Back to Journals » Local and Regional Anesthesia » Volume 18
Effect of External Oblique Intercostal Block on Postoperative Analgesia and Early Recovery in Patients Undergoing Open Liver Resection for Hepatocellular Carcinoma or Intrahepatic Bile Duct Stones: A Randomized Controlled Clinical Trial
Authors Ying Q ![]() , Zhu M, Zhang S, Wang L, Zhou R
, Zhu M, Zhang S, Wang L, Zhou R ![]() , Xie K
, Xie K
Received 31 July 2025
Accepted for publication 30 November 2025
Published 4 December 2025 Volume 2025:18 Pages 131—142
DOI https://doi.org/10.2147/LRA.S557373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Qilu Ying,1,2 Manhua Zhu,1,2 Song Zhang,1,2 Lingzhi Wang,1,2 Ruifen Zhou,1,2 Kaiyun Xie1,2
1Department of Anesthesiology, The Affiliated LiHuiLi Hospital of Ningbo University, Ningbo, Zhejiang Province, People’s Republic of China; 2Health Science Center, Ningbo University, Ningbo, Zhejiang Province, People’s Republic of China
Correspondence: Manhua Zhu, Department of Anesthesiology, The Affiliated LiHuiLi Hospital of Ningbo University, Ningbo, Zhejiang Province, People’s Republic of China, Email [email protected]
Purpose: External oblique intercostal (EOI) block has recently emerged as a promising analgesic method for the upper abdominal surgery. This study aimed to assess the effect of EOI block on postoperative analgesia and early recovery following open liver resection (OLR).
Patients and Methods: In this prospective, randomized, controlled trial, 64 patients scheduled for OLR were randomly allocated into EOI group and control group. EOI group received 30 mL of 0.25% ropivacaine bilaterally 30 min before induction of general anesthesia, whereas control group did not receive any block. The primary outcomes were sufentanil consumption 24 h after surgery. The secondary outcomes mainly included: the visual analogue scale (VAS) pain scores at rest and on coughing at 2, 12, 24, 48 h postoperatively; number of analgesia pump compression 24 h postoperatively; quality of recovery-15 (QoR-15) scale score 48 h after surgery; Pittsburgh sleep quality index (PSQI) score the first night postoperatively; and plasma levels of norepinephrine (NE), cortisol (Cor), high mobility group box protein 1 (HMGB1), tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) 1h before surgery and 6 h postoperatively.
Results: A total of 60 patients had completed the study (n = 30 per group). Sufentanil consumption 24 h postoperatively in EOI group was less than that in control group (mean difference: 4.45 μg, 95% CI, 1.6– 7.2, P=0.003). The VAS scores at 2, 12, 24 h postoperatively; number of analgesia pump compression; and PSQI scores were significantly lower in EOI group than in control group. QoR-15 scale scores were higher in EOI group. The plasma levels of NE, Cor, HMGB1, TNF-α and IL-6 at 6 h postoperatively in EOI group were significantly lower than in control group.
Conclusion: EOI block given to patients undergoing OLR could provide effective postoperative analgesia, enhance the quality of postoperative recovery, and attenuate postoperative stress and inflammation.
Keywords: external oblique intercostal block, open liver resection, postoperative pain, early recovery
Introduction
Hepatocellular carcinoma (HCC) ranks among the leading causes of cancer-related mortality worldwide.1 Surgical resection remains the most efficacious curative approach for HCC and intrahepatic bile duct stones.2 However, open liver resection (OLR) can be associated with severe postoperative pain. The intensity of pain can be attributed to the extensive surgical trauma involved, leading to various physiological and psychological complications. Adequate pain management is crucial not only for patient comfort but also for promoting recovery and reducing the risk of chronic pain syndromes.3
Thoracic epidural analgesia (TEA) has been considered as an effective method for pain therapy following upper abdominal surgeries. However, its use has been limited in certain patients undergoing OLR due to pre- or post-operative coagulopathy and the risk of hypotension, particularly with higher thoracic epidural infusions.3 Intrathecal morphine presents another regional analgesic option. And Patient-controlled intravenous analgesia (PCIA) is used for conventional pain management in patients after OLR. But its utilization is accompanied by potential complications such as nausea, respiratory depression, and potential tolerance or dependence.4 Furthermore, altered liver function in the postoperative period may impair opioid metabolism, limiting their safe dosage and potentially leading to inadequate analgesia, delayed mobilization, and hindered recovery. Given these challenges, there remains an urgent need to explore other effective and safety analgesic strategies following OLR.
With the development in multimodal analgesia (MMA), fascial plane block (FPB) techniques have gained attraction as an adjunct for postoperative analgesia following abdominal surgeries.5 External oblique intercostal (EOI) block is a novel FPB first described by Hamilton et al6 in 2021, which achieves dermatomal sensory blockade from T6 to T11. Its sensory blockade range is consistent with the T7-T10 dermatomes required for analgesia following OLR. It was reported that the potential advantages of EOI include technically simple to perform, superficial injection site, and wide sensory range.6 Although case reports suggest EOI block’s efficacy in upper abdominal surgery,7,8 its application in OLR remains unexplored. And, there is still a lack of randomized controlled clinical trials of EOI block for analgesia after OLR. The hypothesize is that EOI block may provide superior opioid-sparing effects compared to PCIA while avoiding TEA’s coagulation risks in OLR patients. The aim of this study is to investigate the effect of EOI block on postoperative analgesia and early recovery following OLR. The primary objective is to compare the sufentanil consumption within the first 24 hours postoperatively between patients receiving EOI block in addition to PCIA and those receiving PCIA alone.
Materials and Methods
Study Design and Patients
This randomized prospective double-blind clinical trial was approved by the Affiliated LiHuiLi Hospital of Ningbo University Ethics Committee (NO. KY2023PJ077). The study was registered at chictr.org.cn (identifier: ChiCTR2300070045; date of registration: March 31, 2023). Written informed consent was obtained from all participants prior to enrollment. The study ran from April 1, 2023 to December 31, 2023.
Patients undergoing OLR under general anesthesia were recruited in the Affiliated LiHuiLi Hospital of Ningbo University.
Inclusion Criteria
- Aged between 18–80 years old.
- American Society of Anesthesiologists Classification (ASA) Grade II to III.
- Diagnosed with HCC or intrahepatic bile duct stones and scheduled for OLR.
Exclusion Criteria
- Severe cardiac dysfunction (New York Heart Association class III or IV); severe respiratory disease; preexisting cerebrovascular disease; significant hepatic impairment (Child-Pugh B or C) or renal insufficiency (eGFR < 30 mL/min/1.73 m2).
- Preoperative psychiatric disorders and cognitive impairment.
- History of drug abuse or addiction.
- Allergy to local anesthetics (LA).
- Infection at the puncture site.
- Prior surgeries at the operative site.
- Language communication disorder.
- Inability to successfully accomplish the tests.
- Patients who require mechanical ventilation after surgery.
- Refusal to participate.
Randomization and Blinding
All subjects who meet the criteria were randomly allocated to EOI group and control group in a 1:1 ratio. The randomization sequence was generated using a computer-generated random number table by an independent biostatistician who was not involved in the subsequent study. Based on this list, one nurse who was blinded to group allocation prepared sealed opaque envelopes for each patient. The sealed opaque envelopes containing the study number were opened by an experienced senior anesthesiologist who was not involved in any subsequent aspects of the study. She prepared the study drug, performed the EOI block according to the group, and was not involved in subsequent anesthesia management and data collection. Two data collectors were responsible for recording all result measurements. Patients, anesthesiologists, surgeons, nurses, data collectors and statisticians were all blinded to the study.
Ultrasound-Guided EOI Block
After entering the operating room, all patients were monitored with a 5-lead electrocardiogram (ECG), pulse oximetry (SpO2), and non-invasive arterial blood pressure (NIBP). A peripheral intravenous line was established and midazolam 1 mg IV was given before ultrasound scan. Patients in the EOI group underwent ultrasound-guided bilateral EOI block as described by Elsharkawy et al.9 Patients were placed in supine position with their ipsilateral arm abducted, a linear probe was positioned in the parasagittal plane at the level of the 6th rib between the anterior axillary and midclavicular lines. The 6th and 7th ribs, subcutaneous tissue, intercostal muscles between ribs, external oblique muscle, pleura, and lung were identified. After disinfection and puncture point injection with 2% lidocaine (1 mL), a 21G×100 mm nerve block needle was inserted into the fascial plane between the external oblique muscle and intercostal muscles using an in-plane technique with a inferolateral-to-superomedial trajectory. The needle tip position was confirmed by injecting 2 mL normal saline, then 30 mL of 0.25% ropivacaine was given slowly on each side (Figure 1). Patients in the control group only received an ultrasound scan of the EOI plane at the level of the 6th rib, as well as puncture point injection with normal saline (1 mL) but did not receive EOI block. The extent of sensory dermatomal block with a cold test was assessed on all patients 20 minutes after EOI block. A nurse anesthetist, who was not involved in the study, performed the sensory block tests.
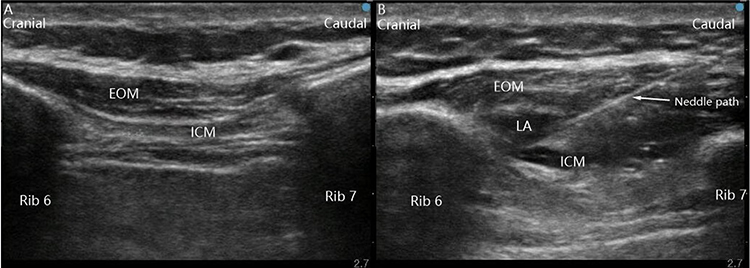 |
Figure 1 Image of ultrasound-guided EOI block. (A) pre block. (B) post block. LA disseminates between the external oblique muscle and intercostal muscles. The arrow indicates the path of the needle. Abbreviations: EOM, external oblique muscle; ICM, intercostal muscles; LA, local anesthetic. |
Anesthesia Management
Invasive radial arterial blood pressure, right internal jugular vein catheterization and bispectral index (BIS) monitor were added before induction. Both groups received standardized general anesthesia. All patients were pre-oxygenated with 100% oxygen 6 L/min for a duration of 3–5 minutes. Anesthesia was induced intravenously with propofol 2 mg/kg, sufentanil 0.3 to 0.4 μg/kg, and rocuronium 0.6 mg/kg. After tracheal intubation, mechanical ventilation with a tidal volume of 6–8 mL/kg and respiratory rate of 12–14 bpm was initiated to maintain end-tidal CO2 at 35 to 45 mmHg. The anesthesia was maintained with a continuous intravenous infusion of propofol 0.1–0.15 mg/kg/min and remifentanil 0.1–0.2 μg/kg/min to maintain the BIS between 40 to 60. Intermittent rocuronium was injected to maintain muscle relaxation. During the surgery, the infusion rate of remifentanil was titrated based on real-time hemodynamic: if blood pressure or heart rate deviated by >20% from baseline, the dose was adjusted in 0.03 μg/kg/min increments (or decrements for hypotension/bradycardia) at 5-minute intervals. After surgery, all patients were transferred to the Post-Anesthesia Care Unit (PACU), and the endotracheal tube was removed once they met extubation criteria.
Analgesia Management
Sufentanil (0.15 μg/kg) was administered intravenously 10 min before the end of the surgical. Patient-controlled intravenous analgesia (PCIA) pump contained 1 μg/mL sufentanil and 0.1 mg/mL tropisetron (total volume: 100 mL), set to deliver a 2 mL/h background infusion, 0.5 mL bolus doses, and a 15-minute lockout time. In the surgical ward, patients received 40mg of parecoxib sodium intravenously every 12 h after surgery. If the static visual analogue scale (VAS) score was ≥4, an intravenous injection of tramadol 100 mg was given.
Outcomes
The primary outcomes were sufentanil consumption 24 h after surgery.
The secondary outcomes included: (1) the VAS pain scores at rest and on coughing at 2, 12, 24, 48 h postoperatively; (2) number of analgesia pump compression 24 h postoperatively; (3) sensory block plane; (4) intraoperative reminfentanil consumption; (5) the frequency of requiring rescue analgesia 24 h after surgery; (6) quality of recovery-15 (QoR-15) scale score 48 h after surgery; (7) Pittsburgh sleep quality index (PSQI) score the first night postoperatively; (8) plasma levels of norepinephrine (NE), cortisol (Cor), high mobility group box protein 1 (HMGB1), tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) 1h before surgery (baseline) and 6 h postoperative; (9) and adverse events 24 h after surgery, including postoperative nausea and vomiting (PONV), pruritus, pneumothorax, respiratory depression and LA systemic toxicity (LAST).
The VAS was used to assess the patient’s pain severity. The VAS is a validated, unidimensional measure of pain intensity. It consists of a 10-cm horizontal line, anchored by two verbal descriptors: “no pain” (score of 0) and “worst pain imaginable” (score of 10). The scores were interpreted as follows: 0, no pain; 1–3, mild pain; 4–6, moderate pain; 7–10, severe pain.
The QoR-15 scale includes 15 items to evaluate five dimensions: physical comfort (5 items), emotional state (4 items), physical independence (2 items), psychological support (2 items) and pain (2 items). Each item is scored from 0 to 10, with the total score ranging from 0 (poorest recovery quality) to 150 (poorest recovery quality).10
The PSQI11 consists of 18 self-reported items comprising 7 components: sleep quality, sleep latency, hours of sleep, sleep efficiency, sleep disturbances, use of hypnotic agents, and daytime dysfunction. Each component ranges from 0 to 3, the total score ranges from 0 to 21, with lower scores indicating better sleep quality.
Assay of Plasma Samples
Venous blood samples (5 mL) were collected from all subjects 1 h before surgery and 6 h after surgery. Blood samples were centrifuged at 1000 × g for 20 min at 4 °C, and the plasma was collected and stored at −80 °C for subsequent analysis. The concentrations of NE, Cor, HMGB1, TNF-α, and IL-6 were tested using the enzyme-linked immunosorbent assay (ELISA) method.
Statistical Analysis
The sample size was calculated using IBM SPSS Sample Power version 3.0 (IBM Corp., Armonk, New York, USA). A pilot study of 10 patients in each group showed that a mean sufentanil consumption 24 h after surgery of 49.5 μg with standard deviation (SD) of 4.55 in the EOI group and 53.2 μg with SD of 4.77 in the control group. 26 patients per group was required to achieve a statistical power of 0.8 with a significance level (α) of 0.05. Assuming a possible dropout rate of 20%, a total of 32 subjects per group were planned for recruitment.
The statistical analysis was conducted using version 25.0 of the Statistical Package for Social Science (SPSS). The normality of the data distribution was evaluated with the Shapiro–Wilk test. Continuous data were presented as mean± SD or median (M) and interquartile (IQR) and compared using the t-test or Mann–Whitney U-test, as appropriate. Comparison between groups at different time points were performed using repeated-measures ANOVA. Categorical data were presented as n (%) and compared using the χ2 test or Fisher’s exact test. A P-value below 0.05 was considered statistically significant.
Results
In this prospective randomized study, 70 patients were assessed for eligibility between April 1, 2023 and December 31, 2023. Four patients did not meet the inclusion criteria, and two patients declined to participate. A total of 64 patients were randomly assigned to two groups. One patient was converted to laparoscopic surgery in the EOI group. One patient’s surgery was cancelled after randomization in the control group. And two patients (one in each group) were lost to follow up. Therefore, 60 patients were included in the analysis (n = 30 per group). The CONSORT flow diagram for this study is depicted in Figure 2. Baseline demographic and clinical characteristics are presented descriptively in Table 1.
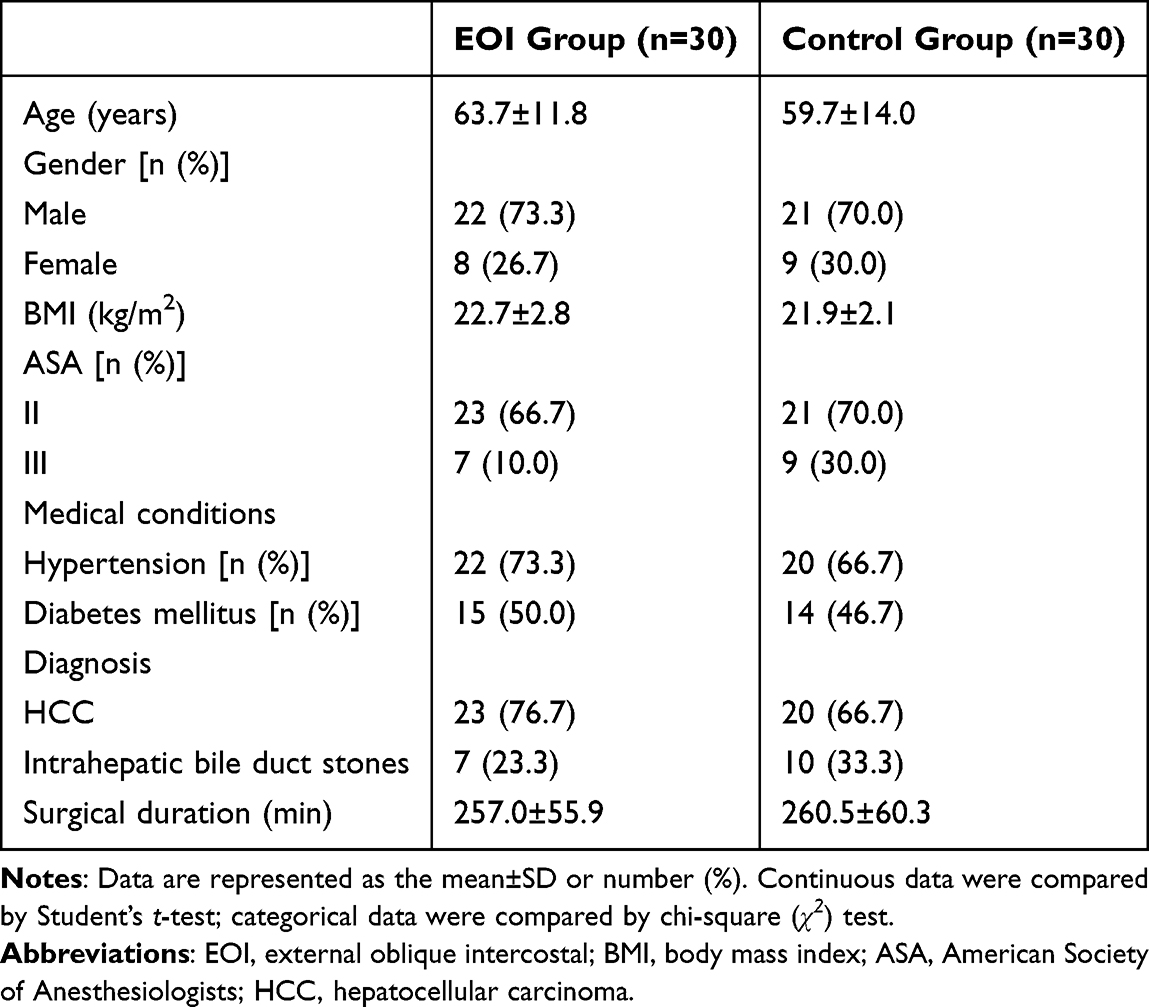 |
Table 1 Clinical Baseline Characteristics of the Patients |
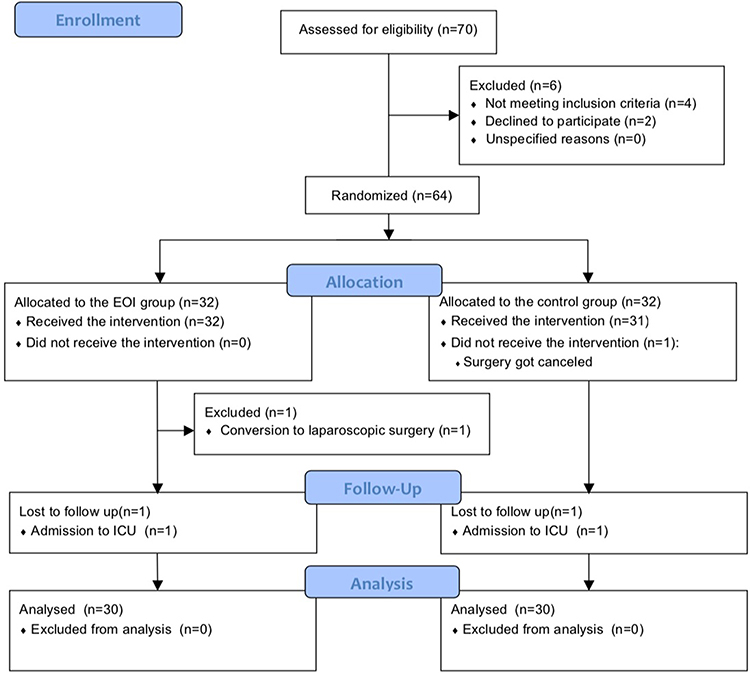 |
Figure 2 CONSORT diagram. Abbreviations: CONSORT, consolidated standards of reporting trials; EOI, external oblique intercostal block. |
Primary Outcome
Patients in the EOI group had lower sufentanil consumption 24 h after surgery than the control group (52.7±4.7 μg vs 57.1±6.2 μg, P=0.003), with a mean difference of 4.45 (95% CI, 1.6–7.2) (Figure 3).
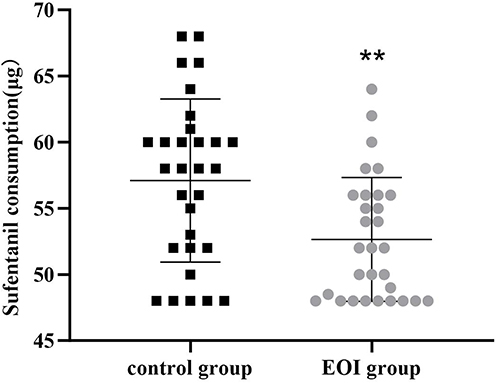 |
Figure 3 Sufentanil consumption 24 h after surgery. Compared with the control group, **P<0.01. Data were compared by Student’s t-test. Abbreviations: EOI, external oblique intercostal. |
Secondary Outcomes
As shown in Table 2, the VAS scores at rest and when coughing at 2, 12, and 24 h postoperatively were statistically significantly lower in the EOI group than in the control group (Mann–Whitney U-test, all P<0.05, Table 2). However, the VAS scores at rest and when coughing did not differ 48 h between the two groups after surgery (Mann–Whitney U-test, all P>0.05, Table 2). The number of analgesia pump compression 24 h postoperatively were significantly lower in the EOI group than that in the control group (Student’s t-test, t=3.857, P=0.000, Table 3).
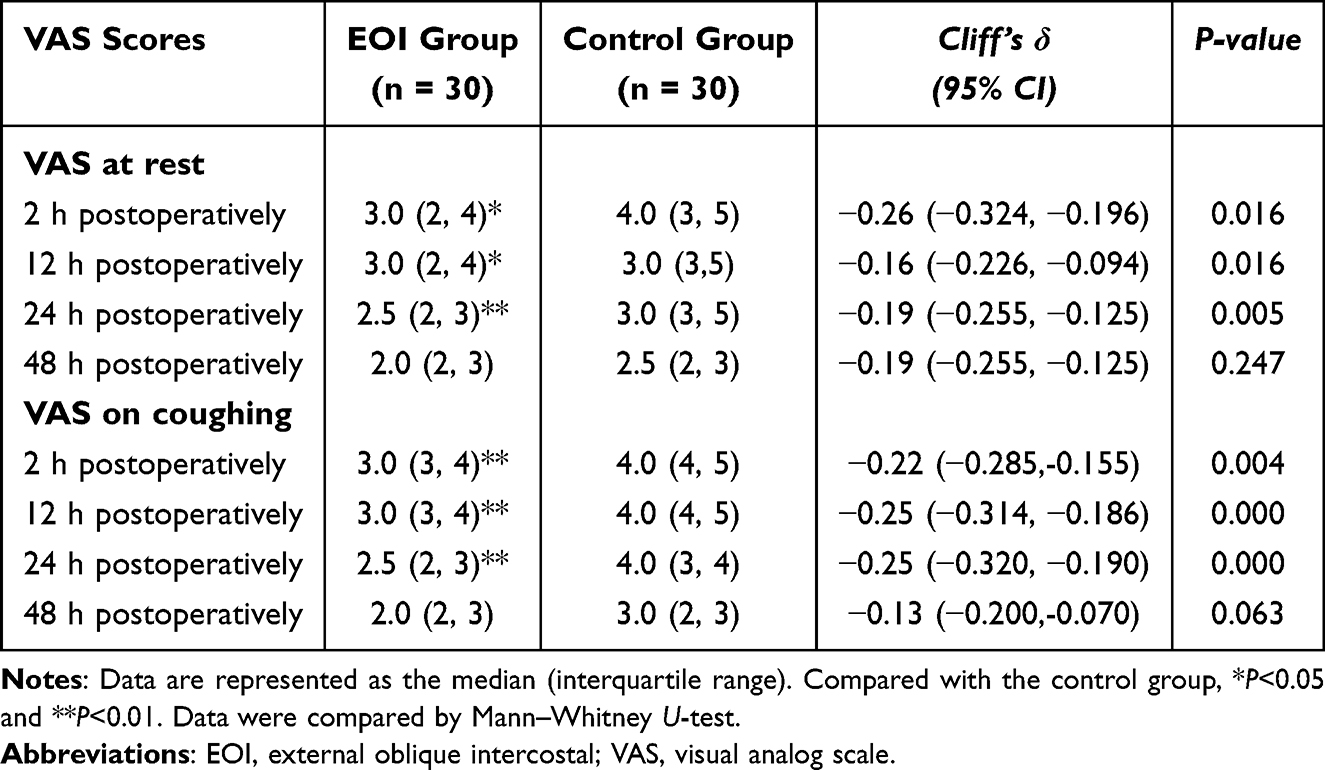 |
Table 2 VAS Scores at Rest and on Coughing |
 |
Table 3 Intraoperative Reminfentanil Consumption and Postoperative Conditions |
We observed the range of sensory blocks in patients who received EOI block, the affected dermatomes were located between T6 and T11, and mainly between T6 and T10 (Figure 4).
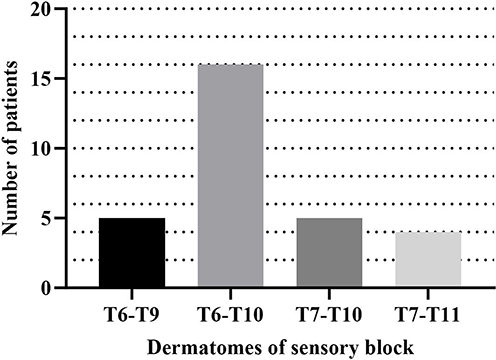 |
Figure 4 Dermatomes of the sensory block in patients who received EOI block. |
Intraoperative reminfentanil consumption and the frequency of rescue analgesia 24 h after surgery were significantly lower in the EOI group than those in the control group (Student’s t-test, t=3.679, P=0.000; and Chi-square test, χ2=4.022, P=0.045). The scores of QoR-15 scale were higher in the EOI group 48 h after surgery than those in the control group (Student’s t-test, t=5.826, P=0.000). Compared to the control group, PSQI scores in the EOI group were significantly lower on the first night after surgery (Mann–Whitney U-test, P=0.000, Table 3).
The plasma levels of NE, Cor, HMGB1, TNF-α and IL-6 were significantly higher at 6 h postoperatively than at baseline in both groups (paired Student’s t-test, all P<0.05). Compared with the control group, the levels of NE, Cor, HMGB1, TNF-α and IL-6 were significantly lower in the EOI group at 6 h postoperatively (paired Student’s t-test, all P<0.05, Figures 5 and 6).
 |
Figure 5 The plasma levels of NE and Cor at different time points between the two groups. (A) NE levels. (B) Cor levels. Error bars represent the mean + SD. Compared with the control group, *P<0.05; compared with baseline, #P<0.05. Data were compared by paired Student’s t-test. Abbreviations: NE, norepinephrine; Cor, cortisol. |
 |
Figure 6 The plasma levels of HMGB1, TNF-α and IL-6 at different time points between the two groups. (A) HMGB1 levels. (B) TNF-α levels. (C) IL-6 levels. Error bars represent the mean + SD. Compared with the control group, *P<0.05; compared with baseline, #P<0.05. Data were compared by paired Student’s t-test. Abbreviations: HMGB1, high mobility group box; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6. |
No severe complications, such as pneumothorax, respiratory depression, and LAST occurred in either group. The incidence of PONV was significantly reduced in the EOI group compared to the control group (Chi-square test, χ2=6.239, P=0.012). The incidence of pruritus was comparable between the two groups (Fisher’s exact test, P=1.000, Table 4).
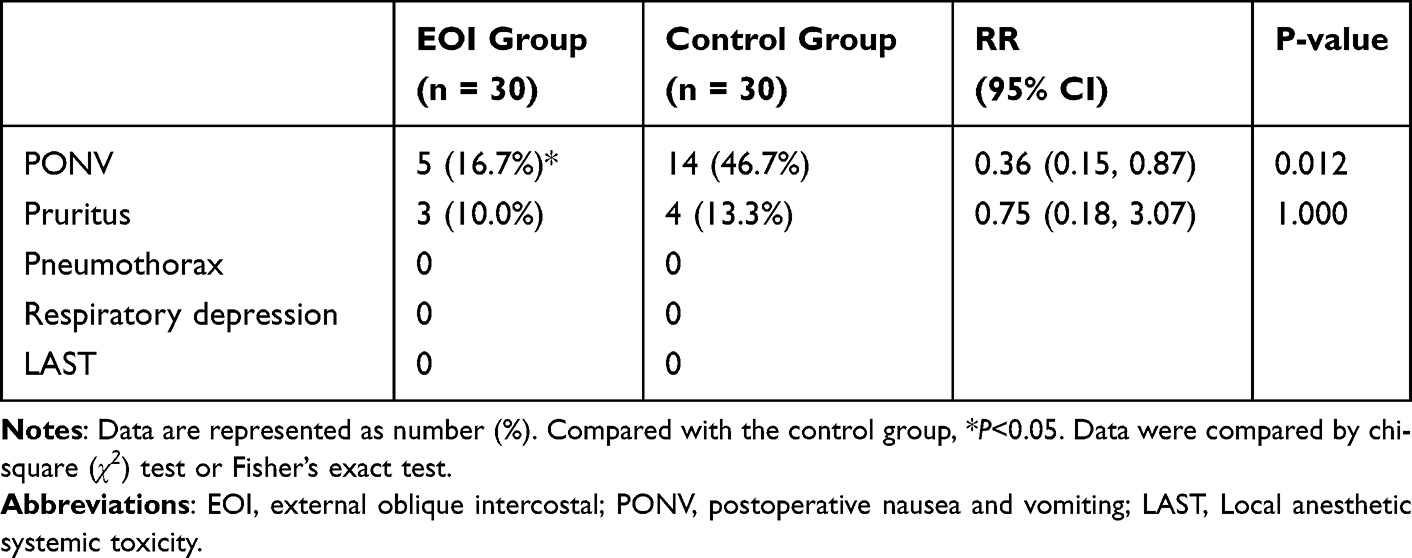 |
Table 4 Incidence of Adverse Events |
Discussion
The results of the present study suggested that EOI block can provide effective postoperative analgesia for patients undergoing OLR, attenuated postoperative stress and inflammatory responses and enhanced the quality of early postoperative recovery.
OLR often employs a right subcostal reverse L-shaped incision,12 extending from the xiphoid process along the right costal margin to the 12th rib tip, with an incision length ranging between 20–25 cm. The subcostal incision is mainly innervated by the intercostal nerves T6-T10. Transection of the skin and muscle, rib retraction, and injury of the anterior and lateral branches of intercostal nerves is associated with significant trauma, resulting in severe postoperative pain, stress responses, and an increased risk of complications, ultimately leading to delayed recovery.13
Achieving satisfactory analgesia after OLR surgery has always been a challenging goal. The Procedure-Specific Postoperative Pain Management (PROSPECT) guidelines support TEA as an effective option for OLR, particularly in appropriate patients. However, its use may be limited due to coagulopathy, hemodynamic instability, and the need for early postoperative mobilization.3 Compared to the ESPB and QLB, it is easier to perform with the patient in the supine position, and has advantages for obese patients with fewer complications.14 The utility of the EOI block is increasingly being recognized in other upper abdominal procedures, such as bariatric surgery15 and oncologic resections,16 highlighting its broad applicability.
The results demonstrated a statistically significant but modest reduction in sufentanil consumption in the EOI group, corresponding to a 7.7% decrease compared to the control group in the first 24 h postoperatively. While this reduction in opioid use alone may not reach the threshold for clinical significance, the EOI block demonstrated important combined benefits across multiple recovery parameters. Compared to the control group, the VAS scores at rest and on coughing; number of analgesia pump compression 24 h postoperatively; intraoperative reminfentanil consumption; as well as the need of rescue analgesia within 24 h postoperatively in the EOI group were significantly reduced. The results were consistent with the case report by Liotiri et al,8 who applied the EOI block in three adult patients undergoing liver surgery, and found that it was an effective and opioid-sparing FPB for postoperative analgesia after liver surgery. However, there was no significant difference in VAS scores at 48 h postoperatively between the two groups, which may be attributed to the fact that a single EOI block was used in this study. Although ropivacaine is a long-acting local anesthetic, a single-shot nerve block provide can only provide pain relief for about 10–20 h.17 In this study, the sensory blockade in the EOI group was observed to range from T6-T10 between the bilateral mid-axillary lines. This finding is consistent with reports from cadaveric study and clinical case series,9 implying that EOI block can target the nerve innervation of OLR incision and provide effective early postoperative analgesia.
In this study, the Chinese version of the QoR-15 questionnaire was used to evaluate the recovery quality of patients 48 h after surgery. The QoR-15 scores at 48 h postoperatively in the EOI group were significantly higher than those in the control group. An increasing number of studies have found that FPBs, such as ESPB for laparoscopic cholecystectomy and serratus intercostal interfascial plane block for open upper abdominal wall surgery, can improve patients’ QoR-15 scores postoperatively.18,19 The results were consistent with the above studies, indicating that the EOI block can improve the quality of early recovery for patients undergoing OLR. In the study, the sleep quality was evaluated by the PSQI score. The results showed that patients receiving EOI block had significantly lower PSQI scores on the first night after surgery, which could be attributed to both the reduced postoperative pain and improved emotional state in the EOI group.
The application of nerve blocks in surgical patients and their impact on postoperative inflammation and stress response have been investigated in previous studies. Liu et al20 found that TAPB reduced perioperative levels of NE and Cor in patients undergoing radical gastrectomy. Cai et al21 performed serratus anterior plane block on patients undergoing upper abdominal surgery and found a decrease in the IL-6 and TNF-α levels 24 h postoperatively. In this study, the plasma levels of NE, Cor, HMGB1, TNF-α, and IL-6 at 6 h after surgery were higher than those before surgery, suggesting that stress and inflammation were caused by surgical trauma. And the levels of all the above stress and inflammation indexes in the EOI group were significantly lower than those in the control group 6 h postoperatively, indicating that EOI block can effectively reduce stress and inflammation, which may be related to EOI block in alleviating surgical trauma and relieving postoperative pain.
Taken together, these findings suggest that while the opioid-sparing effect of EOI block may be modest, its combined benefits in pain control, recovery quality, sleep outcomes, and modulation of stress/inflammatory responses represent a meaningful advancement in postoperative recovery for OLR patients.
No severe adverse reactions, such as pneumothorax or respiratory depression, were observed in this study, indicating a high safety of EOI block, possibly due to the relatively superficial injection site and injection being far away from blood vessels and nerves. Furthermore, the incidence of PONV was significantly reduced in the EOI group, which may be related to the lower consumption of sufentanil after surgery. The results are consistent with the findings of Hung et al,22 who reported that ESPB significantly decreased the incidence of PONV compared with control treatments in patients undergoing liver surgery.
This study also has several limitations. Firstly, this study was conducted at a single center with a relatively small sample size, which was calculated with a power of 80% to detect the primary outcome, potentially limiting the ability to detect smaller but still clinically meaningful differences in secondary outcomes. And all participants were Chinese patients undergoing OLR. While our findings provide insights into this specific population, their generalizability to other demographics or surgical settings remains uncertain. Multicenter studies involving diverse demographics are needed to validate the results. Secondly, single injections of EOI block was employed in this study, resulting in limited analgesia duration. Further research is required to confirm the analgesic effect of continuous EOI block. Thirdly, due to serum samples only being collected up to 6 h postoperatively, it is not possible to reflect the long-term changes in certain inflammatory stress indicators. Fourth, plasma levels of ropivacaine were not monitored. Considering the potential alterations in drug metabolism among patients undergoing liver surgery, there may be a risk of systemic toxicity. However, according to the literature,23 this study used 0.25% ropivacaine, which is the minimum effective concentration for FPB, and no cases of LAST were observed among the patients. Lastly, the single-center design and limited sample size precluded subgroup or sensitivity analyses. Future multi-center studies with larger cohorts are needed to explore these important questions.
Based on the findings and limitations of this study, investigating the efficacy and safety of continuous EOI block via catheter insertion is a crucial next step to extend the analgesic benefits beyond 24 hours. The effect of EOI block can be verified in more diverse populations and its potential benefits on other clinical outcomes, such as chronic postoperative pain incidence, can be explored.
Conclusion
The ultrasound-guided EOI block given to patients undergoing open liver resection reduced the postoperative consumption of sufentanil and showed trends toward improved analgesia, postoperative recovery and sleep quality, and attenuate postoperative stress and inflammation. However, these findings require verification in larger, multicenter studies with pre-specified hierarchical endpoints.
Abbreviations
ASA, America Society of Anesthesiologist; BIS, bispectral index; BMI, body mass index; Cor, cortisol; ECG, electrocardiogram; ELISA, enzyme-linked immunosorbent assay; EOI, External oblique intercostal; ESPB, erector spinae plane block; FPB, fascial plane block; HCC, Hepatocellular carcinoma; HMGB1, high mobility group box protein 1; IL-6, interleukin-6; IQR, interquartile; LA, local anesthetics; LAST, LA systemic toxicity; MMA, multimodal analgesia; NE, norepinephrine; NIBP, non-invasive arterial blood pressure; OLR, open liver resection; PACU, Post-Anesthesia Care Unit; PCIA, Patient-controlled intravenous analgesia; PONV, postoperative nausea and vomiting; PSQI score, Pittsburgh sleep quality index score; QLB, quadratus lumborum block; OLR, open liver resection; QoR-15 scale score, quality of recovery-15 scale score; SD, standard deviation; SPO2, pulse oximetry; TAPB, transversus abdominis plane block; TEA, Thoracic epidural analgesia; TNF-α, tumor necrosis factor-α; VAS pain scores, the visual analogue scale pain scores.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee of the Affiliated LiHuiLi Hospital of Ningbo University, China (NO. KY2023PJ077). The protocol was registered at the Chinese Clinical Trial Registry (https://www.chictr.org.cn) (prospectively registered). The initial registration date was 31/03/2023. All procedures performed in this study involving human participants were following the Ethical Standards of the Institutional Ethics Committee, as well as the 1964 Helsinki Declaration and subsequent amendments or comparable ethical standards. All patients signed written informed consent forms before surgery.
Acknowledgments
The study was supported by the Department of Anesthesiology, Department of Hepatology and pancreatology, The Affiliated LiHuiLi Hospital of Ningbo University, Ningbo, China. The authors would like to appreciate the efforts of all medical staff and the patients for their participation in this study. QoR-15 scale and PSQI were used in this study with permission from the respective developers. Heartfelt thanks are extended to them for their authorization.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Ningbo Health Youth Technical Backbone Talents Project (2023QNJSGG-ZMH).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shan S, Jia JD. The clinical management of hepatocellular carcinoma in China: progress and challenges. Clin Mol Hepatol. 2023;29(2):339–341. doi:10.3350/cmh.2023.0077
2. Zhou HY, Song TQ. Conversion therapy and maintenance therapy for primary hepatocellular carcinoma. Biosci Trends. 2021;6(15):155–160. doi:10.5582/bst.2021.01091
3. Dieu A, Huynen P, Lavand’Homme P, et al. Pain management after open liver resection: Procedure-Specific Postoperative Pain Management (PROSPECT) recommendations. Reg Anesth Pain Med. 2021;46(5):433–445. doi:10.1136/rapm-2020-101933
4. Zhang XP, Wei WT, Huang Y, et al. Efficacy and safety of patient-controlled epidural analgesia versus patient-controlled intravenous analgesia following open hepatectomy: a single-center retrospective study. Heliyon. 2023;10(1):e23548. doi:10.1016/j.heliyon.2023.e23548
5. Albrecht E, Chin KJ. Advances in regional anaesthesia and acute pain management: a narrative review. Anaesthesia. 2020;75(S1):e101–110. doi:10.1111/anae.14868
6. Hamilton DL, Manickam BP, Wlson MAJ, et al. External oblique facial plane block. Reg Anesth Pain Med. 2019;44(4):528–529. doi:10.1136/rapm-2018-100256
7. Cosarcan SK, Ercelen O. The analgesic contribution of external oblique intercostal block: case reports of 3 different surgeries and 3 spectacular effects. Medicine. 2022;101(36):e30435. doi:10.1097/MD.0000000000030435
8. Liotiri D, Diamantis A, Papapetrou E, et al. External oblique intercostal (EOI) block for enhanced recovery after liver surgery: a case series. Anaesth Rep. 2023;11(1):e12225. doi:10.1002/anr3.12225
9. Elsharkawy H, Kolli S, Soliman LM, et al. The external oblique intercostal block: anatomic evaluation and case series. Pain Med. 2021;22(11):2436–2442. doi:10.1093/pm/pnab296
10. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
11. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
12. Chang SB, Palavecino M, Wray CJ, et al. Modified Makuuchi incision for foregut procedures. Arch Surg. 2010;145(3):281–284. doi:10.1001/archsurg.2010.7
13. Dudek P, Zawadka M, Andruszkiewicz P, et al. Postoperative analgesia after open liver surgery: systematic review of clinical evidence. J Clin Med. 2021;10(16):3662. doi:10.3390/jcm10163662
14. Turunc E, Dost B, Ozel ES, et al. Bilateral ultrasound-guided external oblique intercostal block vs modified thoracoabdominal nerve block through perichondrial approach for postoperative analgesia in patients undergoing laparoscopic sleeve gastrectomy surgery: a randomized controlled study. Obes Surg. 2024;34(10):3726–3734. doi:10.1007/s11695-024-07454-4
15. Ozel ES, Kaya C, Turunc E, et al. Analgesic efficacy of the external oblique intercostal fascial plane block on postoperative acute pain in laparoscopic sleeve gastrectomy: a randomized controlled trial. Korean J Anesthesiol. 2025;78(2):159–170. doi:10.4097/kja.24569
16. Srinivasaraghavan N, Seshadri RA, Ramasamy Y, et al. Bilateral external oblique intercostal plane block versus intravenous morphine for rescue pain relief in patients with epidurals following upper abdominal surgeries: a randomized controlled trial. A a Pract. 2025;19(7):e02019. doi:10.1213/XAA.0000000000002019
17. Xiao J, Cai MH, Wang XR, et al. Time course of action and pharmacokinetics of ropivacaine in adult and elderly patients following combined lumbar plexus-sciatic nerve block. Int J Clin Pharmacol Ther. 2010;48(9):608–613. doi:10.5414/CPP48608
18. Lin Z, Chen C, Xie S, et al. Systemic lidocaine versus erector spinae plane block for improving quality of recovery after laparoscopic cholecystectomy: a randomized controlled trial. J Clin Anesth. 2024;97:111528. doi:10.1016/j.jclinane.2024.111528
19. Fernández MT, López S, Aguirre JA, et al. Serratus intercostal interfascial plane block in supraumbilical surgery: a prospective randomized comparison. Minerva Anestesiol. 2021;87(2):165–173. doi:10.23736/S0375-9393.20.14882-X
20. Liu RZ, Qin HY, Wang M, et al. Transversus abdominis plane block with general anesthesia blunts the perioperative stress response in patients undergoing radical gastrectomy. BMC Anesthesiol. 2019;19:205. doi:10.1186/s12871-019-0861-0
21. Cai Z, Xie R, Xu T, et al. Comparison of ultrasound-guided serratus anterior plane block and thoracic paravertebral block in postoperative analgesia and inflammation control in patients undergoing upper abdominal surgery. Pak J Med Sci. 2023;39(1):23–27. doi:10.12669/pjms.39.1.6849
22. Hung KC, Chang LC, Chen IW. Erector spinae plane block reduces postoperative nausea and vomiting in liver surgery. Int J Surg. 2024;110(9):5987–5988. doi:10.1097/JS9.0000000000001707
23. Wang QR, Ma T, Hu J, et al. Minimum effective volume of ropivacaine for ultrasound-guided adductor canal plus IPACK block in total knee arthroplasty: A double-blind, randomized dose-finding trial. J Orthop Surg. 2022;30(2):10225536221122339. doi:10.1177/10225536221122339
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.