Back to Journals » Journal of Blood Medicine » Volume 16
Effect of Haplo-Allogeneic Hematopoietic Stem Cell Transplantation Timing on Patients with Severe Aplastic Anemia Without Histocompatible Matched Sibling Donor
Authors Fan D, Xiao F, Zhao J, Yan XQ, Liu Q, Liu L ![]() , Wang WQ, Qin WW
, Wang WQ, Qin WW
Received 12 February 2025
Accepted for publication 10 June 2025
Published 17 June 2025 Volume 2025:16 Pages 293—306
DOI https://doi.org/10.2147/JBM.S520719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Dan Fan,1,* Fang Xiao,1,* Jiayi Zhao,2,* Xue Qian Yan,1 Qiang Liu,1 Li Liu,1 Wen Qing Wang,1 Wei Wei Qin1
1Department of Hematology, Tangdu Hospital, Fourth Military Medical University, Xi’an, 710038, People’s Republic of China; 2Shanghai Institute of Hematology, State Key Laboratory of Medical Genomics, National Research Center for Translational Medicine at Shanghai, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Wei Qin, Email [email protected]
Background: Comparative studies on frontline haploidentical HSCT (haplo-HSCT) versus salvage haplo-HSCT after immunosuppressive therapy (IST) failure in severe aplastic anemia (SAA) are limited. To evaluate the effects of different transplantation timing on patient survival, the incidence of graft-versus-host disease (GVHD), and the risk of infection on the outcomes of patients with SAA.
Methods: This retrospective study included 82 SAA patients who underwent haplo-HSCT using the “Beijing protocol”. Patients who underwent allogeneic HSCT within 3 months after diagnosis were in the first-line HSCT group, and patients who were treated with initial IST and followed with allogeneic HSCT after treatment failure or relapse were in the salvage HSCT group. Patients were categorized into the frontline HSCT group (n=40, 48.8%) and the salvage HSCT group (n=42, 51.2%) based on transplantation timing. All 82 patients received grafts from related haploidentical donors. Follow-up was until January 1, 2024, and all patients were followed for more than 12 months with a median follow-up of 49 (12– 126) months, except for dead cases.
Results: Multivariate analysis identified salvage HSCT (HR: 5.344, 95% CI: 1.904– 14.995), ferritin levels > 1000 (HR: 5.588, 95% CI: 1.696– 18.414), and CMV infection (HR: 11.909, 95% CI: 2.335– 60.725) as independent risk factors for graft failure. The overall survival rate was significantly higher in the front HSCT group (90%, 36/40) compared to the salvage HSCT group (71.4%, 30/42) with mortality rates of 10.0% (4/40) and 28.6% (12/42), respectively (p=0.029). The expected 5-year OS was significantly higher in the frontline HSCT group compared to the salvage group. Salvage HSCT, ECOG score ≥ 1, and ferritin levels > 1000 were identified as independent risk factors for prognosis.
Conclusion: Frontline haplo-HSCT demonstrates superior survival and safety compared to salvage haplo-HSCT in young SAA patients without a matched sibling donor, warranting further clinical adoption.
Keywords: salvage haploidentical transplantation, frontline haploidentical transplantation, severe aplastic anemia, immunosuppressive therapy
Introduction
Characterized with pancytopenia of the peripheral blood and hypocellular marrow, severe aplastic anemia (SAA) is a life-threatening, immune-mediated disorder caused by the immunologic destruction of hematopoietic stem cells.1,2 The annual incidence of aplastic anemia is ~2/million in Europe and North America. However, aplastic anemia appears to be 2 to 3-fold more common in Asia than in the West.3 For the population threaten by the disease, the gender ratio is close to 1:1, and two age peaks are observed with one in mid to late childhood and a second among the elderly.4,5
SAA is a life-threatening hematologic disease, with historical two-year mortality exceeding 40%, primarily due to infections and bleeding complications.2,3
As hematopoietic stem cell transplantation (HSCT) from a histocompatible matched sibling donor (MSD) could improve the prognosis, it remains the preferred therapy for children and young adults with SAA.6 However, for only less than 30% patients in China have a MSD considering the demographics of China, Haploidentical-HSCT (Haplo-HSCT) could be an alternative to shorten the waiting time to find a suitable donor in such cases.7
With the advance of transplantation, such as the modification of the conditioning regimen and a more acceptable incidence of graft-versus-host disease (GVHD), haplo-HSCT can be considered as a frontline treatment for children and adolescent without a MSD or an unrelated donor (URD), according to the recommendations from the Chinese Society of Hematology.8 Researches comparing frontline Haplo-HSCT to salvage Haplo-HSCT following IST failure are limited, despite the fact that numerous reports have compared the results of frontline IST to that of frontline haplo-HSCT.9,10 This study retrospectively endeavored to examine the effectiveness of haplo-HSCT as a frontline treatment modality in comparison to that as a remedy in young patients with SAA who lack an MSD.
Methods
Patients
We retrospectively analysed the clinical data of 82 patients who underwent haplo-HSCT according to the Beijing Protocol11 without an HLA-matched sibling donor between May 1, 2013, and November 30, 2022, at the Tangdu Hospital Affiliate to Fourth Military Medical University, and all patients were diagnosed with acquired SAA or VSAA according to standard criteria.12 Patients who underwent allogeneic HSCT within 3 months after diagnosis were in the first-line HSCT group, and patients who were treated with initial IST and followed with allogeneic HSCT after treatment failure or relapse were in the salvage HSCT group. All patients in the salvage HSCT group had primary or relapsed SAA/VSAA refractory to prior IST, with no cases of transfusion-dependent non-severe aplastic anemia (TD-NSAA) included in the cohort. Follow-up was until January 1, 2024, and all patients were followed for more than 12 months with a median follow-up of 49 (12–126) months, except for dead cases. All protocols of the clinical trial followed the Declaration of Helsinki and were approved by the Ethics Committee of Tangdu Hospital Affiliate to Fourth Military Medical University. Ethics Committee Approval Number: K202402-13. All patients and donors provided written informed consent.
Conditioning Regimens
Conditioning regimens included1 FLU/CY: Fludarabine (Flu),30 mg·m−2·d−1, intravenously (i.v)., day −5 to −2; Cyclophosphamide (Cy),50 mg·kg−1·d−1, i.v., day −5 to −2;2 BU/CY:Busulfan (Bu) 3.2 mg·kg−1·d−1, i.v., day −5 to −2; CY 50 mg·kg−1·d−1, i.v., day −5 to −2. Sixty-eight patients received rabbit anti-thymocyte globulin (ATG) (2.5 mg·kg−1·d−1, i.v., days −5 to −2, rabbit, SangStat, Lyon, France). In the salvage HSCT group, 14 patients received pig anti-thymocyte globulin (25 mg·kg−1·d−1, i.v., days −5 to −2, porcine, Wuhan Institute of Biological Products, Wuhan, China) for previous use of rATG.
GVHD Prophylaxis and Treatment
Prophylaxis against GVHD is composed of CsA, mycophenolate mofetil (MMF) and short-course methotrexate. CsA was administered i.v. on day −9 at 3 mg·kg−1·d−1 in 2 divided doses over 12 hours and was administered orally when the patients’ bowel function had returned to normal. The dose of CsA was adjusted based on the serum trough concentration in the range of 200 to 250 ng·mL−1. MMF was administered on day −9 at 1 g·d−1 in 2 divided doses for adults, and 0.5 g·d−1 in 2 divided doses for pediatric patients. Methotrexate was administered 15 mg·m−2 on day +1,10 mg·m−2, on day +3, day +6, and day +11, respectively. After 30–40 days, the dose of MMF was gradually reduced if the patient with normal hemogram, complete chimerism and there was no obvious occurrence of GVHD. After 9 months, the dose of CsA gradually decreased to discontinued within 3–6 months in the absence of GVHD. If GVHD occurs, CSA would be administrated longer, and the dose would be adjusted to therapeutic concentrations.
For grade II-IV aGVHD, the regimen included methylprednisolone (1–2 mg·kg−1) which gradually decreased after the onset and switched to prednisone orally. For steroid-refractory aGVHD(SR-GVHD), Ruxolitinib, CD 25 monoclonal antibody, or mesenchymal stromal cells would be applied. For cGVHD, methylprednisolone combined with CsA was administrated. Patients presenting with cGVHD were preferred to be treated with CsA in combination with prednisone. Glucocorticoids were preferred for cutaneous cGVHD after 2018, with the addition of Ruxolitinib if it was ineffective.
Stem Cell Collection and Infusion
Three patients received peripheral blood stem cells (PBSCs) (2 donors aged <14 years and 1 patient aged 11 years), two of whom were infused with umbilical cord-derived mesenchymal stem cells (MSCs) on day 4 after transplantation. Other 79 patients received both bone marrow (BM) and PBSCs. Donors were infused with 8–10 ug·kg−1·d−1 granulocyte colony-stimulating factor (G-CSF) for 5 days. Bone marrow hematopoietic stem cells were collected on day 4, and PBSCs were collected on day 5/6. In case of ABO incompatibility, erythrocytes were depleted using the blood cell separator. The target count of mononuclear cells was ≥ 6×108 /kg and CD34+ cells were ≥ 2×106 /kg. After June 2021, 18 patients in total, comprising 12 salvage transplant recipients and 6 frontline transplant recipients, were simultaneously infused with 1.15 × 106·kg−1 (range, 0.94–1.69 × 106·kg−1) umbilical cord-derived MSCs on day +4. MSCs were from the Cord Blood Bank of Shandong Province.
Supportive Care and Post-Transplantation Surveillance
All patients were taken to the laminar-flow wards for protective isolation after medicinal baths and skin preparation until hematopoietic recovery. Voriconazole or Caspofungin was administrated to prevent fungal infections. Ganciclovir was administrated from day −9 to day −2 and Acyclovir from day 1 to month 12 to prevent viral infections. From day 6, rhG-CSF was administrated subcutaneously until the absolute neutrophil count (ANC) was >1×109 / L. TPO was administrated to promote platelet implantation, and some patients were treated with oral TPO-RAs after 2019. Irradiated red blood cells and platelet were infused intermittently according to blood cell counts. CMV-DNA and EBV-DNA were retested weekly after transplantation. After hematopoietic reconstruction, the chimeric rate was monitored using short tandem repeat (STR) PCR if donor-recipient sex matched, or chromosomes of donor-recipient sex mismatched on day +30, +60, +90, +180, +360 and +720. In the condition of continuous declination of hemogram, the chimeric rate would be monitored to figure out secondary graft failure (GF).
Definitions
Hematopoietic reconstruction was defined as an ANC >0.5 × 109 /L for 3 days in succession, and platelet (PLT) count >20 ×109 /L for 7 consecutive days without transfusion. The chimeric rate was monitored using short tandem repeat (STR) PCR if donor-recipient sex matched, or chromosomes of donor-recipient sex mismatched. Primary graft failure (GF) was defined as ANC <0.5 × 106 /L continuously with low or depleted donor chimerism by the 28th day, whereas secondary GF was defined as neutropenia (ANC <0.5 × 109 /L) with donor chimerism due to the loss of function of previously complete transplantation. The diagnosed of acute GVHD (aGVHD) and chronic GVHD (cGVHD) was according to standard criteria.13,14 Patients who survived >30 days after successful transplantation were analyzed for aGVHD, while patients surviving >100 days without GF were analyzed for cGVHD. CMV or EBV DNA ≥ 500 copies/mL in plasma was defined as CMV or EBV reactivation. Overall survival (OS) was defined as the time from HSCT to death from any cause or last follow-up. Transplant-related mortality (TRM) was defined as death without recurrence of prior disease. General condition was scored according to the Eastern Cooperative Oncology Group (ECOG) scoring system.
Statistical Analysis
The baseline characteristics and discrepancy were analysed descriptively. The differences of continuous and categorical variables between two groups were assessed using t-test, Mann–Whitney U-test, chi-square test or Fisher‘s precise test. Probabilities of OS and TRM were performed using the Kaplan–Meier method and compared using the Log rank test. Whether any of the chosen characteristics were predictive of the endpoints was ascertained by the univariate and multivariate analyses. The multivariate analysis of factors with p <0.10 in univariate analysis was performed in Cox proportional regression models. All statistical analyses were performed using IBM PS tatistics (25IBM, Armonk, NY, USA), while the cumulative incidence, survival curves, GVHD curves, and graft dysfunction curves were generated using R (version V4.3.1). P <0.05 was considered to indicate statistical significance.
Results
Basic Characteristics
Eighty-six patients diagnosed with SAA/VSAA underwent haploidentical allogeneic HSCT, among which 4 patients died during conditioning, and a total of 82 patients were finally enrolled. Forty of them (48.8%) underwent frontline HSCT, while the remaining 42 patients (51.2%) underwent salvage HSCT. Fifty-two patients were male, and 30 patients were female. The median age of the patients in the frontline HSCT group and the salvage HSCT group was 15 years (range, 6–34) and 18 years (range, 5–55), respectively. The median time to HSCT after diagnosis was 1 month (range, 0.5–3) in the frontline HSCT group, with 6 patients treated with brief CSA and the remaining 34 patients treated with supportive and symptomatic therapies only. While in the salvage HSCT group, the median time to HSCT was 42 months (range, 5–240). All patients in the salvage HSCT group received relevant treatment before transplantation, including 14 of them underwent ATG + CSA regimen, and others received CSA regimen. In the frontline HSCT group, 37 of 40 patients (92.5%) were diagnosed with VSAA, with 10 patients (23.8%) in the salvage HSCT group diagnosed with VSAA. In both groups, 6 and 12 patients were infused with umbilical cord-derived MSCs on day +4, respectively. All donors were related to haploidentical donors. Except for the type of disease (SAA/VSAA), time to HSCT after diagnosis, whether or not receiving IST, and the median ferritin level, no significant differences in age, gender, ECOG score, donor-recipient sex match, conditioning regimen were observed between the two groups (Table 1).
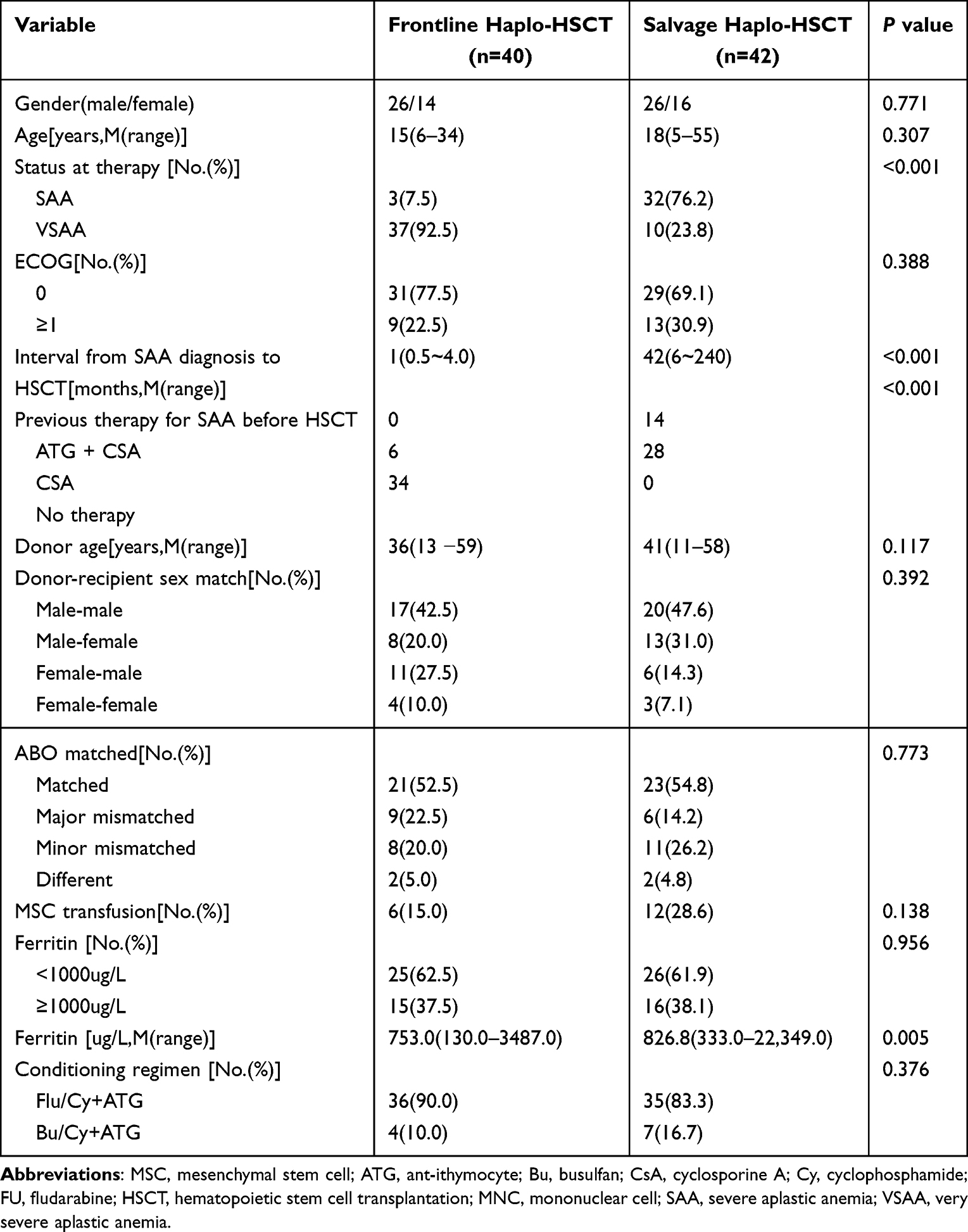 |
Table 1 Characteristics of Patients Before Transplantation |
Hematopoietic Reconstruction and Engraftment
Doses of infused mononuclear cells (p=0.454) and CD34+ cells (p=0.297) were not significantly different in the two groups. The median times to ANC engraftment were 14 days (range, 11–21) and 15 days (range, 10–27), respectively. The cumulative implantation rate of ANC on day +30 was 100% in both groups (p=0.14, Figure 1A). The time to PLT engraftment was 15 days (range, 8–32) and 16 days (range, 8–42) in the two groups, and the cumulative implantation rate of PLT on day +30 was 97.5% and 85.7%, respectively (p=0.4, Figure 1B). No statistical difference in the time to hematopoietic reconstruction was observed between the two groups (p>0.05).
 |
Figure 1 The cumulative incidence of engraftment after transplantation in the Frontline Haplo-HSCT and Salvage Haplo-HSCTgroups. (A) Neutrophil engraftment. (B) Platelet engraftment. |
In the frontline HSCT group, all 40 patients succeed to achieve hematopoietic reconstruction without primary or secondary GF. In the salvage HSCT group, 2 of 42 patients failed to achieve hematopoietic reconstruction, 1 of whom received second transplantation to achieve reconstruction on day +31 but died of pulmonary infection in month +26, the other one experienced auto-hematopoietic recovery on day +73 and survived until the end of follow-up with normal blood hemogram. Four patients were fully chimeric but experienced poor PLT engraftment with PLT count <20 ×109 /L continuously until the death. No significant difference in the incidence of GF was viewed (p=0.259) (Table 2).
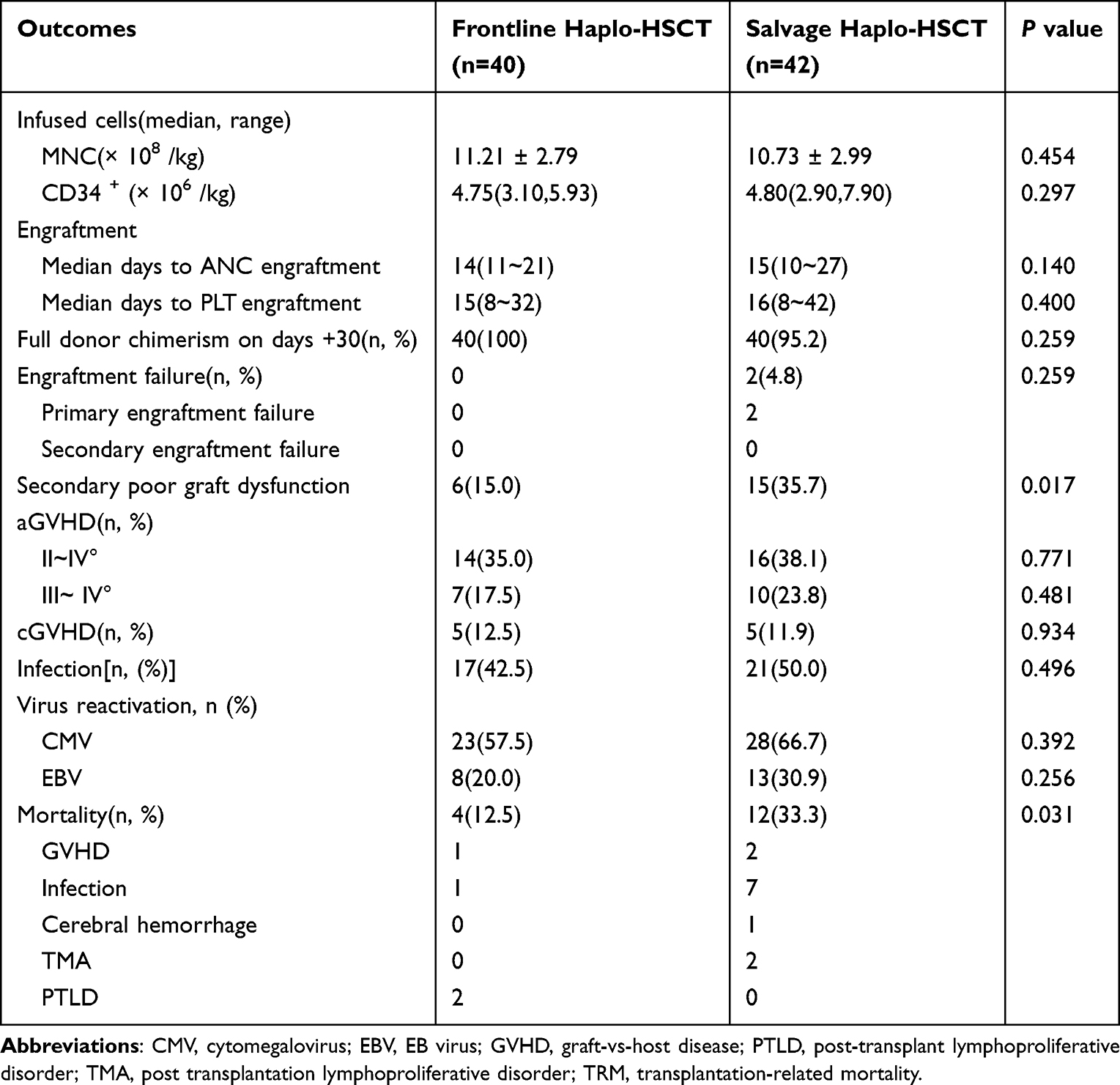 |
Table 2 Outcomes of Transplantation and Associated Data |
GVHD
The incidence of grade II–IV aGVHD in the frontline haplo-HSCT group and the salvage Haplo-HSCT group, was 35% (14/40) and 38.1% (16/42) (=0.771). The incidence of grade III–IV aGVHD in the both group was 17.5% (7/40) and 23.8% (10/42) (p=0.481). The incidence of cGVHD in the both group was 12.5% (5/40) and 11.9% (5/42) (p=0.934), respectively. No significant differences in the incidence of grade II–IV aGVHD, grade III–IV aGVHD, or cGVHD between the two groups were observed (Figure 2).
 |
Figure 2 The cumulative incidence of GVHD after transplantation in the Frontline Haplo-HSCT and Salvage Haplo-HSCTgroups. (A) Grade II–IV aGVHD. (B) Grade III–IV aGVHD. (C) cGVHD. |
The multivariate analysis of grade II–IV GVHD revealed that the conditioning regime consisted of Flu/Cy + ATG (HR: 0.255, 0.078–0.829), ABO compatibility (HR: 0.360, 0.141–0.918) were independent protective factors (Table 3). We did not find the independent risk factors associated with II–IV aGVHD. Salvage HSCT treatment (HR: 5.009, 1.057–23.729) and pre-transplant ferritin >1000ug/L (HR: 4.893, 1.427–16.781) were independent risk factors for grade III–IV aGVHD (Table 3). Univariate analysis showed that MSC infusion was associated with the occurrence of grade II–IV aGVHD, but multivariate analysis showed that none of grade II–IV aGVHD, grade III–IV aGVHD, or cGVHD was associated with MSC infusion (Figure 3).
 |
Table 3 Multivariate Analysis of Adverse Factors Associated with GVHD, PGF and Survival Outcomes |
 |
Figure 3 The cumulative incidence of GVHD with MSC infusion. (A) Grade II–IV aGVHD. (B) Grade III–IV aGVHD. (C) cGVHD. |
Secondary Poor Graft Dysfunction
Six of 40 patients (15%) in the frontline group and 15 of 42 patients (35.7%) in the salvage group experienced graft dysfunction, and the incidence of poor graft dysfunction in the salvage HSCT group was significantly higher (p=0.017) (Figure 4). The multivariate analysis revealed that salvage haplo-HSCT (HR: 5.344, 1.904–14.995), ferritin >1000ug/L (HR: 5.588, 1.696–18.414) and CMV infection (HR: 11.909, 2.335–60.725) were the independent risk factors (Table 3), and MSC infusion was not associated with the incidence of poor graft dysfunction (Figure 4).
 |
Figure 4 The cumulative incidence of sPGF after transplantation in the Frontline Haplo-HSCT and Salvage Haplo-HSCTgroups (A) and MSC infusion (B). |
Infections
The incidence of infection after HSCT was 42.5% (17/40) in the frontline group and 50.0% (21/42) in the salvage group. No significant differences in the incidence of infection between the two groups were observed (p=0.496) (Table 2). The most common infection was the pulmonary infection (17 of 82 patients) followed by the blood stream infection.
On 100 days post-transplantation, the most common infection was the CMV viremia, which occurred in 23 (57.5%) patients receiving frontline haplo-HSCT and 28 (66.7%) patients receiving salvage haplo-HSCT (p=0.392). Two cases developed CMV disease (1 CMV retinitis and 1 CMV enteritis). Of them, 1 case was CMV enteritis which improved, and the other one was CMV retinitis, who lost vision in the right eye. Epstein–Barr virus viremia occurred in 8 (20.0%) and 13 (30.9%) patients in the frontline and salvage haplo-HSCT groups, respectively (p=0.256). Two cases developed lymphoproliferative disorders (PTLD), both of them died. One of whom died in 2 months post-transplantation resulting in hemophagocytic syndrome. The other one case, a 31-year-old male patient was diagnosed with PTLD three months after transplantation and received six courses of rituximab (600 mg) treatment. At ten months post-transplantation, a biopsy of a pharyngeal mass confirmed the diagnosis of NK/T-cell lymphoma. The patient was subsequently treated with the CELOP regimen (cyclophosphamide, etoposide, vincristine, pegaspargase, and dexamethasone). However, during the myelosuppression phase following chemotherapy, the patient developed cerebral hemorrhage secondary to thrombocytopenia, ultimately resulting in death.
Survival
The endpoint of follow-up was January 1, 2024. The median follow-up for surviving patients was 44 (range, 12–126) months. A total of 66 patients survived by the end of follow-up. The 5-year OS of the frontline HSCT group was 90.0% (36/40), and the mortality rate was 10.0% (4/40) with 1 death from GVHD, 1 death from infection, and 2 deaths from PTLD. In the salvage HSCT group, the 5-year OS was 71.4%(30/42), and the mortality rate was 28.6%(12/42) with 2 deaths from GVHD, 7 deaths from infection, 1 death from cerebral hemorrhage, and 2 deaths from TMA. A statistically significant difference was observed in the cumulative mortality rate between the 2 groups (p=0.029) (Figure 5). All 12 patients who died in the salvage HSCT group had high-risk factors. Among them, 6 patients had a disease duration of more than 96 months, 3 of whom combined with cardiac and renal dysfunction. Four of the patients with a disease duration of less than 1 year had VSAA and 1 patient was >50 years old. Also, 9 of the 12 dead cases were with ferritin >1000ug/L. The 5-year estimated OS was significantly higher in the frontline HSCT group than in the salvage HSCT group (89.8% versus 71.0%, p=0.029) (Figure 6).
 |
Figure 5 The cumulative incidence of TRM after HSCT in the Frontline Haplo-HSCT and Salvage Haplo-HSCTgroups. |
 |
Figure 6 OS in the Frontline Haplo-HSCT and Salvage Haplo-HSCTgroups. |
The multivariate analysis revealed that salvage HSCT (HR: 6.883, 1.094–43.297), ECOG score ≥1 (HR: 7.638, 1.829–31.903), and ferritin >1000ug/L (HR: 7.545, 1.745–32.624) were the independent risk factors for prognosis (Table 3).
Discussion
Considering the risk of infection and bleeding, treatment should be initiated as soon as possible once SAA is diagnosed. For patients ≤40 years old with an MSD, the vast majority of patients can successfully achieve hematopoietic reconstruction after allogeneic HSCT, which is based on suppressing immunity and removing hematopoiesis. Hematopoiesis is restored in approximately two weeks, and this method has clear advantages over IST for significantly lower mortality related to bleeding and infection. Considering advantages mentioned above, there is no doubt that allogeneic HSCT is the frontline option for younger patients with MSD. However, for approximately 2/3 patients lack of a suitable MSD, IST combined with TPO-RA or MUD-HSCT may be a viable option.15 However, a problem which cannot be ignored is that a proportion of patients experience treatment failure after IST. IST is associated with a significant risk of relapse and clonal evolution,16 according to previous reports. Additionally, IST frequently results in the improvement of cytopenia rather than curing it,2,9 for IST maintains residual hematopoietic function.9 Therefore, this proportion of patients still need to accept salvage HSCT. Under these circumstances, haplo-HSCT is an alternative, especially considering the demographic composition of Chinese family. Currently, with the advance of HSCT, such as the optimization of donor selection, the modification of the conditioning regimen, the development in T cell manipulations, the supportive care of transplant-related complications, the long-term OS shows a significant improvement and the incidence of GVHD is more acceptable,17 all of which remove the insurmountable obstacles to the application of haplo-HSCT.
Recently, HID-HSCT has achieved comparable clinical efficacy to MSD-HSCT in both first-line and salvage treatment of SAA.18–20 In a retrospective study carried out in 342 SAA patients,21 no statistically significant difference was observed in 9-year OS and FFS between first-line haplo-HSCT and first-line MSD (87.1±2.5% vs 89.3±3.7%, P=0.173 and 86.5±2.6% vs 88.1±3.8%, P=0.257), and during long-term follow-up, the rates of return to normal life for first-line haplo-HSCT and first-line MSD patients were essentially equivalent. This result implied that first-line haplo-HSCT could be an alternative option for SAA patients without an MSD or URD. Therefore, regarding the SAA treatment guideline, British Society for hematology recommends HID-HSCT as second-line treatment following failed IST therapy for refractory SAA.12 In addition, haplo-HSCT is currently the first-line treatment of option for younger patients who lack an MSD or URD, according to the consensus from The Chinese Society of Hematology.8 In a research by Liu et al,22 the results suggested that the rate of normal blood counts in the HID-HSCT group was significantly higher than that in the IST group (90.8% vs 18.8%, p<0.0001), as well as the rate of FFS and the rate of healthy living (77.8% vs 48.0%, p<0.0001). In a retrospective analysis of IST and haplo-HSCT as the treatment of 491 young patients with SAA/VSSA in East Asia,23 Geng C et al noticed that there was a significant difference in FFS between the two groups (P<0.05), with a substantial reduction in FFS in the IST group with time, but essentially stable FFS in the haplo-HSCT group. Furthermore, Cheng Y et al24 found that FFS was significantly lower in the frontline IST group than in the frontline haplo-HSCT group (52.6±10.5% versus 89.3±5.8, P=0.008), and in the analysis of single factor and multi-factor regression, the only risk factor of FFS was the use of IST instead of haplo-HSCT. In another trial25 comparing the efficacy of first-line haplo-HSCT and IST as the treatment for patients with SAA, the results showed that although OS was essentially comparable between the two groups, FFS was significantly higher in the first-line haplo-HSCT group than in the IST group, while hematopoietic reconstitution was faster in the former group. With the use of platelet receptor agonists, the superiority of the efficacy of MRD-HSCT and IST combined with eltrombopag has drawn people’s attention. A multicenter prospective study found that although no statistical differences in 3-year OS were noted between the MRD-HSCT group and the IST+EPAG group (84.2%±3.5% vs 89.7±3.1%, P=0.164), the difference in 3-year FFS was significant (81.4%±4.0% vs 59.1±4.9%, P=0.002).26 This result suggests that MRD-HSCT remains a first-line treatment option for patients aged <40 years. In this research, the median follow-up for all patients was 44 (range, 12–126) months, and the 5-year estimated FFS was 89.8%, which were consistent with the literature reported before.15
However, haplo-HSCT as a frontline treatment is still not widely accepted, with many guidelines preferring it as a salvage therapy in the event of failure of frontline IST.12 For refractory relapsed AA is a highly lethal bone marrow failure disease, allogeneic HSCT is usually recommended for this group of patients. However, only a minority of patients have an MSD. As a result, a growing number of experienced transplant centers are attempting haplo-HSCT. Comparing the haplo-HSCT as the first-line and salvage treatment of SAA, Dufour C et al27 found that though salvage haplo-HSCT after failure of IST still achieved acceptable OS and FFS, the salvage HSCT group had a higher incidence of aGVHD and cGVHD, and the rate of OS in patients aged >12 years decreased with age, and the incident of secondary tumors increased, either. A recent study10 retrospectively evaluated the clinical data of 49 patients divided into frontline IST group, n=29 (including savage haplo-HSCT group after IST failure, n=12), and frontline haplo-HSCT group, n=20. Though the incidences of aGVHD, cGVHD and severe infections were comparable between the salvage haplo-HSCT group and frontline haplo-HSCT group, a significant difference in the 3-year EFS was observed (41.7% versus 80.0%, P=0.046). A multicenter prospective study from the BMT CTN28 showed an 1-year OS of 81% (95% CI: 62–91) for salvage haplo-HSCT and recommend haplo-HSCT as the salvage therapy for SAA. Xu LP et al19 included 287 patients with refractory relapsed SAA who underwent salvage haplo-HSCT, with a median follow-up of 4.56 years, and a 9-year estimated OS and FFS of 85.4±2.1% and 84.0%±2.2%, respectively. In this study, age and ECOG were independent prognostic factors affecting survival. In another similar study including 41 patients treated with salvage haplo-HSCT,29 the median follow-up was 26 months and the 3-year OS was 80.3% ± 5.1%. The studies mentioned above suggested that salvage haplo-HSCT could be an option for SAA after IST failure. However, comparing with first-line haplo-HSCT, salvage haplo-HSCT has an elevated incidence of aGVHD and cGVHD.
In this research, we retrospectively assessed the clinical data and prognosis of young adult with SAA who underwent frontline haplo-HSCT and salvage haplo-HSCT after IST failure, respectively. No significant differences are observed in the median time of hematopoietic reconstruction, and the incidences of aGVHD, cGVHD and severe infection between the two groups. Whereas, compared with the salvage haplo-HSCT group, the 5-year estimated OS was significantly higher in the front-line HSCT group (89.8% versus 71.0%, p=0.029), and it is comparable with that in patients who received MSD-HSCT in a study reported before.15 In addition, all 12 dead cases in the salvage HSCT group had high-risk factors: 6 patients had a disease duration of more than 96 months, 3 of whom combined with cardiac and renal dysfunction. Four of the patients with a disease duration of less than 1 year had VSAA, and 1 patient was >50 years old. Also, 9 of the 12 dead cases were with ferritin >1000ug/L. The discrepancy in survival and engraftment failure rates between the two groups could be attributed to iron overload, continued transfusions, increased susceptibility to infection, and the time to HSCT after diagnosis. As a result, front-line haplo-HSCT rather than salvage haplo-HSCT is recommended for SAA patients without MSD or MUD.
Just as previous studies have shown, iron overload could lead to increased mortality, graft failure, and increased incidence of GVHD. In this research, a greater proportion of cases in the salvage HSCT group showed ECOG status scores exceeding 1. While the number of patients with ferritin levels more than 1000 ug/L did not differ significantly between the two groups, the extent of ferritin elevation was higher in the salvage HSCT group. Additionally, the incidence of III~IV°GVHD and graft failure was significantly higher among patients with elevated ferritin levels, which was also identified as an independent risk factor of mortality. Xu LP et al showed a more favorable implantation rate using G-CSF/ATG as pretreatment regime.20
MSCs are critical supportive cells within the bone marrow microenvironment. Over recent decades, the clinical application has increased due to their notable immunomodulatory effects. SAA, characterized by bone marrow failure, has been confirmed to be abnormal in the bone marrow microenvironment. Studies have shown that when co-cultured with MSCs from patients with AA, both the proliferative capacity and clone-forming ability of peripheral blood mononuclear cells and CD34+ cells are significantly reduced.30–32 Bone marrow-derived MSCs, located in the bone marrow stroma, are essential for immunomodulation and hematopoietic support. Their immunomodulatory functions primarily depend on cytokine secretion and enhanced cell–cell contact.33 Given their biological properties such as immunomodulation, tissue repair, angiogenesis, and anti-apoptotic effects, MSCs are increasingly utilized in cell therapy.34 Bone marrow stromal cell damage from radiotherapy prior to allogeneic hematopoietic stem cell transplantation may also result in delayed stem cell implantation, thus limiting clinical application. Although HSCT offers a potential cure for AA, complications such us bone marrow stromal cell damage arising from pre-transplant radiotherapy may also result in delayed engraftment, thus limiting clinical application. Ding et al devised a protocol combining HSCT with MSC reinfusion, reporting a median follow-up of 40 months and an OS rate of 87.15 ± 3.3%. MSCs have demonstrated efficacy in preventing and treating GVHD. Umbilical cord-derived MSCs, in particular, have shown potential for reducing GVHD incidence, and promoting engraftment.35 However, concerns that MSCs may increase the risk of post-transplant viral and bacterial infections still exist. Recently, MSC infusions administered on day +4 in both the frontline and salvage treatment groups from June 2021 onwards could reduce GVHD incidence, but there was no significant difference in engraftment rates between the two groups.
Undeniably, there are several limitation in this research. A prospective multicenter study should be conducted to further confirmed the results in the future as this is a retrospective research with a relative small sample size. Despite the fact that the aforementioned baseline conditions are not significantly different, individuals in the salvage treatment group typically had worse general conditions following IST failure. As a result, it is challenging to identify the primary causes of the frontline haplo-HSCT group’s improved prognosis. Additionally, the usage of rabbit ATG instead of horse ATG may have an impact on the efficacy of IST. Furthermore, access to a suitable donor and financial issues may influence the treatment option.
In conclusion, compared with salvage haplo-HSCT, frontline haplo-HSCT shows superior efficacy and safety for pediatric and younger adult patients with primary SAA lacking MSD, though further validation in broader age groups is warranted. However, it still need more confirmation with a larger size of samples.
Data Sharing Statement
This declaration is not applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work. This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-4954353/v1.
References
1. Young NS. Aplastic Anemia. N Engl J Med. 2018;379(17):1643–1656. doi:10.1056/NEJMra1413485
2. Peslak SA, Olson T, Babushok DV. Diagnosis and treatment of aplastic anemia. Curr Treat Options Oncol. 2017;18(12):70. doi:10.1007/s11864-017-0511-z
3. Young NS, Kaufman DW. The epidemiology of acquired aplastic anemia. Haematologica. 2008;93(4):489–492. doi:10.3324/haematol.12855
4. Montané E, Ibáñez L, Vidal X, et al. Epidemiology of aplastic anemia: a prospective multicenter study. Haematologica. 2008;93(4):518–523. doi:10.3324/haematol.12020
5. Issaragrisil S, Kaufman DW, Anderson T, et al. The epidemiology of aplastic anemia in Thailand. Blood. 2006;107(4):1299–1307. doi:10.1182/blood-2005-01-0161
6. Barone A, Lucarelli A, Onofrillo D, et al. Diagnosis and management of acquired aplastic anemia in childhood. guidelines from the marrow failure study group of the pediatric haemato-oncology Italian association (AIEOP). Blood Cells Mol Dis. 2015;55(1):40–47. doi:10.1016/j.bcmd.2015.03.007
7. Pongtanakul B, Das PK, Charpentier K, Dror Y. Outcome of children with aplastic anemia treated with immunosuppressive therapy. Pediatr Blood Cancer. 2008;50(1):52–57. doi:10.1002/pbc.21377
8. Zhang XH, Chen J, Han MZ, et al. The consensus from The Chinese Society of Hematology on indications, conditioning regimens and donor selection for allogeneic hematopoietic stem cell transplantation: 2021 update. J Hematol Oncol. 2021;14(1):145. doi:10.1186/s13045-021-01159-2
9. Yoshida N, Kobayashi R, Yabe H, et al. First-line treatment for severe aplastic anemia in children: bone marrow transplantation from a matched family donor versus immunosuppressive therapy. Haematologica. 2014;99(12):1784–1791. doi:10.3324/haematol.2014.109355
10. Yang S, Yuan X, Ma R, et al. Comparison of outcomes of frontline immunosuppressive therapy and frontline haploidentical hematopoietic stem cell transplantation for children with severe aplastic anemia who Lack an HLA-matched sibling donor. Biol Blood Marrow Transplant. 2019;25(5):975–980.
11. Chang YJ, Zhao XY, Huang XJ. Granulocyte colony-stimulating factor-primed unmanipulated haploidentical blood and marrow transplantation. Front Immunol. 2019;10:2516. doi:10.3389/fimmu.2019.02516
12. Killick SB, Bown N, Cavenagh J, et al. Guidelines for the diagnosis and management of adult aplastic anaemia. Br J Haematol. 2016;172(2):187–207. doi:10.1111/bjh.13853
13. Harris AC, Young R, Devine S, et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: a report from the mount sinai acute GVHD international consortium. Biol Blood Marrow Transplant. 2016;22(1):4–10. doi:10.1016/j.bbmt.2015.09.001
14. Jagasia MH, Greinix HT, Arora M, et al. national institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: i. the 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. 2015;21(3):389–401.e1. doi:10.1016/j.bbmt.2014.12.001
15. Samarasinghe S, Steward C, Hiwarkar P, et al. Excellent outcome of matched unrelated donor transplantation in paediatric aplastic anaemia following failure with immunosuppressive therapy: a United Kingdom multicentre retrospective experience. Br J Haematol. 2012;157(3):339–346. doi:10.1111/j.1365-2141.2012.09066.x
16. Kamio T, Ito E, Ohara A, et al. Relapse of aplastic anemia in children after immunosuppressive therapy: a report from the Japan childhood aplastic Anemia study group. Haematologica. 2011;96(6):814–819. doi:10.3324/haematol.2010.035600
17. Liu Z, Zhang Y, Xiao H, et al. Cotransplantation of bone marrow-derived mesenchymal stem cells in haploidentical hematopoietic stem cell transplantation in patients with severe aplastic anemia: an interim summary for a multicenter Phase II trial results. Bone Marrow Transplant. 2017;52(5):704–710. doi:10.1038/bmt.2016.347
18. Xu LP, Wang SQ, Wu DP, et al. Haplo-identical transplantation for acquired severe aplastic anaemia in a multicentre prospective study. Br J Haematol. 2016;175(2):265–274. doi:10.1111/bjh.14225
19. Lp X, Zl X, Wang SQ, et al. Long-term follow-up of haploidentical transplantation in relapsed/refractory severe aplastic anemia: a multicenter prospective study. Sci Bull. 2022;67(9):963–970. doi:10.1016/j.scib.2022.01.024
20. Xu LP, Jin S, Wang SQ, et al. Upfront haploidentical transplant for acquired severe aplastic anemia: registry-based comparison with matched related transplant. J Hematol Oncol. 2017;10(1):25. doi:10.1186/s13045-017-0398-y
21. Zl X, Lp X, Wu DP, et al. Comparable long-term outcomes between upfront haploidentical and identical sibling donor transplant in aplastic anemia: a national registry-based study. Haematologica. 2022;107(12):2918–2927. doi:10.3324/haematol.2022.280758
22. Liu L, Zhang Y, Jiao W, et al. Comparison of efficacy and health-related quality of life of first-line haploidentical hematopoietic stem cell transplantation with unrelated cord blood infusion and first-line immunosuppressive therapy for acquired severe aplastic anemia. Leukemia. 2020;34(12):3359–3369. doi:10.1038/s41375-020-0933-7
23. Geng C, Liu X, Chen M, Yang C, Han B. Comparison of frontline treatment with intensive immunosuppression therapy and HLA-haploidentical hematopoietic stem cell transplantation for young patients with severe aplastic anemia - A meta analysis. Leuk Res. 2020;88:106266. doi:10.1016/j.leukres.2019.106266
24. Cheng Y, Xu Z, Zhang Y, et al. First-line choice for severe aplastic anemia in children: transplantation from a haploidentical donor vs immunosuppressive therapy. Clin Transplant. 2018;32(2). doi:10.1111/ctr.13179.
25. Xu ZL, Zhou M, Jia JS, et al. Immunosuppressive therapy versus haploidentical transplantation in adults with acquired severe aplastic anemia. Bone Marrow Transplant. 2019;54(8):1319–1326. doi:10.1038/s41409-018-0410-3
26. Liu L, Lei M, Fu R, et al. Matched related transplantation versus immunosuppressive therapy plus eltrombopag for first-line treatment of severe aplastic anemia: a multicenter, prospective study. J Hematol Oncol. 2022;15(1):105. doi:10.1186/s13045-022-01324-1
27. Dufour C, Pillon M, Passweg J, et al. Outcome of aplastic anemia in adolescence: a survey of the severe aplastic Anemia working party of the European group for blood and marrow transplantation. Haematologica. 2014;99(10):1574–1581. doi:10.3324/haematol.2014.106096
28. DeZern AE, Eapen M, Wu J, et al. Haploidentical bone marrow transplantation in patients with relapsed or refractory severe aplastic anaemia in the USA (BMT CTN 1502): a multicentre, single-arm, Phase 2 trial. Lancet Haematol. 2022;9(9):e660–e9. doi:10.1016/S2352-3026(22)00206-X
29. Lu Y, Sun RJ, Zhao YL, et al. Unmanipulated haploidentical hematopoietic stem cell transplantation achieved outcomes comparable with matched unrelated donor transplantation in young acquired severe aplastic anemia. Biol Blood Marrow Transplant. 2018;24(9):1881–1887. doi:10.1016/j.bbmt.2018.05.015
30. Medinger M, Drexler B, Lengerke C, Passweg J. Pathogenesis of acquired aplastic anemia and the role of the bone marrow microenvironment. Front Oncol. 2018;8:587. doi:10.3389/fonc.2018.00587
31. Schoettler ML, Nathan DG. The pathophysiology of acquired aplastic anemia: current concepts revisited. Hematol Oncol Clin North Am. 2018;32(4):581–594. doi:10.1016/j.hoc.2018.03.001
32. Hamzic E, Whiting K, Gordon Smith E, Pettengell R. Characterization of bone marrow mesenchymal stromal cells in aplastic anaemia. Br J Haematol. 2015;169(6):804–813. doi:10.1111/bjh.13364
33. Broglie L, Margolis D, Medin JA. Yin and Yang of mesenchymal stem cells and aplastic anemia. World J Stem Cells. 2017;9(12):219–226. doi:10.4252/wjsc.v9.i12.219
34. Galderisi U, Peluso G, Di Bernardo G. Clinical trials based on mesenchymal stromal cells are exponentially increasing: where are we in recent years? Stem Cell Rev Rep. 2022;18(1):23–36. doi:10.1007/s12015-021-10231-w
35. Ding L, Han DM, Zheng XL, et al. A study of human leukocyte antigen-haploidentical hematopoietic stem cells transplantation combined with allogenic mesenchymal stem cell infusion for treatment of severe aplastic anemia in pediatric and adolescent patients. Stem Cells Transl Med. 2021;10(2):291–302. doi:10.1002/sctm.20-0345
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.