Back to Journals » Clinical Ophthalmology » Volume 20
Early Visual Performance and Subjective Experience After Bilateral Implantation of a Novel Fully Refractive Extended Depth of Focus Intraocular Lens
Authors McNeely RN ![]() , Stewart SA, Mandal N, Moore JE
, Stewart SA, Mandal N, Moore JE
Received 21 February 2026
Accepted for publication 15 April 2026
Published 17 May 2026 Volume 2026:20 600320
DOI https://doi.org/10.2147/OPTH.S600320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Richard N McNeely,1 Stephen A Stewart,1,2 Niraj Mandal,1 Jonathan E Moore1,3,4
1Cathedral Eye Clinic, Belfast, NI, UK; 2School of Medicine, Dentistry and Biomedical Sciences, Queen’s University, Belfast, NI, UK; 3College of Health and Life Sciences, Aston University, Birmingham, UK; 4Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Jonathan E Moore, Cathedral Eye Clinic, Belfast, NI, UK, Email [email protected]
Purpose: To outline the early postoperative visual performance and subjective quality of vision (QoV) after implantation of a new fully refractive extended depth of focus intraocular lens (IOL).
Patients and Methods: The study enrolled 103 patients undergoing bilateral phacoemulsification with implantation of the Tecnis PureSee IOL (Johnson & Johnson). Refraction, uncorrected (UDVA) and best-corrected (CDVA) distance visual acuities, uncorrected intermediate (UIVA) and near (UNVA) visual acuities, defocus curves, electronic reading desk, QoV questionnaire and a halo and glare simulator were evaluated 3 months postoperatively.
Results: Mean binocular UDVA, UIVA and UNVA were − 0.06 ± 0.07, 0.05 ± 0.08 and 0.20 ± 0.08 logMAR respectively. At 3 months, 83% were within ± 0.50D and 99% within ± 1.00D of the refractive aim. Minimal dysphotopsias and overall QoV scores of 8.68 ± 1.13 for the day and 8.08 ± 1.58 at night were reported. Of all patients, 98.1% reported better vision than preoperatively and 86.4% would recommend the procedure. Spectacle independence for distance, intermediate, and near was achieved in 100%, 94.2% and 66% of patients respectively.
Conclusion: The Tecnis PureSee IOL provided excellent distance and intermediate vision with good functional near vision. Patients reported high postoperative QoV and subjective functional vision, with minimal visual side effects.
Keywords: EDOF intraocular lens, defocus curve, spectacle Independence, quality of vision
Introduction
Extended depth of focus (EDOF) intraocular lenses (IOLs) are now widely used in cataract surgery and refractive lens exchange. EDOF IOLs are designed to enhance the range of vision through elongation of the focal point while maintaining high visual quality and low incidence of dysphotopsia. There are numerous EDOF IOLs available with differing optical designs, including diffractive technology, pinhole effect and wavefront shaping optics.1,2 EDOF IOLs have been found to provide excellent unaided distance and intermediate vision and high levels of patient satisfaction,3–6 and functional near vision can be enhanced through using a micro-monovision approach to further improve spectacle independence rates.7
Ongoing evolution of EDOF technology aims to further optimize postoperative visual performance. A new EDOF IOL (Tecnis PureSee) has recently been introduced with a purely refractive design aiming to broaden the range of vision while maintaining a level of contrast sensitivity and dysphotopsias similar to monofocal IOLs. Since the introduction of this new purely refractive EDOF IOL laboratory studies have been published,8–11 with one optical bench study8 outlining similarity to a diffractive EDOF IOL but with a better dysphotopsia profile. Furthermore, the IOL has been shown to tolerate refractive error.12 Subsequently, two clinical studies comparing the PureSee IOL in cohorts of 60 and 25 patients with an enhanced monofocal IOL demonstrated favourable outcomes.13,14 As this IOL remains relatively new, there is still a lack of large-scale, clinically focused studies. Therefore, this study sought to present the early clinical data of a group of patients who received comprehensive assessment of both objective and subjective parameters in order to provide a clinical understanding of how this latest generation refractive EDOF IOL performs. This study aims to provide clinicians with a clear and full understanding of the early clinical performance of the Tecnis PureSee IOL.
Materials and Methods
This retrospective study recruited consecutive patients who underwent refractive lens exchange or cataract surgery with implantation of EDOF IOLs (Tecnis PureSee, Johnson & Johnson Vision Inc., Irvine, CA, USA) between July 2024 and July 2025. This study used only unidentifiable patient data and additionally all patients gave their informed consent for their anonymized data to be submitted for audit and publication. This study was conducted in compliance with the tenets of the Declaration of Helsinki, and was approved by Health and Social Care Research Ethics Committee (protocol code: 23/NI/0005). Exclusion criteria were any other ocular pathology, previous corneal surgery, corneal disease, amblyopia, ocular inflammation, a history of glaucoma or retinal detachment, neuro-ophthalmic disease, macular disease, and posterior capsular opacification requiring Nd:YAG laser capsulotomy.
All patients received comprehensive preoperative ophthalmological examination including uncorrected (UDVA) and corrected (CDVA) distance visual acuities, refractive status, ocular dominance, corneal tomography and pupillometry (MS-39 AS-OCT; CSO, Firenze, Italy), optical biometry and keratometry (IOLMaster700, Carl Zeiss Meditec AG, Jena, Germany), retinal optical coherence tomography (Cirrus 4000 OCT; Carl Zeiss Meditec), slit-lamp examination and fundoscopy. A detailed ocular history was taken to determine a history of amblyopia or any previous treatments. The IOL power was calculated using the Barrett Universal II formula or the EVO 2.0 formula.
Follow-up examinations were performed 3 months postoperatively. Postoperative examinations included, monocular and binocular UDVA, CDVA, UIVA at 70cm and UNVA at 40cm, and subjective refraction. Defocus curve assessment was obtained monocularly and binocularly using the best distance refractive correction. Reading performance was assessed on a sample of the patients included using the Salzburg Reading Desk postoperatively at fixed distances of 40cm and 66cm. Reading acuity in logMAR, reading velocity in words per minute (wpm), reading duration in seconds and letter size are reported in this study. Measurements were taken from the smallest readable sentences read with a minimum velocity of 80 wpm. Defocus curves and reading desk performance are presented with smaller cohorts of patients due to availability of data. Patients also completed a purpose-developed quality of vision (QoV) questionnaire (Supplementary Questions 1) as utilised in previous studies.7,15 The questionnaire assessed the effect of certain visual phenomena and dysphotopsias, with patients responding not at all (0), a little (1), quite (2), or very (3). In addition, to gain an understanding of how the patient actually perceives their QoV and therefore how satisfied they are postoperatively, the patient was then asked to rate his or her QoV on a linear scale out of 10 (0 the worst, 10 the best). To further assess visual disturbances a Halo & Glare Simulator (Carl Zeiss Meditec AG) was utilized. The simulator is computer-based and presents a night driving scene where the patient manually selects the type, size, and intensity of halo and glare on a subjective scale between 0 and 100. Additionally, patient experience was assessed through a purpose-developed satisfaction questionnaire regarding their distance, intermediate and near vision, glasses use and their overall satisfaction. The questions and possible responses are outlined in Supplementary Questions 2. This study reports responses to each individual item from both questionnaires, alongside QoV (0–10) scores and global satisfaction ratings, to highlight specific negative symptoms or sources of dissatisfaction while also presenting overall satisfaction outcomes.
Intraocular Lens
The Tecnis DEN00V PureSee (Johnson & Johnson Vision Inc., Irvine, CA, USA) EDOF IOL is a new fully refractive EDOF IOL. It is a 1-piece aspheric acrylic posterior chamber IOL. The IOL has an anterior aspheric surface and a posterior refractive surface which creates the continuous change in IOL power which extends the depth of focus. The IOL is made of hydrophobic acrylic material with C loop haptics. The overall length is 13.0mm and has a 6.00 mm optic diameter. The available powers are +5.0 to +34.0 D in 0.50 D increments. The IOL is preloaded in the Tecnis Simplicity™ Delivery System injector.
The Tecnis DET PureSee is the toric version of the EDOF IOL. The IOL is available in powers +5.0 to +34.0 D in 0.50 D increments, with cylinder power ranging from 1.00D to 6.00D on the IOL plane.
Surgical Technique
Surgery was performed by three surgeons (S.A.S, N.M, J.E.M). The surgery was completed with clear corneal phacoemulsification performed under Sub-Tenon anaesthesia and the foldable IOL was inserted through a 2.4 mm incision. A 5.5 mm anterior capsulorhexis was created and the IOL implanted into the capsular bag. The Zeiss Callisto Eye (Carl Zeiss Meditec AG) was utilised to rotationally align toric IOLs. The refractive aim of the first operated eye was the first myopic target. A subjective refraction was completed on the first operated eye to determine if an adjustment was required to achieve the first myopic target in the second eye. Furthermore, a slight adjustment for more myopia was targeted in the second eye if it was deemed that UNVA could be improved further, to a maximum of −0.88D. The second eye was operated within 1 week of first eye surgery.
Statistical Analysis
Preoperative and postoperative parameters were reported in means and standard deviations or percentages. Median and interquartile range were used to outline the Salzburg reading desk findings. The independent t test was used to compare continuous normal data between eyes, and the Wilcoxon rank-sum test when assessing nonparametric data between preoperative and postoperative assessments. Following the methods outlined by Goodall et al,16 a sample size of 54 patients was required for an 90% statistical power when assessing the difference in refractive status of two group within this study The standard deviation (SD) determined to be 0.4D, which was motivated by insights gained through results from previous studies of EDOF IOLs.7 A 0.25 D difference in refractive error, which is the lowest measurable value through subjective refraction was considered to be clinically significant. For all statistical analysis, the level of significance was a P value less than 0.05.
Results
This study included 206 eyes of 103 patients with a mean age of 61 ± 7.89 (45 to 81). Table 1 outlines the demographics and preoperative clinical data. No adverse events occurred in this cohort of patients.
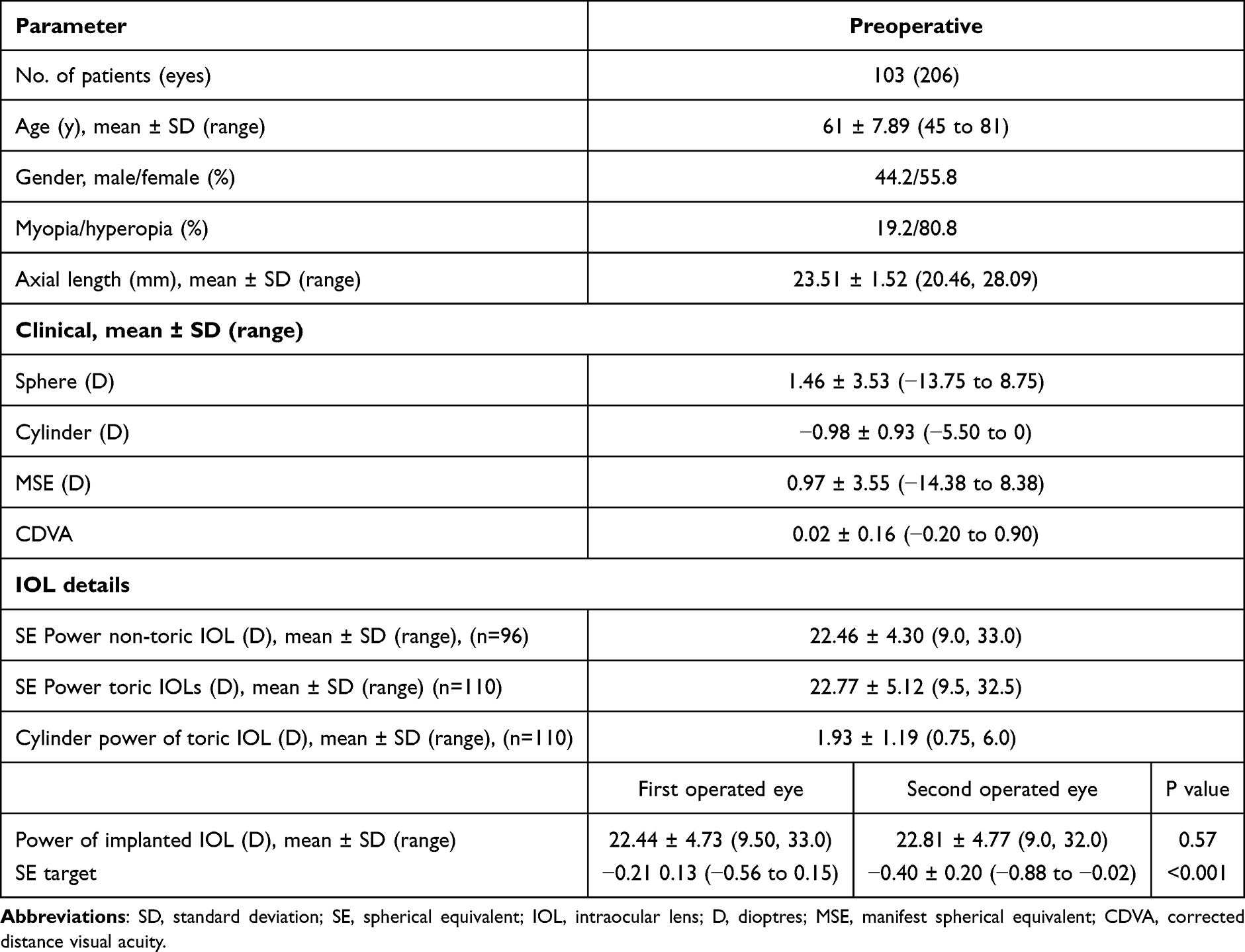 |
Table 1 Demographics and Preoperative Clinical Data |
Visual Acuity
Table 2 outlines the monocular and binocular UDVA, UIVA, and UNVA at the 3 months postoperative assessment. Binocular UDVA was −0.06 ± 0.07 logMAR, binocular UIVA was 0.05 ± 0.08 logMAR and binocular UNVA was 0.20 ± 0.08 logMAR. The second operated eye had a significantly more myopic postoperative refraction and provided significantly superior monocular UNVA compared to the first operated eye. Figure 1 outlines the binocular cumulative UDVA, UIVA, and UNVA with 100% of patients achieving a UDVA of 0.1 logMAR or better, 100% achieving 0.2 logMAR or better for UIVA and 99.05% achieving 0.4 logMAR for UNVA.
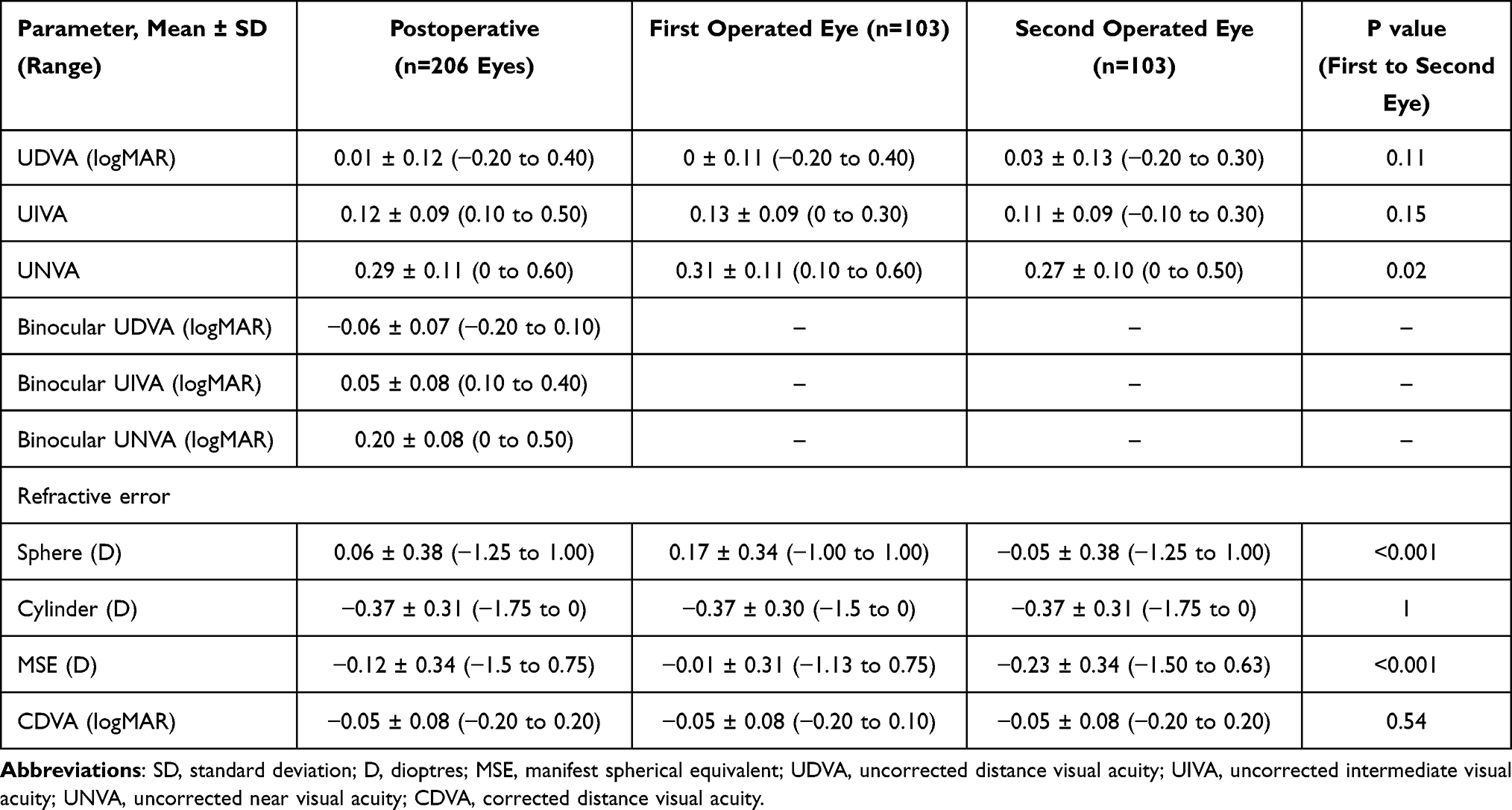 |
Table 2 Postoperative Clinical Data – 3 Months Postoperatively |
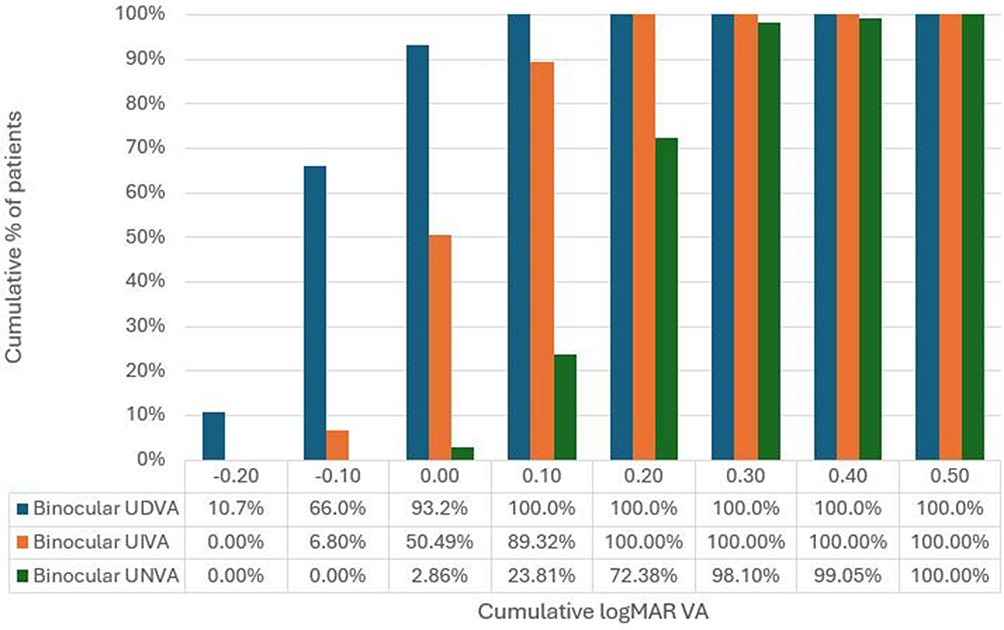 |
Figure 1 Cumulative binocular uncorrected distance, intermediate and near visual acuity 3 months postoperatively. Abbreviations: UDVA, uncorrected distance visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected Near visual acuity. |
Binocular defocus curve assessment was performed on 42 patients, and monocular defocus curve data was collected on 88 eyes. Figure 2 shows the binocular and monocular mean defocus curves 3 months postoperatively. The binocular and monocular defocus curve displayed a peak at 0.00 D with both curves having an inverted U-shape curve. A progressive and smooth reduction in visual acuity is observed as myopic defocus increases. The monocular defocus curve showed a mean visual acuity better than 0.20 logMAR within approximately +1.0 D and −2.00 D. The binocular defocus curve showed the same shape of curve but with slightly superior mean visual acuity at each step.
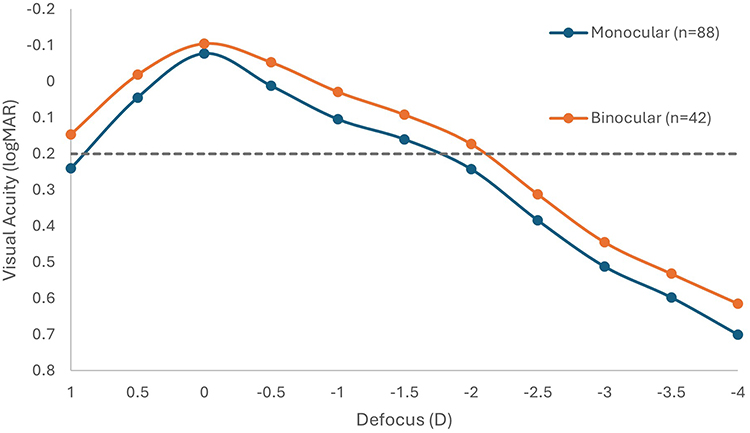 |
Figure 2 Binocular and monocular defocus curves. |
Refractive Outcomes
Table 2 shows the refractive outcomes 3 months postoperatively. Figure 3 displays the accuracy to the refractive target with 83% of eyes within ± 0.50D and 99% within ± 1.00D. The mean absolute error in this cohort 3 months postoperatively was 0.29 ± 0.22 D. Figure 4 outlines the postoperative subjective refractive cylinder, where 82.5% of eyes had 0.50 D or less, and 97.5% of eyes had 1.00D or less.
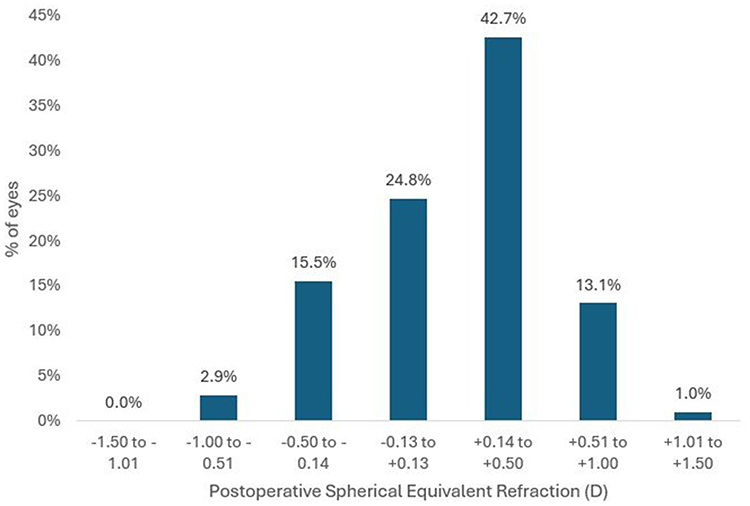 |
Figure 3 Accuracy to the intended spherical equivalent refraction 3 months postoperatively. Abbreviations: D, dioptres; SE, spherical equivalent. |
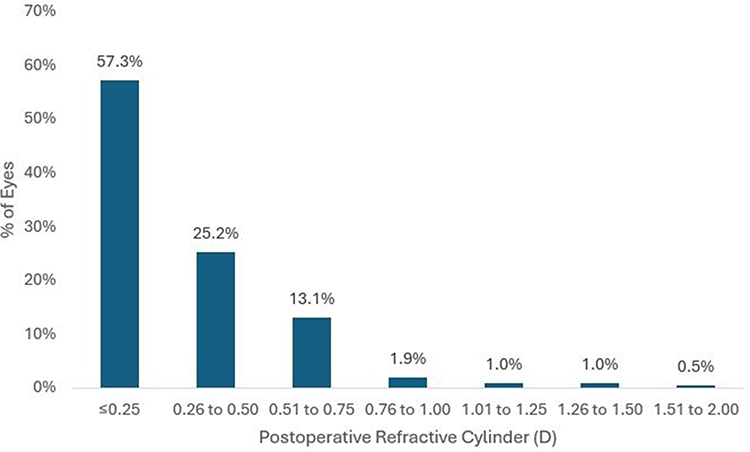 |
Figure 4 Postoperative refractive cylinder 3 months postoperatively. |
Toric versions of the IOL were implanted in 110 eyes and the mean residual refractive cylinder in these cases was −0.43 ± 0.33 D. Figure 5 outlines the cumulative percentages of both the preoperative corneal astigmatism and postoperative refractive cylinder for eyes implanted with toric IOLs.
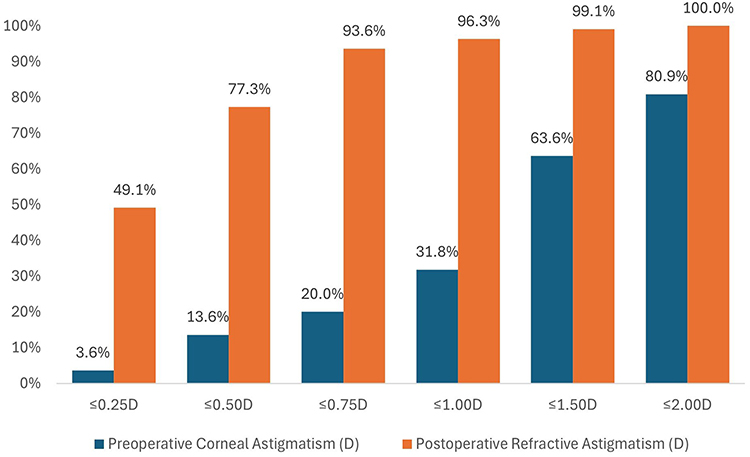 |
Figure 5 Cumulative histogram of the magnitude of the preoperative corneal and postoperative refractive cylinder, in eyes implanted with toric IOLs (n=110). |
Patient-Reported Outcomes
Table 3 outlines the responses to the QoV questionnaire utilizing 0–3 for individual symptoms and 0–10 overall score. The overall day QoV score was 8.68 ± 1.13 and the overall night score was 8.08 ± 1.58. Table 4 reports that 34 patients (33%) reported they experienced glare postoperatively, with 73.5% reporting to be either “not at all” or “a little” annoyed by this visual disturbance. The percentage of patients who reported halos was 34%, with 80% reporting an annoyance of either “not at all” or “a little”. Table 5 highlights overall satisfaction and glasses use. The percentage of patients that were “more than fulfilled” or fulfilled with the procedure was 73.8%. One hundred percent of patients reported to never require distance glasses, and 94.2% reported spectacle independence for intermediate vision and 66% for near vision.
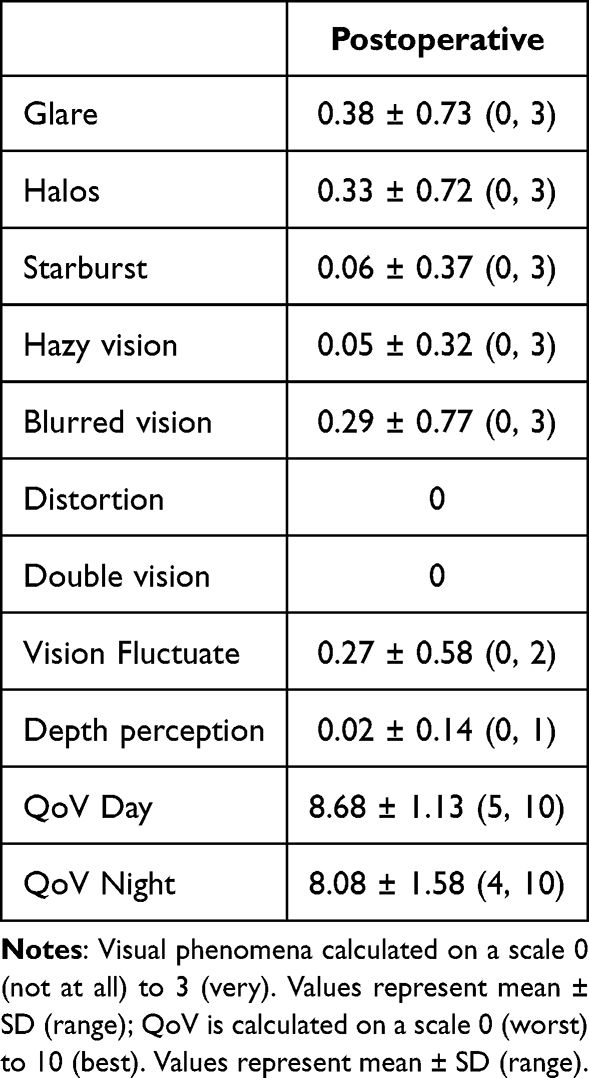 |
Table 3 Visual Phenomena – 3 Months Postoperatively |
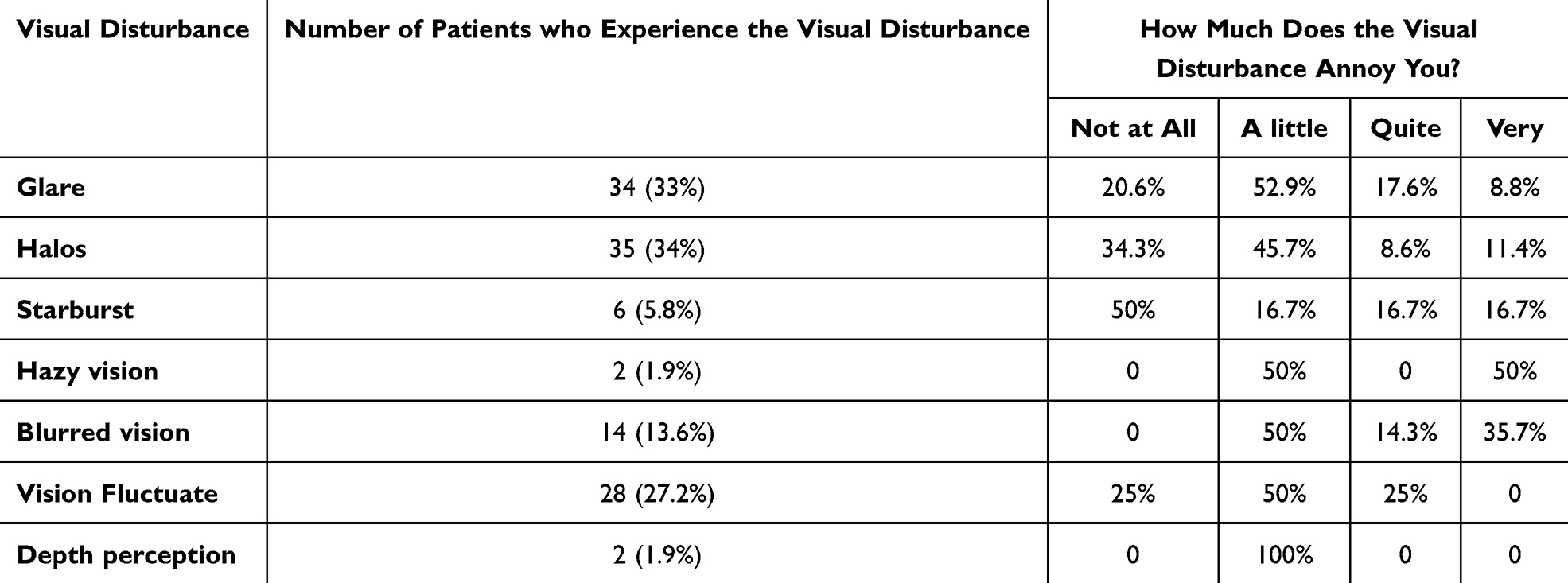 |
Table 4 Frequency of Symptoms – 3 Months Postoperatively (N= 103 Patients) |
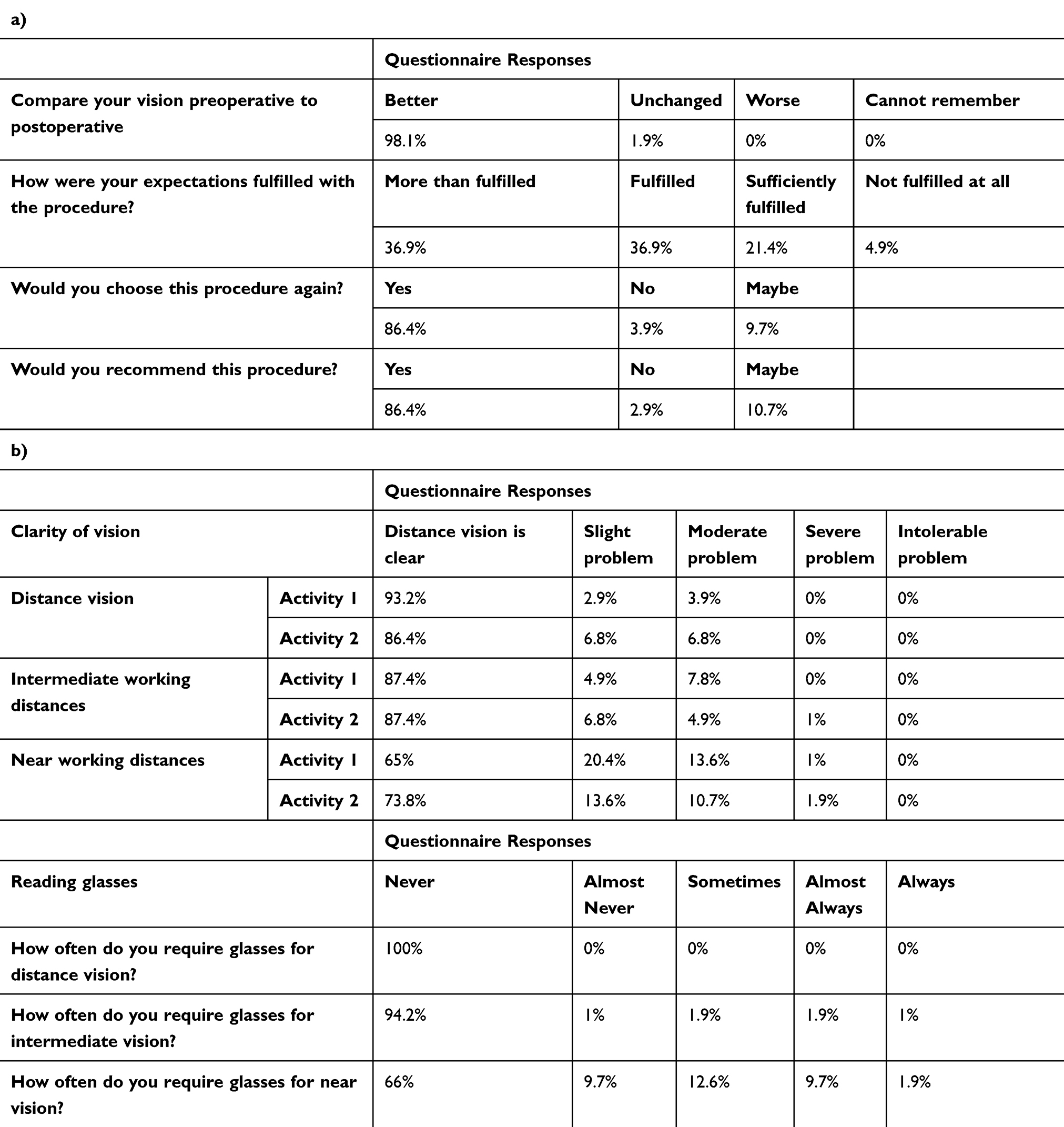 |
Table 5 Postoperative patient reported outcomes (n= 103 patients), a) overall satisfaction outcomes, b) visual and glasses use satisfaction outcomes |
Figure 6 reports the size and intensity of glare, halo and starbursts found with the halo and glare simulator in patients reporting postoperative dysphotopsias.
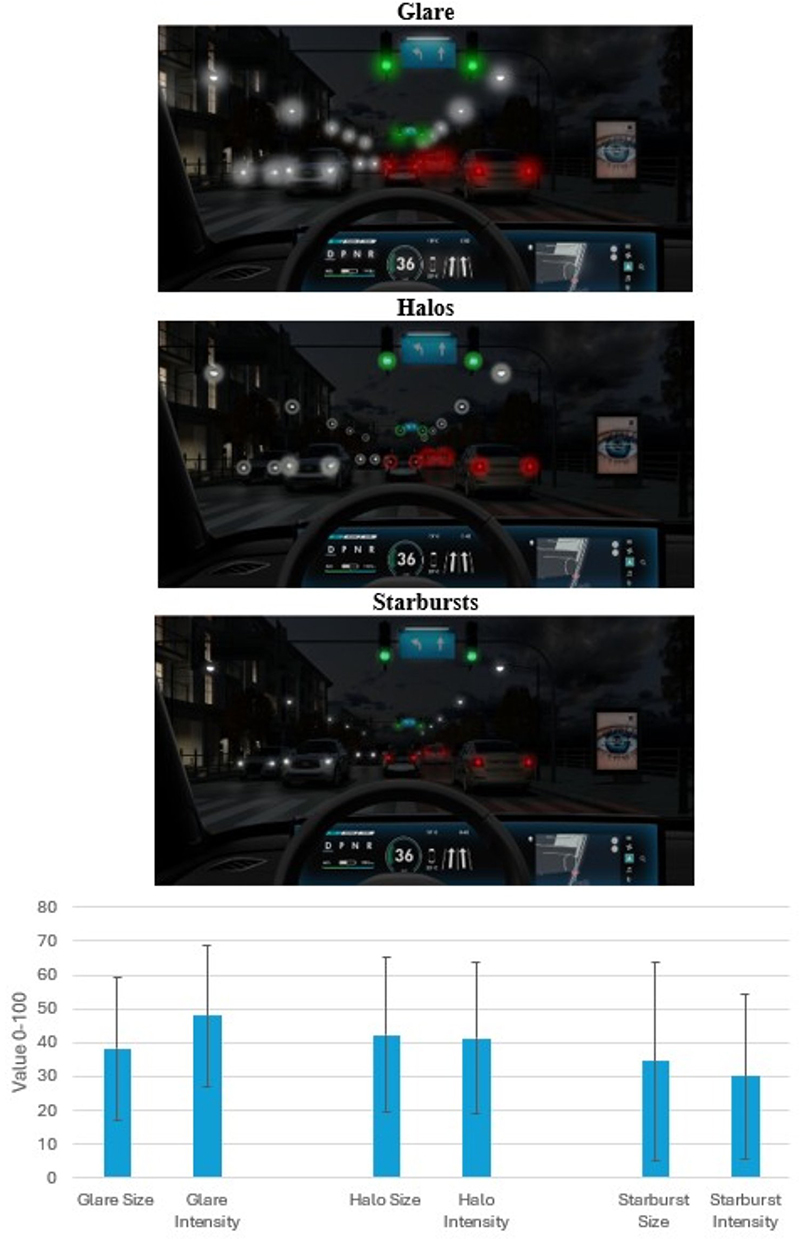 |
Figure 6 Results of Halo and Glare Simulator (Carl Zeiss Meditec AG, Jena, Germany). Depicted mean values for perceived glare, halo, starbursts, and mean ± SD values. |
Reading Performance
Table 6 displays the monocular and binocular reading performance found with the Salzburg Reading Desk at fixed distances of 40 cm and 66 cm. A median monocular reading acuity of 0.22 logMAR at 40 cm with a reading speed of 108.5wpm and letter size of 2.00M was found. Binocular reading acuity at 40cm was 0.10 logMAR at 125wpm and a letter size of 1.25M. Monocular reading acuity at 66cm was 0.13 logMAR with a rate of 122wpm and a letter size of 1.25M. A superior reading performance was noted binocularly at 66cm with reading acuity of 0.04 logMAR, at a rate of 104wpm and letter size of 1.00M.
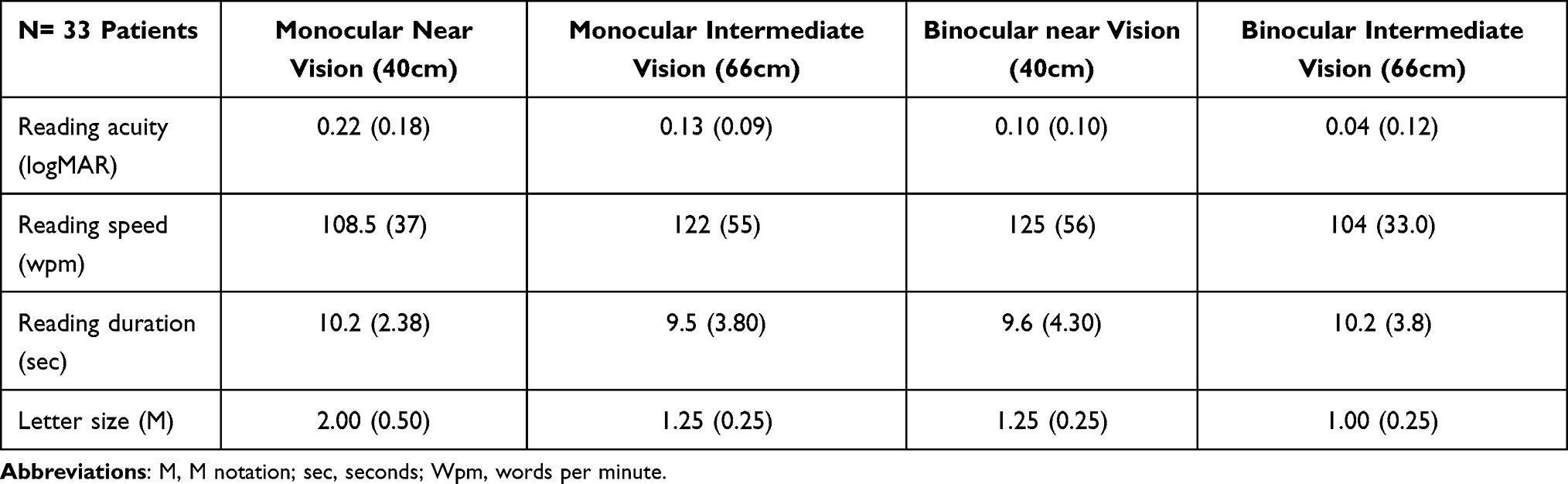 |
Table 6 Median Monocular and Binocular Near and Intermediate Distance Reading Performance with the Salzburg Reading Desk |
Discussion
EDOF IOLs are increasingly being used not only in cataract patients, but also in individuals without cataracts who desire to reduce their dependence on spectacles after surgery. A wide variety of EDOF IOLs are available to surgeons, with new options continually emerging as technology advances. When a new IOL is introduced, it is important to try and fully understand the clinical performance, both objective visual and refractive outcomes and also the subjective patient experience. Therefore, the aim of this current study is to present the early clinical and patient-reported outcomes of this new EDOF IOL in 103 patients who received bilateral implantation.
In this current study, the EDOF IOL displayed excellent binocular and monocular UDVA. The binocular UDVA was −0.06 ± 0.07 logMAR (Table 2) and all patients achieved 0.1 logMAR or better. These UDVA outcomes results are comparable to those of a conventional monofocal IOL and an enhanced monofocal IOL, with a study reporting binocular UDVA of −0.04 ± 0.09 logMAR and −0.03 ± 0.10 logMAR respectively.17 A recent study12 with the same EDOF IOL showed an inferior mean binocular UDVA of −0.03 ± 0.08 logMAR with 98.6% achieving 0.1 logMAR or better when compared to this present study. Similarly, a study4 of a nondiffractive EDOF IOL reported monocular and binocular UDVA of 0.04 ± 0.06 logMAR and 0.02 ± 0.03 logMAR respectively, with each eye having an emmetropic refractive aim. Clear intermediate vision is an important modern visual demand, and the bilateral implantation in this study provided excellent UIVA (Table 2), with 100% of patients achieving 0.2 logMAR or better 3 months postoperatively. This appears to be superior to other EDOF IOLs with a refractive aim of emmetropia.18 A recent prospective study19 comparing two novel EDOF IOLs reported binocular UIVA of 0.04 ± 0.11 and 0.15 ± 0.11 logMAR for the two groups following bilateral implantation utilizing a mini-monovision approach, compared to 0.05 ± 0.08 logMAR in this current study.
EDOF IOLs frequently provide functional vision however, it is well recognised that near vision is reduced compared to multifocal IOLs.20 As expected, this study reports inferior binocular UNVA when compared to diffractive multifocal IOLs,15,21 however performs comparably to other similar EDOF IOLs.22–24 Increasing the myopic target in the nondominant eye can improve UNVA without compromising QoV.7 A study utilising a mini-monovision approach reported a mean postoperative spherical equivalent of −0.58 ± 0.36D in the nondominant eye which resulted in mean binocular UNVA of 0.22 ± 0.12 logMAR.23 In comparison, this present study found a mean binocular UNVA of 0.20 ± 0.08 logMAR, despite a less myopic postoperative spherical equivalent in each eye.23 These findings indicate that this EDOF IOL delivers excellent performance, providing an extended range of clear vision and achieving outcomes comparable to or superior to other EDOF options. Direct comparison with other EDOF IOLs, including the differing optical designs,2 would be beneficial.
The study further evaluated differences between the first and second operated eyes. If it was deemed clinically necessary, the second eye was targeted for more myopia than the fellow first eye. Therefore, the second eye had a significantly greater myopic refractive target which ranged from −0.88 to −0.02D (Table 1). The real-life postoperative refractive outcomes are outlined in Table 2 where a clinically superior monocular UNVA in the second operated eye was also reported. Further research on the tolerance of monovision with this IOL would be valuable to determine whether higher levels of monovision significantly improve UNVA without compromising QoV.
The postoperative reading performance was also assessed with the reading desk which outlined excellent visual outcomes. The EDOF IOL in this current study showed superior reading acuity and wpm, letter size (Table 6) for both intermediate and near vision than a previous study25 reporting the reading performance of an EDOF IOL with a diffractive echelette design. Direct comparison between different IOL designs is required, however this study appears to display a good reading performance at both intermediate and near distances, and the reading desk outcomes corroborate the logMAR UIVA and UNVA values (Table 2).
Defocus curve assessment further highlights the range of vision found with this IOL, with a visual acuity of 0.2 logMAR or better being achieved to a negative range of approximately −2.00 D, which meets the standards required for EDOF IOLs.26 The defocus curve in this study was found to be similar to another study of the same IOL27 however superior to that presented in another study.13 Binocular defocus curve assessment showed superior visual acuity at each step resulting in a slightly longer range of focus (Figure 2), and was comparable to another diffractive EDOF IOL,28 however it shows a superior defocus range compared to other studies of an EDOF IOL (PureSee) and a monofocal-plus IOL.14
A high predictability was found, with 83% within ± 0.50D and 99% within ± 1.00D of the refractive aim (Figure 3). This is superior to that reported by the European registry of quality outcomes for cataract and refractive surgery where it is indicated that 73.7% of eyes are within ± 0.5D of target.29 Despite this high accuracy, there appears to be a small hyperopic tendency 3 months postoperatively. As this is a newly introduced IOL design, further refinement of the IOL constants should lead to improved refractive outcomes. Additionally, the magnitude of residual refractive astigmatism is low with 82.5% and 97.5% achieving ≤ 0.50D and ≤ 1.00D. There were 110 eyes that required a toric IOL in this study, and Figure 5 presents the postoperative refractive cylinder in these cases, where 77.3% and 96.3% had residual refractive cylinder ≤ 0.50D and ≤ 1.00D respectively. This is consistent with a previous study of toric and non-toric enhanced monofocal IOLs, which found that 81.3% and 81.6% of eyes in their respective groups had a refractive cylinder of 0.50 D or less.7
Patient-reported outcomes were also outlined in this study. The individual questions of a QoV questionnaire are outlined in Table 3. There is a low incidence of each symptom with high overall QoV scores for both day and night. Our previous study which reports QoV in the same manner displays a higher incidence of glare and halos and an inferior night QoV score with a diffractive multifocal IOL, as one would expect.15 This supports the advantage of using EDOF IOLs to reduce unwanted postoperative dysphotopsias. Comparison to an enhanced monofocal IOL, in another study reporting QoV in the same manner, reports a mean glare score of 0.38 ± 0.77, halo score of 0.18 ± 0.59 and starburst score of 0.20 ± 0.52.7 The halo score is minimally higher, and the starburst score is lower in this current study (Table 3). Table 4 also reports the frequency of visual disturbances, demonstrating a low incidence with minimal associated annoyance. Comparison to other EDOF IOLs show a similar frequency of visual disturbances. A study reports that 85% reported “none” or “just a little”, when asked “How much do you notice glare or halos around lights in dim light situations?”.30 In this current study 91.3% reported “none” or “a little” to glare, and 93.2% reported “none” or “a little” to halos individually. Figure 6 presents an image of the size and intensity of glare, halos and starbursts in those patients who report these symptoms. To our knowledge there is no study which presents the dysphotopsias for this IOL in this manner. Assessment of patient satisfaction and visual function shows a high level of postoperative satisfaction (Table 5), with 98.1% reporting to have better vision than preoperatively, and 73.8% were “more than fulfilled” or “fulfilled” with the procedure. High satisfaction for distance and intermediate vision was reported with 100% and 94.2% completely spectacle independent for these distances. For near vision, 66% of patients were completely spectacle independent, with 9.7% reporting that they “almost never” required glasses. When asked about functional near vision, 85.4% for activity 1 and 87.4% for activity 2 reported to have “clear” or “slight problem”. Spectacle independence is lower than multifocal IOLs,31 however, spectacle independence in this current study is significantly greater compared to a study of an EDOF IOL which reported only 33% reported to never need glasses.30 Compared with diffractive EDOF IOLs, which function essentially as low-powered multifocal IOLs,2 complete spectacle independence for near vision was achieved in 86.66% of cases.32 It appears this IOL produces few visual disturbances while providing a high postoperative satisfaction rate. Patient expectations should be managed with regards to complete spectacle independence.
A limitation of the current study is the absence of direct comparison of this EDOF IOL to other bilateral implantations of similar IOLs. Also, the retrospective design of this study is a limitation and the inclusion of both cataract and refractive lens exchange patients. Assessment with a longer postoperative follow-up is also required to assess the stability of visual and refractive outcomes and determine if QoV alters over time. Furthermore, an understanding of the rate of Nd:YAG laser capsulotomy and possible rates of laser enhancement with this new IOL should be presented in the future. The aim of this study was to report the outcomes of a cohort of patients in a real-world clinical setting, and it does appear to highlight a range of clear unaided visual acuity that is comparable to other studies of EDOF IOL. However, as noted, there are limitations. A prospective study design incorporating a control group will be necessary in the future to achieve a more comprehensive understanding and meaningful comparison of this IOL. Additionally, our future work will include assessment of the performance of these IOLs in eyes with previous myopic and hyperopic laser vision correction, which is of particular interest.
Conclusion
In conclusion, this retrospective study of clinical outcomes found that bilateral implantation of this new fully refractive EDOF IOL provides excellent uncorrected vision for distance and intermediate, and functional near vision providing high near satisfaction. There appears to be minimal early dysphotopsias and high overall QoV satisfaction. This IOL combination seems to be an effective approach to achieve a range of vision with minimal visual disturbances, however spectacles for near vision may still be required. This study provides the clinician with information on how this IOL clinically performs 3 months postoperatively, and may help guide preoperative discussion regarding expected visual outcomes and glasses use.
Disclosure
SS received speaker fees from Johnson and Johnson and Carl Zeiss Meditec. JM reports travel supports from Cristalens, Schwind, and Carl Zeiss; Speaker/lectures fees from Cristalens, Schwind, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. McNeely RN, Moore JE, Mehta JS, Ting DSJ. Presbyopia-correcting intraocular lenses in eyes with corneal conditions: an update. Curr Opin Ophthalmol. 2026;37(1):16–14. doi:10.1097/ICU.0000000000001175
2. Megiddo-Barnir E, Alió JL. Latest development in extended depth-of-focus intraocular lenses: an update. Asia-Pac J Ophthalmol. 2023;12(1):58–79. doi:10.1097/APO.0000000000000590
3. Győry JF, Németh G, Pesztenlehrer N. Assessing the clinical outcomes of a novel EDOF intraocular lens: a functional classification approach. BMC Ophthalmology. 2025;25(1):293. doi:10.1186/s12886-025-04114-8
4. Giannuzzi F, Carlà MM, Margollicci F, et al. Functional outcomes and quality of life after AcrySof IQ Vivity intraocular lens implantation in a real-world study. Sci Rep. 2024;14(1):20620. doi:10.1038/s41598-024-69960-w
5. Asena L, Kirci Dogan İ, Oto S, Dursun Altinors D. Comparison of visual performance and quality of life with a new nondiffractive EDOF intraocular lens and a trifocal intraocular lens. J Cataract Refract Surg. 2023;49(5):504–511. doi:10.1097/j.jcrs.0000000000001142
6. Pantanelli SM, O’Rourke T, Bolognia O, Scruggs K, Longenecker A, Lehman E. Vision and patient-reported outcomes with nondiffractive EDOF or neutral aspheric monofocal intraocular lenses. J Cataract Refract Surg. 2023;49(4):360–366. doi:10.1097/j.jcrs.0000000000001123
7. McNeely RN, Stewart S, Mandal N, Moutari S, Barsam A, Moore JE. the influence of the level of monovision upon early outcomes following the bilateral implantation of an enhanced monovision intraocular lens. Vision. 2025;9(2):41. doi:10.3390/vision9020041
8. Alarcon A, Del Aguila Carrasco A, Gounou F, Weeber H, Cánovas C, Piers P. Optical and clinical simulated performance of a new refractive extended depth of focus intraocular lens. Eye. 2024;38(Suppl S1):4–8. doi:10.1038/s41433-024-03041-0
9. Niknahad A, Wu Z, Son H-S, Auffarth GU, Khoramnia R, Łabuz G. Evaluation of Clareon Vivity and PureSee intraocular lenses: optical quality, depth of focus and misalignment effects. Sci Rep. 2025;15(1):26943. doi:10.1038/s41598-025-07970-y
10. Son H-S, Łabuz G, Wu Z, et al. Optical differentiation of presbyopia-correcting intraocular lenses with improved intermediate vision from a single manufacturer. J Refract Surg. 2025;41(10):e1098–e1105. doi:10.3928/1081597X-20250805-05
11. Schmid R, Borkenstein AF. Optical bench evaluation of the latest refractive enhanced depth of focus intraocular lens. Clin Ophthalmol. 2024;18:1921–1932. doi:10.2147/OPTH.S469849
12. Black DA, Bala C, Alarcon A, Vilupuru S. Tolerance to refractive error with a new extended depth of focus intraocular lens. Eye. 2024;38(Suppl S1):15–20. doi:10.1038/s41433-024-03040-1
13. Corbett D, Black D, Roberts TV, et al. Quality of vision clinical outcomes for a new fully-refractive extended depth of focus intraocular lens. Eye. 2024;38(Suppl S1):9–14. doi:10.1038/s41433-024-03039-8
14. Kim DY, Park ESY, Park H, et al. Comparative outcomes of the next-generation extended depth-of-focus intraocular lens and enhanced monofocal intraocular lens in cataract surgery. J Clin Med. 2025;14(14):4967. doi:10.3390/jcm14144967
15. McNeely RN, Stewart SA, Moore JE. Visual performance and subjective experience 3 months and 12 months after combined implantation of 2 new complementary continuous phase multifocal intraocular lenses. J Cataract Refract Surg. 2023;49(9):921–928. doi:10.1097/j.jcrs.0000000000001236
16. Goodall EA, Moore J, Moore T. The estimation of approximate sample size requirements necessary for clinical and epidemiological studies in vision sciences. Eye. 2009;23(7):1589–1597. doi:10.1038/eye.2009.105
17. Dell SJ, Hannan SJ, Venter JA, et al. Comparative analysis of clinical and patient-reported outcomes of a new enhanced monofocal IOL and a conventional monofocal IOL. Clin Ophthalmol. 2024;18:1157–1169. doi:10.2147/OPTH.S456332
18. Song MY, Kang KH, Lee H, Kim T-I, Koh K. A comparative study of two extended depth of focus intraocular lenses. Eye Contact Lens. 2022;48(10):433–438. doi:10.1097/ICL.0000000000000931
19. Wanten JC, Bauer NJC, Berendschot TTJM, van den Biggelaar FJHM, Nuijts RMMA. Two novel extended depth-of-focus intraocular lenses targeted for mini-monovision: a prospective randomized controlled trial. Am J Ophthalmol. 2025;276:286–296. doi:10.1016/j.ajo.2025.04.024
20. Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Ame J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
21. Rementería-Capelo LA, Contreras I, Gros-Otero J, Mariñas L, Ruiz-Alcocer J. Visual quality, patient satisfaction, and photic phenomena with a diffractive intraocular lens and its new evolved materials version. J Refract Surg. 2024;40(11):e877–e883. doi:10.3928/1081597X-20240923-02
22. Megiddo-Barnir E, Cantó-Cerdán M, Medalle RS, et al. A comparative evaluation of visual, refractive, and patient-reported outcomes of four premium intraocular lenses. Int Ophthalmol. 2025;45(1):389. doi:10.1007/s10792-025-03777-y
23. Won YK, Choi SH, Chung T-Y, Lim DH. Clinical outcomes after bilateral implantation of a wavefront-shaping extended depth of focus (EDOF) IOL with mini-monovision. J Clin Med. 2024;13(11):3225. doi:10.3390/jcm13113225
24. Sabur H, Unsal U. Visual outcomes of non-diffractive extended-depth-of-focus and enhanced monofocal intraocular lenses: a case-control study. Eur J Ophthalmol. 2023;33(1):262–268. doi:10.1177/11206721221125004
25. Attia MSA, Auffarth GU, Kretz FTA, et al. Clinical evaluation of an extended depth of focus intraocular lens with the salzburg reading desk. J Refract Surg. 2017;33(10):664–669. doi:10.3928/1081597X-20170621-08
26. Ribeiro F, Dick HB, Kohnen T, et al. Evidence-based functional classification of simultaneous vision intraocular lenses: seeking a global consensus by the ESCRS functional vision working group. J Cataract Refract Surg. 2024;50(8):794–798. doi:10.1097/j.jcrs.0000000000001502
27. Alfonso-Bartolozzi B, Martinez-Alberquilla I, Fernández-Vega-Cueto L, et al. Optical and visual outcomes of a new refractive extended depth of focus intraocular lens. J Refract Surg. 2025;41(4):e333–41. doi:10.3928/1081597X-20250221-02
28. Wu T, Wang Y, Yu J, et al. Comparison of dynamic defocus curve on cataract patients implanting extended depth of focus and monofocal intraocular lens. Eye Vis. 2023;10(1):5. doi:10.1186/s40662-022-00323-0
29. Lundström M, Brocato L, Dickman M, et al. EUREQUO annual report 2017 based on data from the European registry of quality outcomes for cataract and refractive surgery. 2017. Available from: https://www.escrs.org/media/dkrdfwxk/eurequo_annual_report2017.pdf.
30. Hovanesian JA, Jones M, Allen Q. The Vivity extended range of vision IOL vs the panoptix trifocal, ReStor 2.5 active focus and ReStor 3.0 multifocal lenses: a comparison of patient satisfaction, visual disturbances, and spectacle independence. Clin Ophthalmol. 2022;16:145–152. doi:10.2147/OPTH.S347382
31. Zhu D, Ren S, Mills K, Hull J, Dhariwal M. Rate of complete spectacle independence with a trifocal intraocular lens: a systematic literature review and meta-analysis. Ophthalmol Therapy. 2023;12(2):1157–1171. doi:10.1007/s40123-023-00657-5
32. Ganesh S, Brar S, Rp N, Rathod D. Clinical outcomes, contrast sensitivity, reading performance and patient satisfaction following bilateral implantation of AT LARA 829MP EDoF IOLs. Clin Ophthalmol. 2021;15:4247–4257. doi:10.2147/OPTH.S331860
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.