Back to Journals » Clinical Ophthalmology » Volume 20
Effect of Anesthesia Technique on the Postoperative Rotational Stability of Toric Intraocular Lenses
Authors Liu M ![]() , Cao G, Ge J, Huang Y, Liu X
, Cao G, Ge J, Huang Y, Liu X
Received 29 October 2025
Accepted for publication 19 January 2026
Published 5 February 2026 Volume 2026:20 577701
DOI https://doi.org/10.2147/OPTH.S577701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Min Liu,1,2 Guangliang Cao,2 Jiajia Ge,2 Yusen Huang,2 Xiaomin Liu1,2
1State Key Laboratory Cultivation Base, Shandong Key Laboratory of Eye Diseases, School of Ophthalmology, Shandong First Medical University, Qingdao, Shandong, People’s Republic of China; 2Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, Qingdao, Shandong, People’s Republic of China
Correspondence: Xiaomin Liu, Eye Institute of Shandong First Medical University, Qingdao, 266071, People’s Republic of China, Email [email protected]
Purpose: To compare the effects of topical versus peribulbar anesthesia on the early rotational stability of toric intraocular lenses (Toric IOLs).
Patients and Methods: In this prospective cohort study, 240 eyes undergoing phacoemulsification with Toric IOL implantation at Qingdao Eye Hospital were analyzed. Preoperative ocular parameters were recorded. Postoperative outcomes at 1 day, 1 week, and 1 month included Toric IOL rotation, uncorrected distance visual acuity (UDVA), residual astigmatism, intraocular pressure, and the rate of IOL repositioning. Binary logistic regression identified factors associated with repositioning.
Results: Baseline characteristics were similar between groups. On day 1, mean IOL rotation was significantly lower in the peribulbar group (3.61 ± 2.53°) than in the topical group (4.65 ± 5.40°, P=0.003), and UDVA was better (P=0.046). At 1 week, rotation remained smaller in the peribulbar group (P=0.040). By 1 month, no significant differences were found in rotation, UDVA, or residual astigmatism. Repositioning occurred in 1/112 (0.9%) peribulbar and 8/116 (6.9%) topical cases (P=0.034). Logistic regression confirmed anesthesia type as an independent factor for repositioning (P=0.045).
Conclusion: Peribulbar anesthesia enhances early postoperative rotational stability of Toric IOLs and reduces the need for repositioning.
Keywords: Toric IOL, cataract surgery, repositioning, rotational stability, anesthesia
Introduction
Cataract remains one of the leading causes of blindness worldwide, and phacoemulsification with intraocular lens (IOL) implantation is currently the only effective treatment. With rising patient expectations for postoperative visual quality, cataract surgery has shifted from simply restoring vision to achieving optimal refractive outcomes. Corneal astigmatism is a major limiting factor for postoperative uncorrected visual acuity and overall visual quality. Multiple studies reported that approximately 40–47% of cataract surgery candidates have preoperative corneal astigmatism ≥ 1.0 diopters (D),1–3 indicating that a substantial proportion of patients may benefit from simultaneous astigmatic correction.
Since the early 2000s, Toric IOL have become a preferred option for correcting corneal astigmatism during cataract surgery, offering a broader correction range, improved predictability, and greater postoperative stability than corneal or limbal relaxing incisions.4–8 The effectiveness of Toric IOL depends critically on precise alignment between the IOL cylinder axis and the corneal steep meridian; each 1° of off-axis rotation is associated with an approximate 3–3.3% loss of astigmatic correction, and rotations approaching 30° can essentially abolish the corrective effect.9–11 Consequently, rotational stability is a key determinant of refractive success. Factors reported to influence Toric IOL stability include axial length, capsular bag fibrosis, IOL material and haptic design, and surgical technique—for example, a continuous curvilinear capsulorhexis with a diameter of 5.0–5.8 mm is generally recommended.12–15
Previous studies have indicated that the risk of Toric IOL rotation is highest within the first day to one week after surgery, a period during which ocular motility is considered a key contributing factor.16–20 It is therefore hypothesized that restricting eye movement in this early postoperative phase may enhance the early stability of the toric IOL.
In cataract surgery, Peribulbar and topical anesthesia are the two most commonly used local anesthesia techniques. Although numerous studies have compared their differences in surgical analgesia, patient comfort, and short-term complications,21 the influence of anesthesia method on Toric IOL rotational stability has not been systematically evaluated. The pharmacological mechanisms of these two techniques are fundamentally distinct: topical anesthesia provides only intraoperative surface analgesia, whereas peribulbar anesthesia additionally induces reversible akinesia. More importantly, the duration of action of local anesthetic agents varies significantly. The combination of a short-acting agent (lidocaine) with a long-acting one (ropivacaine) can markedly prolong the recovery time of postoperative ocular motility. This extended period of akinesia may overlap with the high-risk phase of greatest Toric IOL instability, potentially influencing its rotational stability.
However, a significant gap exists in the current literature regarding this specific issue. Therefore, this study proposes the central hypothesis that, compared to topical anesthesia using 0.5% proparacaine hydrochloride alone, a standardized peribulbar anesthesia employing a long-acting mixture (2% lidocaine combined with 1% ropivacaine) will significantly reduce the magnitude of toric IOL rotation during the critical postoperative period by prolonging postoperative akinesia, thereby achieving better axial stability and visual outcomes. To test this hypothesis, we designed a prospective cohort study to systematically compare the effects of the two aforementioned anesthetic techniques on early postoperative toric IOL rotational stability, aiming to provide evidence-based insights for optimizing anesthetic strategy and improving surgical prognosis.
Data and Methods
Study Design
This study is a prospective, observational cohort study. It does not interfere with clinical decision-making. Instead, patients are prospectively followed and compared in two naturally occurring cohorts based on the actual anesthesia regimen adopted following preoperative assessment and shared decision-making between physicians and patients. The aim is to explore the impact of different anesthesia methods on early rotational stability after Toric IOL implantation.
Ethics and Informed Consent
This study was conducted at the Department of Cataract, Qingdao Eye Hospital, affiliated with Shandong First Medical University. Ethical approval was obtained from the institutional Ethics Committee (No. [2024]14), and all procedures adhered to the Declaration of Helsinki. The study was registered at a public clinical trial registry (ChiCTR2400087830) prior to the beginning of the study. Written informed consent was obtained from each participant, and personal identifiers were removed to ensure confidentiality.
Research Cohort and Participants
Patients who underwent phacoemulsification and Toric intraocular lens (IOL) implantation between February and August 2024 were enrolled. Inclusion criteria: (1) Cataract confirmed and graded as grade 3 by the Lens Opacities Classification System III (LOCS III); (2) corneal astigmatism ≥1.5 diopters (D); (3) willingness to receive Toric IOL implantation. Exclusion criteria: (1) Irregular corneal astigmatism, corneal or scleral disease, or other ocular comorbidities; (2) prior ocular surgery; (3) significant risk factors for IOL instability such as abnormal globe morphology or extreme axial length.
Preoperative Examination
All patients underwent a comprehensive ophthalmic evaluation within 24 hours before surgery. Uncorrected distance visual acuity (UDVA) was assessed using a standard logarithmic chart and converted to logMAR values. Other examinations included subjective refraction, slit-lamp biomicroscopy (BM900, Haag-Streit AG, Switzerland, Europe), widefield fundus imaging (California RG, Optos, UK, Europe), corneal topography (OCULUS Pentacam 70100, OCULUS Optikgeräte GmbH, Germany, Europe), axial length measurement (IOL Master 700, Carl Zeiss Meditec AG, Germany, Europe), macular OCT (RTVUE XR, optovue, USA), corneal endothelial cell count (NSP-9900 II, Konan, Japan), and intraocular pressure (IOP, Canon TX-20, Canon Medical System, USA) measured by a non-contact tonometer.
Preoperative Axis Marking
All markings were performed by the same surgeon under a slit-lamp biomicroscope with the patient seated upright and fixating straight ahead. A narrow-slit beam was aligned through the pupil center, and sterile marking pens were used to indicate the corneal incision site and the planned IOL axis.
Anesthesia Protocol
Based on clinical practice, patients were divided into two cohorts:
(1) Topical anesthesia: 0.5% Alcaine instilled into the conjunctival sac until effective.
(2) Peribulbar anesthesia: A 25-mm needle was inserted at the supraorbital and infraorbital rims. After confirming no blood aspiration, 3 mL each of 2% lidocaine and 1% ropivacaine were slowly injected into the upper and lower peribulbar spaces, followed by gentle ocular compression until the globe was soft.
Grouping rationale: The choice of anesthesia method is determined through comprehensive assessment of the patient’s ocular conditions (eyelid tension, ocular mobility), systemic status, anticipated surgical duration, and patient preference, following mutual consultation between the primary surgeon and the patient.
Intraocular Lens
The TECNIS Toric II (Johnson & Johnson Vision) is a monofocal, aspheric Toric IOL featuring negative spherical aberration (-SA) to enhance contrast sensitivity and reduce night glare. It has a 6.0 mm optical zone and is available in models ZCT150–ZCT400, covering spherical powers from +6.00 D to +30.00 D and astigmatic corrections from 1.0 D to 6.0 D. The IOL model and intended axis were calculated preoperatively using the manufacturer’s proprietary software.
Surgical Procedure
Standard phacoemulsification and Toric IOL implantation were performed using a 2.2 mm clear corneal main incision and a 1.0 mm side port. A continuous curvilinear capsulorhexis of approximately 5.5 mm was created, and the Toric IOL was aligned according to preoperative markings. All surgeries were performed by the same experienced surgeon using the same phacoemulsification system. At the end of surgery, tobramycin–dexamethasone ointment was applied, and the operated eye was bandaged.
Postoperative Medication
All patients received an identical postoperative regimen: 1% prednisolone acetate eye drops, 4 times daily for 2 weeks; 0.1% bromfenac sodium eye drops, 2 times daily for 6 weeks; 0.3% gatifloxacin ophthalmic gel, 4 times daily for 1 week; Tobramycin–dexamethasone ophthalmic ointment, once nightly for 1 week.
Postoperative Follow-up
Patients were examined at postoperative day 1, week 1, and month 1. Evaluations included objective refraction, UDVA (converted to logMAR), Toric IOL axis position, and IOP. On day 1, IOL alignment was assessed using a slit-lamp with a rotating slit, ensuring accurate head and gaze positioning despite transient corneal edema. At week 1 and month 1, IOL rotation was measured after pupil dilation using the iTrace Visual Function Analyzer (Tracey Technologies, USA, North America). A postoperative IOL rotation >10° was considered the threshold for surgical repositioning.
Statistical Analysis
All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test and Q–Q plots were used to assess the normality of continuous data. Normally distributed variables were expressed as mean ± standard deviation (SD) and compared using the independent-samples t-test; non-normally distributed data were expressed as median (Q1, Q3) and analyzed with the Mann–Whitney U-test. Categorical variables were compared using the chi-square test or Fisher’s exact test where appropriate. Binary logistic regression was used to evaluate the influence of anesthesia type and axial length on the likelihood of Toric IOL repositioning. A P value <0.05 was considered statistically significant.
Results
Patient Profile
At the 1-month postoperative follow-up, 8 patients in the peribulbar anesthesia group and 4 in the topical anesthesia group were lost to follow-up, representing an overall loss rate of 5%. Ultimately, data from 228 patients (228 eyes) were analyzed—112 in the peribulbar anesthesia group and 116 in the topical anesthesia group. Preoperative baseline characteristics, including demographic and ocular parameters, showed no statistically significant differences between the two groups (P > 0.05), indicating good comparability (Table 1).
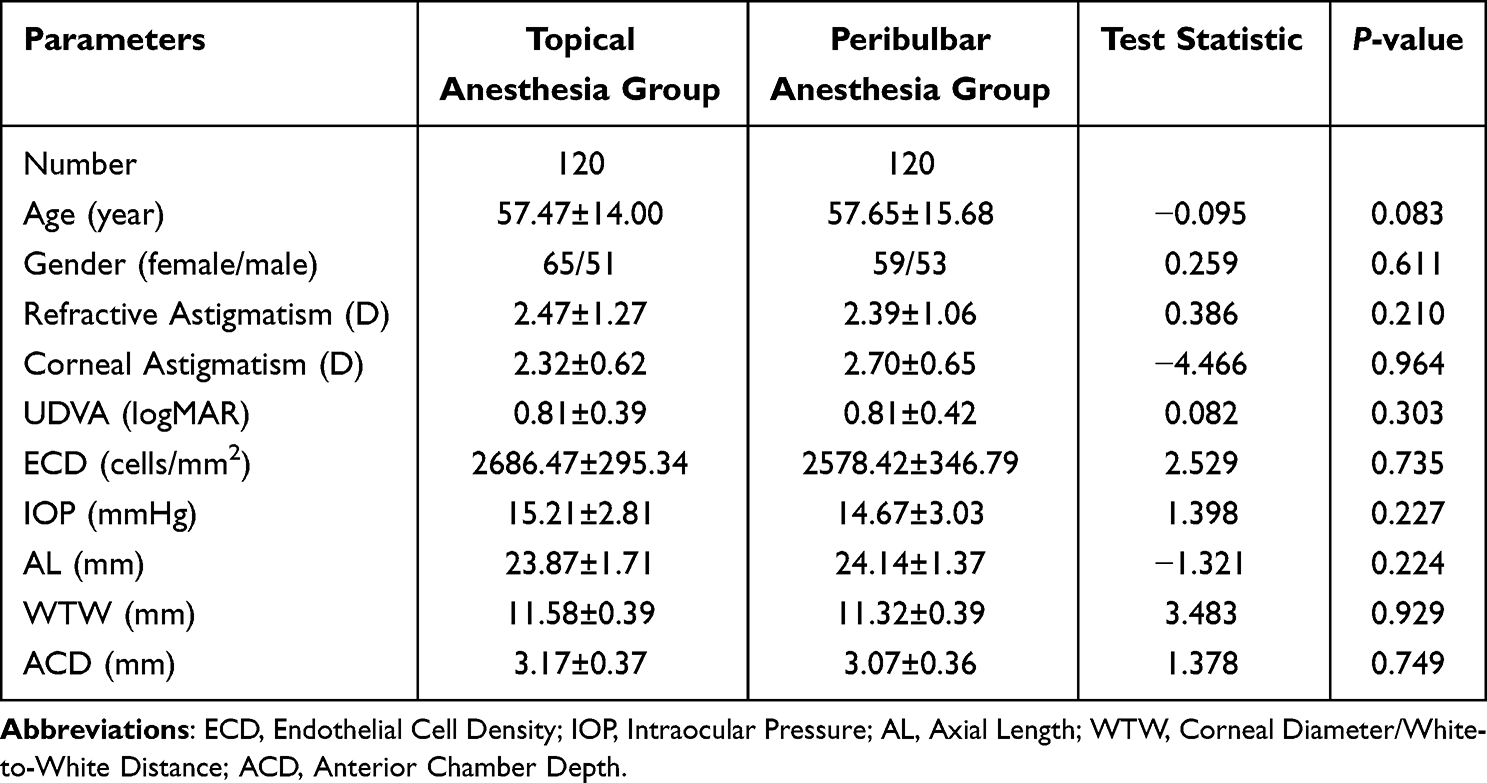 |
Table 1 Baseline Demographic and Clinical Parameters of the Studied Patients |
Incidence of Surgical Repositioning
During the 1-month follow-up, the cumulative incidence of Toric IOL surgical repositioning differed significantly between the groups: 1/112 (0.9%) in the peribulbar anesthesia group versus 8/116 (6.9%) in the topical anesthesia group (χ2=3.949, P=0.034) (Table 2). Details of the degree and timing of significant rotation (>10°) in patients who required repositioning are summarized in Table 3. At each time point, repositioning incidence was calculated based on the number of patients remaining under observation; eyes that had already undergone repositioning were excluded from subsequent analyses.
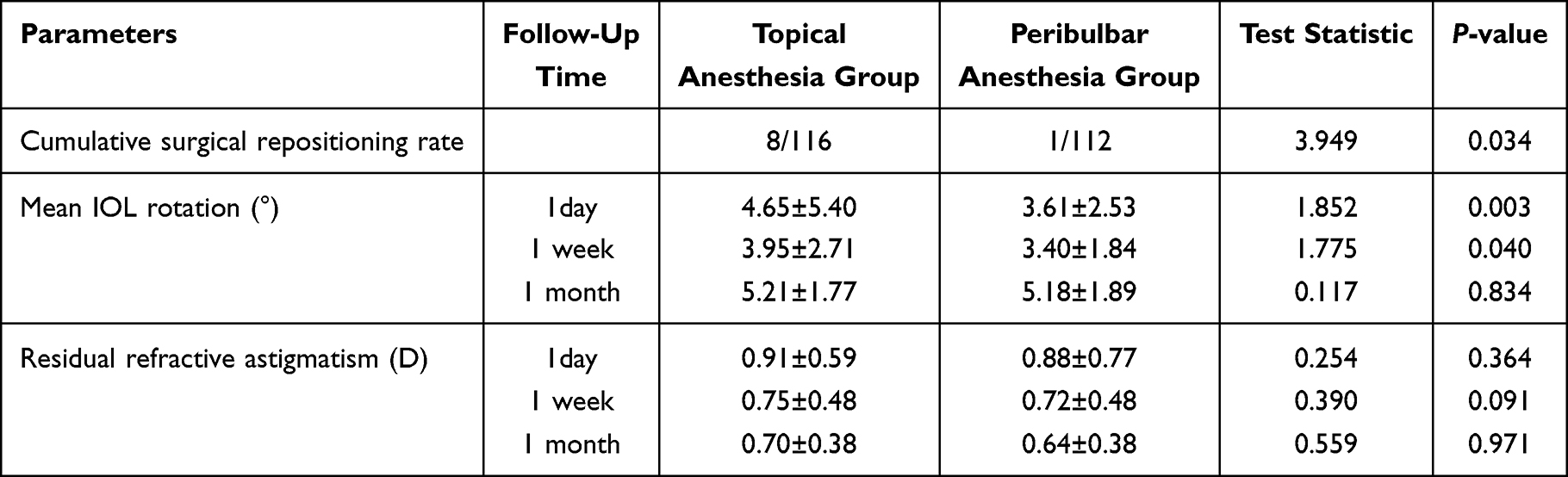 |
Table 2 Repositioning Rate, IOL Rotation, and Residual Astigmatism: Group Comparison |
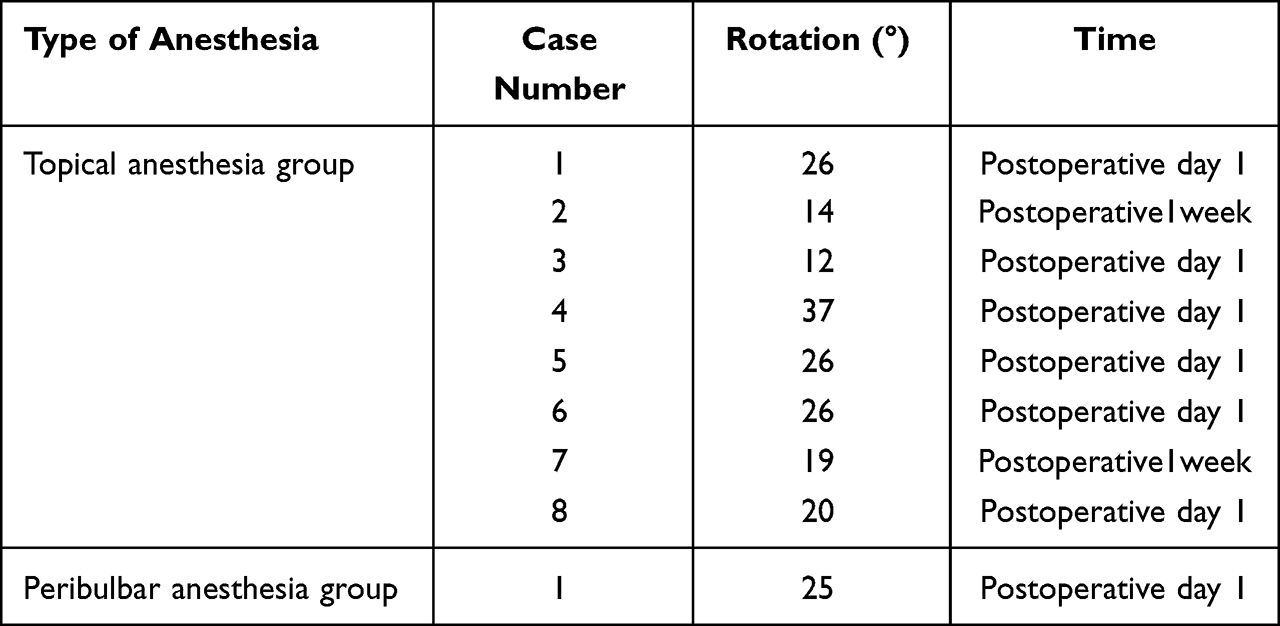 |
Table 3 Degree and Timing of Postoperative IOL Rotation |
Postoperative Toric IOL Rotation
On postoperative day 1 and week 1, the mean rotation of Toric IOLs was significantly smaller in the peribulbar anesthesia group compared with the topical anesthesia group (day 1: t=1.852, P=0.003; week 1: t=1.775, P=0.040). By 1 month postoperatively, the mean rotational degree no longer showed a statistically significant difference between the two groups (Table 2).
Postoperative Residual Refractive Astigmatism
At postoperative day 1, week 1, and month 1, the mean residual refractive astigmatism did not differ significantly between the peribulbar and topical anesthesia groups (day 1: t=0.254, P=0.364; week 1: t=0.390, P=0.091; month 1: t=0.559, P=0.971) (Table 2).
Postoperative UDVA and IOP
UDVA showed progressive improvement in both groups at each postoperative time point (day 1, week 1, and month 1). On postoperative day 1, mean UDVA was significantly better in the peribulbar anesthesia group (logMAR 0.21 ± 0.16) than in the topical anesthesia group (logMAR 0.27 ± 0.26; t = –1.444, P = 0.046). At week 1 and month 1, the intergroup differences in UDVA were not statistically significant (Table 4). At 1 month postoperatively, 81 eyes (72.32%) in the peribulbar group and 91 eyes (78.45%) in the topical group achieved UDVA ≥ 0.8, with no significant difference between groups (χ2 = 1.000, P = 0.317). There were no statistically significant differences in mean IOP between the peribulbar and topical anesthesia groups on postoperative day 1, week 1, or month 1 (Table 4).
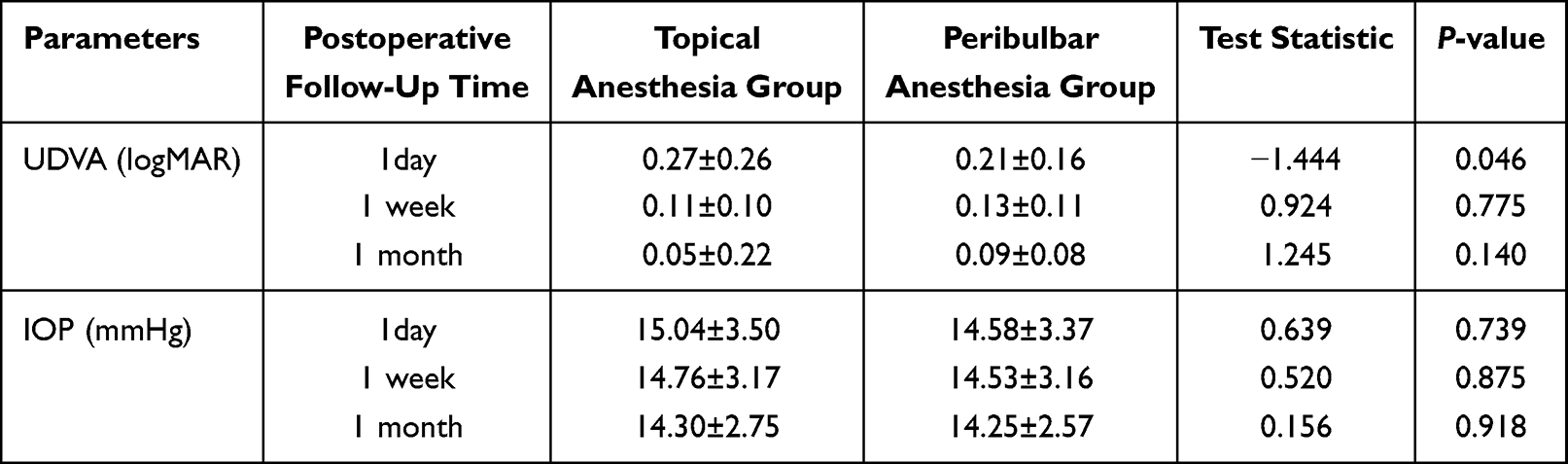 |
Table 4 Uncorrected Visual Acuity and Intraocular Pressure at 1 Month Postoperatively |
Binary Logistic Regression Analysis
Binary logistic regression analysis demonstrated that anesthesia method was significantly associated with postoperative Toric IOL repositioning. In the unadjusted model including anesthesia type alone, anesthesia method was a significant predictor (P = 0.049, OR = 8.222). After adjusting for axial length, anesthesia method remained significant (P = 0.045, OR = 8.512), while axial length itself was not (P = 0.476, OR = 1.162) (Table 5).
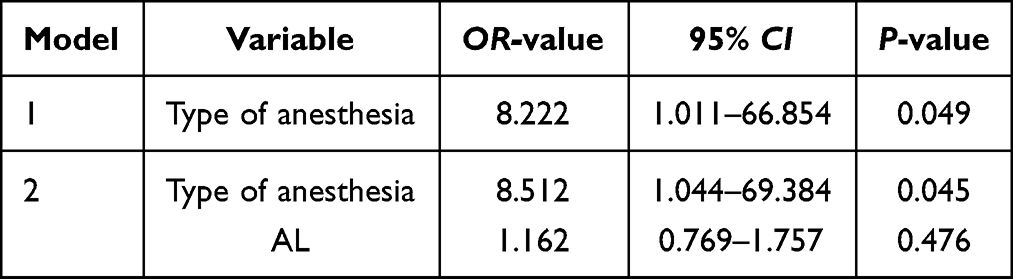 |
Table 5 Binary Logistic Regression Analysis |
Discussion
This prospective cohort study systematically evaluated the influence of topical versus peribulbar anesthesia on the early postoperative rotational stability of Toric IOLs in cataract surgery. Our findings demonstrate that the choice of anesthesia technique significantly affects Toric IOL stability, particularly during the early postoperative period.
On postoperative day 1, eyes receiving peribulbar anesthesia exhibited superior rotational stability and better UDVA compared with those under topical anesthesia. This finding can be explained by the mechanistic differences between the anesthetic techniques. Peribulbar anesthesia achieves ocular akinesia by blocking the oculomotor, trochlear, abducens, and ciliary nerves. The duration of action of anesthetic drugs can last 4 to 6 hours, which not only facilitates precise axial positioning during surgery but also maintains ocular stability in the early postoperative period through sustained anesthetic effects.22,23 This promotes the initial secure seating and integration of the IOL within the capsular bag. Previous studies have indicated that the majority of Toric IOL rotation occurs within the first hour to one day after surgery, underscoring the critical importance of ocular akinesia during and immediately following the procedure.18–20 In contrast, under topical anesthesia, patients retain the ability to move their eyes. Involuntary ocular movements, potentially triggered by surgical manipulation or postoperative stimuli, may increase the risk of Toric IOL axis deviation either during or in the early hours after surgery.21,24,25
As the postoperative period progressed, we observed a dynamic change in the differences between the two groups. By postoperative week 1, although the peribulbar anesthesia group maintained an advantage in rotational stability, the difference in UDVA between the groups was no longer statistically significant. By postoperative month 1, the difference in rotational stability between the two groups had essentially disappeared. This temporal pattern suggests that the influence of different anesthetic techniques on Toric IOL stability is concentrated primarily in the early postoperative phase, whereas long-term stability is more closely associated with capsular biological processes, such as fibrosis and contraction. With the progression of postoperative capsular fibrosis and contraction, the Toric IOL becomes biologically fixed. This observation aligns with findings from previous studies indicating that the majority of Toric IOL rotation occurs in the early postoperative period, after which its position tends to stabilize.19,26,27
Regarding visual quality, this study found that a significant difference in the degree of rotation on postoperative day 1 was accompanied by a corresponding difference in UDVA, while no statistically significant difference was observed in residual refractive astigmatism. This issue can be analyzed as a statistical problem. In this study, significant rotation occurred in 8 cases of toric intraocular lenses within the topical anesthesia group, compared to only 1 case in the peribulbar anesthesia group. The majority of patients maintained stable intraocular lens positioning or experienced only mild rotation. This distribution within the population weakened the impact of the few rotational events on the overall results for the group-level astigmatism analysis, leading to the absence of statistically significant differences in the statistical tests.
Regarding the influence of axial length, this study preliminarily explored the correlation between axial length and the postoperative event of requiring IOL repositioning using binary logistic regression analysis. In the two constructed models, axial length did not demonstrate statistical significance. This finding is consistent with conclusions from some previous studies,28,29 suggesting that under specific conditions, axial length may not be an independent strong risk factor for significant Toric IOL rotation that necessitates surgical intervention.
It is important to emphasize that, in addition to the anesthesia technique, surgical skill, IOL design, and patient-specific ocular biological parameters (such as capsular bag diameter and ciliary sulcus morphology) are also well-established as key factors influencing postoperative rotational stability of Toric IOLs. Previous studies have confirmed that a continuous curvilinear capsulorhexis, thorough removal of viscoelastic material, and IOL selection based on precise biometry are fundamental to ensuring long-term stability.30 To better isolate and investigate the independent effect of the anesthesia technique, this study implemented strict standardization and control of major confounding factors during the design phase: all surgeries were performed by the same experienced surgeon, adhering to a unified protocol, ensuring maximal consistency in surgical technique.15
In summary, the results of this study elucidate the dynamic characteristics of how different anesthetic modalities influence postoperative Toric IOL stability. The core finding demonstrates that compared to topical anesthesia, peribulbar anesthesia utilizing long-acting agents effectively reduces the magnitude of Toric IOL rotation in the early postoperative period, particularly within the first 24 hours. This finding confirms our initial hypothesis that pharmacologically prolonging postoperative ocular immobilization time can serve as an active intervention to enhance early stability following toric IOL implantation.
However, as a prospective cohort study, this research has certain limitations. The most fundamental limitation is that the assignment of patients to receive either peribulbar block or topical anesthesia was not randomized but was based on clinical assessment and shared decision-making between the physician and patient. Although no statistically significant differences were found in baseline characteristics such as age and axial length between the two groups, there remains the possibility that unknown or difficult-to-measure confounding factors influenced both group assignment and outcomes. Secondly, while the single-surgeon, single-center design ensured technical consistency, it also limits the generalizability of the findings. Whether the conclusions hold true in other centers or with surgeons employing different technical nuances requires further verification. Future research by our team is planned to involve prospective randomized controlled trials with multi-center collaboration and larger sample sizes to further investigate the impact of anesthetic technique on Toric IOL rotational stability, thereby enabling a more comprehensive evaluation of the feasibility and rationale for applying peribulbar anesthesia in Toric IOL implantation surgery.
Conclusion
The choice of anesthesia significantly influences the early postoperative rotational stability of Toric IOLs. Peribulbar anesthesia enhances short-term lens stability and reduces the likelihood of IOL repositioning, offering a practical advantage in cataract surgery requiring astigmatic correction.
Data Sharing Statement
The data supporting this study’s findings are available upon requests from the corresponding author, Xiaomin Liu, upon reasonable request.
Funding
This study was supported by the National Natural Science Foundation of China (82301190, 82171027) and the Natural Science Foundation of Shandong Province (ZR2023QH156).
Disclosure
All authors have no conflicts of interest to declare in this work.
References
1. Anderson DF, Dhariwal M, Bouchet C, et al. Global prevalence and economic and humanistic burden of astigmatism in cataract patients: a systematic literature review. Clin Ophthalmol. 2018;12:439–8. doi:10.2147/OPTH.S146829
2. Pang YL, Yuan L, Cao XG, et al. [Characteristics and analysis of corneal astigmatism in age-related cataract patients over 50 years old]. Zhonghua Yan Ke Za Zhi. 2020;56(5):349–355. doi:10.3760/cma.j.cn112142-20190618-00323
3. Wu Z, Liu C, Chen Z. Prevalence and age-related changes of corneal astigmatism in patients undergoing cataract surgery in Northern China. J Ophthalmol. 2020;2020:6385098. doi:10.1155/2020/6385098
4. Shimizu K, Misawa A, Suzuki Y. Toric intraocular lenses: correcting astigmatism while controlling axis shift. J Cataract Refract Surg. 1994;20(5):523–526. doi:10.1016/S0886-3350(13)80232-5
5. Lake JC, Victor G, Clare G, et al. Toric intraocular lens versus limbal relaxing incisions for corneal astigmatism after phacoemulsification. Cochrane Database Syst Rev. 2019;12(12):Cd012801. doi:10.1002/14651858.CD012801.pub2
6. Poll JT, Wang L, Koch DD, et al. Correction of astigmatism during cataract surgery: toric intraocular lens compared to peripheral corneal relaxing incisions. J Refract Surg. 2011;27(3):165–171. doi:10.3928/1081597X-20100526-01
7. Nanavaty MA, Bedi KK, Ali S, et al. Toric intraocular lenses versus peripheral corneal relaxing incisions for astigmatism between 0.75 and 2.5 diopters during cataract surgery. Am J Ophthalmol. 2017;180:165–177. doi:10.1016/j.ajo.2017.06.007
8. Nagpal R, Sharma N, Vasavada V, et al. Toric intraocular lens versus monofocal intraocular lens implantation and photorefractive keratectomy: a randomized controlled trial. Am J Ophthalmol. 2015;160(3):479–86.e2. doi:10.1016/j.ajo.2015.06.007
9. Titiyal JS, Kaur M, Jose CP, et al. Comparative evaluation of toric intraocular lens alignment and visual quality with image-guided surgery and conventional three-step manual marking. Clin Ophthalmol. 2018;12:747–753. doi:10.2147/OPTH.S164175
10. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631–1636. doi:10.1016/j.jcrs.2008.04.041
11. Schallhorn SC, Hettinger KA, Pelouskova M, et al. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47(8):991–998. doi:10.1097/j.jcrs.0000000000000560
12. Ruhswurm I, Scholz U, Zehetmayer M, et al. Astigmatism correction with a foldable toric intraocular lens in cataract patients. J Cataract Refract Surg. 2000;26(7):1022–1027. doi:10.1016/S0886-3350(00)00317-5
13. Chang P, Chen D, Hu B, et al. Effect of capsular bend on the rotational stability of toric intraocular lens. Eye. 2023;37(3):480–485. doi:10.1038/s41433-022-01964-0
14. Li ES, Vanderford EK, Xu Y, et al. Rotational stability of toric intraocular lenses by lens model and haptic design: systematic review and single-arm meta-analysis. J Cataract Refract Surg. 2024;50(9):976–984. doi:10.1097/j.jcrs.0000000000001486
15. Li S, Li X, He S, et al. Early postoperative rotational stability and its related factors of a single-piece acrylic toric intraocular lens. Eye. 2020;34(3):474–479. doi:10.1038/s41433-019-0521-0
16. Ma D, Yu W, Cai L, et al. Optimal timing of repositioning surgery for a plate-haptic toric intraocular lens: a multicenter retrospective study. J Refract Surg. 2023;39(2):120–126. doi:10.3928/1081597X-20221221-02
17. Schartmüller D, Schwarzenbacher L, Meyer EL, et al. Comparison of long-term rotational stability of three commonly implanted intraocular lenses. Am J Ophthalmol. 2020;220:72–81. doi:10.1016/j.ajo.2020.07.019
18. Singh A, Kapoor G, Baranwal VK, et al. Rotational stability of Toric intraocular lenses. Med J Armed Forces India. 2022;78(1):68–73. doi:10.1016/j.mjafi.2020.03.014
19. Miyake T, Kamiya K, Amano R, et al. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40(10):1654–1660. doi:10.1016/j.jcrs.2014.01.044
20. Schartmüller D, Schriefl S, Schwarzenbacher L, et al. True rotational stability of a single-piece hydrophobic intraocular lens. Br J Ophthalmol. 2019;103(2):186–190. doi:10.1136/bjophthalmol-2017-311797
21. Johnston RL, Whitefield LA, Giralt J, et al. Topical versus peribulbar anesthesia, without sedation, for clear corneal phacoemulsification. J Cataract Refract Surg. 1998;24(3):407–410. doi:10.1016/S0886-3350(98)80332-5
22. Ortiz M, Blanco D, Serra J, et al. Peribulbar anaesthesia: the role of local anaesthetic volumes and Thiomucase in motor block and intraocular pressure. Eur J Anaesthesiol. 1995;12(6):603–607.
23. Alhassan MB, Kyari F, Ejere HO. Peribulbar versus retrobulbar anaesthesia for cataract surgery. Cochrane Database Syst Rev. 2015;2015(7):Cd004083. doi:10.1002/14651858.CD004083.pub3
24. Zhao LQ, Zhu H, Zhao PQ, et al. Topical anesthesia versus regional anesthesia for cataract surgery: a meta-analysis of randomized controlled trials. Ophthalmology. 2012;119(4):659–667. doi:10.1016/j.ophtha.2011.09.056
25. Zehetmayer M, Radax U, Skorpik C, et al. Topical versus peribulbar anesthesia in clear corneal cataract surgery. J Cataract Refract Surg. 1996;22(4):480–484. doi:10.1016/S0886-3350(96)80046-0
26. Sasaki K, Eguchi S, Miyata A, et al. Anterior capsule coverage and rotational stability of an acrylic toric intraocular lens. J Cataract Refract Surg. 2021;47(5):618–621. doi:10.1097/j.jcrs.0000000000000489
27. Kim JH, Lee D, Cha YD, et al. The analysis of predicted capsular bag diameter using modified model of capsule measuring ring in Asians. Clin Exp Ophthalmol. 2008;36(3):238–244. doi:10.1111/j.1442-9071.2008.01726.x
28. Mencucci R, Favuzza E, Guerra F, et al. Clinical outcomes and rotational stability of a 4-haptic toric intraocular lens in myopic eyes. J Cataract Refract Surg. 2014;40(9):1479–1487. doi:10.1016/j.jcrs.2013.12.024
29. Ang RET, Tañá-Rivero P, Pastor-Pascual F, et al. Rotational stability after implantation of an aspheric toric monofocal IOL with a double C-loop haptic design in normal and high axial lengths. Clin Ophthalmol. 2025;19:2393–2403. doi:10.2147/OPTH.S530593
30. Lin X, Ma D, Yang J. Exploring anterion capsular contraction syndrome in cataract surgery: insights into pathogenesis, clinical course, influencing factors, and intervention approaches. Front Med. 2024;11:1366576. doi:10.3389/fmed.2024.1366576
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.