Back to Journals » Research and Reports in Urology » Volume 18
Early Progressive Disease During Nivolumab Plus Ipilimumab Therapy Predicts Poor Survival in Japanese Patients with Advanced Renal Cell Carcinoma: A Single-Center 12-Week Landmark Study
Authors Furubayashi N ![]() , Tsujita J, Takayama A, Shiraishi Y, Nakamura M, Negishi T
, Tsujita J, Takayama A, Shiraishi Y, Nakamura M, Negishi T
Received 27 March 2026
Accepted for publication 30 May 2026
Published 5 June 2026 Volume 2026:18 612372
DOI https://doi.org/10.2147/RRU.S612372
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Nobuki Furubayashi, Jiro Tsujita, Azusa Takayama, Yuta Shiraishi, Motonobu Nakamura, Takahito Negishi
Department of Urology, National Hospital Organization Kyushu Cancer Center, Fukuoka, Japan
Correspondence: Nobuki Furubayashi, Department of Urology, National Hospital Organization Kyushu Cancer Center, Notame 3-1-1, Minami-ku, Fukuoka, 811-1395, Japan, Tel +81-925413231, Fax: +81-925514585, Email [email protected]
Background: It is clinically important to identify early progressive disease (PD) during nivolumab plus ipilimumab therapy for advanced renal cell carcinoma (RCC). However, the predictors of early PD are unclarified. We evaluated the prognostic impact and baseline predictors of early PD.
Materials and Methods: We retrospectively reviewed consecutive patients with advanced RCC who received nivolumab plus ipilimumab at Kyushu Cancer Center between September 2018 and January 2026. Tumor response was assessed using the RECIST version 1.1 guidelines. Early PD was defined as PD within 12 weeks from treatment initiation or PD at the first radiologic assessment. Overall survival (OS) was evaluated at the 12-week landmark. Cox regression was used to identify prognostic factors for landmark OS, and logistic regression was used to explore predictors of early PD.
Results: The 12-week landmark cohort comprised 38 patients (early PD, n=14; non-early PD, n=24). Landmark OS was significantly shorter in the early PD group than in the non-early PD group (median, 12.9 vs. 66.1 months; log-rank P< 0.001). In multivariable Cox regression, early PD (hazard ratio 3.67; 95% confidence interval 1.28– 10.59; P=0.016) and International Metastatic RCC Database Consortium (IMDC) poor risk (hazard ratio 3.16; 95% confidence interval 1.24– 8.07; P=0.016) were independently associated with worse OS. In exploratory multivariable logistic regression, non-clear cell histology was significantly associated with early PD (odds ratio 9.01; 95% confidence interval 1.45– 56.20; P=0.019).
Conclusion: Early PD during nivolumab plus ipilimumab identifies a high-risk population with markedly inferior survival. Non-clear cell histology was significantly associated with early PD in exploratory multivariable analysis and may help guide individualized first-line treatment selection and patient counseling in advanced RCC.
Plain Language Summary: Some patients with advanced kidney cancer treated with nivolumab plus ipilimumab experience rapid tumor growth soon after starting therapy, and these patients often have poor outcomes. We examined whether early disease worsening predicts survival and which baseline factors are linked to early worsening. We reviewed 40 patients treated at a single cancer center and performed a 12-week landmark analysis of 38 patients who were followed up for more than 12 weeks. Patients with early disease worsening had markedly shorter survival than those without early worsening. We also found that the non-clear cell tumor type was strongly associated with early worsening. These findings may help clinicians identify patients who are unlikely to benefit from nivolumab plus ipilimumab and may support informed discussions with patients when selecting first-line treatment options.
Keywords: advanced renal cell carcinoma, nivolumab, ipilimumab, early progressive disease, landmark analysis, non-clear cell histology, overall survival, IMDC risk classification
Introduction
Multiple immune checkpoint inhibitor (ICI)–based combinations have become established as standard first-line options for advanced renal cell carcinoma (RCC). Nivolumab plus ipilimumab demonstrates an overall survival (OS) benefit compared with sunitinib, with a subset of patients achieving deep and durable responses and long-term survival in extended follow-up analyses of the Phase III CheckMate 214 trial.1,2 Furthermore, ICI-based immuno-oncology (IO) combinations with tyrosine kinase inhibitors (TKIs) (IO+TKI), such as lenvatinib plus pembrolizumab and nivolumab plus cabozantinib, have shown high objective response rates and strong early disease control, expanding the therapeutic landscape and increasing the complexity of regimen selection.3,4 Contemporary clinical guidelines therefore emphasize risk-adapted, individualized treatment selection based on tumor biology, patient factors, and clinical urgency.5–7
Despite these advances, a clinically important subset of patients experiences rapid disease progression shortly after the initiation of ICI-based therapy, and this rapid progression is often associated with poor prognosis and limited opportunity for subsequent benefit. This phenomenon is conceptually aligned with primary resistance to immune checkpoint blockade, a major unmet clinical challenge across tumor types.8–10 Among patients with advanced RCC, it is important to identify those at high risk of early treatment failure because available first-line regimens differ in their typical response kinetics and durability profiles. IO+TKI regimens generally provide higher early response rates, whereas nivolumab plus ipilimumab causes a tail in survival curves consistent with durable long-term benefit in selected patients.1–4
Early treatment outcomes may also be influenced by histological subtype. Although most pivotal ICI combination trials primarily enrolled patients with clear cell RCC, patients with non-clear cell RCC comprise a heterogeneous group with distinct biology and variable sensitivity to systemic therapy. Evidence supporting the efficacy of ICI-based combinations for non-clear cell RCC remains limited, and outcomes are often less favorable than those observed for clear cell RCC, underscoring the need for practical predictors that can guide regimen selection in real-world settings.11–15 In routine practice, risk stratification tools such as the International Metastatic RCC Database Consortium (IMDC) model remain widely used and have retained prognostic relevance in the current immunotherapy era.16–18
Given the growing range of effective first-line options for advanced RCC, identifying patients at risk of early treatment failure may help inform individualized regimen selection. Such information may also support patient counseling and shared decision-making regarding the balance between early disease control and the potential for durable benefit.19,20 In Japan, the J-ENCORE study, a multicenter prospective observational study, has provided important real-world evidence regarding the effectiveness and safety of nivolumab plus ipilimumab in Japanese patients with advanced or metastatic RCC. The J-ENCORE study also evaluated early progression and its associated factors in routine clinical practice. However, because J-ENCORE was designed to assess nationwide real-world outcomes, further single-institution analyses focusing on a landmark-based evaluation of early PD and detailed clinical interpretation may complement these multicenter data.21,22 Therefore, we conducted a retrospective single-center study using a 12-week landmark analysis aligned with the routine first radiologic assessment after induction therapy. The aim of this study was to evaluate the prognostic impact of early progressive disease (PD) during nivolumab plus ipilimumab therapy in patients with advanced RCC and to explore baseline predictors of early PD, with a focus on histological subtype.
Patients and Methods
Patients
This retrospective, single-center cohort study included consecutive patients with advanced RCC who received systemic therapy at Kyushu Cancer Center between September 2018 and January 2026. Among 54 patients treated with systemic therapy during the study period, 40 who received ipilimumab plus nivolumab were included in the present analysis. Baseline clinical, pathological, and laboratory data at treatment initiation were extracted from the electronic medical records.
Treatment, Response Assessment, and Definition of Early PD
Patients were treated with ipilimumab plus nivolumab in accordance with routine clinical practice. Because the induction phase consists of four cycles administered over approximately 12 weeks, radiologic evaluation was generally performed at 12-week intervals corresponding to the routine response assessments. Tumor response and disease progression were evaluated in accordance with the Response Evaluation Criteria in Solid Tumors version 1.1. guidelines.23 Early PD was defined as PD within 12 weeks after treatment initiation or PD at the first radiologic assessment.
Endpoints and 12-Week Landmark Analysis
The primary endpoint was OS. To minimize immortal time bias24 and to align with the routine first response assessment after completion of the induction phase, a 12-week landmark approach was applied. Patients who died before 12 weeks or had insufficient follow-up (<12 weeks) were excluded, leaving 38 patients in the landmark cohort. The cohort was categorized into early PD (n=14) and non-early PD (n=24) groups based on the disease status within the first 12 weeks, and landmark OS was defined as the time from the 12-week landmark to death from any cause.
Statistical Analysis
Categorical variables are presented as numbers (percentages), while continuous variables are presented as medians (interquartile ranges (IQRs)). Group comparisons were performed using Fisher’s exact test (or the chi-squared test, as appropriate) for categorical variables. The Mann–Whitney U-test was used to compare continuous variables. OS was estimated using the Kaplan–Meier method and compared using the Log rank test. Cox proportional hazards regression was performed to evaluate factors associated with landmark OS; given the limited number of events, the multivariable model included a limited number of clinically relevant variables selected a priori to avoid overfitting. Logistic regression was used to explore predictors of early PD. Because of the limited number of early PD events, the multivariable logistic regression model was restricted to a small number of clinically relevant variables selected a priori to avoid overfitting. Automated stepwise variable selection was not used because such procedures may produce unstable estimates in small exploratory datasets. Because IMDC risk classification incorporates Karnofsky performance status,16 ECOG performance status was not included simultaneously with IMDC risk in the multivariable logistic regression model to minimize collinearity. The logistic regression analyses were interpreted as exploratory. All analyses were performed using EZR (version 1.68), and two-sided P values of <0.05 were considered statistically significant.25
Ethics
The study protocol was approved by the institutional review board of Kyushu Cancer Center (approval no. 2014–99). The requirement for informed consent was waived due to the retrospective nature of the study.
Results
Patient Selection
A total of 40 patients with advanced RCC who received nivolumab plus ipilimumab were initially assessed. Of these, two patients were excluded before the 12-week landmark: one patient died before 12 weeks and one had insufficient follow-up. Consequently, 38 patients were included in the landmark analysis cohort: 14 patients (36.8%) with early PD and 24 patients (63.2%) without early PD (Figure 1).
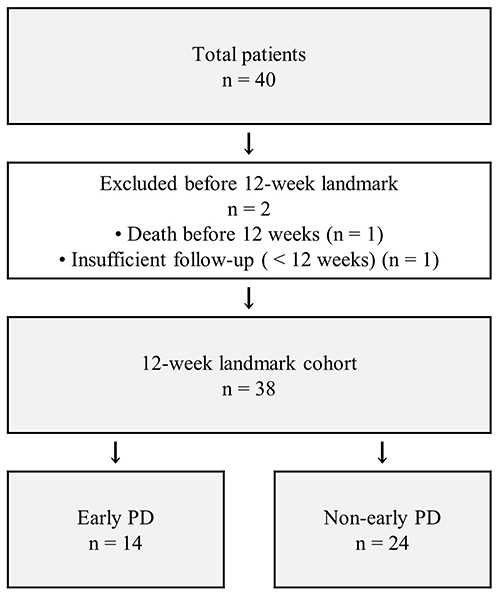 |
Figure 1 Flow diagram of patient selection for the 12-week landmark cohort. |
Baseline Characteristics of the Overall Cohort
The baseline characteristics of the overall cohort (n = 40) are summarized in Table 1. The median age was 72 years (IQR, 67–76), and 24 patients (60.0%) were men. Clear cell carcinoma was observed in 31 patients (77.5%), while nine patients (22.5%) had non-clear cell carcinoma. Among the nine patients with non-clear cell RCC, the histological subtypes were papillary RCC in one patient, unclassified RCC in five, mucinous tubular and spindle cell carcinoma in one, collecting duct carcinoma in one, and MiT family translocation RCC in one. According to the IMDC risk classification, 28 patients (70.0%) were classified as intermediate risk and 12 (30.0%) were classified as poor risk. Other baseline characteristics are shown in Table 1.
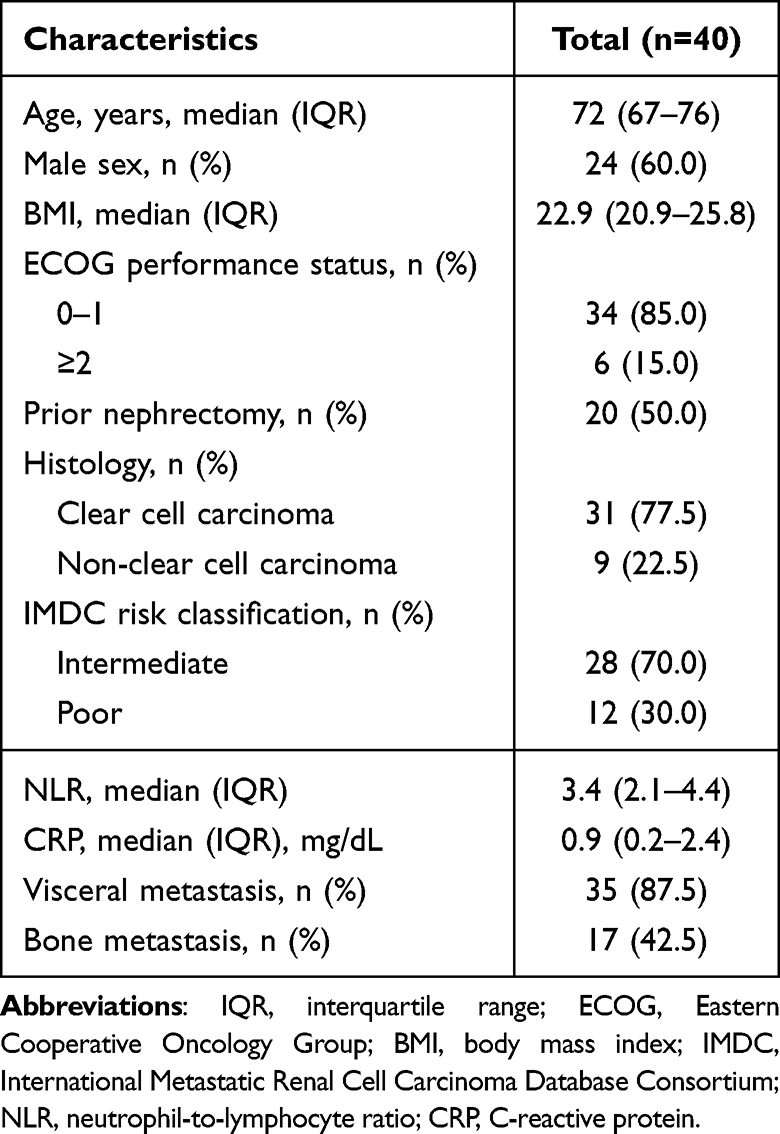 |
Table 1 Patient Characteristics |
Differences Between the Early PD and Non-Early PD Groups
The baseline characteristics stratified by early PD status are summarized in Table 2. There were no significant differences between the early PD and non-early PD groups in age, sex, body mass index, prior nephrectomy, NLR, C-reactive protein concentration, or presence of visceral or bone metastases. However, the histological subtype differed significantly between the groups. Non-clear cell carcinoma was more frequent in the early PD group than in the non-early PD group (50.0% vs. 8.3%, P = 0.006). The early PD group numerically included more patients with ECOG performance status ≥2 (28.6% vs. 8.3%, P = 0.167), IMDC poor risk classification (50.0% vs. 20.8%, P = 0.081), and higher NLR values (median 4.0 vs. 3.2, P = 0.082), although these differences did not reach statistical significance. Regarding induction treatment exposure, among the 14 patients classified as having early PD in the 12-week landmark cohort, six did not complete all four induction cycles of ipilimumab. None of these six patients discontinued induction because of grade ≥3 adverse events; all six discontinued induction because of early disease progression.
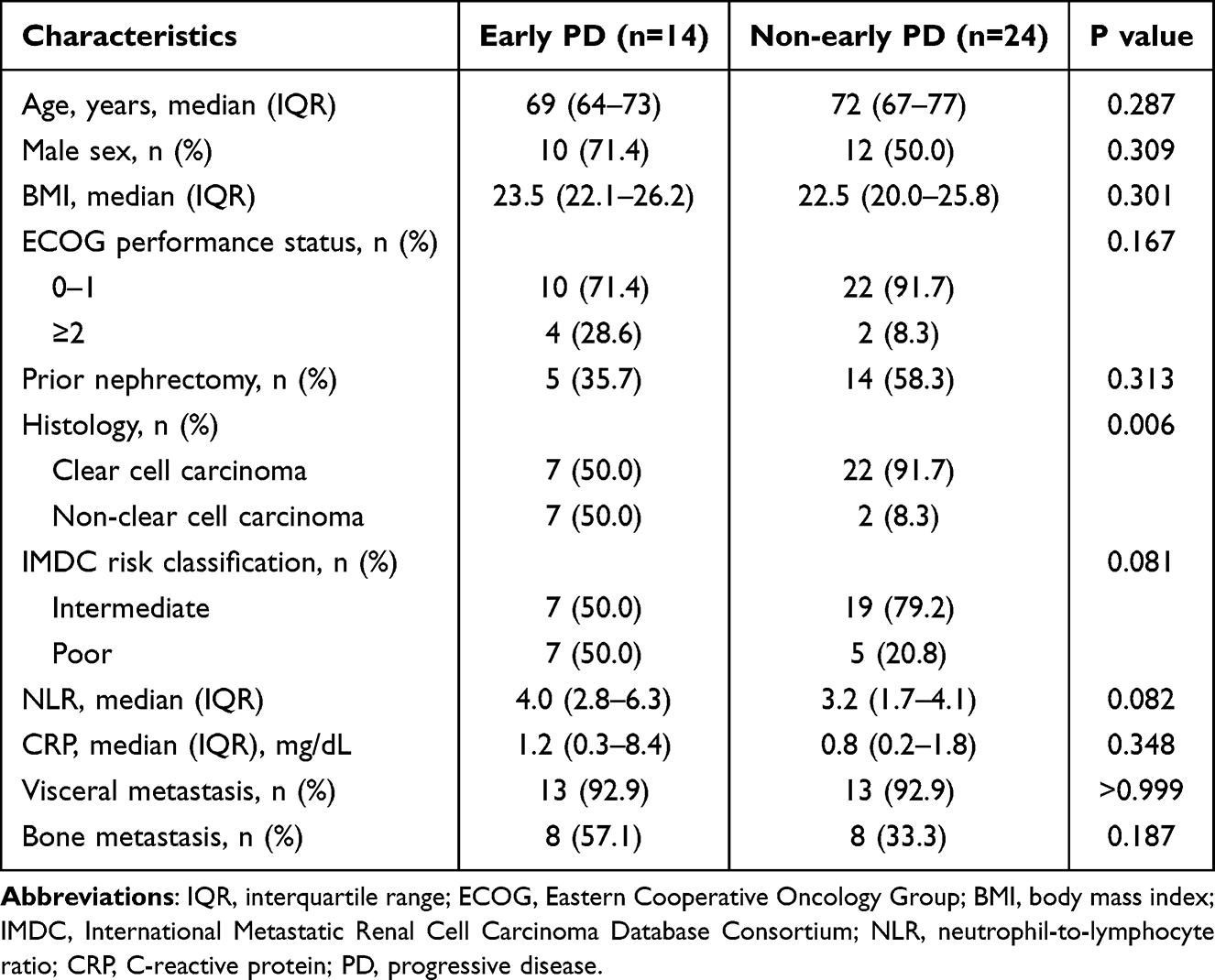 |
Table 2 Baseline Characteristics According to Early Progressive Disease Status in the 12-week Landmark Cohort |
OS in Accordance with Early PD Status
Kaplan–Meier analysis of OS from the 12-week landmark demonstrated significantly poorer OS in patients with early PD compared with those without early PD (Figure 2). The median OS was 12.9 months (95% CI, 1.9–24.9) in the early PD group and 66.1 months (95% CI, 27.9–not reached) in the non-early PD group (log-rank P < 0.001).
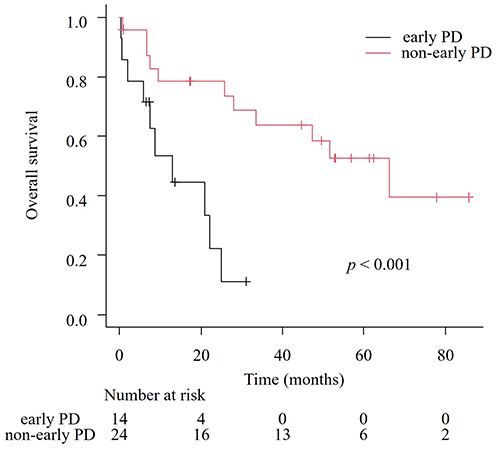 |
Figure 2 Overall survival in accordance with early progressive disease (PD) status from the 12-week landmark. |
Prognostic Factors for OS
Univariable Cox regression analysis identified several factors significantly associated with worse OS, namely early PD, IMDC poor risk classification, ECOG performance status ≥2, non-clear cell histology, and higher NLR (Table 3). Early PD was strongly associated with inferior OS (hazard ratio (HR), 4.83; 95% CI, 1.74–13.33; P = 0.002). Similarly, IMDC poor risk classification was associated with significantly worse OS compared with intermediate risk (HR, 4.11; 95% CI, 1.68–10.06; P = 0.002). Worse OS was also significantly associated with an ECOG performance status of ≥2 (HR, 4.33; 95% CI, 1.60–11.70; P = 0.004), non-clear cell histology (HR, 4.38; 95% CI, 1.75–10.97; P = 0.002), and a higher NLR (HR, 1.45; 95% CI, 1.16–1.81; P = 0.001).
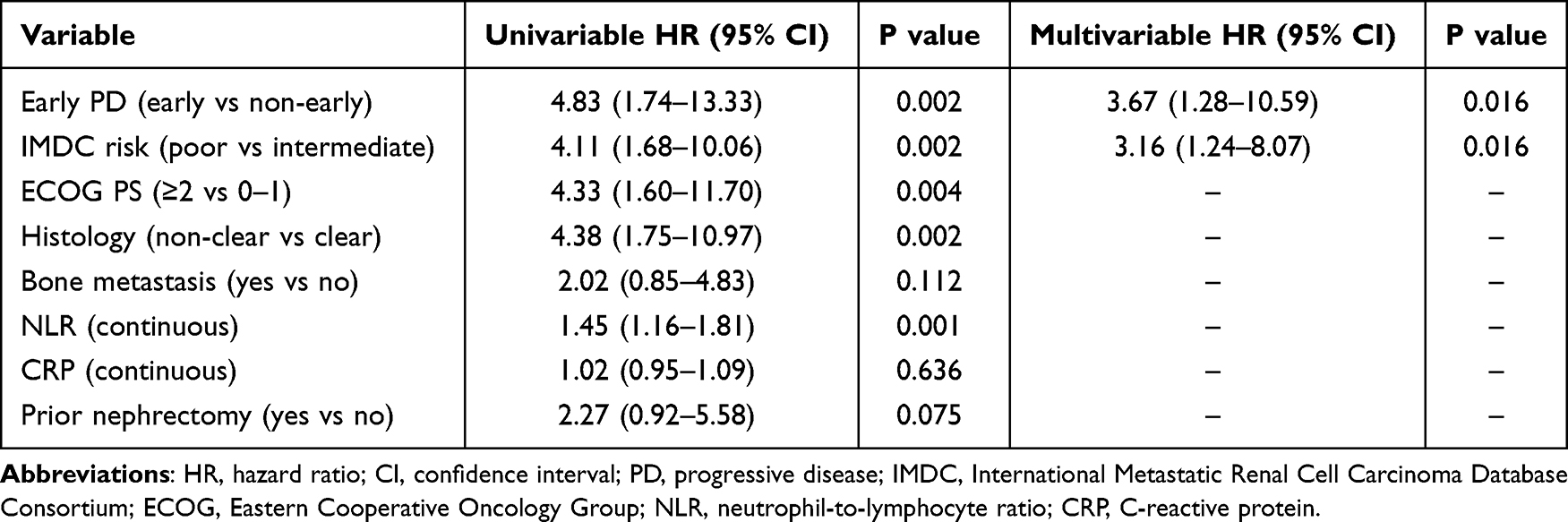 |
Table 3 Cox Proportional Hazards Regression Analysis for Landmark Overall Survival |
Multivariable Cox regression analysis including early PD and IMDC risk classification demonstrated that both factors remained independently associated with OS. Inferior OS was independently associated with early PD (HR, 3.67; 95% CI, 1.28–10.59; P = 0.016) and IMDC poor risk classification (HR, 3.16; 95% CI, 1.24–8.07; P = 0.016).
Predictors of Early PD
Univariable logistic regression analysis identified non-clear cell histology as a significant predictor of early PD (odds ratio (OR), 11.00; 95% CI, 1.84–65.70; P = 0.009) (Table 4). IMDC poor risk classification (OR, 3.80; 95% CI, 0.90–16.00; P = 0.069) and higher NLR (OR, 1.42; 95% CI, 0.98–2.06; P = 0.061) were not significantly associated with early PD.
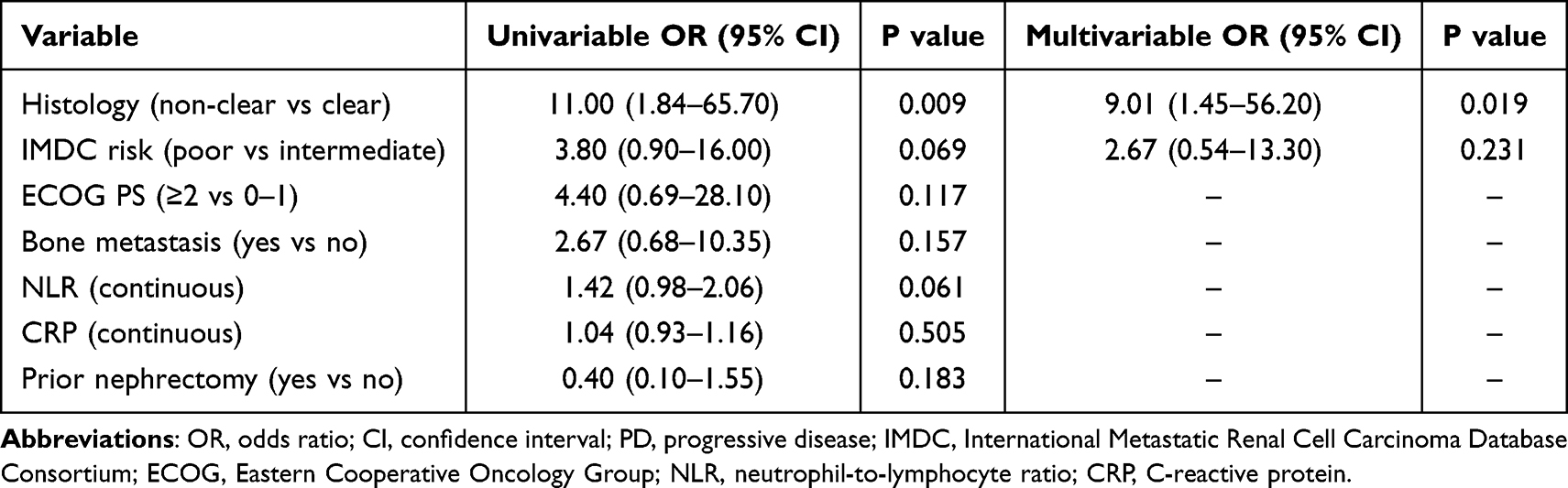 |
Table 4 Logistic Regression Analysis for Predictors of Early Progressive Disease |
In the exploratory multivariable logistic regression model including histology and IMDC risk classification, non-clear cell histology remained significantly associated with early PD (OR, 9.01; 95% CI, 1.45–56.20; P = 0.019), whereas IMDC risk classification was not significantly associated with early PD (OR, 2.67; 95% CI, 0.54–13.30; P = 0.231).
Discussion
In this retrospective study using a 12-week landmark analysis, we demonstrated that early PD during nivolumab plus ipilimumab therapy was strongly associated with inferior OS in patients with advanced RCC. Furthermore, non-clear cell histology showed a significant association with early PD in exploratory multivariable analysis. These findings highlight the clinical importance of early disease kinetics and histological subtype in guiding treatment strategies and prognostic assessment. To our knowledge, few studies have evaluated predictors of early PD using a landmark approach in patients with advanced RCC treated with nivolumab plus ipilimumab.
Our results confirmed that patients with advanced RCC treated with nivolumab plus ipilimumab who experienced early PD had significantly worse survival outcomes compared with those without early PD. This observation is consistent with previous studies demonstrating that a subset of patients treated with ICIs experience rapid disease progression and poor prognosis.1,9,10,26 In particular, the concept of primary resistance to immune checkpoint inhibition is being increasingly recognized as a major clinical challenge.8 Although early PD generally reflects primary resistance, atypical response patterns such as pseudoprogression can occur with immune checkpoint inhibitors and may complicate early radiologic interpretation in a minority of cases.27,28 In the present cohort, no patient classified as having early PD subsequently showed tumor shrinkage or a clinical course consistent with pseudoprogression. The ability to identify patients at risk of early treatment failure is therefore critical for optimizing treatment selection.
Our findings should be interpreted in the context of the Japanese multicenter J-ENCORE study. J-ENCORE provided prospective real-world evidence regarding the effectiveness and safety of nivolumab plus ipilimumab in Japanese patients with advanced or metastatic RCC and evaluated factors associated with early progression. In that study, early progression was associated with poor outcomes, and factors such as poor-risk disease, liver metastasis, elevated baseline CRP, and high NLR were reported to be associated with early progression. In contrast, the present study used a 12-week landmark design and found that non-clear cell histology was significantly associated with early PD in exploratory multivariable analysis. Although our study was limited by its single-center design and small sample size, our findings may complement J-ENCORE by highlighting histological subtype as a practical baseline factor associated with early treatment failure in routine clinical practice.21,22
The present study also found that the IMDC poor risk classification was independently associated with worse OS, which is consistent with its established prognostic value in advanced RCC.16 The IMDC model has been widely validated in the era of ICI therapy and remains a key tool for risk stratification and treatment decision-making.29 Our findings further support the continued relevance of the IMDC classification in patients receiving nivolumab plus ipilimumab.
Beyond clinical risk models, tumor-intrinsic factors such as histological subtype may further refine early risk assessment and help identify patients who are unlikely to benefit from IO+IO therapy. Importantly, we found that non-clear cell histology was strongly associated with early PD. Although nivolumab plus ipilimumab has demonstrated durable long-term efficacy in treating predominantly clear cell RCC, there is limited evidence for its efficacy in non-clear cell subtypes.30 There is little prospective research into non-clear cell RCC; however, available studies—including the dedicated non-clear cell cohort in the CheckMate 920 trial evaluating nivolumab plus ipilimumab and the KEYNOTE-427 cohort B evaluating pembrolizumab monotherapy, and the KEYNOTE-B61 Phase 2 trial evaluating pembrolizumab plus lenvatinib—have reported variable activity across histological subtypes and generally less favorable outcomes for non-clear cell RCC compared with clear cell RCC, underscoring the need for practical baseline predictors of early treatment failure.11–15 Our findings suggest that non-clear cell histology may be associated with an increased risk of early treatment failure, which has important implications for treatment selection. Because non-clear cell RCC comprises biologically heterogeneous subtypes, the association between non-clear cell histology and early PD should not be interpreted as uniform across all non-clear cell subtypes. In the present cohort, non-clear cell RCC included papillary RCC, unclassified RCC, mucinous tubular and spindle cell carcinoma, collecting duct carcinoma, and MiT family translocation RCC. However, the small number of patients within each subtype precluded subtype-specific conclusions regarding sensitivity to nivolumab plus ipilimumab.
Combination IO+TKI therapy has demonstrated higher objective response rates and improved progression-free survival compared with nivolumab plus ipilimumab, particularly in patients requiring rapid disease control.3,31 These findings suggest that IO+TKI therapy may be a reasonable option for patients at high risk of early PD, including those with non-clear cell histology. However, nivolumab plus ipilimumab remains the only regimen that has demonstrated durable long-term survival benefits in a subset of patients, with a plateau in OS curves indicating the potential for long-term disease control.1,2 This unique characteristic distinguishes IO+IO therapy from IO+TKI combinations, which typically require continuous treatment and rarely achieve treatment-free durable remission.
In this context, our findings underscore the importance of shared decision-making in treatment selection for advanced RCC. Given the trade-off between early disease control and the potential for durable response, physicians should carefully discuss the benefits and risks of each treatment strategy with patients. Patients at higher risk of early PD may prefer IO+TKI therapy to maximize the likelihood of early tumor control, whereas other patients may accept the risk of early progression in exchange for the possibility of durable long-term remission with nivolumab plus ipilimumab. Importantly, our findings should not be interpreted as evidence that nivolumab plus ipilimumab should be uniformly avoided in patients with high-risk features. In the present landmark cohort, five patients with IMDC poor-risk disease, two patients with ECOG performance status ≥2, and two patients with non-clear cell histology were included in the non-early PD group. These findings indicate that some patients with baseline high-risk features may still avoid early PD and potentially derive clinical benefit from nivolumab plus ipilimumab. Therefore, these factors should be used to support risk communication, close early monitoring, and shared decision-making, rather than serving as absolute criteria for excluding patients from IO+IO therapy. In line with this concept, we previously reported a young patient with metastatic mucinous tubular and spindle cell carcinoma, a rare subtype of non-clear cell RCC, who was treated with nivolumab plus ipilimumab based on a shared decision-making process despite the limited evidence supporting immunotherapy in this population.32 In that case, the patient’s young age and strong preference for long-term disease control were key factors influencing treatment selection, and combination immunotherapy resulted in favorable clinical outcomes. This experience suggests that treatment decisions should not rely solely on histological subtype or statistical risk factors but should also incorporate individual patient characteristics, preferences, and treatment goals. Taken together, these findings suggest that nivolumab plus ipilimumab remains a reasonable treatment option, even in patients at higher risk of early PD, provided that patients are fully informed and actively involved in treatment decision-making. Personalized treatment selection through shared decision-making may be particularly important for advanced RCC, which has multiple effective treatment options available.
The present study has several limitations. First, this was a retrospective single-institution study with a small sample size, which may limit the generalizability of our findings. Second, as treatment selection was not randomized, potential selection bias cannot be excluded. Furthermore, subsequent therapies after early PD may have influenced OS. Although most patients with early PD received second-line systemic therapy, two patients could not receive subsequent therapy because of clinical deterioration, which may have contributed to the poor survival outcomes observed in the early PD group. Third, the small number of events limited the number of variables that could be included in multivariable analyses. Nevertheless, the landmark analysis design minimized immortal time bias and allowed for more accurate assessment of the prognostic impact of early PD. Despite these limitations, our findings provide clinically meaningful insights into early treatment response and its implications for survival and treatment decision-making. Further large-scale prospective studies are warranted to validate these findings and to develop predictive models for early treatment failure.
Conclusions
In this single-center retrospective study using a 12-week landmark approach, early PD during nivolumab plus ipilimumab was independently associated with poor OS in patients with advanced renal cell RCC. Furthermore, non-clear cell histology was significantly associated with early PD in exploratory multivariable analysis. These findings may help identify patients at risk of early treatment failure and support individualized first-line treatment selection through shared decision-making.
Abbreviations
RCC, renal cell carcinoma; BMI, body mass index; CI, confidence interval; CRP, C-reactive protein; ECOG, Eastern Cooperative Oncology Group; ECOG PS, Eastern Cooperative Oncology Group performance status; HR, hazard ratio; ICI, immune checkpoint inhibitor; IMDC, International Metastatic Renal Cell Carcinoma Database Consortium; IO, immuno-oncology; IQR, interquartile range; NLR, neutrophil-to-lymphocyte ratio; OR, odds ratio; OS, overall survival; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; TKI, tyrosine kinase inhibitor.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the National Hospital Organization Kyushu Cancer Center (approval number: 2014-99). The requirement for written informed consent was waived because of the retrospective nature of the study; however, an opt-out option was provided via the websites of Kyushu Cancer Center. Patient confidentiality was strictly maintained throughout the study. All data were de-identified prior to analysis and were handled in accordance with institutional policies. This study was conducted in compliance with the principles of the Declaration of Helsinki.
Acknowledgments
The authors thank Kelly Zammit, BVSc, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare that they have no conflicts of interest for this study.
References
1. Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–11. doi:10.1056/NEJMoa1712126
2. Tannir NM, Albigès L, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 8-year follow-up results of efficacy and safety from the phase III CheckMate 214 trial. Ann Oncol. 2024;35(11):1026–1038. doi:10.1016/j.annonc.2024.07.727
3. Motzer R, Alekseev B, Rha S-Y, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384(14):1289–1300. doi:10.1056/NEJMoa2035716
4. Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829–841. doi:10.1056/NEJMoa2026982
5. Bex A, Abu Ghanem Y, Albiges L, et al. European association of urology guidelines on renal cell carcinoma: the 2025 update. Eur Urol. 2025;87(6):683–696. doi:10.1016/j.eururo.2025.02.020
6. Powles T, Albiges L, Bex A, et al. Renal cell carcinoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(8):692–706. doi:10.1016/j.annonc.2024.05.537
7. Motzer RJ, Jonasch E, Agarwal N, et al. NCCN guidelines® insights: kidney cancer, version 2.2024. J Natl Compr Canc Netw. 2024;22(1):4–16. doi:10.6004/jnccn.2024.0008
8. Sharma P, Hu-Lieskovan S, Wargo JA, et al. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. 2017;168(4):707–723. doi:10.1016/j.cell.2017.01.017
9. Champiat S, Dercle L, Ammari S, et al. Hyperprogressive disease is a new pattern of progression in cancer patients treated by Anti-PD-1/PD-L1. Clin Cancer Res. 2017;23(8):1920–1928. doi:10.1158/1078-0432.CCR-16-1741
10. Park HJ, Kim KW, Won SE, et al. Definition, incidence, and challenges for assessment of hyperprogressive disease during cancer treatment with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Network Open. 2021;4(3):e211136. doi:10.1001/jamanetworkopen.2021.1136
11. Tykodi SS, Gordan LN, Alter RS, et al. Safety and efficacy of nivolumab plus ipilimumab in patients with advanced non-clear cell renal cell carcinoma: results from the Phase 3b/4 CheckMate 920 trial. Journal for ImmunoTherapy of Cancer. 2022;10(2):e003844. doi:10.1136/jitc-2021-003844
12. McDermott DF, Lee J-L, Ziobro M, et al. Open-label, single-arm, phase ii study of pembrolizumab monotherapy as first-line therapy in patients with advanced non–clear cell renal cell carcinoma. Journal of Clinical Oncology. 2021;39(9):1029–1039. doi:10.1200/JCO.20.02365
13. Albiges L, Gurney H, Atduev V, et al. Pembrolizumab plus lenvatinib as first-line therapy for advanced non-clear-cell renal cell carcinoma (KEYNOTE-B61): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2023;24(8):881–891. doi:10.1016/S1470-2045(23)00276-0
14. Vera-Badillo FE, Templeton AJ, Duran I, et al. Systemic therapy for non-clear cell renal cell carcinomas: a systematic review and meta-analysis. Eur Urol. 2015;67(4):740–749. doi:10.1016/j.eururo.2014.05.010
15. Zhang T, Gong J, Maia MC, et al. Systemic therapy for non-clear cell renal cell carcinoma. Am Soc Clin Oncol Educ Book. 2017;37:337–342. doi:10.1200/EDBK_175572
16. Heng DYC, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009;27(34):5794–5799. doi:10.1200/JCO.2008.21.4809
17. Hahn AW, Alhalabi O, Msaouel P, et al. Validation of prognostic scoring systems for patients with metastatic renal cell carcinoma enrolled in Phase I clinical trials. ESMO Open. 2020;5(6):e001073. doi:10.1136/esmoopen-2020-001073
18. Ernst MS, Navani V, Wells JC, et al. Outcomes for international metastatic renal cell carcinoma database consortium prognostic groups in contemporary first-line combination therapies for metastatic renal cell carcinoma. Eur Urol. 2023;84(1):109–116. doi:10.1016/j.eururo.2023.01.001
19. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
20. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431. doi:10.1002/14651858.CD001431.pub5
21. Nishimoto K, Kimura G, Sazuka T, et al. The effectiveness and safety profile of nivolumab-plus-ipilimumab in previously untreated japanese patients with advanced or metastatic renal cell carcinoma: j-ENCORE study. Int J Urol. 2025;32(8):961–972. doi:10.1111/iju.70076
22. Hamamoto S, Nozawa M, Shirotake S, et al. A minimum 3-year follow-up of nivolumab-plus-ipilimumab in japanese patients with advanced or metastatic renal cell carcinoma: a final analysis of the J-ENCORE study. Int J Urol. 2026;33(3):e70400. doi:10.1111/iju.70400
23. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
24. Suissa S. Immortal time bias in pharmaco-epidemiology. Am J Epidemiol. 2008;167(4):492–499. doi:10.1093/aje/kwm324
25. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
26. Motzer RJ, Rini BI, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol. 2019;20(10):1370–1385. doi:10.1016/S1470-2045(19)30413-9
27. Seymour L, Bogaerts J, Perrone A, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18(3):e143–e152. doi:10.1016/S1470-2045(17)30074-8
28. Elias R, Kapur P, Pedrosa I, et al. Renal cell carcinoma pseudoprogression with clinical deterioration: to hospice and back. Clin Genitourin Cancer. 2018;16(6):485–488. doi:10.1016/j.clgc.2018.07.015
29. Ko JJ, Xie W, Kroeger N, et al. The international metastatic renal cell carcinoma database consortium model as a prognostic tool in patients with metastatic renal cell carcinoma previously treated with first-line targeted therapy: a population-based study. Lancet Oncol. 2015;16(3):293–300. doi:10.1016/S1470-2045(14)71222-7
30. Albiges L, Tannir NM, Burotto M, et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 4-year follow-up of the phase III CheckMate 214 trial. ESMO Open. 2020;5(6):e001079. doi:10.1136/esmoopen-2020-001079
31. Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1116–1127. doi:10.1056/NEJMoa1816714
32. Furubayashi N, Taguchi K, Negishi T, et al. Cytoreductive nephrectomy after combination of nivolumab plus ipilimumab for mucinous tubular and spindle cell carcinoma of the kidney with bone metastases: a case report. in vivo. 2022;36(1):510–521. doi:10.21873/invivo.12732
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.