Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Ciprofol on Postoperative Delirium in Elderly Patients Undergoing Hip Surgery: A Randomized Controlled Trial
Authors Chen Z ![]() , Liu YY, Hu Q
, Liu YY, Hu Q ![]() , Wang JS
, Wang JS ![]() , Cao RY, Yu ST, Lu F, Zhong ML, Liang WD
, Cao RY, Yu ST, Lu F, Zhong ML, Liang WD ![]() , Wang L
, Wang L ![]()
Received 11 March 2025
Accepted for publication 16 July 2025
Published 19 July 2025 Volume 2025:19 Pages 6207—6218
DOI https://doi.org/10.2147/DDDT.S524319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qiongyu Guo
Zhen Chen,1 Ying-Ying Liu,1 Qian Hu,1 Jia-Sheng Wang,1 Rui-Yang Cao,1 Su-Ting Yu,2 Feng Lu,3,4 Mao-Lin Zhong,3,4 Wei-Dong Liang,3,4 Lifeng Wang3,4
1The First Clinical Medical College of Gannan Medical University, Ganzhou, Jiangxi, People’s Republic of China; 2Guangdong Provincial People’s Hospital Ganzhou Hospital, Ganzhou, Jiangxi, People’s Republic of China; 3Department of Anesthesiology, First Affiliated Hospital of Gannan Medical University, Ganzhou, Jiangxi, People’s Republic of China; 4Ganzhou Key Laboratory of Anesthesiology, The First Affiliated Hospital of Gannan Medical University, Ganzhou, Jiangxi, People’s Republic of China
Correspondence: Lifeng Wang, Department of Anesthesiology, First Affiliated Hospital of Gannan Medical University, 128 Jinling Road, Golden Development Zone, Ganzhou City, Jiangxi Province, 341000, People’s Republic of China, Email [email protected]
Purpose: As a novel intravenous anaesthetic, ciprofol is widely used in clinical practice. However, its potential association with postoperative delirium (POD) is unclear. Silent information regulator factor 3(SIRT3) could regulate mitochondrial function, initiate mitochondrial autophagy, and has played an important role in maintaining normal neuronal cell function. This trial aimed to explore the effect of ciprofol on the pathogenesis of POD and whether SIRT3 had a correlation with the pathogenesis of POD.
Patients and methods: One hundred fourteen elderly patients scheduled for elective hip joint surgery were included in this randomized controlled, double blind study. The patients were randomly assigned at a 1:1 ratio to either the ciprofol group (Group C, induction of anaesthesia with 0.3 mg/kg ciprofol) or the propofol group (Group P, induction of anaesthesia with 1.5 mg/kg propofol). On postoperative days 1 and 3, the 3D-CAM scale was used to assess whether POD occurred in both groups of patients.
Results: No statistically significant difference was observed in the general condition of the patients in the two groups. Within the first 3 days after surgery, the incidence of POD was lower in Group C than in Group P (5.5% vs 20%; P = 0.022). At 1 min of administration, ciprofol had less circulatory effects and a lower incidence of injection pain, but a higher incidence of muscle twitching than propofol. On postoperative day 1, SIRT3 expression was greater in Group C than in Group P (P = 0.028). Additionally, SIRT3 expression was found to be correlated with POD. The serum SIRT3 level on postoperative day 1 had an area under the receiver operating characteristic (ROC) curve of 0.8540 (P < 0.001), with a detection threshold of 1.565 ng/mL, yielding a sensitivity of 0.820 and a specificity of 0.900.
Conclusion: In this study, we found that ciprofol was associated with a lower incidence of POD and had a minimal impact on circulatory function. SIRT3 expression and POD were correlated. A serum SIRT3 level less than 1.565 ng/mL on postoperative day 1 may indicate a likelihood of POD, highlighting its potential diagnostic value.
Keywords: postoperative delirium, ciprofol, total hip arthroplasty, silent information regulator factor 3
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Lu has been published for this article.
Introduction
Postoperative delirium (POD) is an acute confusional state characterized by fluctuations in attention and consciousness, disorientation, memory impairment, perceptual disturbances, and cognitive disarray. It is one of the most common postoperative complications in elderly patients.1,2 POD not only prolongs the hospital stay, reduces long-term quality of life, and increases the socioeconomic burden but also may lead to death.3,4 POD may be associated with factors such as age, ASA classification, level of education, hypoalbuminemia, surgical trauma, and intraoperative hypotension;5,6 however, its exact pathogenesis remains unclear. Recent studies revealed that neuroinflammation,7 oxidative stress,8 and mitochondrial dysfunction9 may be key mechanisms underlying the development of POD. Exploring the pathogenesis of and risk factors for POD as well as implementing early interventions targeting these factors is highly valuable for reducing the incidence of POD.
Owing to the aging of the population, hip joint diseases are becoming increasingly prevalent. Hip arthroplasty has been shown to improve quality of life of elderly patients with hip disorders.10 Currently, approximately one million hip replacement surgeries are performed worldwide each year, a number that may double over the next 20 years.11 Patients undergoing such procedures are predominantly elderly, and postoperative delirium (POD) is highly prevalent among hip replacement patients, especially on the third postoperative day, with an incidence ranging from 28% to 61%.12,13 This may be associated with factors such as significant blood loss, intraoperative circulatory instability, extensive surgical trauma, and postoperative pain.14
Ciprofol is a novel intravenous anaesthetic independently developed in China. Its molecular structure is based on propofol, with the introduction of a cyclopropyl group, which enhances its affinity for γ-aminobutyric acid type A (GABAA) receptors. The potency of ciprofol is approximately 4 to 5 times greater than that of propofol. Compared with propofol, ciprofol offers several advantages, including greater potency, a lower incidence of injection pain, and minimal effects on the circulatory and respiratory systems.15 It may also exhibit neuroprotective effects.16,17 The mechanisms underlying these effects include reductions in oxidative stress, inflammatory responses, and antiapoptotic actions, as well as an increase in aerobic glycolysis in astrocytes.18–20
Silent information regulator factor 3 (SIRT3) is a nicotinamide adenine dinucleotide (NAD+)-dependent deacetylase involved in mitochondrial metabolic processes, including energy production, the tricarboxylic acid cycle, and oxidative stress regulation.21 SIRT3 plays a critical role in processes such as tumorigenesis and aging.22,23 Studies have shown that the activation of SIRT3 can reduce the incidence of postoperative delirium (POD) and provide significant neuroprotective effects. The mechanisms underlying these effects involve improvements in mitochondrial dysfunction, reductions in neuroinflammation and oxidative stress, and the activation of autophagy through the AMPK/mTOR pathway.24–26 SIRT3 could regulate the deacetylation of manganese superoxide dismutase (MnSOD) by inhibition of NLRP3 production in vivo and reduces the levels of inflammatory factors and oxidative stress.27,28 Meanwhile, SIRT3 deficiency upregulates the expression of inflammation-related proteins, including NLRP3, caspase-1, P20 and IL-1β.29 The naturally occurring SIRT3 agonist trilobatin has also been shown to reduce CNS inflammation and exert neuroprotective effects, accompanied by inactivation of the TLR4/NF-κB pathway.30 However, clinical evidence supporting these findings is lacking.
Thus, the aim of this study is to observe the incidence of postoperative delirium (POD) in elderly patients after hip replacement surgery under anaesthesia with ciprofol and to explore whether ciprofol can reduce the incidence of POD in this population. An additional aim of this study is to preliminarily investigate whether there is an association between SIRT3 expression and POD and explore whether a reduction in SIRT3 expression predict POD.
Methods
Study Design
This study is a prospective, double-blind, randomized controlled trial approved by the Ethics Review Committee of the First Affiliated Hospital of Gannan Medical University (Ethical Approval No. LLSC-2024009). The trial was registered with the Chinese Clinical Trial Registry on January 31, 2024 (ChiCTR2400080542). The study was conducted in adherence to the principles outlined in the Declaration of Helsinki, and informed consent was obtained from all patients or their legal representatives.
Randomization was performed using SPSS 27.0 software. The study participants were assigned numbers corresponding with the order in which they were enrolled, and the random seed 20240131 was set. The RV.Uniform function in SPSS was used for random number generation. The SPSS Visual Binning function was then used to divide the samples into two equally sized groups on the basis of the random numbers generated.
Each group allocation was placed in an opaque envelope, with the corresponding number (1–114) written on the outside. The sealed envelopes were handed to the researchers. Researchers who were not involved in the trial were responsible for the randomization process. After the participants were enrolled, they were sequentially numbered, and the corresponding numbered envelope was opened. Participants were then assigned to their respective groups and anaesthetized with the medication corresponding with the number in the envelope. The anaesthesiologist responsible for administering the medication did not participate in any other aspect of the trial but was solely responsible for managing intraoperative drug usage. Another blinded anaesthesiologist recorded various data during the procedure. The same lead surgeon performed all the surgeries. Patients, other healthcare team members, and the research personnel responsible for patient recruitment, data collection, and follow-up assessments were unaware of the group assignments. In the case of an emergency, the doctor or researcher may reveal the patient’s assigned group and remove the patient from the study to ensure their safety.
Study Population
The inclusion criteria were as follows: 1. Elderly patients who had indications for hip replacement surgery and consented to elective surgery; 2. were aged between 60 and 80 years; 3. were classified as American Society of Anaesthesiologists (ASA) physical status I–III; 4. had a body mass index (BMI) between 18 and 28 kg/m²; 5. could speak Mandarin and had no barriers to communication, such as an education level greater than 9 years; 6. had a preoperative Mini-Mental State Examination (MMSE) score ≥ 26 points; and 7. had no significant abnormalities in cardiac, pulmonary, hepatic, or renal function.
The exclusion criteria were as follows: 1. Patients with a history of cognitive impairment, dementia, or delirium before surgery. 2. Patients with severe depression, schizophrenia, or other psychiatric or neurological disorders, or those who have used antipsychotic or antidepressant medications. 3. Patients who use anti-inflammatory drugs, corticosteroids, or other hormonal medications or have a history of alcohol or drug dependence. 4. Patients with severe visual, auditory, or speech impairments that prevent them from completing the tests. 5. Patients who are allergic to propofol or ciprofol.
The criteria for withdrawal from the study were as follows: 1. Patients or their legal representatives who requested withdrawal from the study during the observation period. 2. Patients or their legal representatives who refused to cooperate postoperatively. 3. Patients with an intraoperative blood loss volume > 800 mL or who required hospitalization for more than 3 months. 4. Patients whose surgeries exceeded 3 hours or who experienced severe adverse events, such as severe allergic reactions, during surgery.
Procedures
Patients fasted for 6 h and were not allowed to drink for 2 h before surgery, and no preanaesthetic medication was administered. After entering the operating room, peripheral venous access was established, and monitoring of blood pressure (BP), electrocardiogram (ECG), heart rate (HR), pulse oximetry (SpO2), respiratory rate (RR), and the Narcotrend index (NI) was performed. Under local anaesthesia, radial artery puncture was performed for arterial catheterization for invasive arterial blood pressure monitoring and blood gas analysis. All patients in both groups received femoral nerve block (15 mL of 0.375% ropivacaine) and lateral femoral cutaneous nerve block (5 mL of 0.375% ropivacaine) under ultrasound guidance. The sensory block level was assessed 15 minutes later, and upon sufficient blockade, anaesthesia was induced.
Anaesthesia was induced on the basis of standard body weight calculations, and slow intravenous injections were administered. Ciprofol is 4–5 times more potent than propofol; therefore, we used the lowest dose of the equivalent.31 Group C received ciprofol 0.3 mg/kg, and Group P received propofol 1.5 mg/kg. Once an adequate depth of anaesthesia was achieved, sufentanil 0.5–1.0 µg/kg and rocuronium 0.6–1.0 mg/kg were administered. After the muscles were adequately relaxed, endotracheal intubation was performed under direct laryngoscopic guidance. After intubation, the ventilation parameters were adjusted as follows: tidal volume, 6–8 mL/kg; respiratory rate, 12–16 breaths/min; I:E ratio, 1:2; and oxygen flow, 2 L/min. Immediately thereafter, maintenance drugs were infused: for Group P, propofol 4–6 mg/(kg h) and remifentanil 0.05–0.2 µg/(kg min); for Group C, ciprofol 0.8–1.2 mg/(kg h) and remifentanil 0.05–0.2 µg/(kg min). The infusion rates of propofol, ciprofol, and remifentanil were adjusted according to the NI, maintaining the NI between 40 and 60 and the end-tidal carbon dioxide pressure (PetCO2) at 35–45 mmHg. Intermittent doses of rocuronium were given to maintain muscle relaxation. If the patient’s intraoperative blood pressure decreased by more than 20% from baseline, 6 mg of ephedrine was administered intravenously. If the heart rate dropped below 50 beats per minute, 0.5 mg of atropine was administered intravenously. At the end of the surgery, propofol, ciprofol, and remifentanil were discontinued, and 4 mg of ondansetron was administered intravenously for postoperative antiemesis. If POD was diagnosed postoperatively, haloperidol (5 mg) was administered intramuscularly.
All patients received patient-controlled intravenous analgesia (PCIA) postoperatively. The PCIA formula was as follows: sufentanil 2 µg/kg + ondansetron 12 mg + 0.9% sodium chloride, prepared to a total volume of 100 mL.
Remedial measures: Given that all the patients enrolled were elderly, benzodiazepines were not used to reduce the risk of increasing the incidence of POD.32 Only intravenous anaesthetics, ciprofol and propofol, were used for anaesthesia induction. If the NI did not fall below 60 within 1 minute of ciprofol or propofol injection, a remedial dose of sedatives was administered: for Group C, 0.1 mg/kg ciprofol was given; for Group P, 0.5 mg/kg propofol was given. If, after the remedial dose, the NI still did not fall below 60, a second remedial dose was given until the desired depth of anaesthesia was achieved.
Endpoints
Primary Outcome Measure: The incidence of postoperative delirium (POD) within the first 3 days after surgery. Patients were screened for POD on postoperative day 1 (D1) and postoperative day 3 (D3) using the 3D-CAM scale. This scale is an improvement of the CAM and consists of 10 evaluator-rated items, 10 observer-rated items, and 2 selective items, with each item being classified as “correct” or “incorrect.” These 22 items are categorized into 4 features: feature 1—acute changes or fluctuations in mental status; feature 2—attention deficits; feature 3—changes in level of consciousness; and feature 4—disorganized or confused thinking. A diagnosis of delirium is made if the patient is positive for Feature 1 and Feature 2, along with any positive result from Feature 3 or Feature 4.
Secondary Outcome Measures: Mean arterial pressure (MAP), heart rate (HR), and Narcotrend index (NI) values recorded at the following time points: upon entry into the operating room (T0), 1 minute after drug administration (T1), 2 minutes after drug administration (T2), 3 minutes after drug administration (T3), after intubation (T4), after position change (T5), at the start of surgery (T6), and at the end of surgery (T7). The frequency of remedial sedative doses and the time taken to reach the appropriate depth of anaesthesia were recorded. The number of times that ephedrine and atropine were administered intraoperatively was also noted. On D1 and D3, patients were followed up to inquire about the occurrence of adverse events, including nausea, vomiting, and pain.
Serum Biomarker Measurements: Peripheral blood samples (4 mL) were collected from patients at T0, D1, and D3, centrifuged at 4000 × g for 10 minutes, and the serum was stored at −80°C. Serum SIRT3 levels were measured at T0, D1, and D3 using enzyme-linked immunosorbent assay (ELISA) kits produced by Bioswamp Life Science Lab, Wuhan, China. The absorbance at 450 nm was measured using a microplate reader. A standard curve was constructed with the concentration of standard samples on the x-axis and optical density (OD) values on the y-axis. The concentration of SIRT3 in each serum sample was calculated by comparing its OD value to the OD value of known standards. All analyses were repeated and quantified according to the manufacturer’s protocol, and the mean value was used for analysis. All the serum samples were processed by the same laboratory technician every three months.
Statistical Analysis
This experiment is a randomized controlled trial, with the control group being the propofol group (Group P) and the experimental group being the ciprofol group (Group C). The primary outcome measure of this study was the incidence of postoperative delirium (POD) in patients. According to previous studies, the incidence of POD in elderly patients who underwent orthopaedic surgery under propofol anaesthesia was 27%,33 whereas the incidence of POD in elderly patients anaesthetized with ciprofol was 7%.16 Setting both α = 0.05 and β = 0.2, with an equal number of patients in both groups, the minimum sample size required for each group was 52 patients according to calculations using PASS 15 statistical software. Considering a 10% loss to follow-up rate, 57 patients were required per group, for a total of 114 patients.
Data were analysed and processed using SPSS 27.0 statistical software. For normally distributed continuous data, values are expressed as means ± standard deviations, and independent sample t tests were used for intergroup comparisons. Nonnormally distributed continuous data are presented as medians (interquartile ranges), and Mann‒Whitney U-tests were used for intergroup comparisons. Categorical data are expressed as frequencies (percentages), and chi-square or Fisher’s exact tests were used for intergroup comparisons. Repeated measures analysis of variance was used to compare haemodynamic parameters (MAP, HR) and serum biomarkers (SIRT3) at different time points, with Bonferroni correction applied. A P value <0.05 indicated statistical significance.
Results
Baseline Measurements
A total of 209 patients were recruited, and 114 patients were enrolled and randomly assigned to two groups. One patient was excluded because of a surgery duration >3 hours, and three patients withdrew from the study because they refused postoperative follow-up and blood sampling (Figure 1). Ultimately, data from 110 patients were analysed. There were no statistically significant differences between the two groups in terms of age, sex, BMI, ASA classification, preoperative MMSE score, surgery duration, or intraoperative blood loss volume (P > 0.05) (Table 1).
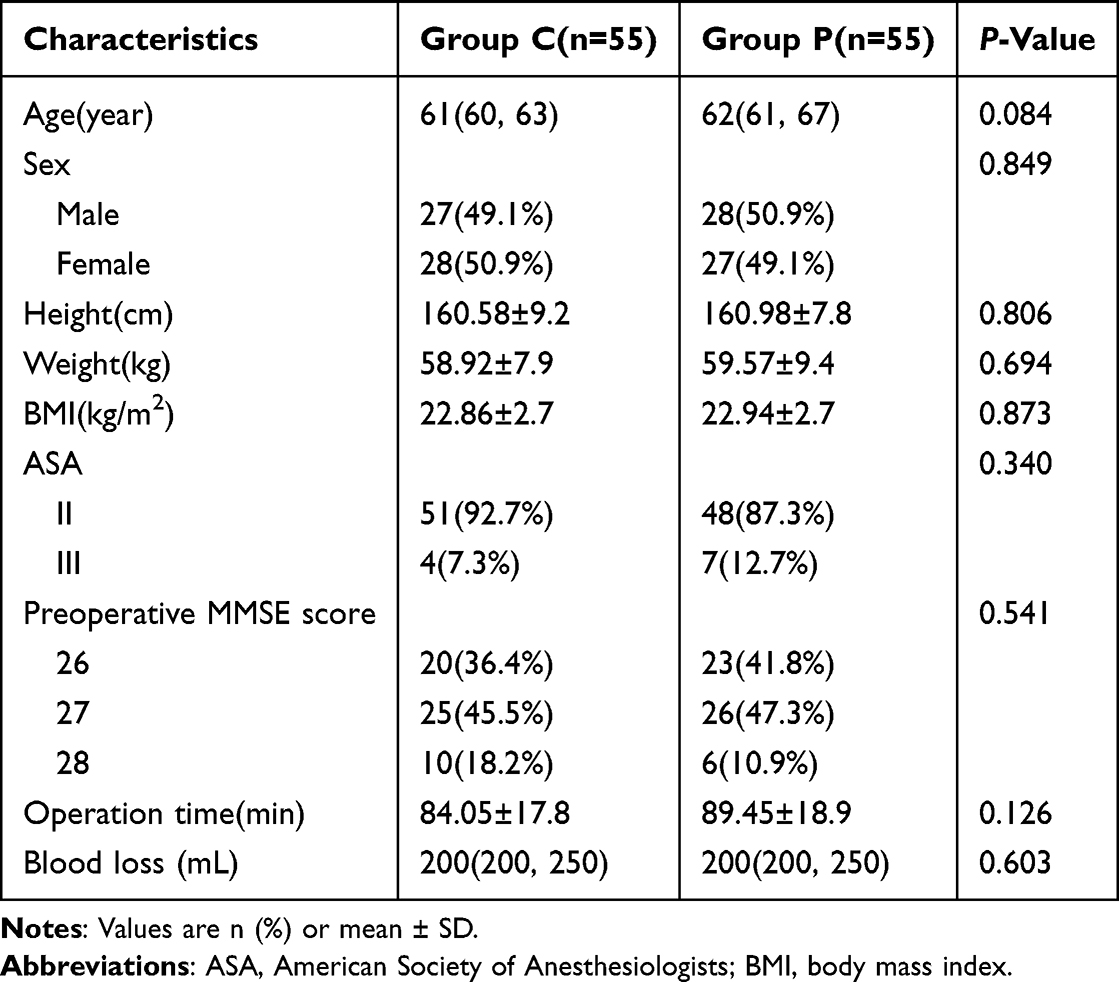 |
Table 1 Comparison of General Data and Intraoperative Variables Between the Two Groups |
 |
Figure 1 Flow chart. |
Primary Outcomes
Our study revealed that within the first 3 days after surgery, the overall incidence of postoperative delirium (POD) in Group C was lower than that in Group P (P = 0.022). On postoperative day 1, the incidence of POD in Group C was significantly lower than that in Group P (P = 0.047). However, there was no significant difference in the incidence of POD between the two groups from postoperative day 1 to day 3 (P = 0.618) (Table 2).
 |
Table 2 Comparison of the Incidence of Postoperative Delirium |
Secondary Outcomes
At T0, there were no statistically significant differences in the MAP or HR between the two groups. One minute after induction (T1), the MAP and HR in Group P were significantly lower than those in Group C (Figure 2). Moreover, during surgery, the number of patients in Group C who required ephedrine was significantly lower than that in Group P (23 vs 42, P < 0.001) (Table 3). At T0, there were no significant differences in the NI values between the two groups. At T1, T2, T5, and T7, the NI values were significantly different between the two groups. The NI values in Group C were higher than those in Group P at 1 minute and 2 minutes after drug administration (Figure 3). Anaesthesia was successfully induced in all patients (100% success rate), but the time to reach an adequate depth of anaesthesia in Group C (97.27 ± 43.1 seconds) was significantly longer than that in Group P (63.45 ± 35.1 seconds) (P < 0.001). During induction, 17 patients (30.9%) in Group C required one additional dose of ciprofol, and 8 patients (14.5%) required two additional doses. In contrast, 22 patients (40.0%) in Group P required one additional dose of propofol, and 4 patients (7.3%) required two additional doses. However, the differences in the number of additional sedative doses between the two groups were not statistically significant (Table 4).
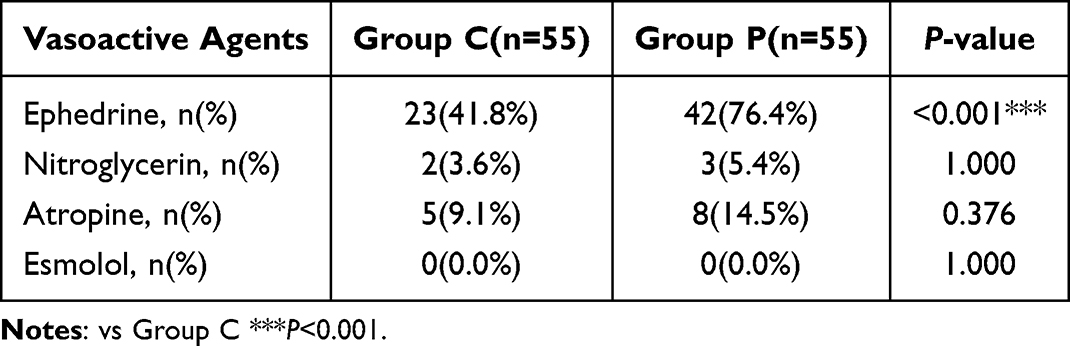 |
Table 3 Comparison of the Use of Vasoactive Drugs Between the Two Groups |
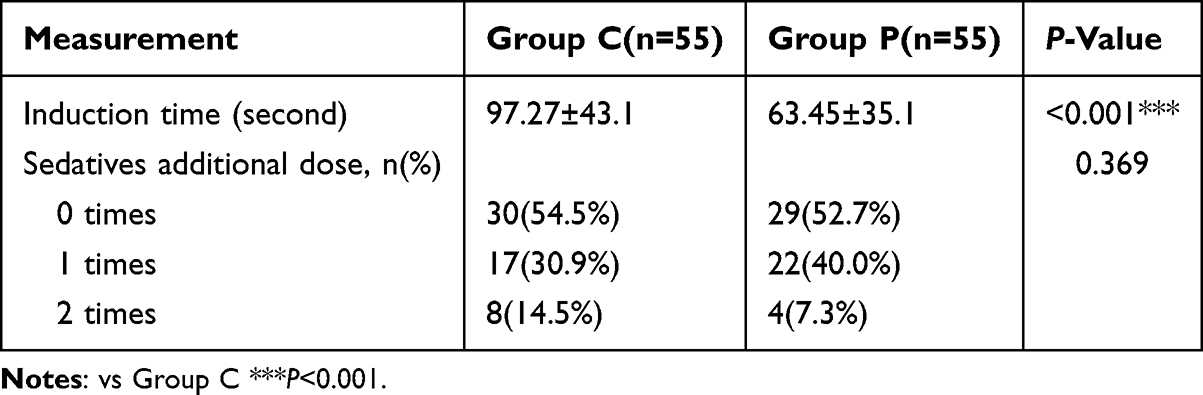 |
Table 4 Comparison of Induction Time and Number of Additional Sedatives Administered |
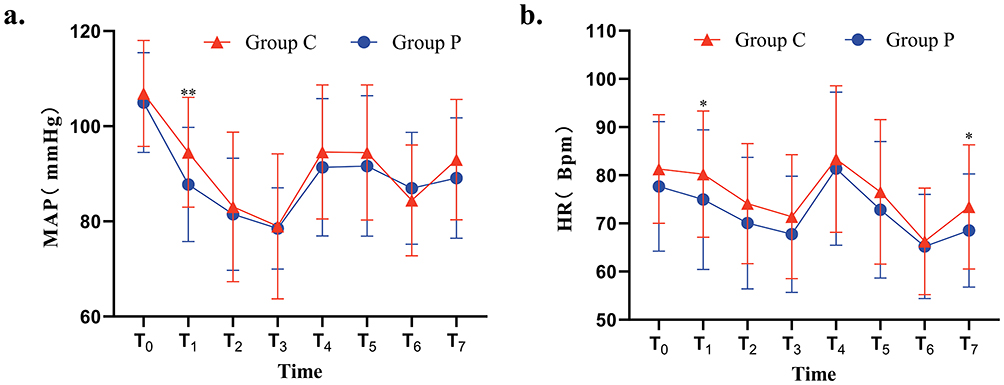 |
Figure 2 MAP (a) and HR (b) at different time points in the two groups. vs Group C *P<0.05, **P<0.001. |
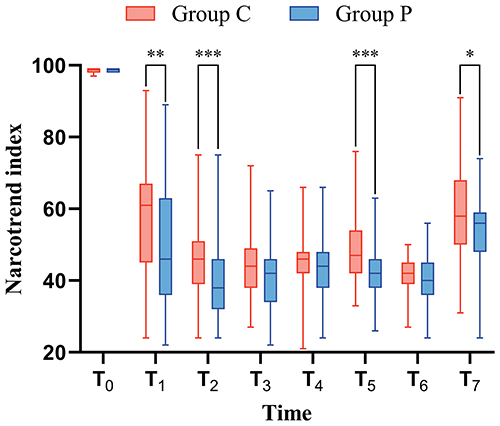 |
Figure 3 Narcotrend index values at different time points in the two groups. vs Group C *P<0.05, **P<0.01, ***P<0.001. |
We also observed some complications during and after surgery. During anaesthesia induction, 8 patients (14.5%) in Group C experienced muscle tremors, whereas only 2 patients (3.6%) in Group P experienced muscle tremors (P = 0.047). Thirteen patients (23.6%) in Group P experienced injection pain, whereas no patients in Group C reported injection pain (P < 0.001). There were no significant differences between the two groups in terms of postoperative nausea and vomiting (P > 0.05) (Table 5).
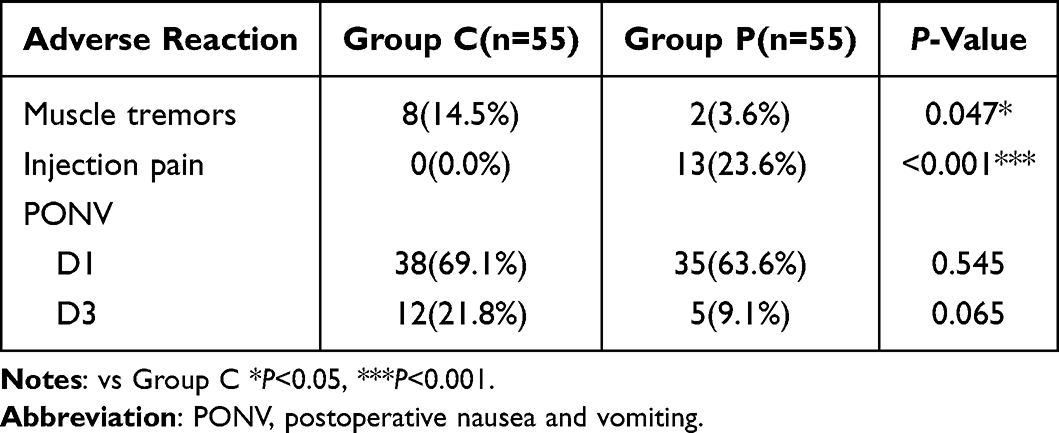 |
Table 5 Comparison of Complications Between the Two Groups |
We also compared the SIRT3 expression levels in the two groups at different time points. On postoperative day 1, the serum SIRT3 levels in Group C were higher than those in Group P (P < 0.05) (Figure 4a). However, on postoperative day 3, there was no significant difference in the serum SIRT3 level between the two groups (P > 0.05) (Figure 4a). The ROC curve for serum SIRT3 levels on postoperative day 1 showed an area under the curve (AUC) of 0.8540 (P < 0.001), with a threshold of 1.565 ng/mL, corresponding to a sensitivity of 0.820 and a specificity of 0.900 (Figure 4b). The ROC curve for postoperative day 3 had an AUC of 0.8703 (P > 0.05) (Figure 4c). We believe that levels of SIRT3 less than 1.565 ng/mL measured on postoperative day 1 may be of value in the diagnosis of POD.
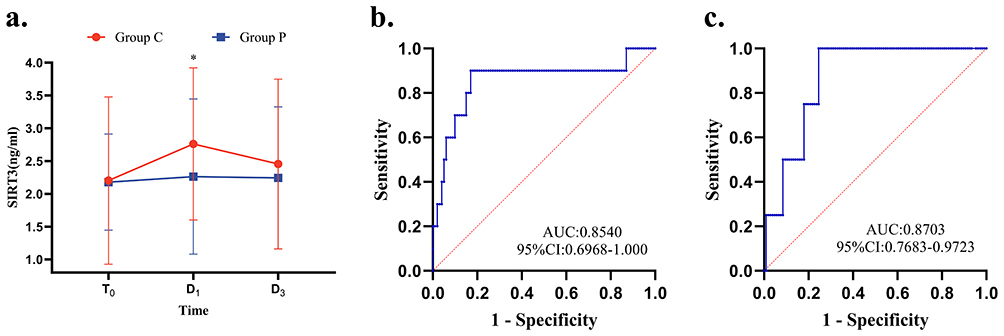 |
Figure 4 Changes in the expression of SIRT3 over time (a) and ROC curves of SIRT3 level and POD ((b) day 1, (c) day 3) vs Group C *P<0.05. |
Discussion
In this study, the clinical data of 114 elderly patients who underwent hip fracture surgery were analysed, and both ciprofol and propofol were found to be safe for anaesthesia induction and maintenance during such surgeries. We observed that the incidence of postoperative delirium (POD) was lower with ciprofol than with propofol, and there was less impact on haemodynamics during surgery, along with a lower incidence of injection pain. Additionally, ciprofol did not increase the incidence of postoperative complications.
Propofol is the most common intravenous anaesthetic used during the perioperative period, and it has been shown to reduce the incidence of POD to some extent.34,35 The potential mechanisms include a reduction in inflammatory cytokine production, attenuation of tumour necrosis factor-α (TNF-α) effects on the blood‒brain barrier, and inhibition of hippocampal neuronal apoptosis.36–38 In a previous study, propofol was found to promote type 1 inositol triphosphate receptor (InsP3R-1) activation, which in turn induced mitochondrial autophagy to provide cytoprotection.39 SIRT3 exerts its anti-inflammatory effects mainly through the regulation of mitochondrial autophagy.40 The anti-inflammatory effects of propofol may have some link to SIRT3. Ciprofol and propofol are structurally similar and may have similar functions, but the specific mechanism by which cyclobenzaprine is associated with mitochondrial autophagy is unclear. However, propofol often leads to dose-dependent hypotension, causing significant haemodynamic fluctuations that may increase the risk of postoperative complications such as renal dysfunction, myocardial injury, and even mortality.41,42 Ciprofol, on the other hand, has a safe therapeutic window (0.15–0.9 mg/kg), a low incidence of injection pain, and minimal cardiovascular effects.43 In previous studies, researchers recommended a 0.3 mg/kg dose of ciprofol for elderly patients.44 However, this may be a relatively low starting dose, as we excluded the use of benzodiazepines to avoid their potential impact on POD. As a result, some elderly patients in our study did not achieve an ideal depth of anaesthesia with a 0.3 mg/kg dose of ciprofol, and remedial doses were administered during the procedure. While a 0.3 mg/kg dose is considered relatively safe, a dose of 0.4 mg/kg may also be a safe option when using ciprofol alone. This finding aligns with that of another study, although the risk of hypotension may be slightly higher with a 0.4 mg/kg dose.45 However, as this study did not specifically investigate this topic, no definitive conclusions can be drawn.
Our study revealed that, after anaesthesia induction, both groups of patients experienced varying degrees of decreases in MAP and HR. However, with ciprofol, the reduction in MAP and HR was less pronounced, and the patients’ haemodynamics were more stable This finding is consistent with that of previous research.46 This suggests that ciprofol has a smaller circulatory suppressive effect, which may be due to its greater potency compared to propofol, allowing for lower clinical doses and resulting in lower plasma drug concentrations. Consequently, the effects on receptors or channels related to circulatory suppression are smaller. Furthermore, the metabolites of ciprofol are pharmacologically inactive, which may also contribute to its lesser impact on circulation.
Injection pain is one of the most common adverse reactions associated with propofol. The incidence of injection pain associated with propofol is approximately 70%.47 Injection pain can lead to patient anxiety, distressing memories, and decreased satisfaction.48 The pain may be caused by two mechanisms: free propofol directly stimulating nociceptors in the vein wall or its active component activating the kallikrein-kinin system upon contact with the vascular endothelium, leading to the release of bradykinin. The intensity of pain is positively correlated with the aqueous concentration of the drug.48,49 In our study, 23.6% of patients in the propofol group experienced injection pain, whereas no injection pain was reported in the ciprofol group, indicating a significant difference in incidence, possibly because the introduction of a cyclopropyl group into ciprofol increases its lipophilicity and hydrophobicity, resulting in its much lower aqueous concentration compared to propofol.50 Second, the clinical dosage of ciprofol is usually lower than that of propofol, causing less irritation to the vessel wall.43
The onset time for propofol is approximately 30 seconds to 1 minute.51 However, ciprofol has a longer onset time. In our study, we observed that with ciprofol, the NI value decreased more gradually, with an average onset time of 97s, than with propofol, which was only 63s. The possible reason for this is that ciprofol has high lipophilicity and a low aqueous concentration, making its active component release slower. Therefore, in clinical practice, when it is not possible to monitor anaesthetic depth, the administration of muscle relaxants is recommended at least 2 minutes after ciprofol administration to avoid the feeling of suffocation or near-death due to the efficacy of muscle relaxants appearing prior to sedation.
During the anaesthesia induction phase, we also observed that 8 participants in the ciprofol group developed myoclonus, a phenomenon that has been noted by some researchers.52 Additionally, a small number of patients exhibited excitation, such as delirium and involuntary movements, during the anaesthesia induction phase. This may also be related to the slower onset time of the ciprofol, causing patients to remain in a shallower state of anaesthesia for a longer period (similar to the excitement stage in Guedel’s stages of anaesthesia). This shallow anaesthetic state may cause anxiety in patients, leading to myoclonus and other manifestations. Furthermore, in our study, we observed that approximately 2–3 minutes after intubation, the NI values in Group C were higher than those in e Group P, with some patients’ NI exceeding 60, necessitating immediate administration of sedative and anaesthetic drugs. In clinical practice, it is important to maintain the depth of anaesthesia and sedation after induction to avoid intraoperative awareness.
Propofol reduces the incidence of POD. However, in this study, we found a statistically significant difference in the incidence of POD on postoperative day 1 between the two groups: 3.6% in Group C versus 14.5% in Group P (P < 0.05). This finding suggests that the use of ciprofol during surgery is associated with a lower incidence of POD, although the exact mechanisms remain unclear.53 SIRT3 is the only member of the sirtuin family that plays a role in extending the human lifespan and is linked to the onset of neurodegenerative diseases.54 Recent studies have revealed that SIRT3 can reduce the incidence of postoperative cognitive dysfunction (POCD), with its primary mechanisms including the inhibition of hippocampal neuroinflammation, maintenance of mitochondrial function, and activation of autophagy.25,26,55 In this study, we measured the expression of SIRT3 in the peripheral blood of both groups at three time points, preoperatively, on postoperative day 1, and on postoperative day 3, and explored the correlation between the onset of POD and SIRT3 expression. We found that the expression of SIRT3 increased postoperatively in both groups, possibly because surgical trauma stimulated the expression of SIRT3, thereby inhibiting the expression of inflammatory cytokines and reducing oxidative stress.56 The expression of SIRT3 was greater in the ciprofol group than in the propofol group, which may be associated with the lower incidence of POD in this group. To further explore this, we performed univariate logistic regression analysis and found that the expression of SIRT3 in the serum on postoperative day 1 may have diagnostic value for the occurrence of POD. SIRT3 has potential value for the diagnosis of POD when serum levels fall below 1.565 ng/mL.
This study also has several limitations. First, postoperative delirium (POD) in this study was solely assessed using the 3D-CAM scale, and the use of a single assessment method may introduce some bias, with underestimation of the incidence of POD. Second, we only administered a 0.3 mg/kg dose of ciprofol and was unable to evaluate the clinical effects of higher doses of ciprofol, such as whether it results in a faster onset of anaesthesia or further reduces the incidence of POD. Third, the participants in this study were predominantly aged 60–65 years, with fewer elderly patients aged 75 years and above. As a result, 45.5% of patients in Group C who received a 0.3 mg/kg dose of ciprofol required one or more remedial sedative doses. In contrast, the study by LU,52 which included patients aged 75 years and older, revealed that a 0.3 mg/kg dose of ciprofol successfully induced anaesthesia in all patients. The age distribution in our study of elderly patients aged 60–80 years was not uniform; thus, the conclusions may not be applicable to the entire elderly population. In addition, this study was a single-centre study that lacked external validation; guidelines are lacking for elderly patients over the age of 80 years. Therefore, we look forward to multicentre, large-sample studies or stratified analyses based on age to guide medication use in all age groups of elderly patients.
Conclusion
In this study, we found that ciprofol could be safely and effectively used for anaesthesia in elderly (aged 60–80 years) hip arthroplasty patients. Ciprofol had a minimal impact on circulatory function, could reduce the use of intraoperative vasoactive drugs, had a low incidence of injection pain, and was associated with a lower incidence of POD. There may be a correlation between SIRT3 expression and the onset of POD. A serum SIRT3 level less than 1.565 ng/mL on postoperative day 1 may indicate a likelihood of POD and serve as a predictor of POD onset.
Data Sharing Statement
Data are available to researchers on request for the purpose of reproducing the results or replicating the procedure by directly contacting the corresponding author.
Ethics Approval
The study was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Gannan Medical University (No. LLSC-2024009).
Consent Statement
All study participants or their legally authorized representative provided informed consent.
Funding
Key Research and Development Projects of Ganzhou (Program No. GZ2024YLJ109).
Disclosure
L-FW receives grants from the Key Research and Development Projects of Ganzhou (Program No. GZ2024YLJ109). The authors report no other conflicts of interest in this work.
References
1. Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. 2022;77(1):92–101. doi:10.1111/anae.15607
2. Wilson JE, Mart MF, Cunningham C, et al. Delirium. Nat Rev Dis Primers. 2020;6(1):90. doi:10.1038/s41572-020-00223-4
3. Fan Y, Yuan L, Ji M, Yang J, Gao D. The effect of melatonin on early postoperative cognitive decline in elderly patients undergoing Hip arthroplasty: a randomized controlled trial. J Clin Anesth. 2017;39:77–81. doi:10.1016/j.jclinane.2017.03.023
4. Goldberg TE, Chen C, Wang Y, et al. Association of Delirium With Long-term Cognitive Decline: a Meta-analysis. JAMA Neurol. 2020;77(11):1373–1381. doi:10.1001/jamaneurol.2020.2273
5. Brown CH, Neufeld KJ, Tian J, et al. Effect of Targeting Mean Arterial Pressure During Cardiopulmonary Bypass by Monitoring Cerebral Autoregulation on Postsurgical Delirium Among Older Patients: a Nested Randomized Clinical Trial. JAMA Surg. 2019;154(9):819–826. doi:10.1001/jamasurg.2019.1163
6. Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. 2008;108(1):18–30. doi:10.1097/01.anes.0000296071.19434.1e
7. Yang T, Velagapudi R, Terrando N. Neuroinflammation after surgery: from mechanisms to therapeutic targets. Nat Immunol. 2020;21(11):1319–1326. doi:10.1038/s41590-020-00812-1
8. Guo Y, Li Y, Zhang Y, et al. Post-operative delirium associated with metabolic alterations following hemi-arthroplasty in older patients. Age Ageing. 2019;49(1):88–95. doi:10.1093/ageing/afz132
9. Liu Y, Song F, Yang Y, et al. Mitochondrial DNA methylation drift and postoperative delirium in mice. Eur J Anaesthesiol. 2022;39(2):133–144. doi:10.1097/EJA.0000000000001620
10. Learmonth ID, Young C, Rorabeck C. The operation of the century: total Hip replacement. Lancet. 2007;370(9597):1508–1519. doi:10.1016/S0140-6736(07)60457-7
11. Pivec R, Johnson AJ, Mears SC, Mont MA. Hip arthroplasty. Lancet. 2012;380(9855):1768–1777. doi:10.1016/S0140-6736(12)60607-2
12. Lee KH, Ha YC, Lee YK, Kang H, Koo KH. Frequency, risk factors, and prognosis of prolonged delirium in elderly patients after Hip fracture surgery. Clin Orthop Relat Res. 2011;469(9):2612–2620. doi:10.1007/s11999-011-1806-1
13. Bhushan S, Huang X, Duan Y, Xiao Z. The impact of regional versus general anesthesia on postoperative neurocognitive outcomes in elderly patients undergoing Hip fracture surgery: a systematic review and meta-analysis. Int J Surg. 2022;105:106854. doi:10.1016/j.ijsu.2022.106854
14. Krenk L, Kehlet H, Bæk Hansen T, Solgaard S, Soballe K, Rasmussen LS. Cognitive dysfunction after fast-track Hip and knee replacement. Anesth Analg. 2014;118(5):1034–1040. doi:10.1213/ANE.0000000000000194
15. Liao J, Li M, Huang C, et al. Pharmacodynamics and Pharmacokinetics of HSK3486, a Novel 2,6-Disubstituted Phenol Derivative as a General Anesthetic. Front Pharmacol. 2022;13:830791. doi:10.3389/fphar.2022.830791
16. Liu Z, Jin Y, Wang L, Huang Z. The Effect of Ciprofol on Postoperative Delirium in Elderly Patients Undergoing Thoracoscopic Surgery for Lung Cancer: a Prospective, Randomized, Controlled Trial. Drug Des Devel Ther. 2024;18:325–339. doi:10.2147/DDDT.S441950
17. Liang Z, Liu J, Chen S, et al. Postoperative quality of recovery comparison between ciprofol and propofol in total intravenous anesthesia for elderly patients undergoing laparoscopic major abdominal surgery: a randomized, controlled, double-blind, non-inferiority trial. J Clin Anesth. 2024;99:111660. doi:10.1016/j.jclinane.2024.111660
18. Yang Y, Xia Z, Xu C, Zhai C, Yu X, Li S. Ciprofol attenuates the isoproterenol-induced oxidative damage, inflammatory response and cardiomyocyte apoptosis. Front Pharmacol. 2022;13:1037151. doi:10.3389/fphar.2022.1037151
19. Liu X, Ren M, Zhang A, Huang C, Wang J. Nrf2 attenuates oxidative stress to mediate the protective effect of ciprofol against cerebral ischemia-reperfusion injury. Funct Integr Genomics. 2023;23(4):345. doi:10.1007/s10142-023-01273-z
20. Yang Y, Zhou D, Min S, et al. Ciprofol ameliorates ECS-induced learning and memory impairment by modulating aerobic glycolysis in the hippocampus of depressive-like rats. Pharmacol Biochem Behav. 2024;239:173775. doi:10.1016/j.pbb.2024.173775
21. Zhou L, Pinho R, Gu Y, Radak Z. The Role of SIRT3 in Exercise and Aging. Cells. 2022;11(16):2596. doi:10.3390/cells11162596
22. Diao Z, Ji Q, Wu Z, et al. SIRT3 consolidates heterochromatin and counteracts senescence. Nucleic Acids Res. 2021;49(8):4203–4219. doi:10.1093/nar/gkab161
23. Kim HS, Patel K, Muldoon-Jacobs K, et al. SIRT3 is a mitochondria-localized tumor suppressor required for maintenance of mitochondrial integrity and metabolism during stress. Cancer Cell. 2010;17(1):41–52. doi:10.1016/j.ccr.2009.11.023
24. Liu Y, Cheng A, Li YJ, et al. SIRT3 mediates hippocampal synaptic adaptations to intermittent fasting and ameliorates deficits in APP mutant mice. Nat Commun. 2019;10(1):1886. doi:10.1038/s41467-019-09897-1
25. Liu Q, Sun YM, Huang H, et al. Sirtuin 3 protects against anesthesia/surgery-induced cognitive decline in aged mice by suppressing hippocampal neuroinflammation. J Neuroinflammation. 2021;18(1):41. doi:10.1186/s12974-021-02089-z
26. Li S, Zhou Y, Hu H, et al. SIRT3 Enhances the Protective Role of Propofol in Postoperative Cognitive Dysfunction via Activating Autophagy Mediated by AMPK/mTOR Pathway. Front Biosci. 2022;27(11):303. doi:10.31083/j.fbl2711303
27. Shen T, Wu Y, Wang X, et al. Activating SIRT3 in peritoneal mesothelial cells alleviates postsurgical peritoneal adhesion formation by decreasing oxidative stress and inhibiting the NLRP3 inflammasome. Exp Mol Med. 2022;54(9):1486–1501. doi:10.1038/s12276-022-00848-3
28. Zhang J, Zhao Y, Wang S, Li G, Xu K. CREBH alleviates mitochondrial oxidative stress through SIRT3 mediating deacetylation of MnSOD and suppression of Nlrp3 inflammasome in NASH. Free Radic Biol Med. 2022;190:28–41. doi:10.1016/j.freeradbiomed.2022.07.018
29. Song S, Ding Y, Dai GL, et al. Sirtuin 3 deficiency exacerbates diabetic cardiomyopathy via necroptosis enhancement and NLRP3 activation. Acta Pharmacol Sin. 2021;42(2):230–241. doi:10.1038/s41401-020-0490-7
30. Gao J, Chen N, Li N, et al. Neuroprotective Effects of Trilobatin, a Novel Naturally Occurring Sirt3 Agonist from Lithocarpus polystachyus Rehd. Mitigate Cerebral Ischemia/Reperfusion Injury: involvement of TLR4/NF-κB and Nrf2/Keap-1 Signaling. Antioxid Redox Signal. 2020;33(2):117–143. doi:10.1089/ars.2019.7825
31. Luo Z, Tu H, Zhang X, et al. Efficacy and Safety of HSK3486 for Anesthesia/Sedation in Patients Undergoing Fiberoptic Bronchoscopy: a Multicenter, Double-Blind, Propofol-Controlled, Randomized, Phase 3 Study. CNS Drugs. 2022;36(3):301–313. doi:10.1007/s40263-021-00890-1
32. Athanassoglou V, Cozowicz C, Zhong H, et al. Association of perioperative midazolam use and complications: a population-based analysis. Reg Anesth Pain Med. 2022;47(4):228–233. doi:10.1136/rapm-2021-102989
33. Ren A, Zhang N, Zhu H, Zhou K, Cao Y, Liu J. Effects of Preoperative Anxiety on Postoperative Delirium in Elderly Patients Undergoing Elective Orthopedic Surgery: a Prospective Observational Cohort Study. Clin Interv Aging. 2021;16:549–557. doi:10.2147/CIA.S300639
34. Li W-X, Luo R-Y, Chen C, et al. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: a randomized controlled preliminary trial. Chin Med J. 2019;132(4):437–445. doi:10.1097/CM9.0000000000000098
35. Miller D, Lewis SR, Pritchard MW, et al. Intravenous versus inhalational maintenance of anaesthesia for postoperative cognitive outcomes in elderly people undergoing non-cardiac surgery. Cochrane Database Syst Rev. 2018;8(8):Cd012317. doi:10.1002/14651858.CD012317.pub2
36. Geng YJ, Wu QH, Zhang RQ. Effect of propofol, sevoflurane, and isoflurane on postoperative cognitive dysfunction following laparoscopic cholecystectomy in elderly patients: a randomized controlled trial. J Clin Anesth. 2017;38:165–171. doi:10.1016/j.jclinane.2017.02.007
37. Ding XW, Sun X, Shen XF, et al. Propofol attenuates TNF-α-induced MMP-9 expression in human cerebral microvascular endothelial cells by inhibiting Ca(2+)/CAMK II/ERK/NF-κB signaling pathway. Acta Pharmacol Sin. 2019;40(10):1303–1313. doi:10.1038/s41401-019-0258-0
38. Xu Z, Lu Y, Wang J, Ding X, Chen J, Miao C. The protective effect of propofol against TNF-α-induced apoptosis was mediated via inhibiting iNOS/NO production and maintaining intracellular Ca(2+) homeostasis in mouse hippocampal HT22 cells. Biomed Pharmacother. 2017;91:664–672. doi:10.1016/j.biopha.2017.04.110
39. Ren G, Zhou Y, Liang G, et al. General Anesthetics Regulate Autophagy via Modulating the Inositol 1,4,5-Trisphosphate Receptor: implications for Dual Effects of Cytoprotection and Cytotoxicity. Sci Rep. 2017;7(1):12378. doi:10.1038/s41598-017-11607-0
40. Yuan Y, Yuan L, Yang J, et al. Autophagy-deficient macrophages exacerbate cisplatin-induced mitochondrial dysfunction and kidney injury via miR-195a-5p-SIRT3 axis. Nat Commun. 2024;15(1):4383. doi:10.1038/s41467-024-47842-z
41. Phillips AT, Deiner S, Mo Lin H, Andreopoulos E, Silverstein J, Levin MA. Propofol Use in the Elderly Population: prevalence of Overdose and Association With 30-Day Mortality. Clin Ther. 2015;37(12):2676–2685. doi:10.1016/j.clinthera.2015.10.005
42. Wijnberge M, Geerts BF, Hol L, et al. Effect of a Machine Learning-Derived Early Warning System for Intraoperative Hypotension vs Standard Care on Depth and Duration of Intraoperative Hypotension During Elective Noncardiac Surgery: the HYPE Randomized Clinical Trial. JAMA. 2020;323(11):1052–1060. doi:10.1001/jama.2020.0592
43. Liang P, Dai M, Wang X, et al. Efficacy and safety of ciprofol vs. propofol for the induction and maintenance of general anaesthesia: a multicentre, single-blind, randomised, parallel-group, phase 3 clinical trial. Eur J Anaesthesiol. 2023;40(6):399–406. doi:10.1097/EJA.0000000000001799
44. Duan G, Lan H, Shan W, et al. Clinical effect of different doses of ciprofol for induction of general anesthesia in elderly patients: a randomized, controlled trial. Pharmacol Res Perspect. 2023;11(2):e01066. doi:10.1002/prp2.1066
45. Li X, Yang D, Li Q, et al. Safety, Pharmacokinetics, and Pharmacodynamics of a Single Bolus of the γ-aminobutyric Acid (GABA) Receptor Potentiator HSK3486 in Healthy Chinese Elderly and Non-elderly. Front Pharmacol. 2021;12:735700. doi:10.3389/fphar.2021.735700
46. Gan TJ, Bertoch T, Habib AS, et al. Comparison of the Efficacy of HSK3486 and Propofol for Induction of General Anesthesia in Adults: a Multicenter, Randomized, Double-blind, Controlled, Phase 3 Noninferiority Trial. Anesthesiology. 2024;140(4):690–700. doi:10.1097/ALN.0000000000004886
47. Picard P, Tramèr MR. Prevention of pain on injection with propofol: a quantitative systematic review. Anesth Analg. 2000;90(4):963–969. doi:10.1097/00000539-200004000-00035
48. Euasobhon P, Dej-Arkom S, Siriussawakul A, et al. Lidocaine for reducing propofol-induced pain on induction of anaesthesia in adults. Cochrane Database Syst Rev. 2016;2(2):Cd007874. doi:10.1002/14651858.CD007874.pub2
49. Tan CH, Onsiong MK. Pain on injection of propofol. Anaesthesia. 1998;53(5):468–476. doi:10.1046/j.1365-2044.1998.00405.x
50. Qin L, Ren L, Wan S, et al. Design, Synthesis, and Evaluation of Novel 2,6-Disubstituted Phenol Derivatives as General Anesthetics. J Med Chem. 2017;60(9):3606–3617. doi:10.1021/acs.jmedchem.7b00254
51. Ainiwaer D, Jiang W. Efficacy and safety of ciprofol versus propofol for anesthesia induction in adult patients received elective surgeries: a meta‑analysis. BMC Anesthesiology. 2024;24(1):93. doi:10.1186/s12871-024-02479-9
52. Lu YF, Wu JM, Lan HY, Xu QM, Shi SQ, Duan GC. Efficacy and Safety of General Anesthesia Induction with Ciprofol in Hip Fracture Surgery of Elderly Patients: a Randomized Controlled Trial. Drug Des Devel Ther. 2024;18:3951–3958. doi:10.2147/DDDT.S475176
53. Hirsch J, DePalma G, Tsai TT, Sands LP, Leung JM. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery. Br J Anaesth. 2015;115(3):418–426. doi:10.1093/bja/aeu458
54. Ansari A, Rahman MS, Saha SK, Saikot FK, Deep A, Kim KH. Function of the SIRT3 mitochondrial deacetylase in cellular physiology, cancer, and neurodegenerative disease. Aging Cell. 2017;16(1):4–16. doi:10.1111/acel.12538
55. Zhao H, Fan M, Zhang J, Gao Y, Chen L, Huang L. Amyloid beta-induced mitochondrial dysfunction and endothelial permeability in cerebral microvascular endothelial cells: the protective role of dexmedetomidine. Brain Res Bull. 2025;220:111137. doi:10.1016/j.brainresbull.2024.111137
56. Liu X, Xie X, Li D, et al. Sirt3-dependent regulation of mitochondrial oxidative stress and apoptosis contributes to the dysfunction of pancreatic islets after severe burns. Free Radic Biol Med. 2023;198:59–67. doi:10.1016/j.freeradbiomed.2023.01.027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.