Back to Journals » Clinical Ophthalmology » Volume 10
Effect of benzalkonium chloride-free latanoprost ophthalmic solution on ocular surface in patients with glaucoma
Authors Walimbe T, Chelerkar V, Bhagat P, Joshi A, Raut A
Received 22 December 2015
Accepted for publication 16 March 2016
Published 9 May 2016 Volume 2016:10 Pages 821—827
DOI https://doi.org/10.2147/OPTH.S102976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Tejaswini Walimbe,1 Vidya Chelerkar,2 Purvi Bhagat,3 Abhijeet Joshi,4 Atul Raut4
1Walimbe Eye Clinic, 2PBMA’s H.V. Desai Eye Hospital, Pune, 3Glaucoma Clinic, M and J Western Regional Institute of Ophthalmology, Civil Hospital, Ahmedabad, 4Clinical Research Department, Sun Pharma Advanced Research Company Ltd., Mumbai, India
Introduction: Benzalkonium chloride (BAK), included as a preservative in many topical treatments for glaucoma, induces significant toxicity and alters tear breakup time (TBUT). BAK-containing latanoprost, an ester prodrug of prostaglandin F2a, can cause ocular adverse events (AEs) associated with BAK. The purpose of this study was to evaluate the efficacy and safety of BAK-free latanoprost.
Patients and methods: A prospective, open-label, single-arm, multicenter, 8-week study in patients with primary open-angle glaucoma or ocular hypertension taking BAK-containing latanoprost for ≥12 months was performed. Patients were switched to BAK-free latanoprost ophthalmic solution 0.005% administered once daily, and eyes were assessed after 28 and 56 days. Primary efficacy and safety variables were TBUT and treatment-emergent AEs, respectively.
Results: At day 56, 40 eyes were evaluable. Mean TBUT increased significantly from baseline (3.67±1.60 seconds) to 5.03±2.64 and 6.06±3.39 seconds after 28 and 56 days of treatment with BAK-free latanoprost (P<0.0001). Ocular Surface Disease Index© (OSDI©) score also decreased significantly to 12.06±13.40 and 7.06±10.75 at 28 and 56 days, respectively, versus baseline (18.09±18.61, P<0.0001). In addition, inferior corneal staining score decreased significantly to 0.53 from baseline (0.85, P=0.0033). A reduction in conjunctival hyperemia and intraocular pressure was observed at both time points. No treatment-related serious AEs were evident and 12 (26.08%) treatment-emergent AEs occurred in seven patients, with eye pain and irritation being the most frequent. No clinically significant changes in vital signs or slit lamp examinations were observed.
Conclusion: Results indicate that switching from BAK-containing latanoprost to BAK-free latanoprost resulted in significant improvements in TBUT, OSDI© score, and inferior corneal staining score, and measurable reductions in conjunctival hyperemia score. Furthermore, BAK-free latanoprost was well tolerated with only mild-to-moderate and self-limiting AEs. BAK-free latanoprost appears to be effective in protecting ocular surface integrity in glaucoma patients but further studies are needed to confirm this beneficial effect.
Keywords: tear breakup time, TBUT, Ocular Surface Disease Index, OSDI©, inferior corneal staining score, conjunctival hyperemia, intraocular pressure, glaucoma, ocular surface
Introduction
Glaucoma is a chronic, progressive disease that cannot be cured, but can only be controlled by adequate and appropriate prolonged, and sometimes lifelong, treatment. The most effective drugs for increasing outflow of aqueous humor, and thus reducing intraocular pressure (IOP), are the PGF2α analogs.1,2 For most patients suffering from glaucoma and ocular hypertension, pharmacologic therapy with topical PGF2α analogs, which are powerful ocular hypotensive agents, remains the primary intervention.2
In the majority of IOP-lowering products, the concentration of benzalkonium chloride (BAK) ranges from 0.004% to 0.02% in different solutions. At these concentrations, patients with dry eyes or those using medication with frequent dosing may be at risk of experiencing the adverse effects of BAK.3
Results from a number of studies have indicated that chronic application of eye drops induces significant cytological and histological impairment in ocular tissues, and the preservatives are the main components responsible for these observed changes.4–7 Prostaglandin analog preparations are often preserved with BAK. BAK disrupts the lipid layer that normally spreads over the watery lacrimal film and reduces the evaporation rate from the corneal surface. BAK, a cationic detergent, may solubilize the thin lipid layer, thereby permitting free evaporation of water and hence drying. BAK may also encourage dissolution of the conjunctival mucin layer adsorbed on the surface of the corneal epithelium, resulting in an increase in surface tension at the epithelial surface causing the tear film to retract from the affected areas, which then appears as dry spots.8
BAK destabilizes the tear film indirectly by decreasing the density of goblet cells in the conjunctival epithelium, compromising the ability of the tear film to provide protection and trophic factors to the cornea. Histopathological and impression cytology studies have demonstrated inflammation, squamous metaplasia, and subconjunctival fibrosis in the conjunctiva and Tenon’s capsule associated with the use of topical preservatives. These side effects are dose-dependent and increase with frequency of instillation.7
BAK is degraded to hydrogen peroxide and has been shown to damage ocular tissue by inducing apoptosis and increasing the concentrations of inflammatory markers.9 Furthermore, BAK alters tear film quality and tear breakup time (TBUT) and leads to ocular surface diseases. Studies of conjunctival biopsy specimens indicate that the conjunctiva is significantly infiltrated by inflammatory cells, fibroblasts, or both in multitreated patients.10
Latanoprost, an ester prodrug of PGF2α, was the first of the currently available topical PGF2α analogs to be approved for glaucoma or ocular hypertension and is still widely used around the world.11 In common with other PG therapies, latanoprost can cause ocular adverse events (AEs) associated with BAK. An improved BAK-free latanoprost ophthalmic solution has been developed and shown to have similar efficacy in reducing IOP compared with the BAK-containing latanoprost ophthalmic solution, but with improved tolerability.12 We conducted a study in which patients using BAK-containing latanoprost were switched to BAK-free latanoprost to quantify the changes in TBUT, inferior corneal staining score, Ocular Surface Disease Index© (OSDI©) score, and IOP. The results are reported in this manuscript.
Materials and methods
Study design and population
This study was registered with the Clinical Trials Registry – India. CTRI number: CTRI/2010/091/002822. This was a prospective, open-label, single-arm, multicenter, 8-week study and included three clinic visits. Men and women ≥18 years of age with primary open-angle glaucoma or ocular hypertension with TBUT <6 seconds who were taking any clinically available form of BAK-containing latanoprost ophthalmic solution 0.005% monotherapy for at least 12 months were recruited. The study was approved by the Ethics Committee of H.V. Desai Eye Hospital, the Ethics Committee of M and J Institute of Ophthalmology, and the Indian National Ethics Committee. All patients gave their written informed consent to participate in the study. Patients meeting eligibility criteria (Table 1) were switched to BAK-free latanoprost ophthalmic solution 0.005% (Sun Pharma Advanced Research Company Ltd., Mumbai, India). On visit 1 (day 0, screening), patients were dispensed BAK-free latanoprost ophthalmic solution 0.005% and subsequently instilled one drop once daily in the evening for 56 days in one or both eyes as per inclusion criteria. Safety and efficacy evaluations were performed at follow-up visits 2 (day 28) and 3 (day 56).
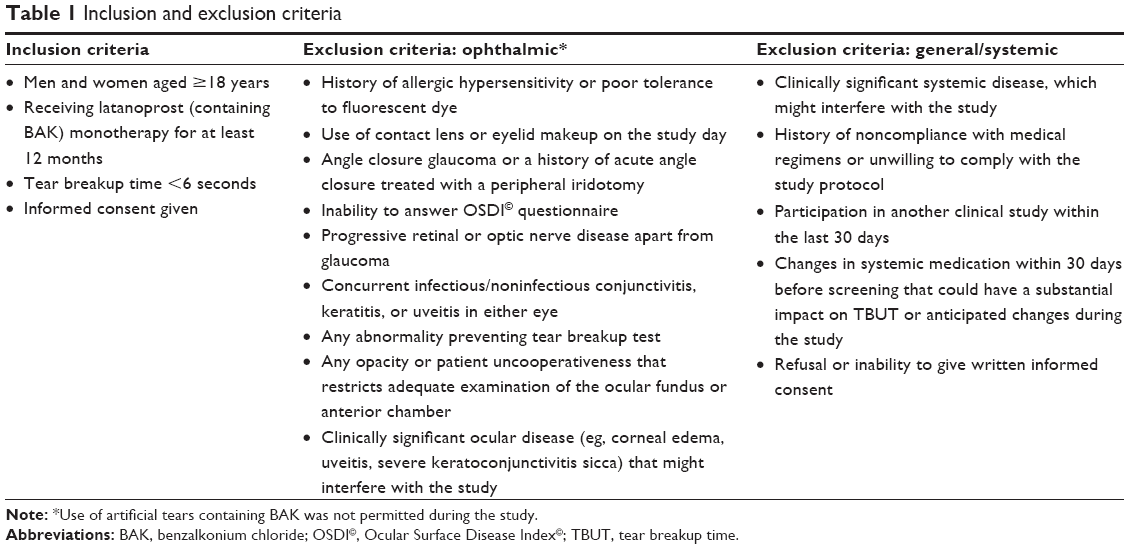 | Table 1 Inclusion and exclusion criteria |
Study assessments
Efficacy
The primary efficacy variable was TBUT, which was evaluated in seconds at visits 2 and 3 (days 28 and 56, respectively). Secondary efficacy variables included inferior corneal staining score, which was measured on a scale of 0–4 (0= none, 1= mild, 2= moderate, 3= severe, 4= confluent); OSDI© (copyright Allergan, Inc., Irvine, CA, USA) 12-item patient-reported outcome questionnaire score (defines ocular surface as normal [0–12 points], mild [13–22 points], moderate [23–32 points], or severe [33–100 points]);13 conjunctival hyperemia grading using a 4-point scale ranging from 0 to 3 units (0= none, 1= mild, 2= moderate, 3= severe); and IOP, which was measured by Goldmann applanation tonometer from baseline at visits 2 (day 28) and 3 (day 56).
Safety
The primary safety variable was treatment-emergent AEs reported by each patient and classified using the Medical Dictionary for Regulatory Activities (MedDRA) system organ class and preferred term. The secondary safety variable was vital sign measurements.
Statistical analysis
Efficacy data were presented descriptively as sample number, mean, and standard deviation. Efficacy was assessed in the intent-to-treat population with last observation carried forward, which included all enrolled patients who had a baseline visit assessment, received at least one dose of study medication, and had at least one on-therapy efficacy assessment, and in the per-protocol population, which included all enrolled patients who received at least one dose of the study medication, had at least one posttreatment assessment, and no major protocol violation. Safety data were evaluated from all patients who received at least one dose of study medication (the safety population).
In this single-arm study, mean changes from baseline from day 0 to day 28 and day 0 to day 56 were analyzed using the paired t-test to check whether the mean of the differences between paired samples differed from baseline to postbaseline assessment. A P-value of 0.05 was considered statistically significant.
Results
Patient disposition
A total of 46 eyes were enrolled in the study at three sites in India. Six eyes were prematurely terminated from the study and four eyes were lost to follow-up. One patient (two eyes) was excluded from the per-protocol population (n=34 eyes) due to a discrepancy in study medication dispensing.
The intent-to-treat population included 40 eyes at days 28 and 56. The safety analysis, performed in all enrolled patients who received at least one dose of study medication, included 46 eyes. Patient demographics and disposition are summarized in Table 2. At baseline, patient eyes had been treated with BAK-containing latanoprost for a mean (standard deviation) of 1.94 years (±1.0). Ophthalmic evaluation of the eyes before treatment is detailed in Table 3.
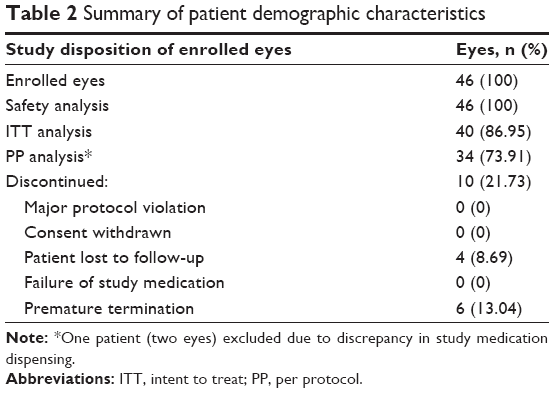 | Table 2 Summary of patient demographic characteristics |
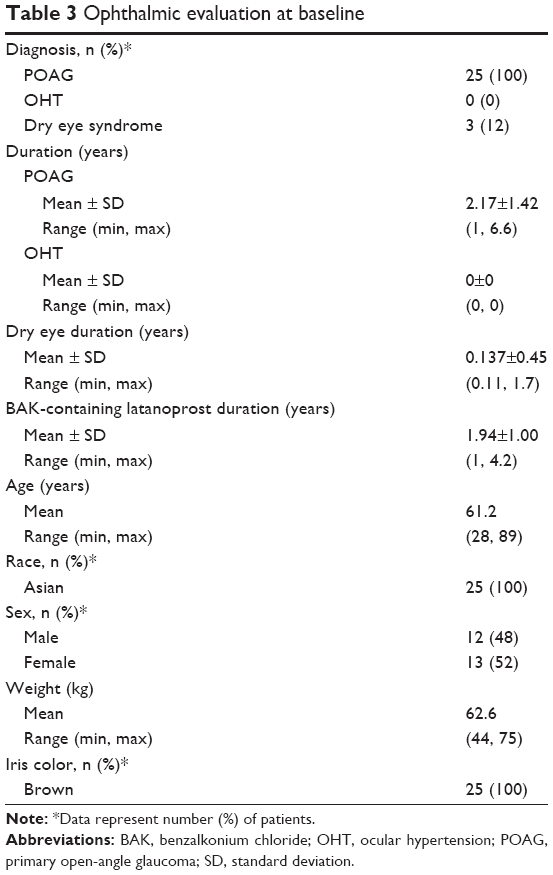 | Table 3 Ophthalmic evaluation at baseline |
Efficacy
Results for the intent-to-treat population (last observation carried forward) are presented later in the “Results” section.
TBUT evaluation
Mean TBUT at the baseline visit was 3.67±1.60 seconds and increased to 5.03±2.64 seconds after 28 days of treatment, and to 6.06±3.39 seconds after 56 days of treatment with BAK-free latanoprost. At both days 28 and 56, these mean changes from baseline were statistically significant (both P<0.0001) with measurable clinical improvement observed in TBUT (Figure 1).
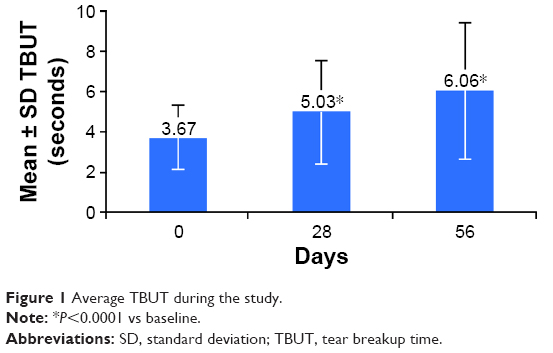 | Figure 1 Average TBUT during the study. |
OSDI© evaluation
The mean OSDI© score at the baseline visit was within the mild category at 18.09±18.61, which decreased to 12.06±13.40 after 28 days of treatment (P=0.0001), and fell to within the normal category at 7.06±10.75 after 56 days of treatment (P<0.0001) with BAK-free latanoprost, indicating a statistically significant change from baseline and measurable clinical improvement in OSDI© score at both visits (Figure 2).
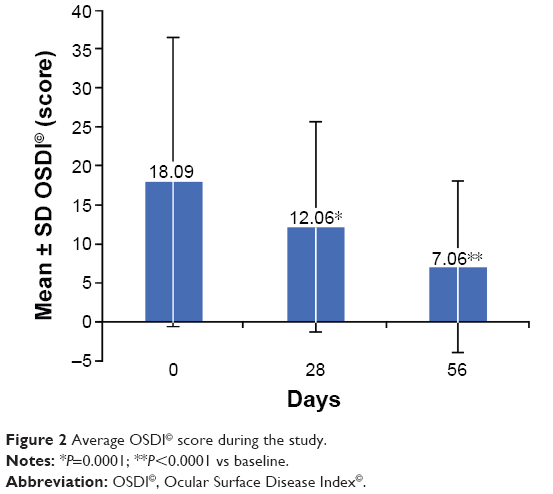 | Figure 2 Average OSDI© score during the study. |
Inferior corneal staining
The mean inferior corneal staining score at baseline was 0.85±0.69, which decreased to 0.68±0.62 after 28 days of treatment (P=0.0701), and significantly decreased to 0.53±0.60 after 56 days of treatment (P=0.0033) with BAK-free latanoprost.
Conjunctival hyperemia
The mean conjunctival hyperemia score was 0.48±0.75 at baseline, which decreased to 0.33±0.52 after 28 days of treatment and to 0.35±0.48 after 56 days of treatment with BAK-free latanoprost, but did not reach statistical significance for either assessment.
Intraocular pressure
The mean IOP was 14.43±3.55 mmHg at the baseline visit, 13.73±4.0 mmHg after 28 days of treatment, and 13.70±4.26 mmHg after 56 days of treatment, indicating no statistically significant change.
Safety
All 46 eyes enrolled were evaluated as part of the safety analysis. No treatment-related serious AEs were observed during the study. In total, 12 (26.08%) treatment-emergent AEs, including eight ocular and four nonocular, were reported in seven patients. The most frequently reported AE was eye pain experienced in three eyes (6.52%), followed by eye irritation in two eyes (4.34%). Table 4 summarizes the AEs by the MedDRA system organ class and preferred term. Overall, three patients (with six eyes) discontinued the study because of an AE; of these, two patients discontinued because of an ocular AE and one patient discontinued because of a nonocular AE.
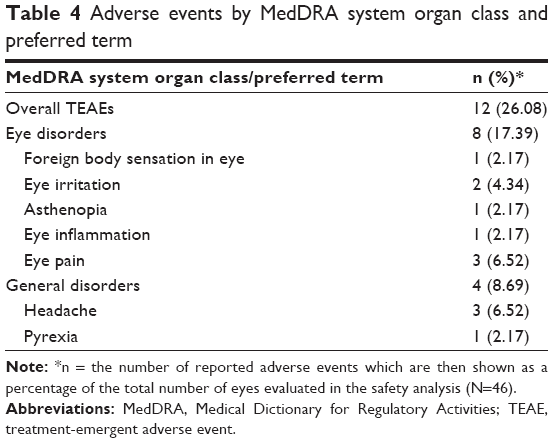 | Table 4 Adverse events by MedDRA system organ class and preferred term |
No clinically significant change in vital signs was observed from baseline (day 0) to the end-of-study visit (day 56). In addition, there was no clinically significant change in slit-lamp examination from baseline (day 0) to the end-of-study visit (day 56).
Discussion
The deleterious effects of BAK have been well documented, most notably its effects on the ocular surface. Common side effects include conjunctival hyperemia, decreased tear production, tear film instability, and superficial punctate keratitis.
Short-term exposure to BAK alters the precorneal mucin, which is important in maintaining the integrity of the tear film.14 BAK reduces TBUT,15 which contributes to dry eye, reduces the rate of removal of other noxious substances, and counteracts the protective effects of tears to the cornea. Particularly with chronic exposure, BAK also disrupts the corneal epithelial barrier16 and produces significant infiltration by inflammatory cells in the conjunctival stroma close to the limbus,10 thus compromising the epithelial barrier and resulting in corneal damage and conjunctival cell infiltration.17
In an ophthalmic product formulation, BAK has several positive attributes, but can also cause dose-dependent detrimental effects on healthy ocular tissue. At a BAK concentration of 0.0001%, arrest of cellular growth takes place.18 A BAK concentration of 0.01% induces cellular apoptosis and at a concentration of 0.05%–0.1%, necrosis occurs.19 Therefore, the inherent detergent properties of BAK disrupt the lipid layer of the tear film, resulting in increased aqueous tear evaporation and decreased TBUT.20
The corneal neurotoxicity of topical BAK 0.01% or 0.1% solution has been studied on the corneal nerves of Thy 1-YFP+ neurofluorescent mouse eyes.21 Corneas treated with BAK showed significantly lower nerve fiber density and aqueous tear production together with increased inflammatory cell infiltration and fluorescein staining after 1 week, especially with 0.1% BAK treatment. Two forms of BAK-induced neurotoxicity were observed – reversible neurotoxicity characterized by axonopathy and recovery, and irreversible neurotoxicity (nerve degeneration and regeneration). Furthermore, nerve fiber length was reduced by both concentrations of BAK.
BAK is associated with a decrease in density of goblet cells resulting in decreased mucin production and decreased tear film stability. Together, these effects on tear film contribute to dry eye symptoms and ocular discomfort in glaucoma patients who already experience a decreased rate of basal tear turnover. Even in patients who do not experience discomfort, signs of tear film instability and corneal epithelial damage can be found.20
The BAK detergent property allows it to solubilize the corneal epithelium and promote penetration of the active drug and preservative itself, thus accumulating in ocular tissue. Therefore, reducing preservative load is of vital importance in patients on long-term topical therapy.20
In our study, patients with a baseline TBUT <6 seconds who had been treated with BAK-containing latanoprost 0.005% for at least 12 months were switched to BAK-free latanoprost ophthalmic solution 0.005%. Significant improvements were observed in mean TBUT, mean OSDI© questionnaire score, and mean inferior corneal staining score after 56 days of BAK-free latanoprost. The OSDI© questionnaire was used as it is a valid and reliable method to quantify dry eye syndrome.22 There was also a nonsignificant decrease in conjunctival hyperemia score and IOP with BAK-free latanoprost. BAK-free latanoprost was well tolerated with treatment-related AEs being mild-to-moderate and self-limiting in nature.
Our results with BAK-free latanoprost are similar to those reported previously.4,7 Using quality-of-life questionnaires, Rossi et al4 found that risk factors for the development of ocular surface disease in 233 patients treated for glaucoma with IOP-lowering drugs included the number and prolonged use of medications and total exposure to BAK. A prospective epidemiological survey of 4,107 patients with chronic open-angle glaucoma also found that the incidence of ocular toxicity was reduced and a significant reduction in symptoms occurred when patients were treated with preservative-free eye drops.7 Assessments of 20 patients with glaucoma (40 eyes) who switched from latanoprost with 0.02% BAK to travoprost with sofZia™ (borate, zinc, and sorbitol) showed that the discontinuation of BAK led to a statistically significant increase in TBUT (P<0.001) and a decrease in mean inferior corneal staining score and mean OSDI© in patients with low TBUT scores (both P<0.001).23 These results confirmed that BAK may increase OSDI© by disrupting the tear film and increasing conjunctival inflammation.
In a study comparing a once-daily BAK-free fixed-dose combination of 0.005% latanoprost plus 0.5% timolol with both drugs administered separately (same concentrations as the combination) in 227 patients with open-angle glaucoma or ocular hypertension, the fixed-dose combination of latanoprost and timolol had similar IOP-lowering efficacy to the drugs administered concomitantly and significantly better IOP-lowering efficacy compared with either drug as monotherapy.24 Furthermore, there was no difference in AEs between the treatment groups. The results of our study confirm that switching from BAK-containing latanoprost to BAK-free latanoprost can maintain IOP-lowering efficacy while reducing ocular side effects.
Attempts to reduce overall BAK load for patients are important. BAK-free latanoprost is a good option for patients with ocular surface disease, patients who are on long-term therapy, or those who do not tolerate the effects of BAK because of discomfort, and may help to improve compliance.
Conclusion
Switching from BAK-containing latanoprost to BAK-free latanoprost resulted in significant improvements in TBUT, OSDI© score, and inferior corneal staining score, and measurable reductions in conjunctival hyperemia score. Furthermore, BAK-free latanoprost was well tolerated with only mild-to-moderate and self-limiting AEs. BAK-free latanoprost appears to be effective in protecting ocular surface integrity in patients with glaucoma. Further studies are needed to confirm this beneficial effect.
Acknowledgments
The authors thank Santosh Kumar from JSS Medical Research India Ltd for performing the statistical analyses; and Ray Ashton and Diane Kwiatkoski of Quintiles, for their editorial assistance in the preparation of this manuscript, which was funded by Sun Pharma Advanced Research Company Ltd. Sponsorship for this study and article processing charges were funded by Sun Pharma Advanced Research Company Ltd.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Tejaswini Walimbe, Vidya Chelerkar, and Purvi Bhagat have received research grants and nonfinancial support from Sun Pharma Advanced Research Company Ltd., Mumbai, India. Abhijeet Joshi and Atul Raut are employees of Sun Pharma Advanced Research Company Ltd., which funded this study. The authors report no other conflicts of interest in this work.
References
Ting NS, Li Yim JF, Ng JY. Different strategies and cost-effectiveness in the treatment of primary open angle glaucoma. Clinicoecon Outcomes Res. 2014;6:523–530. | ||
Toris CB, Gabelt BT, Kaufman PL. Update on the mechanism of action of topical prostaglandins for intraocular pressure reduction. Surv Ophthalmol. 2008;53 Suppl 1:S107–S120. | ||
Freeman PD, Kahook MY. Preservatives in topical ophthalmic medications: historical and clinical perspectives. Expert Rev Ophthalmol. 2009;4(1):59–64. | ||
Rossi GC, Pasinetti GM, Scudeller L, Raimondi M, Lanteri S, Bianchi PE. Risk factors to develop ocular surface disease in treated glaucoma or ocular hypertension patients. Eur J Ophthalmol. 2013;23(3):296–302. | ||
Baudouin C. Detrimental effect of preservatives in eyedrops: implications for the treatment of glaucoma. Acta Ophthalmol. 2008;86(7):716–726. | ||
Jaenen N, Baudouin C, Pouliquen P, Manni G, Figueiredo A, Zeyen T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341–349. | ||
Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86(4):418–423. | ||
Wilson WS, Duncan AJ, Jay JL. Effect of benzalkonium chloride on the stability of the precorneal tear film in rabbit and man. Br J Ophthalmol. 1975;59(11):667–669. | ||
Epstein SP, Chen D, Asbell PA. Evaluation of biomarkers of inflammation in response to benzalkonium chloride on corneal and conjunctival epithelial cells. J Ocul Pharmacol Ther. 2009;25(5):415–424. | ||
Baudouin C, Pisella PJ, Fillacier K, et al. Ocular surface inflammatory changes induced by topical antiglaucoma drugs: human and animal studies. Ophthalmology. 1999;106(3):556–563. | ||
Alm A. Latanoprost in the treatment of glaucoma. Clin Ophthalmol. 2014;8:1967–1985. | ||
Rouland JF, Traverso CE, Stalmans I, et al. Efficacy and safety of preservative-free latanoprost eyedrops, compared with BAK-preserved latanoprost in patients with ocular hypertension or glaucoma. Br J Ophthalmol. 2013;97(2):196–200. | ||
Miller KL, Walt JG, Mink DR, et al. Minimal clinically important difference for the ocular surface disease index. Arch Ophthalmol. 2010;128(1):94–101. | ||
Chung SH, Lee SK, Cristol SM, et al. Impact of short-term exposure of commercial eyedrops preserved with benzalkonium chloride on precorneal mucin. Mol Vis. 2006;12:415–421. | ||
Baudouin C, de Lunardo C. Short-term comparative study of topical 2% carteolol with and without benzalkonium chloride in healthy volunteers. Br J Ophthalmol. 1998;82(1):39–42. | ||
Ishibashi T, Yokoi N, Kinoshita S. Comparison of the short-term effects on the human corneal surface of topical timolol maleate with and without benzalkonium chloride. J Glaucoma. 2003;12(6):486–490. | ||
Noecker RJ, Herrygers LA, Anwaruddin R. Corneal and conjunctival changes caused by commonly used glaucoma medications. Cornea. 2004;23(5):490–496. | ||
Tsai JH, Derby E, Holland EJ, Khatana AK. Incidence and prevalence of glaucoma in severe ocular surface disease. Cornea. 2006;25(5):530–532. | ||
De Saint JM, Brignole F, Bringuier AF, Bauchet A, Feldmann G, Baudouin C. Effects of benzalkonium chloride on growth and survival of Chang conjunctival cells. Invest Ophthalmol Vis Sci. 1999;40(3):619–630. | ||
Rosin LM, Bell NP. Preservative toxicity in glaucoma medication: clinical evaluation of benzalkonium chloride-free 0.5% timolol eye drops. Clin Ophthalmol. 2013;7:2131–2135. | ||
Sarkar J, Chaudhary S, Namavari A, et al. Corneal neurotoxicity due to topical benzalkonium chloride. Invest Ophthalmol Vis Sci. 2012;53(4):1792–1802. | ||
Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118(5):615–621. | ||
Horsley MB, Kahook MY. Effects of prostaglandin analog therapy on the ocular surface of glaucoma patients. Clin Ophthalmol. 2009;3:291–295. | ||
Bhagat P, Sodimalla K, Paul C, et al. Efficacy and safety of benzalkonium chloride-free fixed-dose combination of latanoprost and timolol in patients with open-angle glaucoma or ocular hypertension. Clin Ophthalmol. 2014;8:1241–1252. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.