Back to Journals » International Journal of Women's Health » Volume 6
Effect of hormonal contraceptives on lipid profile and the risk indices for cardiovascular disease in a Ghanaian community
Authors Asare G, Santa S, Ngala RA ![]() , Asiedu B, Afriyie D, Amoah A
, Asiedu B, Afriyie D, Amoah A
Received 29 December 2013
Accepted for publication 2 April 2014
Published 3 June 2014 Volume 2014:6 Pages 597—603
DOI https://doi.org/10.2147/IJWH.S59852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Video abstract.
Views: 404
George A Asare,1 Sheila Santa,1 Robert A Ngala,2 Bernice Asiedu,1 Daniel Afriyie,3 Albert GB Amoah4
1Department of Medical Laboratory Sciences, University of Ghana School of Allied Health Sciences (SAHS), Korle-bu, Ghana; 2Department of Molecular Medicine, School of Medical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 3Department of Pharmacology, University of Ghana Medical School Korle-bu, Ghana; 4Department of Medicine, University of Ghana Medical School, Korle-bu, Ghana
Background: Hormonal contraceptives (HCs) have been shown to alter lipid profile among various population groups with different patterns of dyslipidemia and cardiovascular (CV) risk. The study aimed at determining the lipid profile pattern and CV risk in a Ghanaian cohort.
Methods: Purposive random sampling was done. Forty-seven and 19 cases were on oral contraceptives (OCs) and injectable contraceptives (ICs), respectively; five were on subdermal implant. Twenty-four non-users served as controls. Biodemographic and lipid profiles were determined. Total cholesterol (TC), high-density lipoprotein cholesterol (HDLC), low-density lipoprotein cholesterol (LDLC), and very-low-density lipid lipoprotein cholesterol (VLDLC), were determined. Castelli index I and II were calculated.
Results: The mean age difference between the HC and control groups was insignificant. However, diastolic blood pressure (BP) differences were significant (P=0.006). The body mass index (BMI) of the OC and IC groups were significantly different from the control group (P=0.003 and P=0.008, respectively). TC levels for the control and case groups were 3.35±0.62 mmol/L and 4.07±0.91 mmol/L, respectively (P=0.002). LDLC levels for the control and case groups were 1.74±0.57 mmol/L and 2.38±0.84 mmol/L, respectively (P=0.003). Castelli index I (TC/HDLC) and II (LDLC/HDLC) were significantly different between the control and OC groups (P=0.026 and P=0.014, respectively). Spearman’s rho correlation showed significant influence of HC use on TG (P=0.026), TC (P=0.000), LDLC (P=0.004), and VLDLC (P=0.026) over time.
Conclusion: HC use is associated with significant increases in BMI, diastolic BP, TC, LDLC, and Castelli index I and II. These changes carry a potential risk in the development of CV disease.
Keywords: oral, injectable, implant, cholesterol, body mass index
Introduction
Seven factors influence cardiovascular (CV) health. The presence of four ideal health behaviors: non-smoking, body mass index (BMI) <25 kg/m2, physical activity at goal level, and diet consistent with current guideline recommendations, defines CV health. Three other factors that contribute to ideal CV health are untreated total cholesterol (TC) ≤200 mg/dL, untreated blood pressure (BP) ≤120/80 mmHg, and untreated fasting blood sugar of ≤100 mg/dL.1
Eight CV risk factors include alcohol use, tobacco use, high BP, BMI >25 kg/m2, high cholesterol, high blood glucose, low fruit and vegetable intake, and low physical activity. These together account for 61% of CV disease deaths2 and over 75% of deaths resulting from ischemic and hypertensive heart diseases.3 One of the four major contributors of non-communicable diseases (NCD) causing morbidity and mortality worldwide is CV disease (CVD). In 2008, this accounted for 31% of all global deaths, of which 80% occurred in developing countries.4 Most middle income countries have been affected by an increasing trend in CVD, while the trend in high income countries is on the decline.5
Metabolic risk factors include obesity,6 hypertension, type 2 diabetes, high serum cholesterol, and dyslipidemia.7 Estrogen also affects the CV system through its impact on CV risk factors such as the lipid profile. Oral contraceptives (OCs) alter the lipid profile through the genomic pathway, in which estrogen receptor alterations affect hepatic apolipoprotein upregulation.8 Studies in pre-menopausal women using OCs have shown a dose-related response in their lipid profiles. Women using a 20 μg ethinyl estradiol (EE)/100 μg levonorgestrel (LNG) OC have demonstrated reductions in high-density lipoprotein cholesterol (HDLC) together with small increases in low-density lipoprotein cholesterol (LDLC), and triglycerides (TG), in contrast to a 30 μg EE/150 μg LNG OC.9 The amount of lipid alteration also depends on the delivery route. A study on women receiving two different types of progestin-only pills (desogestrel 75 μg/day or LNG 30 μg/day) showed that minimal lipid profile changes occurred except for decreasing trends with levels of HDLC, its subfractions, and apolipoprotein-I and -II.10
In Ghana, most women reporting to family planning clinics use Depo-Provera (depot medroxyprogesterone acetate [DMPA]; Pfizer, Inc., New York, NY, USA), an injectable contraceptive (IC), with a few depending on OCs. DMPA is said to increase LDLC and decrease HDLC.11 Additionally, glucose metabolism is affected by decreasing glucose tolerance over time;12 increasing insulin resistance and decreasing beta cell function.13 The effects of estrogen seem to be a contributive factor to metabolic syndrome (MS). The prevalence of MS among medical cases and controls in a hospital in Ghana was 54% and 18%, respectively, with the prevalence increasing with advancing age, using the Adult Treatment Panel III (ATPIII) criteria.14 In another study, the overall prevalence of MS as measured by the International Diabetic Federation (IDF) and ATPIII criteria were 35.9% and 15.0%, respectively, among rural Ghanaians.15 Hypertension and central obesity were the two components with the highest frequency among individuals with MS. However, the impact of ICs and OCs on obesity, MS, and CV disease is not known nationally.
Materials and methods
The study aimed at determining whether hormonal contraceptive (HC) use among Ghanaian women produced any risk factors for the development of dyslipidemia and CV disease markers.
Study site and design
Ethical clearance (MS-ET/M.3-P 3.3/2013-2014) was obtained from the Ethics and Protocol Review Committee of the University of Ghana Medical School (UGMS). Written informed consent was obtained from each patient. This was a community study of adult females from the Zongo Community attending a Reproductive Healthcare Clinic in Wa, Ghana. Subjects who were already on HCs were recruited. Purposive random sampling technique was used.16 The inclusion criteria were as follows: females between the ages of 20 and 49 years; females on OCs, ICs, and subdermal implant (IMP) contraceptives; and females without predisposing factors or conditions to CV disease prior to contraceptive use. Furthermore, females who had never used any form of contraceptives were used as age-matched controls. The exclusion criteria included the following: females on other forms of contraceptives other than OCs, ICs, and IMPs; females below 20 years and females above 49 years. Details of contraceptive type and hormonal content were noted and later classified. Types of OCs used by participants were; progesterone-only HC pill (0.035 mg norethindrone) and the combined OC pill (0.03 mg EE and 0.15 mg LNG). The mean duration of use of all HCs was 60.08 months. The Helsinki Declaration of 1964, with revision in October 2008 was observed. In all, 71 cases attending the clinic were sampled, alongside 24 age-matched controls.
Data and blood sample collection
A questionnaire was administered to obtain basic information on age, duration of drug use, contraceptive type, etc. Anthropometric measurement was obtained by measuring height using a portable stadiometer (Seca GmbH & Co, KG, Hamburg, Germany). Height was recorded to the nearest 0.1 cm, with subjects barefooted. Weight was measured using a Seca 770 floor digital scale to the nearest 0.1 kg, with subjects in minimum clothing. BMI was computed as (weight [kg])/(height [m])2. BP was measured three times on the left arm with a 5-minute break in between using the Omron 705 CP oscillometric monitor (Kyoto, Japan). The mean of the three measurements was used. Cases with BP readings ≥140/90 mmHg were regarded as hypertensive. Three milliliter blood samples were taken from all subjects into gel separator tubes. After clotting, blood samples were centrifuged at 3,000 rpm for 10 minutes. Serum was aliquoted into Eppendorf tubes and stored at −20°C until use.
Biochemical analysis
TC, HDLC, LDLC, TG, and very-low-density lipoprotein cholesterol (VLDLC) tests were conducted using Biosystem kits on an A25 Biosystem autoanalyzer (Barcelona, Spain).
Statistical analysis
SPSS software (v20.0; IBM Corporation, Armonk, NY, USA) was used for data management and statistical analysis. The results were expressed as mean ± standard deviation. Differences in continuous data were compared using Student’s t-test (two groups) and one-way analysis of variance (ANOVA; three or more groups) followed by the Bonferroni post-hoc test. Relationships between variables were ascertained by Spearman’s correlation coefficient. All results were considered significant at the 5% level of probability.
Results
The age range of cases was 20–49 years and that of the controls, 20–47 years. The mean ages of the two groups were 30.93±5.84 years (cases) and 29.25±8.09 years (control) and were not statistically significantly different. Of the cases, 19 were on OCs (progesterone-only pill [0.035 mg norethindrone] or combined estrogen and progesterone [0.03 mg EE and 0.15 mg LNG]), 47 were on an IC (Depo-Provera [150 mg medroxyprogesterone]), and five were on a subdermal contraceptive IMP (the subdermal IMP was a progesterone-only contraceptive also known as Implanon [Merck & Co, Inc., Whitehouse Station, NJ, USA]. This off-white, non-biodegradable rod contains 68 mg etonogestrel, with a release rate of approximately 0.060–0.070 mg/day in week 5–6, followed by a decline to approximately 0.035–0.045 mg/day at the end of the first year).
The mean duration of contraceptive use was 60.08 months. Prolonged bleeding (n=15), abdominal pain (n=7), and weight gain (n=3) were reported by cases.
The BMI for the case group was 25.34±4.4 kg/m2, while that of the control group was 21.73±0.75 kg/m2 (P=0.001; Table 1). Systolic BP (SBP) did not differ much; however, diastolic BP (DBP) was 68.75±1.81 mmHg (control group) and 78.80±14.02 mmHg (case group) (P=0.006). Eight in the case group were hypertensive. Significant changes in lipid profile were observed with TC and LDLC. TC levels for the control and case groups were 3.35±0.62 mmol/L and 4.07±0.91 mmol/L, respectively (P=0.002). LDLC levels for the control and case groups were 1.74±0.57 mmol/L and 2.38±0.84 mmol/L, respectively (P=0.003; Table 1).
 | Table 1 Patient characteristics, including physical age (years); menarche age (years); duration of contraceptive use (months); blood pressure profile (mmHg); BMI (kg/m2); lipid profile (mmol/L) CV risk indices of the control group and the case group (hormonal contraceptive group) |
When data was stratified according to contraceptive type, Castelli risk index I (TC/HDLC) and II (LDLC/HDLC) were significantly different between the control and OC group (P=0.026 and P=0.014, respectively; Table 2). Furthermore, DBP was 68.75±1.81 mmHg (control group), whilst that of the IC and IMP groups were 78.57±1.97 mmHg and 87.4±10.6 mmHg, respectively. DBP was statistically significantly different between the control and IC groups (P=0.019) and control and IMP groups (P=0.025; Table 2). For the lipid profile, significant differences were observed for TC and LDLC (control versus [vs] OC group, P=0.002; control group vs IC group, P=0.018). Although values were within the normal reference intervals, increases were observed with OC and IC use. Similarly, LDLC was statistically significantly different between the control and OC groups; and control and IC groups (P=0.002 and P=0.039, respectively). The BMI of the IMP group was almost the same as the control group. However, the BMI of the OC group (26.4±1.12 kg/m2) and IC group (25.24±0.63 kg/m2) were statistically significantly different from the control group (21.73±0.75 kg/m2; P=0.003 and P=0.008, respectively) and were in the overweight range.
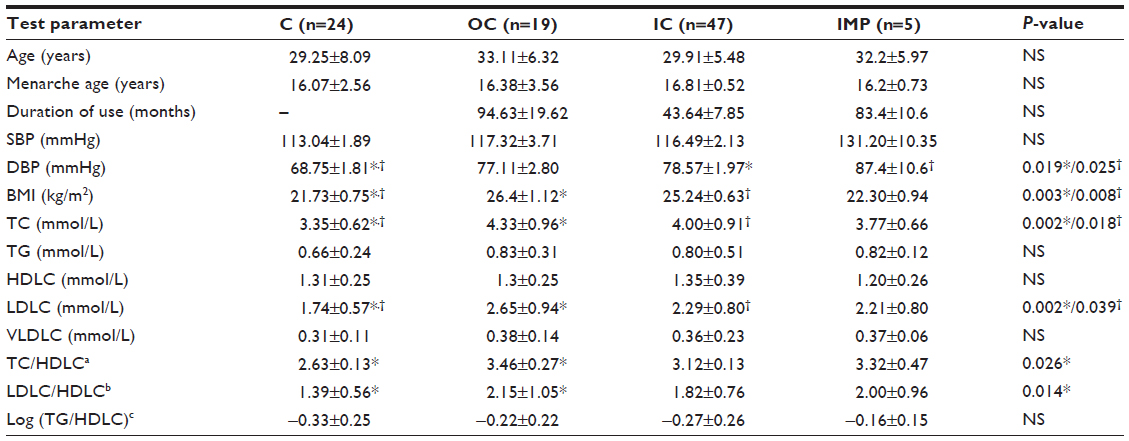 | Table 2 Patient characteristics, including physical age (years), menarche age (years), duration of contraceptive use (months), blood pressure profile (mmHg), BMI (kg/m2); lipid profile (mmol/L) CV risk indices of the C, OC, IC, and IMP contraceptive groups |
Discussion
This study focused on the changes in some lipoprotein biomarkers over time. SBP did not show any statistically significant differences among the two groups. However, DBP was statistically significantly different between the groups. When the data was stratified, statistically significant differences were observed between the control group and the IC group as well as the control group and the IMP group. In a similar study, DBP was higher in OC users than in patients not using contraceptives.17 Furthermore, the DBP of OC users was significantly higher than the DBP in users of other forms of contraceptives.17 In this study, IMP users had higher DBP than the OC or IC users. Women using OCs for more than 8 years presented higher age-adjusted BP levels than women using OCs for shorter periods. An increase in DBP is a common feature of HC use. It is possible that withdrawal from the use of OCs can lower DBP. Indeed, when this was tested in 171 women on OCs for 6 months, both the DBP and SBP declined by 10.4 mmHg and 15.1 mmHg, respectively.18 However, the association between HC use and CV risk factors among 2,285 young German girls aged 13–17 years gave relative contributions of HC use to be <1% for SBP and DBP.19 Other age-related factors may be involved in BP increase. BP measurements are therefore very important and increase in DBP is regarded as a pre-hypertension marker. Five reports showed that women who did not have BP measurements prior to OC initiation had a higher risk for acute myocardial infarction (MI) and ischemic stroke than women who did have BP measurements.20 The effects of natural estrogens on hepatic metabolism of estrogen-dependent markers such as liver proteins are milder than the synthetic estrogens. The 17α-ethinyl group on synthetic EE impedes inactivation of the entire molecule, thereby leading to a stronger effect on the liver. Hence, even in non-oral administration, the impact of EE is still strong on the liver production of hepatic proteins.21 Because of the molecular and structural properties of EE, which seem to resemble endogenous steroids, a high hepatic production of angiotensinogen is attained, which makes EE a thousand times more powerful than endogenous steroids. This triggers the renin–angiotensin–aldosterone pathway, thereby causing an increase in BP.22
TC and LDLC were significantly different in the HC group compared to the control group of this study. In both cases, higher results were obtained as a result of HC use. When the data were stratified, statistically significant differences were seen in the OR and IC groups for both TC and LDLC when compared to the control group. Similar statistically significant TC and LDLC elevations in the uninterrupted use of DMPA for 3–5 years were reported in a cohort of 140 subjects aged 20–35 years.23 In the Toronto Nutrigenomics and Health Study, which involved 783 subjects, lipid metabolism biomarkers were also statistically significantly higher among HC users.24 However, the pattern was different in a study by Okeke et al.25 In that study, 26 IC users and seven OC users were matched with 50 non-users of reproductive age in Nigeria. There was a significant change in TG and LDLC levels; TGs increased and LDLC decreased.25 The LDLC results obtained in the present study were thus contrary to the findings of the study by Okeke et al. Furthermore, no statistically significant change in TC and HDLC levels in women on OCs was observed in that study. However, a significant increase was observed in the TC of the OC group and a slight but statistically non-significant HDLC increase in the IC group of the present study. In the study by Okeke et al,25 HDLC was significantly increased in the IC group. In a longitudinal study by Nessa et al,26 HDLC did not increase over a 5-year period. However, in the study by Berenson et al,27 HDLC increased initially (6 months) among IC users but later returned to baseline after 3 years. Earlier studies carried out among 125 Kenyan women on OCs (Eugynon® [Schering AG, Berlin, Germany]: 500 μg dL-norgestrel/50 μg EE or Microgynon® [Bayer AG, Leverkusen, Germany]: 150 μg LNG plus 30 μg EE) showed a significant HDLC increase after twelve cycles.28 Lipid profile biomarkers are therefore disturbed with no clear pattern.
BMI differences were statistically significantly different between contraceptive and non-contraceptive users. The raw data showed that 23.9% of those on HCs were pre-obese. The control group and the IMP groups had normal BMI. The OC and IC groups had mean BMI that were statistically significantly different compared to the control and were pre-obese by the WHO classification (25–29.9 kg/m2). However, in an African-American group, BMIs of the control and OC groups were in the pre-obese and normal ranges, respectively.29 In another study, 226 DMPA users showed weight increase compared to the 603 controls over a follow-up period of 6 years among Brazilian women.30 Similarly, Piccoli et al31 observed that OC use was a predictor for weight increase among Swedish women in a long-term study. However, in another long-term longitudinal study, there was no statistically significant difference in weight increase in women grouped according to use or non-use of OC or duration of OC use. Age was the only factor that predicted weight increase. Furthermore, there was no correlation between weight change and OC use or duration of OC use.32 In two separate surveys, one in the UK and the other in the US, 73% and 50% respectively, believed that OCs could lead to weight gain.33,34 Although overweight was established in this study among contraceptive users, BMI was within the pre-obese range. It appears that HC use indirectly affects CV risk through mechanisms involving weight gain and obesity. Obesity is said to reduce the efficacy of contraceptives because of their pharmacokinetic alterations. However, obesity is a well-established CV risk factor, associated with cardiometabolic risk factors6 including hypertension, type 2 diabetes, and high serum cholesterol.7 The relationship between abnormal lipid levels and risk for coronary heart disease and MI in all regions of the world has been established.35 In this study, the atherogenic risk index was not statistically significant. However, the Castelli risk indices I (TC/HDLC) and II (LDLC/HDLC) (CV risk indices) were significant in the OC group compared to the control group. Values were lower in the IC group but higher than the control group. Differences were not statistically significant in this latter group. On the contrary, Okeke et al25 reported significantly lower Castelli index I and II in the OC group. In African-American women, OC use was associated with an increase in markers of CV risk.29 Similarly, Oyelola,36 in his study on Nigerian women, observed higher Castelli I and II indices in OC users than in non-users, and no change in these ratios among IC users. In this study, Spearman’s rho correlation predicted an increase in TG, TC, LDLC, and VLDLC over time (Table 3).
 | Table 3 Influence of hormonal contraceptive use on lipid profile over time |
Conclusion
This study therefore suggests some potential CVD risk with HC use through an indirect mechanism of BMI increase, which appears to be a more consistent marker in the literature in relation to HC use than the lipid profile. A longitudinal study is further suggested, as little data are available on the relationship between Ghanaian cohorts and HC use.
Acknowledgment
The researchers are grateful to the University of Ghana–Danish Universities Academic Partnership, under the platform of human health (PHH) in the Building Stronger Universities (BSU) program, for funding this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Lloyd-Jones DM, Hong Y, Labarthe D, et al; American Heart Association Strategic Planning Task Force and Statistics Committee. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation. 2010;121(4):586–613. | |
World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva, Switzerland: World Health Organization; 2009:28. Available at: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. Accessed April 28, 2014. | |
Parry CD, Patra J, Rehm J. Alcohol consumption and non-communicable diseases: epidemiology and policy implications. Addiction. 2011;106(10):1718–1724. | |
World Health Organization. Global Atlas on cardiovascular disease prevention and control. Geneva, Switzerland: World Health Organization; 2011; pp 136. Available at: http://www.world-heart-federation.org/fileadmin/user_upload/documents/Publications/Global_CVD_Atlas.pdf. Accessed April 28, 2014. | |
Khan M, Mensah GA. Epidemiology of Cardiovascular Disease. In: Institute of Medicine (US) Committee on Preventing the Global Epidermic of Cardiovascular Disease: Meeting the Challenges in Developing Countries; In: Fuster V, Kelly BB, editors. Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health. Washington, DC: National Academies Press; 2010:49–124. | |
Tsismenakis AJ, Christophi CA, Burress JW, Kinney AM, Kim M, Kales SN. The obesity epidemic and future emergency responders. Obesity. 2009;17(8):1648–1650. | |
Nelms M, Sucher KP, Lacy K, Roth SL. Nutrition Therapy and Pathophysiology. 2nd ed. Belmont, CA: Cengage Learning, Inc.; 2010. | |
Jones DR, Schmidt RJ, Pickard RT, Foxworthy PS, Eacho PI. Estrogen receptor-mediated repression of human hepatic lipase gene transcription. J Lipid Res. 2002;43(3):383–391. | |
Endrikat J, Klipping C, Cronin M, et al. An open label, comparative study of the effects of a dose-reduced oral contraceptive containing 20 microg ethinyl estradiol and 100 microg levonorgestrel on hemostatic, lipids, and carbohydrate metabolism variables. Contraception. 2002;65(3):215–221. | |
Barkfeldt J, Virkkunen A, Dieben T. The effects of two progestogen-only pills containing either desogestrel (75 microg/day) or levonorgestrel (30 microg/day) on lipid metabolism. Contraception. 2001;64(5):295–299. | |
Enk L, Landgren BM, Lindberg UB, Silfverstolpe G, Crona N. A prospective, one-year study on the effects of two long acting injectable contraceptives (depot-medroxyprogesterone acetate and norethisterone oenanthate) on serum and lipoprotein lipids. Horm Metab Res. 1992;24(2):85–89. | |
Crook D, Godsland IF, Wynn V. Oral contraceptives and coronary heart disease: modulation of glucose tolerance and plasma lipid risk factors by progestins. Am J Obstet Gynecol. 1988;158(6 Pt 2):1612–1620. | |
Watanabe RM, Azen CG, Roy S, Perlman JA, Bergman RN. Defects in carbohydrate metabolism in oral contraceptive users without apparent metabolic risk factors. J Clin Endocrinol Metab. 1994;79(5):1277–1283. | |
Akpalu J, Akpalu A, Ofei F. The metabolic syndrome among patients with cardiovascular disease in Accra, Ghana. Ghana Med J. 2011;45(4):161–166. | |
Gyakobo M, Amoah AG, Martey-Marbell DA, Snow RC. Prevalence of the metabolic syndrome in a rural population in Ghana. BMC Endocr Disord. 2012;12:25. | |
Kemper E, Stringfield S, Teddlie C. Mixed methods sampling strategies in social science research. In: Tashakkori A, Teddlie C, editors. Handbook of Mixed Methods in Social and Behavioral Research. Thousand Oaks, CA: Sage; 2003:273–296. | |
Lubianca JN, Faccin CS, Fuchs FD. Oral contraceptives: a risk factor for uncontrolled pressure among hypertensive women. Contraception. 2003;67(1):19–24. | |
Lubianca JN, Moreira LB, Gus M, Fuchs FD. Stopping oral contraceptives: an effective blood pressure-lowering intervention in women with hypertension. J Hum Hypertens. 2005;19(6):451–455. | |
Du Y, Rosner BM, Knopf H, Schwarz S, Dören M, Scheidt-Nave C. Hormonal contraceptive use among adolescent girls in Germany in relation to health behavior and biological cardiovascular risk factors. J Adolesc Health. 2011;48(4):331–337. | |
Tepper NK, Curtis KM, Steenland MW, Marchbanks PA. Blood pressure measurement prior to initiating hormonal contraception: a systematic review. Contraception. 2013;87(5):631–638. | |
Brito MB, Nobre F, Vieira CS. Hormonal contraception and cardiovascular system. Arq Bras Cardiol. 2011;96(4):e81–e89. | |
Sitruk-Ware R. New progestagens for contraceptive use. Hum Reprod Update. 2006;12(2):169–178. | |
Mia AR, Siddiqui NI, Islam MN, Khan MR, Shampa SS, Rukunuzzaman M. Effects of prolonged use of injectable hormonal contraceptive on serum lipid profile. Mymensingh Med J. 2005;14(1):19–21. | |
Josse AR, Garcia-Bailo B, Fischer K, El-Sohemy A. Novel effects of hormonal contraceptive use on the plasma proteome. PLoS One. 2012;7(9):e45162. | |
Okeke CU, Braide SA, Okolonkwo BN, et al. Comparative effects of injectable and oral hormonal contraceptives on lipid profile. Eur J Cardio Med. 2012;2(1):20–23. | |
Nessa A, Latif SA, Uddin MM, Hussain MA. Serum HDL-cholesterol in women using low dose oral contraceptives. Mymensingh Med J. 2007;16(Suppl 2):S3–S6. | |
Berenson AB, Rahman M, Wilkinson G. Effect of injectable and oral contraceptives on serum lipids. Obstet Gynecol. 2009;114(4):786–794. | |
Maina FW, Sekadde-Kigondu CB, Ojwang PJ, Mati JK. Changes in plasma HDL-cholesterol in women using oral contraceptives in Kenya. East Afr Med J. 1987;64(7):442–447. | |
Frempong BA, Ricks M, Sen S, Sumner AE. Effect of low-dose oral contraceptives on metabolic risk factors in African-American women. J Clin Endocrinol Metab. 2008;93(6):2097–2103. | |
Pantoja M, Medeiros T, Baccarin MC, Morais S, Fernandes AM. [Variation of weight among users of the contraceptive with depot-medroxyprogesterone acetate according to body mass index in a six-year follow-up]. Rev Bras Ginecol Obstet. 2009;31(8):380–384. Portuguese. | |
Piccoli A, Crosignani P, Nappi C, Ronsini S, Bruni V, Marelli S; Italian EVRA Contrast Study Group. Effect of the ethinylestradiol/norelgestromin contraceptive patch on body composition. Results of bioelectrical impedance analysis in a population of Italian women. Nutr J. 2008;7:21 | |
Lindh I, Ellström AA, Milsom I. The long-term influence of combined oral contraceptives on body weight. Hum Reprod. 2011;26(7):1917–1924. | |
Oddens BJ, Visser AP, Vemer HM, Everaerd WT, Lehert P. Contraceptive use and attitudes in Great Britain. Contraception. 1994;49(1):73–86. | |
Wysocki S. A survey of American women regarding the use of oral contraceptives and weight gain. Int J Gynecol Obstet. 2000; 70(Suppl 1):114. | |
Yusuf S, Hawken S, Ounpuu S, et al; INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. | |
Oyelola OO. Fasting plasma lipid, lipoproteins and apolipoproteins in Nigerian women using combined oral and progestin-only injectable contraceptives. Contraception. 1993;47(5):445–454. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.