Back to Journals » Clinical Optometry » Volume 18
Effect of High-Energy Visible Light–Filtering Spectacle Lenses on Distance Contrast Sensitivity
Authors Rampersad N, Hansraj R ![]()
Received 4 January 2026
Accepted for publication 8 April 2026
Published 28 May 2026 Volume 2026:18 593543
DOI https://doi.org/10.2147/OPTO.S593543
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Nishanee Rampersad, Rekha Hansraj
Discipline of Optometry, School of Health Sciences, University of Kwazulu-Natal, Durban, South Africa
Correspondence: Nishanee Rampersad, Discipline of Optometry, School of Health Sciences, University of KwaZulu-Natal, Westville Campus, Private Bag X54001, Durban, South Africa, Tel +27 31 260 7562, Fax +27 31 260 7666, Email [email protected]
Purpose: High-energy visible (HEV) light–filtering spectacle lenses, which selectively decrease transmission of short wavelength visible light, have been increasing in popularity in recent years despite much debate about their potential ocular benefits. This study reports on the effect of HEV light–filtering spectacle lenses on distance contrast sensitivity (CS).
Patients and Methods: The study included 30 healthy young adults aged 18 to 35 years. Binocular CS was measured with the Pelli–Robson test in both photopic and mesopic illumination using three commercially available HEV light–filtering spectacle lenses and a clear uncoated control lens. Data were analyzed with descriptive and inferential statistics.
Results: There was no difference in CS measurements among the four test lenses in either photopic (x2(3, n = 30) = 5.28, p = 0.153) or mesopic (x2(3, n = 30) = 0.92, p = 0.821) illumination. The CS measurements were significantly higher in photopic illumination than mesopic illumination for all four test lenses (Z ≤ – 3.54, p ≤ 0.010) with mean differences ranging from 0.08 to 0.10 logCS.
Conclusion: The HEV light–filtering spectacle lenses have no clinically meaningful effect on distance CS in young adults in both photopic and mesopic illumination. These results would be useful for eye care personnel when prescribing HEV light–filtering spectacle lenses.
Keywords: high-energy visible light, high-energy visible light–filtering spectacle lenses, spectacle lenses, contrast sensitivity, visual performance
Introduction
High-energy visible (HEV) light–filtering lenses, also referred to as blue-blocking lenses, have been increasing in popularity in recent years.1,2 This may be because of preclinical studies, involving animal models and cell cultures, showing an association between short wavelength visible light (400–500 nm) and retinal phototoxicity.3,4 Furthermore, the digital revolution resulted in considerable changes in digital technology and widespread adoption of digital devices, which are backlit by light-emitting diodes that have high relative amounts of HEV light in their emission spectra,5 for many aspects of daily life. Despite the increasing presence of HEV light in modern society, there is reassuring evidence that human exposure to HEV light fails to reach the international safety limits and is considerably lower than exposure from sunlight.5,6 Nevertheless, there have been marketing claims that HEV light–filtering spectacle lenses, which selectively decrease transmission of short wavelength visible light, maintain ocular health, enhance visual performance and improve sleep quality. However, recent systematic reviews concluded that there is unclear evidence on the potential ocular benefits of using HEV light–filtering spectacle lenses.2,7,8
Contrast sensitivity (CS), which assesses the ability to detect differences in luminance between an object and its background, is an important indicator of visual performance. Assessment of CS provides useful information on the quality of vision that is sometimes not detected with standard visual acuity and visual field assessments.9 For instance, individuals with relatively good Snellen high contrast visual acuity may report symptoms and complain of poor vision because of impaired CS.10,11 In addition, CS assessment has been used to detect and monitor ocular diseases, such as cataracts and age-related macular degeneration, and evaluate the effectiveness of therapeutic interventions.9–11 Good CS is essential for performing everyday tasks such as driving, reading, recognizing faces, identifying signage and navigating through environments with these tasks being important for both quality of life and safety.11 Moreover, CS is critical for visual functions including detecting motion and recognizing patterns in addition to visual acuity and visual field.10
Previous studies that have evaluated the impact of HEV light–filtering spectacle lenses on visual function have reported on colour discrimination,12,13 night vision,13 motion perception14 and photostress recovery times.15 Only few studies reporting on the effect of HEV light–filtering spectacle lenses on CS have been found.16,17 The study by Leung et al16 used the Mars test as their middle-aged presbyopic participants with mean age of 47.2 ± 0.7 years required higher powered reading additions that prevented evaluation of CS with the commercially available CVS-1000 at 2.5 meters. Furthermore, the targets in the Mars test subtend 2.5° at the recommended 50 centimeter (cm) test distance and only provide an evaluation of CS at near.18 Alzahrani et al17 evaluated chromatic contrast sensitivity in five participants using a computer-based visual search task involving stimuli of a narrow contrast range. Given that everyday tasks typically involve objects of varying size and contrast levels that are often viewed at different distances,11 it is important to evaluate the effect of HEV light–filtering spectacle lenses on CS using tests with different spatial frequencies and/or contrast levels. As HEV light–filtering spectacle lenses have been designed for everyday use to minimized exposure to HEV light, eyecare professionals and patients need to better understand the impact (if any) of these lenses on visual function specifically CS. Therefore, this study reports on the effect of HEV light–filtering spectacle lenses on distance CS.
Materials and Methods
Data collection commenced after ethical approval from the relevant research ethics committee (University of KwaZulu–Natal Biomedical Research Ethics Committee 00004362/2022). The study was conducted according to the principles of the Declaration of Helsinki and all participants provided written informed consent before participating. The sample size was determined assuming 90% power, 95% confidence interval with a Z value of 1.96 and yielded 27.19 After adjusting by 10% for potential dropouts and incomplete data, a minimum sample size of 30 participants was calculated. Studies that have small samples are useful to report on perceptual effects rather than measure general performance within populations.20 Therefore, the small sample in this quantitative study had sufficient power to investigate if HEV light filtering–filtering spectacle lenses have any effect on distance CS rather than quantifying the magnitude of the effect and/or comparing the effect between different populations.20
Eligible participants were individuals aged 18 to 35 years with unaided visual acuity of at least 6/6 in each eye, no media opacities and emmetropia (defined as spherical equivalent of ±0.50 D or less with maximum 0.75 D of refractive astigmatism.21 As the study enrolled healthy young adults, individuals with systemic conditions, currently using medication and history of ocular conditions, trauma or surgery, particularly affecting the cornea, crystalline lenses, aqueous or vitreous humor,9 were excluded. All participants that passed an initial screening, which consisted of case history, distance visual acuity using a Snellen chart, refraction (non-cycloplegic objective with a Keeler streak retinoscope and subjective with a trial case and frame) and ocular health assessment (ophthalmoscopy with a Keeler ophthalmoscope and white light evaluation), proceeded to data collection for CS measurements.
The Pelli–Robson test, developed by Pelli, Robson and Wilkins, was used to measure distance CS at the recommended test distance of one meter.22 The test chart is 84 cm high, 59 cm wide and consists of 48 Sloan letters that subtend 2.8°at the recommended test distance.23 Thus, CS is evaluated using intermediate spatial frequency English letter targets.22 The Sloan letters are arranged in eight rows of six letters forming two letter triplets on each row. The three letters in each triplet have the same contrast level and differ from the successive triplet by a constant factor of 0.15 log units (or a factor of 1/√2).22 The logCS measurements range from 0.00 log units (high contrast) to 2.25 log units (low contrast) corresponding to contrast values from 100% to 0.56% respectively.10 Thus, the Pelli-Robson chart is designed whereby the contrast levels decrease across and down the test chart for each triplet while the letter size remains constant. The Pelli–Robson test assesses the ability of the observer to recognize the letters as the difference in luminance between the Sloan letters and the background progressively decreases.
The study used four plastic afocal test lenses including three commercially available HEV light–filtering spectacle lenses and one clear uncoated control lens. The spectral transmission curves and characteristics (refractive index (n), center thickness (t) and Abbe number) for the four test lenses are shown in Figure 1. Overall, the transmission values for the three commercially available HEV light–filtering spectacle lenses ranged from 44% to 50% compared with 63% for the uncoated control lens for wavelengths 300 to 550 nm. All four test lenses had the same center thickness with similar refractive indices and Abbe numbers (Figure 1). To allow for use with a trial frame, the test lenses were cut and fitted into standard full aperture trial lens holders.
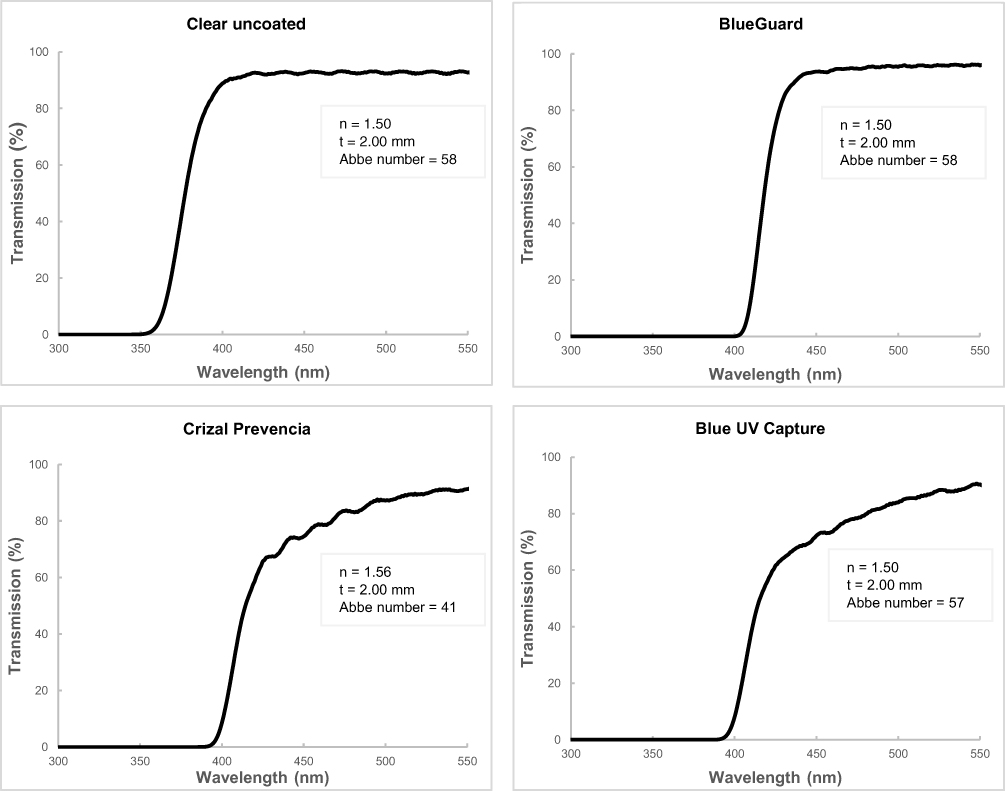 |
Figure 1 Transmission curves of the four test lenses. |
The CS measurements were taken with participants’ natural pupil and under binocular viewing conditions as this reflects real-world viewing conditions.9 In this study, CS was measured in both photopic (85 cd/m2) and mesopic (3 cd/m2) illumination. The latter was achieved with mesopic test filters as the luminance of the Pelli-Robson chart changes when viewed through mesopic filters (Good-Lite, US). Half of the sample started with photopic illumination while the other half started with mesopic illumination to prevent any order effects on the CS measurements. Participants were allowed a 15-minute adaptation period in the different illumination conditions (either photopic or mesopic) before any measurements consistent with the other studies measuring CS in different illumination conditions.24–26 After this adaption period, CS was measured with the four test lenses in a randomized sequence to minimise order effects. Participants wore each test lens in the trial frame for a minimum of two minutes before taking the CS measurement as has been done previously.17
When measuring the CS, participants were instructed to read the letters in a conventional way from left to right starting at the top (containing letters of high contrast) and proceeding downwards (containing letters of low contrast) until at least two of the three letters in a triplet were incorrectly identified. Participants were allowed to guess the letter optotypes even if they appeared faint, particularly for the rows at the bottom of the chart and were allowed time to do so. In this way, participants were encouraged to identify as many letters as possible on the chart while care was taken not to provide any feedback on the accuracy of the identified letters. As per the manufacturer’s recommendation, the logCS value of the last correctly identified triplet was recorded as the participant’s threshold CS.22
All measurements were performed in a standardized clinical environment with uniform lighting provided by fluorescent light bulbs in ceiling-mounted fittings. These light bulbs were not changed throughout data collection and the room windows were covered with blockout blinds. The room illuminance was 519 lux when measured using a light meter wherein the average of five measurements was determined. Only one researcher, who was an experienced optometrist, performed data collection using the same test instructions and end points. The Pelli-Robson charts were carefully placed to ensure that glare sources and reflections off the surface of the chart were minimized. Two versions of the Pelli–Robson test (charts 1 and 2), which are identical except for different letter sequences, were used to minimise the possibility of memorization when testing with the different test lenses. The Pelli-Robson CS test is easy to explain, administer and score and has demonstrated good test–retest repeatability.9,27 Consequently, it is the most commonly used CS test in vision science research and clinical settings.10,23
Data were captured and analyzed with the Statistical Package for Social Sciences. Normality testing, using the Shapiro–Wilk test and graphical inspection of the histograms, revealed that the CS measurements were asymmetrically distributed. The continuous data are summarized using descriptive statistics including mean, standard deviation, median, interquartile range, percentage and range. The Wilcoxon signed-rank test was used to assess for differences in mean logCS measurements in the two illumination conditions with the same test lens. The Friedman test assessed for differences in mean logCS measurements among the four test lenses in photopic and mesopic illumination. Probability (p) values that were less than 0.05 were considered statistically significant.
Results
The mean age of the sample was 21.2 ± 1.4 years and 87% of participants were female. The mean spherical equivalent refraction was +0.04 ± 0.21 D (range, –0.25 to +0.50 D) in the right eye and +0.05 ± 0.25 D (range, –0.50 to +0.50 D) in the left eye. Table 1 summarizes the CS measurements (medians, interquartile ranges, means and standard deviations) for the four test lenses in photopic and mesopic illumination. As expected, the mean CS measurement was higher in photopic than mesopic illumination in all four test lenses with differences ranging from 0.08 to 0.10 logCS (Table 1). The median CS measurements were significantly higher under photopic illumination than under mesopic illumination for all four test lenses (Z ≤ –3.54, p < 0.05). There was no significant difference in CS measurements among the four test lenses in either photopic (x2(3, n = 30) = 5.28, p = 0.153) or mesopic (x2(3, n = 30) = 0.92, p = 0.821) illumination.
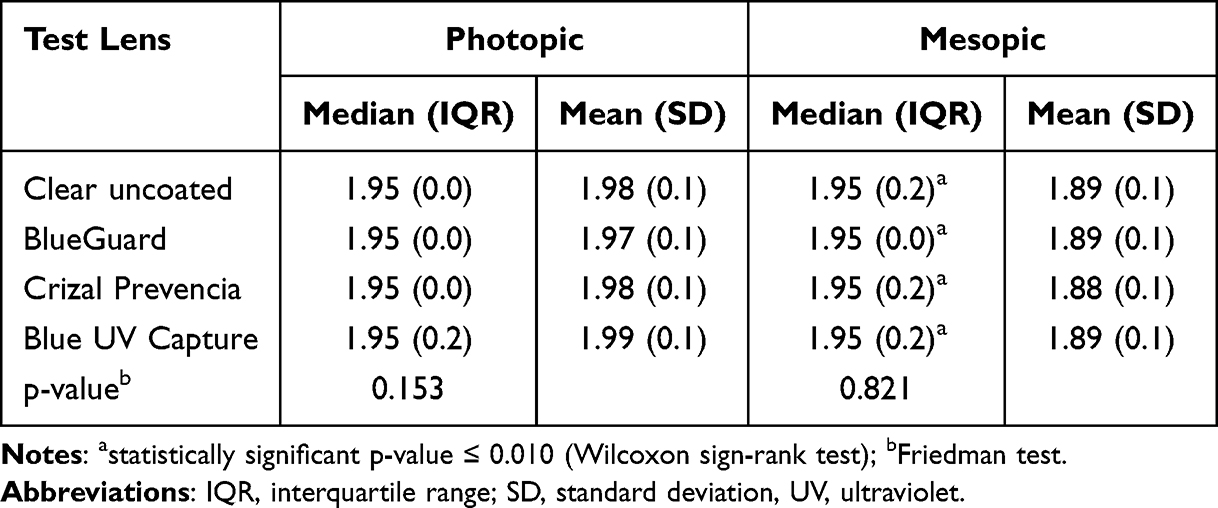 |
Table 1 Contrast Sensitivity Measurements (in Log Units) for the Four Test Lenses in Photopic and Mesopic Illumination |
Discussion
This study reports on the effect of HEV light–filtering spectacle lenses on distance CS in both photopic and mesopic illumination. Given the lack of clinical guidelines for eye care professionals to inform the prescribing of HEV light–filtering spectacle lenses in professional practice,1 it is necessary to understand their impact (if any) on visual function. In this regard, data on the impact of these lenses may help eye care professionals have more informed discussions with their patients as there is scarcity of high-quality studies that address the effect of these lenses on visual performance.2 As HEV light–filtering spectacle lenses reduce transmission of short wavelength visible light and are being worn for everyday use, it is important to understanding their impact on visual performance particularly in conditions of reduced illumination.
The literature shows conflicting reports on the effect of HEV light–filtering lenses on CS with some studies noting no effects16,24,25 while others have reported improvement in CS.28,29 The findings of previous studies should be interpreted cautiously as contradictory results may be explained by differences in the spectral transmission properties of the filters used, tests and targets therein used to measure CS, the absence or presence of glare conditions and the characteristics of the participants in terms of age and ocular media characteristics. In an early study, Zigman28 showed that a yellow filter, which absorbed wavelengths less than 480 nm, significantly improved CS in the spatial frequency range of 3–12 cycles per degree in 14 participants with mean age of 64 years. More recently, Cozza et al29 reported significantly better CS measurements at 12 cycles per degree with a blue-blocking filter in 20 adults with mean age of 48 years. These two studies, which reported that the lenses used had a discernible yellow appearance, attributed the improvement in CS at certain angular frequencies to reduced intraocular scattering and chromatic aberrations that consequently improved optical quality of the retinal images.28,29 Short wavelength visible light undergoes more intraocular scattering and results in reduced retinal image clarity and contrast.29 This intuitively suggests that lenses that selectively attenuate transmission of short wavelength visible light would reduce intraocular scatter and positively impact CS although the characteristics of the filter used and participants appears to influence the visual function results.
In this study, the HEV light–filtering spectacle lenses did not influence the distance CS measurements relative to the clear uncoated control lens in both photopic and mesopic illumination. The results showed a neutral impact on distance CS as the logCS difference between the control lens and the HEV light–filtering spectacle lenses was less than the value of one triplet (0.15 log units) in the Pelli–Robson test. A difference of at least 0.30 log units, or two triplets in the Pelli–Robson test chart, between two measurements is considered clinically meaningful.30 This implies that the three HEV light–filtering spectacle lenses in this study had no clinical or statistical impact on distance CS measurements in both lighting conditions consistent with results of previous studies that also used modern generation HEV light–filtering spectacle lenses.16,25 The inclusion of healthy young adults without ocular media anomalies and modern generation HEV light–filtering spectacle lenses, which show modest attenuation of short wavelength visible light,13 may explain the absence of any impact on distance CS in this study. It is also possible that the nature of the Pelli–Robson test may account for these results, as the targets therein are achromatic and correspond to 1–2 cycles per degree.30 As other studies noted changes in CS at higher spatial frequencies28,29 and with blue colored targets,17 it suggests that the Pelli–Robson test may be insensitive to the changes in CS because of its inherent characteristics. Therefore, future studies should consider using CS tests containing chromatic targets, particularly blue colored, with a broader range of spatial frequencies across the CS function when evaluating the impact of HEV light–filtering lenses.
The CS measurements with the test lenses were significantly higher in photopic than mesopic illumination aligned with findings from previous studies.24,26 This implies that CS is adversely impacted by changes in lighting as the measurements were better in photopic illumination. With decreasing illumination, the Purkinje shift describes the change in the spectral sensitivity of the eye with a resulting shift towards the shorter wavelengths compared with photopic illumination.31 In this regard, the Purkinje shift highlights the importance of understanding the behavior of short wavelength light particularly when using HEV light–filtering spectacle lenses. Taken together, the findings in this study imply that there were no meaningful differences in mean CS measurements between the clear uncoated control and the three HEV light–filtering spectacle lenses and that the reduced illumination is primarily responsible for the reduced CS measurements in mesopic conditions. However, these differences were ≤0.10 logCS and lower than one triplet in the Pelli–Robson test, implying they may have minimal clinical importance. In a theoretical study containing statistical analysis, Alzahrani et al13 calculated that scotopic vision was reduced by 5 to 24% with commercially available HEV light–filtering spectacle lenses. Nevertheless, eye care professionals should consider these results and advise patients of the unintended effects on visual performance in conditions of reduced illumination, especially when undertaking visually demanding tasks such as driving.
Strengths of this study included counterbalancing of the illumination condition and randomization of the test lenses to prevent order effects as well as inclusion of healthy young adults to minimise the impact of age and ocular media changes on the CS measurements.26 Despite this, the study has four main limitations that need to be acknowledged. Firstly, there was a possibility of learning effects with repeated testing though two versions of the Pelli–Robson test with differing letter sequences were used to minimise this. Furthermore, each Pelli–Robson chart consists of 10 Sloan letters, which further prevents the possibility of memorization. Secondly, the sample was predominantly female and had a relatively narrow age range and different results may be obtained in elderly individuals and those with ocular conditions that cause ocular media anomalies. Indeed, if HEV light–filtering spectacle lenses impact CS, it would be important to know this as increasing age and presence of certain ocular diseases cause changes in CS.26 Future studies should therefore include elderly individuals and those with ocular conditions as such data would be important. Thirdly, each step or triplet in the Pelli–Robson test corresponds to 0.15 logCS and may have been too large to detect minute changes in CS although the clinical impact of changes smaller than 0.15 logCS remains unknown. Nevertheless, future studies should consider CS tests that are more sensitive to detect small changes and assess the entire CS function at the different spatial frequencies to evaluate the impact of HEV light–filtering spectacle lenses on this important aspect of visual performance. Lastly, this study did not investigate CS under conditions of glare and future studies should consider this.
Conclusion
The results of this study showed that HEV light–filtering spectacle lenses have no clinically meaningful effect on distance CS when measured with the Pelli–Robson test in young adults under both photopic and mesopic illumination. These results would be useful for eye care personnel that may be prescribing HEV light–filtering spectacle lenses.
Data Sharing Statement
Data generated for the study is available on request from the corresponding author.
Acknowledgments
The authors thank Dr Dessie for assistance with the statistical analysis.
Funding
This work was supported by the National Research Foundation of South Africa (Grant Number 138247).
Disclosure
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article. The author reports no conflicts of interest in this work.
References
1. Downie LE. Blue-light filtering ophthalmic lenses: to prescribe, or not to prescribe. Ophthalmic Physiol Opt. 2017;37(6):640–7. doi:10.1111/opo.12414
2. Lawrenson JG, Hull CC, Downie LE. The effect of blue-light blocking spectacle lenses on visual performance, macular health and the sleep-wake cycle: a systematic review of the literature. Ophthalmic Physiol Opt. 2017;37(6):644–654. doi:10.1111/opo.12406
3. Noell WK, Walker VS, Kang BS, Berman S. Retinal damage by light in rats. Invest Ophthalmol. 1966;5(5):450–473.
4. Kuse Y, Ogawa K, Tsuruma K, Shimazawa M, Hara H. Damage of photreceptor-derived cells in culture induced by light emitting diode-derived blue light. Sci Rep. 2014;4(1):1–12. doi:10.1038/srep05223
5. O’hagan JB, Khazova M, Price LLA. Low-energy light bulbs, computers, tablets and the blue light hazard. Eye. 2016;30(2):230–233. doi:10.1038/eye.2015.261
6. Rosenfield M. Living with blue light exposure. Rev Optom. 2019;156(9):56–60.
7. Vagge A, Ferro Desideri L, Del Noce C, Di Mola I, Sindaco D, Traverso CE. Blue light filtering ophthalmic lenses: a systematic review. Semin Ophthalmol. 2021;36(7):541–548. doi:10.1080/08820538.2021.1900283
8. Singh S, Keller PR, Busija L, et al. Blue-light filtering spectacle lenses for visual performance, sleep and macular health in adults. Cochrane Database Syst Rev. 2023;8:CD013244. doi:10.1002/14651858.CD013244.pub2
9. Elliot DB. Contrast sensitivity and glare testing. In: Benjamin WJ, editor. Borish’s Clinical Refraction. Philadelphia: Butterworth-Heinmann; 2006:247–288.
10. Richman J, Spaeth GL, Wirostko B. Contrast sensitivity basics and a critique of currently available tests. J Cataract Refract Surg. 2013;39(7):1100–1106. doi:10.1016/j.jcrs.2013.05.001
11. Ginsburg AP. Contrast sensitivity and functional vision. Int Ophthalmol Clin. 2003;43(2):5–15. doi:10.1097/00004397-200343020-00004
12. Baldasso M, Roy M, Boon MY, Dain SJ. Effect of blue-blocking lenses on colour discrimination. Clin Exp Optom. 2021;104(1):56–61. doi:10.1111/cxo.13139
13. Alzahrani HS, Khuu SK, Roy M. Modelling the effect of commercially available blue-blocking lenses on visual and non-visual functions. Clin Exp Optom. 2020;103(3):339–346. doi:10.1111/cxo.12959
14. Ali A, Roy M, Alzahrani HS, Khuu SK. The effect of blue light filtering lenses on speed perception. Sci Rep. 2021;11(1):17583. doi:10.1038/s41598-021-96941-0
15. Alzahrani HS, Khuu SK, Ali A, Roy M. The effect of blue-blocking lenses on photostress recovery times. Optom Vis Sci. 2020;97(11):995–1004. doi:10.1097/OPX.0000000000001601
16. Leung TW, Leung RWH, Kee CS. Blue-light filtering spectacle lenses: optical and clinical performances. PLoS One. 2017;12(1):e0169114. doi:10.1371/journal.pone.0169114
17. Alzahrani HS, Roy M, Honson V, Khuu SK. Effect of blue-blocking lenses on color contrast sensitivity. Clin Exp Optom. 2020;104(2):207–214. doi:10.1111/cxo.13135
18. Mars Perceptrix Corporation. The Mars Letter Contrast Sensitivity Test User Manual. Chappaqua: The Mars Perceptrix Corporation; 2013.
19. Browner WS, Newman TB, Hulley SB. Estimating smaple size and power: applications and examples. In: Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB, editors. Designing Clinical Research. Philadelphia: Lippincott Williams & Wilkins; 2007:65–94.
20. Anderson AJ, Vingrys AJ. Small samples: does size matter. Invest Ophthalmol Vis Sci. 2001;42(7):1411–1413.
21. Galvis V, Tello A, Camacho PA, Gómez LM, Rey JJ, Serrano AA. Definition of refractive errors for research studies: spherical equivalent could not be enough. J Optom. 2021;14(2):224–225. doi:10.1016/j.optom.2020.10.003
22. Pelli DG, Robson JG, Wilkins AJ. The design of a new letter chart for measuring contrast sensitivity. Clin Vision Sci. 1988;2(3):187–199.
23. Arditi A. Improving the design of the letter contrast sensitivity test. Invest Ophthalmol Vis Sci. 2005;46(6):2225–2229. doi:10.1167/iovs.04-1198
24. Domínguez-Vicent A, Helghe E, Wahlberg Ramsay M, Venkataraman AP. Photopic and mesopic contrast sensitivity function in the presence of glare and the effects of filters in young adults. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.772661
25. Lian Y, Lu W, Huang H, Wu G, Xu A, Jin W. The long-term effect of blue-light blocking spectacle lenses on adults’ contrast perception. Front Neurosci. 2022;16:1–6. doi:10.3389/fnins.2022.898489
26. Herrero-Gracia A, Hernández-Andrés R, Luque MJ, Díez-Ajenjo MA. Age-related changes in contrast sensitivity function under different illumination conditions. Clin Exp Optom. 2025;108(7):880–885. doi:10.1080/08164622.2025.2483265
27. Lovie-Kitchin JE, Brown B. Repeatability and intercorrelations of standard vision tests as a function of age. Optom Vis Sci. 2000;77(8):412–420. doi:10.1097/00006324-200008000-00008
28. Zigman S. Light filters to improve vision. Optom Vis Sci. 1992;69(4):325–328. doi:10.1002/j.1538-9235.1992.tb02924.x
29. Cozza F, Compagnoni MM, Airoldi C, et al. The effects of two longpass filters on visual performance. J Optom. 2020;13(2):102–112. doi:10.1016/j.optom.2019.07.001
30. Elliot DB, Sanderson K, Conkey A. The reliability of the Pelli-Robson contrast sensitivity chart. Ophthalmic Physiol Opt. 1990;10(1):21–24.
31. Rosenfield M. Refractive status of the eye. In: Benjamin WJ, editor. Borish’s Clinical Refraction. Philadelphia: Butterworth-Heinemann; 2006:3–34.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.