Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Nebulized Dexmedetomidine on Postoperative Nausea and Vomiting in Female Patients Undergoing Radical Thoracoscopic Lung Cancer Resection: A Single-Center Randomized Controlled Trial
Authors Liu X ![]() , Zhu H, Zhao Y, Yang Y, Li B
, Zhu H, Zhao Y, Yang Y, Li B ![]() , Wei W, Wei L, Zhang J, Zhang W
, Wei W, Wei L, Zhang J, Zhang W
Received 5 August 2025
Accepted for publication 26 October 2025
Published 12 November 2025 Volume 2025:19 Pages 10061—10073
DOI https://doi.org/10.2147/DDDT.S558129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Xinmin Liu,1,* Haipeng Zhu,2,* Yi Zhao,3 Yulong Yang,3 Bing Li,1 Wenxue Wei,4 Li Wei,4 Jiaqiang Zhang,1 Wei Zhang1
1Department of Anesthesiology and Perioperative Medicine, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China; 2Department of Anesthesiology, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China; 3Department of Anesthesiology and Perioperative Medicine, Henan University People’s Hospital, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China; 4Department of Thoracic Surgery, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Zhang, Department of Anesthesiology and Perioperative Medicine, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China, Tel +86-13838299702, Email [email protected]
Purpose: This study aimed to investigate the effect of nebulized dexmedetomidine on postoperative nausea and vomiting (PONV) in female patients undergoing radical thoracoscopic lung cancer resection.
Patients and Methods: Patients were enrolled and randomized into the nebulized dexmedetomidine group (Dex group) and the normal saline group (NS group). The primary outcome was the overall incidence of PONV within 48 hours postoperatively. Secondary outcomes included the incidence and grade of PONV at multiple postoperative time points (T1: during PACU stay; T2: from PACU discharge to 8 hours postoperatively; T3: 8– 16 hours postoperatively; T4: 16– 24 hours postoperatively; T5: 24– 32 hours postoperatively; T6: 32– 40 hours postoperatively; T7: 40– 48 hours postoperatively), postoperative sore throat (POST), Visual Analogue Scale (VAS) scores at the above time points, use of rescue analgesics and antiemetics, Quality of Recovery 15-item scale (QoR-15) scores et al.
Results: A total of 64 eligible patients were enrolled, with 57 completing the study. There was no statistically significant difference in the overall incidence of PONV within 48 hours postoperatively between two groups. However, the incidence of PONV and POST in the Dex group was significantly lower than that in the NS group at T2. The area under the curve of VAS in the Dex group was significantly lower than that in the NS group within 24 hours and 48 hours postoperatively. The Dex group had a significantly lower rate of rescue analgesic use and higher postoperative QoR-15 scores within 48 hours postoperatively compared with the NS group.
Conclusion: Nebulized inhalation of 1 μg/kg dexmedetomidine preoperatively can reduce the incidence of early postoperative PONV, enhance postoperative analgesia, alleviate postoperative sore throat, and improve postoperative recovery quality in female patients undergoing radical lung cancer surgery.
Trial Number and Registry Url: Registration number, ChiCTR2400086070; https://www.chictr.org.cn/bin/project/edit?pid=235076.
Keywords: postoperative nausea and vomiting, nebulized inhalation, female, lung cancer surgery, dexmedetomidine
Introduction
Postoperative nausea and vomiting (PONV) remain a common perioperative complication. Clinical evidence indicates that the overall incidence of postoperative nausea and vomiting (PONV) following general anesthesia ranges from 20% to 30%, and can be as high as 80% in high-risk populations without prophylactic interventions. This issue severely impedes patients’ postoperative recovery.1 Females have a 2–3 folds higher incidence of PONV than males, making gender a strong risk factor.2
Current management of PONV adopts a multidimensional approach, with pharmacotherapy as the cornerstone. Commonly used agents include 5-HT3 receptor antagonists, dopamine receptor antagonists, glucocorticoids, and anticholinergics.3,4 However, these drugs have specific limitations: 5-HT3 antagonists may cause headache, dizziness, or QT interval prolongation;5–7 dopamine antagonists can lead to drowsiness or extrapyramidal reactions; and anticholinergics are limited by cognitive impairment and xerostomia. Given ongoing controversies regarding drug metabolism, duration of efficacy, and optimal dosing, safer and more effective strategies for PONV management are urgently needed.
Dexmedetomidine (Dex), a selective α2-adrenergic receptor agonist, has attracted increasing attention due to its opioid-sparing effect, reduction in anesthetic requirements, central sympathetic inhibition, non-respiratory sedation mimicking natural sleep, and dose-dependent cardiovascular regulation.6,8,9 Its anti-PONV mechanisms include: 1) central antiemetic effects through modulation of noradrenergic neurotransmission in the nucleus accumbens and inhibition of 5-hydroxytryptamine release;10 and 2) indirect reduction of nausea triggers via opioid-sparing effects. A prospective randomized trial in patients undergoing lung cancer lobectomy showed that intraoperative Dex (0.5 μg/kg/h) reduced the 24-hour incidence of PONV and opioid consumption compared with controls.11 Additional studies have confirmed that intravenous Dex infusion reduces PONV.12,13 Nevertheless, intravenous Dex is associated with serious adverse events, particularly hypotension and bradycardia.14
Nebulized inhalation of Dex has been proposed as a route with less hemodynamic impact, avoiding transient bradycardia and hypotension.15,16 Studies demonstrated that nebulized Dex improves laryngoscopy tolerance and attenuates stress responses during intubation without adverse effects.17,18 Bhalotra et al showed that nebulized Dex (1 μg/kg) for awake intubation provides efficacy comparable to intravenous administration, with better post-intubation comfort and reduced mucosal spraying.19
In summary, while Dex shows significant anti-PONV potential,6,8,10 its intravenous use is limited by side effects such as bradycardia and hypotension in clinical practice.14 Nebulized inhalation, a non-invasive route, has shown clinical advantages in reducing systemic adverse effects.17,18 Most existing research focuses on intravenous Dex, leaving the preventive effect and mechanism of nebulized Dex on PONV unclear. This randomized controlled trial aims to evaluate the impact of nebulized Dex on the incidence of PONV in female patients, exploring its correlation with postoperative pain and rehabilitation metrics to optimize perioperative PONV management.
Materials and Methods
Study Subjects
Female patients scheduled for elective radical thoracoscopic lung cancer resection at the Department of Thoracic Surgery, Henan Provincial People’s Hospital, between April 2, 2024, and January 31, 2025, were enrolled. The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Review Committee of Henan Provincial People’s Hospital [(2024) Ethical Review No. 68] and registered in the China Clinical Trial Registry (ChiCTR2400086070). Written informed consent was obtained from all participants.
Inclusion criteria: female patients undergoing elective radical thoracoscopic lung cancer resection; age <75 years; ASA physical status I–III; undergoing intravenous general anesthesia; estimated surgery duration >1 hour. Exclusion criteria: history of thoracic surgery; receipt of analgesics (including opioids), antiemetics, or adrenocorticotropic hormones within 24 hours preoperatively; patients receiving radiotherapy perioperatively; severe cardiovascular/cerebrovascular diseases or hepatic/renal dysfunction; cognitive impairment or poor compliance affecting postoperative efficacy assessment; postoperative intensive care unit (ICU) admission; change in surgical procedure; patient withdrawal of informed consent or lost to follow-up.
Eligible patients were randomized using a computerized system into two groups for different pretreatment: patients in the nebulized Dex group inhaled 5 mL normal saline containing 1 μg/kg dexmedetomidine using a handheld micromesh nebulizer 30 minutes before anesthesia induction (in a seated position, with a lip-occluded mouthpiece, and voluntary oral-nasal inhalation during calm respiration), while patients in the NS group received 5 mL normal saline nebulization using the same method.
Procedure
Surgeons, anesthesiologists, follow-up staff, statisticians, and patients were blinded to group allocation. Preoperatively, peripheral venous access was established, and vital signs (HR, SpO2, NIBP, ECG) were monitored. Ultrasound-guided internal jugular vein and radial artery cannulation were performed. After puncture, nebulization was administered according to the subject number pending surgery. An anesthesiology nurse blinded to the study prepared the agents for each group in identical 5 mL syringes, which were then sealed in sequentially numbered envelopes. This study used a computer-based randomization system to assign eligible subjects into two groups receiving different pretreatment regimens: Dex group, patients inhaled 5 mL of normal saline solution containing 1 μg/kg dexmedetomidine via a handheld mesh nebulizer (Model YS-68; Guangdong Shunde Tongtai Medical Technology Co., Ltd., Foshan, China) 30 minutes before anesthesia induction; NS group, patients received nebulization with an equal volume (5 mL) of normal saline at the same time point, following the same procedures as the Dex group. During administration, patients remained seated with lips sealed around the mouthpiece and performed spontaneous inhalation through the oral-nasal route during calm breathing.
Emergency unsealing documents were stored in sealed envelopes and accessed solely for treatment adjustment in cases of severe adverse reactions.
Anesthesia induction/maintenance: Upon admission to the operating room, 5 mg dexamethasone and 0.5 mg penehyclidine hydrochloride were administered. Anesthesia induction was achieved with intravenous administration of 0.03–0.05 mg/kg midazolam, 0.3–0.5 μg/kg sufentanil, 0.1–0.4 mg/kg etomidate, and 0.6–1.0 mg/kg rocuronium. After double-lumen endotracheal intubation (35-Fr), propofol combined with remifentanil was administered to maintain BIS at 40–60; cisatracurium was added as needed for muscle relaxation. 5 mg tolansetron was administered 20 minutes before the end of surgery.
Intraoperative management: Volume-controlled ventilation was used to maintain end-tidal CO2 35–45 mmHg. Hemodynamic goals: MAP/HR fluctuations ≤20% of baseline. 2–12 μg/min norepinephrine was administered when MAP decreased by more than 20%; a 0.2 mg bolus of nicardipine was given when MAP increased by more than 20%; 0.3 mg atropine was used when HR decreased by more than 20%. Postoperative analgesia: 0.5 mg/kg oxycodone and 10 mg tropisetron were diluted to 100 mL (background infusion: 2 mL/h, bolus: 2 mL, lockout: 15-minute).
Anesthesia recovery: In the PACU, neuromuscular blockade was antagonized with neostigmine combined with atropine. Patients with a Steward’s awakening score ≥4 and stable vital signs were transferred to the ward. Rescue medications were given for pain/PONV by ward physicians.
Demographics and Perioperative Variables
Baseline data included age, height, weight, American Society of Anesthesiologists (ASA) physical status, history of hypertension, history of diabetes, history of motion sickness or PONV, history of non-thoracic surgery, Apfel score, preoperative anxiety score, total infusion volume, blood loss, urine volume, surgery time, anesthesia duration, intraoperative sufentanil, intraoperative remifentanil, intraoperative propofol, intraoperative norepinephrine, atropine, and PACU stay duration.
Outcomes
The primary outcome of this study was the overall incidence of PONV within 48 hours postoperatively. Secondary outcomes included: incidence/grade of PONV at multiple postoperative time points (T1: during PACU stay; T2: from PACU discharge to 8 hours postoperatively; T3: 8–16 hours postoperatively; T4: 16–24 hours postoperatively; T5: 24–32 hours postoperatively; T6: 32–40 hours postoperatively; T7: 40–48 hours postoperatively); POST; hoarseness; postoperative VAS scores (PACU, 8 h, 16 h, 24 h, 32 h, 40 h, 48 h postoperatively); AUC of VAS scores over 24 hours and 48 hours postoperatively; intraoperative use of vasoactive drugs; PACU stay duration; number of PCIA presses within 48 hours; sleep quality scores; use of rescue analgesics/antiemetics; first oral intake time, first solid food time, first ambulation time; and postoperative QoR-15 scores.
Sample Size
Using PASS statistical software, this prospective, double-blind, randomized controlled trial randomized participants into the nebulized dexmedetomidine (Dex) group or normal saline (NS) group, with the primary endpoint defined as the incidence of PONV within 48 hours postoperatively. Pilot data showed that the incidence of PONV in female patients undergoing thoracic surgery was approximately 65%, while that in the Dex group was approximately 33%. Under a two-sided test framework with a significance level of α=0.05 and statistical power of 80%, and after accounting for an expected 15% loss-to-follow-up rate, the final sample size calculation determined that a total of 64 participants were required for both groups.
Statistical Analysis
Statistical analyses were performed using SPSS 27.0. Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (Mean ± SD), and intergroup comparisons were performed using the independent samples t-test. Non-normally distributed data were reported as median (interquartile range, Median (IQR)), with group comparisons using the Mann–Whitney U-test. Categorical variables were described as frequencies (percentages). For nominal categorical variables, intergroup comparisons were performed using the Pearson χ2-test or Fisher’s exact test based on theoretical frequencies. Ordered categorical variables were compared between groups using the Mann–Whitney U-test. Statistical significance was set at a two-tailed α=0.05, with p < 0.05 indicating statistical significance.
Results
Characteristics of Patients
68 patients were assessed for eligibility, and 4 patients declined to participate. A total of 64 female patients scheduled for radical thoracoscopic lung cancer resection at Henan Provincial People’s Hospital between April 2, 2024, and January 31, 2025, were enrolled, with 57 completing the study (29 in the Dex group and 28 in the NS group). Reasons for attrition included 2 conversions from thoracoscopic to open surgery, 2 voluntary withdrawals, 2 postoperative ICU admissions, and 1 loss to follow-up (Figure 1).
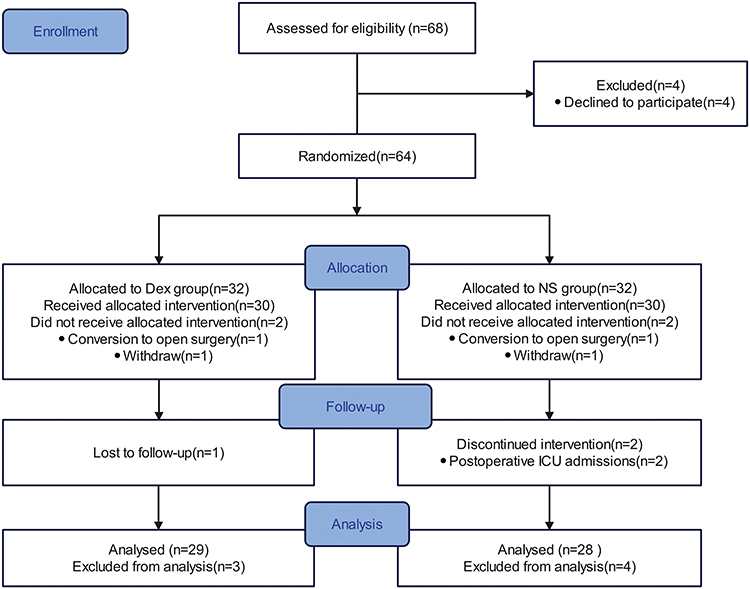 |
Figure 1 Flow chart of this study. |
Baseline characteristics, including age, height, weight, history of motion sickness/PONV, smoking status, history of hypertension/diabetes, preoperative anxiety scores, and Apfel simplified risk scores, showed no significant intergroup differences (Table 1). Intraoperative parameters were also comparable between the two groups (p>0.05) (Table 2).
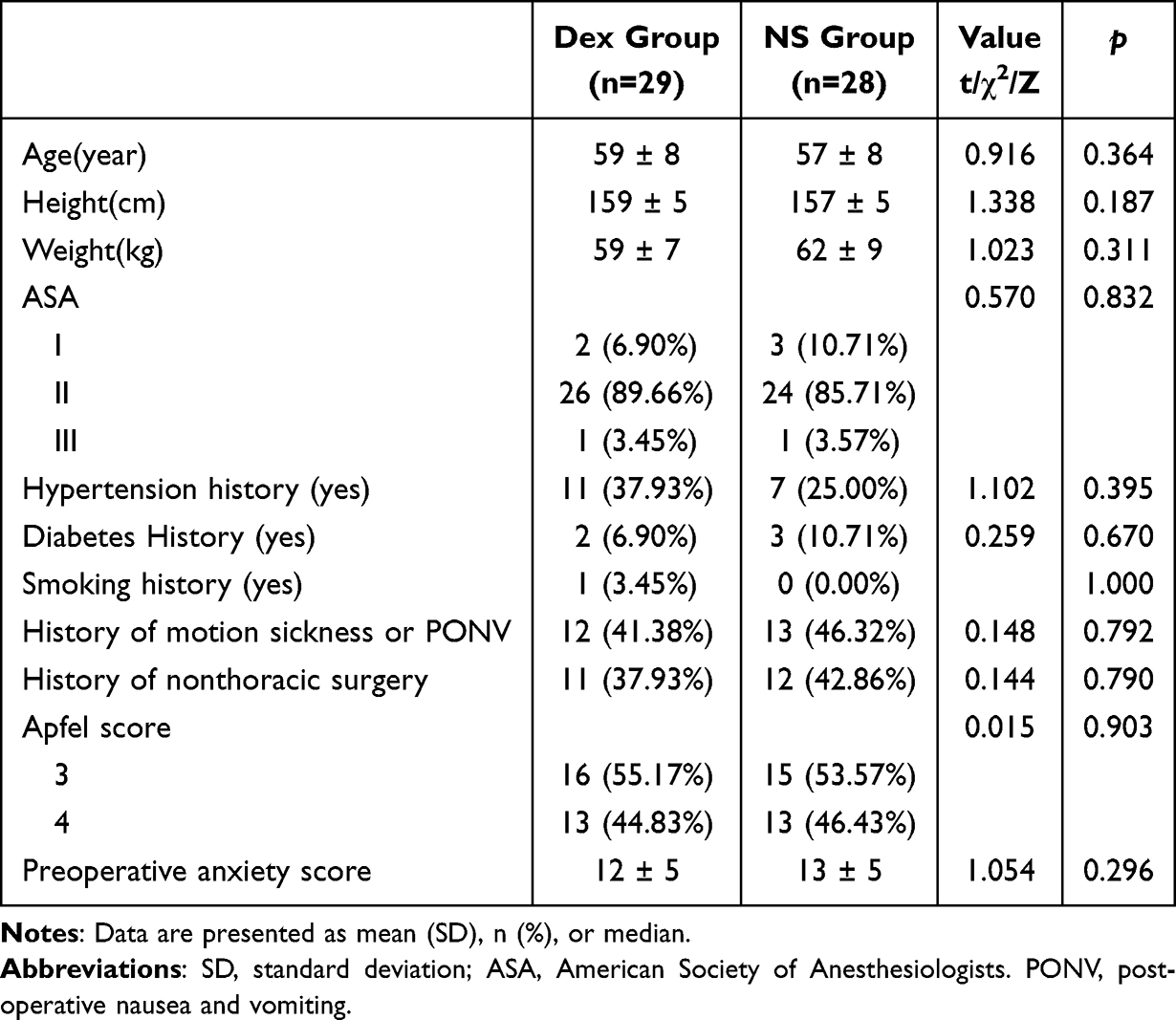 |
Table 1 Patients Characteristics |
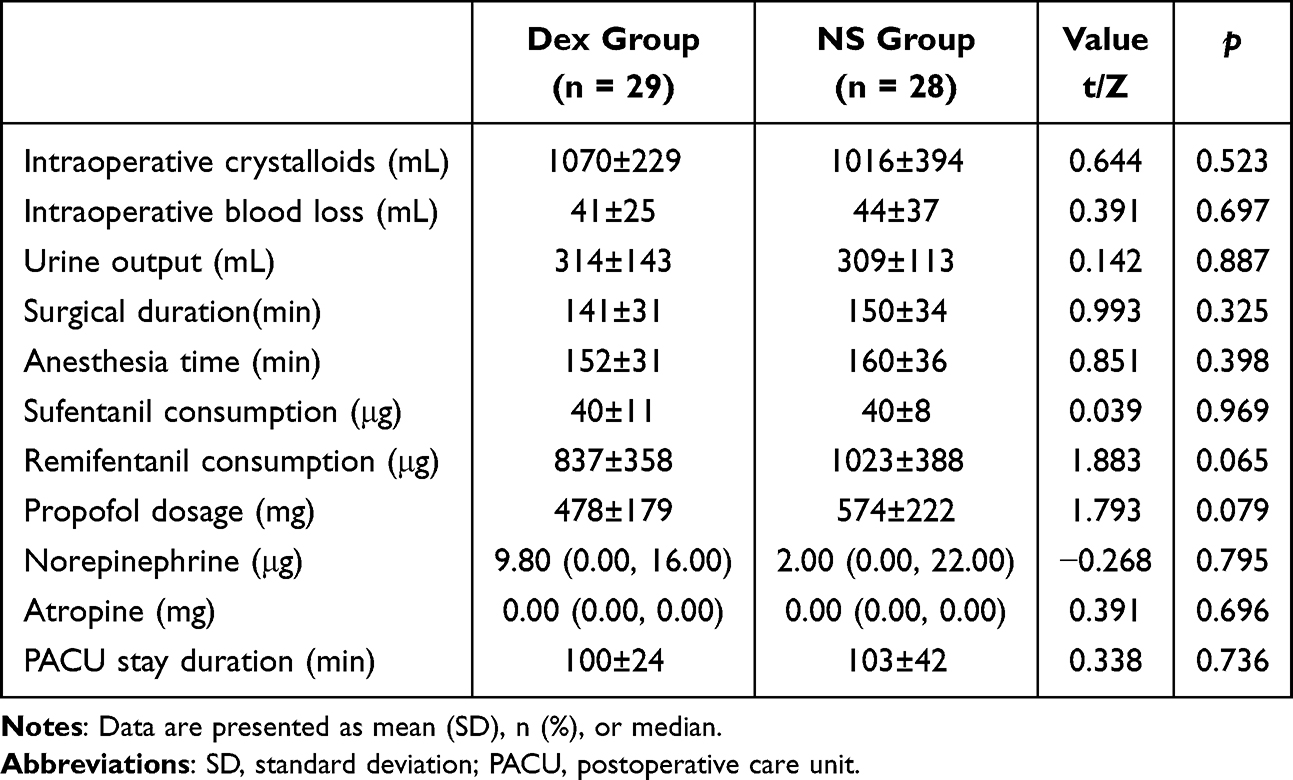 |
Table 2 Intraoperative Baseline Data |
Primary Outcome
There was no statistically significant difference in the overall incidence of PONV within 48 hours postoperatively between the two groups (55.17% vs 60.71%, p=0.672) (Table 3). This indicates that nebulized dexmedetomidine failed to reduce the overall incidence of postoperative nausea and vomiting (PONV) within 48 hours postoperatively.
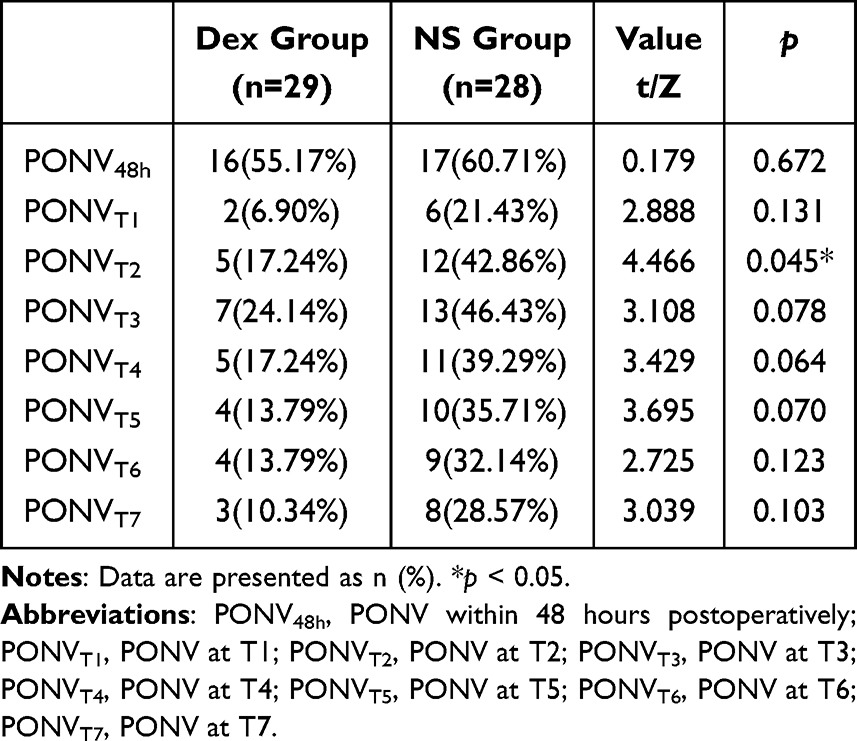 |
Table 3 Comparison of PONV Incidence at Different Postoperative Time Points |
Secondary Outcomes
PONV Incidence and Grade
A statistically significant difference in the incidence of PONV was observed between the Dex and NS groups during the postoperative T2 period (17.24% vs 42.86%, p=0.045), with the Dex group having a lower incidence (Figure 2). There were no significant differences in PONV grades between the two groups across all postoperative time periods (T1-T7) (Figure 2 and Table 4). This indicates that nebulized dexmedetomidine reduced the incidence of early PONV.
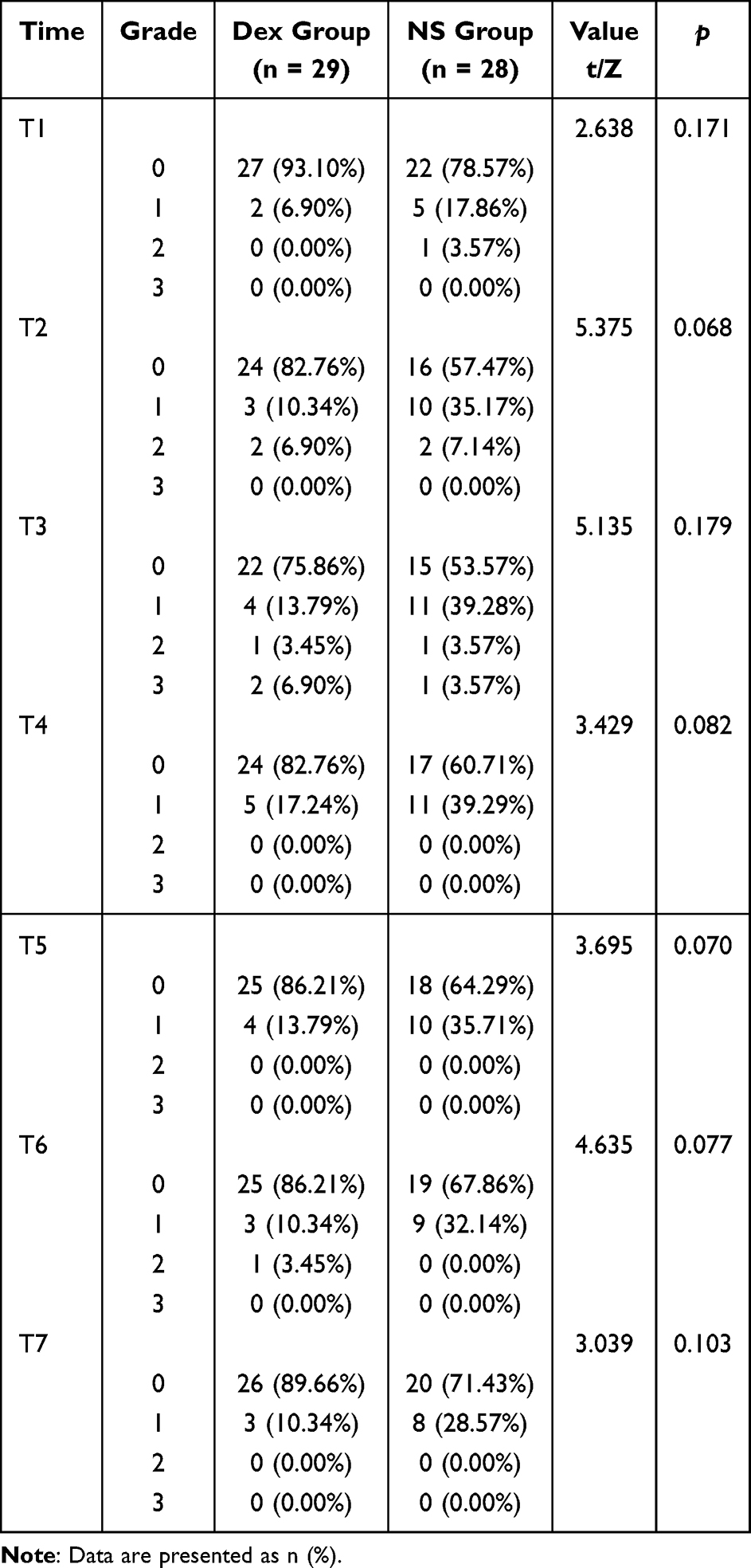 |
Table 4 Comparison of PONV Grades at Different Periods |
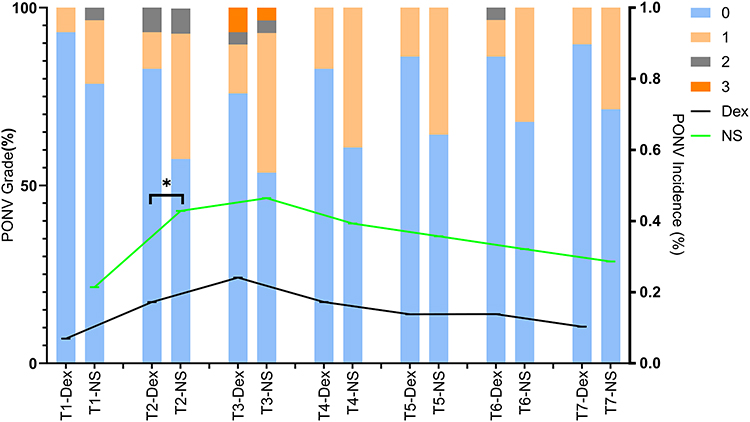 |
Figure 2 Comparison of PONV incidence and grade at different periods. The x-axis represents postoperative time points, the left vertical axis indicates the incidence rate of different grades of PONV, and the right vertical axis indicates the incidence rate of PONV. At time point T2, the dexmedetomidine group showed a significantly lower incidence of PONV compared to the normal saline (NS) group. There was no statistically significant difference in PONV grades between the two groups at any postoperative time point. *p< 0.05. Abbreviations: Dex, Dex group; NS, NS group. |
Postoperative Pain
There was no statistically significant difference in VAS scores between the two groups at all postoperative time points; however, the area under the curve (AUC) of VAS in the Dex group was significantly lower than that in the NS group within 24 hours and 48 hours postoperatively (Table 5). This indicates that nebulized dexmedetomidine improved the overall analgesic effect during the first two postoperative days.
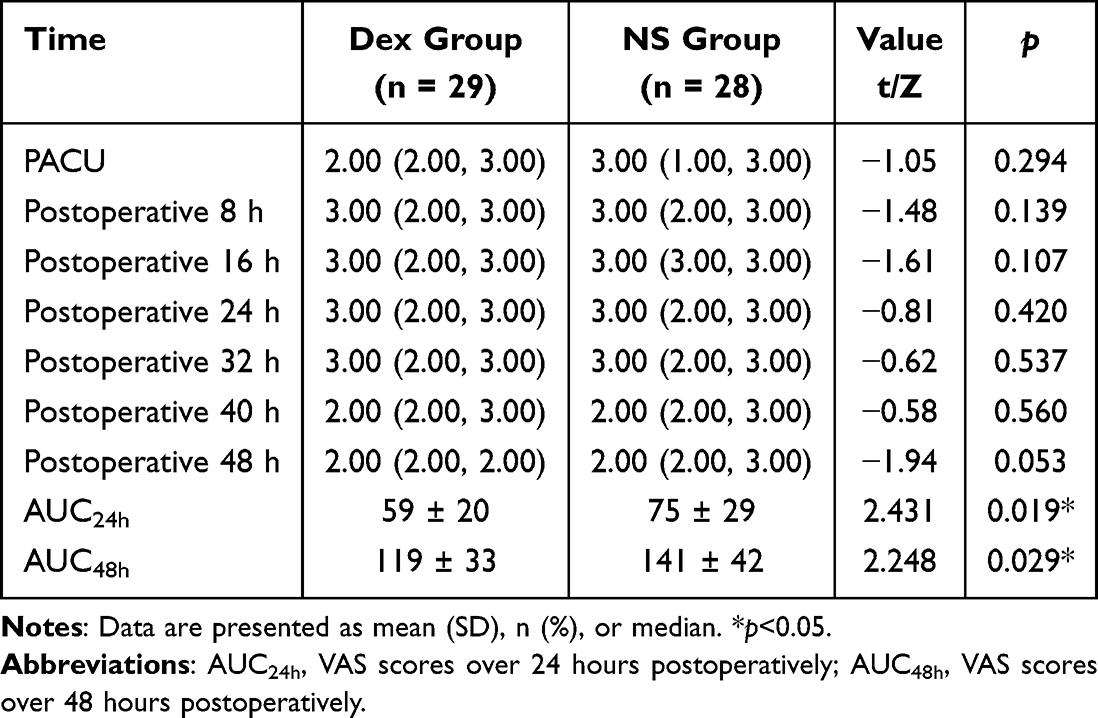 |
Table 5 Comparison of Postoperative VAS Scores at Different Time Points Between Groups |
Further analysis of time-dependent VAS pain score curves using the Area Under the Curve (AUC) method revealed significant intergroup differences. The AUC values from the Post-Anesthesia Care Unit (PACU) to 24 hours postoperatively were 59±20 in the Dex group and 75±29 in the NS group (p=0.019), indicating a lower cumulative pain burden in the Dex group. Similarly, the AUC from PACU to 48 hours postoperatively also showed a statistically significant reduction in the Dex group compared with the NS group (Table 5). The AUC values from the Post-Anesthesia Care Unit (PACU) to 48 hours postoperatively were 119±33 in the Dex group and 141±42 in the NS group (p=0.029).
POST Incidence and Grade
Nebulized dexmedetomidine improved sore throat in the early postoperative period. There was no statistically significant difference in the overall incidence of postoperative sore throat (POST) within 48 hours postoperatively between the two groups (27.6% vs 50.0%, p=0.082). However, a statistically significant difference was observed in the incidence of POST during the T2 period, with the Dex group having a lower incidence (17.2% vs 42.9%, p=0.035) (Figure 3).
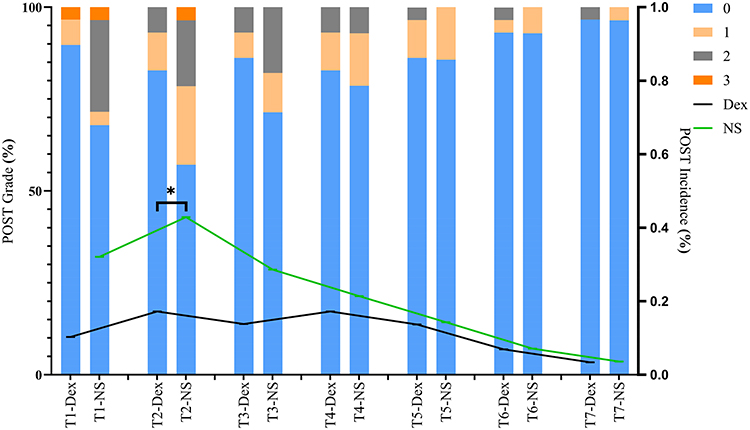 |
Figure 3 Comparison of POST incidence and grade at different postoperative time periods. The x-axis represents time, the left vertical axis depicts POST grades, and the right vertical axis indicates the incidence of postoperative sore throat (POST). At time point T2, a statistically significant difference in the incidence of POST was observed between the two groups, with the Dex group having a significantly lower incidence than the NS group (*p<0.05). However, there was no statistically significant difference in POST grades between the groups. Abbreviations: Dex, Dex group; NS, NS group. |
Regarding POST severity grading, significant intergroup differences were noted during both T1 (p=0.038) and T2 (p=0.032) periods, with patients in the Dex group having lower POST grades than those in the NS group in both time intervals (Figure 3).
Postoperative Hoarseness
There were no statistically significant intergroup differences in the overall incidence of postoperative hoarseness within 48 hours postoperatively, or in the incidence and grading of hoarseness across all time periods from T1 to T7 (p>0.05) (Figure 4).
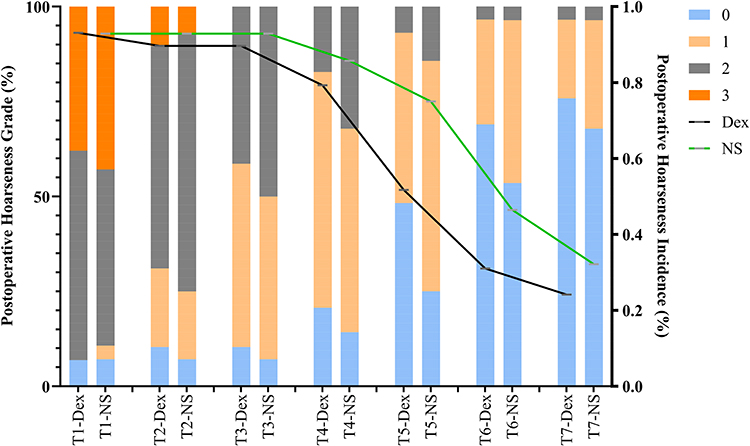 |
Figure 4 Comparison of postoperative hoarseness incidence and grade at different time periods. The x-axis represents time, the left vertical axis depicts postoperative hoarseness grades, and the right vertical axis indicates the incidence of postoperative hoarseness. No statistically significant differences in either postoperative hoarseness grades or incidence were found between the two groups. |
Postoperative Recovery
There were no statistically significant intergroup differences in postoperative sleep scores at 48 hours, administration of rescue antiemetic medications, time to first oral water intake, first food intake, or first out-of-bed activity (p>0.05) (Table 6). In contrast, the Dex group had a significantly lower rate of rescue analgesic use within 48 hours postoperatively compared with the NS group (13.79% vs 39.29%, p=0.038) (Table 6). Additionally, the Dex group had significantly higher postoperative QoR-15 scores (101±13 vs 92±10, p=0.006), indicating better recovery quality (Table 6). This indicates that, consistent with the previous AUC results of the VAS scores, nebulized dexmedetomidine improved the quality of early postoperative analgesia and also enhanced the quality of postoperative recovery.
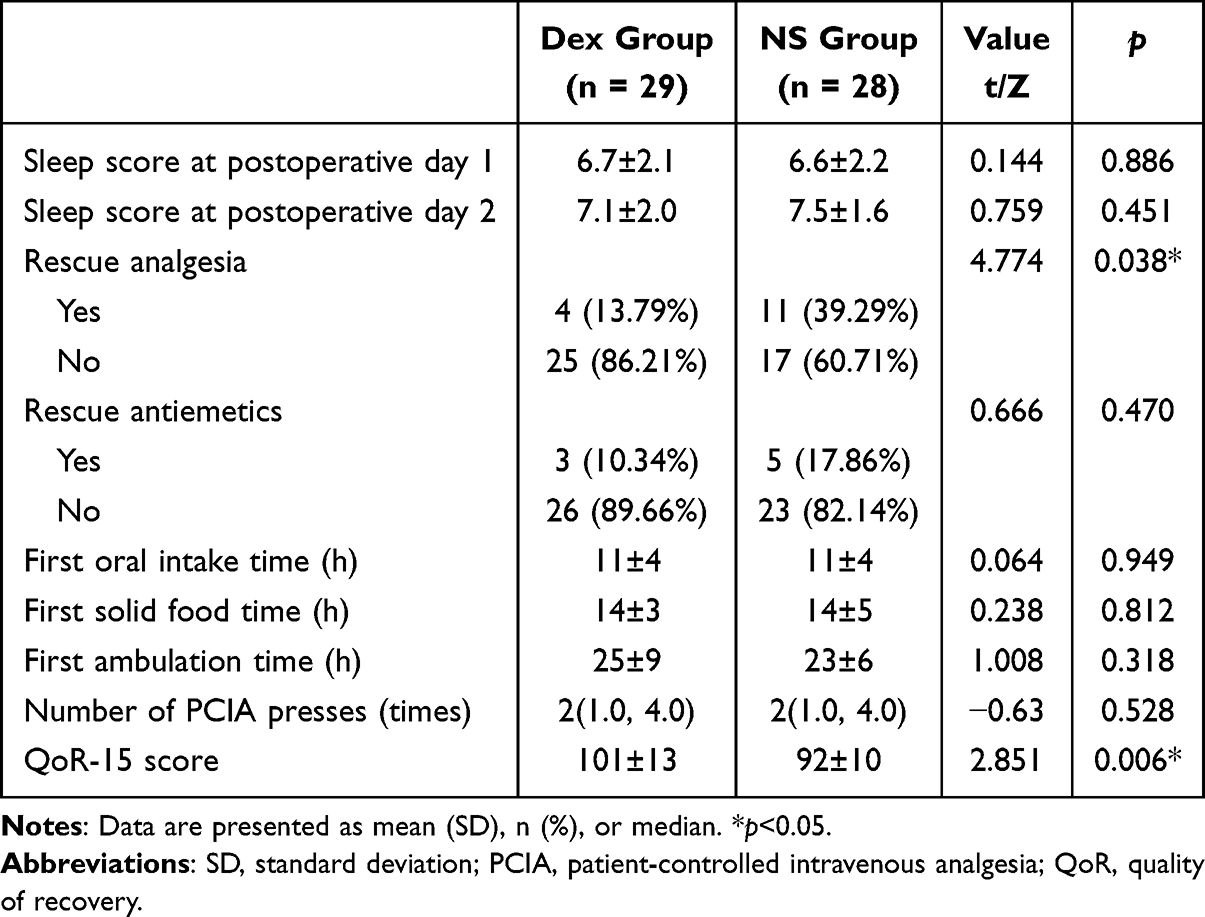 |
Table 6 Comparison of Postoperative Rehabilitation Outcomes Between the Two Groups |
Discussion
To our knowledge, this is the first study to investigate the effect of nebulized 1 μg/kg Dex on the incidence of PONV in female patients undergoing radical thoracoscopic lung cancer surgery. The study yielded two main findings: 1. preoperative Dex nebulization reduced the incidence of early postoperative nausea and vomiting; 2. preoperative Dex nebulization decreased the AUC of VAS scores over 24 and 48 hours postoperatively, reduced the incidence and severity of POST, decreased the need for rescue analgesia, and improved postoperative recovery quality. This is the first study to adopt nebulized dexmedetomidine administration for female patients a high risk population for PONV. Given the safety, non-invasiveness, and efficacy of nebulization, our study provides a novel method for reducing the incidence of PONV in female patients undergoing this type of surgery.
Bhalotra’s study demonstrated that nebulized dexmedetomidine administration is associated with significantly lower incidences of bradycardia and hypotension compared with intravenous infusion.19 Nebulization represents an important administration route for dexmedetomidine, and research has shown that preoperative inhalation of 1 μg/kg dexmedetomidine effectively reduces postoperative VAS pain scores.20 A retrospective study indicates that the optimal intravenous dose of dexmedetomidine for reducing PONV ranges from 50–100 μg, while the optimal dosage of nebulized dexmedetomidine for PONV prevention remains unclear. In this study, a 1 μg/kg dexmedetomidine nebulization regimen was selected based on preclinical testing and previous studies. Although preoperative nebulization of 2 μg/kg dexmedetomidine has been reported to facilitate pediatric sedation without severe adverse events, preliminary testing in adults revealed a 50% incidence of bradycardia with this dosage, presumably due to excessive α2-receptor-mediated sympathetic inhibition. Thus, 1 μg/kg was adopted in this study.
The period of 24–48 hours postoperatively is a high-incidence window for PONV. In this study, the incidence of PONV within 48 hours postoperatively was set as the primary outcome, and we found that preoperative nebulization of 1 μg/kg dexmedetomidine failed to reduce this primary outcome. We hypothesize that the underlying reasons may be as follows: first, dexmedetomidine has a relatively short elimination half-life of only 2–4 hours, so the efficacy of a single dose administered before anesthesia induction may not extend to a longer postoperative period; second, the patients enrolled in this study were inherently a high-risk population for PONV, which requires a combination of multiple interventions for management.
Given that the occurrence of PONV exhibits time-dependent dynamic characteristics, our analysis of secondary outcomes also revealed that the incidence of PONV during the postoperative T2 time period was lower in the nebulized dexmedetomidine group than in the control group. This indicates that our intervention can still significantly reduce the incidence of PONV during the early postoperative recovery phase. This is consistent with Wang et al’s report of a transient reduction in PONV (<6 hours) with dexmedetomidine11 and Miller’s team’s finding that nebulized dexmedetomidine peaks within 60 minutes, maintains therapeutic levels briefly, and has a half-life of 2 hours, precluding 48-hour coverage.13 Previous studies have shown that intravenous administration of dexmedetomidine before surgery can reduce the incidence of early postoperative nausea in high-risk populations with three risk factors, which also supports the results of our current study.21
Dexmedetomidine exerts analgesic effects by activating spinal and brainstem α2 receptors, inhibiting nociceptive signaling and central sensitization, while suppressing substance P release from spinal dorsal horn neurons to reduce cortical pain transmission.22 A study on cesarean delivery demonstrated that 1 μg/kg nebulized dexmedetomidine alleviates postoperative headache.23 Consistently, our study found that the Dex group had a significantly smaller AUC of VAS scores from PACU to 24 hours and 48 hours postoperatively than the NS group. Reduced postoperative rescue analgesiadespite comparable intraoperative remifentanil use suggests that dexmedetomidine reduces opioid requirements via synergistic analgesia, potentially contributing to PONV suppression. Collectively, dexmedetomidine may reduce perioperative opioid consumption and the demand for rescue analgesia through multimodal analgesia.
Large-caliber tracheal tubes are a recognized risk factor for POST.24,25 Thoracic surgery requires double-lumen endobronchial intubation for one-lung ventilation, which carries a higher risk of POST than single-lumen tubes.26 Notably, nebulized dexmedetomidine reduced the early incidence of POST in this trial, consistent with the findings of Thomas et al in thyroidectomy.27 Due to its unique local aerosol absorption characteristics, dexmedetomidine can act directly on the glottic region, thereby reducing the incidence of postoperative sore throat. This may involve both analgesic and anti-inflammatory mechanisms: dexmedetomidine inhibits TLR4/NF-κB-mediated release of IL-1β, TNF-α, IL-6, and MCP-1, attenuating intubationinduced local inflammation.28,29
Despite the absence of intergroup differences in postoperative ambulation latency and sleep scores, the Dex group had significantly higher QoR-15 scores, reflecting improved overall satisfaction with the recovery experience. The QoR-15 scale, a multidimensional assessment encompassing nociception, emotional state, and instrumental activities of daily living, showed score improvement potentially linked to reduced early-phase PONV, alleviated dysphagia, and optimized analgesia control. In addition to its roles in enhancing postoperative analgesia, preventing PONV, and relieving POST, the anxiolytic efficacy of dexmedetomidine supported by robust evidence likely reduces postoperative anxiety by inhibiting noradrenaline release in the nucleus accumbens, thereby improving overall recovery satisfaction.30 Collectively, these findings indicate that nebulized dexmedetomidine improves the overall perception of postoperative recovery.
This study has some limitations. First, only a fixed 1 μg/kg preinduction protocol was used. Trials of 2 μg/kg dexmedetomidine nebulization were prematurely terminated due to hemodynamic instability. Second, the study did not explore administration timing (preoperative/intraoperative/postoperative) or dose-response relationships. Third, the single-center design necessitates multicenter validation to confirm external validity. Fourth, although intravenous dexmedetomidine has been shown to downregulate PONV-associated neurotransmitters (eg, serotonin, substance P), this study did not dynamically monitor these mediators, limiting the clarification of mechanisms.
Conclusion
Preoperative nebulized inhalation of 1 μg/kg dexmedetomidine before anesthesia induction significantly reduces the incidence of early postoperative PONV, enhances postoperative analgesic efficacy, reduces the occurrence of postoperative sore throat, and improves postoperative recovery quality in female patients undergoing radical lung cancer surgery. For female patients undergoing video-assisted thoracoscopic radical resection of lung cancer, preoperative nebulized dexmedetomidine is recommended to reduce the incidence of PONV.
Abbreviations
PONV, Postoperative Nausea and Vomiting; Dex, Dexmedetomidine; BIS, Bispectral Index; QoR-15, Quality of Recovery-15; PACU, Post-Anesthesia Care Unit; VAS, Visual Analogue Scale; AUC, Area Under the Curve; NS, Normal Saline; POST, Postoperative Sore Throat; VATS, Video-Assisted Thoracoscopic Surgery; ICU, Intensive Care Unit; PCIA, Patient-Controlled Intravenous Analgesia; 5-HT, 5-Hydroxytryptamine; ASA, American Society of Anesthesiologists; NIBP, Non-Invasive Blood Pressure; SpO2, Peripheral Oxygen Saturation; MAP, Mean Arterial Pressure; HR, Heart Rate; FiO2, Fraction of Inspired Oxygen; ECG, Electrocardiogram; ERAS, Enhanced Recovery After Surgery; IBP, Invasive Blood Pressure.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding author if reasonable.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Henan Provincial People’s Hospital, No. 7, Weiwu Road, Zhengzhou, Henan, China. Written informed consent was obtained from all subjects participating in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Medical Science and Technology Research Plan Joint Construction Project of Henan Province (LHGJ20200059) and the Henan Province Middle-aged and Young Health Science and Technology Innovation Outstanding Youth Talent Training Project (grant NO. YXKC2021025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang N, Ding P, Zheng D-Y, et al. Wearable transcutaneous electrical acupoint stimulation bracelet for prevention of postoperative nausea and vomiting in patients undergoing hysteroscopic surgery: a randomised controlled trial. Br J Anaesth. 2022;129(4):e85–e87. doi:10.1016/j.bja.2022.06.028
2. Apfel CC, Heidrich FM, Jukar-Rao S, et al. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br J Anaesth. 2012;109(5):742–753. doi:10.1093/bja/aes276
3. Weibel S, Rücker G, Eberhart LH, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev. 2020;10(10):CD012859. doi:10.1002/14651858.CD012859.pub2
4. Chen W, Li G, Jiang K, et al. Dexamethasone for postoperative nausea and vomiting in papillary thyroid carcinoma patients: a randomized clinical trial. J Am College Surg. 2022;235(3):454–467. doi:10.1097/XCS.0000000000000309
5. Tricco AC, Soobiah C, Blondal E, et al. Comparative efficacy of serotonin (5-HT3) receptor antagonists in patients undergoing surgery: a systematic review and network meta-analysis. BMC Med. 2015;13(1):136. doi:10.1186/s12916-015-0371-y
6. Kovac AL. Comparative pharmacology and guide to the use of the serotonin 5-HT3 receptor antagonists for postoperative nausea and vomiting. Drugs. 2016;76(18):1719–1735. doi:10.1007/s40265-016-0663-3
7. Tricco AC, Blondal E, Veroniki AA, et al. Comparative safety and effectiveness of serotonin receptor antagonists in patients undergoing chemotherapy: a systematic review and network meta-analysis. BMC Med. 2016;14(1):216. doi:10.1186/s12916-016-0761-9
8. Stoops S, Kovac A. New insights into the pathophysiology and risk factors for PONV. Best Pract Res Clin Anaesth. 2020;34(4):667–679. doi:10.1016/j.bpa.2020.06.001
9. Horn CC, Wallisch WJ, Homanics GE et al. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi:10.1016/j.ejphar.2013.10.037
10. De Boer HD, Detriche O, Forget P. Opioid-related side effects: postoperative ileus, urinary retention, nausea and vomiting, and shivering. a review of the literature. Best Pract Res Clin Anaesth. 2017;31(4):499–504. doi:10.1016/j.bpa.2017.07.002
11. Wang X, Wang K, Wang B, et al. Effect of oxycodone combined with dexmedetomidine for intravenous patient-controlled analgesia after video-assisted thoracoscopic lobectomy. J Cardiothoracic Vasc Anesthesia. 2016;30(4):1015–1021. doi:10.1053/j.jvca.2016.03.127
12. Lu Y, Fang -P-P, Yu Y-Q, et al. Effect of intraoperative dexmedetomidine on recovery of gastrointestinal function after abdominal surgery in older adults: a randomized clinical trial. JAMA Network Open. 2021;4(10):e2128886. doi:10.1001/jamanetworkopen.2021.28886
13. Zhang Y, Zhou Y, Hu T, et al. Dexmedetomidine reduces postoperative pain and speeds recovery after bariatric surgery: a meta-analysis of randomized controlled trials. Surg Obesity Related Dis. 2022;18(6):846–853. doi:10.1016/j.soard.2022.03.002
14. Beloeil H, Garot M, Lebuffe G, et al. Balanced opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery: the postoperative and opioid-free anesthesia (POFA) randomized clinical trial. Anesthesiology. 2021;134(4):541–551. doi:10.1097/ALN.0000000000003725
15. Shankar K, Rangalakshmi S, Kailash P et al. Comparison of hemodynamics and opioid sparing effect of dexmedetomidine nebulization and intravenous dexmedetomidine in laparoscopic surgeries under general anesthesia. Asian J Anesthesiol. 2022;60(1):33–40. doi:10.6859/aja.202203_60(1).0005
16. Liu X, Li Y, Kang L, Wang Q. Recent advances in the clinical value and potential of dexmedetomidine. JIR. 2021;14:7507–7527. doi:10.2147/JIR.S346089
17. Misra S, Behera BK, Mitra JK et al. Effect of preoperative dexmedetomidine nebulization on the hemodynamic response to laryngoscopy and intubation: a randomized control trial. Korean J Anesthesiol. 2021;74(2):150–157. doi:10.4097/kja.20153
18. Kumar NRR, Jonnavithula N, Padhy S et al. Evaluation of nebulised dexmedetomidine in blunting haemodynamic response to intubation: a prospective randomised study. Indian J Anaesth. 2020;64(10):874–879.
19. Bhalotra AR, Arya M, Singh R et al. Comparative evaluation of nebulized versus intravenous dexmedetomidine on intubating conditions during awake fiberoptic nasotracheal intubation. J Clin Anesthesia. 2024;95:111461. doi:10.1016/j.jclinane.2024.111461
20. Soliman OM, Aboulfotouh AI, Abdelhafez AM et al. Nebulized dexmedetomidine versus neostigmine/atropine for treating post-dural puncture headache after cesarean section: a double-blind randomized controlled trial. Minerva Anestesiol. 2023;89(10):867–875. doi:10.23736/S0375-9393.22.16906-3
21. Song Y, Shim JK, Song JW, et al. Dexmedetomidine added to an opioid-based analgesic regimen for the prevention of postoperative nausea and vomiting in highly susceptible patients: a randomised controlled trial. Eur J Anaesthesiol. 2016;33(2):75–83.
22. Kaye AD, Chernobylsky DJ, Thakur P, et al. Dexmedetomidine in enhanced recovery after surgery (ERAS) protocols for postoperative pain. Curr Pain Headache Rep. 2020;24(5):21. doi:10.1007/s11916-020-00853-z
23. Soliman OM, Aboulfotouh AI, Abdelhafez AM et al. Nebulized dexmedetomidine versus neostigmine/atropine for treating post-dural puncture headache after cesarean section: a double-blind randomized controlled trial. Minerva Anestesiol. 2021;74(2):150–157.
24. Ali S, Khan A, Ashfaq AD. Comparison of two different sizes of endotracheal tracheal tube for postoperative sore throat in breast cancer patients undergoing surgeries. Cureus. 2021;13(1):e12896. doi:10.7759/cureus.12896
25. El-Boghdadly K, Bailey CR, Wiles MD. Postoperative sore throat: a systematic review. Anaesthesia. 2016;71(6):706–717. doi:10.1111/anae.13438
26. Liang J, Liu J, Qiu Z, et al. Effect of esketamine gargle on postoperative sore throat in patients undergoing double-lumen endobronchial intubation: a randomised controlled trial. DDDT. 2023;17:3139–3149. doi:10.2147/DDDT.S430077
27. Thomas D, Chacko L, Raphael P. Dexmedetomidine nebulisation attenuates post-operative sore throat in patients undergoing thyroidectomy: a randomised, double-blind, comparative study with nebulised ketamine. Indian J Anaesth. 2020;64(10):863–868. doi:10.4103/ija.IJA_406_20
28. Li B, Li Y, Tian S, et al. Anti-inflammatory effects of perioperative dexmedetomidine administered as an adjunct to general anesthesia: a meta-analysis. Sci Rep. 2015;5(1):12342. doi:10.1038/srep12342
29. Puls R, Von Haefen C, Bührer C, Endesfelder S. Dexmedetomidine protects cerebellar neurons against hyperoxia-induced oxidative stress and apoptosis in the juvenile rat. IJMS. 2023;24(9):7804. doi:10.3390/ijms24097804
30. Wei L, Li X, Li T, et al. Effect of dexmedetomidine plus propofol versus propofol alone on postoperative anxiety and depression, efficacy, and satisfaction in patients who undergo painless induced abortion. Tohoku J Exp Med. 2025. doi:10.1620/tjem.2025.J026
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.