Back to Journals » Psychology Research and Behavior Management » Volume 12
Effect of eye movement desensitization and reprocessing (EMDR) on severity of stress in emergency medical technicians
Authors Behnammoghadam M, Kheramine S ![]() , Zoladl M, Cooper RZ, Shahini S
, Zoladl M, Cooper RZ, Shahini S ![]()
Received 10 October 2018
Accepted for publication 27 February 2019
Published 18 April 2019 Volume 2019:12 Pages 289—296
DOI https://doi.org/10.2147/PRBM.S190428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Mohammad Behnammoghadam,1 Shirali Kheramine,2 Mohammad Zoladl,3 Rebecca Zahra Cooper,4 Sharif Shahini1
1Student Research Committee, Yasuj University of Medical Sciences; 2Clinical Psychology, School of Medicine, Social Determinants of Health, Research Center, Yasuj University of Medical Sciences; 3Department of Nursing, Yasuj University of Medical Sciences, Yasuj, Iran; 4Psychology, Murdoch University, Perth, Australia
Background and objectives: People working in health care centers and hospitals, especially the emergency departments, often experience severe stresses due to the nature of their jobs. The current study was aimed at determining the effect of eye movement desensitization and reprocessing (EMDR) on severity of stress of medical emergency technicians.
Materials and methods: In the current field trial, 50 emergency medical technicians working in emergency medical centers were selected by convenience sampling method and randomly assigned to either the intervention or control group; each group had 25 subjects. In the intervention group, EMDR training was provided during five consecutive sessions, while in the control group the subjects did not receive any intervention. The data collection instrument in the study, in addition to the demographic questionnaire, was the Alken stress scale. Data had normal distribution and were analyzed using independent t, the Mann–Whitney, or chi-squared tests, and their within-group comparisons were performed by paired t and marginal homogeneity tests.
Results: The mean score of stress before and after the intervention in the intervention and control groups was 32.2±7.8 and 33.6±13.8, respectively. However, after EMDR implementation, the intensity of stress in the intervention and control groups was 25.9±7.3 and 33±13.1, respectively and the difference between the groups was statistically significant (P<0.05). Chi-squared test showed that after the intervention, the degree of stress intensity in the experimental group was lower than that of the control group, and there was a significant difference between the groups in terms of stress intensity (P<0.05).
Conclusion: The current study results indicated that EMDR technique significantly reduced the intensity of stress in the intervention group and can be helpful to control stress experienced by emergency medical staff.
Keywords: stress, emergency medical technicians, eye movement desensitization reprocessing
Introduction
Generally, stress is defined as a stimulus or response that is associated with physiological seizure and anxiety.1 Cognitive-relational theory is one of the best theories in stress and stress tolerance, first proposed by Lazarus and Folkman in 1984. Based on this theory, stress is defined as a special relationship between the person and his environment, in such a way that the person evaluates stress as an over-fulfilling task or expectation and considers it as a threat to his resources or welfare.1
Stress and anxiety are commonly experienced by all humans, but some people are more likely to be subjected to this tense situation based on the nature of their jobs.2 They include medical and therapeutic staff, especially medical emergency technicians, that face many challenges due to stressful conditions in the workplace and the care of dying patients or the ones in emergency situations. According to the fact that it is the medical emergency team that first faces the accident scene, they are more susceptible to stress and anxiety.3 Any mistakes caused by lack of stress control in this occupation can lead to loss of life.4,5 Research also suggests that long-term exposure to occupational stresses can lead to job burnout, post-traumatic stress disorder (PTSD), and consequently, a reduction in feelings, commitment, and loss of motivation.5
Stress and job burnout not only threaten the health and well-being of clinicians and medical technicians, but they are also associated with medical errors and lower quality of medical care.6,7
Therefore, since emergency medical personnel have a great deal of responsibility (they are responsible for people's lives) and the nature of their jobs requires contact with patients in acute or expired situations, they need to receive anxiety control and treatment training.8 We reviewed and presented different stress control methods. Psychological treatments such as cognitive-behavioral therapy (CBT), massage therapy, exercise, cognitive therapy, muscle relaxation, music therapy, aromatherapy, and guided-imagery therapy are among them.
Eye movement desensitization and reprocessing (EMDR) is one of the stress management methods. It is a new and safe method without any side effects and does not rely on speech therapy and drug therapy, but only uses regular and rapid movements of the patients' eyes.9
This therapeutic method has been used for different populations such as children, couples, victims of sexual assault, people with anxiety disorders, people with depression, and people with phantom pain, etc.10
Studies show that this method is rather successful in controlling stress and anxiety of individuals in different situations and results showed that EMDR leads to stress control and promotion of health in patients undergoing hemodialysis.11 It is also a successful technique in controlling stress and anxiety in people who experienced unpleasant events such as war, earthquake, and rape.11–14
Another study evaluated the effectiveness of this technique in people who recently experienced stressful situations. Their results showed the effectiveness of EMDR techniques and the prevention of subsequent stresses in such patients.15
Haugen et al, in a review study, showed that compared with other methods, EMDR technique was more effective in reducing and controlling stress in police officers, firefighters, and emergency medical personnel.16
Although studies indicate high anxiety and stress experienced by medical staff, few studies have looked at the importance of stress management and effective stress management methods among nurses, health care professionals, students, and emergency medical technicians.2,3,17 Considering the raised issues and the necessity of paying attention to mental and physical health of medical emergency technicians who are responsible for the health of the community, the current study was aimed at evaluating the effect of EMDR technique on the intensity of stress experienced by medical emergency technicians.
Materials and methods
The current placebo-controlled, field trial study was registered on the Iranian Clinical Trial Registry Website (code: IRCT20180102038191N1). The study population consisted of all emergency medical technicians working at Medical Emergency Services, urban and road stations in Kohgiluyeh and Boyer-Ahmad Province in 2017. The inclusion criteria were: employed as one of the technician classes (rescuer, basic, middle, or senior technician) at 115 center of pre-hospital medical emergency services, age range 18–55 years, working at 115 pre-hospital medical emergency services as their main job, not employed in administrative departments or communication center of 115 pre-hospital medical emergency services, no drug addiction, no hearing or vision impairment, and concurrently, getting scores above 19 in the Alken stress scale, and provided written informed consent to participate in the study. The exclusion criteria were: no motivation to cooperate, intolerance to the treatment, absent for more than one therapeutic session, imprecise completion of data collection instruments, transfer or death of the technician.
The sample size was set to 50 individuals based on calculations and including 20% probable dropouts; as 25 subjects in each group.
The results of Raboni et al's study (2006) into the effects of desensitization with eye movement and reprocessing on the variables of situational anxiety and general stress, as the most similar variables to the dependent variables of the present study (death, anxiety, and stress), were used; which included S1=10.14, S2=4.86, µ1=47.86, and µ2=34.43 for situational anxiety and S1=1.3, S2=0.69, µ1=3.14, and µ2=1 for general stress. Then, according to the following formula and considering the type 1 error equal to 0.01 (99% confidence level) and the type 2 error equal to 10% (test power of 90%; Raboni et al, 2014b), 20.89 and 14.09 were calculated for data on situational anxiety and general stress, respectively.
Finally, considering the highest sample size needed for each of the study groups and a possible attrition of 20%, a total of 50 people was estimated as the sample size with 25 people for each group.
During random block assignment, the order of the participants in the intervention and control groups was determined as follows.
By multiplying the number of study groups (two groups) by 2, the number of samples per block was calculated as 4; then, by calculating the factorial of each block sample size (4!=4×3×2×1=24), the number of blocks generated from all possible orders was obtained as 24; since the number of people in each block was 4 and the estimated sample size was 50 based on the following description, by matching 13 random numbers generated by Sample Randomizer with the mentioned block numbers, the order of 50 research subjects was determined, numbers 1–50 were allocated to the subject and control groups, and the random allocation list was edited.
After explaining the objectives of the study and obtaining informed consent from the participants, as the first step, they were asked to complete the Elkin stress symptoms scale. In the current study, the stress symptom scale, developed by Elkin in 1999, was employed to measure the degree and level of stress intensity.18 This scale, applicable to all age groups, includes 41 symptoms of stress and to complete it, the person has to determine the status of each of the symptoms in the last 2 weeks based on a four-option Likert scale from never (0) to always.3 Total scores range from 0–132, and higher scores indicate higher stress levels. On this scale, stress intensity is graded as follows: score 0–19 below average, 20–39 average, 40–49 relatively higher than average, and 50 and over much higher than average.19
In the current study, the original scale was translated from English into Persian and after back-translation into English the contents were adapted to those of the original version; then, the Persian version was reviewed by five professors of psychology, English language, and Persian language and literature, and modifications and revisions were made; accordingly, the content and formal validity of the Elkin stress symptoms scale were confirmed. It is noteworthy that based on the data of the current study, the reliability of this scale using the Cronbach’s alpha coefficient was 0.87.
A number was assigned to the subjects who concurrently got a score of above 19 in the SSS, and by matching that number with the block random allocation list, the technicians were assigned to the intervention or control group, and the process was continued until the completion of the estimated sample size.
Subjects in the intervention group received EMDR training in five consecutive 45–90 sessions, as a research intervention based on the approved protocol, and according to the following eight stages:
- History taking and treatment design: while communicating with the subject, the history was taken and the treatment process was designed.
- Preparation: by describing the process, the subject was being prepared for EMDR implementation.
- Evaluation: the subjects were asked to recall the problematic distressing events and measure their subjective units of disturbance using an 11-degree mental disorder scale from 0–10. Zero means a lack of mental discomfort, and 10 means the maximum mental discomfort. Then, in a test to assess the validity of cognitions as one of the other pre-test scales, they were asked to express their positive beliefs and rank it from 1–7 in a seven-point scale. One means completely false and 7 means perfectly true. Then, after applying this technique, both of the scales were re-evaluated.
- Desensitization: according to Shapiro, the inventor of this technique, at this stage the subject is asked to imagine the most prominent part of an annoying scene, focusing on the negative recognition of the scene that the subject previously described in a brief sentence expressing a harmful event such as “I am guilty“ or “it is really terrible or disturbing to me“, to concentrate on emotions and physical states related to tension and anxiety, and then, after determining which part of the body is affected by the anxiety, the subject is instructed to follow the rapid movements of the therapist’s finger just about 30 cm away from his eyes, from right to left and vice versa, across his field of vision. This movement involves two rounds of trips to the sides within 1 second, which is considered a cycle, and each 24–24 cycles constitute a set. After each set, the researcher asks the subjects to stop imagining the scene, lean back into the back of their seat, and breathe deeply. Then, the level of mental discomfort and cognitive validity were ranked, evaluated, and recorded. This process, based on the need and motivation of the subjects, was continued until the level of mental discomfort reached 0 or minimum.
- Implementation: the subjects were asked to recall the positive phrases and then repeat the eye movement process.
- Physical scan: subjects were asked to focus on that part of the body that had difficulty during stress or anxiety, and evaluate the problem.
- Completion: this step was to ensure the stability of the subjects at the end of the session.
- Re-evaluation: subjects again completed subjective units of disturbance and VOC scale.20
Obviously, the previously mentioned protocol was performed for subjects in the intervention group, and the control group received no intervention.
Immediately after the completion of the research intervention, the Elkin SSS was completed as the post-test scale by the subjects. Data were analyzed with SPSS version 21 using descriptive statistics and inferential statistical tests based on the normal distribution of the study variables using the one-sample Kolmogorov-Smirnov test with 95% CI.
In the current study, due to the violation of assumptions, ANCOVA was used to ensure the consistency of the intervention and control groups at baseline; also, independent t-test was employed to compare the mean of underlying dependent variables with slight normal distribution between the subjects of the control and intervention groups, and chi-squared test was used to compare the frequency distribution of qualitative variables between the groups at the beginning of the study.
Since variables related to the level of stress severity in medical emergency technicians in all the study subjects, as well as the intervention and control groups, at the beginning of the study (pre-test) and immediately after the intervention (post-test), had a normal distribution, independent t-test was used for inter-group and paired t-test for intra-group comparisons. Also, the Mann–Whitney test was used to compare the variations in degree of stress severity between the groups. It is noteworthy that the results of chi-squared test were used for inter-group and results of marginal homogeneity test for intra-group comparisons of stress severity (qualitative dependent variables) in medical emergency technicians.
All interventional stages of the current study were approved by the Ethics Committee of Yasouj University of Medical Sciences (ethical code: IR.YUMS.REC.1396.139).
The researcher assured all the study participants that they were free to withdraw from the study at any stage. Also, all questionnaires and data collection instruments were completed anonymously and identified just based on the given codes. All collected data were confidential and were used only for the research purposes.
Results
Of the 87 respondents, the first 50 subjects were selected as eligible based on the priority of the time of returning the questionnaire and getting scores above 19 in the Alken stress scale; then, using random block allocation, the eligible subjects were allocated to either the control or intervention groups, each with 25 subjects.
Eligible subjects comprised of 30 medical emergency technicians (60%) working at 115 pre-hospital urban emergency medical stations and 20 medical emergency technicians (40%) working at 115 pre-hospital road medial emergency stations with a mean age of 31.1±5.9 years and work experience of 5.2±8 years; 19 (38%) subjects were single and 31 (62%) married; also, eleven (22%) subjects were employed based on projects, 32 (64%) based on contracts, and seven (14%) were officially employed. In terms of educational level, 20 (40%) subjects had associate degrees and 30 (60%) had bachelor’s degrees. At the beginning of the study, the subjects’ mean score in the Alken stress scale was 32.9±11.21.
The scores obtained by the intervention and control group subjects in terms of the level of stress intensity (quantitative dependent variables) and their variations, as well as the degree of stress intensity (qualitative dependent variables) at post-test (after intervention) were compared using inferential statistics.
Based on the current study results, at the beginning of the study, there was no statistically significant difference between the groups in terms of age, experience, marital status, education level, employment status, and type of emergency services station (P>0.05) (Tables 1 and 2).
 | Table 1 Comparison of the quantitative demographic variables between the study group subjects |
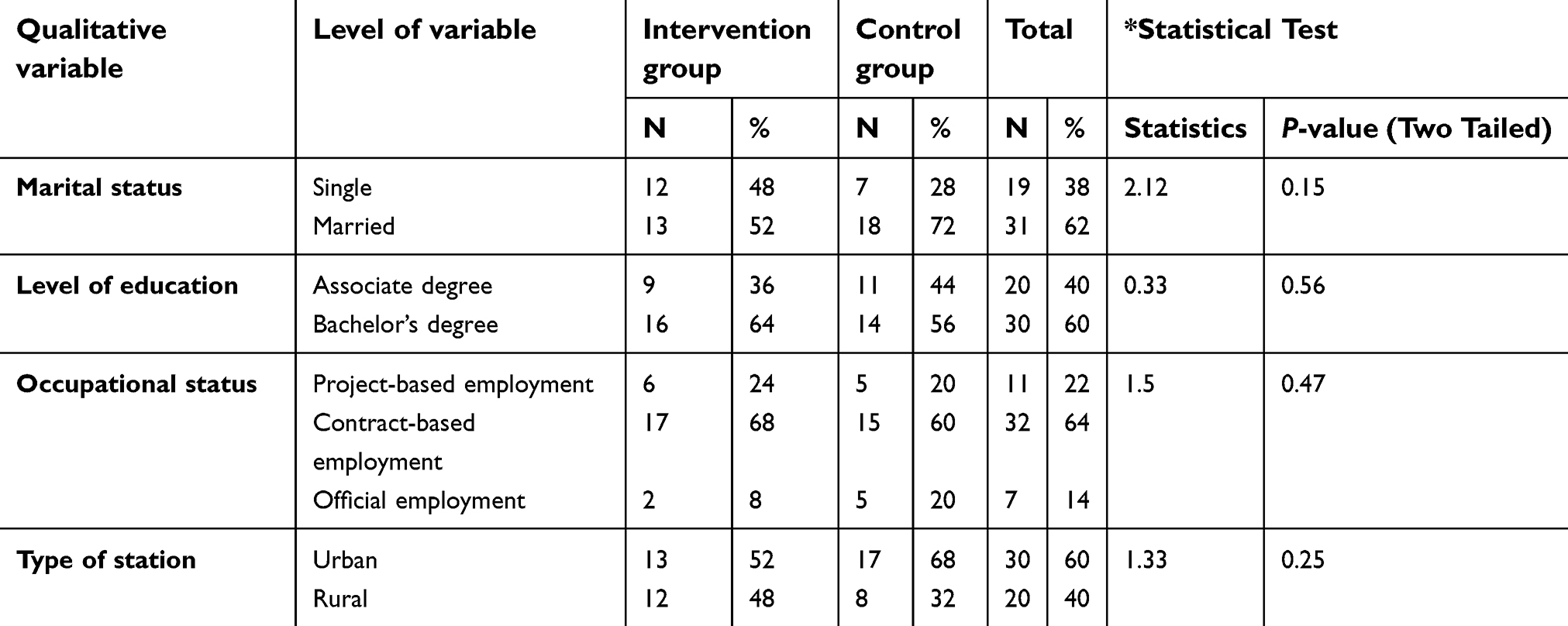 | Table 2 Frequency distribution and comparison of the qualitative demographic variables in the study group subjects |
Also, according to data presented in Table 3, in the intervention group, the level of stress intensity in medical emergency technicians significantly decreased after the intervention compared with baseline (P<0.05), but in the control group, comparison of post-test and pre-test, showed a slight decrease in the level of stress intensity compared with baseline, although the difference was statistically insignificant (P>0.05).
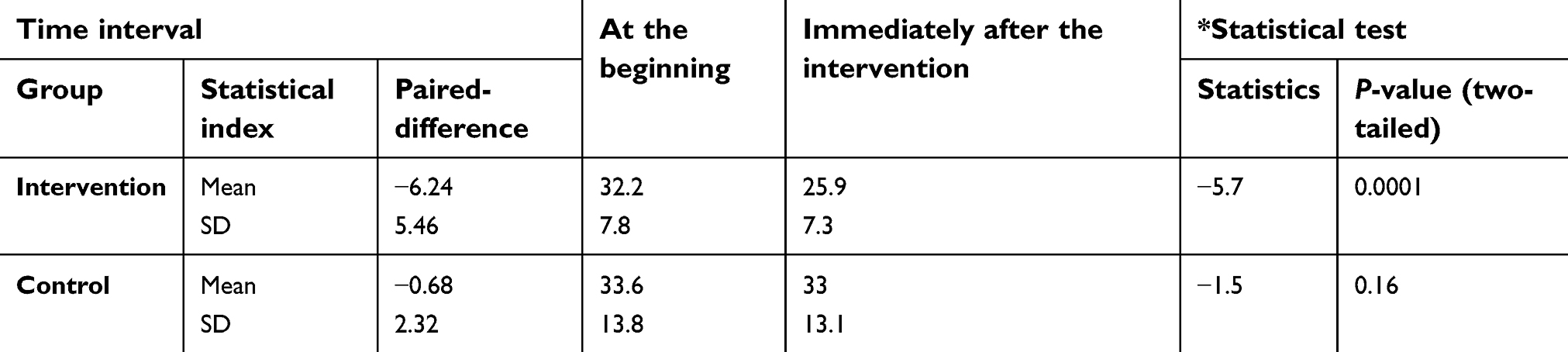 | Table 3 Within-group comparison of severity of stress experienced by medical emergency technicians based on the study groups |
Also, the frequency of stress in higher degrees and much higher than average decreased to zero after the intervention, and the results of the marginal homogeneity test confirmed the significance of decreasing the degree of stress intensity in subjects in the intervention group (P<0.05) (Table 4). However, there was no significant difference in the control group between baseline and immediately after the intervention measures in terms of the degree of stress severity (P<0.05) (Table 4).
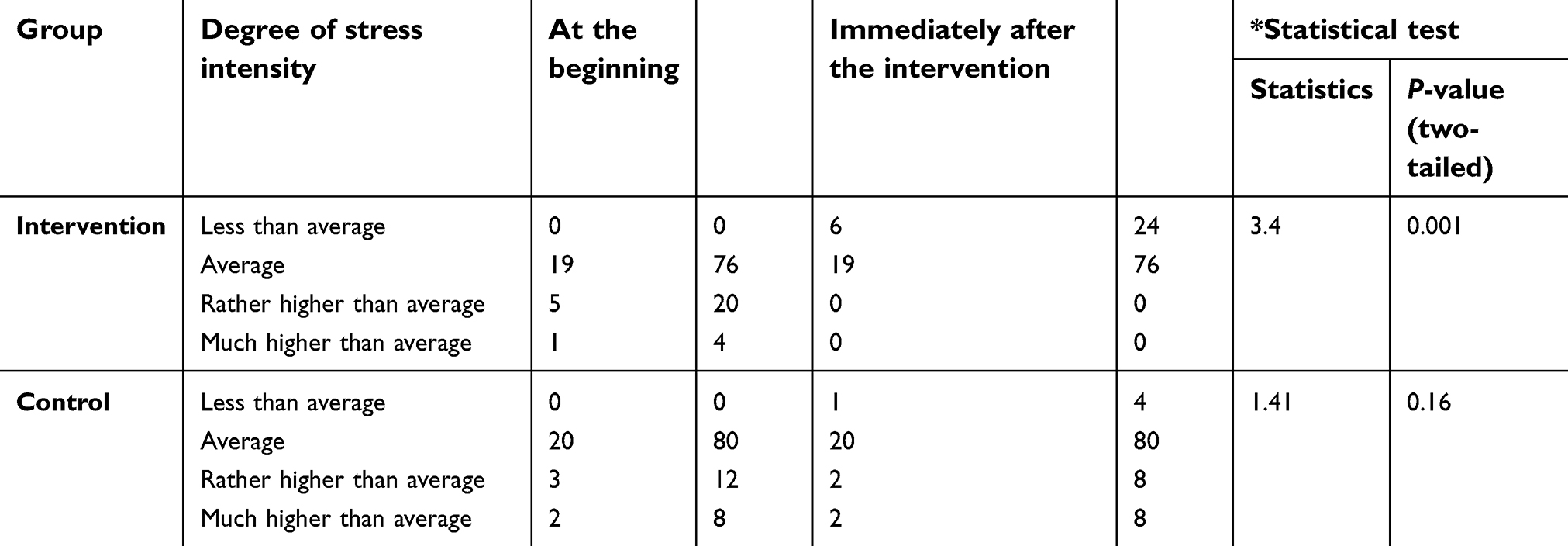 | Table 4 Within-group comparison of degree of severity of stress experienced by emergency medical technicians based on the study groups |
Discussion
Medical emergency technicians are usually the first medical group that observes the incident scene to provide on-scene treatment. Studies show that this therapeutic group is severely exposed to stress.2,3 The current study aimed at investigating the effect of EMDR technique on the stress intensity of medical emergency technicians.
The results of the current study indicated a decrease in stress intensity of medical emergency technicians after the implementation of EMDR technique.
The efficacy of EDMR method has also been shown by various studies. For example, Goldstein and Fiscse studied the effect of this technique on disruptive panic disorder and concluded that this therapeutic approach can be used as a suitable method to treat fears, anxieties, and stresses.21
A review study by Russell, showed that EMDR technique is effective in patients even after one session and can be used as a standard treatment for people with PTSD, which is consistent with the results of the current study. Based on the results of their study, EMDR technique can be used to process aggressive experiences, and by releasing cognitive capacity, the individual can learn from past experiences, and accordingly, easily confront present and future stresses.22
It seems that imagination and imagining a stressful situation in this therapeutic method results in desensitization of anxious situations and accordingly, the level of stress is significantly reduced. This new psychotherapy approach, which is consistent with contemporary theories and relies on the direct process of stored memory, based on neurophysiology is of events that have psychopathological basics.23
Since, in this approach, the therapist discusses all clinical images including past experiences and disturbing thoughts related to common problems in order to release such distressing mental experiences and information, the relief is achieved when such information is appeared and released.12 Shapiro believes that EMDR technique reduces rapid eye movement (REM). In the same field, regarding the EMDR mechanism of action in stress relief, Stickgold has suggested that dual attention in EMDR leads to a bioneurological state similar to REM sleep, which optimizes and supports the cortical integration of previously unpleasant memories to general semantic networks. This integration can then reduce the modulatory actions in the hippocampus, fragmented memories of the trauma, as well as amygdala-related and negative memories.24
This method has faster and higher efficacy than other therapeutic methods such as CBT.25 The pace of this therapeutic approach is related to its safe, emotional, and therapeutic environment that by applying cognitive, visual, and emotional dimensions in short intervals (same as 20 types of eye movement) make it possible to deal with the most intense content.9 According to the results of the study by Rothbam, EMDR technique was more effective than other therapeutic methods.26 Shapiro, in a review study on articles in this field, stated that EMDR allows medical personnel to quickly identify their uncomfortable experiences and effectively control them via memory processing; it can help to solve physical and psychological problems.27 Although the results of most studies indicate higher speed and efficiency of the EMDR method compared with CBT,27–29 Taylor et al considered the efficiency and speed of EMDR similar to other stress management methods.30
Overall, the current study showed that EMDR can significantly reduce the stress level of medical emergency technicians. This is a promising result in the employment of this approach to reduce stress and anxiety in the individuals that should always expect and be ready to confront stressful scenes and provide care for dying patients. In this regard, Braun et al (2010), concluded in their study that providing training on stress management and appropriate coping styles can lead to better provision of medical services and care in health centers.31
It is suggested that a study is conducted to compare EMDR therapy with cognitive therapies in the same people and evaluate the effectiveness of this therapeutic approach with a long-term follow-up.
One of the limitations was the absence of a placebo group – although our study was controlled. Another limitation was small sample size.
Conclusion
The results of the current study demonstrated the efficacy of EMDR technique on reducing and improving stress intensity in medical emergency technicians. The EMDR technique can be used as a non-pharmacological and complementary measure in the process of improving and reducing the intensity of stress experienced by medical emergency technicians in order to improve the quality of the performance and health of medical personnel.
Data sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymized data may be granted following review.
Acknowledgments
The current paper was based on a Master’s degree thesis in adult health nursing in Yasuj University of Medical Sciences. The authors wish to thank all the operational staff of Yasuj Emergency Medical Services Center and Research Deputy of Yasuj University of Medical Sciences for their assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haugen PT, Evces M, Weiss DS. Treating posttraumatic stress disorder in first responders: a systematic review. Clin Psychol Rev. 2012;32(5):370–380.
2. Shiekhy S, Issazadegan A, Basharpour S, Maroei Millan F. The relationship between death obsession and death anxiety, with hope among the Nursing Students of Urmia Medical Sciences University. J Urmia Nurs Midwifery Fac. 2013;11(6):7–8.
3. Sadeghi H, Hoseinzade M, Mehrabi F, Bahrami M, Frouzan R. [Death anxiety in students of medical emergency and emergency technicians of Sabzevar in 2013]. J Sabzevar Univ. 1396;24(6):71–79.
4. Chou LP, Li CY, Hu SC. Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open. 2014;4(2):2013–004185. doi:10.1136/bmjopen-2013-004185
5. Vettor Susan M, Kosinski Frederick A. Work-stress burnout in emergency medical technicians and the use of early recollections. J Employ Couns. 2000;37(4):216–228. doi:10.1002/j.2161-1920.2000.tb01028.x
6. West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. Jama. 2006;296(9):1071–1078. doi:10.1001/jama.296.9.1071
7. Williams ES, Manwell LB, Konrad TR, Linzer M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: results from the MEMO study. Health Care Manage Rev. 2007;32(3):203–212. doi:10.1097/01.HMR.0000281626.28363.59
8. Coleman T. The effect of an instructional module on death and dying on the death anxiety of emergency medical technician trainees. OMEGA-J Death Dying. 1993;27(2):123–129. doi:10.2190/83KH-01LU-C7J2-9BXH
9. Narimani M, Rajabi S. Comparison of the effect of sensitization with eye movement and reprocessing in the treatment of stress disorder (CBT) with cognitive-behavioral therapy (EMDR). J Islamic Azad Univ. 2009;19(4):236–245.
10. Rostaminejad A, Behnammoghadam M, Rostaminejad M, Behnammoghadam Z, Bashti S. Efficacy of eye movement desensitization and reprocessing on the phantom limb pain of patients with amputations within a 24-month follow-up. Int J Rehabil Res. 2017;40(3):209–214. doi:10.1097/MRR.0000000000000227
11. Abbasnejad M, Mahani KN, Zamiad A. [Efficiency of eye movement desensitization reprocessing in reducing unpleasant feelings resulting from earthquake experience]. Psychol Res J. 2006;3(4):105–114.
12. Saboori Moghaddam H, Bakhshi Poorroodsari A, Ghahreman Muharampour N. Effectiveness of eye disease treatment and reprocessing therapy in the treatment of post-traumatic stress disorder due to sexual assault. New Psychol Res. 2014;9(34):57–81.
13. Maredpour A, Naderi F, Mehrabizadeh-Honarmand M. Comparing the efficacy of eye movement desensitization and reprocessing therapy with prolonged exposure therapy on the trauma impact symptoms in veterans suffering from chronic PTSD. yums-armaghan. 2013;18(5):356–367.
14. Behnammoghadam M, Rahimi Mahmoud Abad S, Behnammoghadam A. Successful treatment of a veteran suffering from post-traumatic stress disorder due to war using eye movement desensitization and reprocessing a case report. JMERC. 2014;6(3):125–130.
15. Buydens SL, Wilensky M, Hensley BJ. Effects of the EMDR protocol for recent traumatic events on acute stress disorder: a case series. J EMDR Pract Res. 2014;8(1):2–12. doi:10.1891/1933-3196.8.1.2
16. Haugen PT, Evces M, Weiss DS. Treating posttraumatic stress disorder in first responders: a systematic review. Clin Psychol Rev. 2012;32(5):370–380. doi:10.1016/j.cpr.2012.04.001
17. Masoudzadeh A, Setareh J, Mohammadpour RA, Modanloo Kordi M. A survey of death anxiety among personnel of a hospital in Sari. J-Mazand-Univ-Med-Sci. 2008;18(67):84–90.
18. Irene E. A Major Dilemma in psychotherapy outcome research: disentangling therapists from therapies. Clin Psychol Sci Pract. 1999;6(1):10–32.
19. Okubadejo A. The Photovoice Process in Stress-Induced Depression: How Giving a Voice to the Unheard Through Pictures May Reduce Stress;2013.
20. Kinowski K. Put Your Best Foot Forward: An EDMR-related Protocol for Empowerment Using Somatosensory and Visual Priming of Resource Experiences; 2003.
21. Zeighami R, Behnammoghadam M, Moradi M, Bashti S. Comparison of the effect of eye movement desensitization reprocessing and cognitive behavioral therapy on anxiety in patients with myocardial infarction. Eur J Psychiatry. 2018;32(2):72–76.doi:10.1016/j.ejpsy.2017.09.001
22. Russell MC. Treating combat-related stress disorders: A multiple case study utilizing eye movement desensitization and reprocessing (EMDR) with battlefield casualties from the Iraqi war. Mil Psychol. 2006;18(1):1–18. doi:10.1207/s15327876mp1801_1
23. Mohammad TH, Fazeli M, Mohammad TM. Effectiveness of reducing eye movement eye removal (EMDR) on anxiety reduction. Thought Behav. 2011;6(21):61–68.
24. Stickgold R. EMDR: A putative neurobiological mechanism of action. J Clin Psychol. 2002;58(1):61–75.
25. Marcus SV, Marquis P, Sakai C. Controlled study of treatment of PTSD using EMDR in an HMO setting. Psychotherapy Theory Res Pract Training. 1997;34(3):307. doi:10.1037/h0087791
26. Rothbaum BO. A controlled study of eye movement desensitization and reprocessing in the treatment of posttraumatic stress disordered sexual assault victims. Bull menninger clin. 1997;61:317–334.
27. Shapiro F. The role of eye movement desensitization and reprocessing (EMDR) therapy in medicine: addressing the psychological and physical symptoms stemming from adverse life experiences. Perm J. 2014;18(1):71. doi:10.7812/TPP/13-060
28. Karatzias A, Power K, McGoldrick T, et al. Predicting treatment outcome on three measures for post-traumatic stress disorder. Eur Arch Psychiatry Clin Neurosci. 2007;257(1):40–46. doi:10.1007/s00406-006-0682-2
29. Arabia E, Manca ML, Solomon RM. EMDR for survivors of life-threatening cardiac events: results of a pilot study. J EMDR Pract Res. 2011;5(1):2–13. doi:10.1891/1933-3196.5.1.2
30. Taylor S, Thordarson DS, Maxfield L, Fedoroff IC, Lovell K, Ogrodniczuk J. Comparative efficacy, speed, and adverse effects of three PTSD treatments: exposure therapy, EMDR, and relaxation training. J Consult Clin Psychol. 2003;71(2):330. doi:10.1037/0022-006X.71.2.330
31. Braun M, Gordon D, Uziely B, editors. Associations between oncology nurses’ attitudes toward death and caring for dying patients. Oncol Nurs Forum. 2010;37:E43–E49. doi:10.1188/10.ONF.E43-E49
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.