Back to Journals » International Medical Case Reports Journal » Volume 18
Ectopic Pregnancy within a Cesarean Section Scar: An Unusual Case Report
Authors AL-Osail EM ![]() , Almulhim S
, Almulhim S
Received 6 January 2025
Accepted for publication 24 April 2025
Published 1 May 2025 Volume 2025:18 Pages 521—527
DOI https://doi.org/10.2147/IMCRJ.S515912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Emad M AL-Osail,1 Sager Almulhim2
1Department of General Surgery, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2General Radiology, Imam Abdulrahman Bin Faisal Hospital-National Guard, Dammam, Saudi Arabia
Correspondence: Emad M AL-Osail, Department of General Surgery, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Email [email protected]
Abstract: Ectopic pregnancy represents a significant challenge in obstetrics due to its potential for severe complications, including maternal morbidity and mortality. Caesarean scar ectopic pregnancy is one of the very rare sites of ectopic pregnancy. Any type of surgical scar on the uterine wall (hysterotomy) including caesarean section, myomectomy or history of abnormally adherent placenta or manual removal of placenta increases the risk of surgical scar ectopic pregnancy. Here, we have described a case of caesarean scar ectopic pregnancy in a 43 years female presenting to the emergency department after being referred from a primary centre with complaints of pelvic pain and vaginal bleeding. Ultrasound confirmed the diagnosis of caesarean section scar ectopic pregnancy. The patient was successfully managed with multi dose regime of methotrexate. Early diagnosis and prompt management of caesarean scar ectopic pregnancy is essential to avoid any life-threatening complications or loss of fertility.
Keywords: ectopic, pregnancy, caesarean section scar, hysterotomy, methotrexate
Introduction
Ectopic pregnancy at the site of caesarean section scar is a very rare complication of pregnancy. Studies show that around 1 such case occurs out of 2000 pregnancies.1–3 However, with rise in cases of caesarean section (both first time and in past cases of caesarean section delivery) the incidence of caesarean section ectopic pregnancy cases is on rise. Worldwide, around 18.6% of all births are done by primary caesarean section.4–6
There are published reports of hysterotomy scar ectopic pregnancy following myomectomy, uterine evacuation, past history of abnormally adherent placenta, past history of manual removal of placenta, hysterectomy and in in vitro fertilization.2,6 Hysterotomy scar ectopic pregnancies can be of two types, namely type 1 and type 2. In type 1 variety the gestational sac develops in the myometrium and grows in the direction of the uterine cavity; however, in type 2 variety, the growth of the gestational sac occurs exophytically in the direction of the uterine serosa.2,6 Type 2 variety of the hysterotomy scar ectopic pregnancies might have dreadful outcome as in many such cases spontaneous uterine rupture might occur, leading to profuse haemorrhage, shock and maternal mortality. Another unfortunate outcome is loss of fertility as to control the excessive bleeding and thus to save the patient’s life, hysterectomy might be necessary.
Presenting symptoms include, pain in the pelvic region along with vaginal bleeding and/or occasional spotting during first trimester. However, in many of the cases, there might be no alarming symptoms. Transvaginal ultrasonography is the preferred investigation; sometimes it is combined with transabdominal scan for panoramic view. Magnetic resonance imaging (MRI) is suggested in inconclusive cases with strong clinical suspicion of surgical scar ectopic pregnancy cases.1
The choice of treatment depends on various factors, including gestational age and clinical stability and the levels of beta-hCG.2–4 Available options include expectant management, medical management with methotrexate and surgical intervention.2,4 Other than surgical interventions like surgical excision via hysteroscopy or laparoscopy or laparotomy, vacuum aspiration may also be used in selected cases.2,4 Here, we present a case of surgical scar ectopic pregnancy at the site of a previous caesarean section managed successfully with methotrexate.
Case Presentation
Forty-three Years old pregnant woman presented to the emergency department in 2022. She was at 7 weeks gestation and had a remarkable obstetric history of 10 pregnancies (G10) and four previous live births (P4). The patient had an uneventful past medical and surgical history, except for two previous caesarean sections. She complained of vaginal bleeding, spotting, and pelvic pain since the beginning of her current pregnancy. There was no significant history of drug use, genetic predisposition, or family medical issues.
Clinical assessment revealed a pale appearance, and the patient was found to have a blood pressure reading of 99/66 mmHg, while on the lower end of normal. Her pulse rate was recorded at 96 beats per minute, which is within normal limits for a pregnant woman. Abdominal examination showed a soft abdomen, but localized tenderness was observed at the right hypochondrium. The rest of the physical examination was unremarkable.
Laboratory investigations indicated a human chorionic gonadotropin (hCG) level of 96,837 U/L, which corresponded to the patient’s gestational age. Hemoglobin level was measured at 10.9 grams per deciliter, and the platelet count was within the normal range at 269,000 per microliter. Liver and renal function tests yielded results within normal limits.
Upon admission, a transabdominal ultrasound examination was performed to assess the location and viability of the pregnancy. The ultrasound revealed a small, well-defined sac at the site of the previous cesarean section scar with a crown-rump length (CRL) of approximately 1.2 cm. Notably, a viable fetus was detected within the cesarean scar, confirming a diagnosis of non-ruptured cesarean scar ectopic pregnancy (refer to Figures 1 and 2 for visual representations). Further evaluation showed no evidence of active bleeding or hemoperitoneum.
 |
Figure 1 Ultrasound shows small well-defined sac measuring 1.2 cm at the expected site of prior cesarean section site; non rupture ectopic scar pregnancy. |
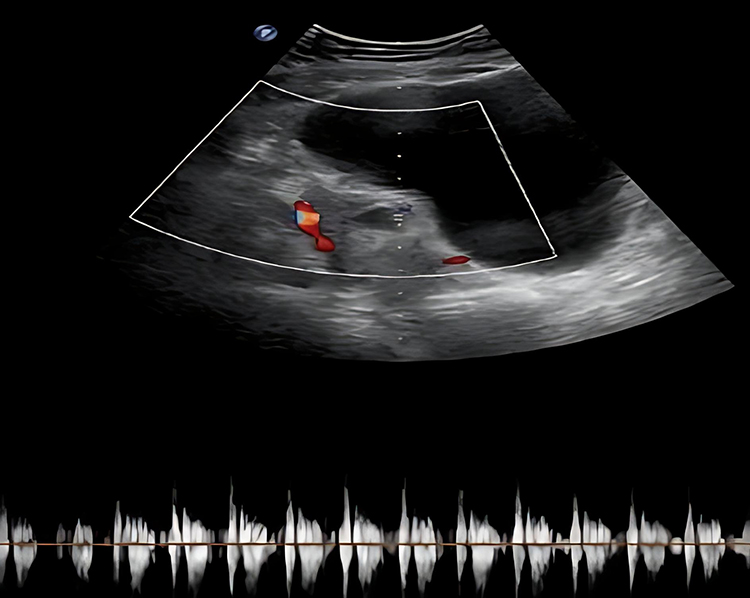 |
Figure 2 Trans abdominal ultrasound showed viable fetus at prior surgical scar site given concern for cesarean scar ectopic pregnancy, possibility of implantation on the prior cesarean scar. |
The patient’s case was managed collaboratively by a multidisciplinary team comprising obstetricians, gynecologists, and maternal–fetal medicine specialists. A comprehensive discussion regarding the available treatment options, associated risks, and benefits was conducted. After careful consideration, a conservative management approach utilizing methotrexate therapy was chosen.
The patient received two doses of methotrexate (50 mg each), administered intramuscularly, following the standard protocol for ectopic pregnancies. The initial dose was administered on the day of admission, and the second dose was given four days later. Throughout her hospital stay, the patient was closely monitored for any signs of complications, such as persistent bleeding, abdominal pain, or deterioration in her clinical condition.
Following treatment, the patient’s clinical condition improved, and her hCG levels were monitored regularly. The patient was hospitalized for a total of 9 days and at the time of discharge, the beta hCG level was measured at 9,473 U/L, indicating a significant reduction from the initial level. Detailed instructions for follow-up care were provided, emphasizing the importance of regular hCG level monitoring and vigilant observation for any signs or symptoms suggestive of persistent ectopic pregnancy or treatment failure.
Despite the comprehensive counseling and instructions provided, the patient did not return to our outpatient department (OPD) for follow-up. Instead, she expressed a preference for continuing her follow-up care at the primary hospital she initially visited. Despite this, efforts were made to establish communication with the primary hospital to ensure the patient received appropriate ongoing care and follow-up (Figure 3).
 |
Figure 3 The progress of the patient case from initial presentation to diagnosis, treatment, and follow-up. |
Discussion
Caesarean section scar pregnancy (CSSP), also known as caesarean scar pregnancy, is considered to be the rarest of the rare type of ectopic pregnancy.1 It is considered to be a life-threatening condition as there is risk of massive blood loss due to uterine rupture and death.2,3
Significant past history (history of caesarean section), presenting symptoms, clinical examination, laboratory investigation and radiological investigations are essential for confirmation of diagnosis. Timely diagnosis and appropriate management are of utmost importance as any delay or wrong diagnosis may cost the patient’s life. There are a number of theories which explain the etiology of uterine scar ectopic pregnancy. The most widely acknowledged one is that the blastocyst invades in the myometrium through a dehiscent tract originating due to past history of hysterectomy like caesarean section, myomectomy, etc., or other significant past events like manual removal of placenta, adherent placenta, etc.2,3
Another commonly recognized theory explaining the etiology of uterine scar ectopic pregnancy is trauma during assisted reproduction technique in cases without any past surgical or significant medical history.4 Painless vaginal bleeding is considered to be the most common presenting symptom besides the absence of any symptoms. One important differential diagnosis of cervical scar ectopic pregnancy is cervical pregnancy. Transvaginal ultrasonography helps to differentiate between the two conditions. In case of cervical pregnancy, there is no myometrium between the gestational sac and the bladder as in cervical pregnancy, the gestational sac grows in the anterior portion of the isthmus.7
To diagnose caesarean section scar pregnancy, ultrasound in sagittal position is helpful as in this position empty uterine cavity as well cervical canal can be seen.8 With the advent of transvaginal sonography and saline infusion sonography, post-caesarean section uterine wall integrity can be assessed in nonpregnant women. In cases of caesarean section scar defects, presence of fluid (saline) can be identified at the site of incision or filling defect can be identified.2,6
There are a number of published case reports regarding diagnosis and management of caesarean section scar ectopic pregnancy.9 Morente LS and her colleagues presented a case series on cesarean section scar ectopic pregnancies diagnosed by transvaginal ultrasonography.9 There is no fixed treatment protocol for cesarean section scar ectopic pregnancies; rather a number of treatment options are available starting from conservative management (expectant management) to surgical intervention. The condition can be life threatening hence urgent diagnosis, and appropriate management is essential to avoid catastrophic outcome. Also, uterine rupture may require hysterectomy to save the patient’s life but at the cost of loss of fertility. Thus, the authors concluded in their case series the importance of transvaginal ultrasound with Doppler. Like the above-mentioned case study, several other authors also documented the importance of utilizing correct imaging techniques for the diagnosis of cases of cesarean section scar ectopic pregnancy.10,11
Similarly in another study by Adams A and her colleague, the importance of prompt diagnosis and appropriate management of cesarean section scar ectopic pregnancy management is stressed.12 In the said study, the authors described a case of cesarean scar pregnancy in a 33 years old female patient presenting to the emergency department with a complaint of suprapubic pain. In our study, we also described a case of cesarean scar pregnancy in a 43 years old female patient attending the emergency department after being referred from a primary centre with complaints of public pain and vaginal bleeding. Like the case described by Adams A and her coauthor, our patient also managed successfully with multidose regimen of methotrexate.12
In another recent case series by Heidar Z and colleagues, a study of caesarean scar ectopic pregnancy was described.13 This case series included four Iranian women aged between 29 and 34 years who were in the 5–7 weeks of pregnancy, similar to our case (reported at 7 weeks of gestation). While our patient received methotrexate and showed a significant reduction in beta-hCG levels, it is important to note that treatment efficacy can vary among patients. In the reported series, all patients were managed with methotrexate injections; however, we will adjust the wording to reflect that while two cases were successfully managed with a single dose of systemic methotrexate, the remaining two patients required a transvaginal ultrasound-guided injection of methotrexate into the gestational sacs. This highlights the variability in treatment responses and the importance of ongoing monitoring to assess treatment effectiveness. Moreover, it is important to emphasize the necessity of appropriate dosing and the various protocols for administering methotrexate. Methotrexate can be administered in single or multidose regimens, and the choice of protocol should be tailored to the individual patient’s condition, including gestational age and clinical stability. Close monitoring of beta-hCG levels is essential to evaluate the effectiveness of treatment and to identify any potential complications.
An alternative medical option for the management of cesarean scar pregnancy (CSP) is the combined use of methotrexate (MTX) and mifepristone. In a systematic review by Stabile et al (2024), the authors evaluated the safety and effectiveness of this combination therapy across seven cases reported in five manuscripts. The review indicated a success rate of 71.4%, particularly effective when beta-human chorionic gonadotropin (B-hCG) levels were below 5,000 mUI/mL and the gestational sac was less than 20 mm. This study highlights the potential of MTX and mifepristone as a first-line treatment option for CSP, emphasizing the need for individualized management based on the patient’s clinical condition and reproductive goals.14
Surgical treatment options for Caesarean section scar pregnancy (CSSP) include cesarean scar resection, laparoscopy, laparotomy, and ultrasound-guided curettage. Cesarean scar resection can be performed via a transvaginal approach or laparoscopy, allowing for excision of the scar tissue and reapproximation of the surrounding myometrium. This method is associated with lower complication rates compared to other surgical options, although the data on outcomes can vary.15
For instance, He et al reported six successful cases of transvaginal removal of ectopic pregnancy tissue, followed by effective repair of the uterine defect. This technique is particularly advantageous for its minimally invasive nature and reduced recovery time.16
Ultrasound-guided suction curettage is another surgical option, although it carries inherent risks, such as uterine perforation and excessive bleeding due to abnormal placentation, especially in exogenic-type CSSP. A retrospective study involving 232 women with CSSP revealed that 82.3% underwent this procedure, with some requiring blood transfusions and even hysterectomy due to uncontrollable bleeding. Given these risks, ultrasound-guided suction curettage is recommended primarily in cases where the internal os is open, the fetus is non-viable, or in instances of persistent vaginal bleeding. The Society of Fetal Medicine suggests operative resection or ultrasound-guided uterine aspiration for surgical management while advising against sharp curettage alone.15,17
Additionally, uterine artery embolization has emerged as a valuable adjunctive treatment, effectively minimizing hemorrhage in patients undergoing subsequent surgical interventions.18
Conclusion
Cesarean section scar ectopic pregnancy is considered one of the rarest types of ectopic pregnancy. Besides the risk of excessive bleeding due to uterine rupture and death, there is also a risk of loss of fertility, as hysterectomy may be required to control excessive bleeding. To avoid the unfortunate outcomes associated with caesarean section scar ectopic pregnancy, early diagnosis and adequate management are essential. Furthermore, diligent follow-up care is crucial to monitor the patient’s recovery, assess beta-hCG levels, and ensure the timely identification of any complications or treatment failures. Ongoing follow-up helps in providing necessary interventions and supports the preservation of reproductive health.
Ethical Approval
I would like to clarify that IRB approval was not required for this case study. This determination was made by the Clinical Research Committee at Imam Abdulrahman Bin Faisal Hospital, which reviewed the case and confirmed that it fell under categories that do not necessitate IRB oversight.
Consent Statements
The approval was granted by the Clinical Research Committee at Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia to publish this study. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
There are no sponsors, and there was no special funding for writing or publication of this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jayaram PM, Okunoye GO, Konje J. Caesarean scar ectopic pregnancy: diagnostic challenges and management options. Obstet Gynaecol. 2017;19(1):13–20. doi:10.1111/tog.12355
2. Seow KM, Hwang JL, Tsai YL, Huang LW, Lin YH, Hsieh BC. Subsequent pregnancy outcome after conservative treatment of a previous Caesarean scar pregnancy. Acta Obstetriciaet Gynecologica Scandinavica. 2004;83(12):1167–1172. doi:10.1111/j.0001-6349.2004.00445.x
3. Green-Top Guideline. Diagnosis and management of ectopic pregnancy: green-top guideline no. 21. BJOG. 2016;123(13):e15–55. A published erratum appears in BJOG. 2017; 124(13):e314. doi:10.1111/1471-0528.14189
4. Maheux-Lacroix S, Li F, Bujold E, Nesbitt-Hawes E, Deans R, Abbott J. Cesarean scar pregnancies: a systematic review of treatment options. J Minim Invasive Gynecol. 2017;24(6):915–925. doi:10.1016/j.jmig.2017.05.019
5. Betrán AP, Ye J, Moller AB, Zhang J, Gülmezoglu AM, Torloni MR. The increasing trend in caesarean section rates: global, regional and national estimates: 1990–2014. PLoS One. 2016;11(2):e0148343. doi:10.1371/journal.pone.0148343
6. Patel MA. Scar ectopic pregnancy. J Obstet Gynaecol India. 2015;65(6):372–375. doi:10.1007/s13224-015-0817-3
7. Rizk B, Holiday CP, Owens S, Abuzeid M. Cervical and caesarean scar ectopic pregnancies: diagnosis and management. Middle East Fertil Soc J. 2013;18(2):67–73. doi:10.1016/j.mefs.2013.01.011
8. Fylstra DL. Ectopic pregnancy not within the (distal) fallopian tube: aetiology, diagnosis, and treatment. Am J Obstet Gynaecol. 2012;206(4):289–299. doi:10.1016/j.ajog.2011.10.857
9. Morente LS, León AIG, Reina MPE, Herrero JRA, Mesa EG, López JSJ. Cesarean Scar Ectopic Pregnancy-Case Series: treatment Decision Algorithm and Success with Medical Treatment. Medicina. 2021;57(4):362. doi:10.3390/medicina57040362
10. Satyam, Swarup MS, Garg A. Ectopic uterine scar pregnancy: a case report. Ultrasound. 2021;29(1):57–63. doi:10.1177/1742271X20933918
11. Torky HA. Cesarean scar ectopic pregnancy: a cause of failed first trimester surgical termination of pregnancy (case report). JBRA Assist Reprod. 2021;25(1):165–167. doi:10.5935/1518-0557.20200039
12. Adams A, Thompson M. Cesarean Scar Ectopic Pregnancy: a Case Report. J Emerg Nurs. 2021;47(5):693–695. doi:10.1016/j.jen.2021.05.008
13. Heidar Z, Zadeh Modarres S, Abediasl Z, Khaghani A, Salehi E, Esfidani T. Cesarean scar pregnancy treatment: a case series. J Med Case Rep. 2021;15(1):506. doi:10.1186/s13256-021-03081-0
14. Stabile G, Vona L, Carlucci S, et al. Conservative treatment of cesarean scar pregnancy with the combination of methotrexate and mifepristone: a systematic review. Women’s Health. 2024;20:1–8.
15. Miller R, Gyamfi-Bannerman C. Society for Maternal-Fetal Medicine consult series #63: cesarean scar ectopic pregnancy. Am J Obstet Gynecol. 2022;227(3):1. doi:10.1016/j.ajog.2022.06.024
16. He M, Chen MH, Xie HZ, et al. Transvaginal removal of ectopic pregnancy tissue and repair of uterine defect for cesarean scar pregnancy. BJOG. 2011;118(9):1136–1139. doi:10.1111/j.1471-0528.2011.02891.x
17. Jurkovic D, Knez J, Appiah A, Farahani L, Mavrelos D, Ross JA. Surgical treatment of cesarean scar ectopic pregnancy: efficacy and safety of ultrasound-guided suction curettage. Ultrasound Obstet Gynecol. 2016;47(4):511–517. doi:10.1002/uog.15857
18. Cao S, Zhu L, Jin L, Gao J, Chen C. Uterine artery embolization in cesarean scar pregnancy: safe and effective intervention. Chin Med J. 2014;127(12):2322–2326. doi:10.3760/cma.j.issn.0366-6999.20140196
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Two Consecutive Ruptured Tubal Ectopic Pregnancies after Interval Bilateral Tubal Ligation
Owiny M, Acen MO, Okeng J, Akello OA
International Medical Case Reports Journal 2024, 17:417-421
Published Date: 8 May 2024
After Ovulation Induction, Women of Childbearing Age Stopped Their Menstruation for 50 days, Was Occured Double Chorionic Biamniotic Sac for Pregnancy in the Interstitial Part of the Tubal: A Case Report
Pan K, Ju W, Wang Y, Zhang Q, Wang R, Zhao S
International Journal of Women's Health 2025, 17:3741-3744
Published Date: 21 October 2025
Management of Viable Cesarean Scar Pregnancies (CSP) with Potassium Chloride (KCl) and the Requirement for Adjunctive Treatments
Babic I, Abudoraehem OS, Alhadab A, Altowaijri O, AlMoussa F, Makhafah T, Alaqeeli A
International Journal of Women's Health 2026, 18:579258
Published Date: 5 February 2026