Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Effect of a nonsurgical treatment program on the gait pattern of idiopathic toe walking: a case report
Authors Szopa A ![]() , Domagalska-Szopa M
, Domagalska-Szopa M ![]() , Gallert-Kopyto W
, Gallert-Kopyto W ![]() , Kiebzak W, Plinta R
, Kiebzak W, Plinta R ![]()
Received 25 August 2015
Accepted for publication 16 December 2015
Published 10 February 2016 Volume 2016:12 Pages 139—146
DOI https://doi.org/10.2147/TCRM.S95052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Andrzej Szopa,1 Małgorzata Domagalska-Szopa,2 Weronika Gallert-Kopyto,1 Wojciech Kiebzak,3 Ryszard Plinta4
1Department of Physiotherapy, 2Department of Medical Rehabilitation, School of Health Sciences, Medical University of Silesia, Katowice, 3Faculty of Health Sciences, Jan Kochanowski University, Kielce, 4Department of Adapted Physical Activity and Sport, School of Health Sciences, Medical University of Silesia, Katowice, Poland
Background: Recent studies have reported many possibilities for the treatment of idiopathic toe walking (ITW); however, none of them have been sufficiently documented. The purpose of this case study was to document the evolution of the gait pattern of a child with severe ITW using the Gillette Gait Index before and after the third and sixth weeks, a nonsurgical treatment program and then every 3 months to 1 year from the start of the treatment. This is significant because the case study shows that a nonsurgical treatment program can be an alternative treatment method for children with severe ITW.
Case description: The case study involved a 5-year-old boy diagnosed with severe ITW. An orthopedist recommended a surgical treatment, but his parents refused to provide consent.
Intervention: The subject participated in a 12-week nonsurgical treatment program that used tone-inhibiting casts (TICs) combined with physiotherapy based on neurodevelopmental treatment principles. The treatment protocol included the following: 1) precast preparation; 2) TICs with treatment; and 3) post-cast treatment to improve the gait pattern.
Outcomes: After treatment with TICs, the range of motion of ankle dorsiflexion during stance had increased, resulting in an almost normalized gait. The patient stopped toe walking for at least 1 year.
Discussion: This study demonstrates that nonsurgical treatment should be considered first, with surgical options reserved for resistant cases; however, further research is required given the current lack of knowledge about treatment outcomes using TICs and the wide use of this treatment modality in children with ITW.
Keywords: tone-inhibiting casts, NDT, ROM of ankle dorsiflexion, Gillette Gait Index
Background
A characteristic feature of idiopathic toe walking (ITW) is a persistent walk with a bilateral toe-walking pattern in children older than 3 years in the absence of a clinically diagnosed neuromuscular disease. The disease always affects both feet. Typically, children begin to walk at the age of 12–15 months. During the early stages of walking, children generally experiment with different foot positions, including walking on their toes, as a part of their motor experiences. By the third year of life, children are expected to walk with a heel–toe gait pattern.1 If walking on their toes persists, it is perceived as ITW, which is defined as toe walking in a child who has been evaluated by a physician and for whom no medical reason for ITW has been identified. ITW occurs in healthy and normally developing children, and it always occurs in both feet. The estimated incidence of ITW in the pediatric population varies from 7% to 24%.2,3
ITW has been defined as the failure of the heel to make contact with the floor at the onset of stance4 or as the absence of a heel rocker. In a normal gait, the term “heel rocker” refers to the progression of the limb with the heel as the pivotal area of support.5 The rear of the foot contacts the floor and rolls into ankle plantar flexion. Without a heel rocker phase, either the midfoot or forefoot touches the floor or the ankle moves toward ankle dorsiflexion (aDF).
Many authors have described the gait patterns of children with ITW based on a three-dimensional gait analysis.6–9 A classification system for the severity of ITW is based on ankle kinematic and kinetic data and comprises the presence of a first rocker, the presence of an early third rocker, and an early predominant first ankle moment.2 This classification includes three types: type 1 (mild), type 2 (moderate), and type 3 (severe).2
ITW is not the result of initial Achilles’ tendon (heel cord) tightness; however, a tight Achilles’ tendon may sometimes develop as a child grows, in which case the phenomenon is called a contracture. When this type of contracture occurs, children can no longer drop their heels to the ground. This situation can lead to complications with their foot and leg positions and can contribute to flat arches and/or outward-rotated leg development when the child tries to maintain heel contact with the ground.
The cause of ITW is not fully known. However, among the factors that could lead to ITW, the following are noteworthy: tactile processing (an increased response to touch sensations), altered proprioceptive processing (sensing the body’s position in space), altered vestibular processing (maintaining balance), visual processing, decreased flexibility of the leg and foot muscles, reduced overall body strength, and family history (parents or siblings with a history of toe walking).10
Recent studies have reported many possibilities for the treatment of ITW, including conservative methods, such as stretching, night splints, serial casting, and botulinum toxin type A (BTX-A) injections, for children with mild and moderate ITW and surgical intervention (Achilles tendon [heel cord] lengthening) for children with severe ITW.7–12 However, a consensus about medical management has not yet been established. There are a few reasons for this. First, there were differences in the base population both within and between studies with regard to pretreatment aDF angle and gait kinematic disturbances. Second, a variety of treatment modalities, algorithms, and posttreatment management strategies were reported. Third, a wide range of outcome measures and follow-up periods were applied, making it difficult to compare the effectiveness of different treatments. Moreover, no studies have evaluated the effects of the different interventions on the level of both body structure (aDF) and function (gait pattern) of children with ITW, as recommended by the World Health Organization International Classification of Functioning, Disability, and Health for Children and Youth. Therefore, the purpose of this case study was to document a nonsurgical treatment program that used tone-inhibiting casts (TICs) combined with neurodevelopmental treatment (NDT) in a 5-year-old boy diagnosed with severe and persistent ITW. The pre- and posttreatment body structure (range of motion [ROM] of aDF) and function (gait index) were compared. This is significant because TICs are generally successful for children with cerebral palsy (CP)13 but not with ITW.
No kinematic studies have explained the mechanisms of TICs in children with ITW; therefore, we can only theorize that the TICs in this case could work. First, in the presented case, the abnormal activity of the foot reflexes (toe-grasping reflex of the foot and support reflex of the legs) and the associated pattern of leg extension that affects foot progression during walking, which are similar to those of children with CP, were observed.
Chain responses following the initial toe-grasping reflex of the foot produce two further stages, which are most easily observed in the reflex. The first follows the initial flexion of the digits and consists of tensing the flexed muscles to produce a strong grasp. A strong tonic component at this stage of the reflex ensures maintenance of the grasp as long as the stimulus persists. The second stage occurs when traction is exerted by the stimulation. These reflexes are easily demonstrable in the neonate but fade rapidly and are seldom observed after 4 or 5 months of age.
The support reflex of the legs is activated when the feet come into contact with a hard substrate and the pressure on the soles causes a reflex extension of the legs. This complex reflex is important for the development of the upright posture and locomotion. Failure of this reflex to appear at the right time delays locomotor development. However, persistence long after it has served its purpose is a sign of neurological abnormality and produces characteristic abnormal gait patterns.
Compared with serial corrective casts, TICs affect heel cord stretching, and the inhibition bars reduce the stimulus to the reflexogeneous area of the toe-grasp reflex and support reflex. Placing the heel inside a TIC increases the ground reaction forces in the reflexogeneous area of the DF. The anterior extension in conjunction with the TICs increases the leverage, causing a downward moment at the calcaneus.
We hypothesized that the combination of increased aDF and inhibited hyperactivity of the foot reflexes (toe-grasping reflex of the foot and support reflex of the legs) can be useful in the treatment of young children with severe ITW by providing a persistent stretch to the gastrocnemius and soleus contractures and improving the gait pattern.
Case description
This case study describes a 5-year-old boy diagnosed with severe and persistent ITW. No risk factors were noted in his perinatal history, and there was no family history of ITW. His psychomotor development proceeded appropriately until the age of 2 years when he started to walk with a toe-walking gait pattern. ITW persisted until he was 4 years of age. Specifically, there was no evidence of increased muscle tone or altered reflexes, and there appeared to be no neuromuscular explanation for the toe walking. The patient exhibited no evidence of foot abnormalities, and the absence of neuromuscular disease, confirmed by magnetic resonance imaging, revealed the clinical diagnosis of ITW. Importantly, although this patient underwent 1 year of physical therapy (PT), including home exercises and nighttime bracing with plastic orthotics to maintain the stretch/flexibility of the Achilles’ tendons, his toe-walking condition worsened over time. In the opinion of an orthopedist, these developments were sufficiently severe to warrant corrective osteotomy, but the patient’s parents refused to provide consent. In this case, a 1-year, nonsurgical treatment program, including TICs combined with a PT program based on NDT principles, was offered and accepted by the parents of the patient.
With both knees in extension, he did not exhibit a passive aDF to neutral plantigrade. Upon clinical evaluation, hyperactivity of the toe-grasping reflex could be observed, which intensified with the placement of the subject in the upright position. The parents estimated that the patient spent 100% of his time on his toes. In addition, bilateral Achilles’ tendon contracture developed, both forefeet were splayed, and a disproportionately wide forefoot was observed compared with the heel and external tibial torsion, which frequently develops to compensate for the lack of a flat foot contact (Figure 1A).
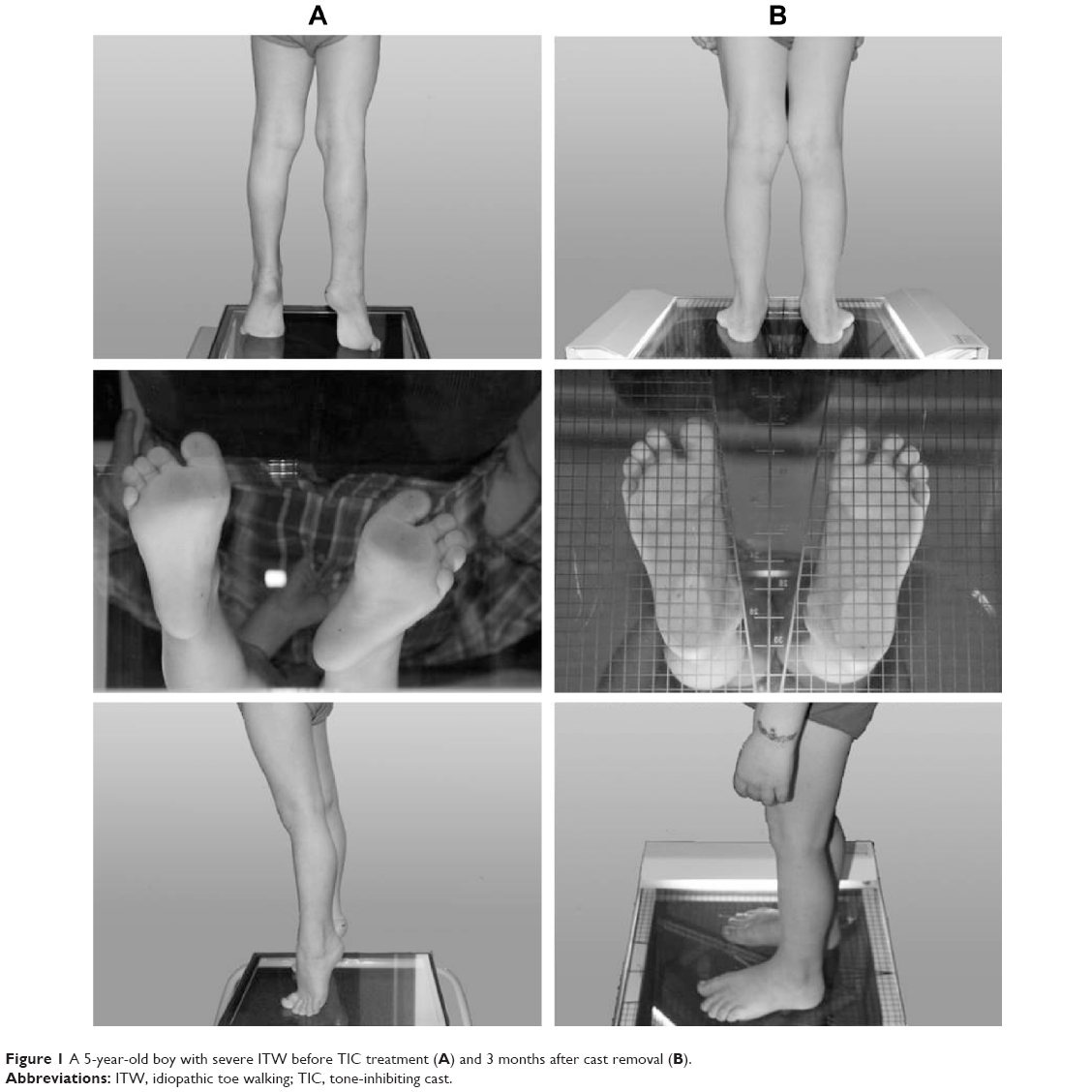 | Figure 1 A 5-year-old boy with severe ITW before TIC treatment (A) and 3 months after cast removal (B). |
Consent/Ethics
Written informed consent was obtained from the parents of the patient for the publication of this case report and any accompanying images. A copy of the written consent will be made available for review by the Editor-in-Chief of this journal. The Bioethical Committee of the Medical University of Silesia in Katowice, Poland approved the current report.
Intervention
Treatment program
The precasting treatment aimed to 1) inhibit an increased response to touch sensations; 2) inhibit abnormal reflex activity in posture and motor patterns (particularly positive support reactions); and 3) increase the ROM of aDF. The precasting protocol (3 weeks, five times per week for 60 minutes per session) included 1) inhibitory techniques of NDT based on sensory input, such as exteroceptive inputs (tactile stimulation), including manual guidance and the therapeutic use of different structures, and proprioceptive inputs, including weight bearing, approximation, stretching, and traction and pressure tapping directed at promoting increased proprioception during standing14 and 2) a stretching exercise without motion (heel cord passive stretching) performed by prolonged pulling down on the heel and pushing up on the foot15 while counting slowly to 25 (40 times) that was performed with the knee flexed at 90° and 20°. Pushing up on the foot requires continued hard pressure on the arch of the foot to prevent dislocation.
Bilateral short (below the knee) walking TICs were used for a period of 3 weeks in the presented case. The casts were applied with the patient in the supine position with the hip and knee flexed at 90°, and the leg and foot were established in the neutral position in all planes. An inhibition bar on both casts was used to reduce the stimulus to the reflexogeneous area of both the toe-grasping reflex of the foot and the support reflex of legs (Figure 2). The heels were strongly fixed inside the casts to increase the ground reaction forces in the reflexogeneous area of the foot reflexes. During casting, facilitation techniques of NDT, which used the improved postural tone in the casts in goal-directed balance activities and gait training, were emphasized.16 The treatment protocol (3 weeks, five times per week for 60 minutes per session) included 1) static balance training comprising the ability to maintain proper posture in different positions (~15 minutes), such as standing, standing with a step forward with a large and then narrow base of support and shifting to one limb; 2) dynamic balance training, which facilitates postural control when the body is moving on a stable surface and when the support surface is moving (~15 minutes); and 3) gait training on the treadmill (~30 minutes).
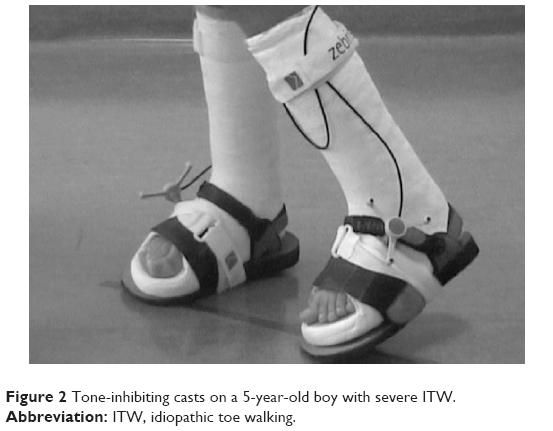 | Figure 2 Tone-inhibiting casts on a 5-year-old boy with severe ITW. |
Excluding plaster sores (pressure areas) and skin irritation after casting, no other adverse events were noted.
The post-cast treatment protocol (6 weeks, 5 days per week for 60 minutes per session) included 1) equilibrium reaction facilitation and balance training via different positions, such as standing with disturbance, standing with a step forward with disturbance, narrow base of support with disturbance, shifting with disturbance, and the use of a Biodex stability system to produce perturbation in all directions (15 minutes); 2) the facilitation of a gait pattern using manual guidance and the therapeutic use of hands during gait training on the treadmill (15 minutes); and 3) gait training in a closed environment using obstacles to transfer new sensorimotor experiences from treatment to everyday activities (15 minutes).
For the first gait training session, the speed of the treadmill was initially set at 90% of the child’s overground walking speed and was gradually increased at each session to increase the length of steps that the child took. The walking speed oscillated from 1.8 km/h in the first session to 3.2 km/h by the end of the treatment program. The incremental speed adjustments depended on the child’s ability to control his gait pattern.
Clinical examination and gait analysis
The pre- and post-cast deficits of passive ROM values around the ankle in two positions (Table 1) were measured separately for each lower limb using an accelerometer-based system,17 and a three-dimensional gait analysis was performed using the Compact Measuring System for 3D Real Time Motion Analysis and WinGait Software (Zebris Medizintechnik GmbH, Isny, Germany).18
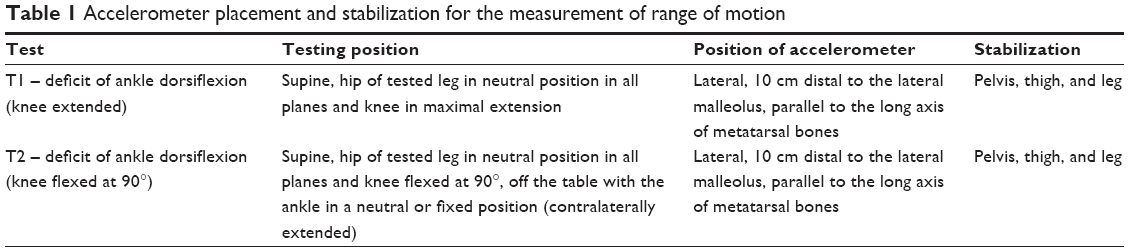 | Table 1 Accelerometer placement and stabilization for the measurement of range of motion |
Before the gait analysis, the following anatomical landmarks were identified using an instrumented pointer: hip joint center, knee rotation center (internal and external), ankle rotation center (internal and external), forefoot landmark (between the second and third metatarsals), and rear foot (heel). The subject was required to walk for at least 10 minutes on a treadmill without shoes. Five gait cycles for the right and left lower limbs were recorded. The data collected were reported using WinGait software.
To characterize the gait pattern, the Gillette Gait Index (GGI) was calculated separately for each lower limb using the procedure described by Schutte et al.19 The GGI uses a single number to measure the deviation of the patient’s gait from the average gait of a subject without pathology. The GGI is based on 16 selected gait parameters taken from objective gait analysis data: time of toe off (% gait cycle), walking speed/leg length, cadence (step per second), mean pelvic tilt (°), range of pelvic tilt (°), mean pelvic rotation (°), minimum hip flexion (°), range of hip flexion (°), peak abduction in swing (°), mean hip rotation in stance (°), knee flexion at initial contact (°), time of peak knee flexion in the swing (% gait cycle), range of knee flexion (°), peak DF in stance (°), peak DF in swing (°), and mean foot progression (°). In the simplest terms, the GGI can be considered a measure of the distance between the set of discrete variables describing a patient’s gait and the average of those variables in people with no gait abnormalities. The GGI has been shown to be efficient in categorizing the pathology in children with CP, clinically applicable19,20 and correlated with physical functioning.21 The precast examination included both clinical tests and a gait analysis before treatment and immediately before the TICs were applied. During post-cast follow-ups, the same examination was repeated immediately after cast removal and 6 weeks, 6 months, and 9 months later.
The examinations were conducted in a functional assessment laboratory at the Department of Physiotherapy, Medical University of Silesia, Katowice, Poland.
Outcomes
The precast examination revealed a large deficit of ROM of aDF, defined as the value from the neutral foot position in both tests (Figures 3 and 4). The GGI calculation (80.1 for the right and 92.7 for the left lower limb) revealed a strong deviation of the patient’s gait from a normal gait pattern (Figure 5). GGI values for typically developing children range from 8.2 to 26.9.19
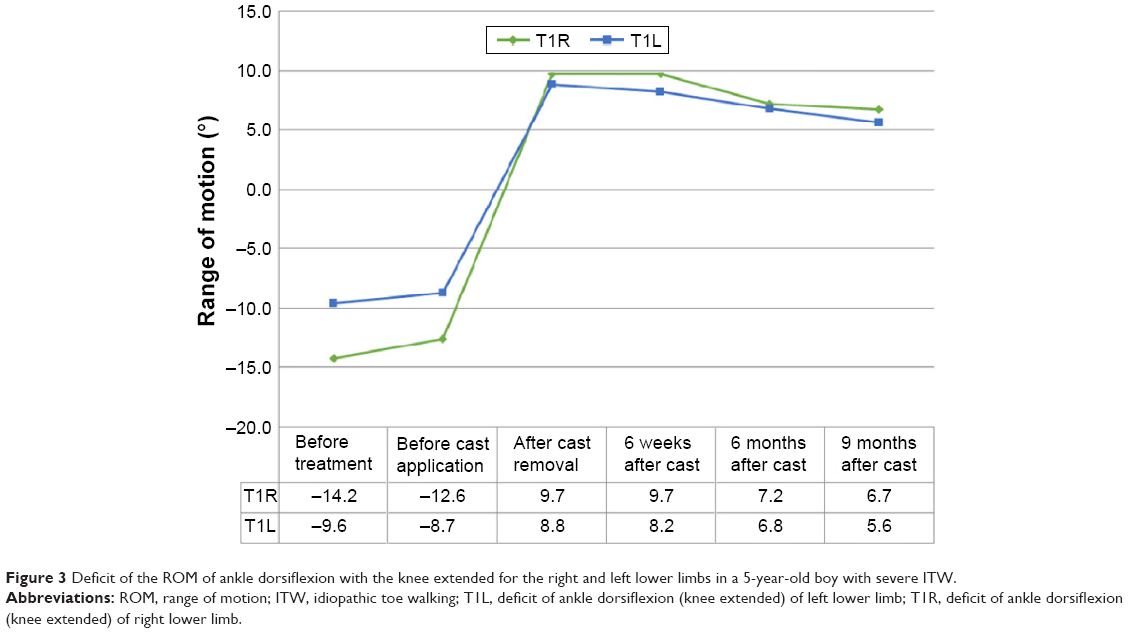 | Figure 3 Deficit of the ROM of ankle dorsiflexion with the knee extended for the right and left lower limbs in a 5-year-old boy with severe ITW. |
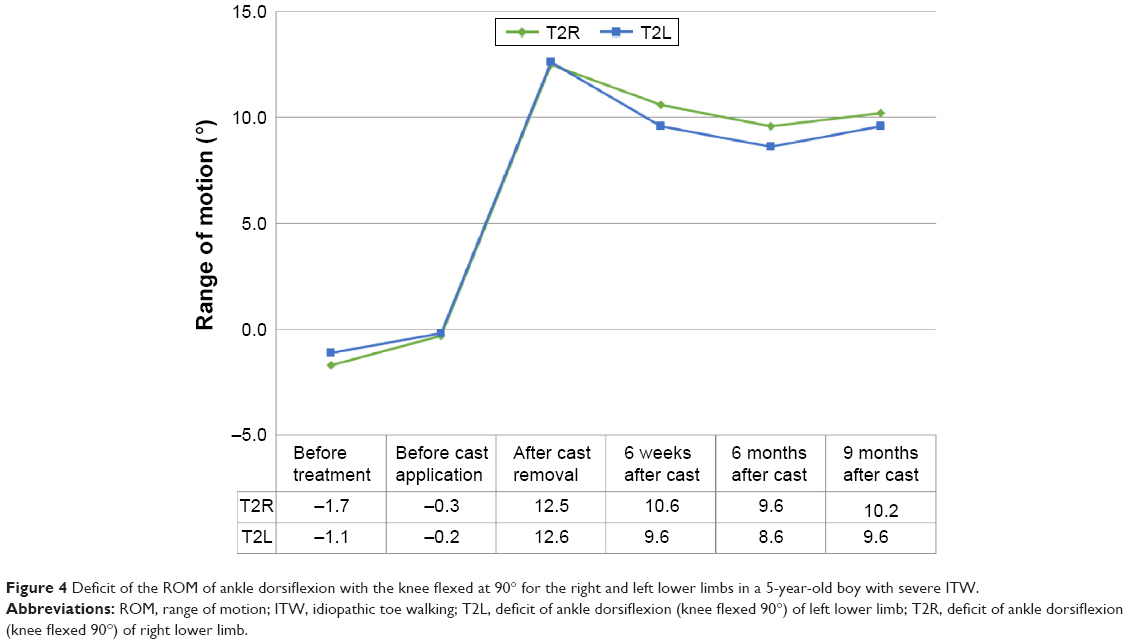 | Figure 4 Deficit of the ROM of ankle dorsiflexion with the knee flexed at 90° for the right and left lower limbs in a 5-year-old boy with severe ITW. |
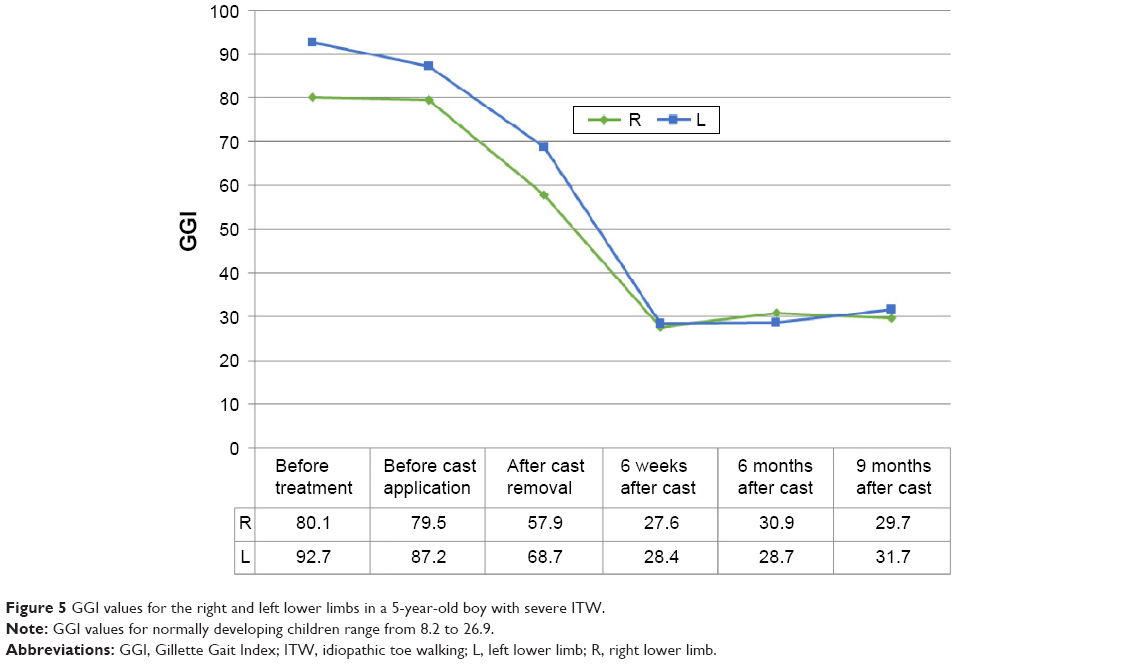 | Figure 5 GGI values for the right and left lower limbs in a 5-year-old boy with severe ITW. |
On the day of TIC application (after 3 weeks of precasting PT), the patient showed only a slight increase in the passive ROM of aDF in both tests with knee extension and knee flexion at 90°, while after cast removal, the ROM of aDF was close to normal and had stabilized at ~9° in both tests (with knee flexion at 90° and knee extension) in both lower limbs (Figures 3 and 4).
The foot-flat position and heel contact with the ground were maintained for both legs during standing, as shown in Figure 1B. Improvements in ankle ROM and its maintenance at the 6- and 9-month post-casting examinations are shown in Figures 3 and 4.
The post-casting gait analysis revealed a small degree of improvement in the gait pattern. A significant improvement in the gait pattern (confirmed by the GGI) did not appear immediately, but it was apparent at 6 weeks after cast removal (Figure 5). The evolution of the subject’s gait pattern, as indicated by the GGI, is shown in Figure 5. Although the final GGI values were not completely characteristic of a normal gait, the GGI values at 3, 6, and 9 months post casting were constant and close to those of normally developing children (Figure 5).
Discussion
ITW is not rare in pediatric orthopedic clinics, and it very often causes significant concern for parents. Toe-walking studies often discuss whether and how to treat ITW.12 The Cincinnati Children’s Hospital Medical Center expended significant effort and developed the Evidence-Based Care Guideline for the management of ITW. This guideline recommends the following sequence of treatment: 1) PT; 2) serial heel cord aDF casts (SC); 3) ankle foot orthosis; 4) Botox injections to the gastrocnemius and soleus (BTX-A); and 4) tendo-Achilles lengthening if other treatments fail.22
There is preliminary evidence of the beneficial effects of PT, SC, BTX-A, and surgery on passive aDF and the kinetics and kinematics of gait.23 Importantly, although all the examined subjects with ITW from the earlier-discussed studies kinematically revealed an increased ankle plantar flexion angle throughout the gait cycle before intervention, only children in the surgical studies had a severe pretreatment deficit of aDF, whereas the children in the cast and BTX-A studies usually presented a normal/near normal ROM of aDF before the treatment.23 SC and BTX-A appear to benefit ITW in the short term by improving aDF and stopping toe walking in most cases. However, the beneficial effects after conservative treatment (PT/casting) do not appear to be sustainable. Additionally, SCs are usually used in children with mild ITW.
Surgical treatment is typically reserved for children with severe ITW and significant ankle equinus.8 This method is effective, but whether the procedure is truly necessary remains unclear. Surgical treatment is the most reliable method in patients who do not respond to nonsurgical treatment, but it is also important to consider the associated potential complications. Surgeons often caution against overlengthening, which is the most common complication. The literature is unclear with respect to the natural history of ITW, whether nonoperative treatment is effective and whether the treatment is ever needed.
This case study is unique, because it documents a nonsurgical treatment program for a subject with severe and persistent ITW and a large aDF deficit as well as equinus contractures connected with external tibial torsion. In the opinion of an orthopedist, the patient required surgical treatment. After the treatment program, both the passive ROM of aDF and aDF during the stance phase increased significantly, resulting in an almost normalized gait, and the patient stopped toe walking for at least 1 year (see the successive GGI).
The treatment program combined TICs with PT based on the NDT approach as preparation for the TICs (precast treatment) as well as post-cast treatment for gait improvement. The aim of the proposed intervention was not only the improvement of the ROM of aDF but also the improvement of the gait pattern by inhibiting the hyperactivity of the foot reflexes (toe-grasping reflex of the foot and support reflex of legs). The proof that the aforementioned strategy was successful is the fact that despite the normalization of the ROM of aDF right after TIC removal, the gait did not show immediate improvements in aDF. This two-step improvement process was the deliberate action of inhibiting the previous abnormal gait pattern (by TICs) followed by facilitating a better gait pattern through the post-cast treatment.
This case study showed that a nonsurgical treatment program can be an alternative to invasive surgery for children with severe ITW. Follow-up research could fill a gap in the literature by reporting on the use of nonsurgical interventions, including TICs combined with PT based on the NDT approach, for children with severe ITW, for whom (invasive) surgery would be the traditional intervention.
Conclusion
This study indicates that nonsurgical treatment of ITW should be considered first, reserving surgical options for resistant cases; however, we acknowledge that this is only one case and further randomized trials are required. Suggestions for further research include a similar study with a larger number of subjects with severe ITW to determine the effect of nonsurgical treatment using TICs on gait patterns in children.
Author contributions
AS and MD-S participated in the conception and design of the study. AS and MD-S performed the experiments and interpreted the data. WG-K analyzed the data. MD-S and AS wrote the article. RP made critical revisions to the manuscript. All the authors reviewed and approved the final version of the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Sutherland D, Olshen R, Cooper L, Woo S. The development of mature gait. J Bone Joint Surg Am. 1980;62(3):336–353. | ||
Armand S, Watelain E, Mercier M, Lensel G, Lepoutre FX. Identification and classification of toe-walkers based on ankle kinematics, using a data-mining method. Gait Posture. 2006;23(2):240–248. | ||
Alvarez C, De Vera M, Beauchamp R, Ward V, Black A. Classification of idiopathic toe walking based on gait analysis: development and application of the ITW severity classification. Gait Posture. 2007;26(3):428–435. | ||
Perry J, Burnfield JM, Gronley JK, Mulroy SJ. Toe walking: muscular demands at the ankle and knee. Arch Phys Med Rehabil. 2003;84(1):7–16. | ||
Perry J, Davids JR. Gait analysis normal and pathological function. J Pediatr Orthop. 1992;12(6):815. | ||
Westberry DE, Davids JR, Davis RB, de Morais Filho MC. Idiopathic toe walking: a kinematic and kinetic profile. J Pediatr Orthop. 2008;28(3):352–358. | ||
McMulkin ML, Baird GO, Caskey PM, Ferguson RL. Comprehensive outcomes of surgically treated idiopathic toe walkers. J Pediatr Orthop. 2006;26(5):606–611. | ||
Stott NS, Walt SE, Lobb GA, Reynolds N, Nicol RO. Treatment for idiopathic toe-walking: results at skeletal maturity. J Pediatr Orthop. 2004;24(1):63–69. | ||
Glanzman AM, Kim H, Swaminathan K, Beck T. Efficacy of botulinum toxin A, serial casting, and combined treatment for spastic equinus: a retrospective analysis. Dev Med Child Neurol. 2004;46(12):807–811. | ||
Williams CM, Tinley P, Curtin M. Idiopathic toe walking and sensory processing dysfunction. J Foot Ankle Res. 2010;3:16. | ||
Clark E, Sweeney JK, Yocum A, McCoy SW. Effects of motor control intervention for children with idiopathic toe walking: a 5-case series. Pediatr Phys Ther. 2010;22(4):417–426. | ||
Dietz F, Khunsree S. Idiopathic toe walking: to treat or not to treat, that is the question. Iowa Orthop J. 2012;32:184–188. | ||
Domagalska M, Szopa A, Czupryna K, Nowotny J, Matyja M. “The inhibiting casts” used in cerebral palsed children. Ortop Traumatol Rehabil. 2006;8(3):291–299. | ||
Bundy AC, Lane S, Murray EA, editors. Sensory Integration: Theory and Practice. 2nd ed. Philadelphia, PA: FA Davis; 2002. | ||
Pin T, Dyke P, Chan M. The effectiveness of passive stretching in children with cerebral palsy. Dev Med Child Neurol. 2006;48(10):855–862. | ||
Mayston MJ. People with cerebral palsy: effects of and perspectives for therapy. Neural Plast. 2001;8(1–2):51–69. | ||
Domagalska M, Szopa A, Syczewska M, Pietraszek S, Kidoń Z, Onik G. The relationship between clinical measurements and gait analysis data in children with cerebral palsy. Gait Posture. 2013;38(4):1038–1043. | ||
Szopa A, Domagalska-Szopa M, Czamara A. Gait pattern differences in children with unilateral cerebral palsy. Res Dev Disabil. 2014;35(10):2261–2266. | ||
Schutte LM, Narayanan U, Stout JL, Selber P, Gage JR, Schwartz MH. An index for quantifying deviations from normal gait. Gait Posture. 2000;11(1):25–31. | ||
Assi A, Ghanem I, Lavaste F, Skalli W. Gait analysis in children and uncertainty assessment for Davis protocol and Gillette Gait Index. Gait Posture. 2009;30(1):22–26. | ||
Romei M, Galli M, Motta F, Schwartz M, Crivellini M. Use of the normalcy index for the evaluation of gait pathology. Gait Posture. 2004;19(1):85–90. | ||
LeCras S, Bouck J, Brausch S, Taylor-Haas A. Cincinnati Children’s Hospital Medical Center: Evidence-Based Clinical Care Guideline for Management of Idiopathic Toe Walking. 2011:1–17. Guideline 040. | ||
Van Kuijk AA, Kosters R, Vugts M, Geurts AC. Treatment for idiopathic toe walking: a systematic review of the literature. J Rehabil Med. 2014;46(10):945–957. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.