Back to Journals » Clinical Interventions in Aging » Volume 20
Effect of Different Neuromuscular Electrical Stimulation Modalities on Clinical and Functional Outcomes in Older Adults with Knee Osteoarthritis: A Randomized Controlled Trial
Authors De Almeida CC, Azevedo KP, De Souza Júnior JR, Moreira LA ![]() , Garcia PA, Almeida IS
, Garcia PA, Almeida IS ![]() , Dantas LO, Marqueti RDC
, Dantas LO, Marqueti RDC ![]() , DeSantana JM
, DeSantana JM ![]() , Durigan JLQ
, Durigan JLQ
Received 5 April 2025
Accepted for publication 23 July 2025
Published 4 November 2025 Volume 2025:20 Pages 1861—1874
DOI https://doi.org/10.2147/CIA.S532469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Camila Cadena De Almeida,1 Klaus Porto Azevedo,1 José Roberto De Souza Júnior,1,2 Leandro Andrade Moreira,1,2 Patrícia Azevedo Garcia,1 Isabella Silva Almeida,1 Lucas Ogura Dantas,3 Rita de Cassia Marqueti,1 Josimari Melo DeSantana,4 João Luiz Quagliotti Durigan1
1Universidade de Brasília, Laboratory of Muscle and Tendon Plasticity, Brasília, DF, Brazil; 2Centro Universitário Do Distrito Federal, Physical Therapy Department, Brasília, DF, Brazil; 3Universidade Federal de São Carlos, São Carlos, SP, Brazil; 4Universidade Federal de Sergipe, Physical Therapy Department, Aracaju, Sergipe, Brazil
Correspondence: João Luiz Quagliotti Durigan, Graduate Program of Rehabilitation Sciences, University of Brasília, Ceilândia, DF, CEP 72220-140, Brasil, Email [email protected]
Introduction: Osteoarthritis (OA) is a chronic degenerative disease characterized by progressive cartilage degeneration, most commonly affecting the knee. Clinical symptoms such as pain, stiffness, and functional limitations significantly impact quality of life. Although neuromuscular electrical stimulation (NMES) is considered a complementary treatment, evidence comparing different waveforms in clinical management remains limited.
Objective: To compare the effects of three different NMES waveforms versus a placebo, applied for four weeks, on pain intensity, disability, and other functional outcomes in individuals with knee osteoarthritis (KOA).
Methods: A randomized clinical trial with 100 participants equally assigned to four groups: transcutaneous electric nerve stimulation (TENS) (n=25), interferential current (IFC) (n=25), Aussie current (n=25), and placebo (n=25). Primary outcomes were pain intensity, disability, and pressure pain threshold and secondary outcomes included aerobic capacity, gait speed, lower limb strength, functional mobility, superficial knee temperature, stability, and fall risk. Primary and secondary outcomes were assessed before and after four weeks.
Results: A significant group x time interaction, with a moderate effect size, was found for the WOMAC index (P = 0.022; η2 = 0.10). Participants of the IFC, Aussie, and Placebo groups presented less disability after the treatment. No significant group × time interactions were observed for the other outcomes (all P > 0.05); however, a main effect of time was identified, with positive changes at week 4 in most variables, except for superficial knee temperature, stability, and risk of falls.
Conclusion: Different NMES protocols did not provide additional benefits over placebo for pain intensity, disability or functional outcomes in people with KOA. These findings highlight the need for further research to refine stimulation protocols and identify patient subgroups that may benefit most from NMES in the management of knee osteoarthritis.
Keywords: knee osteoarthritis, neuromuscular electrical stimulation, older adults
Introduction
Osteoarthritis (OA) is a chronic and degenerative disease characterized by the progressive degradation of cartilage and bone remodeling in synovial joints.1,2 Over time, it leads to changes in the physiological mechanisms of the joint, such as cartilage erosion, synovitis, and subchondral bone sclerosis.3–5 These structural changes result in clinical symptoms such as pain, stiffness, and functional limitations, significantly compromising quality of life, physical well-being, and the ability to perform daily activities.2,6
It is estimated that approximately 240 million people worldwide live with symptomatic OA, making it one of the most prevalent conditions among older adults and women.7 The knee is one of the most commonly affected joints, with prevalence ranging from 7% to 35.1% in adults over 45 years of age.7 Major risk factors for the development of OA include advanced age, obesity, genetic predisposition, and metabolic alterations, all of which play a fundamental role in the pathogenesis of the disease.8,9
Several studies have investigated the effects of different interventions to alleviate symptoms in these patients. Exercise is widely used due to its excellent cost-effectiveness.10–12 Both traditional exercise programs and those delivered online have been shown to improve pain, function, and quality of life.13 Neuromuscular electrical stimulation (NMES) has been considered as a complementary treatment for individuals with KOA, contributing to pain relief14 and increased muscle strength,15 especially when combined with exercise.16 This combination enhanced muscle strength of the quadriceps femoris, the primary dynamic stabilizer of the knee, compared to an active control group.17
Additional evidence reinforces its effectiveness in reducing pain, as measured by the Visual Analog Scale (VAS), when compared to a placebo group. Furthermore, the combination of NMES with other therapeutic approaches has proven to be superior to isolated interventions, not only in pain relief, but also in functional improvement, particularly in the medium and long term.18 An additional study revealed that a single NMES session was able to reduce pain inhibition and increase the distance covered in the 6-minute walk test in individuals with KOA.19
Different waveforms have been used to control pain in individuals with KOA, such interferential current (IFC: 1–200 Hz burst frequency, 4000 Hz carrier frequency range), Aussie current (1–200 Hz burst frequency, 4000 Hz carrier frequency range), and transcutaneous electrical nerve stimulation (TENS: 1–200 Hz frequency range, 100–200 µs),20 have been used to manage chronic pain.21,22 TENS units have been widely used due to their low cost and ease of use and can serve as an independent treatment method treatment23,24 IFC and Aussie currents, however, deliver kilohertz-frequency alternating currents (KFAC), which pass through the tissues simultaneously and intersect with each other.23 It has been claimed that KFAC in general decreases skin impedance, reducing the discomfort normally associated with low-frequency currents, although this assertion has been challenged.25 However, an interesting systematic review with meta-analysis clearly demonstrated that both IFC (KFAC) and low-frequency current (TENS) are effective in reducing pain intensity and have similar effects on pain relief.23
Despite the potential of different NMES waveforms in managing KOA, evidence remains limited.26 Highlighted uncertainty regarding its effectiveness, citing inconclusive results due to small-scale RCTs with methodological flaws. Authors emphasize the need for rigorous, long-term RCTs to establish consistent clinical protocols,23,27,28 as methodological limitations hinder clinical applicability.29 In addition, the effects of KFAC, such as Aussie and IFC currents, on pain management in KOA have only been demonstrated in an acute randomized clinical trial.30 To address the need for RCTs evaluating the effects of NMES on KOA, the present study aimed to compare the effects of TENS, IFC, and Aussie currents on pain, disability, and pressure pain threshold in older adults with KOA, as well as their impact on gait, strength, mobility, knee temperature, postural stability and fall risk. We hypothesized that all NMES modalities would outperform placebo intervention in improving symptoms and function.
Methods
Trial Design
This is a randomized, double-blinded, parallel group, four-arm superiority clinical trial. The study was formed by four groups: (I) a group that received transcutaneous electrical nerve stimulation (TENS); (II) a group that received the interferential current (IFC); (III) a group that received the Aussie current; (IV) a group that received a Placebo intervention. Outcomes were assessed before (T0) and after 4-weeks of intervention (T1). Ethics approval was obtained by the Institutional Review Board of the Health Sciences Faculty, University of Brasília (Approval number: 62256516.2.0000.0030), and all subjects signed a detailed consent form before entering the study. This research was prospectively registered at the Brazilian Registry of Clinical Trials (RBR-875zsw/ Date of registration: 11/24/2017) and reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials).
Participants
Participants were recruited using advertisements within local clinics and hospitals located in the city of Brasília, Brazil. The trial was conducted at the Functional Performance Laboratory of the University of Brasília, Brasília, Brazil between March 2019 and August 2023. We included male and female participants aging 60 years or older with symptoms and radiographic evidence of knee osteoarthritis, confirmed by a minimum score of two on the Kellgren-Lawrence Scale. Additionally, to be included, participants had to experience pain with an intensity of 4 cm or higher on a 10-cm visual analog scale (VAS). Participants were excluded from the study if they had undergone physical therapy in the last three months, received knee injections in the last six months, had a history of hip, knee or ankle surgery in the last twelve months, had medical restrictions such as cardiorespiratory, neurological or rheumatological dysfunctions, or chronic conditions that caused knee pain.
Randomization and Allocation Concealment
Participants were randomized into experimental or placebo groups with an allocation ratio of 1:1:1:1 by means of block randomization (block size of 25) performed with the aid of a sequence of numbers generated on a computer using the website www.random.org. The allocation was hidden by means of opaque and sealed envelopes and numbered consecutively. One researcher generated the allocation sequence, hid the allocation, and allocated participants for interventions.
Blinding
One researcher collected data and performed all study assessments. A second researcher adjusted the parameters of the interventions for all groups. Finally, a third researcher applied and monitored the interventions in all groups. The equipment screen was covered by the second researcher; therefore, the researcher that applied the intervention, and the participants were blinded to group allocation.
Interventions
Protocol was conducted three times per week for four weeks across all groups. Participants were positioned supine with the upper and lower limbs extended. Group-specific parameters were: (I) TENS: 100 Hz pulse frequency, 200 µs phase duration; (II) IFC: 100 Hz burst frequency, 4000 Hz carrier frequency (10 ms burst duration, 10 ms duty cycle interval), 125 µs phase duration; (III) Aussie: 100 Hz burst frequency, 4000 Hz carrier frequency (4 ms burst duration, 16 ms duty cycle interval), 125 µs phase duration; (IV) placebo: 100 Hz pulse frequency, 200 µs phase duration. In the placebo group, the parameters were initially set to 100 Hz frequency and 200 µs pulse duration, identical to the TENS group. However, to ensure proper blinding, the stimulation was delivered only for approximately 40 seconds, with a progressive decrease in intensity until it stopped completely. After that, no electrical current was delivered, but the device remained turned on and electrodes kept connected for the full session duration to mimic the experience of active treatment, as previous described.31 Self-adhesive electrodes (25 cm2) from two channels were placed around the patella: channel 1 near the medial femoral condyle and fibular head, and channel 2 on the lateral femoral condyle and medial tibial plateau. NMES was applied to the most affected knee for 20 minutes, with intensity gradually increased every 5 minutes to match the initial sensory threshold. Participants provided feedback to adjust intensity up to the maximum tolerable sensory threshold (Figure 1).
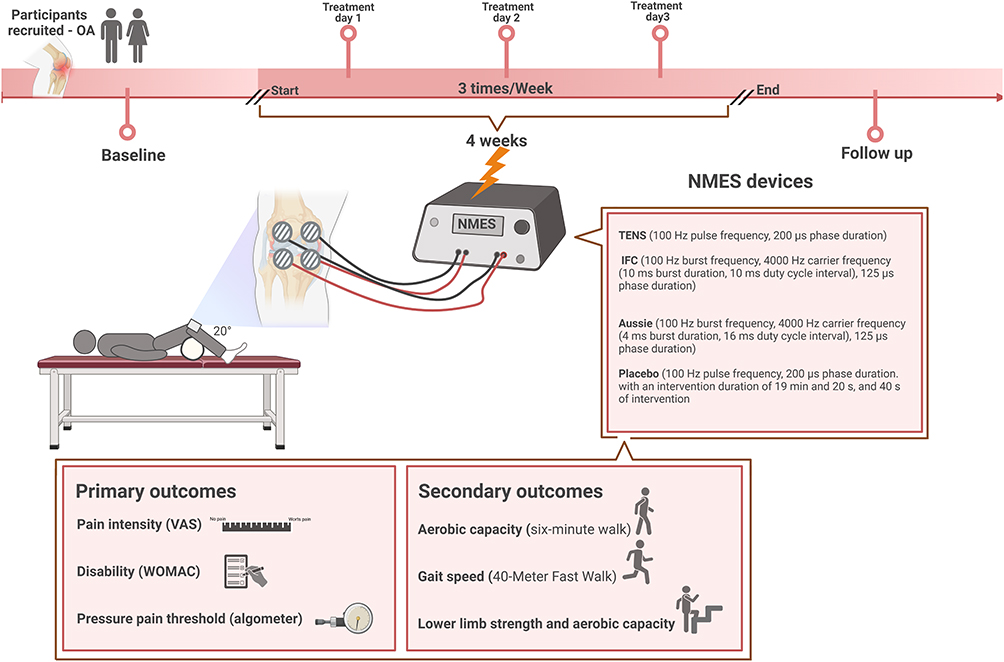 |
Figure 1 Study design. |
Outcomes
Initially, participants were screened to confirm eligibility. Participants’ characteristics such as gender, age, body mass, height, body mass index, physical activity level, and personal history regarding surgery, prosthesis, and comorbidities were collected at the baseline assessment. Primary and secondary outcomes were measured at the baseline assessment and immediately after the four-week intervention period. Assessment was carried out for two days: day one included questionnaires, thermography, BIODEX and Pressure pain threshold and day two included physical measures.
Primary Outcomes
Pain Intensity
Pain intensity was assessed using a visual analogue scale (VAS), which consists of a numerical scale from 0 to 10 points, where 0 means no pain and 10 means the maximum pain ever experienced.32
Pain, Stiffness and Physical Function
Disability was assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire. This tool employs a 5-point Likert scale across three domains: pain, stiffness, and physical function. The pain domain (0–20) includes five questions on discomfort during activities such as walking on a flat surface, climbing stairs, nighttime pain in bed, sitting or lying down, and standing upright. The stiffness domain (0–8) consists of two questions, while the physical function domain (0–68) includes 17 questions. The total WOMAC index score (0–96) provides an overall measure of disability. Lower scores indicate less disability.33
Pressure Pain Threshold
Pressure pain threshold was assessed using a pressure algometer (Kratos DDK, São Paulo, Brazil). Twelve points around the knee were assessed. (I) two cm below the medial epicondyle of the femur; (II) two cm below the lateral epicondyle of the femur; (III) two cm above the base of the patella; (IV) center of the patella; (V) one cm beyond the medial margin of the patella; (VI) one cm beyond the lateral margin of the patella; (VII) two cm below the medial margin of the patella; (VIII) two cm below the lateral margin of the patella; (IX) midpoint between the apex of the patella and the tibial tuberosity; (X) posterior region of the femoral epicondyle; (XI) five cm distal to the tuberosity of the lateral epicondyle; (XII) five cm distal to the tibial tuberosity. Three measurements at each point were performed, with a 1-minute rest between them, and the average of the 12 points was recorded for the analysis.34
Secondary Outcomes
Aerobic Capacity
The six-minute walk test was also used to assess aerobic capacity. The test was conducted on a flat, straight, 20-meter corridor marked with cones at both ends. Participants were instructed to walk as fast as possible for six minutes at a self-selected pace, with the option to slow down or stop if necessary. Standardized verbal encouragement was provided at regular intervals. A single trial was performed, and the total distance walked in meters was used in the analysis. Higher distance indicates better aerobic capacity.35
Gait Speed
The 40-Meter Fast Walk Test was used to assess gait speed. The test was conducted on a flat, straight, 40-meter corridor marked with cones at both ends. Participants were instructed to walk a total distance of 40 meters as fast as possible while maintaining a safe and controlled pace. Standardized verbal encouragement was provided at regular intervals. A single trial was performed, and the total time to complete the task was recorded in seconds for the analysis. Lower time to perform the test indicate higher gait speed.36
Lower Limb Strength and Aerobic Capacity
The stair test was used to assess lower limb strength and aerobic capacity. Participants ascended and descended an 11-step stairway (17 cm per step) as quickly as possible. Use of the handrail for support was optional. A single trial was performed, and the total time to complete the task (from the bottom to the top and back down) was recorded in seconds for the analysis.19
Lower Limb Strength
The 30-Second Chair Stand Test (30CST) was used to assess lower limb strength. Participants began seated in a chair without armrests, with their arms crossed over their chest. They were instructed to stand up and sit down as many times as possible within 30 seconds. A repetition was counted only if the participant fully extended their hips and knees before returning to the seated position.37 Three trials were performed, with a 1-minute rest between each. The total number of repetitions was recorded, and the average of the three trials was used in the analysis.
Functional Mobility
Timed Up and Go (TUG) test was used to assess functional mobility. Participants began seated in a chair without armrests and were instructed to stand up, walk 3 meters, turn around, return to the chair, and sit down. Three trials were performed, with a 1-minute rest between each. The time to complete the task was recorded in seconds, and the average of the three trials was used for the analysis.35
Superficial Knee Temperature
Superficial knee temperature was measured using a real-time thermal thermometer with a 640 x 480-pixel resolution, sensitivity of 0.08°C and an accuracy of ±2°C for absolute temperature measurements (Flir C2™, Wilsonville, Oregon, USA). Superficial knee temperature was measured as a surrogate for knee surface inflammation.38,39 Three images were captured from the lateral, medial, and frontal regions of the knee using a specific software (FLIR Thermal Studio Suite™, Wilsonville, Oregon, USA). The average temperature from these three images was used in the analysis.38
Postural Stability and Fall Risk
Biodex Balance System (Biodex Medical Systems, Inc., Shirley, NY, USA) was used to assess postural stability and fall risk. This system features a dynamic platform with adjustable stability levels, allowing for the evaluation of balance control under varying conditions. Participants performed standardized balance tests while standing on the platform, and postural sway was quantified using stability indices. Global Stability Index (GSI), which reflects overall postural stability, was calculated based on the anterior-posterior stability index (APSI) and medial-lateral stability index (MLSI). The Risk of Falls Index (RFI) was derived by comparing each participant’s GSI to age-matched normative data from the Biodex database.40 Higher GSI values indicate greater postural instability, while higher RFI values suggest an increased risk of falls.
Data Analysis and Sample Size
Data were analyzed using SPSS (Statistical Package for the Social Sciences) version 25.0. Descriptive statistics consisted in means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. Data normality was tested using the Shapiro–Wilk test. One-way ANOVAs were used to compare the general characteristics across study groups. Between-group differences (treatment effects) and their 95% confidence intervals (CIs) were calculated using two-way ANOVAs (parametric data) or Generalized Estimated Equations (GEE) (non-parametric data). The groups (TENS × IFC × Aussie × Placebo) were used as the independent factor, time (T0 × T1) as the repeated factor, and the primary and secondary outcomes as dependent variables. Bonferroni’s post hoc test was applied for pairwise comparisons. A significance level of p < 0.05 was used for all analyses. Effect sizes were determined using partial eta-squared (η2). Values of η2 > 0.01 were defined as small, η2 > 0.06 as medium, and η2 > 0.14 as large.41 Cohen’s d (d) was used for the pairwise comparisons. Values of d = 0.2 were defined as small, d = 0.5 as medium, and d = 0.8 as large.41 An intention-to-treat analysis was performed for all randomized participants. Subgroup analyses were not performed. The sample size was calculated based on the mean score on the VAS for pain intensity, previously reported for a similar population of KOA patients (8.10 ± 1.23 cm).14 An assumption was made that a clinically significant change in VAS scores would have to correspond to 30% of the total value, and a significance level of 0.01 and 95% power were adopted. These criteria led to an estimated minimum sample size of 25 in each group.19
Results
Recruitment and Baseline Data
From a total of 166 participants assessed for eligibility, 100 were recruited and randomly assigned for one of the four study groups between March 2019 and August 2023. Four participants from TENS group, four from IFC group, five from Aussie group 3, and six from placebo group 4 did not complete the intervention and declined to attend the post-intervention assessments. The recruitment process and follow-up are described in the consort flow diagram (Figure 2).
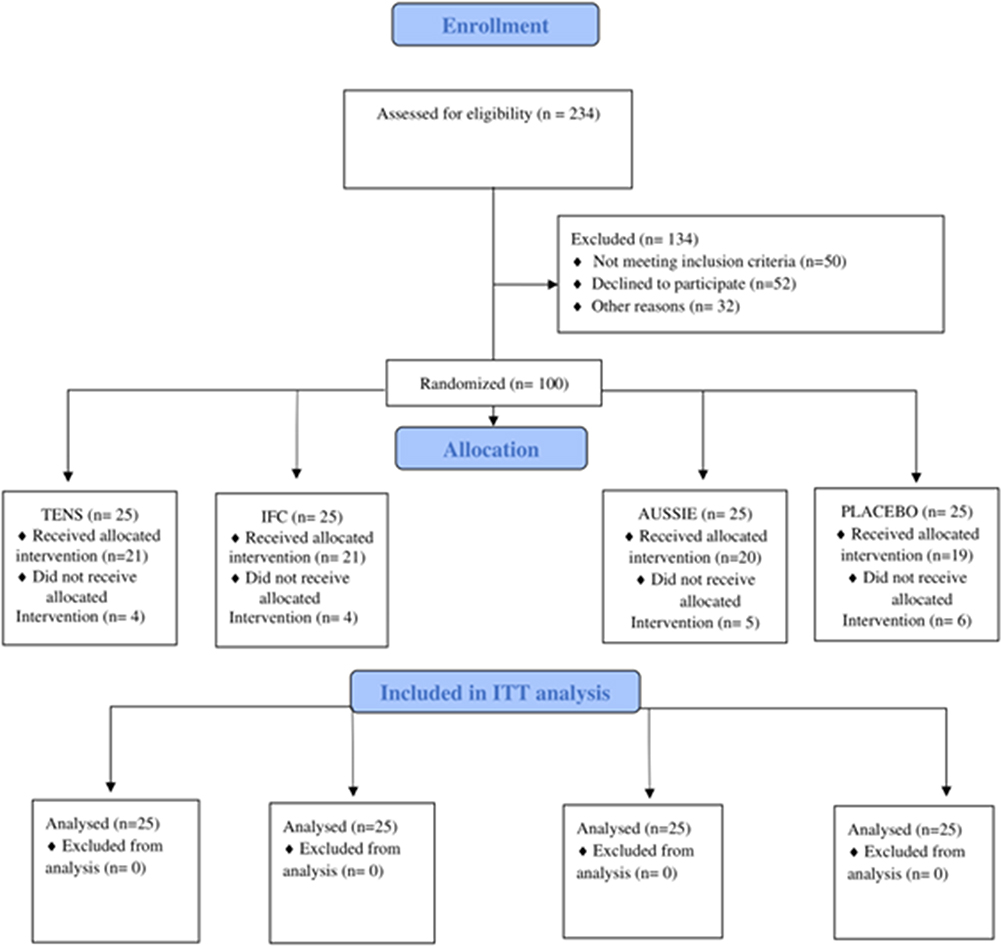 |
Figure 2 Flow diagram of the study. |
Clinical characteristics of the participants can be seen in Table 1. In general, participants were women (88%) with a mean age of 68.02 ± 5.45 years, height of 1.55 ± 0.07 m, weight of 73.04 ± 10.92 kg, and a BMI of 30.20 ± 4.74 kg/m2. Most participants had not undergone knee surgery (95%), did not have associated comorbidities (99%), and did not use prostheses (99%). It is important to note that knee surgeries performed more than 12 months prior to the start of the study, as well as prostheses in regions other than the knee joint, were permitted. Additionally, 31% of participants were classified as physically active at the beginning of the study. No significant between-group differences were found across the groups for the general characteristics (P > 0.05) (Table 1).
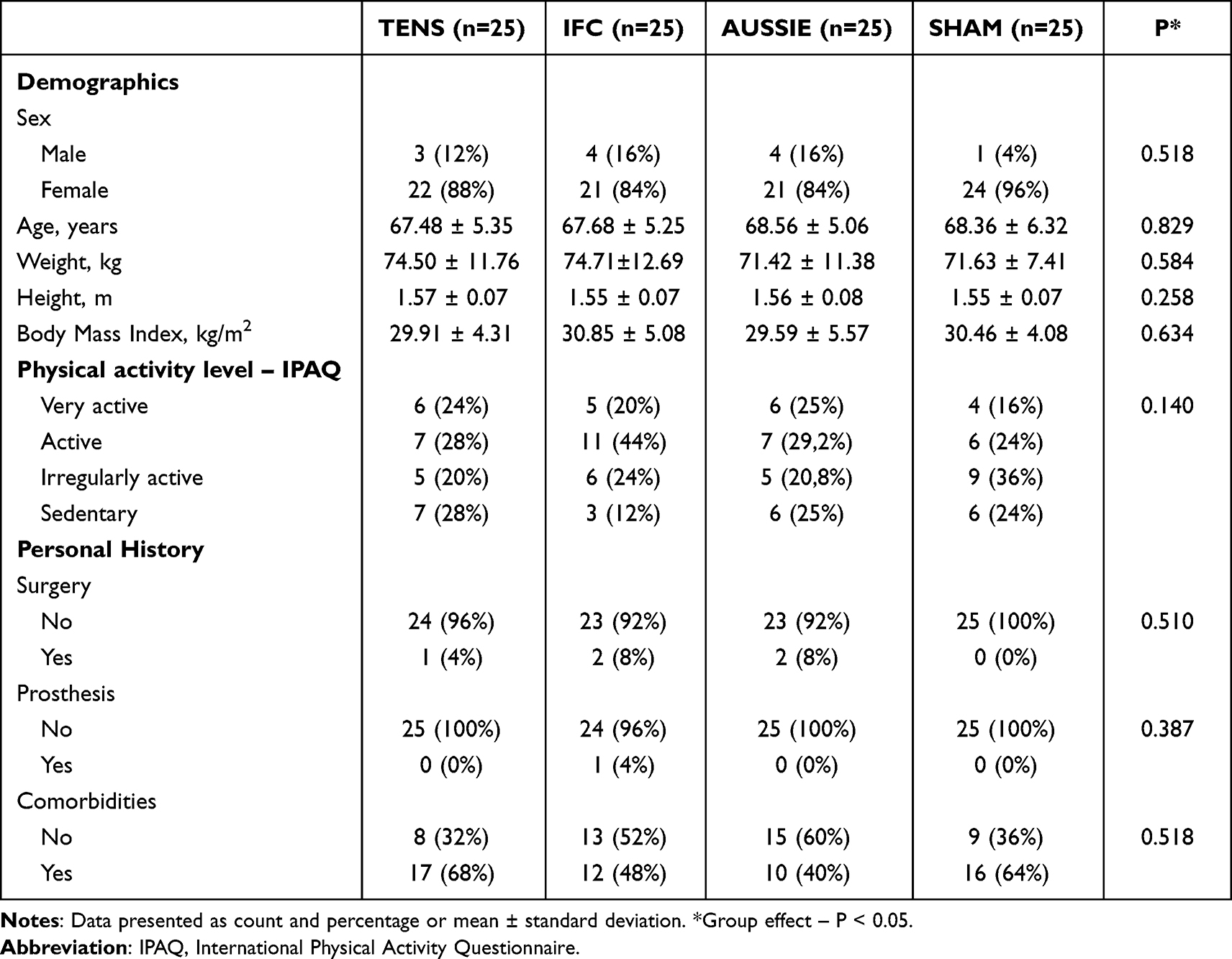 |
Table 1 Baseline Participants Characteristics (n=100) |
Regarding the baseline values of both primary and secondary outcomes, significant between-group differences, with a large effect size, were found only for the pressure pain threshold (P = 0.006, η2 = 0.13), and for the 40-meter fast walk test (P = 0.001, η2 = 0.16). No real differences were found for the pressure pain threshold (P > 0.05). Participants allocated to the TENS group demonstrated a significantly shorter distance, with a large effect size, in the 40-meter fast walk test compared to the AUSSIE group (mean difference= −9.74, 95% CI −15.92 to −3.56, P < 0.001, d= 1.09) (Table 2).
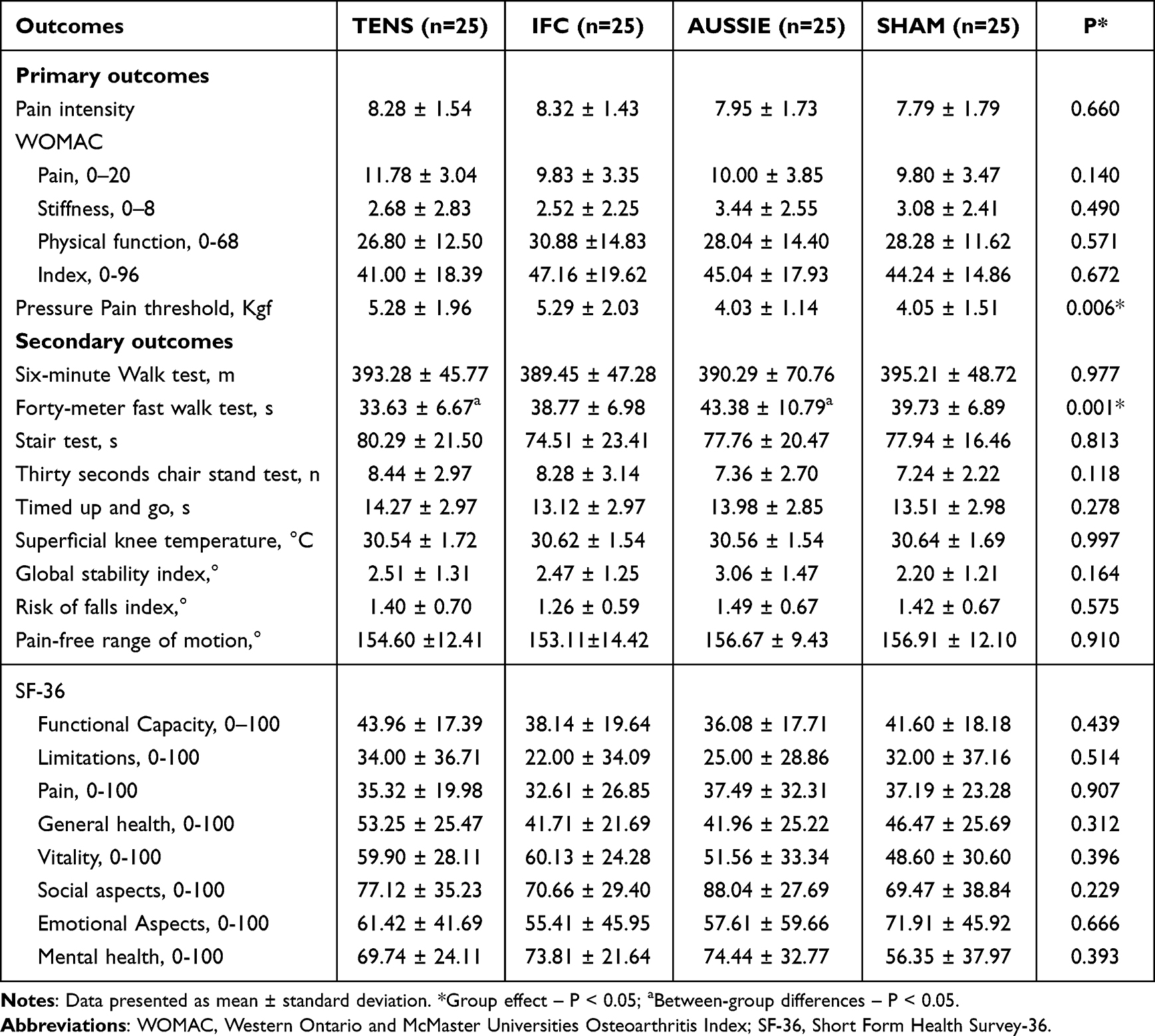 |
Table 2 Baseline Primary and Secondary Outcomes (n=100) |
Primary Outcomes
No significant group x time interactions were found for pain intensity (P = 0.398; η2 = 0.05), pain (P = 0.562; η2 = 0.03), stiffness (P = 0.547; η2 = 0.03), and physical function (P = 0.799; η2 = 0.01) dimensions of the WOMAC questionnaire, and pressure pain threshold (P = 0.858; η2 = 0.21). A time effect was found for all these outcomes (P < 0.05) with positive changes at week 4.
A significant group x time interaction, with a moderate effect size, was found for the WOMAC index (P = 0.022; η2 = 0.10). Participants of the IFC (mean difference = 21.00, 95% CI = 13.69 to 28.32, P < 0.001, d = 1.15), Aussie (mean difference = 8.37, 95% CI = 1.06 to 15.69, P = 0.025, d = 0.42), and Placebo (mean difference = 9.94, 95% CI = 2.62 to 17.25, P = 0.08, d = 0.70) groups presented less disability after the treatment (Table 3).
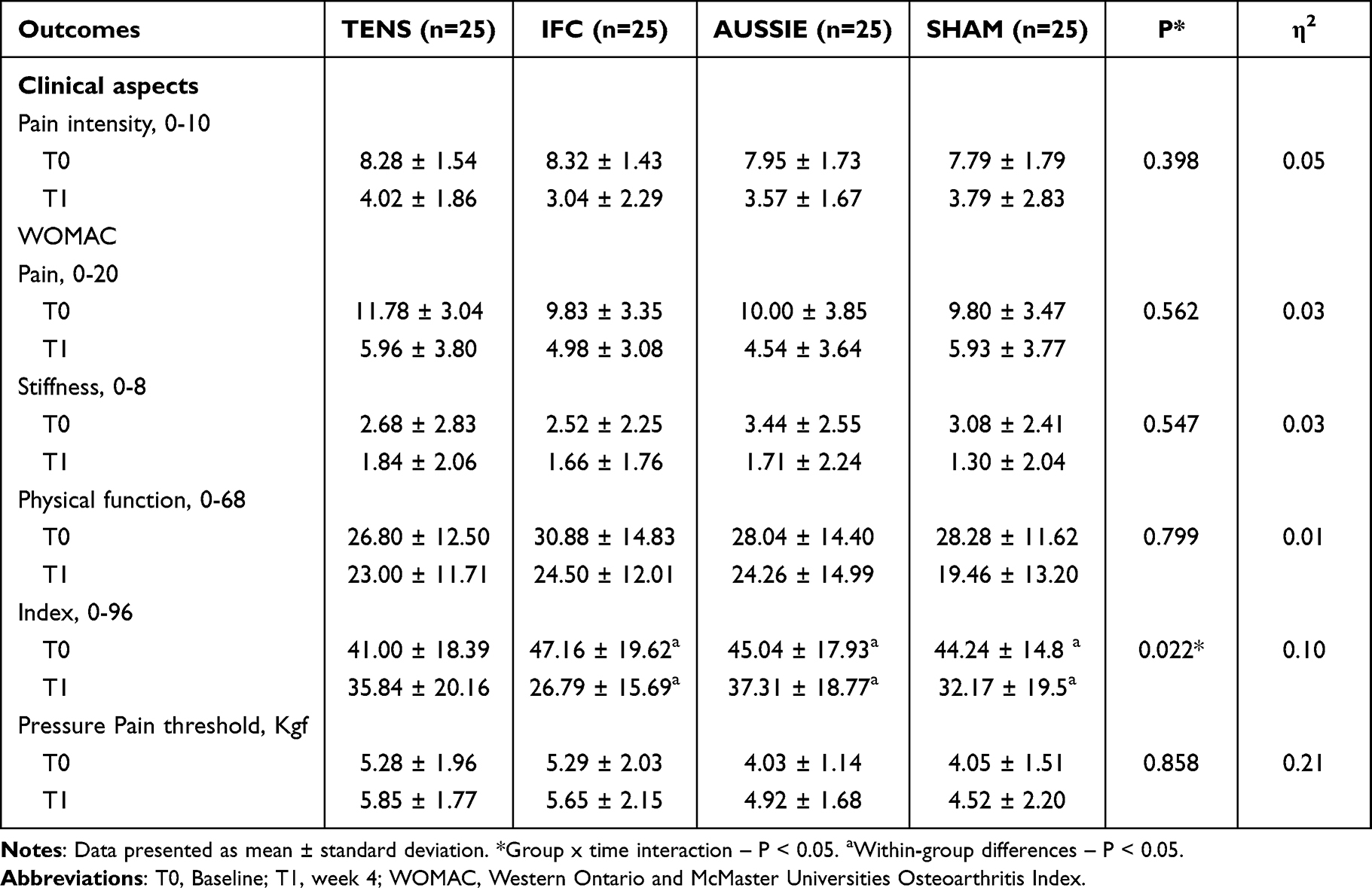 |
Table 3 Treatment Effects on the Primary Outcomes (n=100) |
Secondary Outcomes
No significant group × time interaction was found for the six-minute walk test (P = 0.609; η2 = 0.036), forty-meter fast walk test (P = 0.149; η2 = 0.58), stair test (P = 0.679; η2 = 0.17), thirty second chair stand test (P = 0.768; η2 = 0.058) and timed up and go test (P = 0.864; η2 = 0.029). A time effect was found for all these outcomes (P < 0.05) with positive changes at week 4 (Table 4). Additionally, no significant group × time interactions were found for the superficial knee temperature (P = 0.920; η2 = 0.007), biodex balance global stability index (P = 0.722; η2 = 0.061), and in the biodex balance risk of falls index (P = 0.249; η2 = 0.041) (Table 4).
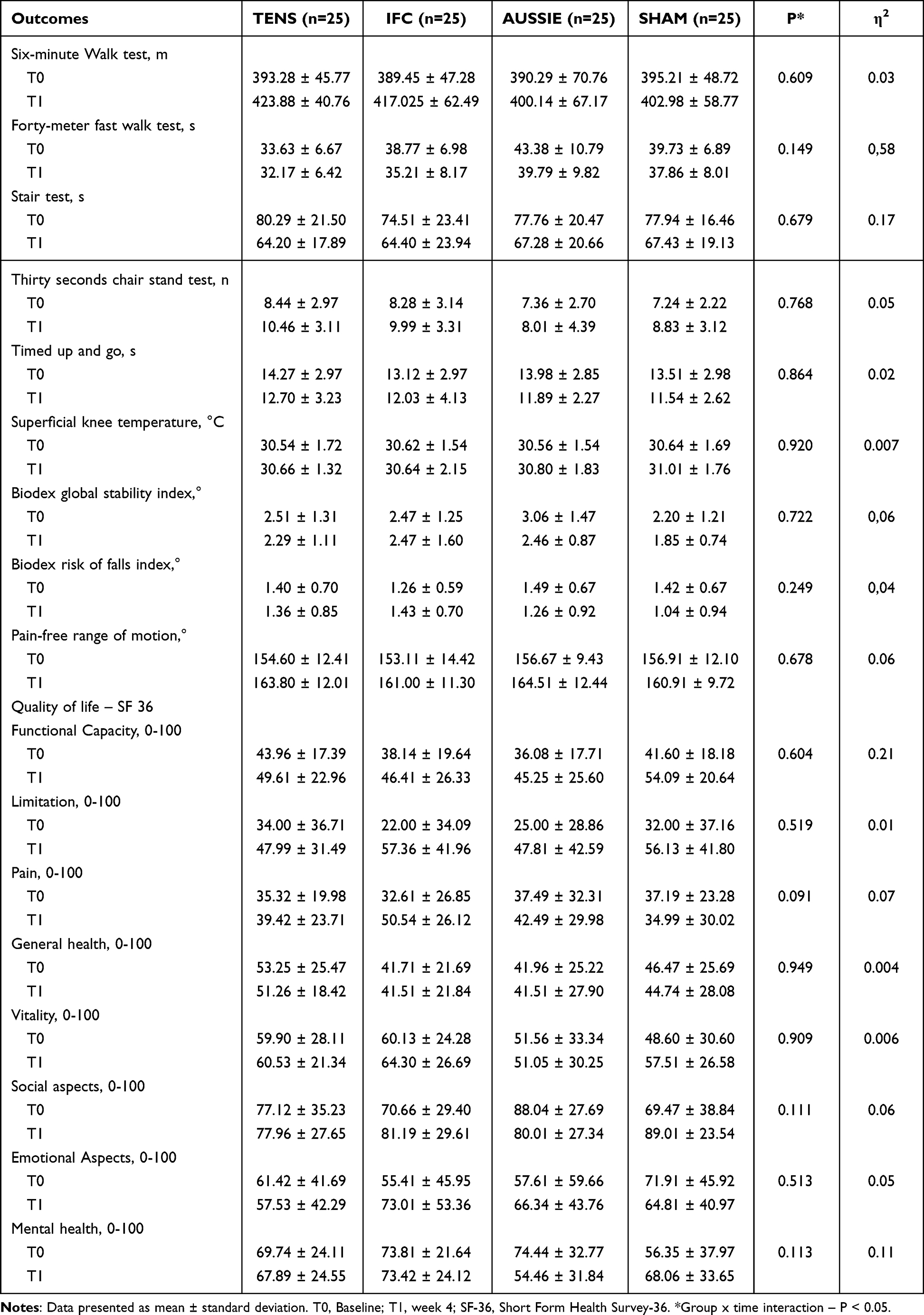 |
Table 4 Treatment Effects on the Secondary Outcomes (n=100) |
Discussion
To our knowledge, this is one of the few studies comparing the effects of different NMES modalities on pain intensity, disability, and pressure pain threshold in individuals with KOA over four weeks, as well as investigating their impacts on aerobic capacity, gait speed, lower limb strength, mobility, superficial knee temperature, stability and fall risk through different functional tests. Both IFC and Aussie groups showed significant improvements in the WOMAC index after treatment, suggesting that these interventions contributed to functional recovery. However, similar results were observed in the placebo group, indicating that NMES, when applied alone, may not be superior to a placebo intervention. Given that 4-weeks of treatment using NMES did not outperform placebo treatment, this study does not suggest that it has an important short-term effect when compared with a placebo control, as a non-pharmacological treatment for people with KOA.
Extensive experimental research on the mechanisms of IFC and Aussie currents for pain management is lacking, with claims often extrapolated from TENS studies. Our findings, with a mean difference of approximately four to five-points in the VAS scale, indicate that the experimental conditions, met the minimum detectable change for knee pain (−1.99) on the VAS pain intensity.42 Pain is not merely a direct consequence of tissue injury, but rather the result of complex interactions between sensory, cognitive, emotional, and contextual inputs within the central nervous system. Pain is influenced by individual expectations, prior experiences, emotions, memories and environmental cues.43 Therefore, we suggest that the improvement seen in the NMES, and placebo groups may be explained in part by the neuromatrix theory of pain presented above, especially for the expectations in the allocated treatment.43–45
Also, participants in our study reported significant levels of pain at the baseline assessment. It can be hypothesized that participants were experiencing a period of symptom exacerbation. Consequently, the improvements noted at the second assessment in four groups could, at least in part, reflect a regression to the mean phenomenon.46 Lastly, pain levels are closely associated with arthrogenic muscle inhibition (AMI) of the quadriceps femoris in patients with KOA.47 The NMES intensity was set at the sensory threshold, which might have been insufficient for meaningful analgesic effects, as higher intensities are often linked to better pain relief.22,48 Also, previous studies have shown that TENS applied for forty and sixty-minutes promoted higher improvements in pain intensity when compared to this same current delivered only for 20 minutes (our protocol) in patients with KOA.49 It is therefore plausible that the intensity and duration of NMES applied in the intervention groups were insufficient to elicit meaningful motor-level contractions capable of overcoming AMI. As a result, the stimulation may not have produced a neuromuscular response robust enough to promote greater improvements in pain and functional performance when compared to the placebo condition.
Despite intensity and duration, another aspect that may have influenced the results was the lack of combination with proper exercise. Our study may not have demonstrated a significant difference compared to a Placebo group because NMES was not applied alongside exercise. No significant functional differences at the end of treatment regarding pain intensity, gait speed, and disability, with mean differences between groups below clinically relevant thresholds were found in a study that compared NMES alone to a placebo group for three weeks.50 The combination of NMES with other interventions yielded significant improvements in pain intensity and disability in KOA patients, with positive effects observed in the short, medium, and long term.18,27 This suggests that the beneficial effects of NMES may surpass those of a placebo intervention when combined with another approach, such as exercise, highlighting the potential synergistic effects of multimodal strategies in KOA management.
No significant improvements were found in aerobic capacity, gait speed, lower limb strength, functional mobility, superficial knee temperature, postural stability and fall risk. These results are consistent with a recent systematic review and meta-analysis, which indicated that NMES applied alone did not improve functional outcome in the 6MWT in individuals with KOA undergoing surgical procedures.51 Also, our hypothesis is supported for a different study,52 which observed improvements in functional performance, as assessed by the ST, TUG, and 6MWT tests, in the group treated with NMES combined with functional activities versus a group that received isolated NMES. These results suggest that combining NMES with other interventions may enhance therapeutic effects not only in pain intensity, but also, in outcomes related to functional performance.
Our findings are particularly relevant given the high prevalence of KOA and its potential to trigger the development of other conditions, such as metabolic syndromes induced by immobilization, which are associated with cardiovascular diseases, recognized factors in determining population mortality.53 Scientific and clinical implications can be formulated based on the results of this study. NMES programs applied in isolation do not show superior results compared to placebo. As evidenced by previous studies,14–16,18,27,52 NMES combined with other interventions has the potential to optimize functional performance and promote significant improvements in the quality of life of individuals with KOA, contributing to physical recovery and increased autonomy in daily activities.
Some limitations of this study must be highlighted. Individuals with comorbidities associated with KOA were included in the study, which may have influenced the results, especially regarding pain intensity and pressure pain threshold. The diversity of these conditions may have generated individual variabilities in the response to treatment, impacting the interpretation of the effects. Additionally, the 20-minute duration of NMES therapy may have been insufficient to detect potential chronic effects of the intervention, limiting the generalization of findings in the long term.22 The inclusion of movement-evoked pain (MEP) as a measurement could significantly enhance the understanding of NMES effects KOA.50 Unlike pain at rest, MEP reflects the pain experienced during functional activities, such as walking or other movements, and is driven by distinct mechanisms.54 Incorporating MEP into the study would allow for a more comprehensive assessment of NMES, particularly regarding pain during movement, which is often more disabling for patients with KOA than static pain. The use of painkillers and other prescribed treatments was not controlled. This may have introduced variability in pain and function outcomes, potentially confounding treatment effects. Future randomized controlled trials should improve the protocol used and investigate the long-term results with appropriate follow-up periods. Also, it is important to explore how individual variables influence treatment responses.
Conclusion
Neuromuscular electrical stimulation, using different modalities (TENS, IFC, and Aussie), did not demonstrate superiority over placebo for pain intensity, disability, pressure pain threshold, gait parameters, strength, mobility, knee temperature, postural stability, and fall risk over a four-week period in individuals with knee osteoarthritis (KOA). Although the IFC and Aussie modalities promoted improvements in the WOMAC index with moderate effect sizes, similar improvements were also observed in the placebo group, suggesting that these results are not superior to the placebo effect. Future research should investigate optimized NMES parameters, extended intervention durations, and combined therapies to enhance effectiveness.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of University of Brasília (protocol code CAAE 62256516.2.0000.0030). Written informed consent has been obtained from the patient(s) to publish this paper.
Data Sharing Statement
The data will be made available by the corresponding author upon reasonable request.
Acknowledgment
The authors would like to thank Danilo Aquino Amorim, Fernanda and Hudson Pinheiro for helping with participant recruitment, the Federal District health secretary, and the staff of University of Brasília – Faculdade de Ciências e Tecnologias em Saúde.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, Brazil (CAPES), Finance Code 001, Fundação de Apoio à Pesquisa do Distrito Federal (FAPDF) (grant numbers 00193.00001222/2021-26; 00193-00001261/2021-23 and 00193-00002357/2022-90, 00193-00001261/2021-23; 00193-00001623/2024-29), and the National Council for Scientific and Technological Development (CNPq; process number 310269/2021; 402816/2023-4; 141130/2023-7).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
2. Yao Q, Wu X, Tao C, et al. Osteoarthritis: pathogenic signaling pathways and therapeutic targets. Signal Transduct Target Ther. 2023;8(1):56. doi:10.1038/s41392-023-01330-w
3. Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64(6):1697–1707. doi:10.1002/art.34453
4. Lei Y, Wang X, Liao J, et al. Shear-responsive boundary-lubricated hydrogels attenuate osteoarthritis. Bioact Mater. 2022;16:472–484. doi:10.1016/j.bioactmat.2022.02.016
5. Donate R, Tamaddon M, Ribeiro V, Monzón M, Oliveira JM, Liu C. Translation through collaboration: practice applied in BAMOS project in in vivo testing of innovative osteochondral scaffolds. Biomater Transl. 2022;3(2):102–104. doi:10.12336/biomatertransl.2022.02.003
6. Loeser RF. Ageing and the pathogenesis of osteoarthritis. Nat Rev Rheumatol. 2016;12(7):412–420. doi:10.1038/nrrheum.2016.65
7. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022;30(2):184–195. doi:10.1016/j.joca.2021.04.020
8. Hamood R, Tirosh M, Fallach N, Chodick G, Eisenberg E, Lubovsky O. Prevalence and incidence of osteoarthritis: a population-based retrospective cohort study. J Clin Med. 2021;10(18):4282. doi:10.3390/jcm10184282
9. Berenbaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage. 2013;21(1):16–21. doi:10.1016/j.joca.2012.11.012
10. Lawford BJ, Hall M, Hinman RS, et al. Exercise for osteoarthritis of the knee. Cochrane. 2024;12. doi:10.1002/14651858.CD004376.
11. Moseng T, Vliet Vlieland TPM, Battista S, et al. EULAR recommendations for the non-pharmacological core management of Hip and knee osteoarthritis: 2023 update. Ann Rheum Dis. 2024;83(6):730–740. doi:10.1136/ard-2023-225041
12. Teo PL. Identifying and prioritizing clinical guideline recommendations most relevant to physical therapy practice for hip and/or knee osteoarthritis. J Orthop Sports Phys Ther. 2019;49(7):501–512. doi:10.2519/jospt.2019.8676
13. Tang L, Wang MM, Wang HX, He XY, Jiang YS. mHealth-based exercise vs. traditional exercise on pain, functional disability, and quality of life in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Front Physiol. 2025;15:1511199. doi:10.3389/fphys.2024.1511199
14. Moezy A, Masoudi S, Nazari A, Abasi A. A controlled randomized trial with a 12-week follow-up investigating the effects of medium-frequency neuromuscular electrical stimulation on pain, VMO thickness, and functionality in patients with knee osteoarthritis. BMC Musculoskelet Disord. 2024;25(1):158. doi:10.1186/s12891-024-07266-8
15. Hammami N, Jdidi H, Khezami MA, et al. Isokinetic strengthening and neuromuscular electrical stimulation protocol impact on physical performances, functional status and quality of life in knee osteoarthritis overweight/obese women. Knee. 2022;39:106–115. doi:10.1016/j.knee.2022.09.004
16. de Paula Gomes CAF, Politti F, de Souza Bacelar Pereira C, et al. Exercise program combined with electrophysical modalities in subjects with knee osteoarthritis: a randomised, placebo-controlled clinical trial. BMC Musculoskelet Disord. 2020;21(1):258. doi:10.1186/s12891-020-03293-3
17. Bispo VA, Bastos JAI, Almeida CCD, Modesto KAG. The effects of neuromuscular electrical stimulation on strength, pain, and function in individuals with knee osteoarthritis: a systematic review with meta-analysis. Fisioterapia e Pesquisa. 2021;28(4):416–426. doi:10.1590/1809-2950/20028528042021
18. Wu Y, Zhu F, Chen W, Zhang M. Effects of transcutaneous electrical nerve stimulation (TENS) in people with knee osteoarthritis: a systematic review and meta-analysis. Clin Rehabil. 2022;36(4):472–485. doi:10.1177/02692155211065636
19. Shimoura K, Iijima H, Suzuki Y, Aoyama T. Immediate effects of transcutaneous electrical nerve stimulation on pain and physical performance in individuals with preradiographic knee osteoarthritis: a randomized controlled trial. Arch Phys Med Rehabil. 2019;100(2):300–306.e1. doi:10.1016/j.apmr.2018.08.189
20. Johnson MI, Tabasam G. A single-blind investigation into the hypoalgesic effects of different swing patterns of interferential currents on cold-induced pain in healthy volunteers. Arch Phys Med Rehab. 2003;84(3):350–7. doi:10.1053/apmr.2003.50005
21. Almeida CC, Silva VZM, Júnior GC. Transcutaneous electrical nerve stimulation and interferential current demonstrate similar effects in relieving acute and chronic pain: a systematic review with meta-analysis. Braz J Phys Ther. 2018A;22:347–354. doi:10.1016/j.bjpt.2017.12.005
22. Vance CGT, Dailey DL, Chimenti RL, Van Gorp BJ, Crofford LJ, Sluka KA. Using TENS for pain control: update on the state of the evidence. Medicina. 2022;58:1332. doi:10.3390/medicina58101332
23. Almeida CC. Transcutaneous electrical nerve stimulation and interferential current demonstrate similar effects in relieving acute and chronic pain: a systematic review with meta-analysis. Braz J Phys Ther. 2018B;22(5):347–354. doi:10.1016/j.bjpt.2017.12.005
24. Goats GC. Physiotherapy treatment modalities Interferential current therapy. Br J Sp Med. 1990;24(2):87. doi:10.1136/bjsm.24.2.87.
25. Alon G. Interferential current news. Phys Ther. 1987;67(2):280–281. doi:10.1093/ptj/67.2.280
26. Rutjes AW, Nüesch E, Sterchi R, Kalichman L. Transcutaneous electrostimulation for osteoarthritis of the knee. Cochrane Database Syst Rev. 2009;4. doi:10.1002/14651858.
27. Chen HL, Yang FA, Lee TH, Liou TH, Escorpizo R, Chen HC. Effectiveness of interferential current therapy in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2022;12(1):9694. doi:10.1038/s41598-022-13478-6
28. Glaviano NR, Saliba S. Can the use of neuromuscular electrical stimulation be improved to optimize quadriceps strengthening? Sports Health. 2016;8(1):79–85. doi:10.1177/1941738115618174
29. Dantas LO, Moreira RFC, Norde FM, Mendes Silva Serrao PR, Alburquerque-Sendín F, Salvini TF. The effects of cryotherapy on pain and function in individuals with knee osteoarthritis: a systematic review of randomized controlled trials. Clin Rehabil. 2019;33(8):1310–1319. doi:10.1177/0269215519840406
30. Azevedo KP, Almeida CC, Garcia PA, et al. Short-term effects of single administration of electrical stimulation waveforms on pain, range of motion and skin temperature in knee osteoarthritis: a double-blinded clinical trial. J Clin Med. 2025. doi:10.1177/0269215518817807
31. Zeng C, Li H, Yang T, et al. Electrical stimulation for pain relief in knee osteoarthritis: systematic review and network meta-analysis. Osteoarthritis Cartilage. 2015;23(2):189–202. doi:10.1016/j.joca.2014.11.014
32. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63 Suppl 11:S240–S252. doi:10.1002/acr.20543
33. Pietrosimone B, Luc-Harkey BA, Harkey MS, et al. Using TENS to enhance therapeutic exercise in individuals with knee osteoarthritis. Med Sci Sports Exerc. 2020;52(10):2086–2095. doi:10.1249/MSS.0000000000002353
34. Imamura M, Rebello-Sanchez I, Parente J, et al. Factors associated with pain pressure threshold in both local and remote sites in knee osteoarthritis. PM R. 2024;16(2):132–140. doi:10.1002/pmrj.13038
35. Dobson F, Hinman RS, Roos EM, et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthritis Cartilage. 2013;21(8):1042–1052. doi:10.1016/j.joca.2013.05.002
36. Ramalho RB, Casonato NA, Montilha VB, Chaves TC, Mattiello SM, Selistre LFA. Construct validity and responsiveness of performance-based tests in individuals with knee osteoarthritis. Arch Phys Med Rehabil. 2024;105(10):1862–1869. doi:10.1016/j.apmr.2024.05.024
37. Skou ST, Roos EM. Physical therapy for patients with knee and hip osteoarthritis: supervised, active treatment is current best practice [published correction appears in Clin Exp Rheumatol. 2020 Sep-Oct;38(5):1036.]. Clin Exp Rheumatol. 2019;37 Suppl 120(5):112–117.
38. Denoble AE, Hall N, Pieper CF, Kraus VB. Patellar skin surface temperature by thermography reflects knee osteoarthritis severity. Clin Med Insights Arthritis Musculoskelet Disord. 2010;3:69–75. doi:10.4137/CMAMD.S5916
39. De Marziani L, Boffa A, Angelelli L, et al. Infrared thermography in symptomatic knee osteoarthritis: joint temperature differs based on patient and pain characteristics. J Clin Med. 2023;12(6):2319. doi:10.3390/jcm12062319
40. Parraca JA, Olivares ST, Carbonell BA, Aparicio GM, Adsuar SJ, Gusi FN. Test-retest reliability of biodex balance SD on physically active old people. J Human Sport Exercise. 2011:444–451. ISSN 1988-5202. doi:10.4100/jhse.2011.62.25
41. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
42. Tubach F, Ravaud P, Baron G, et al. Evaluation of clinically relevant states in patient reported outcomes in knee and Hip osteoarthritis: the patient acceptable symptom state. Ann Rheum Dis. 2005;64(1):34–37. doi:10.1136/ard.2004.023028
43. Melzack R. From the gate to the neuromatrix. Pain. 1999;Suppl 6:S121–S126. doi:10.1016/S0304-3959(99)00145-1 PMID: 10491980.
44. Dieppe P, Goldingay S, Greville-Harris M. The power and value of placebo and nocebo in painful osteoarthritis. Osteoarthritis Cartilage. 2016;24(11):1850–1857. doi:10.1016/j.joca.2016.06.007
45. Rossettini G, Carlino E, Testa M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet Disord. 2018;19:27. doi:10.1186/s12891-018-1943-8
46. Whitney CW, Von Korff M. Regression to the mean in treated versus untreated chronic pain. Pain. 1992;50(3):281–285. PMID: 1280801. doi:10.1016/0304-3959(92)90032-7
47. Seeley MK, Lee H, Son SJ, Timmerman M, Lindsay M, Hopkins JT. A review of the relationships between knee pain and movement neuromechanics. J Sport Rehabil. 2021;31(6):684–693. PMID: 34942599. doi:10.1123/jsr.2021-0020
48. Pantaleão MA, Laurino MF, Gallego NL, et al. Adjusting pulse amplitude during transcutaneous electrical nerve stimulation (TENS) application produces greater hypoalgesia. J Pain. 2011;12(5):581–590. doi:10.1016/j.jpain.2010.11.001
49. Cheing GL, Tsui AY, Lo SK, Hui-Chan CW. Optimal stimulation duration of tens in the management of osteoarthritic knee pain. J Rehabil Med. 2003;35(2):62–68. PMID: 12691335. doi:10.1080/16501970306116
50. Reichenbach S, Jüni P, Hincapié CA, et al. Effect of transcutaneous electrical nerve stimulation (TENS) on knee pain and physical function in patients with symptomatic knee osteoarthritis: the ETRELKA randomized clinical trial. Osteoarthritis Cartilage. 2022;30(3):426–435. doi:10.1016/j.joca.2021.10.015
51. Peng L, Wang K, Zeng Y, Wu Y, Si H, Shen B. Effect of neuromuscular electrical stimulation after total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Front Med. 2021;8:779019. doi:10.3389/fmed.2021.779019
52. Lawson D, Degani AM, Lee K, et al. Use of transcutaneous electrical nerve stimulation along with functional tasks for immediate pain relief in individuals with knee osteoarthritis. Eur J Pain. 2022;26(3):754–765. doi:10.1002/ejp.1903
53. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study [published correction appears in J Am Coll Cardiol. 2021;77(15):1958-1959. doi: 10.1016/j.jacc.2021.02.039.]. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
54. Hilfiker R, Jüni P, Nüesch E, Dieppe PA, Reichenbach S. Association of radiographic osteoarthritis, pain on passive movement and knee range of motion: a cross-sectional study. Man Ther. 2015;20(2):361–365. doi:10.1016/j.math.2014.11.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.