Back to Journals » International Journal of Women's Health » Volume 18
Early Catheter Removal Improves Recovery After Total Abdominal Hysterectomy: A Randomized Trial
Authors Karasaard K ![]() , Temtanakitpaisan A, Temtanakitpaisan T
, Temtanakitpaisan A, Temtanakitpaisan T ![]() , Chumworathayi B
, Chumworathayi B ![]() , Luanratanakorn S, Kietpeerakool C
, Luanratanakorn S, Kietpeerakool C ![]() , Aue-aungkul A
, Aue-aungkul A ![]() , Likitdee N
, Likitdee N ![]() , Itarat Y
, Itarat Y ![]()
Received 7 December 2025
Accepted for publication 20 February 2026
Published 26 February 2026 Volume 2026:18 587143
DOI https://doi.org/10.2147/IJWH.S587143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Kanyanat Karasaard, Amornrat Temtanakitpaisan, Teerayut Temtanakitpaisan, Bandit Chumworathayi, Sanguanchoke Luanratanakorn, Chumnan Kietpeerakool, Apiwat Aue-aungkul, Naratassapol Likitdee, Yuwadee Itarat
Department of Obstetrics and Gynaecology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Amornrat Temtanakitpaisan, Department of Obstetrics and Gynaecology, Faculty of Medicine, Khon Kaen University, 123 Mittraphap Highway, Muang Khon Kaen, Khon Kaen, 40002, Thailand, Tel +6643363030, Fax +6643348395, Email [email protected]
Objective: To evaluate whether early removal of the urinary indwelling catheter enhances postoperative recovery in women undergoing uncomplicated total abdominal hysterectomy (TAH).
Methods: This open-label randomized controlled trial was conducted at a university hospital in Thailand between August 2023 and July 2024. Women aged 18– 65 years scheduled for TAH for benign gynecologic conditions were randomized to early catheter removal (12– 16 hours postoperatively) or standard removal (20– 24 hours). Primary outcomes were time to first ambulation and six-minute walk test (6MWT) distance on postoperative days (POD) 1 and 2. Secondary outcomes included time to first voiding, urinary retention, urinary tract infection (UTI), catheter-related discomfort, hospital stay, costs, and patient satisfaction.
Results: Of 105 patients screened, 100 were randomized; 93 completed the study (46 early removal, 47 standard removal). Baseline characteristics were comparable. Early catheter removal significantly reduced time to ambulation (18.69 ± 4.11 vs 21.41 ± 3.02 hours, p < 0.001) and time to first voiding (19.02 ± 3.72 vs 21.99 ± 3.46 hours, p < 0.001). 6MWT distances on POD1 and POD2 were slightly higher in the early group but not statistically different. Rates of urinary retention, symptomatic UTI, catheter-related discomfort, hospital stay, hospitalization costs, and patient satisfaction were similar across groups.
Conclusion: Early urinary catheter removal within 12– 16 hours after uncomplicated TAH accelerates postoperative recovery, particularly ambulation and voiding, without increasing urinary complications, supporting its integration into ERAS protocols.
Keywords: catheter removal, hysterectomy, recovery
Introduction
Enhanced Recovery After Surgery (ERAS) protocols are increasingly applied across surgical fields to enhance postoperative outcomes by reducing complications and expediting recovery.1 Early ambulation is a core element of ERAS, as it helps lower the risk of respiratory complications, insulin resistance, muscle atrophy, and venous thromboembolism.2 Successful early mobilization, however, is influenced by factors such as effective pain control and the timing of urinary catheter removal.1
In gynecologic surgery, particularly total abdominal hysterectomy (TAH), urinary catheterization is routinely performed to prevent bladder injury intraoperatively3,4 and to monitor urinary output postoperatively.2–4 Despite these benefits, prolonged catheterization is associated with increased risks of urinary tract infection (UTI), delayed mobilization, and extended hospital stays. Current ERAS guidelines recommend catheter removal within 24 hours after surgery,5 yet the optimal timing remains unclear. Prior studies have reported mixed findings, particularly when considering variations in anesthetic techniques and perioperative care.6,7
Given these uncertainties, this study investigates the impact of early urinary catheter removal on postoperative recovery, focusing specifically on functional recovery assessed through early ambulation in women undergoing uncomplicated TAH for benign gynecologic conditions.
Materials and Methods
This open-label, randomized controlled trial (RCT) was conducted at University Hospital, Thailand. All eligible participants were fully informed about the study, and written informed consent was obtained prior to enrollment. Women aged 18–65 years scheduled for total abdominal hysterectomy (TAH) for benign gynecologic conditions were recruited between August 2023 and July 2024. Exclusion criteria were: (1) refusal to participate; (2) history of chemotherapy; (3) neurological or spinal cord disorders; (4) pre-existing urinary dysfunction, including incontinence; (5) urinary tract infection confirmed by urine culture or analysis; (6) allergy to opioids, NSAIDs, or acetaminophen; (7) use of intravenous patient-controlled analgesia (PCA); and (8) anticipated catheter removal in the intervention group between 10 p.m. and 6 a.m. Participants were withdrawn if intraoperative complications occurred, including urinary tract or gastrointestinal injury, blood loss exceeding 1000 mL, postoperative intensive care unit admission, or if the operating surgeon requested catheter removal outside the assigned protocol.
Participants were randomized in a 1:1 ratio to either the intervention group (early urinary catheter removal at 12–16 hours postoperatively) or the control group (standard removal at 20–24 hours postoperatively). Randomization was performed using computer-generated numbers with varying block sizes. Allocation concealment was maintained using sequentially numbered, sealed, opaque envelopes.
Sample Size Calculation
The sample size calculation was based on the primary outcome of time to first ambulation, defined as the interval between the end of surgery and the patient’s first walk. A previous study by Chen et al (2022)8 compared early urinary catheter removal (within 6 hours) with standard removal (within 24 hours) in women undergoing gynecologic surgery under general anesthesia and reported a mean ambulation time of 22 hours in the standard group. Considering the inclusion of spinal anesthesia in our study, we hypothesized that early catheter removal at 12–16 hours would reduce the mean time to ambulation by approximately 4 hours compared with the standard group. With a significance level of 0.05 and a power of 90%, the required sample size was calculated to be 43 patients per group. Allowing for a 10% dropout rate, the final sample size was set at 100 patients (50 per group).
Procedures
All patients underwent a baseline six-minute walk test (6MWT)9 one day before surgery. A weight-adjusted dose of cefazolin, or an alternative for allergies, was given as prophylaxis. Following induction of general anesthesia, a 14-Fr Foley catheter was placed under aseptic technique, and total abdominal hysterectomy was performed in the standard manner with continuous bladder drainage. Catheter removal was assigned to either 12–16 hours (intervention) or 20–24 hours (control).
Perioperative and postoperative care followed ERAS protocols,10 including balanced crystalloids, early diet within 24 hours, multimodal analgesia, and mobilization within the first day. After catheter removal, spontaneous voiding was encouraged; inability to void within 6 hours was defined as urinary retention and managed with intermittent catheterization. If residual urine exceeded 200 mL, the catheter was retained for at least 6 hours. Urine culture was obtained if urinary tract infection (UTI) symptoms occurred. The 6MWT was repeated on postoperative days 1 and 2, with pain (VAS)11 and fall risk (Hendrich II)12 assessed beforehand to ensure safety (VAS <6, Hendrich II <5).
Primary outcomes were time to first ambulation and 6MWT distance on days 1 and 2. Secondary outcomes included time to first void, urinary retention requiring re-catheterization, symptomatic UTIs, hospital stay, catheter-related discomfort (VAS), and patient satisfaction (Numerical Rating Scale).13 Hospital stay was measured from surgery to fulfillment of discharge criteria.
Data Collection and Statistical Analysis
Data were collected using structured case report forms and entered into a secure database. Analyses were performed with SPSS software. Continuous variables were summarized as means with standard deviations, and categorical variables as frequencies and percentages. Group comparisons were conducted using Student’s t-test for continuous variables and Chi-square or Fisher’s exact tests for categorical variables. Statistical significance was defined as p < 0.05.
Results
A total of 105 patients were screened, of whom five were excluded for not meeting eligibility criteria or declining participation. The remaining 100 were randomized equally into intervention and control groups. After randomization, seven patients (four in the intervention group and three in the control group) were withdrawn due to intraoperative or postoperative complications (eg, supracervical hysterectomy, bowel injury, excessive blood loss >1000 mL, or hypovolemic shock). The final analysis included 93 patients (46 in the intervention group and 47 in the control group) (Figure 1).
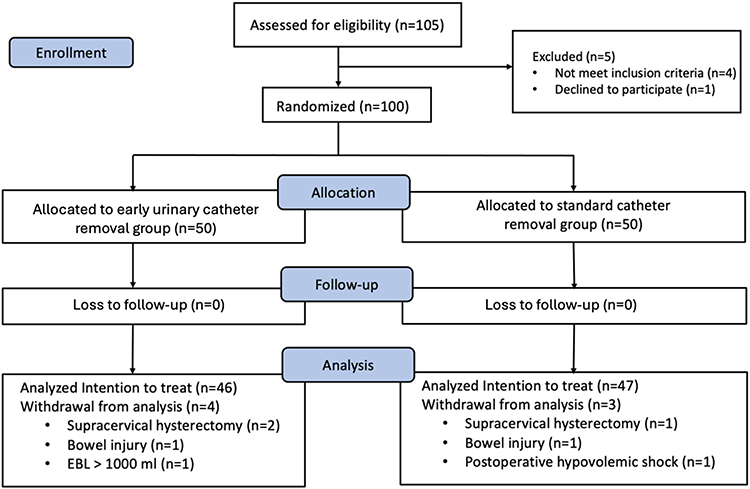 |
Figure 1 Consort flow diagram. |
Baseline demographic and clinical characteristics were comparable between groups (Table 1). Uterine fibroid was the most common surgical indication, accounting for 40% of cases in both groups. Approximately 75% of patients received combined general and spinal anesthesia. Operative duration and estimated blood loss were also similar.
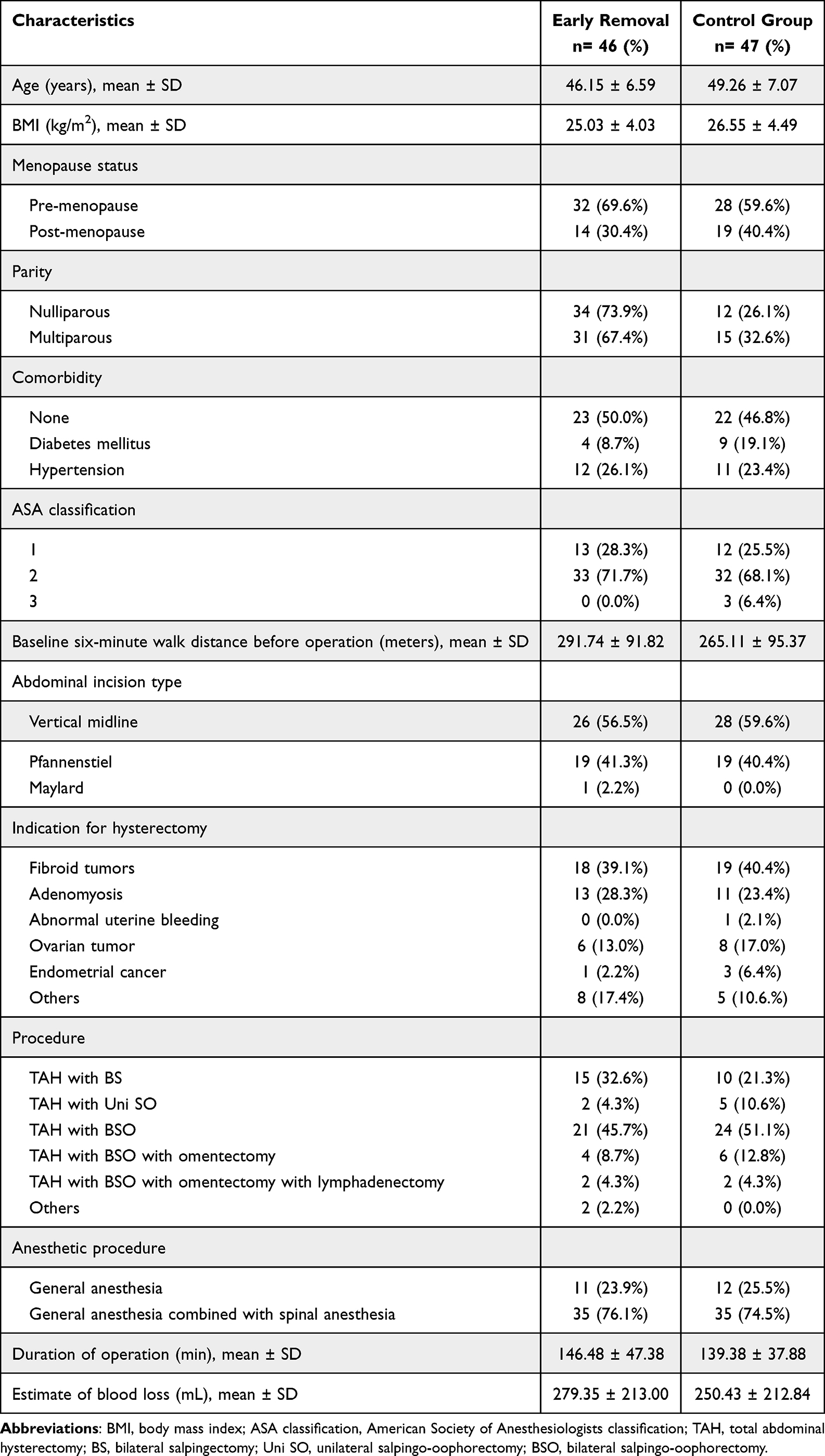 |
Table 1 Patient Baseline Characteristics |
Patients in the early catheter removal group achieved ambulation significantly sooner than those in the control group (18.69 ± 4.11 vs 21.41 ± 3.02 hours, p < 0.001). Six-minute walk distances on postoperative days 1 and 2 were slightly higher in the early removal group but did not differ significantly between groups (p = 0.272 and p = 0.163, respectively). Pre-test pain scores (VAS) on POD1 and POD2 were also comparable (Table 2).
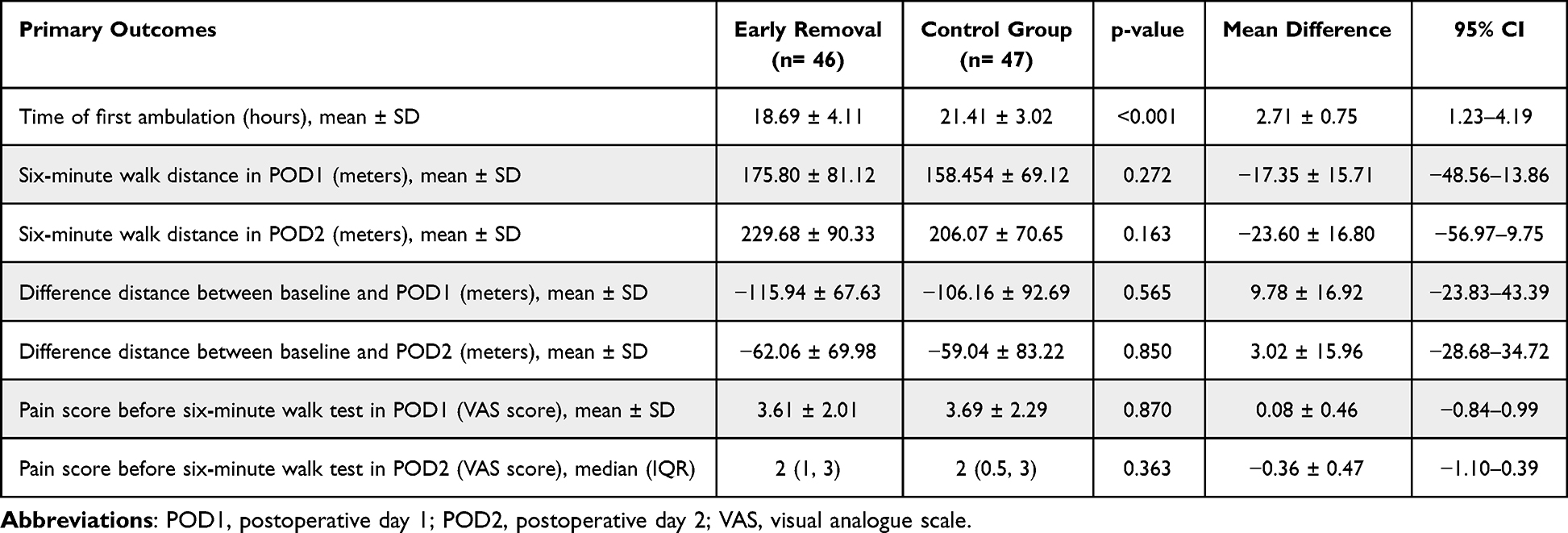 |
Table 2 Primary Outcomes |
Early catheter removal was associated with a shorter time to first voiding (19.02 ± 3.72 vs 21.99 ± 3.46 hours, p < 0.001). Re-catheterization was required in one patient (2.2%) in the early group and none in the control group. Rates of symptomatic UTIs and positive urine cultures were low and not significantly different (Table 3). Length of hospital stay, catheter-related discomfort, hospitalization costs, and overall patient satisfaction (NRS) did not differ significantly between groups.
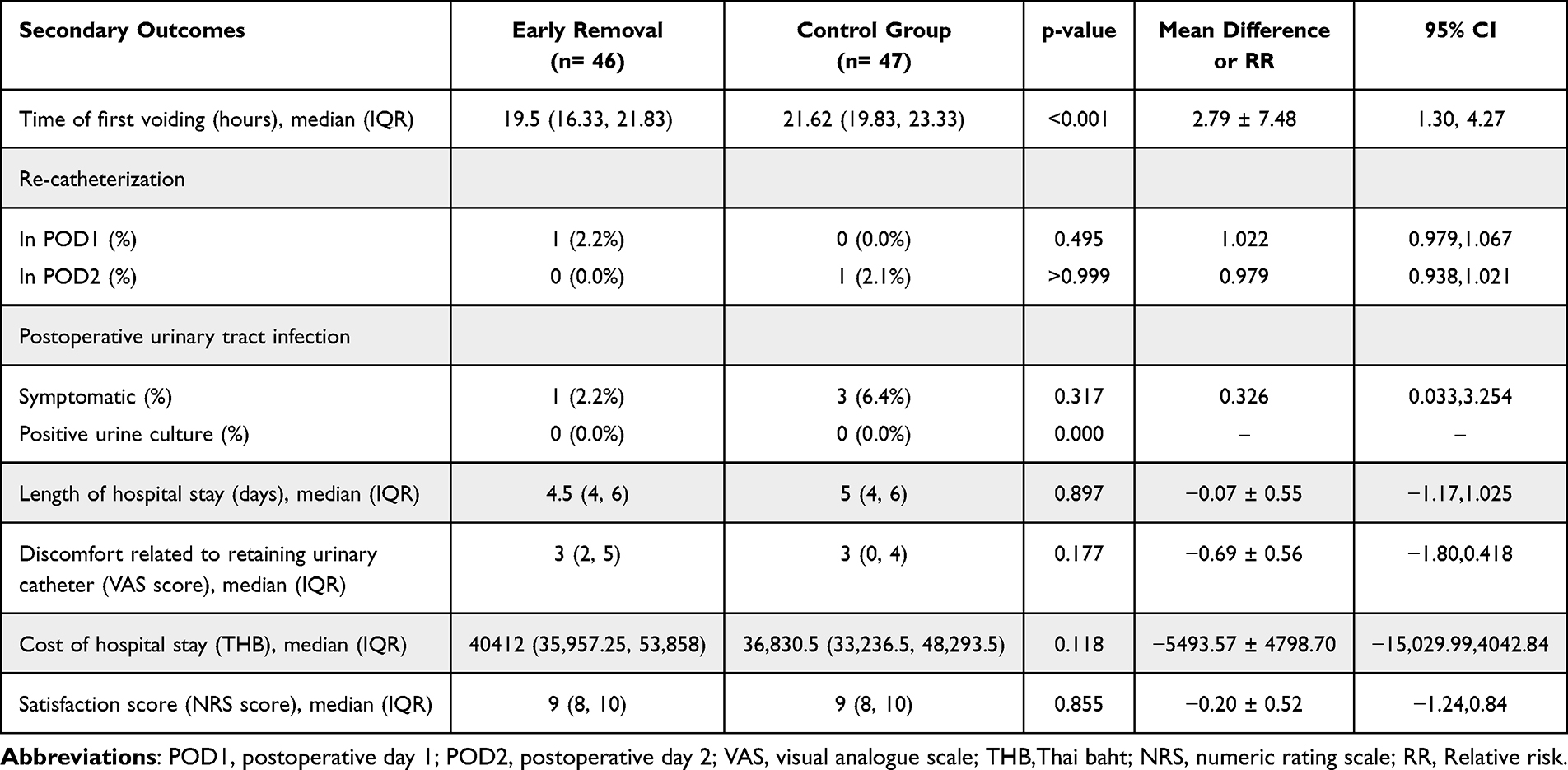 |
Table 3 Secondary Outcomes |
In subgroup analysis by anesthetic technique (Table 4), early catheter removal consistently reduced the time to first ambulation (18.29 ± 3.37 vs 21.60 ± 3.15 hours, p < 0.001) and shortened time to first voiding, without significantly affecting re-catheterization rates.
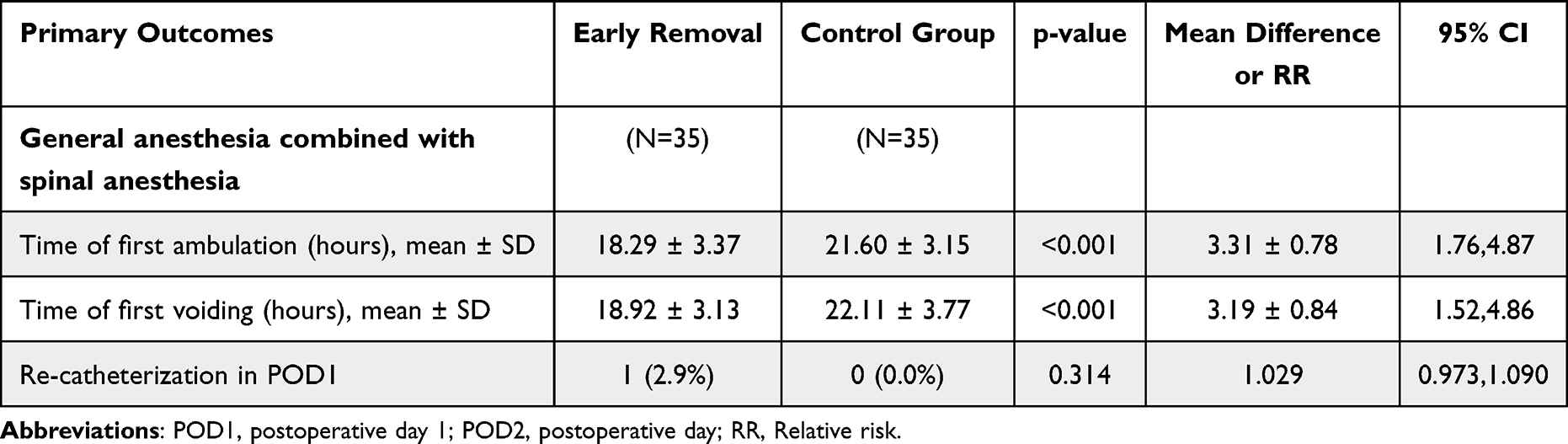 |
Table 4 Subgroup Analysis According to Anesthetic Procedure |
Discussion
The findings of this randomized controlled trial indicate that early removal of the urinary indwelling catheter, within 12 to 16 hours after uncomplicated total abdominal hysterectomy, enhances postoperative recovery without increasing urinary complications. Specifically, early catheter removal significantly reduced both the time to first ambulation and the time to first voiding compared to standard removal at 20 to 24 hours postoperatively.
These results align with previous studies,8 confirming that early catheter removal facilitates earlier mobilization. In our study, the mean time to first ambulation was 18.69 ± 4.11 hours in the early removal group versus 21.41 ± 3.02 hours in the control group (p < 0.001), supporting existing ERAS guidelines that advocate early mobilization to improve postoperative outcomes.10
Similarly, Chiewhatpong et al [2021]14 reported higher six-minute walk distances on postoperative days 1 and 2 in the ERAS group, though differences were not statistically significant. This suggests that while early catheter removal accelerates mobilization, overall functional recovery—as measured by walking distance—remains comparable by the second postoperative day. The lack of significance may be attributed to sample size, interpatient variability, or the short observation period, yet the trend toward improved performance in the early removal group underscores the safety and potential benefits of early ambulation.
A key concern with early catheter removal is the risk of urinary retention and subsequent need for re-catheterization. While some studies6,15,16 have reported higher rates of urinary retention when catheters are removed immediately or within 6 hours after uncomplicated total abdominal hysterectomy, this is not a universal finding.8,17 In the present study, only one patient (2.2%) in the early removal group (12–16 hours postoperatively) required re-catheterization, a rate not significantly different from the control group. Additionally, early catheter removal did not increase the incidence of postoperative urinary tract infections (UTIs), a complication commonly associated with prolonged catheter use. These results are consistent with previous studies3,4,6 demonstrating that early catheter removal can reduce UTI risk. The lack of significant differences in both symptomatic UTIs and re-catheterization rates supports the safety of early urinary catheter removal in patients undergoing uncomplicated total abdominal hysterectomy.
Although early catheter removal led to faster ambulation and voiding, the length of hospital stay was similar between the groups, likely influenced by institutional policies or patient-specific factors rather than the catheter protocol. Consistent with Joshi et al [2014],18 catheter-related discomfort, measured by VAS scores, did not differ significantly between groups. While some previous studies reported that immediate or early catheter removal reduced both time to first ambulation4 and hospital stay,3,8 these effects were not observed in the current study.
Similarly, total hospitalization costs and patient satisfaction were comparable between groups, suggesting that early catheter removal does not increase healthcare expenses or negatively affect patient experience. Notably, patient satisfaction remained high in both groups, with mean NRS scores exceeding 8, underscoring the overall effectiveness of ERAS protocols.
This randomized controlled trial utilized well-defined, objective outcome measures—time to first ambulation, time to first voiding, and six-minute walk distance—strengthening the reliability and clarity of the findings. Randomization helped reduce selection bias, baseline characteristics were balanced between groups, and a low withdrawal rate (<10%) minimized attrition bias. Although participant blinding was not feasible, standardized instructions on early ambulation helped limit measurement bias. Study limitations include its single-center design, which may restrict the generalizability of the findings, and the absence of long-term assessment of urinary outcomes. Furthermore, the results cannot be directly extrapolated to other hysterectomy approaches, such as laparoscopic or vaginal procedures, since the study exclusively involved total abdominal hysterectomy.
Conclusion
Early removal of the urinary indwelling catheter following uncomplicated total abdominal hysterectomy facilitated earlier ambulation without increasing the risk of postoperative complications.
Clinical Trial Registration
The study’s registration number on ClinicalTrials.gov is TCTR20230830002 (The registration date is August 30, 2023), and the first participant enrollment date is August 31, 2023.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Khon Kaen University Ethics Committee for Human Research (HE661140). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
All financial support for this study was provided by the Faculty of Medicine, Khon Kaen University, Thailand.
Funding
This study reports grant from Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand (Grant Number: RA00195).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Tazreean R, Nelson G, Twomey R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J Comp Eff Res. 2021;11(2):121–8. doi:10.2217/cer-2021-0258
2. Nelson G, Bakkum-Gamez J, Kalogera E, et al. Guidelines for perioperative care in gynecologic/oncology: enhanced recovery after surgery (ERAS) society recommendations—2019 update. Int J Gynecol Cancer. 2019;29(4):651–668. doi:10.1136/ijgc-2019-000356
3. Ahmed MR, Sayed Ahmed WA, Atwa KA, et al. Timing of urinary catheter removal after uncomplicated total abdominal hysterectomy: a prospective randomized trial. Eur J Obstet Gynecol Reprod Biol. 2014;176:60–63. doi:10.1016/j.ejogrb.2014.02.038
4. Zhang P, Hu WL, Cheng B, et al. A systematic review and meta-analysis comparing immediate and delayed catheter removal following uncomplicated hysterectomy. Int Urogynecology J. 2015;26(5):665–674. doi:10.1007/s00192-014-2561-0
5. Nelson G, Altman AD, Nick A, et al. Guidelines for postoperative care in gynecologic/oncology surgery: enhanced recovery after surgery (ERAS®) society recommendations — part II. Gynecol Oncol. 2016;140(2):323–332. doi:10.1016/j.ygyno.2015.12.019
6. Huang H, Dong L, Gu L. The timing of urinary catheter removal after gynecologic surgery. Medicine. 2020;99(2):18710. doi:10.1097/MD.0000000000018710
7. Zanfini BA, Paradisi G, Savone R, et al. Bladder function after spinal anesthesia for cesarean section: an urodynamic evaluation. Eur Rev Med Pharmacol Sci. 2012;16(11):1525–1529.
8. Chen SF, Wang PH, Kuo SC, et al. Early and standard urinary catheter removal after gynecological surgery for benign lesions: a quasi-experimental study. Clin Nurs Res. 2022;31(3):489–496. doi:10.1177/10547738211044500
9. Pecorelli N, Fiore JF, Gillis C, et al. The six-minute walk test as a measure of postoperative recovery after colorectal resection: further examination of its measurement properties. Surg Endosc. 2016;30(6):2199–2206. doi:10.1007/s00464-015-4478-1
10. Nelson G, Fotopoulou C, Taylor J, et al. Enhanced recovery after surgery (ERAS®) society guidelines for gynecologic oncology: addressing implementation challenges - 2023 update. Gynecol Oncol. 2023;173:58–67. doi:10.1016/j.ygyno.2023.04.009
11. Bodian CA, Freedman G, Hossain S, et al. The visual analog scale for pain: clinical significance in postoperative patients. Anesthesiology. 2001;95(6):1356–1361. doi:10.1097/00000542-200112000-00013
12. Hendrich AL, Bufalino A, Groves C. Validation of the Hendrich II fall risk model: the imperative to reduce modifiable risk factors. Appl Nurs Res. 2020;53:151243. doi:10.1016/j.apnr.2020.151243
13. van Berckel MMG, Bosma NH, Hageman MGJS, et al. The correlation between a numerical rating scale of patient satisfaction with current management of an upper extremity disorder and a general measure of satisfaction with the medical visit. Hand NYN. 2017;12(2):202–206. doi:10.1177/1558944716662019
14. Chiewhatpong P, Charoenkwan K, Smithiseth K, et al. Effectiveness of enhanced recovery after surgery protocol in open gynecologic oncology surgery: a randomized controlled trial. Int J Gynecol Obstet. 2022;159(2):568–576. doi:10.1002/ijgo.14211
15. Liao X, Xie L. A systematic review and meta-analysis of the timing of indwelling catheter extubation in patients undergoing gynecological and obstetric surgery. Ann Palliat Med. 2021;10(12):12519–12528. doi:10.21037/apm-21-3290
16. Rimmer MP, Henderson I, Keay SD, et al. Early versus delayed urinary catheter removal after hysterectomy: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2020;247:55–60. doi:10.1016/j.ejogrb.2020.01.011
17. Fu CY, Wan L, Shen PY, et al. Feasibility of immediate removal of urinary catheter after laparoscopic gynecological surgery for benign diseases: a meta-analysis of randomized controlled trials. Int J Gynecol Obstet. 2022;159(3):622–629. doi:10.1002/ijgo.14283
18. Joshi B, Aggarwal N, Chopra S, et al. A prospective randomized controlled comparison of immediate versus late removal of urinary catheter after abdominal hysterectomy. J Life Health. 2014;5(2):68. doi:10.4103/0976-7800.133990
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.