Back to Journals » International Journal of Women's Health » Volume 18
Ectopic β-hCG-Expressing Hepatic Neoplasm with Cutaneous Metastasis in a Young Postpartum Woman: A Case Report and Literature Review
Authors Zheng Y, Yang M, Xu W ![]() , Huang P
, Huang P
Received 10 March 2026
Accepted for publication 10 June 2026
Published 15 June 2026 Volume 2026:18 606722
DOI https://doi.org/10.2147/IJWH.S606722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Yameng Zheng,1 Meiqin Yang,2 Wen Xu,1 Pintong Huang1
1Department of Ultrasound, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Ultrasound, Jiande First People’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Pintong Huang, Department of Ultrasound, The Second Affiliated Hospital of Zhejiang University School of Medicine, No. 88 Jiefang Road, Hangzhou, People’s Republic of China, Email [email protected] Wen Xu, Department of Ultrasound, The Second Affiliated Hospital of Zhejiang University School of Medicine, No. 88 Jiefang Road, Hangzhou, People’s Republic of China, Email [email protected]
Abstract: This case report describes a rare presentation of intrahepatic cholangiocarcinoma (ICC) in a 33-year-old postpartum woman, with extensive systemic and cutaneous metastases as the initial clinical manifestations. She presented with a palpable mass on her back and was subsequently found to have hepatic masses accompanied by elevated serum carbohydrate antigen (CA) 19-9 and β-human chorionic gonadotropin (β-hCG). Subsequent imaging and histopathological evaluation confirmed a poorly differentiated ICC with atypical trabecular, nested, and sheet-like growth patterns, without evidence of trophoblastic differentiation. Immunohistochemical analysis revealed a Cytokeratin (CK) 7-negative/CK19-positive immunophenotype and moderate hCG expression (++). In postpartum patients with unexplained β-hCG elevation unrelated to pregnancy, ectopic β-hCG-secreting tumors, such as ICC, should be considered in the differential diagnosis after exclusion of trophoblastic and germ cell neoplasms, particularly when accompanied by elevated carbohydrate antigen 19-9 levels.
Keywords: intrahepatic cholangiocarcinoma, postpartum, contrast-enhanced ultrasound, human chorionic gonadotropin, cutaneous metastasis
Introduction
Intrahepatic cholangiocarcinoma (ICC) is a malignant epithelial neoplasm arising from the intrahepatic bile ducts proximal to the second-order branches. As the second most common primary liver malignancy after hepatocellular carcinoma (HCC), ICC accounts for 15–20% of all primary liver cancers. In recent decades, both its incidence and mortality have increased worldwide.1,2 Owing to its aggressive behavior and insidious onset, most patients with ICC present at an advanced stage. Even after curative surgical resection, long-term survival remains poor because of its high recurrence rate and strong metastatic potential.3
The median age at ICC diagnosis was 67 years,4 with a higher prevalence in men. ICC is rarely diagnosed in patients aged <40 years, except in those with concurrent primary sclerosing cholangitis.5 In pregnancy or the postpartum period, elevated β-human chorionic gonadotropin (β-hCG) levels are most commonly associated with gestational trophoblastic disease and germ cell tumors, which represent key differential diagnoses. However, β-hCG elevation may also result from ectopic production by non-trophoblastic malignancies, including HCC and ICC, although this phenomenon is rare. ICC occurring during pregnancy or the postpartum period with aberrant β-hCG expression is exceptionally uncommon, with only a limited number of cases reported in the literature. This case report describes a case of ICC with extensive systemic metastasis in a 33-year-old postpartum woman, who initially presented with cutaneous metastasis and demonstrated moderate immunohistochemical β-hCG expression.
Case Presentation
A 33-year-old gravida 2, para 2 woman, who had delivered a term infant 5 months earlier, presented to our outpatient department with an incidentally detected lump on the left side of her back present for 1 week. She also reported left neck swelling and numbness in the left upper limb. She underwent annual medical checkups, except during pregnancy, and denied any significant medical or family history. Physical examination revealed a painless 2×2 cm nodule on the left side of the back and tenderness in the left cervical region. Ultrasonography (US) of the superficial mass and left upper limb veins revealed an ill-defined, oval hypoechoic mass within the subcutaneous fat layer of the left back. The mass measured 1.8×0.9 cm and demonstrated moderate vascularity. Unexpectedly, thrombosis was identified in the left internal jugular and subclavian veins. Multiple enlarged lymph nodes were also observed in the left cervical and supraclavicular regions. Laboratory investigations revealed markedly elevated levels of D-dimer (>20,000 ug/L), liver enzymes (alanine aminotransferase (ALT): 109 U/L, aspartate aminotransferase (AST): 107 U/L), and tumor markers (CA 19-9: 8614.6 U/mL, carbohydrate antigen 242: 70.5 U/mL, cyfra21-1: 38.5 ng/mL, cancer antigen 125: 188.0 U/mL, and β-hCG: 4667.8 U/L). However, alpha-fetoprotein (AFP) and hepatitis antibody levels were within normal limits. Chest computed tomography (CT) revealed soft tissue edema at the root of the left neck with multiple small lymph nodes. Multiple hypodense lesions were identified within the liver parenchyma.
To confirm the diagnosis, a comprehensive physical examination was performed. US revealed multiple hepatic masses appearing as inhomogeneous, hypoechoic lesions with ill-defined margins and irregular contours. Color Doppler imaging revealed internal vascular flow within the largest hepatic mass (Figure 1). Contrast-enhanced US (CEUS) revealed early arterial enhancement of the largest lesion, occurring 9s prior to the surrounding hepatic parenchyma. This was followed by mild heterogeneous hyperenhancement, peaking at 16s, with subsequent washout at 26s and hypoenhancement at 132s. These imaging features were highly suggestive of ICC (Figure 2). Abdominal contrast-enhanced CT (CE-CT) revealed multiple hypodense hepatic nodular lesions with inhomogeneous enhancement. The largest lesion measured approximately 9.6×8.3 cm (Figure 3), raising suspicion for hepatic metastases. In addition, multiple enlarged lymph nodes were identified in the retroperitoneal and mesenteric regions, along with multiple nodules in the pelvic mesentery and omentum, accompanied by pelvic effusion. Contrast-enhanced magnetic resonance imaging (MRI) revealed multiple hepatic masses exhibiting hypointensity on T1-weighted imaging, mildly heterogeneous hyperintensity on T2-weighted imaging, hyperintensity on diffusion-weighted imaging, and low apparent diffusion coefficient values. CE-MRI revealed heterogeneous arterial phase enhancement with progressive centripetal enhancement in the portal venous and delayed phases (Figure 4), findings suggestive of ICC. Gastroscopy and transvaginal gynecological US revealed no abnormal findings. Positron emission tomography (PET)–CT revealed multiple hepatic masses with increased glucose uptake. Mild thickening of the omentum and peritoneum was also observed, along with multiple hypermetabolic nodules involving the subcutaneous soft tissues, bones, and lymph nodes, all demonstrating increased glucose uptake. Owing to the presence of systemic metastases, a core needle biopsy of the largest hepatic lesion was performed. Histopathological examination revealed a poorly differentiated adenocarcinoma. Hematoxylin and eosin staining (HE) demonstrated tumor cells arranged in linear, nested, and sheet-like patterns. The tumor cells exhibited eosinophilic cytoplasm, enlarged hyperchromatic nuclei, and prominent nucleoli (Figure 5). No trophoblastic components were identified on microscopic examination. Immunohistochemical analysis revealed positivity for CK (AE1/AE3) (+), CK8 (+), CK18 (+), CK19 (+), SATB2 (+), and hCG (++). Meanwhile, staining was negative for CK7, CK20, CK5/6, GPC3, CDX2, PAX-8, GATA-3, P63, ER-alpha (SP1), PR, CD30, hPL, SALL4, PLAP, inhibin α, and CK5/6. The Ki-67 proliferation index was approximately 80%. FGFR2 gene rearrangement was not detected. Based on the combined clinical, radiological, and histopathological findings, a diagnosis of cholangiocarcinoma (TNM stage IV) was established. The patient subsequently initiated combined chemotherapy and immunotherapy, administered at 3-week intervals, beginning the day after diagnosis. The initial treatment regimen comprised gemcitabine, oxaliplatin, tislelizumab (a programmed cell death protein 1 (PD-1) inhibitor), and denosumab. Denosumab was discontinued after two treatment cycles. Follow-up CT demonstrated regression of the intrahepatic lesions. Tumor markers and β-hCG levels normalized after three treatment cycles. The chemotherapy regimen was subsequently modified, and maintenance treatment was initiated with tislelizumab, capecitabine, and lenvatinib. The lesions continued to regress, with no evidence of disease progression. At 2.5 years after treatment initiation, whole-body PET/CT demonstrated no evidence of metabolically active tumor lesions. The patient remained clinically stable, with a good quality of life, and continued on regular maintenance therapy.
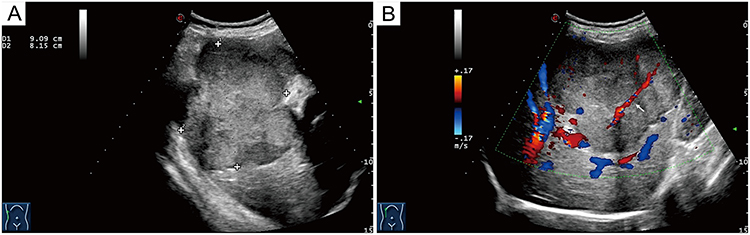 |
Figure 1 Ultrasound features of the hepatic lesion. (A) Ultrasonography demonstrated a large, ill-defined, irregular, heterogeneously hypoechoic lesion measuring 9.09 cm × 8.15 cm in the right hepatic lobe. (B) Color Doppler ultrasonography demonstrates penetrating blood flow within the dominant mass (arrow). |
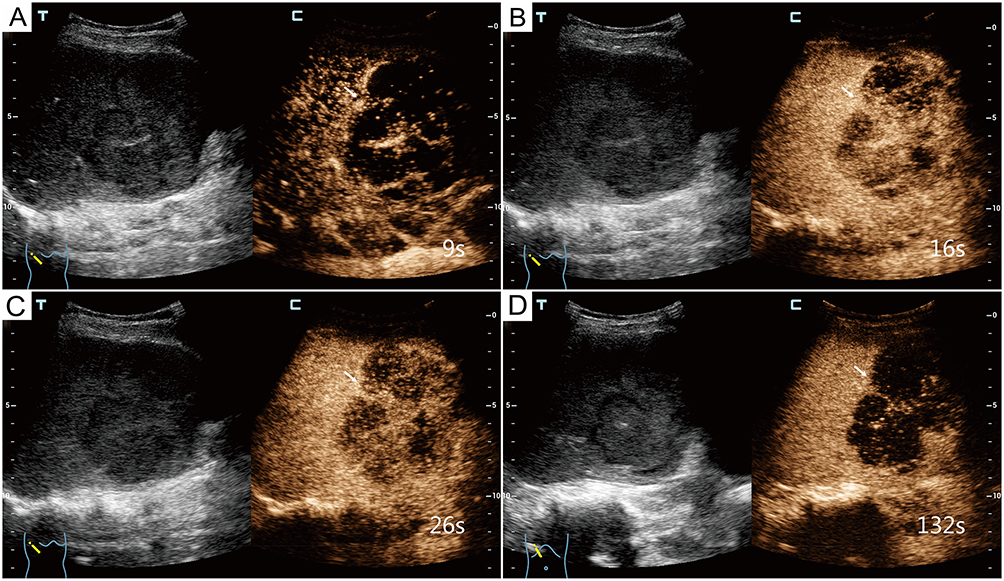 |
Figure 2 Contrast-enhanced ultrasonography (CEUS) of the dominant hepatic lesion (arrow). (A–D) The lesion initiates enhancement at 9s (A), presents mild heterogeneous hyperenhancement at 16s (B), proceeds to washout at 26s (C), and becomes hypoenhancing at 132s (D). Abbreviations: T, conventional tissue B-mode ultrasonography; C, contrast-enhanced CEUS imaging. |
 |
Figure 3 Contrast-enhanced computed tomography (CE-CT) of the dominant hepatic lesion (arrow). (A) Unenhanced CT shows a hypodense lesion (arrow) in the right hepatic lobe. (B and C) The lesion exhibits heterogeneous enhancement in the arterial phase (B) and delayed phase (C). |
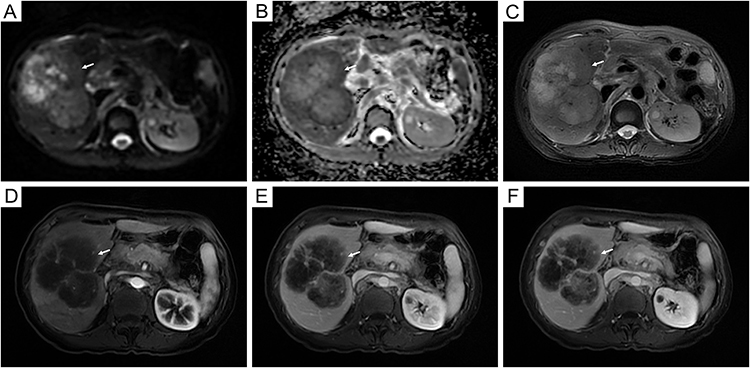 |
Figure 4 Magnetic resonance imaging features of the dominant hepatic lesion (arrow). (A) The lesion demonstrates mild hyperintensity on T2-weighted images. (B) It presents hyperintensity on diffusion-weighted imaging. (C) Marked hypointensity on apparent diffusion coefficient mapping. (D–F) The lesion displays heterogeneous arterial-phase enhancement (D) and progressive centripetal enhancement in the portal venous (E) and delayed phases (F). |
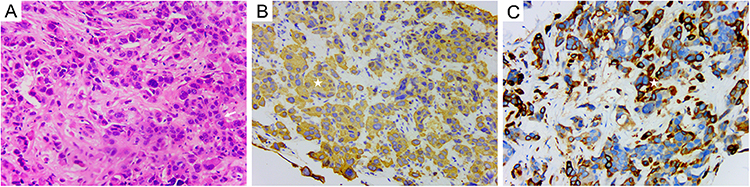 |
Figure 5 Immunohistochemical findings of the dominant right hepatic lesion. (A) Hematoxylin and eosin staining demonstrates tumor cells growing in trabecular, nested, and sheet-like configurations (arrow). (B and C) Tumor cytoplasm exhibits positive brown immunoreactivity (star) for CK19 (B) and hCG (C); original magnification, 200×. |
Discussion
ICC is a rare adenocarcinoma arising from heterogeneous intrahepatic cylindrical or cubic epithelial cells. Based on gross tumour growth patterns, ICC is classified into mass forming (65%), periductal infiltrating (6%), intraductal growing (4%), and mixed type (25%).6
Cholangiocarcinoma during pregnancy or the postpartum period is extremely rare. A PubMed search identified only 15 patients with primary cholangiocarcinoma occurring during pregnancy or the postpartum period between 1998 and 2026.7–21 The 15 reported patients, together with the present patient, were analyzed and summarized in Table 1. Five patients were diagnosed in the postpartum period. The ages ranged from 22 to 40 years. The most common initial symptoms of cholangiocarcinoma were nausea, vomiting, and abdominal pain.7,8,13,14,18,19,21 Other less common initial presentations were also reported, including back pain, bowel and bladder dysfunction,11 pruritus,9,20 and abnormal liver function.10 In this patient, a left back cutaneous nodule represented the initial manifestation of ICC. Cutaneous metastasis (OSCM) of CCA is extremely rare, with the scalp being the frequently involved site. Liu et al22 reviewed 30 patients with cutaneous metastases from cholangiocarcinoma, among whom only 8 presented with cutaneous lesions as the initial manifestation. A comprehensive literature search suggests that this case report is the first to describe an OSCM presenting as the initial sign of ICC in a young postpartum woman. Previous case reports indicate that the nodular type is the most common presentation of OSCM in cholangiocarcinoma, consistent with the present patient. Other reported manifestations include erythematous plaques, abscesses, and ulcerative lesions.23 OSCM is associated with a poor prognosis, with a median survival of approximately 4 months. Clinicians should consider OSCM in the differential diagnosis of cutaneous nodules, particularly in patients with a history of malignancy.
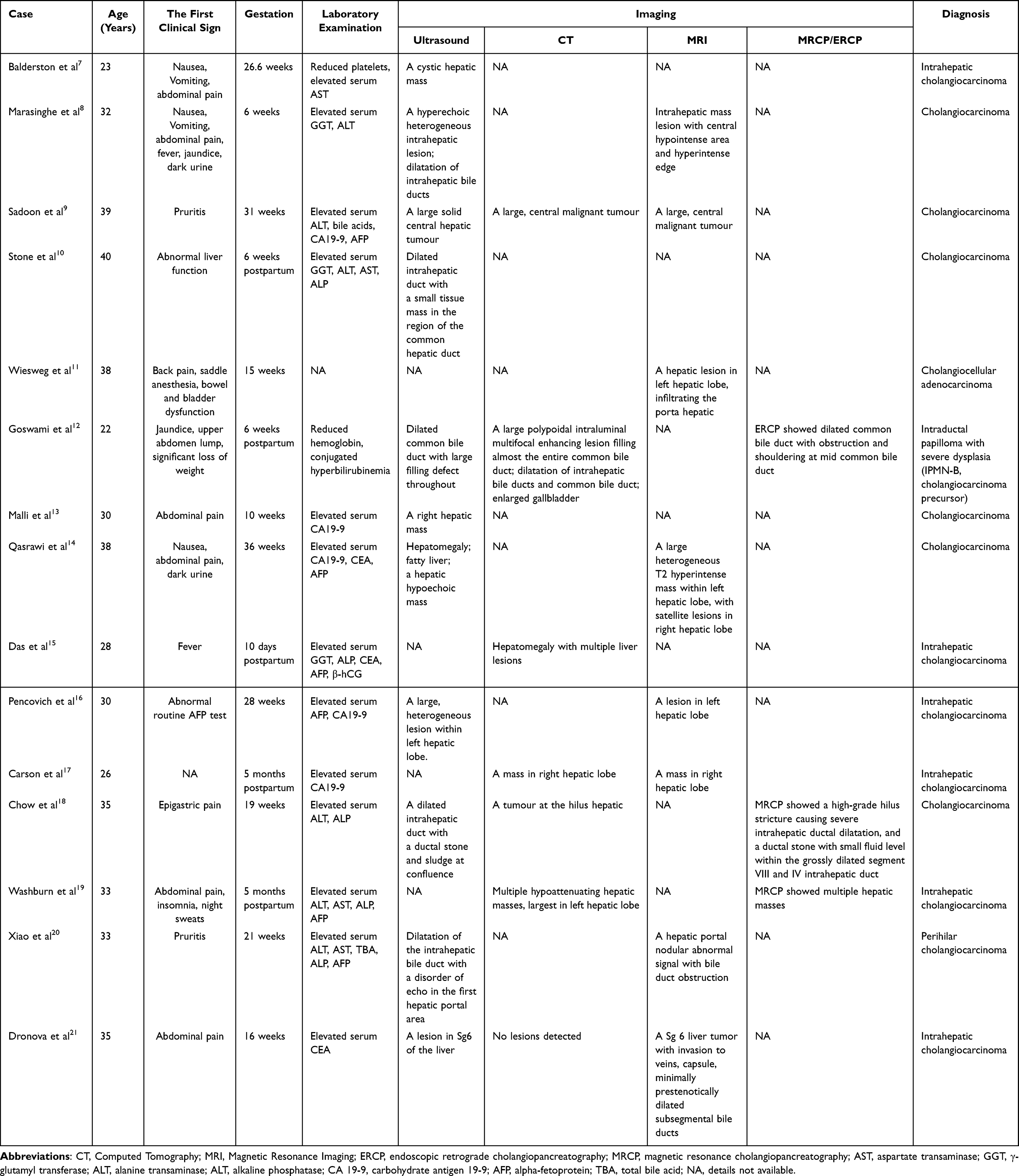 |
Table 1 Cases of Pregnancy and Postpartum Related Cholangiocarcinoma from 1998–2024 |
Although pregnancy-related hormonal and immunological changes have been reported to influence tumor biology, their role in ICC development and progression remains unclear. Established risk factors for ICC include primary sclerosing cholangitis, liver fluke infection, viral hepatitis, hepatolithiasis, congenital biliary anomalies, and other high-risk conditions.6 In this case report, the young patient was diagnosed with ICC 5 months postpartum and had no known risk factors. Pregnancy-related physiological changes may have contributed to tumor progression or delayed clinical recognition. Previous studies suggested that exposure to female reproductive hormones is associated with an increased risk of ICC.24 Oestrogen promotes cholangiocyte proliferation by activating the ERK and PI3K/AKT signaling pathways.25 Additionally, pregnancy-related hormonal changes may impair biliary excretion and contribute to cholestasis and chronic inflammation, both of which are recognized mechanisms in biliary carcinogenesis. Physiological immune tolerance during pregnancy may attenuate antitumour immune surveillance. Furthermore, ectopic β-hCG production has been reported in ICC and has been associated with more aggressive tumor behavior.26 In the present patient, the markedly elevated β-hCG level, followed by normalization after treatment, suggested a tumour-related origin. Collectively, pregnancy-related hormonal and immunological alterations may have contributed to disease progression in this patient; however, a causal relationship cannot be established based on a single patient.
Another notable finding in this patient was the markedly elevated serum β-hCG level of 4667.8 U/L, which initially complicated the diagnostic evaluation. Among previously reported patients with primary cholangiocarcinoma occurring during pregnancy or the postpartum period, elevated serum β-hCG levels were described in only two patients.15,27 Elevated β-hCG is most commonly associated with pregnancy-related conditions, gestational trophoblastic disease, and germ cell tumors. In the present patient, gynecological US and PET/CT excluded pregnancy-associated disorders, retained placental tissue, and primary gynecological malignancies. Notably, primary uterine choriocarcinoma may present as an occult lesion or undergo spontaneous regression.28 Accordingly, unremarkable pelvic imaging findings do not completely exclude metastatic hepatic choriocarcinoma. Although germ cell tumors can produce β-hCG, primary hepatic germ cell tumors are exceedingly rare in adults and typically present with isolated elevations of germ cell tumor markers rather than concurrent increases in biliary markers such as carbohydrate antigen 19-9. HCC was also considered unlikely, given the absence of underlying chronic liver disease and normal AFP levels. Ectopic β-hCG production has been reported in several non-trophoblastic malignancies, including lung, breast, gastric, pancreatic, colorectal, hepatocellular, and biliary tract cancers.29 The differential diagnosis of β-hCG-secreting ICC, primary hepatic choriocarcinoma, and metastatic hepatic choriocarcinoma is summarized in Table 2.30 In this present patient, immunohistochemical analysis demonstrated hCG expression in the liver biopsy specimen, and the serum β-hCG level normalized following systemic treatment. These findings support the conclusion that the elevated β-hCG level most likely resulted from ectopic production by ICC cells. Clinicians should therefore interpret elevated β-hCG levels cautiously in postpartum patients with suspected or confirmed malignancy. After exclusion of more common causes, ectopic β-hCG secretion by non-trophoblastic tumors should be considered in the differential diagnosis.
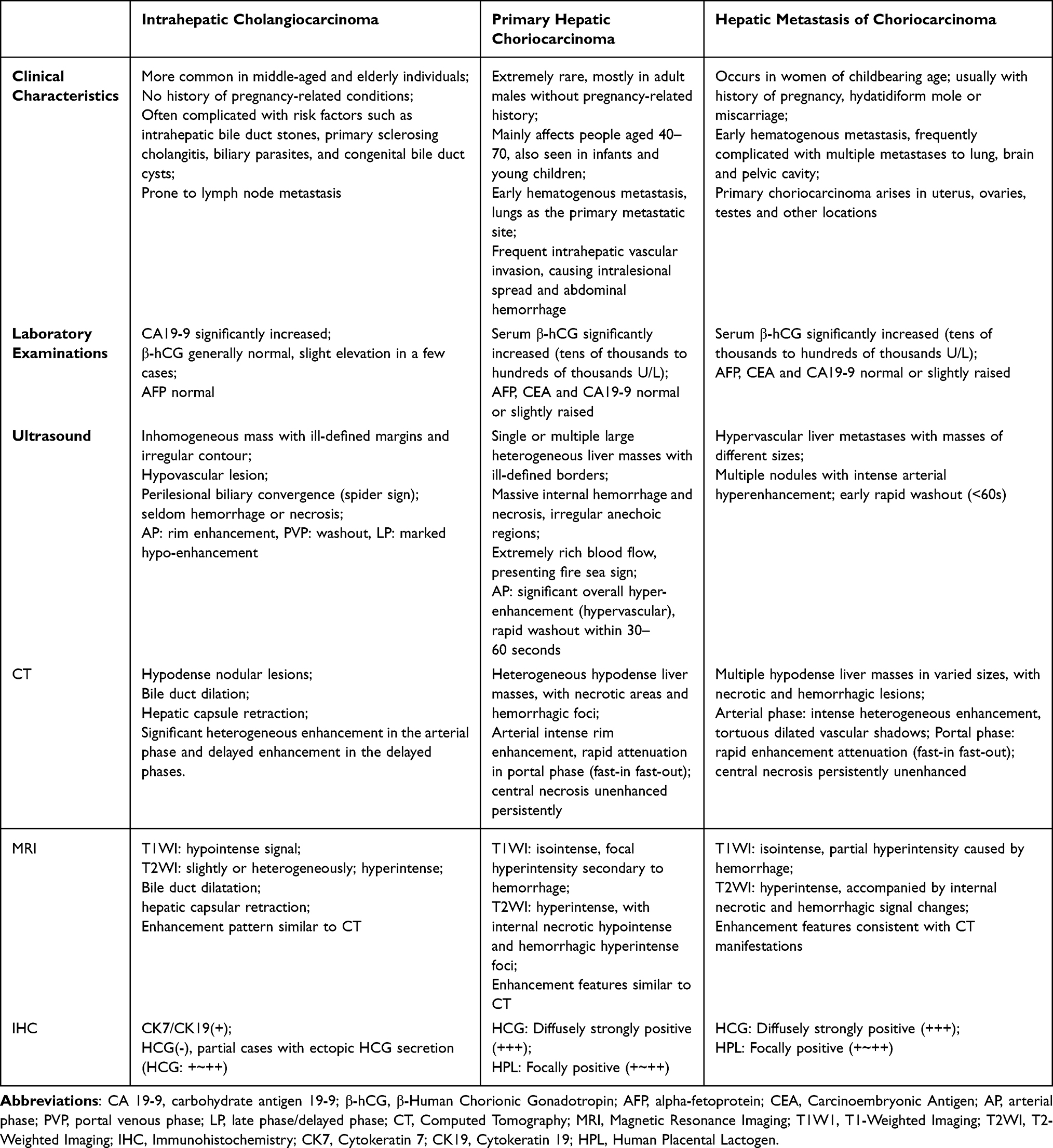 |
Table 2 Differential Diagnosis of Intrahepatic Cholangiocarcinoma, Primary Hepatic Choriocarcinoma and Hepatic Metastasis of Choriocarcinoma |
Contrast-enhanced imaging plays a pivotal role in the early diagnosis and assessment of ICC. US is often the initial imaging modality and typically demonstrates a solitary, heterogeneous mass with ill-defined margins and an irregular shape. On CEUS, mass-forming ICCs exhibit four arterial-phase (AP) enhancement patterns: peripheral irregular rim-like enhancement, heterogeneous hyperenhancement, homogeneous hyperenhancement, and heterogeneous hypoenhancement.31 Mass-forming ICCs typically exhibit washout during the portal venous phase and complete hypoenhancement in the late phase (LP) and persistent hypo enhancement in the post-vascular phase.32 Compared with HCCs, ICCs typically exhibit less intense AP enhancement and early (<60s) hypoenhancement, followed by more pronounced washout. By contrast, HCCs more commonly demonstrate delayed and mild washout.32 CEUS utilizes blood pool tracers to visualize vascular structures and perfusion dynamics, thereby providing detailed information on tumor vascularity and interlesional perfusion characteristics. From a pathophysiological perspective, tumor cells proliferate densely in areas with abundant blood supply. Accordingly, hyperenhanced areas on CEUS indicate an increased tumor cell density.33 The intratumoral distribution of cancer corresponds to distinct contrast-enhancement patterns. On CE-CT, mass-forming ICC typically demonstrates marked heterogeneous enhancement in the arterial phase with progressive delayed enhancement. This pattern is attributed to abundant fibrous stroma and slow infiltration of contrast material into the fibrous tissue.34 Accordingly, CE-CT may reflect the degree of tumor fibrosis. Similar imaging characteristics are also observed on MRI. On MRI, T2 signal intensity varies according to tumor cell density and the proportion of vascular fibrous stromal components. On CE-MRI, mass-forming ICC typically demonstrates a characteristic peripheral washout pattern. This pattern is characterized by intense peripheral enhancement in the arterial phase. It is followed by progressive centripetal enhancement in the venous phase, with simultaneous peripheral washout. This enhancement pattern significantly differs from that of HCC, which typically demonstrates washout in the portal or delayed phase on CE-CT or CE-MRI.35 Despite the large size of the hepatic mass in the present patient, no portal vein invasion or intrahepatic biliary dilation was observed. These findings are consistent with mass-forming ICC arising from small, mucin-poor bile ducts.36 Additionally, multiple enlarged retroperitoneal lymph nodes were identified, suggesting early lymphatic spread and an aggressive biological behavior of ICC with distant nodal metastasis. Notably, early washout was observed on CEUS in this patient. Therefore, differentiation between primary hepatic choriocarcinoma and metastatic hepatic choriocarcinoma remains essential (Table 2).
Hematoxylin and eosin staining revealed a poorly differentiated adenocarcinoma with trabecular, nested, and sheet-like architecture. Tumor cells showed abundant eosinophilic cytoplasm, enlarged hyperchromatic nuclei, and prominent nucleoli, without morphologically identifiable trophoblastic components. Immunohistochemistry demonstrated positivity for epithelial markers AE1/AE3, CK8, CK18, and CK19, consistent with epithelial origin and biliary differentiation. Tumor cells were positive for hCG (++) but negative for hPL, SALL4, and PLAP, excluding trophoblastic differentiation and germ cell neoplasms. GPC3 was negative, supporting the exclusion of HCC. Although CK7 was negative, this does not exclude ICCs. A subset of tumors may lack CK7 expression while retaining CK19 positivity.37 CK19 is considered a more sensitive marker of biliary lineage and associated morphological features. The lesion was ultimately diagnosed as a poorly differentiated adenocarcinoma consistent with atypical ICC. Furthermore, β-hCG immunoreactivity in tumor cells supports ectopic production and provides a plausible explanation for the markedly elevated serum β-hCG level. Short tandem repeat genotyping could have further clarified whether the lesion was of gestational or non-gestational origin; however, this analysis was not performed due to limited tissue availability, representing a limitation of the present case report.
Management of advanced ICC in postpartum women is challenging due to the rarity of this condition and the absence of dedicated treatment guidelines. Systemic therapy remains the cornerstone of management of unresectable or metastatic biliary tract cancer. Gemcitabine-based chemotherapy is the standard first-line approach, with gemcitabine plus cisplatin established as the global standard of care.38 Gemcitabine plus oxaliplatin is a well-accepted alternative, particularly for patients in whom cisplatin is contraindicated or oxaliplatin is preferred due to its more favorable toxicity profile. More recently, immune checkpoint inhibitors (ICIs) have been incorporated into treatment strategies for advanced BTC. Multiple clinical trials have demonstrated improved survival with the addition of PD-1/programmed death-ligand 1 inhibitors to gemcitabine-based chemotherapy.39 In the present patient, the patient initially received gemcitabine, oxaliplatin, tislelizumab (a PD-1 inhibitor), and denosumab. Denosumab was administered for bone metastasis and discontinued after two cycles. Following three treatment cycles, marked regression of intrahepatic lesions and normalization of both tumor markers and serum β-hCG were observed, indicating a robust treatment response and further supporting the diagnosis of ICC. Subsequently, maintenance therapy with ligelizumab, capecitabine, and lenvatinib was initiated to sustain disease control. Although evidence supporting this specific maintenance regimen in ICC remains limited and continues to evolve, this case report highlights the potential value of multidisciplinary evaluation and individualized systemic therapy in postpartum patients with advanced ICC.
Conclusion
ICC occurring during pregnancy or the postpartum period is an exceedingly rare entity that often presents with diverse and atypical clinical features. Although uncommon, cutaneous metastasis may represent the initial manifestation. Due to its insidious onset, early diagnosis of ICC remains challenging. Contrast-enhanced imaging plays a crucial role in the early detection and staging of ICC.
This case report highlights the importance of careful follow-up and comprehensive physical examination in postpartum women with unexplained elevated β-hCG. In postpartum patients with unexplained elevated β-hCG levels and no evidence of pregnancy, ectopic β-hCG-secreting tumors such as ICC should be considered in the differential diagnosis after exclusion of trophoblastic disease and germ cell tumors, particularly when accompanied by elevated CA 19-9 levels.
Ethical Approval
Ethical approval was obtained from the Human Research Ethics Committee of the Second Affiliated Hospital, School of Medicine, Zhejiang University.
Informed Consent
Written informed consent was obtained from the patient for participation in this case study and for publication of clinical data and images.
Acknowledgments
This work was financially supported by the Natural Science Foundation of Zhejiang Province (LQ20H180011).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by the Natural Science Foundation of Zhejiang Province (LQ20H180011).
Disclosure
The authors declare no competing interests in this work.
References
1. Florio AA, Ferlay J, Znaor A, et al. Global trends in intrahepatic and extrahepatic cholangiocarcinoma incidence from 1993 to 2012. Cancer. 2020;126(11):2666–12. doi:10.1002/cncr.32803
2. Banales JM, Cardinale V, Carpino G, et al. Expert consensus document: cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat Rev Gastroenterol Hepatol. 2016;13(5):261–280. doi:10.1038/nrgastro.2016.51
3. Mazzaferro V, Gorgen A, Roayaie S, Droz Dit Busset M, Sapisochin G. Liver resection and transplantation for intrahepatic cholangiocarcinoma. J Hepatol. 2020;72(2):364–377. doi:10.1016/j.jhep.2019.11.020
4. Saha SK, Zhu AX, Fuchs CS, Brooks GA. Forty-year trends in cholangiocarcinoma incidence in the U.S.: intrahepatic disease on the rise. Oncologist. 2016;21(5):594–599. doi:10.1634/theoncologist.2015-0446
5. Zhang H, Yang T, Wu M, Shen F. Intrahepatic cholangiocarcinoma: epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016;379(2):198–205. doi:10.1016/j.canlet.2015.09.008
6. Charbel H, Al-Kawas FH. Cholangiocarcinoma: epidemiology, risk factors, pathogenesis, and diagnosis. Curr Gastroenterol Rep. 2011;13(2):182–187. doi:10.1007/s11894-011-0178-8
7. Balderston KD, Tewari K, Azizi F, Yu JK. Intrahepatic cholangiocarcinoma masquerading as the HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) in pregnancy: case report. Am J Obstet Gynecol. 1998;179(3 Pt 1):823–824. doi:10.1016/s0002-9378(98)70093-6
8. Marasinghe JP, Karunananda SA, Angulo P. Cholangiocarcinoma in pregnancy: a case report. J Obstet Gynaecol Res. 2008;34(4 Pt 2):635–637. doi:10.1111/j.1447-0756.2008.00810.x
9. Sadoon S, Hodgett S. Unusual cause of itching in a pregnancy (cholangiocarcinoma). J Obstet Gynaecol. 2008;28(2):230–231. doi:10.1080/01443610801916296
10. Stone S, Girling JC. Deranged liver function tests in pregnancy: the importance of postnatal follow-up. Obstet Med. 2009;2(1):32–33. doi:10.1258/om.2008.080036
11. Wiesweg M, Aydin S, Koeninger A, et al. Administration of gemcitabine for metastatic adenocarcinoma during pregnancy: a case report and review of the literature. AJP Rep. 2014;4(1):17–22. doi:10.1055/s-0034-1368091
12. Goswami A, Bhargava N, Dadhich S, Chaturvedi KR. A young lady with post-partum jaundice and right upper quadrant lump abdomen: an unusual etiology. Ann Gastroenterol. 2014;27(1):82–84.
13. Malli A, Eisfeld AK, Chen W, Mumtaz K. Pregnancy and aggressive cholangiocarcinoma in a young patient with primary sclerosing cholangitis: 2248. Am J Gastroenterol. 2017;112:S1235.
14. Qasrawi A, Abughanimeh O, Abu Ghanimeh M, Arora-Elder S, Yousef O, Tamimi T. Intrahepatic cholangiocarcinoma masquerading as acute fatty liver of pregnancy: a case report and review of the literature. Case Rep Hepatol. 2018;2018:6939747. doi:10.1155/2018/6939747
15. Das S, Job M, Kodiatte T, Iyadurai R. Atypical presentation of intrahepatic cholangiocarcinoma-Fever and ascites in a postpartum lady. J Family Med Prim Care. 2019;8(11):3748–3751. doi:10.4103/jfmpc.jfmpc_748_19
16. Pencovich N, Younis M, Lessing Y, et al. Major liver resection in pregnancy: three cases with different etiologies and review of the literature. J Matern Fetal Neonatal Med. 2019;32(2):203–211. doi:10.1080/14767058.2017.1376315
17. Carson SW, Craven KE, Nauen D, et al. Rapidly progressive metastatic cholangiocarcinoma in a postpartum patient with cystic fibrosis: a case report. BMC Pulm Med. 2020;20(1):298. doi:10.1186/s12890-020-01337-x
18. Chow CY, Kong CW, To WW. Cholangiocarcinoma in pregnancy: a case report. Hong Kong J Gynaecol Obstet Midwifery. 2021;21(2):76–79.
19. Washburn L, Mahipal A, Jatoi A, Kottschade L, Tran N. Postpartum related intrahepatic cholangiocarcinoma with FGFR2 fusion and severe hyperbilirubinemia with response to FGFR inhibitor pemigatinib: case report and review. J Gastrointest Oncol. 2023;14(6):2627–2636. doi:10.21037/jgo-23-693
20. Xiao C, Cao CJ, Xiao X, Cheng QJ. Perihilar cholangiocarcinoma masquerading as intrahepatic cholestasis of pregnancy: a case report and review of the literature. Front Med. 2024;11:1449865. doi:10.3389/fmed.2024.1449865
21. Dronova VL, Dronov OI, Lyalkin SA, Mokryk OM, Teslyuk RS. Cholangiocarcinoma in twin pregnancy: a case report. Exp Oncol. 2025;47(1):96–101. doi:10.15407/exp-oncology.2025.01.096
22. Liu M, Liu BL, Liu B, et al. Cutaneous metastasis of cholangiocarcinoma. World J Gastroenterol. 2015;21(10):3066–3071. doi:10.3748/wjg.v21.i10.3066
23. Hyun SY, Lee JH, Shin HS, Lee SW, Park YN, Park JY. Cutaneous metastasis from cholangiocarcinoma as the first clinical sign: a report of two cases. Gut Liver. 2011;5(1):100–104. doi:10.5009/gnl.2011.5.1.100
24. Petrick JL, Yang B, Alvaro D, et al. Exogenous hormone use, reproductive factors and risk of intrahepatic cholangiocarcinoma among women: results from cohort studies in the Liver Cancer Pooling Project and the UK Biobank. Br J Cancer. 2020;123(2):316–324. doi:10.1038/s41416-020-0874-3
25. Alvaro D, Mancino MG, Onori P, et al. Estrogens and the pathophysiology of the biliary tree. World J Gastroenterol. 2006;12(22):3537. doi:10.3748/wjg.v12.i22.3537
26. Gores GJ, Francis H, Alpini G. Intrahepatic cholangiocarcinoma: morpho-molecular pathology, tumor reactive microenvironment, and malignant progression. J Hepatol. 2021;74(3):696–712. doi:10.1016/j.jhep.2020.10.017
27. Purtilo DT, Clark JV, Williams R. Primary hepatic malignancy in pregnant women. Am J Obstet Gynecol. 1975;121(1):41–44. doi:10.1016/0002-9378(75)90972-2
28. Mizushima M, Abe M, Todo Y, et al. Hemostasis and life-saving by arterial embolization for a rupture of hepatic metastasis from choriocarcinoma after initiation of EMA/CO therapy: a case report and literature review. Int Cancer Conf J. 2025;14(4):446–452. doi:10.1007/s13691-025-00789-4
29. Chang C, Chen YL, Wang YW, et al. Aberrant trophoblastic differentiation in human cancer: an emerging novel therapeutic target (Review). Oncol Rep. 2024;51(3):43. doi:10.3892/or.2024.8701
30. Shaaban AM, Rezvani M, Haroun RR, et al. Gestational trophoblastic disease: clinical and imaging features. Radiographics. 2017;37(2):681–700. doi:10.1148/rg.2017160140
31. Dietrich CF, Nolsøe CP, Barr RG, et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver-Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med Biol. 2020;46(10):2579–2604. doi:10.1016/j.ultrasmedbio.2020.04.030
32. Little JM, Richardson A, Tait N. Hepatic dystychoma: a five year experience. HPB Surg. 1991;4(4):291–297. doi:10.1155/1991/96304
33. Xu HX, Chen LD, Liu LN, Zhang YF, Guo LH, Liu C. Contrast-enhanced ultrasound of intrahepatic cholangiocarcinoma: correlation with pathological examination. Br J Radiol. 2012;85(1016):1029–1037. doi:10.1259/bjr/21653786
34. Asayama Y, Yoshimitsu K, Irie H, et al. Delayed-phase dynamic CT enhancement as a prognostic factor for mass-forming intrahepatic cholangiocarcinoma. Radiology. 2006;238(1):150–155. doi:10.1148/radiol.2381041765
35. Chen Y, Zhu Y, Chen K, et al. Differentiation between hepatocellular carcinoma and intrahepatic cholangiocarcinoma using contrast-enhanced ultrasound: a systematic review and meta-analysis. Clin Hemorheol Microcirc. 2021;79(2):293–309. doi:10.3233/CH-211145
36. Kendall T, Verheij J, Gaudio E, et al. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019;39(Suppl 1):7–18. doi:10.1111/liv.14093
37. Harada K, Fujikawa T, Uemoto Y, Matsuoka T. Long-term oncological control by repeated minimally invasive hepatectomy for intrahepatic cholangiocarcinoma exhibiting atypical marker expression of CK7-CK20+: a case report. Cureus. 2023;15(12):e50639. doi:10.7759/cureus.50639
38. Vogel A, Bridgewater J, Edeline J, et al. Biliary tract cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(2):127–140. doi:10.1016/j.annonc.2022.10.506
39. Oh DY, He AR, Bouattour M, et al. Durvalumab or placebo plus gemcitabine and cisplatin in participants with advanced biliary tract cancer (TOPAZ-1): updated overall survival from a randomised Phase 3 study. Lancet Gastroenterol Hepatol. 2024;9(8):694–704. doi:10.1016/S2468-1253(24)00095-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.