and surface analyzed Notes: Distinct capital letters comparing the top and bottom surface and the lower case letters comparing the different preheating temperatures within each curing unit are statistically different (p ≤ 0.05). #Differs from QTH unit (p ≤ 0.05). *Differs from control group (p ≤ 0.05). Abbreviations: SD, standard deviation; LED, light-emitting diode; QTH, quartz–tungsten–halogen. |
For both KHN and P, ANOVA showed statistical difference only for factor surface analyzed. Top surface presented a higher KHN compared to bottom (p = 0.0307). Bulk fill composite when cured with QTH unit showed a lower KHN than control group for bottom surface (p ≤ 0.05). Bottom surface resulted in a higher P compared to top surface (p < 0.001). Plasticization of bulk fill composite was higher than control group at all experimental conditions (p ≤ 0.05). These results are illustrated in Table 2.
 | Table 2 Means (SD) of Knoop hardness number (KHN, kg F/mm2) and plasticization (%KHNRed) of composites in terms of light-curing unit, preheating temperature, and surface analyzed Notes: Distinct capital letters comparing the top and bottom surfaces and the lower case letters comparing the different preheating temperatures within each curing unit are statistically different (p ≤ 0.05) for each assay performed. *Differs from control group (p ≤ 0.05). Abbreviations: SD, standard deviation; LED, light-emitting diode; QTH, quartz–tungsten–halogen. |
Table 3 shows that DP was not affected by curing unit and preheating temperature (p > 0.05 and p = 0.2033, respectively), as well as interaction of factors (p > 0.05).
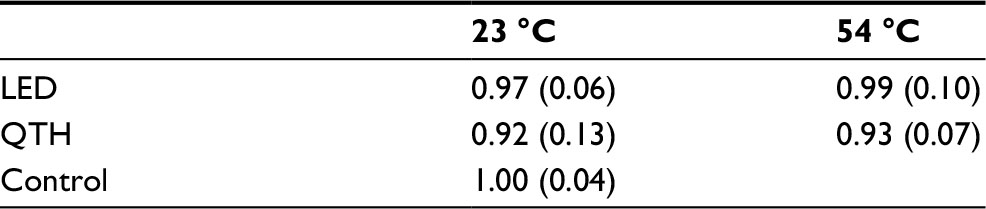 | Table 3 Means (SD) of depth of polymerization of composites in terms of light-curing unit and preheating temperature Notes: There was no statistical difference between light-curing units, preheating temperatures, and experimental groups compared to control group (p > 0.05). Abbreviations: SD, standard deviation; LED, light-emitting diode; QTH, quartz–tungsten–halogen. |
Discussion
According to the results of the present study, both research hypotheses tested were rejected, because only the DC was increased in some situations when composite preheating and polymerization were performed using an LED unit. The technology used for bulk fill flowable composite tested involved the addition of a polymerization modulator chemically embedded in a curable resin backbone leading to the formation of a more relaxed network, allowing a build up with 4-mm increments with an adequate curing rate and minimal polymerization stress. The tested bulk fill restorative material with 4-mm-increment thickness showed a higher monomer conversion rate compared to conventional flowable composite with 2-mm increment used as control.
Adequate cure of deeper portion of restorative materials is the main concern associated with using bulk placement technique for dental composite restorations.12 The DP of bulk fill composite was not affected by any factor. It is stated that a resin-based material with a bottom/top surface ratio higher than 0.8 (80%) is clinically acceptable and defined as sufficiently cured.13 All experimental groups had a bottom/top ratio greater than 0.9, and thus, the bulk fill flowable composite evaluated can be used in 4-mm-increment thickness with an adequate depth of cure. This was proved in the study by Fronza et al3 that evaluated the microhardness of different bulk fill resins in different depths and obtained results similar to the conventional resin.
Resinous materials are softened in aqueous environment due to polymer swelling and reduction of frictional forces between polymer chains.14 Degree of cross-linking in the network of polymeric materials has been indirectly evaluated by polymer softening after ethanol storage.10 The absorption of alcohol molecules by the polar portion of the organic content causes swelling of resin matrix.15 Moreover, insufficient branched polymer is more susceptible to enzymatic attack and plasticization effect by chemical substances that enter during eating and drinking.16
Although the bulk fill material had the highest DC, higher softening was observed for this flowable composite compared to control group. A similar conversion rate may result in different content of linear and cross-linked polymeric chains.10 Surefil SDR is a posterior bulk fill composite designed to be used as a base in Class I and II dental restorations. However, due to high P, this material should not be exposed to oral environment as Class II restorations occur, mainly in greater thickness increments.
The DC of resin-based composites is a crucial factor for the determination of mechanical properties of materials and their biocompatibility.17 FT-IR spectroscopy allows the direct detection of the amount of unreacted C=C, but this property alone is not enough to characterize the 3-dimensional resinous material structure.14 Top surface presents the highest values of DC, KHN, and P resistance compared to bottom, according to the results obtained by Aguiar et al. Light is scattered by the filler particles and absorbed by photo-initiators and any pigments, and both factors reduce the light penetration.6,18,19 Furthermore, most often, LCU tip cannot be placed directly on the material surface due to cavity depth, teeth position, and morphology of fissures and cusps, which decreases irradiance and may impair polymerization efficacy. Approximately, 10% of optical power is lost with 1 mm of air interposed between the curing tip and the material surface to be irradiated.20
In this study, composite preheating increased the conversion rate of bottom surface regardless of LCU. It is reported that the increase in temperature results in a lower viscosity and higher molecular mobility.8,9 Preheating is described as a simple procedure to improve DC, but this reaction is self-limited, principally due to increase in system viscosity resulting in decrease in reactive species mobility imposed by the formation of branched polymer structure.8
LED device promotes a higher DC than QTH unit, regardless of preheating temperature. In this study, the greater irradiance of LED curing unit evaluated probably more active growth centers with a tendency to form branched structure16,21 and showed a higher rate of conversion of monomer into polymer22 compared to halogen unit. Hardness has been used to predict the wear resistance; it is related to conversion rate and inorganic filler content.23–25 KHN was similar to control group, except for bottom surface cured with QTH. Despite the higher filler volume fraction of conventional flowable composite (55%), its lower DC resulted in similar hardness compared to bulk fill flowable composite (44%).
Therefore, this bulk fill flowable base could be used as a liner with a lower thickness in Class II restorations improving marginal sealing and internal adaptation, and decreasing microleakage.26–28 In large and deep cavities, this material could speed up the restoration process, allowing increments up to 4-mm thickness to be cured in one step. However, in Class II restorations, it would be interesting to first rebuild the proximal wall with conventional composite resin prior to bulk placement technique with this material.
Conclusion
The bulk fill flowable composite tested showed an adequate DP with 4-mm-increment thickness, but a high plasticization, and composite preheating can be used as an effective method to improve DC.
Disclosure
The authors report no conflicts of interest in this work.
References
Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, et al. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater. 2011;27(10):955–963. | ||
Bayraktar Y, Ercan E, Hamidi MM, Çolak H. One-year clinical evaluation of different types of bulk-fill composites. J Investig Clin Dent. Epub 2016 Jan 22. | ||
Fronza BM, Rueggeberg FA, Braga RR, et al. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater. 2015;31(12):1542–1551. | ||
Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38(6):618–625. | ||
Ilie N, Schöner C, Bücher K, Hickel R. An in-vitro assessment of the shear bond strength of bulk-fill resin composites to permanent and deciduous teeth. J Dent. 2014;42(7):850–855. | ||
Aguiar FH, Andrade KR, Leite Lima DA, Ambrosano GM, Lovadino JR. Influence of light curing and sample thickness on microhardness of a composite resin. Clin Cosmet Investig Dent. 2009;1:21–25. | ||
Faria-e-Silva AL, Lima AF, Moraes RR, Piva E, Martins LR. Degree of conversion of etch-and-rinse and self-etch adhesives light-cured using QTH or LED. Oper Dent. 2010;35(6):649–654. | ||
Daronch M, Rueggeberg FA, De Goes MF. Monomer conversion of pre-heated composite. J Dent Res. 2005;84(7):663–667. | ||
Fróes-Salgado NR, Silva LM, Kawano Y, Francci C, Reis A, Loguercio AD. Composite pre-heating: effects on marginal adaptation, degree of conversion and mechanical properties. Dent Mater. 2010;26(9):908–914. | ||
Schneider LF, Moraes RR, Cavalcante LM, Sinhoretti MA, Correr-Sobrinho L, Consani S. Cross-link density evaluation through softening tests: effect of ethanol concentration. Dent Mater. 2008;24(2):199–203. | ||
Rueggeberg FA, Hashinger DT, Fairhurst CW. Calibration of FTIR conversion analysis of contemporary dental resin composites. Dent Mater. 1990;6(4):241–249. | ||
Campodonico CE, Tantbirojn D, Olin PS, Versluis A. Cuspal deflection and depth of cure in resin-based composite restorations filled by using bulk, incremental and transtooth-illumination techniques. J Am Dent Assoc. 2011;142(10):1176–1182. | ||
Schattenberg A, Lichtenberg D, Stender E, Willershausen B, Ernst CP. Minimal exposure time of different LED-curing devices. Dent Mater. 2008;24(8):1043–1049. | ||
Kusgoz A, Ülker M, Yesilyurt C, Yoldas OH, Ozil M, Tanriver M. Silorane-based composite: depth of cure, surface hardness, degree of conversion, and cervical microleakage in Class II cavities. J Esthet Restor Dent. 2011;23(5):324–335. | ||
Gerhardt K, Silva AS, Rego G, Sinhoreti MA, Salgado VE, Schneider LF. Bulk and surface properties related to composite filler size. Braz J Oral Sci. 2013;12(4):323–329. | ||
Asmussen E, Peutzfeldt A. Influence of selected components on crosslink density in polymer structures. Eur J Oral Sci. 2001;109(4):282–285. | ||
Alshali RZ, Silikas N, Satterthwaite JD. Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent Mater. 2013;29(9):e213–e217. | ||
Gonçalves F, Kawano Y, Braga RR. Contraction stress related to composite inorganic content. Dent Mater. 2010;26(7):704–709. | ||
Alrahlah A, Silikas N, Watts DC. Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater. 2014;30(2):149–154. | ||
Prati C, Chersoni S, Montebugnoli L, Montanari G. Effect of air, dentin and resin-based composite thickness on light intensity reduction. Am J Dent. 1999;12(5):231–234. | ||
Alkhudhairy FI. The effect of curing intensity on mechanical properties of different bulk-fill composite resins. Clin Cosmet Investig Dent. 2017;9:1–6. | ||
Calheiros FC, Daronch M, Rueggeberg FA, Braga RR. Influence of irradiant energy on degree of conversion, polymerization rate and shrinkage stress in an experimental resin composite system. Dent Mater. 2008;24(9):1164–1168. | ||
Baek DM, Park JK, Son SA, et al. Mechanical properties of composite resins light-cured using a blue DPSS laser. Lasers Med Sci. 2013;28(2):597–604. | ||
Leal A, Paula A, Ramalho A, Esteves M, Ferreira MM, Carrilho E. Roughness and microhardness of composites after different bleaching techniques. J Appl Biomater Funct Mater. 2015;13(4):e381–e388. | ||
Say EC, Civelek A, Nobecourt A, Ersoy M, Guleryuz C. Wear and microhardness of different resin composite materials. Oper Dent. 2003;28(5):628–634. | ||
Hernandes NM, Catelan A, Soares GP, et al. Influence of flowable composite and restorative technique on microleakage of class II restorations. J Investig Clin Dent. 2014;5(4):283–288. | ||
Scotti N, Comba A, Gambino A, et al. Microleakage at enamel and dentin margins with a bulk fills flowable resin. Eur J Dent. 2014;8(1):1–8. | ||
Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater. 2013;29(3):269–277. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.