Back to Journals » International Journal of Women's Health » Volume 8
Effect of aerobic exercise during pregnancy on antenatal depression
Authors El-Rafie M, Khafagy G ![]() , Gamal M
, Gamal M
Received 10 August 2015
Accepted for publication 12 October 2015
Published 24 February 2016 Volume 2016:8 Pages 53—57
DOI https://doi.org/10.2147/IJWH.S94112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Mervat M El-Rafie,1 Ghada M Khafagy,2 Marwa G Gamal3
1Department of Public Health, 2Department of Family Medicine, Faculty of Medicine, Cairo University, Giza, Egypt; 3Family Health Unit, Ministry of Health, Cairo, Egypt
Background: Antenatal depression is not uncommon and is associated with a greater risk of negative pregnancy outcomes.
Aim: Exploring the effect of exercise in preventing and treating antenatal depression.
Methods: This was a prospective interventional controlled study carried out in 100 pregnant women treated at the Ain-Shams Family Medicine Center and Maadi Outpatient Clinic, Cairo, Egypt. The participants were divided into two groups (n=50 in the exercise group and n=50 in the control group). The exercise group regularly attended supervised sessions for 12 weeks. The activities in each session included walking, aerobic exercise, stretching, and relaxation. The control group completed their usual antenatal care. The Center for Epidemiological Studies Depression Scale (CES-D) was used to assess depression symptoms at the first interview and immediately after the 12-week intervention.
Results: Compared to the control group, the exercise group showed significantly improved depressive symptoms as measured with the CES-D after the 12-week intervention on the CES-D (P=0.001). Within groups, the exercise group demonstrated a significant improvement of depressive symptoms from baseline to intervention completion, while the control group demonstrated no significant changes over time.
Conclusion: Exercise during pregnancy was positively associated with reduced depressive symptoms.
Keywords: antenatal depression, pregnant women, exercise
Introduction
Many physical changes, as well as emotional disturbance, occur during pregnancy.1 In addition to external physical changes, some mental health problems such as depression and psychosis significantly increase during pregnancy and in the immediate postnatal period.2 Subtle changes experienced by pregnant women can transform their ability to carry out their normal roles and may affect their quality of life, even if the pregnancy is normal.1
Major depressive disorder (MDD) during pregnancy is neither uncommon nor benign, and its prevalence is estimated as 10%–13%.3 However, women who live in low- and middle-income countries are more vulnerable to both ante- and post-natal depression.4 An African study estimated an antenatal depression prevalence rate of 35%–50%.5 In Egypt, it was found that a significant proportion of pregnant women (~60%) experience prenataldepression.6,7 Studies found that pre- and perinatal complications such as premature labor, low birth weight, poor self-care, compromised mother–child bonding, and longer hospital stay are increased in subjects with depression and prenatal stress.8,9 Antenatal depression is also a strong predictor of postnatal depression; a previous study reported that symptoms in many women with postpartum depression started during pregnancy.10
Interventions for antenatal depression include antidepressants, psychotherapy, physical activity, and alternative therapies.11 As the fetus also indirectly receives the mother’s treatment, many physicians and patients prefer alternatives to medication during pregnancy.12 Even though medication can be used during pregnancy in patients with severe MDD, a number of reports have raised questions about the safety of psychotropic drug use during pregnancy.13 Psychotherapy is a good treatment choice, but it is underutilized for a variety of reasons.14 Therefore, a safe and accessible alternative treatment for antenatal depression is needed. Exercise was previously reported to alleviate MDD symptoms,15 and it is usually the first recommended lifestyle modification to reduce morbidity and mortality.16 We hypothesized that regular exercise may improve antenatal depression.
There have been a few controlled studies to assess the effect of exercise on mood during pregnancy. We aim to explore the effect of exercise in preventing and treating antenatal depression.
Methods
Study design
The study employed a prospective, interventional, controlled design to evaluate the effect of exercise on antenatal depression.
Study site and participants
The study was conducted in Ain-Shams Family Medicine Center Outpatient Clinic and Maadi Clinic, Egypt. The study site was purposefully selected due to the high number of patients treated and the cooperation of health-care workers. In addition, there are few centers concerned with promoting exercise by pregnant women in Cairo. Each clinic was visited once weekly from August 2012 until March 2013. An advertisement was distributed at both clinics describing the research subject and study benefits.
Of 120 pregnant women aged between 20 and 35 years in their second trimester who were enrolled in the study, 100 pregnant women were included in the analyses. Ten participants in both experimental and control groups were lost to follow-up before the 12-week assessment. Participants in the exercise group who attended 29 out of 36 sessions were included in the analysis. Exclusion criteria for the study participants were the presence of known chronic medical conditions such as psychiatric or cardiovascular diseases, risk of preterm labor, old primigravida, patients with previous repeated abortion, polyhydramnios, oligohydramnios, persistent bleeding after the first trimester, uncontrolled thyroid disorder, placenta previa, incompetent cervix,17 or history of infertility. Study participants were equally distributed into two groups. Group 1 (n=50) received the usual prenatal care plus aerobic exercise, and Group 2 (n=50) only received the usual prenatal care.
Study tools
A routine antenatal sheet with a precoded structured questionnaire was used to obtain patients’ histories. A medical examination was completed and documented in a special checklist developed for the purpose of the study. Each subject completed the 20-item Center for Epidemiologic Depression (CES-D) developed by Radloff and Rae.18 The cutoff point for depression on this scale was 16. The CES-D is a suitable instrument for screening for probable MDD among pregnant women receiving antenatal services. It has excellent internal consistency (Cronbach’s α=0.912). Furthermore, the CES-D discriminates well between MDD cases and noncases.19,20
Intervention
All participants underwent focused medical examinations in the initial screening before recruitment. After subject recruitment, follow-up continued for the next 12 weeks. In addition to normal prenatal care, the experimental group regularly attended supervised exercise sessions for 12 weeks (three 60-minute exercise classes per week), commencing at 16–27 weeks of gestation. Each session includes warm-up (10 minutes); aerobic exercise (30 minutes) such as step aerobics (low-step level), stationary bicycling, or treadmill walking; stretching (10 minutes) such as Kegel exercises, pelvic curl, tailor press, back bridge, and crunches; and relaxation (10 minute) such as bending to relieve backache, arm reaches, and shoulder circles. Aerobic activities were prescribed at moderate-to-vigorous intensity. The music-accompanied sessions were supervised by a physician and physiotherapist and were conducted in small groups in a well-ventilated room. The control group continued their normal prenatal care and did not attend the exercise classes. However, the benefits of supervised exercise and its effects on health status were discussed. Symptoms of depression were assessed in all participants using the CES-D in the first interview and immediately after the 12-week intervention.
Statistical analysis
The data were coded and entered using 2010 Microsoft Excel Software (Microsoft Inc., Redmond, WA, USA). Data were analyzed using the Statistical Package of Social Science Software program, version 21 (IBM Corp., Armonk, NY, USA). Quantitative data were summarized as means and standard deviations, and frequencies and percentages were calculated for qualitative data.
Independent sample t-tests were used to compare quantitative variables, and chi square or Fisher’s exact tests were used for qualitative data.
Paired measurements were compared using paired t-tests for quantitative data and chi square or marginal homogeneity tests for qualitative variables.
Ethical consideration
The study was approved by the Family Health and Public Health Councils. Selected members constituted the internal review board to guarantee the ethical conformity of the study. Official approvals were obtained from the managers of the Ain-Shams primary health-care center and Maadi clinic. Informed verbal consent was obtained from all participants before study enrollment after explaining the objectives of the work and procedures. All questionnaire forms and clinical sheets were coded before entry into the secure database to preserve confidentiality.
Results
The baseline characteristics of the participants are shown in Table 1. The mean ages were 26.7 (standard deviation: 2.3) and 28.4 (standard deviation: 2.6) in the exercise and control groups, respectively. In the exercise group, 56% of subjects were primiparous compared to 8% in the exercise group. More subjects in the exercise group were employed (80.0% vs 54%).
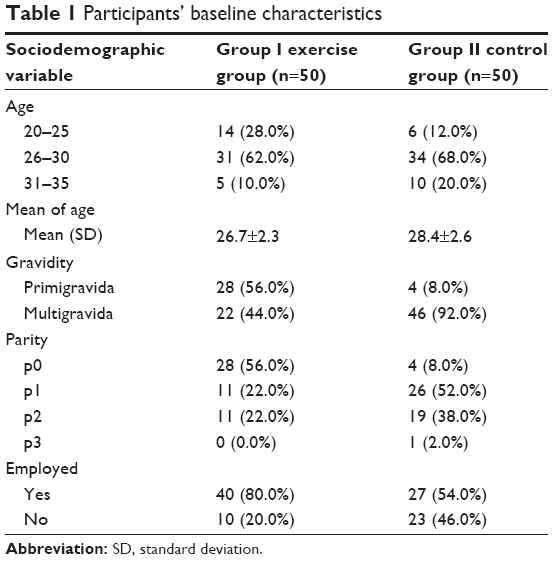 | Table 1 Participants’ baseline characteristics |
As shown in Table 2, there was no significant difference regarding depression score at baseline between Groups I (20.2±6.4) and II (20.0±6.7) (P=0.9). After 12 weeks, the exercise group had a significantly lower depressive symptom score than the control group (P<0.001). The exercise group demonstrated a significant improvement of depressive symptoms after the aerobic exercise program compared to baseline (P<0.001), while the control group demonstrated no significant change over time.
 | Table 2 Depression scores and severities in both groups |
To further examine the relationship between depressed mood and exercise participation, an established cutoff score on the CES-D of 16 was used to classify women as depressed, mild to moderately depressed, or not depressed. At baseline, there was no significant difference between the two groups regarding depression severity. After the intervention, the number of patients in Group I who had no depression, mild-to-moderate depression, and severe depression were 23, 23, and 4, respectively (Table 2). The corresponding numbers of nonexercisers in Group II with different levels of depression were 9, 15, and 26 (P<0.001).
Discussion
We observed a significant reduction in depressive symptoms in Group I following 3 months of supervised aerobic exercise compared to the control subjects in Group II. The final difference between the two groups was 5 points on the 20-point CES-D scale.
At baseline, there was no significant difference between depression scores in Groups I and II (20.2±6.4 vs 20.0±6.7, P=0.9). The high prevalence of depression among women in our study may have been influenced by the political situation of the country during the study period.
These findings add to the body of evidence describing a beneficial effect of exercise during pregnancy. Another study reported that exercise helps in the management of chronic conditions such as diabetes and hypertension, decreases cancer risk, helps in healthy weight maintenance, and offers cardiovascular protection.21
This result was consistent with the 2012 results by Robledo-Colonia et al22 who reported reduced depressive symptoms by 4 points on the CES-D scale when comparing exercising and nonexercising nulliparous groups. Another study of pregnant adolescents found that a 6-week exercise program resulted in increased total self-esteem and a significant decrease in depressive symptoms.23 Goodwin et al24 found that an exercising nulliparous group had a higher psychological well-being score with improvements in somatic symptoms, anxiety, and insomnia, compared to the control group.
Some theories suggest that depression etiologies include hippocampus dysfunction and impaired neurotransmitter activity. Antidepressant medical treatment is based on the hypothesis that neurotransmitter uptake is impaired in mood disorders. Exercise has been found to enhance dopamine, serotonin, and noradrenergic activities in the central nervous system.25 Hippocampal neurogenesis seems to have a positive role in the treatment of psychiatric disorders including depression.26
The available evidence suggests that inactivity during pregnancy is associated with worse mood; women who are physically active during their third trimester were found to be less anxious than inactive women.27
Choosing a suitable and safe treatment for depressed pregnant women is a complex process. In addition to that, alternative treatments for antenatal depression have not been rigorously studied.28 Accessing traditional psychotherapy treatment is difficult for some women due to financial constraints. Thus, other antenatal depression treatments are needed.29
Our findings reveal the importance and cost-effectiveness of supervised exercise during pregnancy in improving antenatal mood changes, in addition to its other health benefits.
Limitations
This study had several limitations that should be acknowledged. The participants and the physicians were not blinded. The feasibility of physical activity during pregnancy may be affected by many barriers (eg, child care responsibilities, work commitments, and pregnancy symptoms). This intervention should be promoted as women are often highly motivated to improve their health to benefit their children, and pregnancy represents an ideal opportunity to adopt healthy lifestyle changes.
The two groups were not similar in gravidity. We initially planned to include primi- and multigravida subjects in our study, but sample selection was mainly based on the patient’s acceptance of the study protocol, and many follow-up losses from the exercise group were multigravida because they had more responsibilities and could not commit to regular participation.
As the pregnancy exercise course has a monthly cost apart from usual antenatal care, many of the intervention group who completed the study were employed and could afford the fee. This likely explains the difference in employment rate between the two groups.
Future randomized controlled trials should study the effects of exercise on antenatal depression in comparison with other treatment modalities. They should also explore the effect of physical exercise on psychological status and assess life quality during pregnancy.
Conclusion
Our results suggest that supervised exercise during pregnancy has a positive effect on antenatal depression as a primary and secondary preventive strategy. Moreover, it is cost-effective, has no side effects, and is time saving compared to other modalities of depression treatment. Indeed, exercise has many advantages that may make it a suitable treatment for depression in pregnancy. Physicians should increase patient awareness of the benefits of exercise for pregnant women and their offspring, and its role in treating antenatal depression.
Disclosure
The authors report no conflicts of interest in this work.
References
Montoya Arizabaleta AV, Orozco Buitrago L, Aguilar de Plata AC, Mosquera Escudero M, Ramírez-Vélez R. Aerobic exercise during pregnancy improves health-related quality of life. A randomised trial. J Physiother. 2010;56(4):253–258. | ||
Stewart DE. Depression during pregnancy. N Engl J Med. 2011;365(17):1605–1611. | ||
Gaynes B, Gavin N, Meltzer-Brody S, et al. Perinatal depression prevalence, screening accuracy, and screening outcomes. Evid Rep Technol Assess. 2005;119:1–8. | ||
Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic review. Obstet Gynecol. 2004;103(4):698–709. | ||
Rochat TJ, Tomlinson M, Bärnighausen T, Newell ML, Stein A. The prevalence and clinical presentation of antenatal depression in rural South Africa. J Affect Disord. 2011;135(13):362–373. | ||
Sabri Y, Nabel H. The impact of anxiety and depression during pregnancy on fetal growth and the birth outcome. Egypt J Psychiatry. 2015;36(2):95–100. | ||
Moussa S, Refaat O, Emad M, Khoweiled A, Goueli T, Ezzat M. Correlates of antenatal bonding (an Egyptian Study). Egypt J Psychiatry. 2012;33(3):126–134. | ||
Wadhwa PD. Psychoneuroendocrine processes in human pregnancy influence fetal development and health. Psychoneuroendocrinology. 2005;30(8):724–743. | ||
Cooper PJ, Murray L, Wilson A, Romaniuk H. Controlled trial of the short- and long-term effect of psychological treatment of post-partum depression. Impact on maternal mood. Br J Psychiatry. 2003;182(5):412–419. | ||
Marcus SM. Depression during pregnancy: rates, risks and consequences – mother risk update. Can J Clin Pharmacol. 2009;16(1):e15–e22. | ||
Rethorst CD, Wipfli BM, Landers DM. The antidepressive effects of exercise: a meta-analysis of randomized trials. Sports Medicine. 2009;39(6):491–511. | ||
Payne JL, Meltzer-Brody S. Antidepressant use during pregnancy: current controversies and treatment strategies. Clin Obstet Gynecol. 2009;52(3):469–482. | ||
Bonari L, Koren G, Einarson TR, Jasper JD, Taddio A, Einarson A. Use of antidepressants by pregnant women: evaluation of perception of risk, efficacy of evidence based counseling and determinants of decision making. Arch Women Ment Health. 2005;8(4):214–220. | ||
Olfson M, Marcus SC. National trends in outpatient psychotherapy. Am J Psychiatry. 2010;167(12):1456–1463. | ||
Hoffman BM, Babyak MA, Craighead WE, et al. Exercise and pharmacotherapy in patients with major depression: one-year follow-up of the SMILE study. Psychosom Med. 2011;73(2):127–133. | ||
Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report. Washington, DC: Department of Health and Human Services. 2008. | ||
Artal RO, Toole M. Guidelines of the American college of obstetricians and gynecologists for exercise during pregnancy and the postpartum period. Br J Sport Med. 2003;37(1):6–12. | ||
Radloff LS, Rae DS. Susceptibility and precipitating factors in depression: sex differences and similarities. J Abnorm Psychol. 1979;88(2):174–181. | ||
Natamba BK, Achan J, Arbach A, et al. Reliability and validity of the center for epidemiologic studies-depression scale in screening for depression among HIV-infected and -uninfected pregnant women attending antenatal services in northern Uganda: a cross-sectional study. BMC Psychiatry. 2014;14:303. | ||
Canady RB, Stommel M, Holzman C. Measurement properties of the Centers for Epidemiological Studies Depression Scale (CES-D) in a sample of African-American and non-hispanic white pregnant women. J Nurs Meas. 2009;17(2):91–104. | ||
Rosendorff C, Black HR, Cannon CP, et al. Treatment of hypertension in the prevention and management of ischemic heart disease: a scientific statement from the American Heart Association Council for High Blood Pressure Research and the Councils on Clinical Cardiology and Epidemiology and Prevention. Circulation. 2007;115(21):2761–2788. | ||
Robledo-Colonia AF, Sandoval-Restrepo N, Mosquera-Valderrama YF, et al. Aerobic exercise training during pregnancy reduces depressive symptoms in nulliparous women: a randomized trial. J Physiother. 2012;(58):9–15. | ||
Koniak-Griffin D. Aerobic exercise, psychological well-being, and physical discomforts during adolescent pregnancy. Res Nurs Health. 1994;17(4):253–263. | ||
Goodwin A, Astbury J, McMeeken J. Body image and psychological well-being in pregnancy. A comparison of exercisers and non-exercisers. Aust N Z J Obstet Gynaecol. 2000;40(4):442–447. | ||
Ploughman M. Exercise is brain food: the effects of physical activity on cognitive function. Dev Neurorehabil. 2008;11(3):236–240. | ||
Nestler EJ, Barrot M, DiLeone RJ, Eisch AJ, Gold SJ, Monteggia LM. Neurobiology of depression. Neuron. 2002;34(1):13–25. | ||
Poudevigne MS, O’Connor PJ. A review of physical activity patterns in pregnant women and their relationship to psychological health. Sports Med. 2006;36(1):19–38. | ||
Shivakumar G, Brandon AR, Snell PG, et al. Antenatal depression: a rationale for studying exercise. Depress Anxiety. 2011;28:234–242. | ||
Goodman JH. Women’s attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth. 2009;36(1):60–69. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.