Back to Journals » International Journal of Women's Health » Volume 18
Effect of an Educational Intervention on Reducing Mistreatment in Gynecology and Obstetrics Services in Guinea: A Client-Reported Before-After Study
Authors Balde MD ![]() , Keita KS
, Keita KS ![]() , Camara S
, Camara S ![]() , Sall AO
, Sall AO ![]() , Diallo BA, Camara M
, Diallo BA, Camara M ![]() , Toure M
, Toure M ![]() , Barry F
, Barry F ![]() , Diallo A, Sidibe T
, Diallo A, Sidibe T
Received 29 January 2026
Accepted for publication 24 May 2026
Published 24 June 2026 Volume 2026:18 599748
DOI https://doi.org/10.2147/IJWH.S599748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Mamadou Dioulde Balde,1 Kaba Saran Keita,1 Sadan Camara,1 Alpha Oumar Sall,1 Boubacar Alpha Diallo,1,2 Moussa Camara,1 Madeleine Toure,1 Fanta Barry,1 Aissatou Diallo,1 Tiany Sidibe1
1Centre for Research in Reproductive Health in Guinea (CERREGUI), Conakry, Guinea; 2Faculty of Health Sciences and Technology, Gamal Abdel Nasser University, Conakry, Guinea
Correspondence: Mamadou Dioulde Balde, (Centre for Research in Reproductive Health in Guinea (CERREGUI), Conakry, Guinea, BP 4880, Tel +224 628 21 33 44, Email [email protected]
Objective: To evaluate the effects of the intervention on the prevention of mistreatment of women in gynecology and obstetrics units in Guinea.
Material and Methods: A pre-post intervention study was conducted to assess the effects of the intervention. The study was carried out on a sample of clients were interviewed before and after the training. The impact of provider training was analyzed using robust Poisson regression models for binary variables.
Results: Multivariate analyses showed an association between the intervention and overall reduction in the risk of experiencing violence or mistreatment of 43% in gynecology (adjusted RR = 0.57; 95% CI: 0.53– 0.62) and 44% in obstetrics (adjusted RR = 0.56; 95% CI: 0.53– 0.59). In gynecology, physical violence decreased by 30% and verbal violence by 22%. In obstetrics, decreases were similar, with a 31% reduction in physical violence and a 27% reduction in verbal violence. All estimates were statistically significant (p < 0.001) after adjustment for confounders.
Conclusion: The intervention contributed to a significant reduced mistreatment in gynecology and obstetrics services. Continued professional training and community awareness are effective strategies for preventing obstetric and gynecological violence.
Keywords: effect, mistreatment, physical violence, verbal violence, healthcare providers, Guinea
Background
Providing high-quality care for women’s health requires respectful and dignified treatment in gynecology and obstetrics services.1,2 Mistreatment during childbirth or gynecological care can result in adverse maternal and neonatal outcomes, deter women from seeking care, and contribute to unintended pregnancies, unrecognized complications, and maternal or infant mortality.1,2 Respectful maternal care emphasizes a patient-centered approach rooted in women’s fundamental human rights.1,2
Since 2015, the World Health Organization (WHO) has used the term “mistreatment” rather than “obstetric violence”. Such abuses constitute violations of human rights and contribute to high maternal mortality.3–5 Mistreatment in gynecological and obstetrical units is recognized globally as a form of violence occurring in medical settings and is condemned by the WHO.6 It refers to abuses experienced by women during reproductive health care, including gynecological consultations, childbirth, and postpartum care. These practices are exacerbated by insufficient provider training, inadequate resources, lack of sanctions, and limited patient awareness of their rights.7–10 Structural factors such as excessive workloads, needs for capacity building, and normalization of abusive practices also hinder efforts to eliminate mistreatment in obstetric care.11
Despite limited systematic data collection, studies indicate a high prevalence of mistreatment in obstetric in Africa, varying across countries and regions.12–14 Prevalence ranges from 20% to 98%, with an estimated average of 47% in East Africa.15 Approximately 37% of women in low- and middle-income countries experience mistreatment obstetric.16 Verbal abuse, in particular, reflects institutional culture, stress, and burnout-factors not easily changed through a single intervention.17
The lack of competence among healthcare professionals is a major barrier to quality care.18 Training programs focused on respectful care and patient-centered communication have demonstrated significant reductions mistreatment obstetric in various African settings.12,19–23 Prior research shows that provider training and community awareness are essential levers for reducing mistreatment and improving quality of care.6,24 Education on sexual and reproductive rights, medical ethics, and communication supports lasting behavioral change.19,20,23 Likewise, awareness campaigns and community involvement help identify, report, and prevent mistreatment obstetric.25,26
In Guinea, multiple studies have documented high levels of mistreatment in gynecology and obstetrics services, including physical, verbal, and other forms of mistreatment.7–9,27 A situational analysis documenting the prevalence and typology of mistreatment in gynecology and obstetrics in Guinea was therefore conducted in 2023.27,28 Lack of training has been shown to be a key factor in the persistence of mistreatment of women.7,8,27,28 However, no study in Guinea has evaluated the effectiveness of a combined provider community intervention to reduce mistreatment. To this end, an intervention focusing on training healthcare providers and community health workers/community relays (CRs) as well as community awareness-raising for the prevention of mistreatment was carried out in the same five health districts than in the situational analysis in Guinea. This study aims to evaluate the effects of the intervention on the prevention of mistreatment of women in gynecology and obstetrics units in Guinea.
Materials and Methods
Study Design
This was a quasi-experimental, before-and-after study without a control group was conducted to assess the effects of the intervention in May and June 2025 in Guinea to evaluate the effects of the intervention. Data before the intervention was collected as part of a situational analysis conducted in January and February 2023, the results of which were published.7,10,27 This analysis served as the basis for the design and implementation of an intervention, the program described below being directly based on the findings of this initial assessment.
Description of the Intervention
The intervention proceeded in three successive stages.
- The first stage consisted of training healthcare providers at the intervention sites. The training lasted 30 days and was facilitated by Amref Health Africa, researchers from the Center for Reproductive Health Research (CERREGUI), and clinical specialists. The training focused on recognizing abuse in gynecology and obstetrics, describing its manifestations, and implicating healthcare providers in combating these practices. Particular emphasis was placed on women’s rights and the establishment of a mechanism for handling complaints from clients. - The second stage involved the trained providers putting their knowledge into practice with clients in gynecology and obstetrics services.
- The third stage involved raising awareness among women of childbearing age in the community, carried out by community health workers and community relays (CHW/CR). We have added the following details: a total of 50 community health workers and community relays were mobilized. They reached approximately 2200 women through educational talks and home visits. These activities were designed to inform women about their rights and the availability of a recourse mechanism in cases of abuse. The women in the community who benefited from the awareness campaign and the clients interviewed as they left the gynecology and obstetrics services were distinct but interconnected groups. The awareness campaign targeted a broader population in the communities served by the health facilities, while the clients interviewed were specifically those who had received care at those same facilities. The causal link between community awareness and the experiences of the interviewed clients can be explained by several mechanisms (women’s autonomy, social pressure…). In addition, the fight against mistreatment in gynecology and obstetrics was integrated as a continuing education module in health services and training institutions for health professionals.
Study Setting
General Context
Guinea is located in West Africa and covers a total area of 245,857 km2, with an estimated population of 13.5 million in 2022.28 The socio-economic context is marked by a high level of poverty (55.2% of the population lives below the poverty line). The country faces a high illiteracy rate (66%), affecting 73% of women and 53% of men, with a primary school attendance rate of 86%. Only 68% of households have access to safe drinking water and 19% to electricity. Women of reproductive age (15–49 years) are particularly vulnerable, and adolescents and young people have limited access to sexual and reproductive health services (only 10 out of 38 health districts provide such services).29 The proportion of women with no formal education is high (68.9%), which limits their ability to access and understand information on sexual and reproductive health and rights, thereby restricting informed decision-making regarding their care.29
The healthcare system in Guinea is organized into three levels: primary, secondary, and tertiary. At the primary level, 407 health centers and 1640 health posts provide frontline care, awareness-raising, and vaccination activities, with the support of community workers and relays. The secondary level comprises 25 prefectural hospitals, 8 regional hospitals, and 6 municipal medical centers. The tertiary level is limited to 3 national hospitals, all located in the capital.30
Specific Setting
The study was carried out in five prefectures representing Guinea’s four natural regions: Labé, Faranah, Boké, Dabola, and Guéckédou. These sites were selected for their geographic and socioeconomic diversity, enabling documentation of vulnerabilities affecting women of reproductive age. In each prefecture, data were collected in a regional or prefectural hospital, an urban health facility, and a rural health facility. Data were obtained from patients upon discharge from consultations or treatments within gynecology and obstetrics services, as well as from the surrounding communities.
Study Population
Data were collected from women upon discharge from consultations or care in the gynecology and obstetrics departments of the five selected prefectures. The inclusion criteria were: being between the ages of 18 and 49, having received gynecological or obstetric care on the day of the survey, and having provided informed consent.
Sample Size and Sampling
The sample size was calculated using Schwartz’s formula for proportions, considering an expected prevalence of 45% of abuse (based on the situational analysis), a margin of error of 5%, a 95% confidence interval, and an anticipated non-response rate of 10%. The result was a minimum sample size of 380 participants for each period. We included 600 women before the intervention and 301 after; the latter number reflects the lack of financial resources at the time of data collection. A total of 901 clients were interviewed at the end of their pre- and post-intervention consultations. Regional or prefectural hospitals and rural health centers were selected purposively (Sannoun for Labé, Banian for Faranah, Kolaboui for Boké, Bissikrima for Dabola, and Guéndembou for Guéckédou). Urban health centers were selected randomly using RandomGenerator software. A systematic sampling method was applied, with every third patient leaving a gynecological or obstetric consultation being invited to participate until the quota was reached at each site.
Data Collection
The post-intervention data concerned exclusively the period after the intervention in order to minimize memory bias and assess the direct impact of the intervention on recent practices. The questionnaire used was adapted from WHO-validated tools for studying obstetric mistreatment and was pre-tested with clients (who were not included in the final sample) to assess its clarity and cultural acceptability.
Study Variables
Dependent Variables
- Mistreatment: Number of instances of mistreatment (physical violence, verbal violence, and other forms of abuse) reported before and after the intervention.
- Physical violence: Number of instances of physical abuse (pinching, kicking, slapping, hitting, tying, applying abdominal pressure, or painful gynecological examination) reported before and after the intervention.
- Verbal violence: Number of verbal mistreatment incidents (yelling, scolding, insulting, mocking, making negative remarks, threatening) reported before and after the intervention.
- Other types of mistreatments: Number of other mistreatment practices (stigmatization, lack of consent, lack of discretion, lack of confidentiality, absence of pain relief during childbirth or after procedures, neglect, lack of communication, lack of autonomy, informal payment) reported before and after the intervention.
Independent Variables
Age, religion, residence, education level, occupation, number of children, history of abuse, status of the health worker, type of health facility, and reason for consultation.
Data Analysis
Data were collected via KoboCollect on tablets, then transferred to Stata for cleaning and analysis. The results concerning maltreatment (presence or absence of each type of maltreatment) were treated as binary variable. Indicators were described and compared between the situational analysis (before the intervention) and the post-intervention assessment. Pearson’s chi-square test of independence was used to determine the statistical significance of differences between the two periods.
The effect of training healthcare providers and raising community awareness was analyzed using a robust Poisson regression model for binary outcomes. The vce(robust) option was applied to correct variance estimation errors. The model was adjusted for several covariates (age, religion, residence, education, profession, number of children, history of mistreatment, health worker status, health facilities, motive for consultation) to control for potential confounding factors. Statistical significance was set at p < 0.05. All analyses were performed using Stata version 17.
Ethical Considerations
This study is based on the analysis of human data and was conducted in strict accordance with the ethical principles set forth in the Declaration of Helsinki. The study protocol was approved by the National Ethics Committee for Health Research of Guinea (Number 162/CNERS/21, November 1, 2021). Free and informed consent was obtained from all participants prior to questionnaire administration. Confidentiality was ensured throughout the study, and all data were anonymized. In addition to obtaining free and informed consent, the following measures were implemented to ensure the well-being of participants during the interviews: a safe and confidential environment, training for interviewers, and the right to refuse or discontinue participation.
Results
Flux Diagram
Figure 1 present the flow of participants in the quasi-experimental before-after study conducted without a control group. A total of 916 individuals were assessed for eligibility and all received the intervention. Of these, 15 participants were excluded from the final analysis, 8 due to refusing to participate and 7 with incomplete data. Consequently, 901 participants were included and analyzed in the final evaluation.
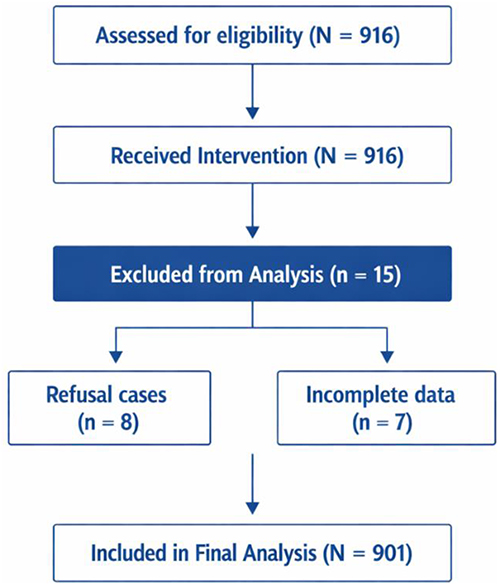 |
Figure 1 Flow diagram of participants in the quasi-experimental before-after study without a control group. Diagram showing participant eligibility assessment (N = 916), intervention received (N = 916), exclusions (n = 15: 8 refusals, 7 incomplete data), and final inclusion in analysis (N = 901). |
Description of the Study Population
The analysis included 600 patients surveyed before the intervention and 301 after the intervention in gynecology and obstetrics departments.
The most represented age groups were 20–24 and 25–29 years, both before (31.5% and 26.2%, respectively) and after the intervention (27.2% and 25.3%, respectively). Regarding place of residence, 74.8% of patients lived in urban areas before the intervention compared to 25.2% in rural areas. After the intervention, the proportion of urban residents slightly decreased (71.8%), while rural residents increased (28.2%), a statistically significant difference.
Educational attainment also differed significantly between the two periods, with the proportion of clients with no formal education decreasing from 44% before the intervention to 39.9% after, and an increase in clients with primary education (24.5% before, 28.6% after). The most common occupations before and after the intervention were homemaker, seamstress, and saleswoman. The majority of clients (approximately 59%) had two or more children in both periods (Table 1).
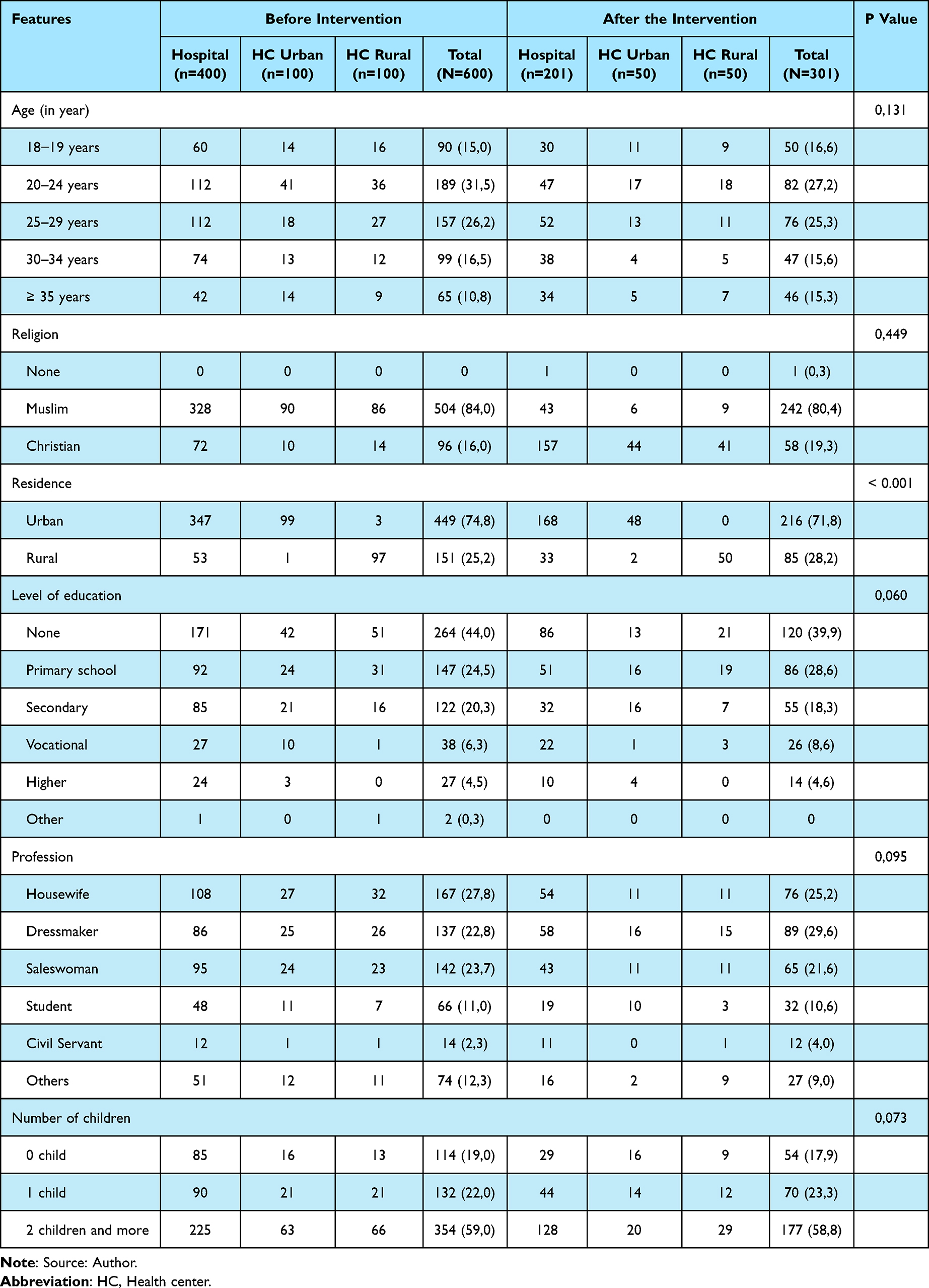 |
Table 1 Sociodemographic Characteristics of Clients Upon Discharge from Consultations or Care in Gynecology and Obstetrics Services |
Frequency of Mistreatment in Gynecology and Obstetrics
A significant decrease in mistreatment was observed after the intervention in both gynecology and obstetrics departments. Reported mistreatment decreased from 45.3% to 12.2% in gynecology and from 32.4% to 8.9% in obstetrics (Figure 2 and Table 2).
 |
Table 2 Frequency of Mistreatment Experienced by Clients in Gynecology and Obstetrics |
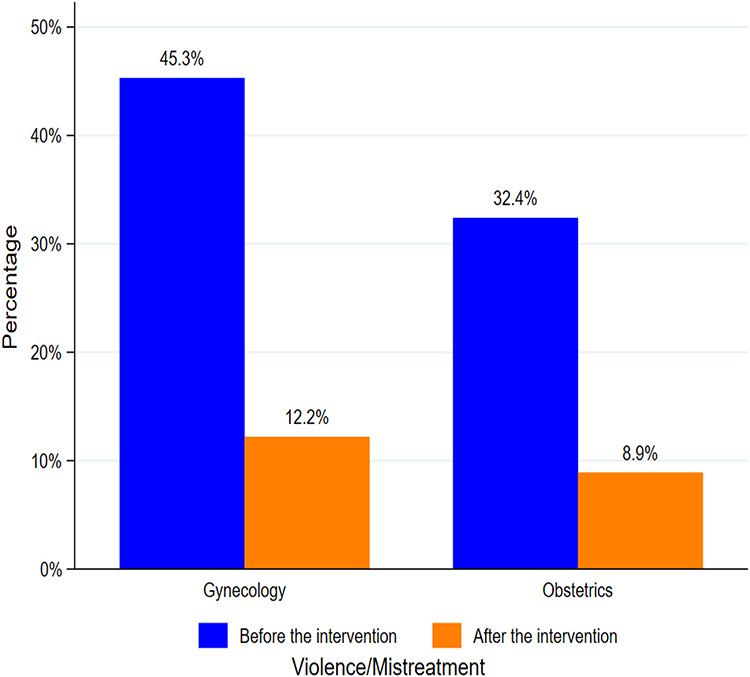 |
Figure 2 Mistreatment experienced by female clients in gynecology and obstetrics. Comparison of reported percentages of violence/mistreatment in gynecology and obstetrics, before and after the intervention. |
Types of Mistreatments Reported by Clients
The study results show a significant reduction in mistreatment after the intervention, across all types of mistreatments. A marked decrease was observed in physical violence (from 21.8% to 6.3%) and verbal violence (from 20.2% to 7%) (Figure 3). A notable decline was also recorded in other forms of mistreatment, including lack of consent (from 13.5% to 3.3%), neglect and insufficient privacy (from 38.3% to 9.6%) and breaches of confidentiality (from 4.3% to 2.7%) (Table 3). The results in Table 3 reveals a statistically significant reduction in other types of mistreatments. Informal payment fell from 25.5% to 5.0%, lack of communication (from 12.8% to 1.6%), lack of autonomy for women (from 16.0% to 2.6%) and lack of hygiene (from 16.8% to 0.7%). The significance threshold used was p < 0.003.
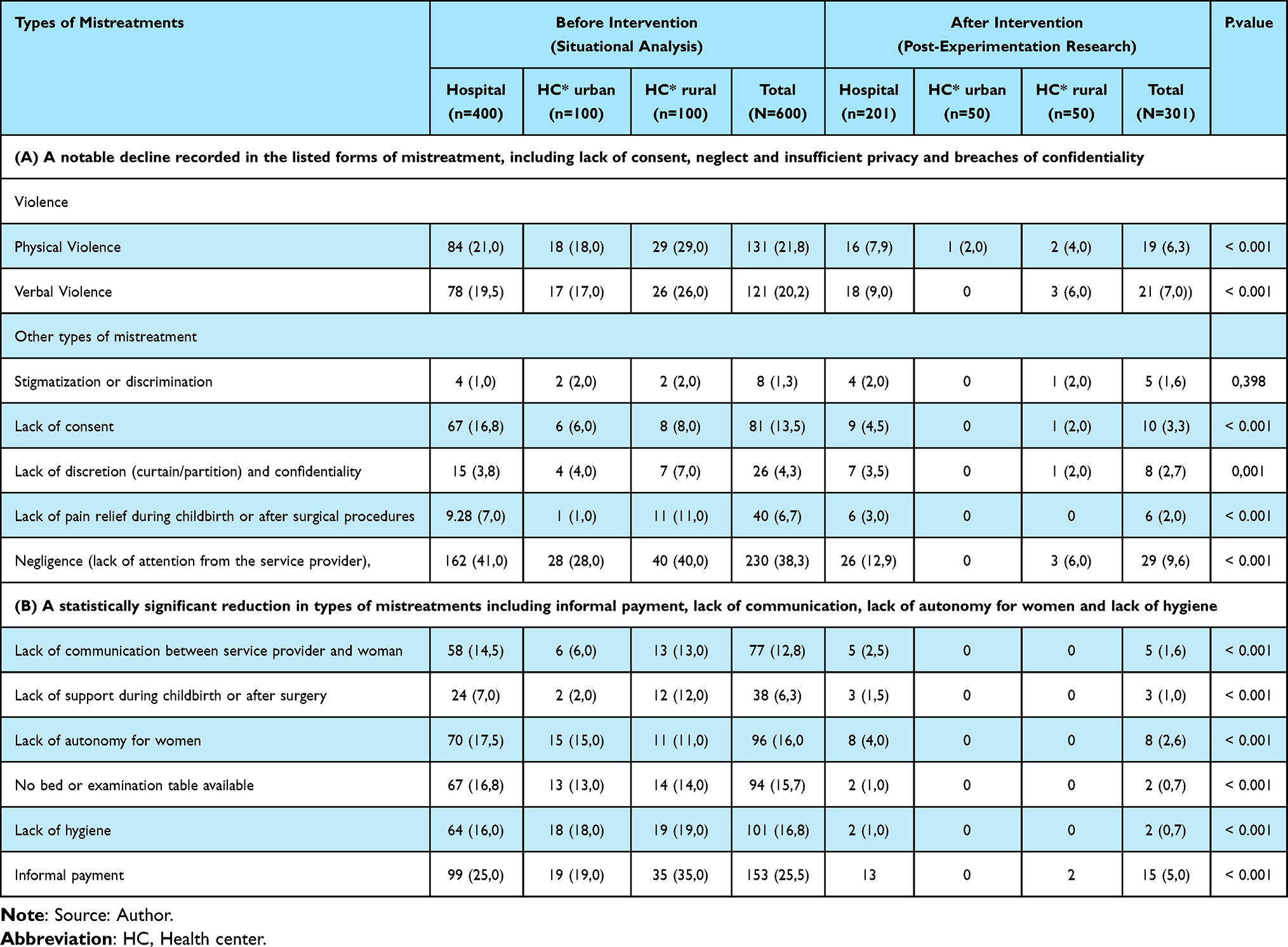 |
Table 3 Types of Mistreatments Reported by Clients |
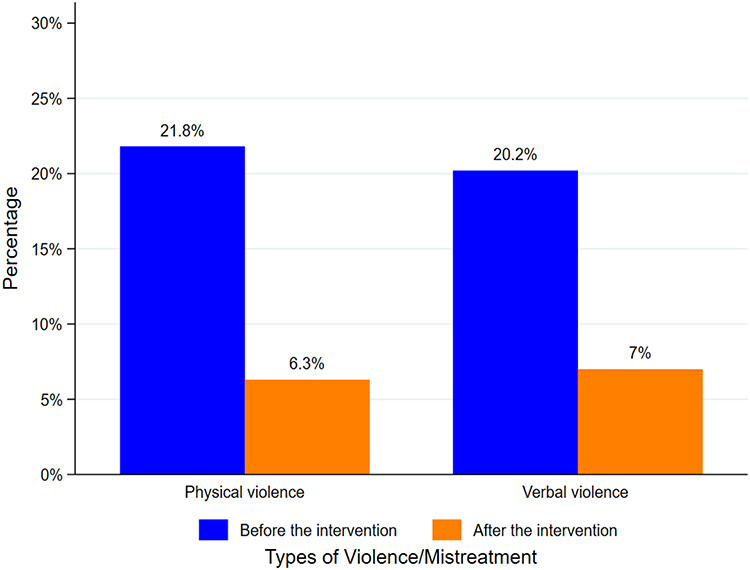 |
Figure 3 Types of gynecological and obstetric violence reported by clients. Comparison of reported percentages of physical and verbal violence in gynecology and obstetrics, before and after the intervention. |
Effects of the Intervention on the Prevention of Mistreatment in Gynecological and Obstetric Services
The analyses were adjusted for age, religion, residence, education, profession, number of children, history of mistreatment, health worker status and health facilities to ensure the validity of the results. The effects were assessed using four main indicators: overall mistreatment, physical violence, verbal violence, and other types of mistreatments. This approach allowed for an objective evaluation of the changes brought about by the intervention in healthcare providers’ practices and clients’ experiences. Robust Poisson regression models were used with standard errors pooled by institution (n=15) to account for the hierarchical nature of the data.
In gynecology: Clients interviewed upon discharge from healthcare facilities reported a 43% reduction in the risk of violence/mistreatment after the intervention (RR = 0.57; 95% CI: [0.53–0.62]). The intervention also resulted in a significant decrease in physical violence, with a 30% reduction in risk (RR = 0.70; 95% CI: [0.63–0.78]). Similarly, verbal abuse declined by 22% (RR = 0.78; 95% CI: [0.69–0.87]). Clients also reported a 42% reduction in the risk of other forms of violence (RR = 0.58; 95% CI: [0.52–0.61]) (Table 4).
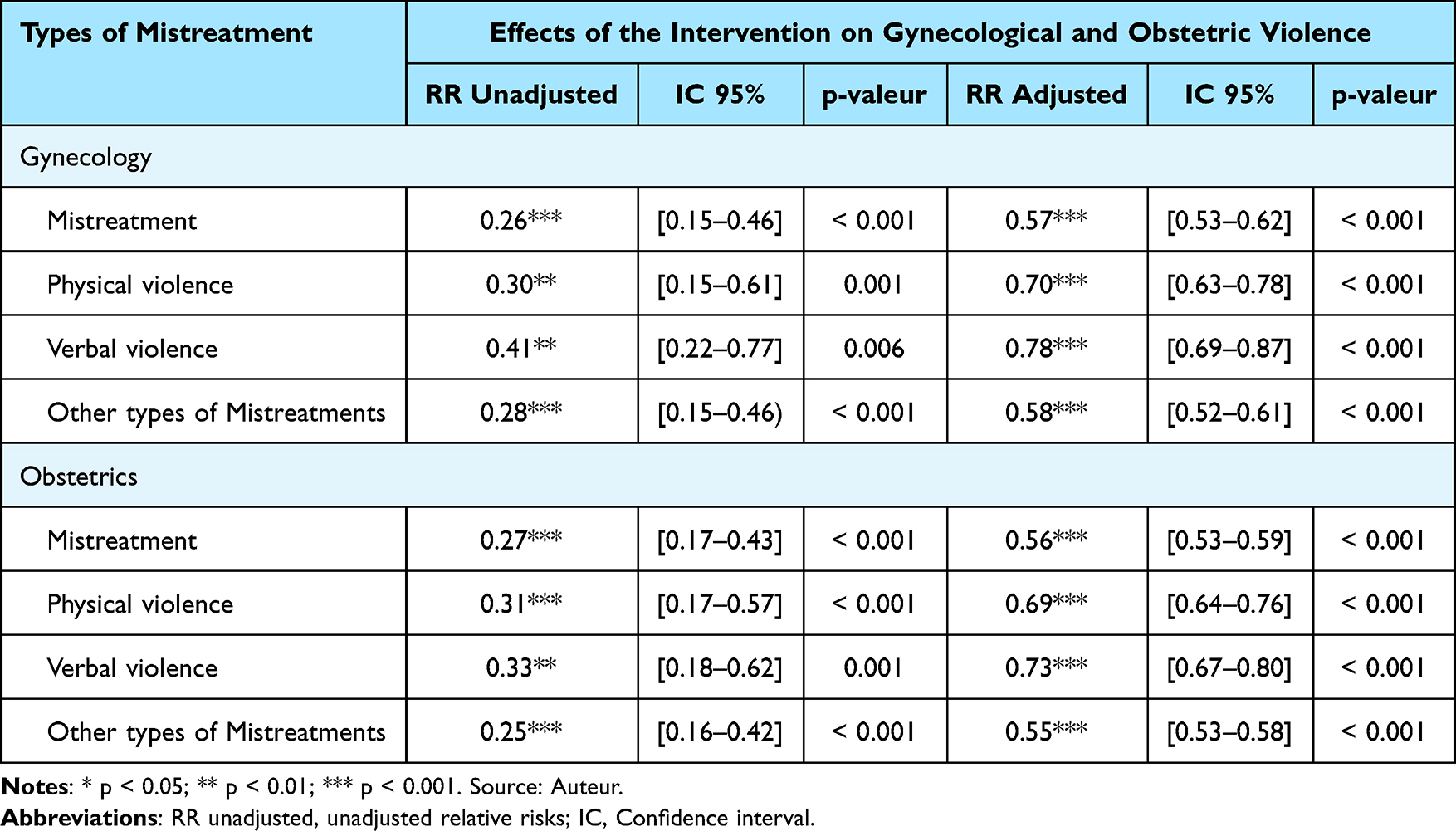 |
Table 4 Effects of the Intervention on Mistreatment in Gynecology and Obstetrics Reported by Clients Upon Discharge from Health Facilities (Multivariate Analysis) |
In obstetrics: An overall reduction in the risk of mistreatment was observed after the intervention. The likelihood of a woman experiencing mistreatment decreased by 44% compared to the situation before the intervention (RR = 0.56; 95% CI: [0.53–0.59]). Physical violence decreased by 31% (RR = 0.69; 95% CI: [0.64–0.76]). The intervention also reduced the risk of verbal violence by 27% (RR = 0.73; 95% CI: [0.67–0.80]). Other forms of mistreatment declined by 45% (RR = 0.55; 95% CI: [0.53–0.58]) (Table 4).
Discussion
This study aims to evaluate the effect pre-post of an intervention focused on training healthcare providers and raising community awareness to prevent gynecological and obstetric mistreatment in Guinea. The results demonstrated an association between the intervention and a reduction in mistreatment in gynecological and obstetric services.
Multivariate analysis was associated with an overall reduction in the risk of experiencing mistreatment of 43% in gynecology (adjusted RR = 0.57; 95% CI: [0.53–0.62]) and 44% in obstetrics (adjusted RR = 0.56; 95% CI: [0.53–0.59]). In gynecology, reductions were observed for physical violence (30%; adjusted RR = 0.70; 95% CI: [0.63–0.78]), verbal violence (22%; adjusted RR = 0.78; 95% CI: [0.69–0.87]), and other forms of mistreatment (42%; adjusted RR = 0.58; 95% CI: [0.52–0.61]). In obstetrics, similar effects were noted, with decreases of 31% for physical violence (adjusted RR = 0.69; 95% CI: [0.64–0.76]), 27% for verbal violence (adjusted RR = 0.73; 95% CI: [0.67–0.80]), and 45% for other forms of mistreatment (RR = 0.55; 95% CI: [0.53–0.58]). All these changes were significant (p < 0.001) after adjusting for confounding variables.
Several mechanisms may explain these improvements. First, the intervention enhanced healthcare providers’ ability to recognize mistreatment and increased awareness among women of reproductive age regarding their sexual and reproductive health rights. This training strengthened providers’ competencies and encouraged behavioral change toward clients. Second, the establishment of a confidential and respectful complaint mechanism for victims of gynecological and obstetric mistreatment contributed to creating a more ethical work environment, reducing both verbal and physical abuse. The intervention also appeared to foster collective awareness among healthcare providers about respectful daily practices. Additionally, it sensitized healthcare professionals to women’s rights, which likely had a positive influence on their attitudes toward respectful maternity care. Consequently, healthcare providers offered better services and informed women more effectively about their rights. The study also revealed significant improvements in women’s attitudes toward obstetric mistreatment after the intervention.
These findings are consistent with recent literature. A review showed that interventions focused on communication and staff training significantly reduce abusive behavior in maternity wards.12 Other studies in Guinea have identified lack of training, heavy workload, and insufficient supervision as contributing factors to violence, and have demonstrated that targeted training improves caregiver–patient relationships.7,8 Moreover, participatory training programs in Sri Lanka and Togo improved healthcare providers’ behavior and reduced obstetric mistreatment.22,23
Awareness-raising activities increased recognition of such mistreatment and empowered women to defend their rights while encouraging healthcare professionals to provide respectful maternity care.20 Our results also align with a review highlighting the effectiveness of multi-component interventions-combining staff training and community outreach-in reducing mistreatment during maternal care by 18% to 66%.30 Some programs also show significant improvements in communication and practices in obstetric services.31 While others emphasize the importance of integrated approaches to achieve lasting reductions in physical and verbal violence.32 These findings support the idea that continuous training and community awareness are essential for establishing a culture of respectful care in gynecology and obstetrics services.
Strengths and Limitations
This study is among the first to evaluate the effects pre-post of an intervention combining training for healthcare providers and community outreach to prevent mistreatment in gynecology and obstetrics services. The use of a pre-post intervention study allowed for a direct assessment of the intervention’s association on reducing mistreatment. The study was conducted in five health districts representing the four natural regions of Guinea, giving the results strong external validity.
Despite including many relevant variables and providing a robust basis for conclusions, some limitations must be acknowledged. The absence of a control group limits causal attribution exclusively to the intervention. Additionally, the short-term evaluation (immediately post-intervention) prevents an assessment of the sustainability of behavioral changes among healthcare providers. Though we adjusted our analyses, residual bias cannot be totally excluded. The women interviewed may have underreported or overreported of mistreatment depending on their memory or perception of the intervention.
Implications for Research and Practice
The results of this study have important implications for improving the quality of obstetric and gynecological care in Guinea. The association to a significant reduction in mistreatment following the intervention confirms that combining healthcare provider training with community awareness is an effective strategy for promoting respectful maternal care. Future research should adopt longitudinal designs to assess the long-term sustainability of these effects.
Conclusion
This quasi-experimental, before-and-after study without a control study conducted in Guinea demonstrated the significant association of an intervention combining healthcare provider training and community outreach in reducing mistreatment in gynecology and obstetrics services. The results show a statistically significant decline in overall violence-including physical, verbal, and other forms in both specialties. However, the lack of a control group limit causal attribution. Policymakers may consider integrating similar interventions, ideally with controlled designs to confirm effectiveness into national maternal and reproductive health plans. Future studies should include control groups and longer follow up to assess sustainability.
Abbreviations
CR, Community Relays; CHW, Community Health Workers; CI, Confidence Interval; FDA, French Development Agency; HC, Health Center; RR, Relative Risk; WHO, World Health Organization.
Ethical Approval
The study was approved by the Institutional Ethics Committee in Guinea (No. 162/CNERS/21, dated 01 November 2021).
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request.
Acknowledgments
We express our gratitude to the French Development Agency for funding this research project and to the consortium of Amref Health Africa and Center for Research in Reproductive Health in Guinea (CERREGUI) for implementing it.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by the French Development Agency (FDA).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Afulani PA, Phillips B, Aborigo RA, Moyer CA. Person-centred maternity care in low-income and middle-income countries: analysis of data from Kenya, Ghana, and India. Lancet Glob Health. 2019;7(1):e96–13. doi:10.1016/S2214-109X(18)30403-0
2. World health Organization. WHO recommendations on intrapartum care for a positive childbirth experience. World Health Organization; 2018. 210.
3. Bohren MA, Vogel JP, Hunter EC, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. 2015;12(6):e1001847. doi:10.1371/journal.pmed.1001847
4. Vogel JP, Bohren MA, Tunçalp Ö, et al. How women are treated during facility-based childbirth: development and validation of measurement tools in four countries - Phase 1 formative research study protocol. Reprod Health. 2015;12:60. doi:10.1186/s12978-015-0047-2
5. Chervenak FA, McLeod-Sordjan R, Pollet SL, et al. Obstetric violence is a misnomer. Am J Obstet Gynecol. 2024;230(3):
6. Derrendinger I. Gynaecological and obstetrical violence, everyone’s business. Wise Women. 2021;20(6):10–13.
7. Sall AO, Diallo R, Balde MD, et al. Mistreatment in the gynaecology and obstetrics units of health facilities: community women’s experiences in Guinea. Int J Reprod Contracept Obstet Gynecol. 2024;13(5):1111–1116. doi:10.18203/2320-1770.ijrcog20241051
8. Balde MD, Diallo R, Kourouma K, et al. Frequency and factors associated with women’s mistreatment in obstetric units in Guinea. Int J Reprod Contracept Obstet Gynecol. 2025;14(1):37–46. doi:10.18203/2320-1770.ijrcog20243924
9. Balde MD, Diallo BA, Bangoura A, et al. Perceptions and experiences of the mistreatment of women during childbirth in health facilities in Guinea: a qualitative study with women and service providers. Reprod Health. 2017;14(1):3. doi:10.1186/s12978-016-0266-1
10. Tajvar M, Alipour S, Atashbahar O, Shakibazadeh E, Saeed AS, Khaledian Z. Promoting respectful maternity care: a quasi-experimental study on the effectiveness of an educational intervention in Iranian hospitals. Reprod Health. 2025;22(1):40. doi:10.1186/s12978-025-01969-4
11. Oluwaseyi OT, Sowunmi CO. Drivers of disrespect and abuse in obstetric care: an integrated review. Int J Nurs. 2024;10(2):57–73.
12. Yalley AA, Jarašiūnaitė-Fedosejeva G, Kömürcü-Akik B, de Abreu L. Addressing obstetric violence: a scoping review of interventions in healthcare and their impact on maternal care quality. Front Public Health. 2024;12:1388858. doi:10.3389/fpubh.2024.1388858
13. Mutiso P. Obstetric Violence in Sub-Saharan Africa: the Struggle for Dignified Maternal Care. 2024. Available from: https://www.newsecuritybeat.org/2024/12/.
14. Shamu S, Abrahams N, Temmerman M, Musekiwa A, Zarowsky C. A systematic review of african studies on intimate partner violence against pregnant women: prevalence and risk factors. PLoS One. 2011;6(3):e17591. doi:10.1371/journal.pone.0017591
15. Gebeyehu NA, Adella GA, Tegegne KD. Disrespect and abuse of women during childbirth at health facilities in Eastern Africa: systematic review and meta-analysis. Front Med. 2023;10:1117116. doi:10.3389/fmed.2023.1117116
16. Hakimi S, Allahqoli L, Alizadeh M, et al. Global prevalence and risk factors of obstetric violence: a systematic review and meta‐analysis. Int J Gynecol Obstet. 2025;169(3):1012–1024. doi:10.1002/ijgo.16145
17. World Health Organization. World Health Organization. The Prevention and Elimination of Disrespect and Abuse During Facility-Based Childbirth: WHO Statement WHO/RHR/14.23. Geneva: World Health Organization; 2015.
18. Ndembi Ndembi AP, Mekuí J, Pheterson G, Alblas M. Midwives and post-abortion care in Gabon: « things have really changed ». Health Hum Rights. 2019;21(2):145–155.
19. Ahmed W, Mochache V, Stein K, et al. A hybrid, effectiveness-implementation research study protocol targeting antenatal care providers to provide female genital mutilation prevention and care services in Guinea, Kenya and Somalia. BMC Health Serv Res. 2021;21(1):109. doi:10.1186/s12913-021-06097-w
20. Taye A, Belachew T. Effect of person-centered intervention on women’s knowledge and attitude towards obstetric violence during facility childbirth in southwest Ethiopia: a quasi-experimental study. BMC Public Health. 2025;25(1):1475. doi:10.1186/s12889-025-22734-z
21. Jardim DMB, Modena CM. Obstetric violence in the daily routine of care and its characteristics. Rev Lat Am Enfermagem. 2018;26:e3069. doi:10.1590/1518-8345.2450.3069
22. Swahnberg K, Zbikowski A, Wijewardene K, et al. Can forum play contribute to counteracting abuse in health care? A pilot intervention study in Sri Lanka. Int J Environ Res Public Health. 2019;16(9):1616. doi:10.3390/ijerph16091616
23. Mathonnet A, Arvis P. Training of health care personnel on obstetric violence: an experience in togo using the forum theatre technique. Epidemiol Public Health. 2023;1(1):1002. doi:10.52768/EpidemiolPublicHealth/1002
24. Shabot SC. We birth with others: towards a Beauvoirian understanding of obstetric violence. Eur J Womens Stud. 2021;28(2):213–228. doi:10.1177/1350506820919474
25. Kolié D, Sow A, Ghesquiere G, et al. Insights into perceptions, responses, and challenges experienced by women and girls’ survivors of sexual violence and their communities in rural Guinea, 2020. Front Glob Womens Health. 2024;5:1365601. doi:10.3389/fgwh.2024.1365601
26. Keith T, Hyslop F, Richmond R. A systematic review of interventions to reduce gender-based violence among women and girls in Sub-Saharan Africa. Trauma Violence Abuse. 2023;24(3):1443–1464. doi:10.1177/15248380211068136
27. Diallo R, Balde MD, Kourouma K, et al. Mistreatment of women during gynecological care in health facilities in Guinea. Int J Reprod Contraception Obstet Gynecol. 2024;14(1):5–12. doi:10.18203/2320-
28. Socieux+. Terms of reference for on-site activities and missions: strengthening the public-private partnership strategy in health and social health protection of the regional directorate of health and public hygiene of the City of Conakry (Guinea). 2024. Report
29. Ministry of Health. Health Statistical Yearbook 2017. Conakry: Ministry of Health, Republic of Guinea; 2017.
30. Kasaye H, Sheehy A, Scarf V, Baird K. The roles of multi-component interventions in reducing mistreatment of women and enhancing respectful maternity care: a systematic review. BMC Pregnancy Childbirth. 2023;23(1):305. doi:10.1186/s12884-023-05640-3
31. Tercan C, Yeniocak AS, Dagdeviren E, Akay E. Effect of mother-baby friendly facility accreditation on midwifery staff’s perceptions of obstetric mistreatment. Gynecol Obstet Reprod Med. 2025;31(1):24–31.
32. Downe S, Nowland R, Clegg A, et al. Theories for interventions to reduce physical and verbal abuse: a mixed methods review of the health and social care literature to inform future maternity care. PLOS Glob Public Health. 2023;3(4):e0001594. doi:10.1371/journal.pgph.0001594
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.