Back to Journals » Drug Design, Development and Therapy » Volume 20
Early Detection and Temporal Progression of Hemidiaphragmatic Paralysis After Supraclavicular Brachial Plexus Block with 20 mL vs 30 mL Ropivacaine: A Randomized Controlled Trial
Authors Bao X, He Z, Ma Y, Xu S, Hu B ![]() , Ma Y, Fang Y, Zhu W, Kang X
, Ma Y, Fang Y, Zhu W, Kang X ![]()
Received 23 January 2026
Accepted for publication 5 June 2026
Published 15 July 2026 Volume 2026:20 598288
DOI https://doi.org/10.2147/DDDT.S598288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiuxia Bao,1,* Zonghong He,2,* Yun Ma,1 Shanshan Xu,1 Bingwei Hu,3 Yi Ma,1 Yan Fang,4 Weiliu Zhu,1 Xianhui Kang5
1Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Anesthesiology, Yinjiang Autonomous Country People’s Hospital, Yinjiang, Guizhou, People’s Republic of China; 3Department of Anesthesiology, Tongde Hospital of Zhejiang Province Afflicted to Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Anesthesiology, The 72nd Group Army Hospital of the People’s Liberation Army (PLA 98th Hospital), Huzhou, Zhejiang, People’s Republic of China; 5Department of Pain, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianhui Kang, Department of pain, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Objective: Hemidiaphragmatic paralysis (HDP) is a recognized complication of supraclavicular brachial plexus block (SCBPB). This study aimed to compare the incidence and temporal progression of HDP following ultrasound-guided SCBPB with 20 mL versus 30 mL of 0.375% ropivacaine.
Methods: Eighty-two patients undergoing removal of internal fixation devices in the upper extremities were randomly allocated to receive 20 mL (Group A) or 30 mL (Group B) of 0.375% ropivacaine for ultrasound-guided SCBPB. The diaphragmatic compound muscle action potential amplitude (Dia CMAP Amp) was measured before (T0) and 5 min (T1), 10 min (T2), 20 min (T3), and 30 min (T4) after SCBPB. The primary outcome was the incidence of HDP, defined as a ≥ 50% decrease in the Dia CMAP Amp from baseline. The secondary outcome was the Dia CMAP Amp at different times.
Results: The risk of HDP was significantly greater in Group B than in Group A (RR=1.972, P=0.011). There was a significant time effect on the incidence of HDP (Wald’s χ 2=15.547, P=0.001); HDP could occur within 5 minutes, and the incidence of HDP at T2, T3 and T4 was 1.222 (P=0.046), 1.889 (P< 0.001) and 1.944 P< 0.001) times greater than that at T1, respectively. The Dia CMAP Amp following SCBPB was significantly different between the ropivacaine groups (Wald’s χ 2=5.517, p=0.019).
Conclusion: HDP can be detected as early as 5 minutes after SCBPB, with incidence plateauing by 20 minutes while CMAP amplitude continues declining. Higher volume (30 mL) nearly doubles HDP risk (RR=1.972). Respiratory monitoring should begin within 5 minutes of block placement.
Keywords: SCBPB, HDP, Dia CMAP Amp, ropivacaine
Introduction
Brachial plexus block is a regional anesthesia technique that involves the injection of local anesthetics around the brachial plexus nerves to provide analgesia during and after upper limb surgery.1 Brachial plexus blocks are becoming increasingly widespread because of their high level of efficacy, safety, and efficiency in routine procedures.2,3 Phrenic nerve block is a frequent collateral effect of the supraclavicular brachial plexus block (SCBPB), with its incidence influenced by the needle insertion technique and the volume,concentration and type of local anesthetic administered.4 Phrenic nerve block is caused by the spread of local anesthetics into the interscalene groove to the epidural space, intervertebral foramen, around the phrenic nerve, and within the muscle.5,6 Approximately 95.7% of patients who undergo SCBPB experience local anesthetic spread into the interscalene groove because of the chimney effect.7 Hemidiaphragmatic paralysis (HDP) is defined as a 50% or greater decrease in the diaphragmatic compound muscle action potential amplitude (Dia CMAP Amp) relative to that at baseline. Some cases of post-SCBPB phrenic nerve block have led to respiratory distress, the need for assisted mechanical ventilation and even prolonged HDP as documented in case reports.8–10 Notably, patients with severe pulmonary disease may be unable to tolerate inadvertent unilateral diaphragmatic weakness,11,12 and even subclinical effects such as sleep-disordered breathing have been linked to unilateral paralysis.13 Therefore, monitoring to ascertain the risk of HDP after SCBPB is important. Several strategies have been proposed to reduce HDP following SCBPB, including lowering the volume of local anesthetic and employing alternative approaches such as the costoclavicular or retroclavicular block. However, our previous study assessed HDP incidence at a single post-block time point (typically 30 minutes), leaving the time course and early temporal progression of HDP following SCBPB poorly characterized. In most studies, HDP was determined by measuring changes in diaphragmatic excursion or thickness via M-mode ultrasonography.14,15 However, these studies revealed that determining HDP in this manner is difficult, particularly if the patient is obese or has undergone left-sided surgery.16 In our clinical practice, we utilize the Dia CMAP Amp, which is not influenced by such factors, to objectively assess HDP.17
In our previous study, we found that the volume of local anesthetics (20 mL vs. 30 mL) also had a significant effect on the onset time of brachial plexus motor nerve fiber block (10 min vs. 5.8 min, respectively, P < 0.05).17 The phrenic nerve is a motor nerve fiber, and the early temporal course of phrenic nerve block has not been investigated in detail. The objective of this study was to compare the effects of different volumes of 0.375% ropivacaine (ie., 20 mL vs. 30 mL) on the incidence of HDP paralysis and the Dia CMAP Amp at different times relative to the induction of SCBPB to explore the temporal patterns of phrenic nerve block and recommend specific monitoring periods for patients undergoing brachial plexus block. The primary outcome was the incidence of HDP, defined as a ≥ 50% decrease in the Dia CMAP Amp from baseline, at 5, 10, 20, and 30 min after SCBPB. These findings can optimize perioperative safety by enabling early detection of phrenic nerve block and timely intervention.
Methods
Study Participants
This study was approved by Medical Ethics Committee (the 72nd Group Army Hospital of the People’s Liberation Army; Ethics Review Number: Hospital (2024) No. 08; Chairperson: Feng Wu,) on 2 August 2024 and was prospectively registered in the Chinese Clinical Registry (ChiCTR2400091951) on November 6th, 2024. The first patient was enrolled on November 9th, 2024. Written informed consent was obtained from all patients prior to enrollment. This study was conducted in accordance with the Declaration of Helsinki. Patients who were scheduled for internal fixation device removal from one of the upper extremities below the shoulder between November 2024 and May 2025 were recruited. The inclusion criteria were as follows: American Society of Anesthesiologists (ASA) physical status I or II; age between 18 and 65 years;body mass index (BMI) between 18 and 28 kg/m2;18 and consent to participate in the study. The exclusion criteria were as follows: contraindications to regional anesthesia (including known allergies to local anesthetics; sensory or motor impairment; coagulation disorders and infection at the injection site); moderate to severe decline in preoperative pulmonary function; or atypical diaphragmatic CMAPs. The drop-out criteria were as follows: block failure; atypical diaphragmatic CMAPs; or a diaphragmatic CMAP amplitude greater than 2000 µV.
The patients were randomly allocated at a 1:1 ratio to Group A (20 mL of 0.375% ropivacaine for SCBPB) or Group B (30 mL of 0.375% ropivacaine) by one of the investigators via a computer generated table of random numbers. Randomization codes were sealed in opaque envelopes that were opened by the block operator (who was uninvolved in data collection) immediately before the procedure. The patients, investigators, and outcome assessors were blinded to group allocation. However, the allocation was communicated confidentially to the block operator prior to block administration.
Diaphragmatic CMAP Induced by Phrenic Nerve Stimulation
A sole technician conducted phrenic nerve conduction studies (PNCSs) via dedicated electromyography acquisition software (NeMus2+, Shenzhen Yingchi Technology Co., Ltd, Shenzhen, China) in accordance with protocols described in prior publications.19–21 The patient was placed in a supine position with the head slightly elevated and turned 30-degrees to the side opposite to the phrenic nerve to be stimulated. A bipolar surface stimulation electrode was positioned at the back edge of the right sternocleidomastoid muscle at the cricoid cartilage level. Two fine subcutaneous needles, which can be tolerated by almost all patients, were used to record the diaphragmatic CMAPs. The first needle was introduced into the diaphragm near the xiphoid process, 16 cm away from the second needle, situated at the corresponding costal margin. A ground electrode was placed between the stimulation and recording electrodes. The right or left phrenic nerve was stimulated at the end of exhalation, utilizing square-wave pulses lasting 0.2 milliseconds. The stimulus intensity was incrementally increased until a consistent response was achieved and the maximum Dia CMAP Amp was reached, defining the point of maximal stimulation. In addition, the phrenic nerve was subjected to supramaximal stimulation, in which the intensity was increased to 10–20% above the level required for maximal stimulation. The timing of the diaphragmatic CMAP, ie., the phrenic nerve conduction time (PNCT), was determined by measuring the interval in milliseconds from the delivery of the stimulus to the initiation of the CMAP. The magnitude of the diaphragm CMAP was quantified by recording the potential from its lowest point to its highest point on the waveform and is expressed in microvolts (µV). The Dia CMAP Amp was measured before the block and then 5, 10, 20, and 30 minutes after the block (Figure 1). The diaphragmatic CMAP amplitude and latency was measured in triplicate at each time point, and the average value was taken. Paralysis of the diaphragm was defined as a >50% reduction in the Dia CMAP Amp.
 |
Figure 1 Waveforms of the diaphragmatic CMAP from a representative patient prior to and 5 min, 10 min, 20 min, and 30 min after induction of SCBPB. Abbreviations: CMAP, Compound muscle action potential; SCBPB, supraclavicular brachial plexus block. |
Supraclavicular Brachial Plexus Block
All patients underwent preparation in the preoperative room prior to surgery. Before SCBPB was induced, an intravenous line was secured. While the patients were breathing normal air, their heart activity (electrocardiography, ECG), oxygen saturation level (SpO2), and blood pressure (measured noninvasively) were continuously monitored. The patients, the anesthesiologists responsible for preparing them in the preoperative area, and the researchers involved in data collection and analysis were all unaware of the group allocation.
All patients received 0.02 mg/kg intravenous midazolam to prevent anxiety. Patients were positioned flat on their backs with their heads turned toward the opposite side of the nerve block. The transducer (frequency 6 to 13 MHz) was closely applied to the supraclavicular fossa, and an ultrasound image of the supraclavicular brachial plexus nerve was obtained lateral to the subclavian artery and above the first rib. The transducer was kept perpendicular to the supraclavicular brachial plexus nerve to achieve optimal image quality. First, the skin and subcutaneous tissues were injected with a 2% lidocaine solution. Then, an in-plane approach was performed to administer 0.375% ropivacaine via a 50-mm, 22-gauge insulated needle. The injection was performed in two phases: first, half of the anesthetic volume was injected laterally in the medial direction, targeting the “corner pocket,” that is, the anatomical junction between the first rib and the subclavian artery.22 Second, the remaining the anesthetic was injected into the most superficial part of the lateral aspect of the brachial plexus, where the trunks and divisions form a cluster.23 The distribution of the anesthetic was closely observed via ultrasound to confirm its effectiveness.
Block Characteristics
After completion of the block, the respiratory parameters noted above, as well as the diaphragmatic CMAP, were evaluated again by the same investigators. Sensory and motor block efficacy was formally assessed 30 minutes post-block. Sensory function was evaluated via ice application to the ulnar (fifth finger), median (second finger palmar aspect), radial (dorsal first interosseous space), and musculocutaneous (lateral forearm) dermatomes using a 0–2 scale (0=normal, 1=reduced, 2=absent sensation). Motor function was tested against resistance for ulnar (finger abduction), median (second/third finger flexion), radial (wrist extension), and musculocutaneous (elbow flexion) nerves (0=normal strength, 1=paresis, 2=paralysis). Successful sensory and motor block required a score of 2 in all territories.23 After complete evaluation was achieved, the patients were transported to the operating room for surgery. If the patient experienced pain, supplementary blocks were administered. If the patient could still not tolerate the procedure after the administration of supplementary blocks, general anesthesia was initiated. Block success was defined as the absence of any supplementary blocks, conversion to general anesthesia, or the administration of opioids to complete the operation. A supplementary block was defined as any block that the surgeon applied at the elbow or wrist or locally administered when part of the nerve area was not fully anesthetized. Block failure was defined as the need for additional opioids for analgesia, supplemental block or conversion to general anesthesia to complete the procedure.24 The patients were monitored to detect any adverse reactions after the block was complete and then followed for 24 hours after local anesthesia induction.
Management of Respiratory Compromise
A predefined stepwise protocol was in place for phrenic nerve paralysis-related respiratory compromise: (1) supplemental oxygen via face mask if SpO2 decreased > 5% from baseline or dyspnea occurred; (2) high-flow nasal cannula therapy if SpO2 remained below 92%; and (3) assisted ventilation if symptoms were refractory.
Sample Size Calculation
The sample size was calculated on the basis of an incidence of HDP of 41% in the 20-mL 0.375% ropivacaine group and of 68% in the 30-mL 0.375% ropivacaine group based on the results of our previous study.17 For this study, we assumed the same level of power (ie., 0.8) and an alpha error of 0.05. The measurement time proportions were 0.167, 0.333, 0.667, and 1.0. Through PASS, we determined that the required sample size was 69 patients. Considering a possible loss to follow-up rate of 15%, 82 patients were ultimately included in this study.
Outcomes
The primary outcome was the incidence of HDP in the two groups, measured at 5 min, 10 min, 20 min and 30 min after the block and expressed as the percentage change in the amplitude from baseline. To improve clinical interpretability, the presence of a phrenic block was defined as a greater than 50% decrease in the Dia CMAP Amp from baseline. The secondary outcome was the Dia CMAP Amp at different time points following SCBPB in each group.
Statistical Analysis
Statistical analyses were performed via IBM SPSS Statistics, V.22 (IBM, Armonk, New York, USA). Data are presented as the means ± standard deviations (SDs) or medians with interquartile ranges (IQRs) according to the normality of the variable distribution as determined with the Shapiro‒Wilk test, and categorical variables are presented as counts and percentages. Repeated measures data were analyzed via generalized estimating equations, and a Poisson log-linear model was employed to compare the incidence of HDP among the groups. A linear model was used to examine differences in Dia CMAP Amp. A P value <0.05 indicated statistical significance.
Results
A total of 82 patients were recruited for this study. Two patients each did not meet the inclusion criteria and opted to receive general anesthesia rather than being included in the study. A total of 78 patients were randomly allocated to the study groups, and the data from 70 patients were ultimately included in the analysis (8 patients excluded post-randomization: 4 in each group) (Figure 2). One patient in each group was hypersensitive to the electrical stimulation, as evidenced by the Dia CMAP Amp surpassing 2000 µV, indicating an abnormality. One patient in Group A and two patients in Group B exhibited markedly abnormal amplitudes and latencies of the diaphragm CMAP, which could be attributed to interference from brachial plexus stimulation. Furthermore, at 30 minutes after block administration, two patients in Group A were observed to have failed to achieve successful sensory and motor blockade. Intraoperatively, one of these patients received a supplemental block, while the other required conversion to general anesthesia. In Group B, one patient failed to achieve successful sensory and motor blockade and received a supplemental block during surgery. Thus, block failure occurred in two patients in Group A and one patient in Group B. There were no significant differences in BMI, age, or sex between the two groups (Table 1). A comparison of the characteristics of the diaphragmatic CMAPs at different times relative to SCBPB in the two groups is presented in Table 2.
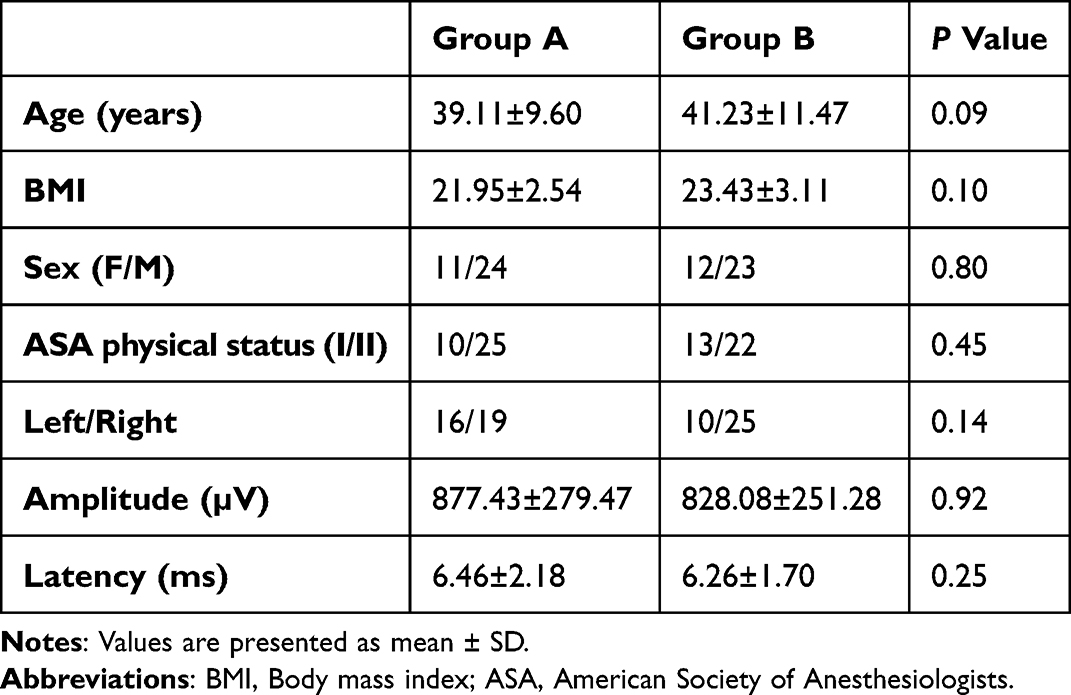 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Participants |
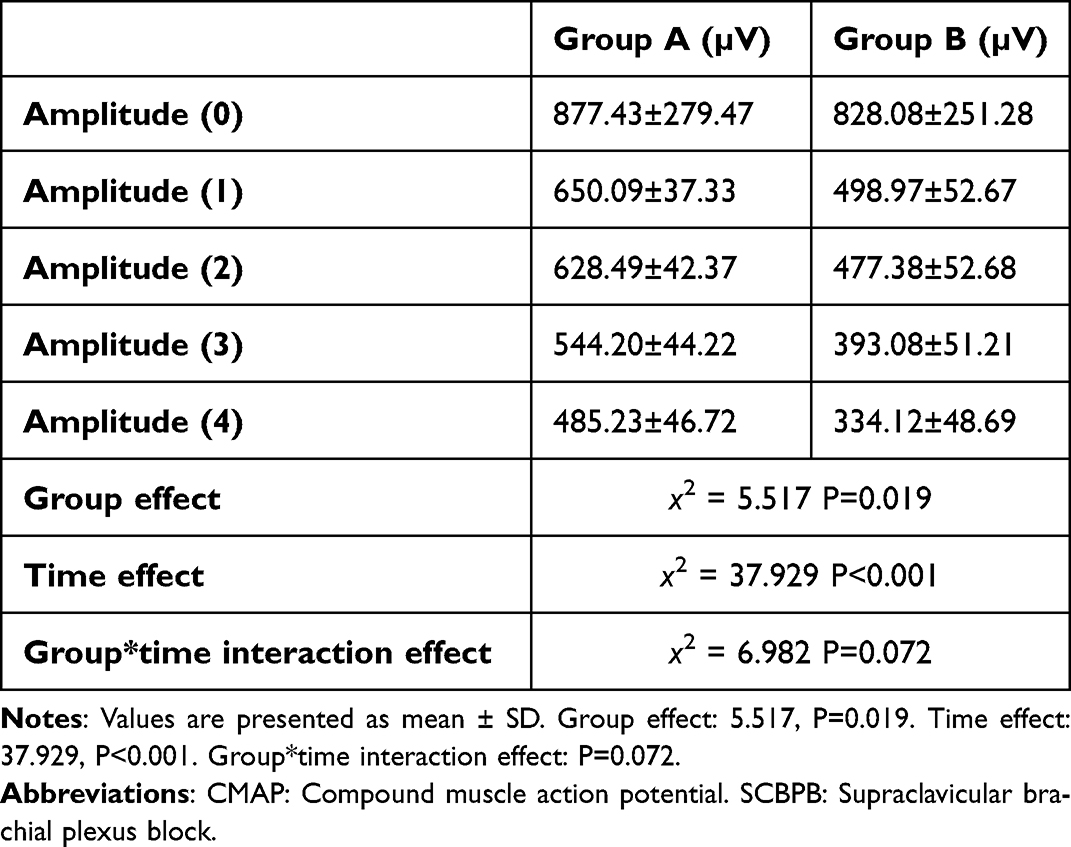 |
Table 2 Comparison of the Amplitude of the Diaphragm CMAP Between the Two Groups Before and at Different Time Points After SCBPB |
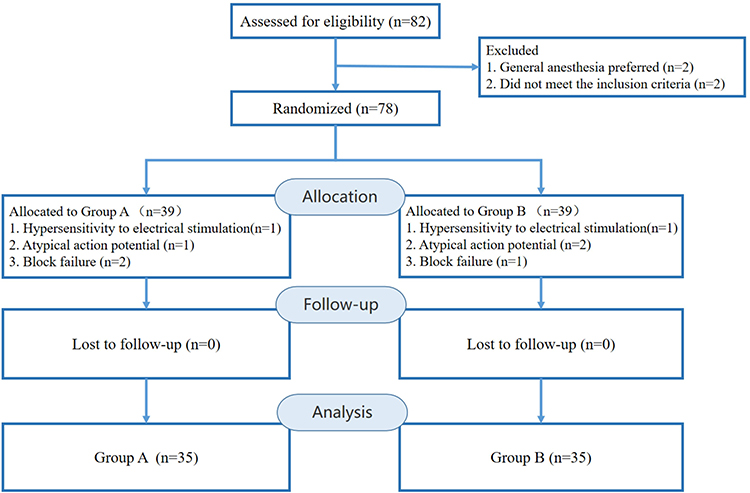 |
Figure 2 Consolidated Standards of Reporting Trials (CONSORT) flow diagram. |
Incidence of Diaphragmatic Paralysis
The incidence of HDP at different times after SCBPB in the two groups is presented in Figure 3. After adjusting for the influence of time, the effect of group on the incidence of HDP was found to be statistically significant (Wald’s χ2=5.179, P=0.023). Specifically, the risk of HDP was 1.972 times greater with the use of 30 mL ropivacaine than with the use of 20 mL ropivacaine for inducing SCBPB (RR=1.972, P=0.011). Moreover, the incidence of HDP at T4 was 12/35 (34.3%) in Group A and 23/35 (65.7%) in Group B. After adjusting for the influence of group, the effect of time on the incidence of HDP was statistically significant (Wald’s χ2=15.547, P=0.001). Specifically, relative to the incidence at T1, the incidence of HDP at T2, T3 and T4 was 1.222 (RR=1.222, P=0.046), 1.889 (RR=1.889, P<0.001) and 1.944 (RR=1.944, P<0.001) times greater, respectively. There was no significant interaction effect between time and group (Wald’s χ2=2.979, P=0.395). In pairwise comparisons, Bonferroni correction was applied at the significance level. There was a significant difference in the incidence of HDP between T2 and T3 (95% CI, 0.05 to 0.28; adjusted P = 0.001).
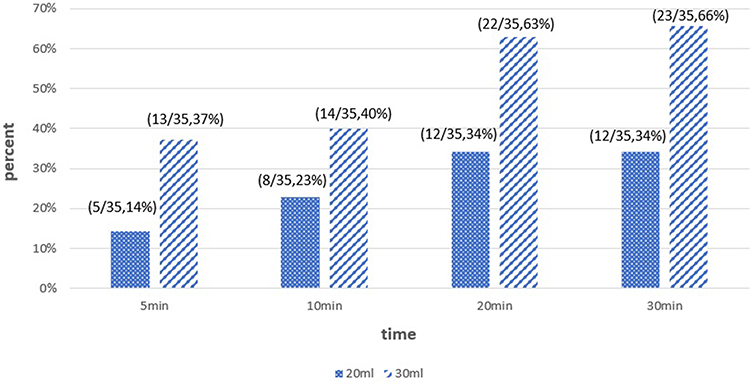 |
Figure 3 Incidence of phrenic block after SCBPB in the two groups. Phrenic block was defined as a more than 50% decrease in the amplitude of the diaphragmatic CMAP from baseline. A greater incidence of phrenic block was observed among subjects receiving 30 mL of ropivacaine than among those receiving 20 mL of ropivacaine across all times (P=0.02). Abbreviations: SCBPB, supraclavicular brachial plexus block; CMAPs, compound muscle action potentials. |
Amplitude of the Diaphragmatic CMAP
The mean Dia CMAP amplitude decreased over the 30 min following SCBPB (Figure 4). PNCT was not a predefined outcome and is presented descriptively in Figure 5. After adjusting for the effect of time, the effect of group (volume of ropivacaine) on the Dia CMAP Amp after anesthesia was statistically significant (Wald’s χ2=5.517, p=0.019). Moreover, the Dia CMAP Amp in Groups A and B at T4 were 485.23±46.72 µV and 334.12±48.69 µV, respectively. After adjusting for the effect of group, the effect of time on the Dia CMAP Amp was statistically significant (Wald’s χ2=37.929, p<0.001). Compared with those at T1, the mean Dia CMAP Amps at T2, T3, and T4 were 21.593 (P=0.104; 95% CI, −47.596 to 4.409), 105.890 (P<0.001, 95% CI, −150.852 to −60.928), and 164.852 (P<0.001, 95% CI, −223.642 to −106.062) lower, respectively. Finally, the interaction between time and group was not statistically significant (Wald’s χ2=6.982, p=0.072). In pairwise comparisons, Bonferroni correction was applied at the significance level. The mean Dia CMAP Amp at T3 was 84.296 (adjusted P<0.001, 95% CI, −127.633 to −40.960) lower than that at T2 and 58.962 (adjusted P<0.001, 95% CI, 26.558 to 91.367) greater than that at T4; these differences were statistically significant.
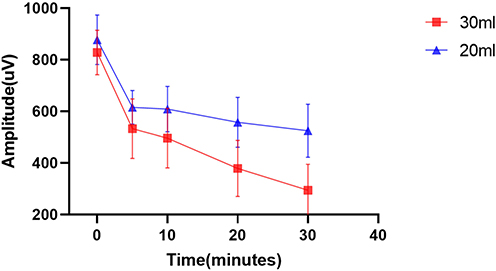 |
Figure 4 Amplitudes of diaphragmatic CMAPs at baseline (T0), 5 minutes (T1), 10 minutes (T2), 20 minutes (T3), and 30 minutes (T4) after SCBPB in the two groups. The diaphragmatic CMAP amplitude was significantly lower in the 30 mL group than in the 20 mL group (P = 0.019). Abbreviations: CMAP, compound muscle action potential; SCBPB, supraclavicular brachial plexus block. |
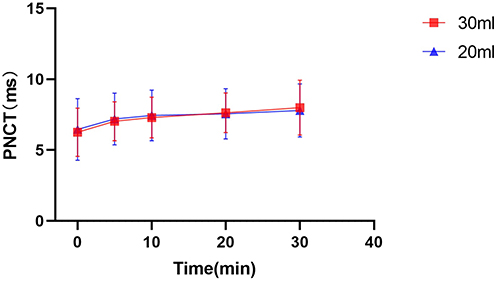 |
Figure 5 Latencies of diaphragmatic CMAPs (phrenic nerve conduction time) at baseline (T0), 5 minutes (T1), 10 minutes (T2), 20 minutes (T3), and 30 minutes (T4) after SCBPB in the two groups. Abbreviations: CMAP, compound muscle action potential; SCBPB, supraclavicular brachial plexus block; PNCT, phrenic nerve conduction time. |
Adverse Events
The complications of the procedure included local anesthetic toxicity, failure to achieve motor and sensory function normalization, a decrease in SpO2, dyspnea, and hoarseness. Oxygen desaturation was defined as an objective decrease in SpO2 >5% from baseline while breathing room air. Dyspnea was defined as the patient’s subjective report of breathlessness or difficulty in breathing when asked to take a deep breath after SCBPB, documented as present or absent by the investigator.25 Four patients in Group A and six patients in Group B developed transient dyspnea, whereas one patient in Group B exhibited oxygen desaturation. For patients with decreased oxygen saturation, the oxygen saturation improved significantly after we administered oxygen via a face mask. There was no statistically significant difference in the incidence of dyspnea or oxygen desaturation between the two groups (P=0.5, P=0.3).
Discussion
In this study, we compared the effects of two volumes of ropivacaine on the incidence of HDP and the Dia CMAP Amps at different times relative to the induction of SCBPB. Ropivacaine with a concentration of 0.375% is commonly used in our clinical practice, as sensory blockade is optimized, and while motor blockade is minimized at this concentration.26 Our previous research17 revealed that the mean onset time for sensory blockade following the induction of SCBPB with different volumes of anesthetic is 5–6 minutes (P>0.05). However, the onset time of motor block in the 30 mL group (5.8±3.8) was significantly shorter than that in the 20 mL group (10.0±3.0) (P<0.05). However, whether differences in the onset time would be observed for phrenic nerve blockade with different volumes of anesthetic for SCBPB induction is unknown. Therefore, in this study, we compared the effects of different volumes of ropivacaine on the incidence of HDP and the Dia CMAP Amp at 5, 10, 20, and 30 min after the block was performed. In this way, we were able to test whether the temporal progression of phrenic nerve block following SCBPB induced with different volumes of anesthetic is consistent. The absence of an interaction effect in the statistical analysis suggests that this hypothesis was confirmed. High-volume (30 mL) local anesthetics were more likely to cause phrenic nerve block and this phenomenon occurs because the “chimney effect” leads to local anesthetic spread into the interscalene groove in approximately 95.7% of patients during SCBPB.7 MRI studies have confirmed that larger volumes of local anesthetic significantly increase cephalad spread to the C4-C6 levels.6 In our study, with concentration held constant (0.375% ropivacaine), reducing the volume from 30 mL to 20 mL decreased HDP incidence from 65.7% to 34.3%, demonstrating a clear volume-dependent effect on phrenic nerve involvement during SCBPB. This is broadly consistent with prior literature; Georgiadis et al11 reported a 70% HDP rate with 25 mL of 0.5% ropivacaine, confirming the high incidence of HDP associated with larger-volume supraclavicular blocks.
We selected the diaphragmatic CMAP as an indicator of HDP because it is less affected by subjective factors and the influence of intercostal and accessory respiratory muscles than the commonly used ultrasound measurements of diaphragmatic excursion and thickness. In such assessments, the participants are instructed to breathe normally and perform a “sniff test” as directed; however, visualization of left hemidiaphragm motion can be challenging, especially in patients with a high BMI, owing to the small size of the splenic window when HDP is diagnosed by ultrasound.24,26 Many studies recruited only patients who underwent right-sided BPB, as M-mode ultrasound of the right hemidiaphragm through the liver acoustic window is easier to perform than that of the left hemidiaphragm through the spleen acoustic window. Thus, it is unclear if the results obtained on the right side apply to the left side. However, this concern was not present in our study involving the diagnosis of HDP via the diaphragmatic CMAP, as we included patients with both right and left brachial plexus blocks. Local anesthetics cause conduction block in an all-or-nothing fashion, primarily affecting CMAP amplitude rather than latency. PNCT was therefore not included as a predefined outcome, and Figure 5 is provided for descriptive purposes only.
The present study addresses several limitations of our previous work17 in important ways. That study demonstrated that reducing the ropivacaine volume from 30 mL to 20 mL decreased HDP incidence, but relied on a single assessment at 30 minutes and could not determine how early phrenic nerve block becomes detectable or how it progresses over time. By employing serial diaphragmatic CMAP measurements at four time points (5, 10, 20, and 30 minutes), the current study reveals three new findings: (a) HDP can be detected as early as 5 minutes after SCBPB; (b) HDP incidence stabilizes by 20 minutes (RR at T3 vs. T4: 1.889 vs. 1.944, P > 0.05), whereas Dia CMAP amplitude continues to decline significantly through 30 minutes (difference: 58.96 µV, adjusted P < 0.001), indicating a dissociation between incidence and severity; and (c) these temporal data support a specific monitoring recommendation — surveillance should begin immediately and continue for at least 20 minutes post-block. Additionally, the current study employed standardized phrenic nerve conduction methodology with repeated measurements, providing more robust electrophysiological characterization than the single-point assessment in the 2019 study. These temporal findings are consistent with Georgiadis et al,11 who reported no significant time effect between 15 and 30 minutes, suggesting HDP was largely established by 15 minutes; however, their two-timepoint design precluded identification of how early HDP can be detected, a gap addressed by our serial measurements beginning at 5 minutes.
In our study, ten patients experienced transient dyspnea, and only one experienced a decrease in oxygen saturation.Although only 14.3% of patients with HDP reported dyspnea, all symptomatic cases occurred in patients with a confirmed Dia CMAP reduction ≥ 50%. Notably, 71.4% of the patients with HDP remained asymptomatic, likely due to compensatory respiratory mechanisms. This discordance underscores that subjective symptoms alone are insufficient to exclude HDP, particularly in healthy individuals. Objective assessment (eg., Dia CMAP or diaphragmatic ultrasound) remains critical for early detection, especially in high-risk populations where silent HDP could precipitate respiratory failure. The low incidence of clinically significant respiratory symptoms despite electrophysiologically confirmed HDP is consistent with findings across different brachial plexus block approaches. Georgiadis et al11 reported no dyspnea despite a 70% HDP incidence following supraclavicular block in patients without pulmonary disease. Similarly, Jo et al14 observed no serious respiratory complications (no dyspnea, desaturation, or pneumothorax) in patients receiving costoclavicular block, even when partial or complete HDP was present. In a more recent study by Robles et al, there was no notable decrease in oxygen saturation among patients exhibiting diaphragmatic dysfunction following superior trunk block; however, 38.9% of these patients experienced dyspnea, and 83.3% experienced reduced breath sounds during auscultation.25 The incidence of dyspnea was greater in Robles’s study than in our study, likely because in our study, patients with obesity or moderate-to-severe pulmonary function decline were excluded. However, the absence of oxygen desaturation in the patients may be attributed to the compensatory increase in the function of the contralateral hemidiaphragm following paralysis of the ipsilateral hemidiaphragm, allowing maintenance of normal oxygen saturation levels. In addition, not all patients show compensatory increases in the function of the contralateral hemidiaphragm when the ipsilateral hemidiaphragm is paralyzed.27 Patients with respiratory system diseases may experience either no or an insufficient increase in the function of the contralateral diaphragm to maintain normal oxygenation. Although HDP might be of little consequence in healthy subjects, it could be deleterious in patients with preexisting diminished pulmonary function. Patients with pulmonary disease are at high risk for postoperative hypoxemia, pneumonia, and respiratory failure.
These findings underscore the critical need for the vigilant monitoring of respiratory symptoms that begin within the first 5 minutes after the block is performed, given that HDP can be detected as early as 5 minutes post-block. Immediate detection of such changes allows for timely intervention, such as oxygen therapy, to alleviate hypoxemia. High-flow nasal cannula (HFNC) oxygenation is particularly effective in maintaining adequate oxygenation levels in patients experiencing respiratory distress.28 As discussed above, HDP incidence stabilized by 20 minutes while Dia CMAP amplitude continued to decline, suggesting that local anesthetics deepen conduction block in already-affected fibers without causing new-onset HDP. This reinforces the need for a monitoring window that begins within 5 minutes and extends for at least 20 minutes post-block. The “saline flush” technique, which involves injecting 20 or 30 mL of normal saline into the interscalene space, has been shown to improve respiratory mechanics, alleviate hypoxia and prevent the need for intubation, even though pain scores remained unaffected.29–31 This technique could be particularly beneficial for patients who do not respond to initial oxygen therapy, especially within the first 20 minutes after SCBPB. By integrating these findings into clinical practice, we can enhance patient safety and reduce the risk of adverse events associated with phrenic nerve block.
This study has several limitations that should be considered. First, this study enrolled relatively healthy patients without any known comorbidities; patients with obesity or severe pulmonary diseases were not included. However, based on the results of this study, we can recommend a specific period of close observation for patients undergoing SCBPB. Simultaneously, we recommend replicating this study in these populations to obtain more generalized conclusions. Second, although there was no significant change in the number of patients who developed HDP between 20 and 30 minutes postoperatively, the Dia CMAP Amp still decreased; that said, we did not observe changes in the Dia CMAP Amp 30 minutes after SCBPB induction. For patients with HDP, we did not note the point at which diaphragmatic function began to recover. Additional research should be conducted to answer these questions. Third, the block operator was unblinded to accommodate volume-specific injection protocols. While this may introduce technical variability, standardized ultrasound-guided protocols with real-time monitoring of anesthetic spread and blinded objective assessments mitigated potential bias. Fourth, the primary endpoint — a ≥50% reduction in Dia CMAP Amp — is a surrogate electrophysiological marker rather than a direct measure of respiratory dysfunction. Although chosen for its objectivity and sensitivity in early detection, future studies should incorporate clinical endpoints such as forced vital capacity and arterial blood gas analysis to better establish the clinical significance of HDP. Fifth, the exclusion of 8 patients after randomization resulted in a per-protocol analysis, which may introduce potential bias. However, all exclusions were based on pre-specified objective technical criteria, and the number of excluded patients was balanced between the two groups (4 per group).
Conclusion
A higher volume (30 mL) of ropivacaine increases the incidence of HDP and is associated with a greater reduction in Dia CMAP Amp following SCBPB in relatively healthy adults (ASA I–II) undergoing upper-extremity internal fixation removal. HDP can be detected as early as 5 minutes post-block, with the incidence plateauing by 20 minutes, while the Dia CMAP Amp continues to decrease within 30 minutes of SCBPB. Early detection and timely intervention are crucial to enhance perioperative safety in patients undergoing SCBPB.
Data Sharing Statement
The individual deidentified participant data that underlie the results reported in this article (including text, tables, and figures) will be made available to researchers who provide a methodologically sound proposal. Requests should be directed to the corresponding author ([email protected]). Data will be available beginning 3 months and ending 5 years following article publication. Proposals may be submitted for any purpose of analysis. The study protocol and statistical analysis plan will also be made available upon request.
Author Contributions
Xiuxia Bao and Zonghong He should be considered co-first authors. This study was designed by BXX, HZH, MY, and KXH. The data were collected by FY, AXF, MY, and ZWL. The data were statistically analyzed by HBW and KXH. The manuscript was prepared by BXX, KXH, WM, FY, and AXF, and was revised by all authors. All authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work. This manuscript was handled by Xiuxia Bao. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Zhejiang Provincial Natural Science Foundation of China under Grant No. LZ24H090002. The funder had no role in the study design, data collection, analysis, interpretation of results, or writing of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. CW Chan, JSH Wong, F Wang, et al. Addition of Liposomal Bupivacaine to Standard Bupivacaine versus Standard Bupivacaine Alone in the Supraclavicular Brachial Plexus Block: a Randomized Controlled Trial. Anesthesiology. 2024;141:732.
2. Feigl GC, Litz RJ, Marhofer P. Anatomy of the brachial plexus and its implications for daily clinical practice: regional anesthesia is applied anatomy. Reg Anesth Pain Med. 2020;45(8):620–12. doi:10.1136/rapm-2020-101435
3. Jones MR, Novitch MB, Sen S, et al. Upper extremity regional anesthesia techniques: a comprehensive review for clinical anesthesiologists. Best Pract Res Clin Anaesth. 2020;34(1):e13–e29. doi:10.1016/j.bpa.2019.07.005
4. Luo Q, Yao W. Modified first-targeted ultrasound window for selective brachial plexus trunk block may reduce the incidence of hemi-diaphragmatic paralysis. Eur J Anaesthesiol. 2023;40(6):450–451. doi:10.1097/EJA.0000000000001825
5. Golarz SR, White JM. Anatomic Variation of the Phrenic Nerve and Brachial Plexus Encountered during 100 Supraclavicular Decompressions for Neurogenic Thoracic Outlet Syndrome with Associated Postoperative Neurologic Complications. Ann Vasc Surg. 2020;62:70–75. doi:10.1016/j.avsg.2019.04.010
6. Stundner O, Meissnitzer M, Brummett CM, et al. Comparison of tissue distribution, phrenic nerve involvement, and epidural spread in standard- vs low-volume ultrasound-guided interscalene plexus block using contrast magnetic resonance imaging: a randomized, controlled trial † †Preliminary results of this study were presented as an abstract during the annual conference of the American Society of Regional Anesthesia (ASRA) in Las Vegas, NV, USA on May 15–16, 2015. Br J Anaesth. 2016;116:405–412. doi:10.1093/bja/aev550
7. Guo CW, Ma JX, Ma XL, et al. Supraclavicular block versus interscalene brachial plexus block for shoulder surgery: a meta-analysis of clinical control trials. Int J Surg. 2017;45:85–91. doi:10.1016/j.ijsu.2017.07.098
8. Song JG, Kim SK, Jeon DG, Kwon MA, Yoo JH. Dyspnea after supraclavicular brachial plexus block in a morbidly obese patient due to phrenic nerve block: a case report. Korean J Anesthesiol. 2009;57(4):511–514. doi:10.4097/kjae.2009.57.4.511
9. Jennes E, Vriens PWHE, Heyligers JMM. Acute dyspnoea during brachial plexus blockade. Ned Tijdschr Geneeskd. 2017;161:D1216.
10. Sm L, Jw W, L Y. Prolonged diaphragm paralysis following interscalene brachial-plexus block for clavicle fracture surgery: a case report. Asian J Surg. 2024;47:4461–4462.
11. Georgiadis PL, Vlassakov KV, Patton ME, et al. Ultrasound-guided supraclavicular vs. retroclavicular block of the brachial plexus: comparison of ipsilateral diaphragmatic function: a randomised clinical trial. Eur J Anaesthesiol. 2021;38(1):64–72. doi:10.1097/EJA.0000000000001305
12. Kim Y, Yoo S, Kim SH, et al. Comparison between low-volume local anesthetic with intravenous dexamethasone and conventional volume without dexamethasone for superior trunk block after arthroscopic shoulder surgery: a randomized controlled non-inferiority trial. Reg Anesth Pain Med. 2024;49(8):558–564. doi:10.1136/rapm-2023-104520
13. S M, Jm M, A D, et al. The impact of unilateral diaphragmatic paralysis on sleep-disordered breathing: a scoping review. Can J Anaesth. 2021;68:1064–1076.
14. Jo Y, Oh C, Lee W-Y, et al. Effect of local anesthetic volume (20 vs. 40 mL) on the analgesic efficacy of costoclavicular block in arthroscopic shoulder surgery: a randomized controlled trial. Korean J Anesthesiol. 2023;77:85–94.
15. Aa B, Jm F, Jm H, et al. Evaluation of Diaphragmatic Function after Interscalene Block with Liposomal Bupivacaine: a Randomized Controlled Trial. Anesthesiology. 2022;136:531–541.
16. J Y, O C, Wy L, et al. Diaphragm-sparing efficacy of subparaneural upper trunk block for arthroscopic shoulder surgery: a randomised controlled trial. Eur J Anaesthesiol. 2024;41:760–768.
17. Bao X, Huang J, Feng H, et al. Effect of local anesthetic volume (20 mL vs 30 mL ropivacaine) on electromyography of the diaphragm and pulmonary function after ultrasound-guided supraclavicular brachial plexus block: a randomized controlled trial. Reg Anesth Pain Med. 2019;44(1):69–75. doi:10.1136/rapm-2018-000014
18. Zhuo Q, Zheng Y, Hu Z, et al. Ultrasound-Guided Clavipectoral Fascial Plane Block With Intermediate Cervical Plexus Block for Midshaft Clavicular Surgery: a Prospective Randomized Controlled Trial. Anesthesia Analg. 2022;135(3):633–640. doi:10.1213/ANE.0000000000005911
19. El-Tantawi GAY, Imam MH, Morsi TS. Phrenic Nerve Conduction Abnormalities Correlate with Diaphragmatic Descent in Chronic Obstructive Pulmonary Disease. COPD. 2015;12(5):516–524. doi:10.3109/15412555.2014.993465
20. Podnar S, Harlander M. Phrenic nerve conduction studies in patients with chronic obstructive pulmonary disease. Muscle Nerve. 2013;47(4):504–509. doi:10.1002/mus.23617
21. de Carvalho M, Pinto S, Swash M. Diaphragm motor responses to phrenic nerve stimulation in ALS: surface and needle recordings. Clin Neurophysiol. 2018;129(2):349–353. doi:10.1016/j.clinph.2017.11.019
22. Kang RA, Chung YH, Ko JS, Yang MK, Choi DH. Reduced Hemidiaphragmatic Paresis With a “Corner Pocket” Technique for Supraclavicular Brachial Plexus Block: single-Center, Observer-Blinded, Randomized Controlled Trial. Reg Anesth Pain Med. 2018;1:1.
23. Roy M, Nadeau M-J, Côté D, et al. Comparison of a single- or double-injection technique for ultrasound-guided supraclavicular block: a prospective, randomized, blinded controlled study. Reg Anesth Pain Med. 2012;37(1):55–59. doi:10.1097/AAP.0b013e3182367b97
24. Park S-K, Lee S-Y, Kim WH, Park H-S, Lim Y-J, Bahk J-H. Comparison of Supraclavicular and Infraclavicular Brachial Plexus Block: a Systemic Review of Randomized Controlled Trials. Anesth Analg. 2017;124:636–644.
25. Robles C, Berardone N, Orebaugh S. Effect of superior trunk block on diaphragm function and respiratory parameters after shoulder surgery. Reg Anesth Pain Med. 2022;47(3):167–170. doi:10.1136/rapm-2021-102962
26. Ferré F, Pommier M, Laumonerie P, et al. Hemidiaphragmatic paralysis following ultrasound-guided anterior vs. posterior suprascapular nerve block: a double-blind, randomised control trial. Anaesthesia. 2020;75(4):499–508. doi:10.1111/anae.14978
27. Rovira L, Kot P, Pozo S, Cano B, De Andrés J. Peri-operative Hemi-diaphragmatic Variations After Brachial Plexus Block Above the Clavicle: a Prospective Observational Study of the Contralateral Side. Ultrasound Med Biol. 2023;49(9):2113–2118. doi:10.1016/j.ultrasmedbio.2023.05.018
28. Rochwerg B, Einav S, Chaudhuri D, et al. The role for high flow nasal cannula as a respiratory support strategy in adults: a clinical practice guideline. Intensive Care Med. 2020;46:2226–2237.
29. Tsui BCH, Price D. Washing off local anaesthetic induced phrenic dysfunction following interscalene block. J Clin Anesth. 2018;49:38–39.
30. Tsui BCH, Dillane D. Reducing and washing off local anesthetic for continuous interscalene block. Reg Anesth Pain Med. 2014;39(2):175–176. doi:10.1097/AAP.0000000000000047
31. Ngai LK, Ma W, Costouros JG, Cheung EV, Horn J-L, Tsui BCH. Successful reversal of phrenic nerve blockade following washout of interscalene nerve block as demonstrated by ultrasonographic diaphragmatic excursion. J Clin Anesth. 2020;59:46–48. doi:10.1016/j.jclinane.2019.06.022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.