Back to Journals » International Medical Case Reports Journal » Volume 17
Early SUSVIMO in Neovascular Age-Related Macular Degeneration: Real Word Case Report and Clinical Implications
Authors Pericak J ![]() , Chin EK
, Chin EK ![]() , Almeida DRP
, Almeida DRP ![]()
Received 3 June 2024
Accepted for publication 9 October 2024
Published 15 October 2024 Volume 2024:17 Pages 849—853
DOI https://doi.org/10.2147/IMCRJ.S475284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jakob Pericak,1,2 Eric K Chin,3,4 David RP Almeida2
1State University of New York at Geneseo, Geneseo, NY, USA; 2Erie Retina Research & Center for Advanced Surgical Exploration, Erie, PA, USA; 3Retina Consultants of Southern California, Redlands, CA, USA; 4Loma Linda Eye Institute; Veterans Affair Hospital, Loma Linda, CA, USA
Correspondence: David RP Almeida, Erie Retina Research & Center for Advanced Surgical Exploration, 300 State Street, Suite 302, Erie, PA, 16507, USA, Tel +1 814.476.6227, Fax +1 888.422.5096, Email [email protected]
Purpose: The current standard of care for neovascular age-related macular degeneration is serial vascular endothelial growth factor (VEGF) inhibitor intravitreal injections at varying treatment intervals. SUSVIMO is a port-delivery system of ranibizumab that serves as an alternative, lower-maintenance treatment.
Methods: A case report from a retinal surgery clinic describing the ocular findings, diagnostic workup, and alternative treatment for an 80-year-old man presenting with new-onset neovascular age-related macular degeneration.
Results: Resolved foveal thickness, macular volume, and subretinal fluid after SUSVIMO implantation OD. The patient showed a better response to SUSVIMO than to previous anti-VEGF injections. Before the first refill, the patient began to experience subretinal fluid; however, it was resolved after the refill.
Conclusion: Although effective, real-world management of neovascular age-related macular degeneration is associated with an extensive treatment burden that can compromise treatment adherence. Herein, we describe how the port delivery system (PDS; SUSVIMO) - a refillable ocular implant that can continuously deliver a novel formulation of ranibizumab with refills possible at six months or longer - is a viable early therapy that mitigates the treatment burden of intravitreal injections.
Keywords: neovascular age-related macular degeneration, SUSVIMO, port delivery system
Introduction
Neovascular age-related macular degeneration (nAMD) involves abnormal choroidal neovascularization leading to central vision loss and is the leading cause of legal blindness in those aged 65 and older.1,2 The current standard of care for nAMD is serial vascular endothelial growth factor (VEGF) inhibitor intravitreal injections at varying treatment intervals. Although effective, current anti-VEGF therapy is limited in real-world vision gains compared to clinical trials and is associated with a significant treatment burden that can compromise patient adherence.
The port delivery system (PDS; SUSVIMO, Genentech/Roche) is a refillable ocular implant that can continuously deliver ranibizumab with refills that are possible at six months or longer. Registry trials of SUSVIMO elucidated equivalent efficacy to anti-VEGF injections but demonstrated a strong patient preference for PDS over repeated intravitreal injections.2 SUSVIMO minimizes treatment burden and can significantly improve vision, anatomic, and compliance outcomes.
Observation
An 80-year-old man presented with new-onset nAMD OD and stable intermediate dry AMD OS. The right eye displayed subretinal hemorrhage, subretinal fluid, and intraretinal fluid with a visual acuity of Snellen 20/200 OD (Figure 1A). A color fundus photograph of the right eye showed subretinal hemorrhage and exudates (Figure 2).
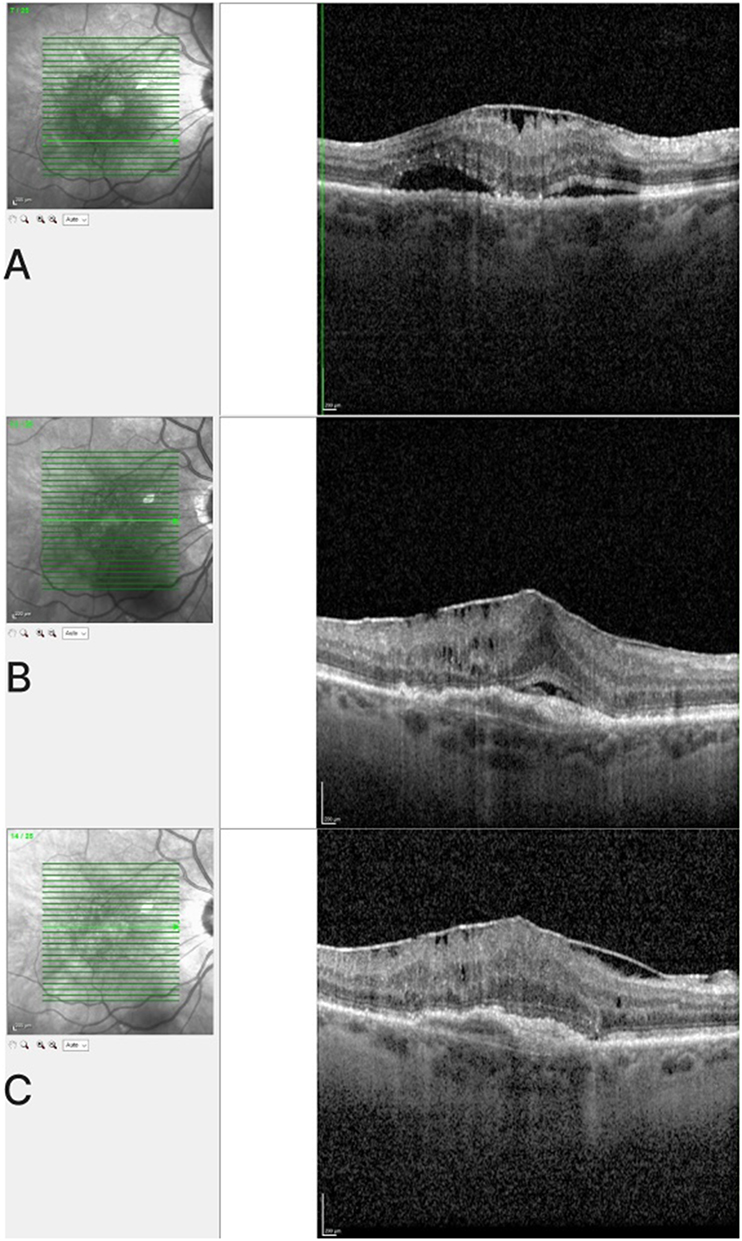 |
Figure 1 OCT images of the right eye. (A) At initial presentation, showing subretinal hemorrhage, subretinal fluid, and intraretinal fluid. (B) After two bevacizumab injections, showing minimal improvement. (C) Eight weeks post-SUSVIMO implant, showing decreased foveal central subfield thickness and macular volume. |
 |
Figure 2 Color fundus photograph of the right eye showing subretinal hemorrhage and exudates. |
After discussing the available treatment options, the patient selected SUSVIMO as the preferred management in the hopes of a more rapid visual recovery with a low treatment burden. Bevacizumab was initially chosen due to its cost-effectiveness and wide availability, as well as being the preferred first-line agent according to our local treatment protocol. Additionally, as per the patient’s insurance requirements and FDA label for SUSVIMO, two anti-VEGF injections were necessary before initiating the port delivery system. The patient received two (2) bevacizumab intravitreal injections at approximately 31 days apart; despite this, Snellen visual acuity remained 20/200 OD (Figure 1B).
The patient underwent SUSVIMO implant OD without any adverse events or complications. A clinical photograph was taken to document the position of the SUSVIMO device (Figure 3). At eight weeks postoperatively, the patient had improved Snellen visual acuity to 20/70 OD. Optical Coherence Tomography (OCT) showed decreased foveal central subfield thickness (CST) and decreased macular volume congruent with an improved anatomic phenotype (Figure 1C). The OCT also revealed the presence of an epiretinal membrane (ERM), which was noted but did not appear to significantly impact the central macular thickness or visual acuity at this time.
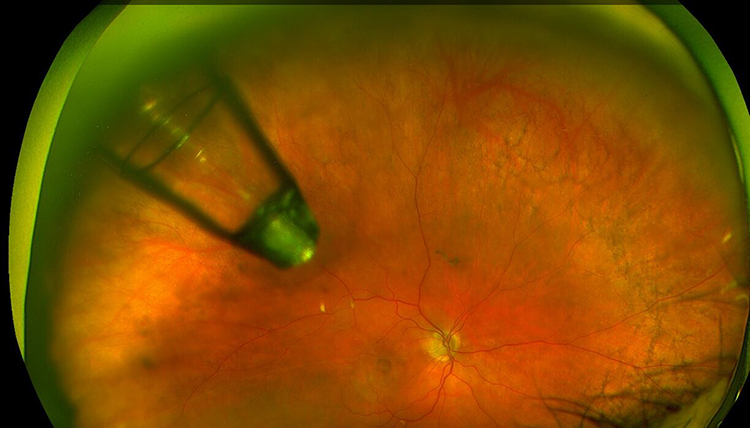 |
Figure 3 Clinical photograph showing the SUSVIMO port delivery system in situ in the patient’s right eye. |
In the case of this implant, the patient elected to continue with SUSVIMO rather than return to traditional monthly anti-VEGF injections. At 11 months post-implant and before the SUSVIMO refill, the patient exhibited recurrent subretinal fluid. It was recommended that the implant be refilled once OD to monitor progression and guide further treatment. After a refill at 12 months post-implant, OCT showed resolving subretinal fluid at 15 months post-implant, and an additional 4-month follow-up appointment was recommended to further monitor progression.
Discussion
This case highlights the improved effects of SUSVIMO as opposed to traditional bevacizumab treatments. The patient had more effective results with SUSVIMO than his prior anti-VEGF injections, including increased visual acuity and decreased foveal thickness. Given the more effective results and fewer visits, the patient did not sacrifice the convenience of SUSVIMO as opposed to monthly injections. External factors must be considered, such as patient adherence, economic burden of treatment, or transportation, when considering the significance of the difference between SUSVIMO and injections.
As of October 2022, the SUSVIMO Ocular Implant and Insertion Tool assembly (lot numbers 3499188, 3523071, Genentech/Roche) has been voluntarily recalled due to an investigation of adverse septum dislodgement of the Port Delivery System. During Phase III clinical trials, additional septum testing was found to be needed regarding multiple refills over the long term. Importantly, no cases of septum dislodgment have been reported by patients who were implanted using the commercial supply of SUSVIMO.
It’s worth noting that an epiretinal membrane was observed on OCT. While the ERM did not appear to significantly impact the treatment outcome in this case, its presence should be considered in the overall management plan, as ERMs can potentially affect visual acuity and treatment response in nAMD patients.
The current prescriber action (Genentech, Roche) states that for patients who have not experienced septum dislodgment, the benefit of SUSVIMO is still more significant than the risk of adverse events, and it has not been significantly impacted. The implant should be thoroughly inspected through the dilated pupil before and after the device is refilled to ensure that the implant is fully intact. The device should not be refilled for patients who have experienced septum dislodgement, as proper function cannot be ensured. The physician and patient can discuss the choice to keep the dislodged device in place based on risks and benefits, including the risks of removing the device.
Conclusions
As evident from our case, a decrease in treatment burden is readily apparent. With repeated success, SUSVIMO should be considered in future cases of nAMD that would enhance the patient’s outcome and provide more convenient care. If administered as first-line therapy for nAMD, SUSVIMO would prevent the early burdens of ranibizumab injections.
Ethical Statement
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a HIPAA (Health Insurance Portability and Accountability Act)-compliant manner.
Informed Consent Statement
The patient provided informed consent for diagnosis, treatment, and follow-up, as per the standard of care in the United States. Written informed consent for the publication of details was obtained from the patient. Institutional approval was not required to publish the case details.
Acknowledgments
The abstract of this paper was presented at the Congress on Controversies in Ophthalmology (COPHy 2024) as a poster presentation with interim findings.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
DA is a research and co-investigator for Acylerin, Alcon, Alimera Sciences, Allergan/Abbvie, Bausch + Lomb, Bayer, Boehringer Ingelheim, Clinical Trials Network, Dutch Ophthalmics (DORC). Eyepoint Pharmaceuticals Genentech, Gyroscope Therapeutics, Novartis, Ocugen, Opthea, Regeneron, Regenxbio, Roche; co-founder of Citrus Therapeutics. EC is a research and co-investigator for Kyowa Kirin, Janssen Biologics, Kodiak, OnPoint Vision, Genentech, Oculis, Bayer, Clearside Biomedical, Valo Health, Inc., Opthea; co-founder of Citrus Therapeutics; shareholder of Apellis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Weeks DE, Conley YP, Tsai HJ, et al. Age-related maculopathy: a genomewide scan with continued evidence of susceptibility loci within the 1q31, 10q26, and 17q25 regions. Am J Hum Genet. 2004;75(2):174–189. PMID: 15168325; PMCID: PMC1216053. doi:10.1086/422476
2. Holekamp NM, Campochiaro PA, Chang MA, et al.; all Archway Investigators. Archway randomized phase 3 trial of the port delivery system with ranibizumab for neovascular age-related macular degeneration. Ophthalmology. 2022;129(3):295–307. PMID: 34597713. doi:10.1016/j.ophtha.2021.09.016
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.