Back to Journals » International Journal of Women's Health » Volume 12
Early Resumption of Sexual Intercourse and Its Associated Factors Among Postpartum Women in Western Ethiopia: A Cross-Sectional Study
Authors Jambola ET ![]() , Gelagay AA
, Gelagay AA ![]() , Belew AK
, Belew AK ![]() , Abajobir AA
, Abajobir AA
Received 30 September 2019
Accepted for publication 16 April 2020
Published 6 May 2020 Volume 2020:12 Pages 381—391
DOI https://doi.org/10.2147/IJWH.S231859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Ebisa Turi Jambola,1 Abebaw Addis Gelagay,2 Aysheshim Kassahun Belew,3 Amanuel Alemu Abajobir4
1Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 2Department of Reproductive Health, Institute of Public Health, University of Gondar, Gondar, Ethiopia; 3Department of Human Nutrition, Institute of Public Health, University of Gondar, Gondar, Ethiopia; 4Maternal and Child Wellbeing Unit, African Population and Health Research Centre, Nairobi, Kenya
Correspondence: Ebisa Turi Jambola
Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia
Tel +251917686021
Fax +251576617980
Email [email protected]
Background: Women are often forced to recommence sexual intercourse after childbirth to maintain intimacy and fulfill their partners’ desires. Early resumption of postpartum sexual intercourse leads to sexual health problems and unwanted pregnancy if not complemented with appropriate contraceptive use. However, sexual practice during the early postpartum period has received little attention in clinical and research settings. The aim of this study was therefore to assess the early resumption of sexual intercourse and its associated factors among postpartum women attending public health institutions in Nekemte town, Western Ethiopia.
Methods: An institution-based cross-sectional study was carried out from March to April 2019. A systematic random sampling technique was used to select 528 postpartum women. An interviewer-administered, pretested, and structured questionnaire was used to collect data. Data were coded and entered into Epi Info 7.2.1, and exported to SPSS version 20.0 to run bivariable and multivariable logistic regressions.
Results: One in five postpartum women (20.2%, 95% CI: 17.1– 23.6) practiced an early resumption of sexual intercourse, of whom three-fifths (58%) did not use any contraceptives. Women’s secondary education (AOR=0.22, 95% CI: 0.07– 0.71), husband’s elementary (AOR=0.23, 95% CI: 0.06– 0.87) and secondary education (AOR=0.25, 95% CI: 0.07– 0.88), as well as women’s fertility status (parity of one) (AOR=3.52, 95% CI: 1.24– 10.01), normal vaginal delivery (AOR=5.44, 95% CI: 1.84– 16.12), giving birth to a male child (AOR=1.94, 95% CI: 1.05– 3.60), desire for another child (AOR=5.71, 95% CI: 1.89– 17.25), and pressure from the husband to initiate intercourse (AOR=9.89, 95% CI: 4.99– 19.58) were significantly associated with early resumption of sexual intercourse.
Conclusion: A significant proportion of postpartum women who resume early sexual intercourse do not use any contraceptives. Interventions that focus on strengthening the integration of postpartum sexual health education and service use are warranted.
Keywords: early resumption of sexual intercourse, postpartum women, Ethiopia
Plain Language Summary
Pregnancy, delivery, and motherhood have a great effect on women’s postpartum sexual well-being. Women in many parts of the world recommence sexual intercourse early during the postpartum period (i.e. before 6 weeks) to maintain intimacy and for other reasons, such as fulfilling their partners’ desire or wishing to reduce possible conflicts in their relationship that may arise from a disparity in sexual desire, although they may lack sexual desire. The World Health Organization (WHO) recommends that all women should be asked about the resumption of sexual intercourse and possible dyspareunia as part of an assessment of their overall well-being following childbirth. However, a sizeable number of postpartum women do not receive information or advice about their sexual health during pregnancy, including when to commence sexual activity after childbirth. Moreover, postpartum sexual health has received little attention from either clinicians’ or researchers’ perspectives. Therefore, the objective of this study was to assess the prevalence of and factors associated with early resumption of sexual intercourse among postpartum women attending public health facilities in Nekemte town, Western Ethiopia. Of the total 509 participants, 103 (20%) resumed sexual intercourse early. Both maternal and paternal educational status, as well as the mother’s fertility status, normal vaginal delivery, giving birth to a male child, a desire for another child, and being pressured by the husband, were significantly associated with early resumption of sexual intercourse. In conclusion, a significant proportion of postpartum women who resume early sexual intercourse do not use any contraceptives. Therefore, interventions that focus on strengthening the integration of postpartum sexual health education and service use are warranted.
Background
Although it is a period of joy and great expectation for parents and their families as they look forward to getting to know and love a new healthy baby, the period following childbirth is accompanied by a critical phase in the lives of both the mothers and their newborn babies. Indeed, pregnancy and childbirth bring many changes to the postpartum sexual health and well-being of mothers.1 Postpartum sexual activity is a common concern that is often not discussed during prenatal or postpartum care and has received little attention from either clinicians or researchers. Consequently, health promotion and education on postpartum sexual health is limited in current maternity care,2,3 especially in developing countries,4 although postpartum sexual health is inseparable from sexuality and sexual function.3,5 The WHO framework recommends that all women should be assessed regarding resumption of sexual intercourse and possible dyspareunia as part of an overall assessment 2–6 weeks following childbirth.6
Although postpartum care is one of the core components of the continuum of care for maternal, newborn, and child health, including sexual health,1,7 only a minority of mothers receive postnatal care compared to antenatal care in sub-Saharan Africa.8 Lack of knowledge and time limitations restrict health-care providers from counseling on sexual life after childbirth.9,10 Moreover, women’s perceptions of their partners’ sexuality may impact their postpartum sexual activity,11 and a sizeable proportion of postpartum women do not receive information or advice about sexual health during pregnancy, including when to recommence sexual activity after birth.12 In different communities of sub-Saharan Africa, sexual abstinence after childbirth is a common cultural practice, and engagement in sexual intercourse after birth is considered a taboo until the child has completely stopped breastfeeding.13 This is also true in Ethiopia, where women do not resume sexual intercourse for some time postpartum owing to cultural and religious issues. However, there is a lack of well-documented evidence on the topic to inform relevant stakeholders.
Although the early resumption of postpartum sexual intercourse may encourage the husband stay at home more, and reduce the chances of contracting sexually transmitted infections (STIs),14 it may lead to sexual morbidities such as vaginal dryness/insufficient lubrication, dyspareunia, and vaginal discharge, as well as unwanted pregnancy when the resumption of intercourse is not accompanied by appropriate contraceptive measures.14–16 This, in turn, can lead to poor maternal and child health outcomes.14 For instance, women may encounter dyspareunia, decreased sexual sensation, reduced sexual satisfaction, and an inability to achieve orgasm.17
Understanding the sexual experiences of women during the postpartum period will play an important role in maintaining family health and also establishing smooth relationships. However, most studies conducted in Ethiopia on women’s health after childbirth have focused predominantly on contraceptive utilization to prevent rapid repeat pregnancies. That is, there is a dearth of research in this regard and limited information on factors that affect women’s early return to sexual activity during the postpartum period. This study therefore aimed to assess the early resumption of sexual intercourse (i.e. before 6 weeks postpartum) and associated factors among postpartum women attending public health institutions in Western Ethiopia.
Methods
Study Design, Period, and Area
An institution-based cross-sectional study was conducted from February to April 2019 in public health facilities in Nekemte town in Western Ethiopia. Administratively, the town is divided into six sub-city administrations or 12 kebeles and an estimated 97,289 (51% females) people live in the town.18 There are four public health institutions, including two hospitals and two health centers, all of which provide integrated maternal newborn and child health (IMNCH) care.
Source and Study Population
All postpartum women attending public health facilities in Nekemte town were the source population. These included postpartum women who came for postnatal care or brought their babies for immunization to these public health facilities 6 weeks after childbirth.
Inclusion Criteria
All mothers who gave birth 6 weeks ago and came for postnatal or child immunization services during the survey period were included in the study.
Exclusion Criteria
Women who were critically ill and unable to provide informed consent to participate in the study were excluded.
Sample Size and Sampling Procedure
The sample size for this study was calculated using a formula for estimation of a single population proportion with the assumption of 95% confidence level, 4% margin of error, and taking a proportion (p) of 27.6% for the early resumption of sexual intercourse from a previous study, conducted in southwest Nigeria.19 Accordingly, the total sample size was 528 and this sample was proportionally allocated to each health facility based on the number of postpartum clients who had received service(s) in the previous month. Then, a systematic random sampling technique was used to select eligible study participants.
Data Collection Procedures and Tools
Data were collected using an interviewer-administered structured questionnaire. The questionnaire was developed by the principal investigator through an extensive literature review.2,15,20-23 It included socio-demographic, socio-economic, obstetric, and sexual history variables. The questionnaire was initially prepared in English, then translated to the local language (Afaan Oromo) and translated back to English by people who were proficient in both languages to maintain consistency. Five married female data collectors (three BSc and two diploma nurses) collected the data and were supervised by two supervisors. Appropriate training and supervision of data collectors, and immediate feedback and review of each completed questionnaire on a daily basis by the principal investigator were in place to ensure data quality. Moreover, a pretest on 10% of the sample was implemented in Nedjo General Hospital.
Data Processing and Analysis
Each completed questionnaire was coded on a prearranged coding sheet and entered into a computer using Epi Info 7.2.1.0, and data were cleaned accordingly and then exported to SPSS version 20.0 for Windows for further analyses. Descriptive analyses such as proportions, frequency distribution, and measures of central tendencies were computed. A principal component analysis was conducted for the wealth index. Bivariable and multivariable regressions were performed between the dependent variable and each of the independent variable, one at a time. Their odds ratios (ORs) and respective 95% confidence intervals (CIs) and p-values were obtained. All variables found to be significant in bivariable analyses (p≤0.2) were fitted to a multivariable logistic regression model. Violations of the regression model assumptions were checked by inspection, multicollinearity test, and variance inflation factors. Model goodness of fit was tested by the Hosmer–Lemeshow model goodness-of-fit test (p=0.11), and a forward stepwise (likelihood ratio) method was used. A p-value of <0.05 at 95% confidence level was used to declare statistical significance.
Study Variables
Dependent Variable
Early resumption of postpartum sexual intercourse was defined as women who resumed sexual intercourse before the end of the first 6 weeks of the postpartum period.21,22 It was then categorized as 1 (early), if women resumed intercourse before 6 weeks, and 0 (recommended time), if they commenced intercourse after 6 weeks of the postpartum period.
Independent Variables
These included socio-demographic, socio-economic, and obstetric factors, and sexual history variables.
Ethical Considerations
Ethical clearance and permission was obtained from the University of Gondar institutional review board (IRB). Permission was also secured from Nekemte town health office and public health facilities included in this study, and from each facility’s mother and child health (MCH) focal person. Informed consent was also obtained from each respondent.
Results
Socio-Demographic Characteristics of the Study Participants
Of the total participants (528), 509 postpartum women participated in the interview, giving a response rate of 96.4%. The mean age of the participants was 25.27 (SD ±4.12) years. Most, 472 (92.7%), were married and about one-third, 164 (32.4%), had a college education. About half, 245 (48.1%), of the women belonged to a poor wealth quantile (Table 1).
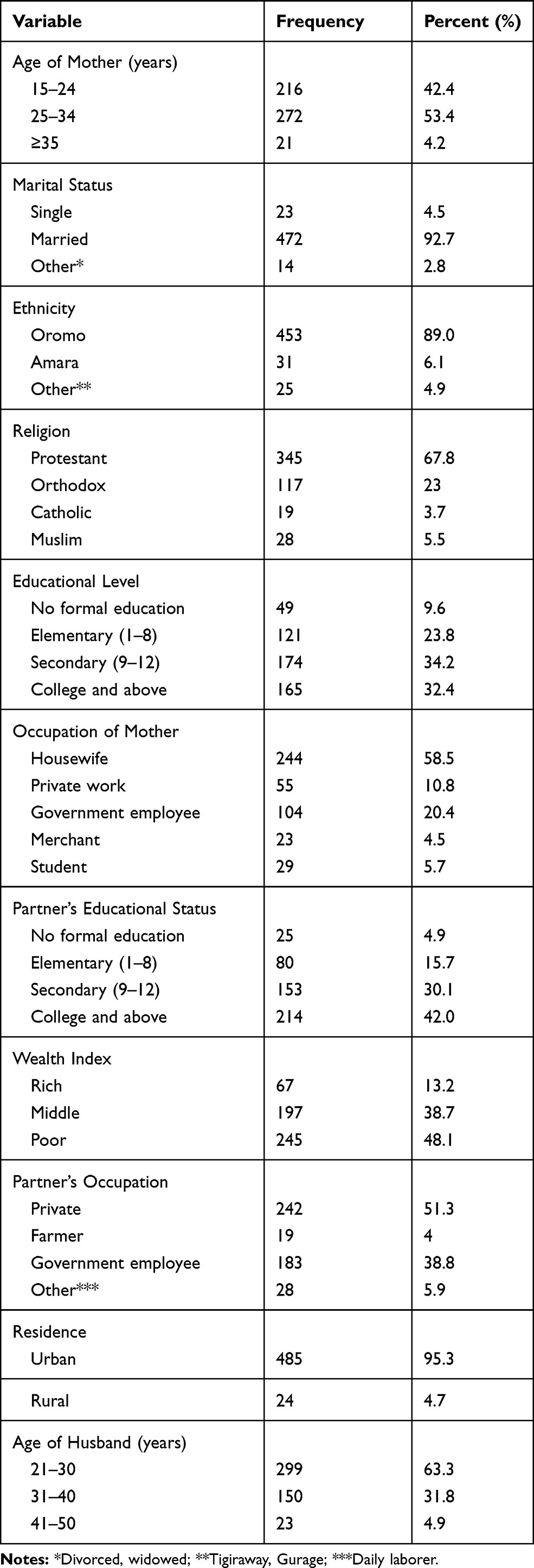 |
Table 1 Socio-Demographic Characteristics of the Postpartum Women Who Visited Public Health Institutions in Nekemte Town, Western Ethiopia, 2019 (n=509) |
Obstetric History and Reproductive Characteristics of Postpartum Women
About four in ten, 200 (39.3%), women had given birth through spontaneous vaginal delivery, and 296 (58.2%) of their babies were male. The majority of respondents, 446 (87.6%), cohabited with the father of the child after delivery. Nearly twothirds (72%) of the respondents were practicing exclusive breastfeeding. More than one-third (38.7%) of women had experienced menses return since the last childbirth. Only 224 (44%) of the participants had used family planning methods during the past 6 weeks. At the time of the interview, 34 (6.7%) of the respondents had experienced incontinence, with urinary incontinence accounting for the majority of cases (97.06%) (Table 2).
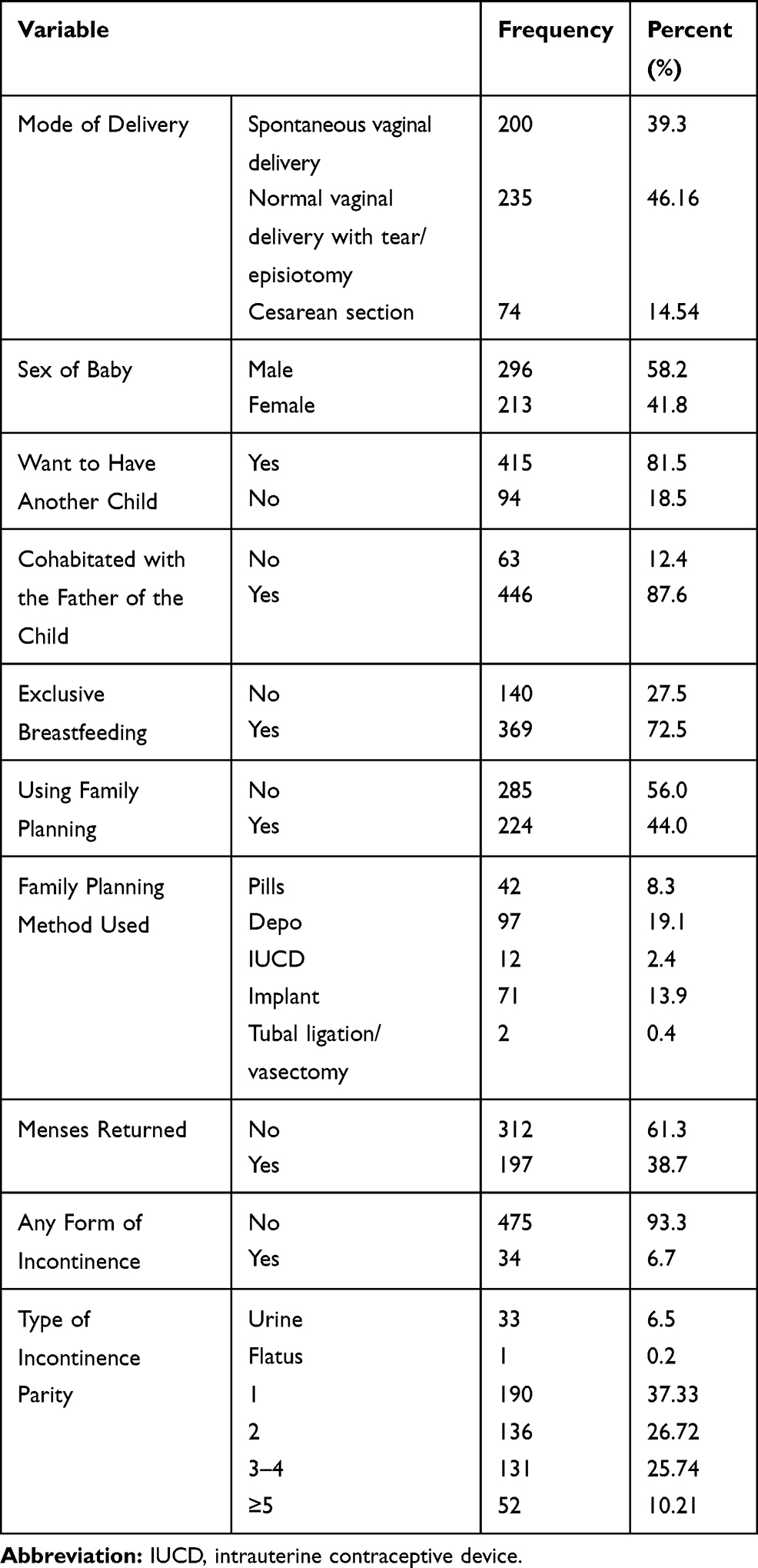 |
Table 2 Obstetric and Reproductive Characteristics of Postpartum Women Who Visited Public Health Institutions in Nekemte Town, Western Ethiopia, 2019 (n=509) |
Resumption of Sexual Intercourse
About two-thirds, 329 (64.6%), of the participants had resumed sexual intercourse at the time of the survey, of whom 103 (20.2%) had commenced within the first 6 weeks of the postpartum period. About 58% of women who resumed coitus within the first 6 weeks postpartum did not use any contraceptive methods. Of the women who had resumed sexual intercourse within the 6 weeks, 48 (46.6%) had experienced pressure from their husband to resume sexual intercourse. Only 86 (16.9%) of the total respondents had received information or advice on postpartum sexual intercourse (Table 3).
 |
Table 3 Sexual Resumption of Postpartum Women Who Visited Public Health Institutions in Nekemte Town, Western Ethiopia, 2019 |
Among those participants who had resumed sexual intercourse, 75 (22.4%) had at least one sexual morbidity or problem at the time of resumption. More than half, 40 (53.4%), of these women resumed early in the first 6 of the postpartum period. The most commonly reported sexual problem was dyspareunia, in 20 (41.73%) (Figure 1). Of those who resumed sexual intercourse early, only 41.8% used contraceptive methods. The majority (71.2%) of the participants who resumed intercourse after 6 weeks complemented it with contraceptive use (Figure 2). About one-third, 180 (35.36%), of the women were yet to commence sexual intercourse at the time of the survey. A total of 80 (44.44%) of the women had not resumed sexual intercourse because they believed that it was not yet acceptable to commence coitus after the birth of the child. The reasons given for not resuming sexual intercourse after delivery are shown in Figure 3.
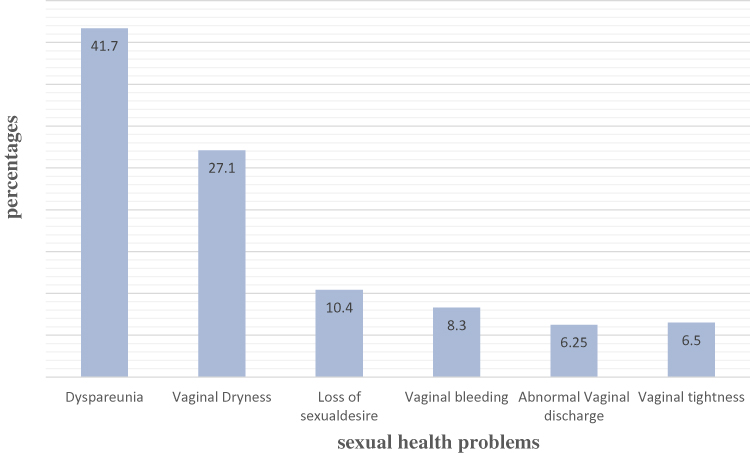 |
Figure 1 Sexual problems experienced among women who resumed sexual intercourse early. |
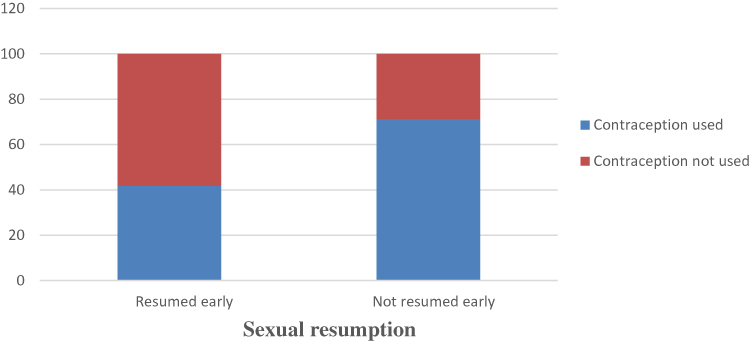 |
Figure 2 Postpartum resumption of sexual intercourse and contraceptive use. |
 |
Figure 3 Reasons for non-resumption of postpartum sexual intercourse. |
Factors Associated with Early Resumption of Sexual Intercourse
Based on binary logistic regression analyses, socio-demographic variables such as maternal age, religion, occupation, education, education of spouses and pressure from husbands, as well as obstetrics and sexual history, including parity, sex of the baby, desire to have another child, using family planning, and return of menses, were associated with resuming sexual intercourse. Most of these variables remained statistically significant at a p-value of <0.05 after adjusted analysis. That is, the odds of early resumption of sexual intercourse were 78% (AOR=0.22, 95% CI: 0.07–0.71) lower for women who had secondary education than for those with no formal education. Similarly, mothers whose husbands had attended elementary school were 77% less likely (AOR=0.23, 95% CI: 0.06–0.87) to resume sexual intercourse than those who had not received any formal education. And mothers whose husbands had attended secondary school were 75% less likely (AOR=0.25, 95% CI: 0.07–0.88) to resume early postpartum sexual intercourse than those who had had no formal education. Study participants who had a parity of one were about four times (AOR=3.5, 95% CI: 1.24, 10.01) more likely to resume early sexual intercourse than those who had had five or more deliveries. Moreover, mothers who had given birth to a male child were nearly two times (AOR=1.94, 95% CI: 1.05–3.60) more likely to resume sexual intercourse within the first 6 weeks postpartum period than those who had given birth to a female child.
Mode of delivery was another important factor which was associated with early resumption of sexual intercourse. That is, mothers who had given birth by normal vaginal delivery were about 5.4 times (AOR=5.44, 95% CI: 1.84–16.12) more likely to resume early sexual intercourse than those who had given birth by cesarean section. Participants who wanted to have another child were about six times (AOR=5.71, 95% CI: 1.89–17.25) more likely to resume sexual intercourse early after childbirth than those who did not want to have another child. Mothers who felt pressure from their husband to resume sexual intercourse were about ten times (AOR=9.89, 95% CI: 4.99–19.58) more likely to resume sexual intercourse during the early postpartum period than who did not (Table 4).
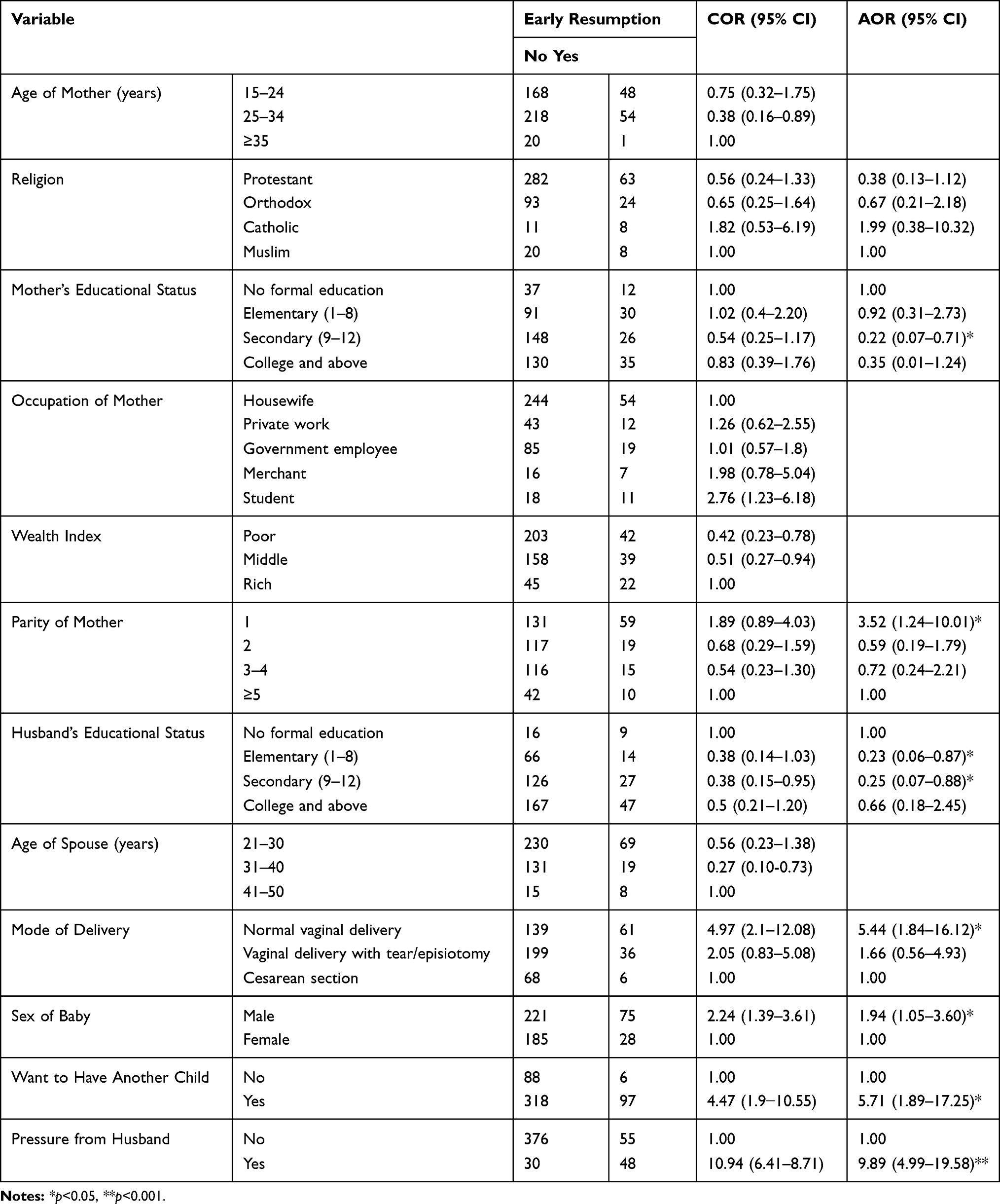 |
Table 4 Bivariable and Multivariable Analysis for Early Resumption of Sexual Intercourse Among Postpartum Women Who Visited Public Health Facilities in Nekemte Town, Western Ethiopia, 2019 |
Discussion
Women’s postpartum sexual health has received little attention compared with other components of the maternal continuum of care. Many health-care providers believe that this topic is a private issue that does not require their thorough consideration. Nevertheless, an early resumption of sexual intercourse is one of the leading causes of rapid repeat pregnancy and sexual dysfunction/problems during the postpartum period. The current study was conducted to determine the prevalence of early resumption of sexual intercourse and its associated factors among postpartum women who came for postnatal care or brought their babies for vaccination (after 6 weeks postpartum) in selected public health institutions in Western Ethiopia. The results of the study revealed that a reasonable proportion of women (20.2%; 95% CI: 17.1–23.6) resumed sexual intercourse during their 6-week postpartum period, which is similar to findings from Uganda (21.9%)21 and Nigeria (21.7%).24 However, this figure is lower than findings from other countries and regions, ranging from 24.4% to 57.7%: Spain (24.4%),20 southwest Nigeria (27.6%),25 Axum (39.4%),26 Malaysia (37.4%),22 Addis Ababa (57.7%),27 and southeast Nigeria (49.3%).28 This variation could be attributed to socio-cultural and socio-demographic differences among both the study participants and their respective countries. For instance, a study conducted in Addis Ababa included only participants who were in a union.27 In this case, couples in a union may practice an early resumption of sex as they spend an extended time together. Another possible explanation for the variations may be differences between the study designs and participants. For instance, the study from southwest Nigeria used a cohort study design and followed women for 6 months.25 This may have resulted in a higher prevalence owing to lower recall bias. Moreover, some study participants were primiparous20 and this could contribute to the difference. Socio-cultural differences could also ostensibly contribute to the observed differences. For instance, resuming sex within a short period of time is considered as a way of celebrating and congratulating the mother and new baby in Uganda. Such a culture usually demands that couples resume sex within 5 days after childbirth as an inherent practice.21,28
In this study, factors significantly associated with the early resumption of sexual intercourse among postpartum women were parity, sex of the baby, wanting to have another child, pressured by their partner to resume sexual intercourse, and using family planning. Specifically, this study found that early resumption of sexual intercourse was significantly influenced by the educational status of the respondents. Women with a secondary level of education were 78% less likely to resume early sexual intercourse than women with no formal education. This finding is supported by a study conducted in Taiwan, where women with an educational level of college or above were less likely to resume early sexual intercourse than women with a lower educational level.29 This may be due to the fact that educated women had better awareness about the effects of early resumption of sexual intercourse and had better decision-making power over their body. Husbands’ education also contributed to less frequent resumption of sexual intercourse. This finding is consistent with findings from a study conducted in Kabale, Uganda, where spousal education was inversely related to early resumption of sexual intercourse.30 Indeed, educated husbands may recognize the effects of early resumption of sexual intercourse on women’s health and rapid repeat pregnancy, and may also have better knowledge about reproductive physiology during the postpartum period.
Furthermore, reproductive history may affect the early resumption of sexual intercourse. For example, primiparous and younger women may resume sexual intercourse at an early stage.21,31,32 This may be explained by the fact that women who had a high parity may not need any more children and want to stay away from early coitus. In other words, older and multiparous women may belong to a more traditional cohort, and, thus, tend to respect the culture of refraining from early resumption of sex. Similarly, giving birth through spontaneous vaginal delivery may also enhance the early resumption of sexual intercourse.20,24,31 This is supported by accumulating evidence that suggests that the mode of delivery could influence the postpartum sexuality, in which there was a significant beneficial effect of cesarean section over operative vaginal delivery, but not over standard vaginal delivery.32–34 This could be due to anxiety and depression, attributed to the fear and pain that women perceive from the stitches associated with the procedure.35
Fertility desire (a desire to have more children) was also one of the factors associated with early resumption of sexual intercourse. This is in line with other studies in which resumption of postpartum sexual intercourse is associated with rapid repeated pregnancy and childbirth.36 Mothers who wanted to have another child were 5.7 times more likely to resume sexual intercourse during puerperium. This finding is similar to the study conducted in southwest Nigeria, in which 73% of mothers who desired more babies resumed coitus within 6 weeks of childbirth.19 It is also in line with a study conducted in Australia, in which resumption of postpartum sexual intercourse was independently significantly associated with rapid repeat pregnancy.36 The justification for this finding may be the fact that when postpartum women resume sexual activity, they may know that they are at risk for pregnancy, which may fulfill their need for another child.
Moreover, the results of this study showed that early resumption of sexual intercourse was significantly influenced by the sex of the child. Women who gave birth to a male child were about 1.94 times more likely to resume coitus early in the postpartum period compared to those who gave birth to a female child. In Ethiopian context (e.g., among Orthodox Christians), this difference may be attributable to religion, as mothers of girls should wait until 80 days for baptism of their children before they resume sexual intercourse, whereas mothers of boys should only wait 40 days for baptism, and hence, resumption of sex. It may also be due to the fact that depression is high among mothers who have given birth to a female child,37 and this, in turn, may be associated with gender preference.38
This study also revealed that the odds of early resumption of sexual intercourse were higher among participants who felt pressure from their husband. Women who experienced pressure from their husband were nearly ten times more likely to resume sexual intercourse early compared to their counterparts. This finding is in agreement with the study conducted in Uganda.30 The finding is also supported by a study conducted in Mulago, Uganda, which reported that spousal demand for sex (46%) was the main reason for resuming early sexual intercourse after childbirth.28 This may be accounted for by gender–power inequalities, where most women are subjected to more restrictions and control than men on postpartum sexual issues.39
Limitations of the Study
Our study is not without some limitations. The results of this study relied on a self-report and on the willingness of participants to give true information, and thus do not provide an objective measure of the time of resumption of sexual intercourse. The phenomena surrounding resumption of intercourse may also have been affected by recall bias. Also, the topic is sensitive and some respondents may not have revealed their real sex life. However, efforts were made to address some of the problems. For example, interviews were conducted in an isolated room and by female data collectors, so as to build trust.
Conclusion and Recommendations
A significant proportion of postpartum women who resume early sexual intercourse do not use any contraceptives. Interventions that focus on strengthening the integration of postpartum sexual health education and service use are warranted. Specifically, health-care providers should strengthen the integration of messages on postpartum sexual health education and family planning into postnatal care. Health-care providers should also capitalize on couple-centered counseling of postpartum sexuality. Finally, replication of a nationally representative study on postpartum resumption of intercourse is suggested to understand the effect of broader socio-cultural contexts on early resumption of postpartum sexual intercourse.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; IDI, in-depth interview; PCA, principal component analysis; SRS, systematic random sampling.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Ethics and Consent Statement
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance and permission was obtained from University of Gondar institutional review board (IRB) with ethical clearance letter Ref No/IPH/180/06/2019 and permission was secured from Nekemte town health office, Nekemte Specialized Hospital, and Wollega University Teaching and Referral Hospital and submitted to each public health facility’s MCH focal person. Verbal informed consent was obtained from each respondent before the interview and this was approved by the University of Gondar. This is acceptable because all participating women were married and anticipated to be empowered to provide consent on their own behalf. Indeed, this has been the trend for women participants residing in areas/communities where early marriage is common and sometimes unavoidable life circumstances.
Acknowledgments
We would like to extend our warm gratitude to the data collectors, supervisors and study participants for their cooperation and support during the study period. The authors are also grateful to the heads of all health facilities for their cooperation and to the University of Gondar and Wollega University for material support.
Author Contributions
ETJ conceived the study, developed the tool, coordinated the data collection activity, and carried out the statistical analysis, interpretation of the results, and writing up the manuscript. AAG and AKB participated in developing the tools and data analysis, and were involved in writing up the report. AAA made substantial contributions to writing up the results and reviewing the manuscript. All authors contributed to data analysis and drafting or revising the article, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by the University of Gondar. The university had no role in the design, analysis, or writing of the study.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization. Postnatal Care for Mothers and Newborns. Highlights from the World Health Organization 2013 Guidelines. RHR/15.05. Geneva; 2015.
2. Leeman LM, Rogers RG. Sex after childbirth: postpartum sexual function. Obstet Gynecol. 2012;119(3):647–655. doi:10.1097/AOG.0b013e3182479611
3. O’Malley D, Higgins A, Smith V. Postpartum sexual health: a principle-based concept analysis. J Adv Nurs. 2015;71(10):2247–2257. doi:10.1111/jan.12692
4. World Health Organization. WHO Technical Consultation on Postpartum and Postnatal Care. Geneva: WHO/MPS/10.03; 2010.
5. World Health Organization. Sexual Health and Its Linkages to Reproductive Health: An Operational Approach; 2017.
6. Postnatal Care for Mothers and Newborns Highlights from the World Health Organization 2013 Guidelines. 2015.
7. Kerber KJ, de Graft-johnson JE, Bhutta ZA, Okong P, Starrs A, Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet (London, England). 2007;370(9595):1358–1369. doi:10.1016/S0140-6736(07)61578-5
8. Duysburgh E, Kerstens B, Kouanda S, et al. Opportunities to improve postpartum care for mothers and infants: design of context-specific packages of postpartum interventions in rural districts in four sub-Saharan African countries. BMC Pregnancy Childbirth. 2015;15(1):131. doi:10.1186/s12884-015-0562-8
9. Jonas K, Crutzen R, van den Borne B, Reddy P. Healthcare workers’ behaviors and personal determinants associated with providing adequate sexual and reproductive healthcare services in sub-Saharan Africa: a systematic review. BMC Pregnancy Childbirth. 2017;17(1):86. doi:10.1186/s12884-017-1268-x
10. Olsson A, Robertson E, Falk K, Nissen E. Assessing women’s sexual life after childbirth: the role of the postnatal check. Midwifery. 2011;27(2):195–202. doi:10.1016/j.midw.2009.04.003
11. Hipp LE, Kane Low L, van Anders SM. Exploring women’s postpartum sexuality: social, psychological, relational, and birth-related contextual factors. J Sex Med. 2012;9(9):2330–2341. doi:10.1111/j.1743-6109.2012.02804.x
12. Woolhouse H, McDonald E, Brown SJ. Changes to sexual and intimate relationships in the postnatal period: women’s experiences with health professionals. Aust J Prim Health. 2014;20(3):298–304. doi:10.1071/PY13001
13. Dada O, Akesode F, Olanrewaju D, et al. Infant feeding and lactational amenorrhea in Sagamu, Nigeria. Afr J Reprod Health. 2002;6(2):39–50. doi:10.2307/3583129
14. Sule-Odu A, Fakoya T, Oluwole F, et al. Postpartum sexual abstinence and breastfeeding pattern in Sagamu, Nigeria. Afr J Reprod Health. 2008;12(1):96–100.
15. Anzaku A, Mikah S. Postpartum resumption of sexual activity, sexual morbidity and use of modern contraceptives among nigerian women in jos. Ann Med Health Sci Res. 2014;4(2):210–216. doi:10.4103/2141-9248.129044
16. Kinuthia J, Richardson BA, Drake AL, et al. Sexual behavior and vaginal practices during pregnancy and postpartum: implications for HIV prevention strategies. J Immune Def Syndr. 2017;74(2):142–149. doi:10.1097/QAI.0000000000001225
17. McDonald E, Woolhouse H, Brown SJ. Consultation about sexual health issues in the year after childbirth: a cohort study. Birth. 2015;42(4):354–361. doi:10.1111/birt.12193
18. CSA I. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International. 430; 2012.
19. Adanikin AI, Awoleke JO, Adeyiolu A, Alao O, Adanikin PO. Resumption of intercourse after childbirth in southwest Nigeria. Eur J Contracept Reprod Health Care. 2015;20(4):241–248. doi:10.3109/13625187.2014.971742
20. Trivino-Juarez JM, Romero-Ayuso D, Nieto-Pereda B, et al. Resumption of intercourse, self-reported decline in sexual intercourse and dyspareunia in women by mode of birth: a prospective follow-up study. J Adv Nurs. 2018;74(3):637–650. doi:10.1111/jan.13468
21. Alum AC, Kizza IB, Osingada CP, Katende G, Kaye DK. Factors associated with early resumption of sexual intercourse among postnatal women in Uganda. Reprod Health. 2015;12:107. doi:10.1186/s12978-015-0089-5
22. Radziah M, Shamsuddin K, Jamsiah M, et al. Early resumption of sexual intercourse and its determinants among postpartum Iban mothers. Int J Reprod Contracept Obstetrics Gynecol. 2013;124–129.
23. Abdool Z, Thakar R, Sultan AH. Postpartum female sexual function. Eur J Obstet Gynecol Reprod Biol. 2009;145(2):133–137. doi:10.1016/j.ejogrb.2009.04.014
24. Iliyasu Z, Galadanci HS, Danlami KM, Salihu HM, Aliyu MH. Correlates of postpartum sexual activity and contraceptive use in Kano, Northern Nigeria. Afr J Reprod Health. 2018;22(1):103–112. doi:10.29063/ajrh2018/v22i1.10
25. Egbuonu I, Ezechukwu C, Chukwuka J, Ikechebelu J. Breast-feeding, return of menses, sexual activity and contraceptive practices among mothers in the first six months of lactation in Onitsha, South Eastern Nigeria. J Obstet Gynaecol. 2005;25(5):500–503. doi:10.1080/01443610500171250
26. Abraha TH, Teferra AS, Gelagay AA. Postpartum modern contraceptive use in northern Ethiopia: prevalence and associated factors. Epidemiol Health. 2017;39.
27. Tesfay F, Mesfin E, Gedefaw A. Resumption of postpartum sexual intercourse and use of modern contraceptive among in-union women in Addis Ababa: cross sectional study. Ethiop J Reprod Health. 2018;10(1):22–33.
28. Odar E, Wandabwa J, Kiondo P. Sexual practices of women within six months of childbirth in Mulago hospital, Uganda. Afr Health Sci. 2003;3(3):117–123.
29. Chang SR, Chang TC, Chen KH, Lin HH. Sexual function in women 3 days and 6 weeks after childbirth: a prospective longitudinal study using the Taiwan version of the female sexual function index. J Sex Med. 2010;7(12):3946–3956. doi:10.1111/j.1743-6109.2010.01752.x
30. Osinde MO, Kaye DK, Kakaire O. Influence of HIV infection on women’s resumption of sexual intercourse and use of contraception in the postpartum period in rural Uganda. Int J Gynecol Obstetrics. 2012;116(2):171–172. doi:10.1016/j.ijgo.2011.09.018
31. Rowland M, Foxcroft L, Hopman WM, Patel R. Breastfeeding and sexuality immediately post partum. Can Fam Physician. 2005;51:1366–1367.
32. Kahramanoglu IB, Hamzaoglu M, Kubra K, Verit O, Ferda F, Yucel O. The impact of mode of delivery on the sexual function of primiparous women: a prospective study. Arch Gynecol Obstet. 2017;295(4):907–916. doi:10.1007/s00404-017-4299-7
33. Laganà AS, Butticè S, Vitale SG. Comment on “Impact of mode of delivery on female postpartum sexual functioning: spontaneous vaginal delivery and operative vaginal delivery vs cesarean section. J Sex Med. 2016;13:7.
34. Salvatore Giovanni Vitale ASL, Noventa M, Giampaolino P, et al. Transvaginal bilateral sacrospinous fixation after second recurrence of vaginal vault prolapse. Efficacy Impact Qual Life Sexual. 2018.
35. Antonio Simone Laganà VLLR, Chiara Rapisarda AM, Valenti G, et al. Anxiety and depression in patients with endometriosis: impact and management challenges; 2017.
36. Lewis LN, Doherty DA, Hickey M, Skinner SR. Predictors of sexual intercourse and rapid-repeat pregnancy among teenage mothers: an Australian prospective longitudinal study. Med J Aust. 2010;193(6):338–342. doi:10.5694/j.1326-5377.2010.tb03944.x
37. Kanika Goyal PP, Lal SN, Kaur J, Anthwal P, Puliyel JM. Correlation of infant gender with postpartum maternal and paternal depression and exclusive breastfeeding rates. Breastfeeding Med. 2017;12:5.
38. Azale T, Fekadu A, Hanlon C. Postpartum depressive symptoms in the context of high social adversity and reproductive health threats: a population-based study. Int J Ment Health Syst. 2018;12(1):42. doi:10.1186/s13033-018-0219-x
39. Mbekenga CK, Pembe AB, Darj E, Christensson K, Olsson P. Prolonged sexual abstinence after childbirth: gendered norms and perceived family health risks. Focus group discussions in a Tanzanian suburb. BMC Int Health Hum Rights. 2013;13(1):4. doi:10.1186/1472-698X-13-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.